
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 06 March 2024
Sec. Adolescent and Young Adult Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1324220
 Brigitte Gerstl1,2Bright Opoku Ahinkorah1,2,3
Brigitte Gerstl1,2Bright Opoku Ahinkorah1,2,3 Thomas P. Nguyen1,2,4
Thomas P. Nguyen1,2,4 James Rufus John1,2
James Rufus John1,2 Patrick Hawker1,2Teresa Winata1,2,5Febe Brice1Michael Bowden6,7,8
Patrick Hawker1,2Teresa Winata1,2,5Febe Brice1Michael Bowden6,7,8 Valsamma Eapen1,2,3*
Valsamma Eapen1,2,3*Background: Long term intervention services have proven to be effective in improving mental health (MH) outcomes and the quality of life for children and young people (CYP).
Aim: To synthesize evidence on the effectiveness of long-term interventions in improving MH outcomes for CYP, 0-17 years, presenting with MH conditions.
Methods: A systematic search was carried out and the methodological quality of included long term MH intervention studies were assessed. Six databases were searched for peer-reviewed articles between January 2000 and September 2022.
Results: We found 30 studies that reported on the effectiveness of a range of long-term MH interventions in the form of (i) group therapy, (ii) multisystemic behavior therapy, (iii) general services, (iv) integrated services, (v) psychotherapy, (vi) intensive intervention services, (vii) comprehensive collaborative care, (viii) parent training, and (ix) home outreach service. Among the included studies, seven were rated as high level of evidence based on the National Health and Medical Research Council (NHMRC) levels of evidence hierarchy scale and seven were of moderate quality evidence. Others were rated as lower-quality evidence. Among the studies providing high quality evidence, most were reported for group therapy, general services, and psychotherapy studies demonstrating beneficial effects.
Conclusion: This systematic review provides evidence to demonstrate the benefits of a range of long-term interventions, in a range of settings, can be effective in improving MH outcomes for CYP and their families.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022323324.
Mental health (MH) conditions comprise a broad spectrum of disorders affecting a child and young person’s (CYP) mood, thinking, and behavior. These conditions include chronic and long-term disorders that require sustained interventions and support, addressing the unique challenges faced by CYP over an extended period. MH problems are prevalent among CYP worldwide with 8.8% of CYP having received diagnoses for diverse mental health conditions, imposing a significant burden on public health (1). Available evidence suggests that most common MH disorders in CYP include anxiety, conduct, major depression and mood disorders, and attention-deficit/hyperactivity disorder (ADHD) among others (2–4). Thus, the escalating global prevalence of MH disorders highlight the urgent need for enhanced prevention and treatment strategies.
Acute MH needs in CYP present is characterized by significant and distressing symptoms that require prompt attention and targeted interventions. Acute presentations may include psychosomatic symptoms such as headaches, abdominal pain or discomfort associated with altered bowel function, fatigue, and chronic functional gastrointestinal disorders (such as irritable bowel syndrome) (5). These symptoms, particularly prevalent among school-aged children, significantly contribute to the overall burden of MH challenges (6) They often serve as early indicators of acute distress and require careful consideration in the context of intervention strategies. Epidemiological studies on childhood headaches from around the world report widely variable prevalence rates, with an estimated median frequency of headaches in children and adolescents at 58.4%, ranging from one-month to a lifetime prevalence (7, 8). Approximately 31.5% of children in primary and secondary schools experience headaches twice a month or more over a three-month period (9).
Attention Deficit Hyperactivity Disorder (ADHD), as a prevalent and persistent developmental disorder, exemplifies the need for acute interventions. Characterized by excessive inattention, hyperactivity, or impulsivity, ADHD becomes particularly discernible in the school-age years (10).
To address acute MH needs, it is important to delve into the prevalence of acute presentations, the potential consequences if untreated, and common categories of interventions. Recent international meta-analyses have highlighted increased rates of MH conditions among CYP, emphasizing the urgency of addressing acute presentations (11, 12). The Covid-19 pandemic further emphasized the significance of acute MH interventions, with CYP facing heightened risks during lockdowns, disruptions to education, and increased exposure to stressors (13–17).
There exists a substantial body of research linking poor MH to increased morbidity (12, 13), which can markedly impair quality of life and promote susceptibility to various physical and psychological health issues (18). Furthermore, MH problems are the leading cause of disability among young people (YP) globally, accounting for 45% of disability-related years lost (19). MH issues, if untreated, have the potential to significantly disrupt the wellbeing of children within their homes, schools, and communities. There are several interventions available for addressing MH challenges among CYP. These interventions span psychosocial programs, school-based initiatives, and parent and family-focused strategies, including psychoeducation, skills training, and cognitive-behavioral therapy (CBT). The inclusion of these varied approaches reflects the diverse landscape of interventions aimed at enhancing the mental well-being of CYP. Without proper intervention, CYP facing MH challenges are more prone to academic struggles, involvement with the criminal justice system, reliance on social services, and, in severe cases, the risk of suicide (20, 21). Studies have shown that severe MH issues, including self-harm and suicide among YP (21, 22) are difficult to treat once they have been established. This in turn can cause significant ongoing impacts well into adulthood (23). Hence, it is critical to have systems in place for early identification and treatment of MH conditions to prevent persistence into adulthood.
Besides ongoing MH morbidity for CYP, there is also a significant economic burden on the healthcare system due to high rates of hospital admissions, Emergency Department (ED) presentations, and re-presentations (24, 25). It is estimated that one in seven (14%) CYP aged between 4 and 17 years in Australia (2, 3) have a MH disorder with a recent Australian study estimating the annual incremental healthcare costs related to MH for CYP aged 4-17 years to be $AU234 million (26). In response to the growing demand for MH care among CYP, various preventive interventions, including school-based programs, have been implemented across different settings, yielding positive impacts on the wellbeing of CYP by reducing depression and anxiety through the provision of coping strategies and interventions (27). Moreover, a broad range of intervention approaches, including psychosocial interventions, have been successfully implemented in a variety of health and community settings (22, 28–32). Additionally, parent and family-focused interventions (including psychoeducation, parent and family-skills training, behavioral, psychosocial, and cognitive behavioral therapy [CBT]) are known to be efficacious in improving CYP’s MH outcomes as well as parenting behaviors and family functioning (30, 33).
Considering the prevailing burden and impact of MH disorders among CYP, it is important to identify effective interventions for MH needs. The aim of this study was to assess the effectiveness of long-term interventions specifically tailored for CYP with acute mental health needs, highlighting the need for a comprehensive understanding and addressing both immediate crises and sustained support in CYP aged 0-17 years.
This study was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (34). A protocol for the study has been developed and registered on the Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42022323324).
