 Dilara Kocol1,2*†
Dilara Kocol1,2*† Alexander Bäuerle1,2†Theresa Schadendorf1,2
Alexander Bäuerle1,2†Theresa Schadendorf1,2 Sheila Geiger1,2
Sheila Geiger1,2 Julia Barbara Krakowczyk1,2
Julia Barbara Krakowczyk1,2 Eva-Maria Skoda1,2
Eva-Maria Skoda1,2 Martin Teufel1,2
Martin Teufel1,2- 1Clinic for Psychosomatic Medicine and Psychotherapy, LVR-University Hospital Essen, University of Duisburg-Essen, Essen, Germany
- 2Center for Translational Neuro- and Behavioral Sciences (C-TNBS), University of Duisburg-Essen, Essen, Germany
Introduction: Obesity and depression are inter-related health concerns, demanding a high level of treatment and costs in the health care system. The development of eHealth interventions that simultaneously address obesity and mental health can be supportive in this regard. However, evidence of the efficacy of eHealth interventions in the treatment of depression symptoms in individuals with obesity is lacking. The aim of this systematic literature review is to evaluate the efficacy of existing eHealth interventions for individuals with obesity that target depression symptoms.
Methods: We systematically searched electronic databases (Cochrane Library, PubMed, Scopus) to identify studies published in English between January 2016 and January 2023, that focused on eHealth interventions, targeting depression symptoms in individuals with obesity people. Exclusion criteria were study objectives that (1) focused specifically on one or more metabolic comorbidities of individuals with obesity, e.g., hypertension, hyperlipidemia, diabetes; (2) focused specifically on eating disorders comorbidities e.g., binge eating disorder, and (3) focused specifically on patients before or after bariatric surgery.
Results: The database search identified 214 records. Six articles were included in this review. Sample sizes ranged from 70 to 1267 participants of ages 18-60 years. All included studies were randomized controlled trials. Two of the six included studies were web-based interventions guided either by medical doctors or psychologists. All interventions included video, printed materials, and interactive parts of which two studies integrated elements of Cognitive Behavioural Therapy and Social Cognitive Therapy. The findings showed that eHealth treatment services, supported and guided throughout the intervention had high acceptance and efficacy in the reduction of depression symptoms among individuals with obesity.
Conclusion: EHealth interventions that address and target both mental and physical health with interactive strategies calls for better efficacy in the reduction of depression symptoms. Future eHealth interventions that target depression symptoms in individuals with obesity should integrate digital strategies that address both mental and physical health through interactive modules.
Introduction
One of the most emerging health issues and prevalent chronic diseases worldwide can be ascribed to overweight and obesity (1). Overweight and obesity are defined as abnormal or excessive fat accumulation that can cause several health issues (1). The Body mass index (BMI) is an index of weight-for-height, used to classify overweight and obesity in adults (1). Hereby, a BMI greater than or equal to 25 defines overweight and a BMI greater than or equal to 30 obesity (1). The so-called obesity pandemic has become a significant global health challenge (1). According to data of the World Health Organisation in 2016, around 1.9 billion of people 18 years and older were overweight, of which over 650 million were obese (1). Hereby, the global prevalence of individuals with obesity has almost tripled between the years 1975 and 2016. Current data shows that obesity and overweight turned out to be increasingly prevalent in low- and middle- income countries, in particular in urban areas (1). Based on data from the European Health Interview Survey EHIS conducted in 2019, it became apparent that around 36% of adults in EU Member States were overweight and 17% were obese (2). The outcomes of the Global Burden of Disease study (GBD) conducted in 2017 showed that a BMI above 25 caused 2.4 million deaths in females and 2.3 million deaths in males worldwide. Next to the global deaths, the GBD study analyzed the disability-adjusted life years (DALYs) that can be ascribed to obesity. Hereby, it became apparent that obesity led to 70.7 million DALYs in females and 77.0 million in males. Looking at the number of global deaths and DALYs between 1990 and 2017 in the study showed that the global number of obesity-related DALYs more than doubled in both, men and women (3).