This systematic review utilized six electronic databases to extract studies reporting on the effectiveness of long term (definition below) interventions for MH presentations of CYP aged 0 to 17 years. Articles were searched with date restrictions from January 2000 to March 2022. Articles were limited to the English language. Duplicated studies were removed using Endnote and again in Rayyan software for systematic reviews (35).
The following databases were searched: (1) PubMed; (2) Ovid PsycINFO; (3) Web of Science, via Clarivate; (4) EMBASE; and (5) Cochrane Library. We also searched the reference lists of included studies to identify further relevant literature. The full search strategy is included in Supplementary 1.
The inclusion criteria were as follows: (1) the study reported on the effectiveness of a long-term intervention on MH outcomes for CYP presenting with an acute MH condition. In this review, ‘acute mental health needs’ were defined as instances where a CYP experienced a sudden decline in their MH, often accompanied by significant distress and impaired functioning that required urgent medical attention or intervention in any setting, i.e., hospital or ED). Additionally, long-term interventions were defined as treatment for MH concerns in CYP that lasted for more than eight weeks or involved more than three visits; (2) the age of participants ranged between 0 to 17 years, or where the age range was not reported, the participant’s mean age was less than 18 years; and (3) studies published in the English language.
The following studies were excluded: (1) participant age criteria were not met (participants > 18 years of age); (2) participants were not presenting/attending a long-term intervention for the treatment of a MH condition, (3) the study focused solely on a short-term school-based programs or residential programs that did not meet the definition of long-term interventions; (4) the study focused exclusively on short-term parent-focused interventions, such as shorter duration parent peer support programs, that did not meet the criteria for long-term interventions; (5) the study focused on interventions provided exclusively through justice systems or child welfare systems; (6) the study was a quantitative meta-analysis of published literature, editorial, or scoping review; and (7) the study was not published in English.
Four reviewers (FB, BG, PH, JRJ) independently performed initial title and abstract screening. Two reviewers (FB, PH) independently conducted full-text screening and compared results. A fifth reviewer (TW) was available to resolve or moderate any disagreements about the included articles. Four reviewers (FB, BG, PH, BOA) performed data extraction for the included articles and retrieved full-text reports using a data collection tool.
Table 1 provides a comprehensive overview of each of the included studies, with detailed descriptions of the studies, NHMRC levels of evidence and risk of bias, interventions examined, and the results reported. Among included studies, 7 studies were rated as providing high level of evidence based on the NHMRC levels of evidence hierarchy scale (36–42) followed by 7 studies which were rated as moderate quality evidence (43–49), and 16 articles were of lower quality (50–65). There was considerable variability between study methodologies with nearly half (46%, n=14/30 studies) of the studies used a control group to compare outcomes (36–49) (see Table 1). Where high quality RCT studies were reported, we only present these studies under each of the sub-headings as per the type of interventions (see Table 1).
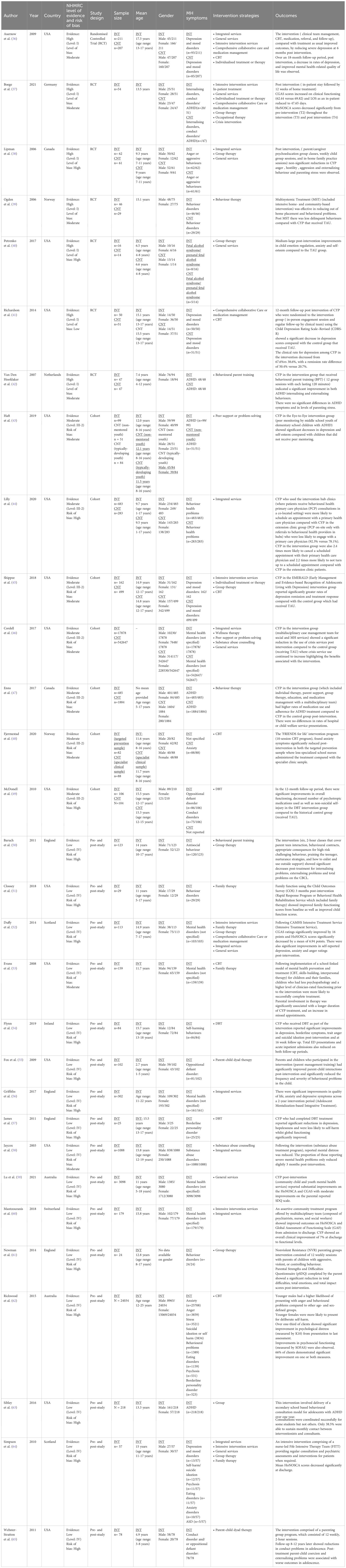
Table 1 Characteristics of long-term intervention studies (n=30 studies).
Further details describing quality assessment, data extraction and Risk of Bias can be found in Appendices 1-3.
This evaluation included identifying effective interventions (mechanisms), their outcomes, and the specific settings and locations (context) in which the interventions were implemented (66).
Our initial search yielded 4,892 results, of which 3,242 were removed as duplicates, resulting in 1,650 articles that were then reviewed. After title and abstract screening, 436 potential studies were assessed for eligibility of full-text screening, and 30 studies met the eligibility criteria. The systematic review process, using the PRISMA flowchart, is depicted in Figure 1.

Figure 1 Prisma statement.
Table 2 summarizes characteristics of the included studies. Studies were conducted in various geographical regions; including the USA (n=14) (36, 40, 41, 43–46, 49, 51, 53, 55, 58, 63, 65), England (n=4) (50, 56, 57, 61), Canada (n=2) (38, 47), Australia (n=2) (59, 62), Norway (n=2) (39, 48), Scotland (n=2) (52, 64), Germany (n=1) (37), Netherlands (n=1) (42), Ireland (n=1) (54), and Switzerland (n=1) (60).