Obesity is associated with an enhanced risk of type 2 diabetes, cancer, stroke, arthritis (4), hypertension, dyslipidemia, cardiovascular risks and musculoskeletal disorders (5). Furthermore, existing data showed that obesity is linked to several mental health problems, especially depression (6–8). It was highlighted that depression and obesity commonly co-exist (9), which was emphasized by a conducted meta-analysis that detected a complex reciprocal pathway between these two diseases (10). A study conducted by Zhang (2021) focused on the bidirectional relationship between body weight and depression and possible explanatory factors and models for this relationship. The outcomes of a psychosomatic-psychotherapeutic evaluation conducted with individuals with obesity showed that one or more mental disorders, especially depression and adjustment disorders, were detectable in more than 50% of the patients (11). Next to these, individuals with obesity experience problems in emotion and behaviour regulation (12), difficulties with peers (13), lower self-esteem (14), and body dissatisfaction (15).
This increase of obesity and the related comorbidities associated with it contribute to high health costs. The results of systematic reviews show that between 1.9% and 4.7% of total annual healthcare costs, and 2.8% of total annual hospital care costs in European countries are attributable to obesity (16, 17).
Due to this high incidence and comorbidity of the double stigma obesity and mental health issues experienced by individuals with obesity (18–20), several mental health research experts proposed to label obesity as a mental disorder in the DSM-V (20, 21). This has led to the establishment of overweight and obesity treatment programs that aim to have, besides the impact on the primary goal of weight management, an influence on the mental health as well (18). Interventions that integrate elements of cognitive behavioural therapy (CBT) have been shown to lead to positive outcomes in improving mental health (22). In general, most mental health interventions for individuals with obesity aim to increase knowledge about potential difficulties associated with dieting by simultaneously providing psychoeducation about weight biology, increased self-esteem and mental health, improved health and eating behaviours, and physical activity, rather than focusing predominantly on weight loss (23, 24).
The high global prevalence of obesity that is highly connected to further physical comorbidities and mental health difficulties (25) requires a high and long-term treatment effort that has financial consequences and leads to an increased burden on the health care system (26, 27). The outcomes of face-to-face treatments in these contexts showed that there was deficient proof of the “scalability, generalisability and long-term sustainability” of face-to-face treatments (28) which opened at that point doors to the establishment of eHealth interventions, including approaches to improve the mental health of individuals with obesity.
EHealth interventions in general can be defined as the usage of information and communication technologies (ICT), aiming an improvement and facilitation in the health care system and health conditions (29). Furthermore, it fosters an option to “enhance the quality, efficiency, and reach of primary and secondary healthcare” (30) in a timely and cost-effectively more flexible way for practitioners and patients (31). In particular, the outcomes of a study conducted by Bauerle et al. (32) emphasized the increased mental health burden during the COVID-19 pandemic and the need for appropriate interventions to support burdened people. Due to the new health system realities created by the COVID-19 pandemic, low-threshold tele-medical approaches provide opportunities in anonymous and effective support and treatment (33).
Several systematic reviews provide evidence for the effectiveness of eHealth interventions in the treatment of individuals with obesity (34–36). The outcomes of a review emphasized the positive impact of Internet interventions on improving disease knowledge, health outcomes, health care utilization and quality of life (37). Based on the gained insights and evidence about the co-existence of obesity and depression, electronic lifestyle programs were developed that target physical and mental health simultaneously (38). These programs also provide success in weight and depression symptom reduction. Due to the fact, that such digital lifestyle programs focusing on individuals in a holistic way have been proven to be effective (39, 40), more eHealth interventions in obesity treatments have been developed (41, 42). The results of a self-guided, eHealth program targeting weight loss and depression in men showed a significant decrease in weight and depression (42).