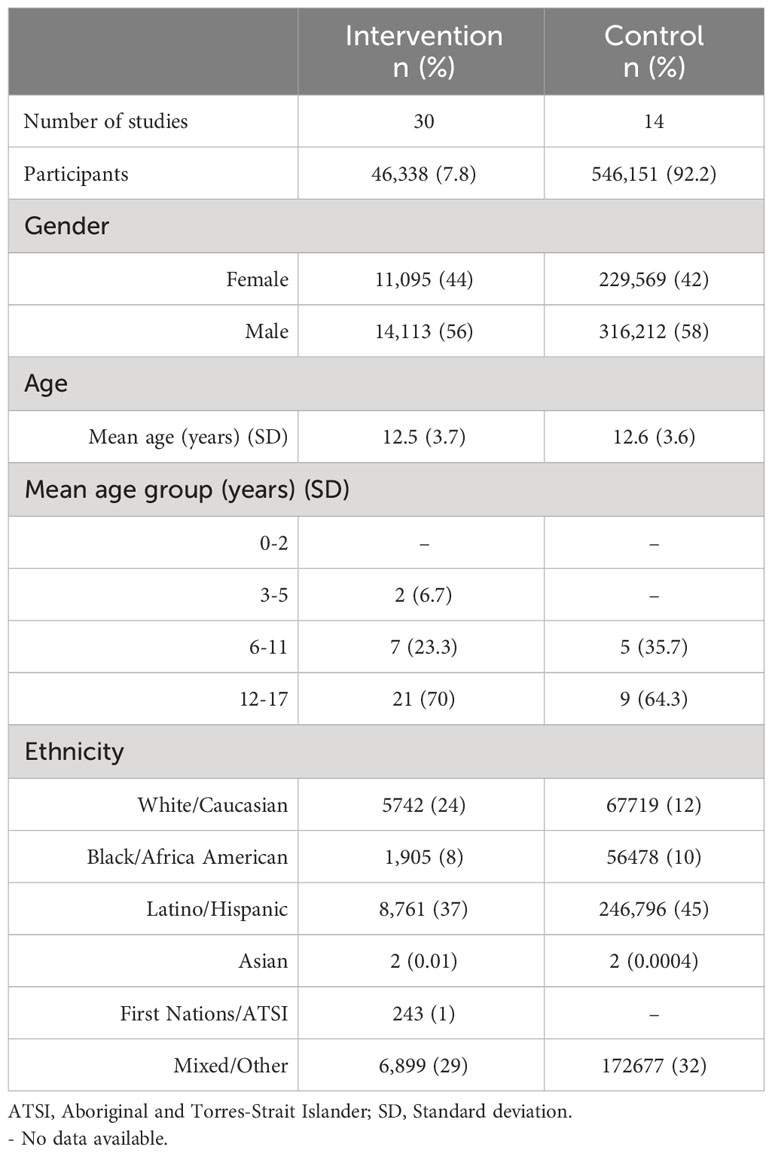
Table 2 Demographic characteristics of participants from the included studies.
Effect of interventions on mental health symptoms
Using a narrative approach, we categorized intervention types according to the following sub-headings described in this section (Table 1).
There were six studies (20%) (RCT (n=1) (38), pre- and post (n=4) (51–53, 64), cohort (n=1) (47) studies) that reported on group therapy interventions. The number of group sessions ranged from between 8-12 sessions over a duration of 13-30 weeks. An RCT (38) of high quality NHMRC evidence, although at a high level of risk of bias, used an adapted, manual-based group CBT program where children were taught problem-solving techniques to manage their temper. The intervention also included parent/caregiver psychoeducation/skill-building group sessions and three in-home family practice sessions to support primary school aged CYP (aged between 7 to 11 years of age) and their families. The RCT found no significant differences and small effect sizes between both groups for all primary outcomes (e.g., child anger and child aggressive behavior). However, the magnitude of improvement (difference scores) was greater in the intervention group on parent-rated measures such as Child Behavior Questionnaire, Parenting Stress Index-Short Form (PSI-SF), compared with the control group (38).
An RCT study (39), of high-quality NHMRC evidence with moderate risk of bias examined the effectiveness of a multisystemic treatment (MST) in reducing behavior problems and preventing out-of-home placement, compared to Regular Child Welfare Services (RS). An assessment was administered at the time of entry into the study (prior to randomization) and after completion of MST treatment (average treatment time was 24.3 weeks, with a range of 7-38 weeks) or approximately 6 months after the intake of the RS group. The results indicated that MST participants were less likely to have left their home compared with RS youth. About 72% of MST and 52% of RS youth lived at home or were under supervision at follow-up. Additionally, YP in the MST group also scored significantly lower on the Self-Report Delinquency Scale (SRD) compared with youth who received RS (39).
General services included psychiatric evaluations and treatment, regular review of MH treatment plans, psychosocial treatment and psychoeducation for families and parents. Among the reviewed studies, eight studies (27%) [cohort studies (n=1) (46), RCT (n=3) (36, 40, 47), pre-and post-studies (n=4) (52, 59, 62, 64)] reported on general services. The duration of general service interventions ranged from 4-10 months. CYP aged between 6-11 years, who engaged with general service interventions had ADHD (47), anger (38), aggression (38) or fetal alcohol spectrum disorders (FASDs) (40). YP aged 12-17 years, receiving general services, presented with a range of MH symptoms such as anxiety (62, 64), aggression (62), ASD (42), behavioral disorders (62), borderline personality disorder (62), depression and mood disorders (36, 62, 64), eating disorders (62, 64), psychosis (62, 64), and self-harm/suicide ideation (62, 64).
One RCT study evaluated the effectiveness of the ‘Families on Track’ Program, designed for children aged 4-8 years with fetal alcohol spectrum disorder. Despite the high risk of bias, the study was considered to provide high-quality evidence. The program’s outcomes were compared to a control group that received a neuropsychological evaluation and a community referral (40). The ‘Families on Track’ program included a diagnostic and neuropsychological evaluation, as well as separate a 30-week program for children and caregivers. Children’s program aimed to develop social competence, while caregivers’ program focused on modifying parenting attitudes through CBT and motivational interviewing strategies. The intervention significantly improved emotional regulation in children, as reported by caregivers. Compared to the control group, the intervention group exhibited a medium-to-large effect size, while the control group showed a medium-sized decline (Emotion Regulation Checklist [ERC] = 1.18). Caregiver-reported self-esteem and anxiety also showed a medium-to-large group effect size (Impairment Rating Scale [IRS] self-esteem = 0.77), although statistical significance was not reached.
A high-quality RCT with moderate risk of bias assessed the long-term stability of CYP with depressive symptoms receiving home treatment (HT) versus a control group undergoing inpatient treatment-as-usual (TAU) (37). HT proved effective, with fewer intervention group patients requiring ambulatory care post-discharge (37.5% vs. 50%), indicating greater stability and reduced outpatient needs. After 4.3 years, 70% of intervention group parents were satisfied, compared to 36.8% in the control group. Furthermore, 43.7% of HT parents found the professional assistance and advice received at home valuable (37).
From the synthesized studies, a total of nine studies focused on a range of integrated services (30%) (pre-and post (n=5) (44, 52, 56, 60, 64), RCT (n=1) (36), cohort (n=3) (46, 47, 58). The duration of all integrated services ranged from 15-35 weeks. CYP (6-11 years) were accessed for ADHD (47), anger (38), aggression (38), and behavioral problems (44). YP (11-17 years)received integrated interventions for adjustment disorder (46), anxiety disorders (52, 60, 64), ASD (46, 64), behavioral disorders (39), conduct disorders (46, 60), depression and mood (46, 52, 60), eating disorders (52, 64), personality disorders (60), psychosis (46, 60, 64), substance use (46, 58), and self-harm/suicide ideation (52, 64, 67).