Despite the emerging empirical evidence highlighted above regarding the inclusion of mental health approaches that specifically target high-prevalence depression in obesity and its electronic treatment programs, there is no clear synthesis of the literature. This lack of understanding leads to limited efforts to address and protect depression symptoms in obesity interventions (43). Hence, it is of relevance to have a clear synthesis of evidence relating to the efficacy of eHealth interventions targeting depression symptoms in individuals with obesity. Therefore, the research question in this systematic literature review is:
How does the efficacy of eHealth interventions, targeting depression symptoms in individuals with obesity compare to a control condition in randomized controlled intervention trials?
Materials and methods
This systematic literature review was performed following the PRISMA guidelines (44).
Search strategy
A comprehensive literature search of the Cochrane Library, PubMed, and Scopus databases was conducted between November 2022 and January 2023. The search results were included into the analyses until January 31, 2023. Additionally, the so-called snowball-method was applied. This involved searching the reference lists of relevant articles for potential articles of potential interest. Further, previously conducted systematic reviews focusing on eHealth interventions in obesity treatment were also screened. The literature search was limited to studies published between January 2016 and January 2023. Two independent researchers conducted the literature search. The following combinations of search terms were used: obes* AND randomized controlled trial AND depress* AND e-health OR mobile OR e-mental health OR web OR tele* AND adult. All included studies were RCTs because RCTs best isolate the effects of a particular intervention and provide evidence for or against a particular intervention. RCT’s represent the gold standard in clinical research. The relevant syntax for each searched database, including the number of results found for each database, are provided in a Supplementary Table 1.
Inclusion/exclusion criteria
The search was designed to identify studies of eHealth interventions, targeting depression symptoms in individuals with obesity. All published (RCTs) of eHealth interventions to reduce depression symptoms, compared with a control condition targeting individuals with obesity were eligible for inclusion in this systematic review. Inclusion criteria were (1) individuals with obesity (BMI = 30 kg/m²) targeted, independent of a specific topographic limitation, ethnicity, or occupational group; (2) an eHealth intervention targeting depression symptoms; (3) a mental health measurement of depression symptoms reported at baseline and post-intervention; (4) a control group; (5) publication in English between January 2016 and January 2023. Exclusion criteria were (1) study objectives that focused specifically on one or more metabolic comorbidities of individuals with obesity, e.g., hypertension, hyperlipidemia, diabetes; (2) focused on eating disorders comorbidities e.g., binge eating disorder, and (3) focused specifically on patients before or after bariatric surgery.
Data extraction and data synthesis
Data extraction was performed independently by D.K and T.S. Thirteen articles were selected for full-text review to assess eligibility for inclusion. A standardized data extraction form was created to capture sample characteristics, intervention characteristics, eHealth approach, measures used in general and measures specifically targeting depression, and findings (Table 1). The authors resolved discrepancies by consensus. The authors first screened titles and abstracts of each article. A list of potential articles was further shortened by reviewing abstracts and performing detailed evaluations by considering the above-mentioned eligibility criteria. See Figure 1 for the progressive flow of the study exclusion process.
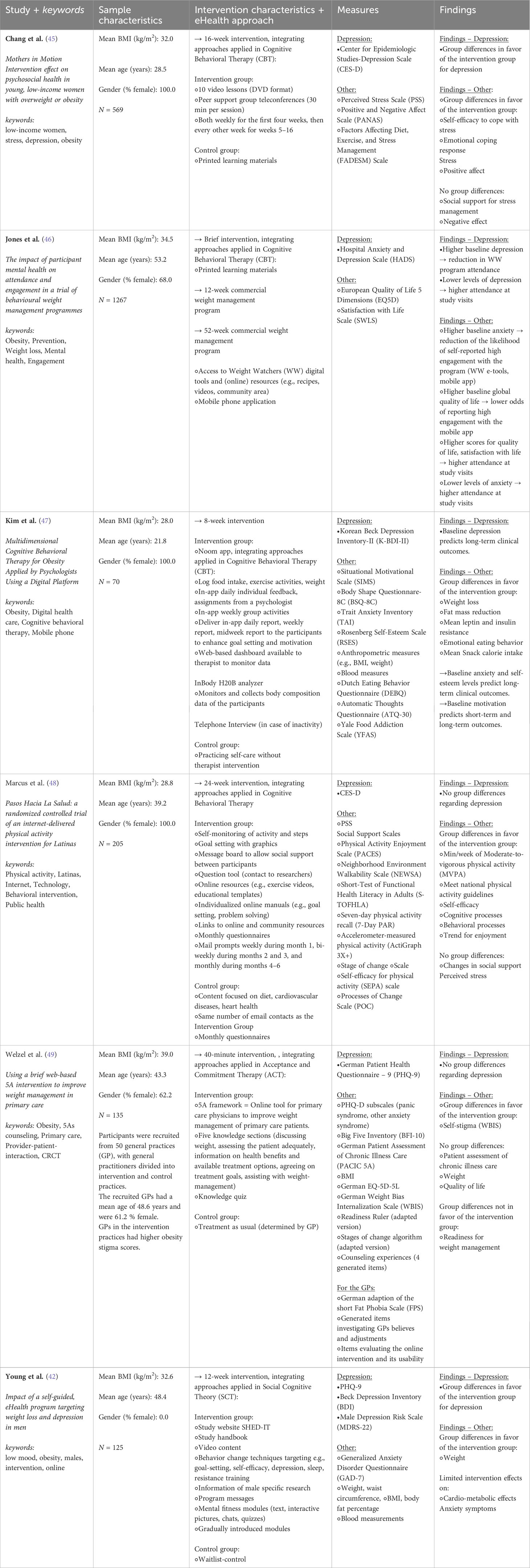
Table 1 Summary of included eHealth interventions to reduce depression in obese people.
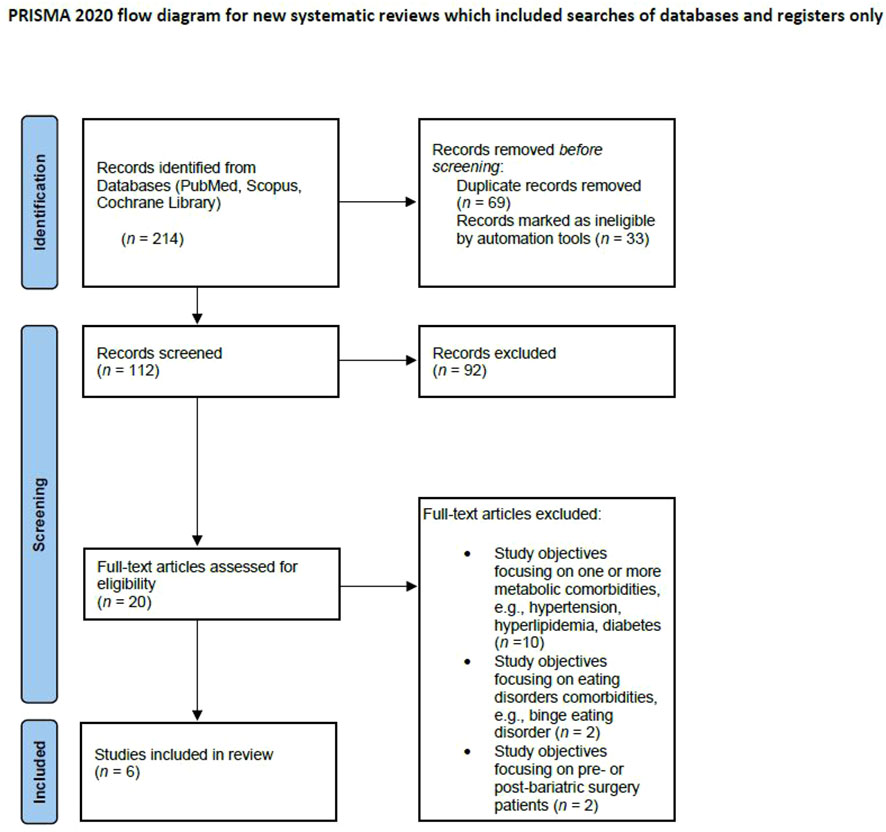
Figure 1 Flow diagram of studies that were identified using the search terms and strategy, articles screened for eligibility, included/excluded with reasons following PRISMA guidelines.