A high-quality RCT with moderate risk of bias evaluated the outcomes of a primary care quality improvement intervention for YP (aged 13-21 years) with depression and compared to a control group that received TAU (36). The intervention, led by a clinical care manager, included consumer education, pharmacological and psychosocial treatment, CBT training, and treatment modality choice. Severe depression scores decreased at 6 months but did not significantly differ from the control group at 18 months. Recovery time was 8.76 months (SD=0.35) for the intervention group and 9.65 months (SD=0.37) for the control group (36).
There were seven studies (23%) [pre-and post (n=5) (45, 48, 53, 57, 62), RCT (n=2) (36, 41)] that explored CBT-based programs for CYP (ages 8-16 years). Most YP (12-17 years) accessed CBT for anxiety (48, 62), aggression (62), behavioral disorders (62), borderline personality disorder (57, 62), depression and mood disorders (36, 41, 45, 62), eating disorders (62), and psychosis (62). There were two RCT studies (36, 41) that reported the effective benefits associated with CBT. One study has been discussed elsewhere given that the intervention reported involved a combination of other MH modalities (i.e., integrated services).
One RCT examined cognitive-behavioral therapy (CBT) sessions and follow-up over six months (36) and compared outcomes with a control group who had received TAU. Results indicated that YP receiving CBT recovered nearly one month earlier (8.76 vs. 9.65 months) than the control group (n=43%). Although not statistically significant, the recovery occurred almost one month (~27 days) earlier in the intervention group.
Three studies (7%) (49) evaluated DBT outcomes in YP (ages 12-17) with borderline personality disorder (BPD) (49), oppositional defiant disorder (ODD) (49), conduct disorder, depression, post-traumatic stress disorder (PTSD), and suicidal tendencies (40, 49, 60). A moderate-quality cohort study (n=41) demonstrated DBT’s efficacy in community MH settings. In this study, YP receiving DBT showed a significant increase in in Children’s Global Assessment Scale (CGAS) scores (mean change=14.14, p<0.001) and lower rates of suicidal/self-harm behavior (49, 54), over 12 months compared to controls (49). Limitations include the historical control group’s limited data.
Five studies (17%) examined intensive intervention services for CYP (ages 7-17) with various MH concerns, including anxiety (62, 64), aggression (62), ASD (64), behavioral disorders (62), depression and mood disorders (36, 45, 62, 64), eating disorders (62, 64), psychosis (62, 64), and self-harm/suicide ideation (62, 64). A community outreach program (Child and Adolescent Mental Health [CAMH]) showed a significant reduction in Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA) scores (mean change: 6.94, p<0.001) and a 65% clinical improvement in 65% of CYP (mean CGAS increase: 16.4 points, p<0.001). Another study demonstrated a substantial decrease in HoNOSCA scores (mean decrease: 10.95, p<0.001) over 23.6 weeks for CYP with mood disorders and self-harm behaviors (57). Additionally, this study also revealed that the analysis of changes using the World Health Organization Quality of Life Instrument (WHOQoL-BREF) indicated significant improvements in psychological (mean: 33.43 to 50.09), physical (mean: 53.43 to 65.26), and environment (mean: 70.0 to 77.87) functioning (64).
Five studies (17%) examined pharmacotherapy for CYP (ages 7-17) primarily targeting depression and mood disorders (36, 41, 45, 52). A high-quality RCT demonstrated the effectiveness of a collaborative care intervention, including antidepressant medications and CBT, for youth aged 13-17 with depression (41). Patients in the intervention group showed a significant decrease in Child Depression Rating Scale-Revised (CDRS-R) scores compared to the control group at 6 months (p<0.001) and 12 months (p<0.001), indicating higher rates of response (67.6% vs. 38.6%) and remission (50.4% vs. 20.7%) (44).
Two studies explored the effectiveness of behavioral parent training (BPT) interventions (42, 50). One RCT study involving children diagnosed with ADHD (42), 12-week group sessions (which comprised of 2 hours of 12-week group sessions over a 5-month period) led to significant improvements in internalizing and externalizing behaviors. While ADHD symptoms and parenting stress remained stable, the reduction in behavioral challenges substantiated the intervention’s effectiveness (42). The other RCT targeted parents of YP with conduct problems and reported notable reductions in internalizing and externalising problems among their adolescent children post-intervention (intervention consisted of 12 parents who underwent six, 2-hour classes covering a range of parent-teen behaviours) (50) (Table 1 details further information about this study). After the program, internalizing problems (Cohen’s d = 0.61) shifted from clinical to non-clinical levels (below 60), while externalizing problems (d = 0.73) remained within the clinical range. Total problem scores transitioned from clinical to borderline range (below 63) with a Cohen’s d of 0.79 (50).
Moreover, the National Longitudinal Survey of Youth (NLSY) study evaluating a parenting program for children diagnosed with Oppositional Defiant Disorder (ODD) and/or conduct disorder provided significant evidence (65). Follow-up data encompassed children aged 3-8 years. Compared with the control group, the intervention group exhibited a higher likelihood of reporting delinquent acts (84% versus 67%), with a lower frequency (42 acts versus 54 acts) (48). Additionally, the intervention group demonstrated reduced rates of sexual activity compared to the control group (21% versus 47.8%). Notably, children in the intervention group with non-clinical ECBI problem scores post-treatment displayed fewer delinquent acts in adolescence compared to those with clinical scores (t (57) = 4.52, p <.001).
A RCT study, deemed of high-quality evidence with moderate risk of bias, reported outcomes of a home treatment intervention for CYP (37). CYP in the intervention group received a shortened inpatient stay (mean = 47.7 days) where discharge was determined by stability in level of functioning. This was followed by 12 weeks of home treatment including case management, psychoeducation, and therapy sessions. and up to three appointments a week. Patients also received supportive therapies (e.g., occupational and music therapy) and had access to crisis management services. Control group CYP had standard inpatient stays (mean = 69.4 days) with similar therapies. Four-year follow-up revealed stable treatment effects in both groups. Parents of intervention CYP expressed higher satisfaction, indicating home treatment as a promising alternative to standard inpatient care (37).
The aim of this study was to evaluate the effectiveness of long-term interventions in enhancing continuity of MH care and reducing crises among CYP. This systematic review encompassed diverse interventions in various settings for CYP facing MH conditions. To translate these findings into actionable strategies, critical considerations emerged. Considerations emerged to translate these findings into strategies, presenting a spectrum of long-term strategies. This review covered a broad spectrum of long-term interventions for CYP with MH conditions across diverse settings.
Among long term interventions presented, group therapy (i.e., anger management group therapy), general services (i.e., psychiatric evaluations), integrated services (i.e., linkage with specialty MH and community services), and various forms of psychotherapy (i.e., individual and group sessions) were commonly reported. Interventions using psychotherapy (combining therapeutic approaches such as, family therapy, DBT and CBT group sessions, and parent-child dyad sessions) provided evidence suggesting potential benefits for improving overall psychological outcomes for CYP and their families/caregivers.