Risk of bias assessment
We used the Cochrane Collaboration’s Risk of Bias Assessment Tool (RoB 2) to assess the risk of bias of the included studies in this systematic review (50). The studies were rated as have ‘low risk’, ‘some concerns’, or ‘high risk’ of bias. The following quality domains were assessed: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result (50).
Results
Main findings of the study
The outcomes of the study by Chang et al. (45) which included elements of the SCT in order to guide the intervention, showed that participants in the intervention group reported significant less depression symptoms than the control group. Results from two of the six included studies (48, 49) showed no significant group differences in depression symptoms. Jones et al. (46) who investigated whether participants’ mental health was associated with the rate of attendance and engagement with the behavioral weight management program (WW) and trial (WRAP) found that a reduction in depression symptoms was associated with higher participation rates in WW sessions. In addition, individuals with obesity who had fewer depression and anxiety symptoms at baseline were more likely to describe higher engagement with the program resources (WW e-tools and mobile phone app). Further, it can be concluded that higher attendance at all study visits up to 5 years follow-up were associated with fewer symptoms of depression. The outcomes of the study conducted by Young et al. (42), that focused on an online weight loss program targeted at men with low mood, showed significant improvements in depression symptoms. The findings of the study by Kim et al. (47) which investigated a new, comprehensive, multifactorial, daily, intensive psychologist coaching based on CBT modules, showed that digital CBT improved the level of depression symptoms. Baseline depression symptoms significantly predicted long-term clinical outcomes.
Qualitative synthesis
Study selection
The systematic database search yielded 187 published studies (see Figure 1). After the screening process, 20 articles were included in the full-text assessment to check eligibility. Of the 20 full-texts, 14 publications were neither in line with the inclusion nor the exclusion criteria, resulting in six publications, which were ultimately included in the in-depth analyses and summary. All included RCTs had a two-arm design. A total of 2371 patients were included in these RCTs.
Summary of included studies
As presented in Figure 1, the search strategy initially yielded 214 records in PubMed, Scopus and Cochrane library. After removing duplicates and records deemed inappropriate, 112 articles remained to be screened. After screening these 112 articles, another 92 were excluded, leaving 20 articles. These articles were assessed for eligibility using the full text. Thus, after assessing the remaining 20 full-text articles, 14 additional articles were excluded due to a) study objectives that were primarily focusing on metabolic comorbidities, e.g., hypertension, hyperlipidemia, diabetes (n = 10), b) study objectives that were focusing primarily on eating disorders comorbidities e.g., binge eating disorder (n = 2) and c) study objectives that were focusing on pre- or post-bariatric surgery patients (n = 2). The final studies included in this review (n = 6) are listed in Figure 1.
Participants and study characteristics
The selected studies included patients from four different countries. Three studies included patients from the United States (42, 45, 48), one study included patients from Germany (49), one study included patients from England (46), and another study included patients from South Korea (47). Sample sizes ranged from 70 to 1267 participants (age range: 18-60 years). Participants included in the review had a mean BMI of 32.4 kg/m². Half of the studies included in the review (n = 3) focused on women. Two studies focused on men and one included both genders in their sample. The oldest included publication was conducted by Marcus et al. (48) in 2016 and tested the efficacy of a 6-month culturally adapted, individually tailored, Spanish-language Internet-based physical activity intervention among Latinas (n = 205). The second study was conducted by Chang et al. (45) and investigated whether a community-based intervention program that included video lessons and joined peer support group teleconferences had an effect on the self-efficacy to cope with stress, emotional coping response, social support for stress management, stress, depression, and positive and negative affect among mothers with obesity (n = 612). The third study was conducted by Kim et al. (47) and tested the efficacy of a comprehensive, multifactorial, daily intensive, coaching program by psychologists based CBT modules in weight management among female participants (n = 70). Three studies which were published in 2021 were included. The study conducted by Welzel et al. (49) implemented and evaluated an online tutorial with the aim of improving weight management and practitioner-patient interactions in primary health care settings among a sample of the German population (n = 185). The fifth included study was conducted by Young et al. (42) and explored the efficacy of a self-guided, eHealth program (SHED-IT: Recharge) to reduce weight and depression symptoms in men with obesity (n = 125). The final included study was conducted by Jones et al. (46) and examined whether mental health was associated with attendance and engagement in a trial of behavioral weight management programs among a sample of the British population (n = 1267).
Measurement of depression
The study conducted by Young et al. (42) was the only one of the six studies included in this review in which depression symptoms was the primary outcome of the study. The primary outcome of the majority of the studies included in this review were change in body weight and physical activity. Nevertheless, all studies made use of validated questionnaires to assess depression symptoms. To investigate depression symptoms in individuals with obesity, Young et al. (42) and Welzel et al. (49) made use of the Patient Health Questionnaire-9 (PHQ-9). The depression symptoms of participants in the studies of Chang et al. (45) and Marcus et al. (48) were measured using the Center for Epidemiologic Studies Depression Scale (CES-D). In addition, Chang et al. (45) integrated the Perceived Stress Scale (PSS) and the Positive and Negative Affect Scale (PANAS) to gain greater insight into the depression symptoms of individuals with obesity who participated in the intervention. The Hospital Anxiety and Depression Scale (HADS), also used in the study by Jones et al. (46) and the Beck Depression Inventory-II (BDI-II) were additional measurements used to determine depression symptoms in participants by Kim et al. (47).
EHealth approach
Welzel et al. (49) investigated the efficacy of a web-based 5A-based weight management counseling program for general practitioners in obesity treatment. The 5A program focuses on “ASK”, assessing health status, “ASSES”, counseling on the health benefits of treatment and available treatment options, “ADVISE”, seeking agreement on weight loss expectations, “AGREE”, agreeing on a treatment plan and goals, and “ASSIST”, assisting the patient in the process of weight management. Based on these 5As obesity management guidelines from the Canadian Obesity Network, a short 5A online tutorial was implemented. This online tutorial comprises an introduction in the beginning and five knowledge sections. Hereby, patients receive information from their primary care physicians in the form of online sheets about obesity-related treatment options (physical exercise, nutrition, psychotherapy, medication, and surgery). At the end of the 5A tutorial a short knowledge quiz was implemented.
The randomized controlled trial (RCT) by Chang et al. (45) was conducted to evaluate a community-based intervention program that integrated ten video lessons at home and participation in ten peer support group teleconferences. During the 16-week intervention, participants watched weekly video lessons (20 minutes per video lesson) about the topic stress management at home (weeks 1-4). From week five onwards until week 16, participants received video lessons on healthy eating and physical activity. After viewing the designated video lessons, participants circled responses on a worksheet that ask them about content of the video lessons. Moreover, they joined peer support group teleconferences (30 minutes per session, weekly for the first four weeks and then every other week for weeks 5-16). These group teleconferences were led by moderators who were peer educators or dietitians from the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), trained in motivational interviewing and group facilitation.
Marcus et al. (48) investigated the efficacy of a culturally and linguistically adapted, individually tailored, Internet-based physical activity intervention compared to a Spanish-speaking wellness contact Internet control group. Participants randomly assigned to the physical activity Internet intervention received access to a study website including the following features: 1) self-monitoring of minutes of activity and steps; 2) goal setting with graphs to compare goals to minutes recorded; 3) message board to foster social support among participants; 4) “Ask the Expert” where participants could anonymously ask questions to a PhD level researcher and 5) online resources such as walking route maps and free exercise videos. Next to these, participants were provided with monthly questionnaires that generated automated tailored physical activity reports. Participants assigned to the control group received access to a Spanish-language website with information on health topics other than physical activity. The web-based content focused on diet and other factors, that were associated with cardiovascular disease risk and integrated information from a series on heart health developed for Latinos by the National Heart Lung and Blood Institute.