Similar findings reported in this study have also been reflected in other systematic reviews by Pilling et al. (32), Piquero et al. (68) and Perderson at el (33). This study substantiates the effectiveness of parent training programs in reducing high-risk challenging behavior for CYP diagnosed with ADHD, emphasizing the effectiveness of psychotherapeutic approaches and parent training programs in managing challenging behaviors, particularly in those diagnosed with ADHD.
Evidence from this study reinforces the efficacy of CBT and family/group-focused interventions in effectively managing anger and aggressive behaviors among CYP. These results align with previous systematic reviews conducted by Das et al. (22) and Pederson et al. (33). Moreover, this study revealed a reduction in delinquent and emotional behaviors among CYP undergoing MST compared to those receiving TAU. However, despite the positive outcomes observed in this study, a systematic review by Littell et al. (65) did not find substantial evidence indicating that MST confers significant advantages over other mental health treatment interventions.
Group therapy emerged as a pivotal intervention, especially in addressing MH challenges among adolescents at high risk of suicide McCauley et al. (69) emphasized the positive outcomes of DBT within a group setting, indicating the potential impact of group therapy in complex MH scenarios. Moreover, the versatility of group therapy extends to the realm of treatment-resistant psychosis, as reported by Polese et al. (70) in their systematic review. They suggested that psychotherapy interventions, including group therapies, could be considered in the context of treatment-resistant psychosis, supporting the broader applicability of group therapy in challenging clinical scenarios.
Recognizing the collaborative and supportive environment that remains integral to group settings is important. This collaborative approach plays a role in achieving therapeutic breakthroughs, especially in challenging clinical scenarios. This review aligns with a growing body of evidence, suggesting that group therapy holds promise not only in conventional psychiatric treatments but also in situations where individuals exhibit heightened risk factors or are not suitable for standard interventions.
Furthermore, the evidence indicates that DBT interventions are effective in mitigating self-harm and suicidal ideation among YP. This aligns with outcomes reported in reviews by DeCou et al. (71), Witt et al. (72), and Hawton et al. (73), all indicating the effectiveness of DBT interventions in reducing suicide-related outcomes. These interventions have shown to decrease the necessity for crisis intervention services. Collectively, the evidence from these systematic review’s advocates for the use of DBT as a promising intervention for YP exhibiting suicidal or self-harm behaviors.
In relation to the duration of psychotherapeutic interventions, it is important to take into consideration the varied temporal scopes inherent in different therapeutic modalities. While our study primarily focused on extended psychotherapeutic interventions exceeding 8 weeks, it is essential to acknowledge the efficacy of psychodynamic psychotherapy with CYP, often requiring a longer duration. A recent systematic review by Midgley et al. (74) evaluated the evidence base for psychodynamic therapy. Their synthesis of findings highlights the effectiveness of psychodynamic therapy in addressing a broad range of MH challenges, particularly internalizing disorders like depression and anxiety, emerging personality disorders, and adversity-experienced children. Importantly, the review reveals that psychodynamic psychotherapy, a modality efficient in these contexts, frequently extends beyond the 8-week benchmark. This emphasizes the necessity of tailoring therapeutic durations based on specific goals and individual needs.
This systematic review has several strengths. We used a priori library search strategy with the use of six databases, with well-defined inclusion and exclusion criteria for the studies. The screening process, as well as the evaluation of risk of bias and NHMRC assessment, involved independent reviewers, ensuring rigorous methodology.
In considering the limitations of this study, it is important to acknowledge that certain studies were classified under multiple categories. This suggests interrelatedness rather than complete independence, as delineated in the text (75). There was also a lack of standardized interventions and outcomes, which precluded meta-analysis. Additionally, we only included studies published in English and did not explore the grey literature. Further high-level, high-quality research using standardized outcome measures is required to support these findings and determine key parameters, such as an optimal frequency and duration for long term intervention programs.
While conducting this systematic review, there is the potential bias associated with encompassing the term CYP. Adolescence, representing a distinct phase marked by biological, social, and role transitions, challenges the homogeneity of the term ‘CYP’ (76). Acknowledging the inherent differences between children and adolescents is crucial, both in clinical practice and research. Sawyer et al. (76) propose an expanded definition of adolescence up to the age of 24, aligning more closely with the extended period of growth and social role transitions. Despite employing the term ‘CYP’ in line with common usage, it is essential to recognize the potential heterogeneity within this broad categorization. Future research should explore age-specific nuances in MH interventions, contributing to more targeted and effective interventions.
There is a need for high-quality, large-scale RCT studies to discern the effectiveness of interventions with long term follow-up data. For example, we presented outcomes associated with parenting programs, however as the studies were of low-quality evidence, a RCT would be required to substantiate the efficacy of the programs. Further, as most studies had well defined, protocol-driven, and well-supervised care (32), evidence for scaling-up and sustainability of MH interventions in lower sociodemographic areas needs to be strengthened (27). Additionally, we did not review any health economic outcomes, further research would be required to determine the cost-effectiveness of different long-term interventions across a wide spectrum of MH symptoms, severity levels, and age groups.
Future research into the benefits of long-term MH interventions, would be required to evaluate the effects of each intervention with a comparison group with consistent and standardized measurement tools, in addressing the specific outcomes of interest.
This systematic review focused on evaluating the impact of long-term interventions designed for CYP experiencing both acute and long-term MH crises. The findings offer insights to inform the development of comprehensive interventions for CYP with MH concerns and their families/caregivers. Our results demonstrate that collaborative care services, CBT, family group-focused interventions, MST, and parent training programs are effective in enhancing MH outcomes for CYP across various outpatient settings, including community services and in-home care. Importantly, these interventions have shown promising reductions in hospital readmission rates, suggesting their potential to mitigate the need for acute inpatient care.
However, the feasibility and acceptability of interventions with lower quality evidence among CYP and their families/caregivers demand further research. Rigorous studies incorporating pre-intervention comparison groups are essential to assess the effectiveness of these interventions in reducing symptomatology and improving MH function and quality of life across diverse MH symptoms, severity levels, and age groups. To enhance MH outcomes for CYP, interventions should prioritize patient safety, seamless care integration, and service quality, while also emphasizing consistent evaluation of novel interventions and therapies. Given the inherently long-term nature of these interventions, sustained effectiveness and success need to be evaluated through comprehensive, extended follow-up studies, ensuring an understanding of their impact over time.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
BG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. BA: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. TN: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. JJ: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. PH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. TW: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. FB: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. MB: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. VE: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research study was funded by the NSW Ministry of Health, Australia.