Young et al. (42) explored whether a gender-tailored, self-guided, eHealth program (SHED-IT: Recharge Program) could help in the reduction of weight and depression in men with obesity with low mood. Hereby, participants took part in a 3-month program that included a combination of eHealth and print resources. At the very beginning, participants received a study handbook and watched two introductory videos on the study website. Participants were then encouraged to complete a series of tasks set out in the study logbook (e.g., setting and reviewing goals), which they received weekly. The focus of this program and the tasks included in it targeted behavior change techniques that align with key constructs of Bandura’s Social Cognitive Theory (SCT) (e.g., self-efficacy, goal setting) to achieve long-term lifestyle change in participants (51). In addition, the topics of sleep, resistance training, and four interactive “mental fitness” modules to combat depression were included. Young et al. (42) created these modules using the eHealth authoring program Articulate Rise. Each module was created with a set of tools such as text, interactive images and diagrams, quizzes on cognitive behavioral skills. Additionally, the program includes cognitive restructuring, mindfulness, behavioral activation, relapse prevention, and completion a thought monitoring diary.
Kim et al. (47) conducted an open-label, active-comparison RCT in order to investigate the efficacy of a psychologist-coaching program based on Cognitive Behavioral Therapy (CBT) modules via digital tools, such as the Noom Coach App and InBody Dial among 70 female participants. The Noom Coach App is a smartphone application, which allows to log food intake, exercise activity, weight, and engagement in in-app group activities, read in-app articles, and interact with a human coach via in-app messages. Moreover, a web-based dashboard is provided to the coaches to monitor participants’ data. The InBody Dial is a body composition measure that can be linked to a mobile app to conveniently measure the user’s body composition. The intervention group used the apps, linked to a therapist intervention via digital health care service that provided daily feedback and assignments for eight weeks. Whereas the control group also used the digital health care service, but practiced self-care without receiving the therapist’s intervention.
Jones et al. (46) randomly assigned 1267 individuals with obesity to either a brief intervention, Weight Watchers (WW) for 12-weeks, or WW for 52-weeks. Participants in the brief intervention received a 32-page printed booklet from the British Heart Foundation with self-help weight management strategies. Participation at WW included weekly WW sessions and engagement with digital tools, such as e-tools and online resources and use of the WW mobile phone app. The WW’s e-tools are an online service, integrating access to support materials (e.g., recipes, videos, community area) and tracking tools.
Risk of bias assessment
Table 2 gives an overview of the risk of bias assessment of the included studies. In terms of the assessed domains, the randomization process was observed with some concerns in two studies, concerns regarding the deviations from intended interventions occurred in 2 studies. Regarding the other domains, no concerns/risk of bias could be overserved.
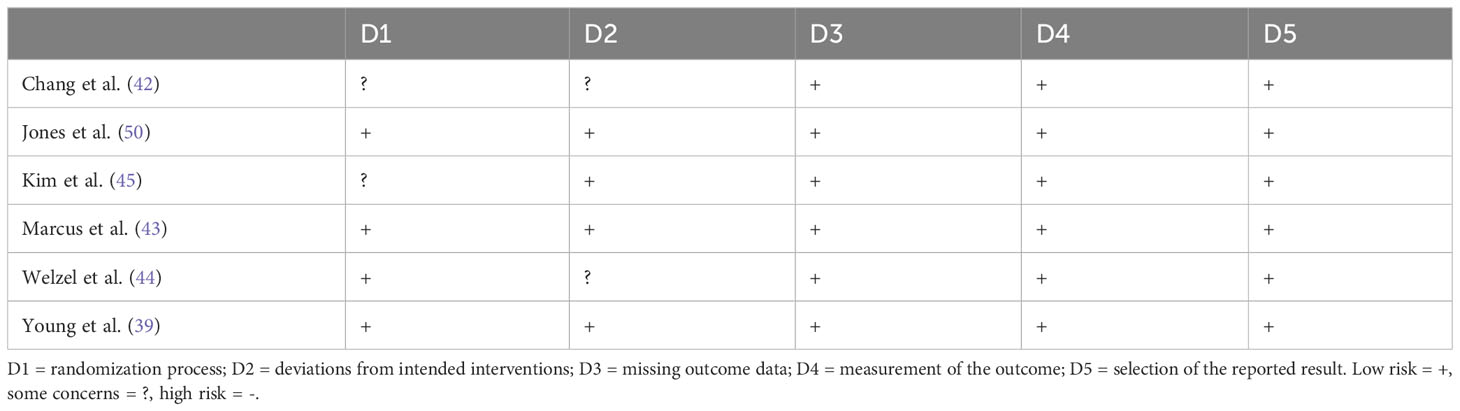
Table 2 Summary of the quality assessment.