We would like to acknowledge the following individuals who have contributed to this study, Ms. Rutu Trivedi, Ms. Catherine Ouyang, and Ms. Madhulikaa Sarjapuram Niranjan.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1324220/full#supplementary-material
1. Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health challenge. Lancet. (2007) 369:1302–13. doi: 10.1016/S0140-6736(07)60368-7
2. LeMoult J, Humphreys KL, Tracy A, Hoffmeister J-A, Ip E, Gotlib IH. Meta-analysis: exposure to early life stress and risk for depression in childhood and adolescence. J Am Acad Child Adolesc Psychiatry. (2020) 59:842–55. doi: 10.1016/j.jaac.2019.10.011
3. Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustun TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. (2007) 20:359. doi: 10.1097/YCO.0b013e32816ebc8c
4. Piao J, Huang Y, Han C, Li Y, Xu Y, Liu Y, et al. Alarming changes in the global burden of mental disorders in children and adolescents from 1990 to 2019: a systematic analysis for the Global Burden of Disease study. Eur Child Adolesc Psychiatry. (2022) 31:1827–45. doi: 10.1007/s00787-022-02040-4
5. Shah K, Ramos-Garcia M, Bhavsar J, Lehrer P. Mind-body treatments of irritable bowel syndrome symptoms: An updated meta-analysis. Behav Res Ther. (2020) 128:103462. doi: 10.1016/j.brat.2019.103462
6. Kelly C, Molcho M, Doyle P, Gabhainn SN. Psychosomatic symptoms among schoolchildren. Int J Adolesc Med Health. (2010) 22:229–35. doi: 10.1515/IJAMH.2010.22.2.229
7. Polese D, Belli A, Esposito D, Evangelisti M, Luchetti A, Di Nardo G, et al. Psychological disorders, adverse childhood experiences and parental psychiatric disorders in children affected by headache: a systematic review. Neuroscience & Biobehavioral Reviews. (2022) 104798:104798. doi: 10.1016/j.neubiorev.2022.104798
8. Abu-Arafeh I, Razak S, Sivaraman B, Graham CJDM. Prevalence of headache and migraine in children and adolescents: A systematic review of population-based studies. J Dev Med Child Neurology. (2010) 52:1088–97. doi: 10.1111/j.1469-8749.2010.03793.x
9. Nieswand V, Richter M, Berner R, von der Hagen M, Klimova A, Roeder I, et al. The prevalence of headache in German pupils of different ages and school types. Cephalalgia. (2019) 39(8):1030–40. doi: 10.1177/0333102419837156
10. Pacheco J, Garvey MA, Sarampote CS, Cohen ED, Murphy ER, Friedman-Hill SR. Annual Research Review: The contributions of the RDoC research framework on understanding the neurodevelopmental origins, progression and treatment of mental illnesses. J Child Psychol psychiatry Allied disciplines. (2022) 63:360–76. doi: 10.1111/jcpp.13543
11. Bohman H, Låftman SB, Cleland N, Lundberg M, Päären A, Jonsson U. Somatic symptoms in adolescence as a predictor of severe mental illness in adulthood: a long-term community-based follow-up study. Child Adolesc Psychiatry Ment Health. (2018) 12:1–12. doi: 10.1186/s13034-018-0245-0
12. Copeland WE, Adair CE, Smetanin P, Stiff D, Briante C, Colman I, et al. Diagnostic transitions from childhood to adolescence to early adulthood. J Child Psychol Psychiatry. (2013) 54:791–9. doi: 10.1111/jcpp.12062
13. Abramson A. How COVID-19 may increase domestic violence and child abuse 2020. Available online at: http://www.apa.org/topics/covid-19/domestic-violence-child-abuse.
14. Swedo E, Idaikkadar N, Leemis R, Dias T, Radhakrishnan L, Stein Z, et al. Trends in US emergency department visits related to suspected or confirmed child abuse and neglect among children and adolescents aged< 18 years before and during the COVID-19 pandemic—United States, January 2019–September 2020. Morbidity and Mortality Weekly Report. (2020) 69(49):1841.
15. Sara G, Wu J, Uesi J, Jong N, Perkes I, Knight K, et al. Growth in emergency department self-harm or suicidal ideation presentations in young people: Comparing trends before and since the COVID-19 first wave in New South Wales, Australia. Aust New Z J Psychiatry. (2022) 57(1):58–68. doi: 10.1177/00048674221082518
16. Osser OV, Jokubkiene L, Valentin L. Cesarean section scar defects: agreement between transvaginal sonographic findings with and without saline contrast enhancement. ULTRASOUND IN OBSTETRICS GYNECOLOGY. (2010) 35:75–83. doi: 10.1002/uog.7496
18. Dey M, Castro RP, Haug S, Schaub MP. Quality of life of parents of mentally-ill children: a systematic review and meta-analysis. Epidemiol Psychiatr Sci. (2019) 28:563–77. doi: 10.1017/S2045796018000409
19. Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10-24 years: a systematic analysis. Lancet. (2011) 377:2093–102. doi: 10.1016/S0140-6736(11)60512-6
20. Deas D, Brown ES. Adolescent substance abuse and psychiatric comorbidities. J Clin Psychiatry. (2006) 67:18. doi: 10.4088/JCP.0706e02
21. Galaif ER, Sussman S, Newcomb MD, Locke TF. Suicidality, depression, and alcohol use among adolescents: a review of empirical findings. Int J Adolesc Med Health. (2007) 19:27–36. doi: 10.1515/IJAMH.2007.19.1.27
22. Das JK, Salam RA, Lassi ZS, Khan MN, Mahmood W, Patel V, et al. Interventions for adolescent mental health: an overview of systematic reviews. J Adolesc Health. (2016) 59:S49–s60. doi: 10.1016/j.jadohealth.2016.06.020
23. Fombonne E, Wostear G, Cooper V, Harrington R, Rutter M. The Maudsley long-term follow-up of child and adolescent depression: I. Psychiatr outcomes adulthood. Br J Psychiatry. (2001) 179:210–7. doi: 10.1192/bjp.179.3.210
24. Mitchell RJ, McMaugh A, Lystad RP, Cameron CM, Nielssen O. Health service use for young males and females with a mental disorder is higher than their peers in a population-level matched cohort. BMC Health Serv Res. (2022) 22:1–9. doi: 10.1186/s12913-022-08789-3
25. Cullen P, Leong RN, Liu B, Walker N, Steinbeck K, Ivers R, et al. Returning to the emergency department: a retrospective analysis of mental health re-presentations among young people in New South Wales, Australia. BMJ Open. (2022) 12:e057388. doi: 10.1136/bmjopen-2021-057388
26. Le LK-D, Shih S, Richards-Jones S, Chatterton ML, Engel L, Stevenson C, et al. The cost of Medicare-funded medical and pharmaceutical services for mental disorders in children and adolescents in Australia. PloS One. (2021) 16:e0249902. doi: 10.1371/journal.pone.0249902
27. Barry MM, Clarke AM, Jenkins R, Patel V. A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health. (2013) 13:1–19. doi: 10.1186/1471-2458-13-835
28. Bradshaw M, Gericke H, Coetzee BJ, Stallard P, Human S, Loades M. Universal school-based mental health programmes in low-and middle-income countries: A systematic review and narrative synthesis. Prev Med. (2021) 143:106317. doi: 10.1016/j.ypmed.2020.106317
29. Kohn R, Saxena S, Levav I, Saraceno B. The treatment gap in mental health care. Bull World Health Organization. (2004) 82:858–66.
30. Sharma M, Perera C, Ipince A, Bakrania S, Shokraneh F, Idele P, et al. PROTOCOL: Child and adolescent mental health and psychosocial support interventions: An evidence and gap map of low-and middle-income countries. Campbell Systematic Rev. (2022) 18:e1221. doi: 10.1002/cl2.1221
31. Weisz JR, Kuppens S, Ng MY, Eckshtain D, Ugueto AM, Vaughn-Coaxum R, et al. What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice. Am Psychol. (2017) 72:79. doi: 10.1037/a0040360
32. Pilling S, Fonagy P, Allison E, Barnett P, Campbell C, Constantinou M, et al. Long-term outcomes of psychological interventions on children and young people’s mental health: A systematic review and meta-analysis. PloS One. (2020) 15:e0236525. doi: 10.1371/journal.pone.0236525
33. Pedersen GA, Smallegange E, Coetzee A, Hartog K, Turner J, Jordans MJ, et al. A systematic review of the evidence for family and parenting interventions in low-and middle-income countries: child and youth mental health outcomes. J Child Family Stud. (2019) 28:2036–55. doi: 10.1007/s10826-019-01399-4
34. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J surgery. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
35. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Systematic Rev. (2016) 5:1–10. doi: 10.1186/s13643-016-0384-4
36. Asarnow JR, Jaycox LH, Tang L, Duan N, LaBorde AP, Zeledon LR, et al. Long-term benefits of short-term quality improvement interventions for depressed youths in primary care. Am J Psychiatry. (2009) 166:1002–10. doi: 10.1176/appi.ajp.2009.08121909
37. Boege I, Corpus N, Weichard M, Schepker R, Young P, Fegert JM. Long-term outcome of intensive home treatment for children and adolescents with mental health problems - 4 years after a randomized controlled clinical trial. Child Adolesc Ment Health. (2021) 26:310–9. doi: 10.1111/camh.12500
38. Lipman EL, Boyle MH, Cunningham C, Kenny M, Sniderman C, Duku E, et al. Testing effectiveness of a community-based aggression management program for children 7 to 11 years old and their families. J Am Acad Child Adolesc Psychiatry. (2006) 45:1085–93. doi: 10.1097/01.chi.0000228132.64579.73
39. Ogden T, Hagen KA. Multisystemic treatment of serious behaviour problems in youth: Sustainability of effectiveness two years after intake. Child Adolesc Ment Health. (2006) 11:142–9. doi: 10.1111/j.1475-3588.2006.00396.x
40. Petrenko CLM, Pandolfino ME, Robinson LK. Findings from the families on track intervention pilot trial for children with fetal alcohol spectrum disorders and their families. Alcoholism: Clin Exp Res. (2017) 41:1340–51. doi: 10.1111/acer.13408
41. Richardson LP, Ludman E, McCauley E, Lindenbaum J, Larison C, Zhou C, et al. Collaborative care for adolescents with depression in primary care: a randomized clinical trial. Jama. (2014) 312:809–16. doi: 10.1001/jama.2014.9259
42. Van Den Hoofdakker BJ, van der Veen-Mulders L, Sytema S, Emmelkamp PMG, Minderaa RB, Nauta MH. Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: A randomized controlled study. J Am Acad Child Adolesc Psychiatry. (2007) 46:1263–71. doi: 10.1097/chi.0b013e3181354bc2
43. Haft SL, Chen T, LeBlanc C, Tencza F, Hoeft F. Impact of mentoring on socio-emotional and mental health outcomes of youth with learning disabilities and attention-deficit hyperactivity disorder. Child Adolesc Ment Health. (2019) 24:318–28. doi: 10.1111/camh.12331
44. Lilly RG, Meadows TJ, Sevecke-Hanrahan JR, Massura CE, Golden ME, O'Dell SM. Hub-extension model and access to pediatric behavioral integrated primary care. Clin Pract Pediatr Psychol. (2020) 8:220–7. doi: 10.1037/cpp0000358
45. Shippee ND, Mattson A, Brennan R, Huxsahl J, Billings ML, Williams MD. Effectiveness in regular practice of collaborative care for depression among adolescents: A retrospective cohort study. Psychiatr Services. (2018) 69:536–41. doi: 10.1176/appi.ps.201700298
46. Cordell KD, Snowden LR. Reducing mental health emergency services for children served through California's full service partnerships. Med Care. (2017) 55:299–305. doi: 10.1097/MLR.0000000000000641
47. Enns JE, Randall JR, Smith M, Chateau D, Taylor C, Brownell M, et al. A multimodal intervention for children with ADHD reduces inequity in health and education outcomes. Can J Psychiatry. (2017) 62:403–12. doi: 10.1177/0706743717692301
48. Fjermestad KW, Wergeland GJ, Rogde A, Bjaastad JF, Heiervang E, Haugland BSM. School-based targeted prevention compared to specialist mental health treatment for youth anxiety. Child Adolesc Ment Health. (2020) 25:102–9. doi: 10.1111/camh.12366
49. McDonell MG, Tarantino J, Dubose AP, Matestic P, Steinmetz K, Galbreath H, et al. A pilot evaluation of dialectical behavioural therapy in adolescent long-term inpatient care. Child Adolesc Ment Health. (2010) 15:193–6. doi: 10.1111/j.1475-3588.2010.00569.x
50. Baruch G, Vrouva I, Wells C. Outcome findings from a parent training programme for young people with conduct problems. Child Adolesc Ment Health. (2011) 16:47–54. doi: 10.1111/camh.2011.16.issue-1
51. Clossey L, Simms S, Hu C, Hartzell J, Duah P, Daniels L. A pilot evaluation of the rapid response program: A home based family therapy. Community Ment Health J. (2018) 54:302–11. doi: 10.1007/s10597-018-0231-2
52. Duffy F, Skeldon J. A CAMHS Intensive Treatment Service: Clinical outcomes in the first year. Clin Child Psychol Psychiatry. (2012) 19:90–9. doi: 10.1177/1359104512468287
53. Evans GD, Radunovich HL, Cornette MM, Wiens BA, Roy A. Implementation and utilization characteristics of a rural, school-linked mental health program. J Child Family Stud. (2008) 17:84–97. doi: 10.1007/s10826-007-9148-z
54. Flynn D, Kells M, Joyce M, Corcoran P, Gillespie C, Suarez C, et al. Innovations in Practice: Dialectical behaviour therapy for adolescents: multisite implementation and evaluation of a 16-week programme in a public community mental health setting. Child Adolesc Ment Health. (2019) 24:76–83. doi: 10.1111/camh.12298
55. Fox RA, Holtz CA. Treatment outcomes for toddlers with behaviour problems from families in poverty. Child Adolesc Ment Health. (2009) 14:183–9. doi: 10.1111/j.1475-3588.2009.00527.x
56. Griffiths H, Noble A, Duffy F, Schwannauer M. Innovations in Practice: Evaluating clinical outcome and service utilization in an AMBIT-trained Tier 4 child and adolescent mental health service. Child Adolesc Ment Health. (2017) 22:170–4. doi: 10.1111/camh.12181
57. James AC, Winmill L, Anderson C, Alfoadari K. A preliminary study of an extension of a community dialectic behaviour therapy (DBT) programme to adolescents in the looked after care system. Child Adolesc Ment Health. (2011) 16:9–13. doi: 10.1111/camh.2011.16.issue-1
58. Jaycox LH, Morral AR, Juvonen J. Mental health and medical problems and service use among adolescent substance users. J Am Acad Child Adolesc Psychiatry. (2003) 42:701–9. doi: 10.1097/01.CHI.0000046846.56865.F9
59. Lu ZQ, de Geus H, Roest S, Payne L, Krishnamoorthy G, Littlewood R, et al. Characteristics and treatment outcomes of children and adolescents accessing treatment in Child and Youth Mental Health Services. Early intervention in psychiatry. (2022) 16(12):1297–308. doi: 10.1111/eip.13275
60. Mantzouranis G, Baier V, Holzer L, Urben S, Villard E. Clinical significance of assertive community treatment among adolescents. J Soc Psychiatry. (2019) 54:445–53. doi: 10.1007/s00127-018-1613-z
61. Newman M, Fagan C, Webb R. Innovations in Practice: The efficacy of nonviolent resistance groups in treating aggressive and controlling children and young people: A preliminary analysis of pilot NVR groups in Kent. Child Adolesc Ment Health. (2014) 19:138–41. doi: 10.1111/camh.12049
62. Rickwood DJ, Mazzer KR, Telford NR, Parker AG, Tanti CJ, McGorry PD. Changes in psychological distress and psychosocial functioning in young people visiting headspace centres for mental health problems. Med J Australia. (2015) 202:537–42. doi: 10.5694/mja14.01696
63. Sibley MH, Olson S, Morley C, Campez M, Pelham WE. A school consultation intervention for adolescents with ADHD: barriers and implementation strategies. Child Adolesc Ment Health. (2016) 21:183–91. doi: 10.1111/camh.12159
64. Simpson W, Cowie L, Wilkinson L, Lock N, Monteith G. The effectiveness of a community intensive therapy team on young people's mental health outcomes. Child Adolesc Ment Health. (2010) 15:217–23. doi: 10.1111/j.1475-3588.2009.00546.x
65. Webster-Stratton C, Rinaldi J, Reid JM. Long-term outcomes of incredible years parenting program: predictors of adolescent adjustment. Child Adolesc Ment Health. (2011) 16:38–46. doi: 10.1111/camh.2011.16.issue-1
66. Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. A product ESRC Methods Programme Version. (2006) 1:b92.
67. McBee-Strayer SM, Thomas GV, Bruns EM, Heck KM, Alexy ER, Bridge JA. Innovations in Practice: Intensive crisis intervention for adolescent suicidal ideation and behavior - an open trial. Child Adolesc Ment Health. (2019) 24:345–9. doi: 10.1111/camh.12340
68. Piquero AR, Jennings WG, Diamond B, Farrington DP, Tremblay RE, Welsh BC, et al. A meta-analysis update on the effects of early family/parent training programs on antisocial behavior and delinquency. J Exp Criminology. (2016) 12:229–48. doi: 10.1007/s11292-016-9256-0
69. McCauley E, Berk MS, Asarnow JR, Adrian M, Cohen J, Korslund K, et al. Efficacy of dialectical behavior therapy for adolescents at high risk for suicide: A randomized clinical trial. JAMA Psychiatry. (2018) 75:777–85. doi: 10.1001/jamapsychiatry.2018.1109
70. Polese D, Fornaro M, Palermo M, De Luca V, de Bartolomeis A. Treatment-resistant to antipsychotics: A resistance to everything? Psychotherapy in treatment-resistant schizophrenia and nonaffective psychosis: A 25-year systematic review and exploratory meta-analysis. Front Psychiatry. (2019) 10:210. doi: 10.3389/fpsyt.2019.00210
71. DeCou CR, Comtois KA, Landes SJ. Dialectical behavior therapy is effective for the treatment of suicidal behavior: A meta-analysis. Behav Ther. (2019) 50:60–72. doi: 10.1016/j.beth.2018.03.009
72. Witt KG, Hetrick SE, Rajaram G, Hazell P, Taylor Salisbury TL, Townsend E, et al. Psychosocial interventions for self-harm in adults. Cochrane Database Syst Rev. (2021) 4:Cd013668. doi: 10.1002/14651858.CD013668.pub2
73. Hawton K, Witt KG, Salisbury TLT, Arensman E, Gunnell D, Hazell P, et al. Psychosocial interventions following self-harm in adults: a systematic review and meta-analysis. Lancet Psychiatry. (2016) 3:740–50. doi: 10.1016/S2215-0366(16)30070-0
74. Midgley N, Mortimer R, Cirasola A, Batra P, Kennedy E. The evidence-base for psychodynamic psychotherapy with children and adolescents: A narrative synthesis. Front Psychol. (2021) 12:662671. doi: 10.3389/fpsyg.2021.662671
75. Tennant R, Goens C, Barlow J, Day C, Stewart-Brown S. A systematic review of reviews of interventions to promote mental health and prevent mental health problems in children and young people. J Public Ment Health. (2007) 6(1):25–32. doi: 10.1108/17465729200700005
Keywords: mental health services, child and adolescent mental health services, mental health intervention, psychological distress, evidence base
Citation: Gerstl B, Ahinkorah BO, Nguyen TP, John JR, Hawker P, Winata T, Brice F, Bowden M and Eapen V (2024) Evidence-based long term interventions targeting acute mental health presentations for children and adolescents: systematic review. Front. Psychiatry 15:1324220. doi: 10.3389/fpsyt.2024.1324220
Received: 19 October 2023; Accepted: 12 February 2024;
Published: 06 March 2024.
Edited by:
Yuka Kotozaki, Iwate Medical University, JapanReviewed by:
Daniela Polese, Sapienza, ItalyCopyright © 2024 Gerstl, Ahinkorah, Nguyen, John, Hawker, Winata, Brice, Bowden and Eapen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valsamma Eapen, di5lYXBlbkB1bnN3LmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.