Discussion
The aim of this systematic review was to synthesize evidence from RCTs on the efficacy of eHealth interventions that target depression symptoms in individuals with obesity.
Due to emerging empirical evidence about depression symptoms experienced by individuals with obesity and the limited amount of eHealth interventions targeting this, a clear synthesis of this literature is of high relevance. Hence, a clear synthesis of the evidence relating to the efficacy of eHealth interventions targeting depression symptoms in individuals with obesity is of special relevance for the development of further interventions. So, the outcome of this review may assist in the development of further eHealth interventions that, specifically target the needs and demands of individuals with obesity and depression symptoms.
In total six RCTs were included in this systematic review. The overall quality of the studies included int his review was assessed as good. In general, the outcomes of the review showed that the majority of the included eHealth interventions were efficient in reducing depression symptoms in individuals with obesity. Nevertheless, the outcomes underlined the lack of interventions designed for individuals with obesity and depression symptoms as a primary outcome, based on the fact that only one the study of Young et al. (42) had depression symptoms as primary outcome. Hence, it is of high relevance for future studies and interventions to focus on this.
Besides that, it became apparent that study participants in the two interventions that did not show a significant difference in the depression symptoms experienced a limited user acceptance of the eHealth interventions (48, 49) compared to study participants in the other studies included in this review. This is in line with research which concluded, that the user acceptance for eHealth modalities is a vital precondition for such interventions to be effective and integrated in clinical settings (52). An additional factor that influences the efficacy of such eHealth interventions is the rate of attendance at the online sessions. Jones et al. (46) concluded that higher attendance rates correlated with lower levels of depression symptoms and higher life satisfaction scores. This underlines the outcomes of previous research emphasizing the association between attendance, engagement, and adherence in such interventions (53, 54).
Evaluation of the content of the different interventions showed that more variation in intervention content, modes of delivery and sequence of intervention messages correlated with lower post-intervention depressive scores (45). The outcomes of studies conducted by Chang et al. (45), Kim et al. (47), and Young et al. (42) showed that a multidimensional approach with human feedback and support based on elements of the CBT and SCT are most effective in the treatment of depression symptoms in individuals with obesity. Hereby, these interventions were fully tailored in multifactorial domains: the behavioral, cognitive, emotional, motivational, and physical domains. The majority of previous eHealth interventions focused on the mental health in individuals with obesity focused on diet, physical activity, weight loss or the combination of these (55–57). This emphasizes once again the complex reciprocal pathway between mental and bodily diseases and the importance of the treatment of both parts simultaneously in the treatment of individuals with obesity. On top of that, it underlines the relevance of the inclusion of cognitive features in obese treatment in order to achieve changes in the cognitive distortions, experienced by individuals with obesity. In contrast to such interventions, those focusing primarily on education through materials, i.e., non-interactive strategies showed less success in reducing depression symptoms (48, 49). Thus, interactive modules as used in the SHED-IT recharge intervention, conducted by Young et al. (42), that combined activities with educative materials, seemed to be particularly effective in the reduction of depression symptoms. The outcomes of this systematic review are in line with the outcomes of previously conducted meta-analyses and reviews, which showed that especially Internet-delivered Cognitive Behavioural Therapy (ICBT) is as effective as face-to-face therapy in the treatment of various mental disorders, such as depression, anxiety disorders and panic disorders (58, 59).
Strengths and limitations of the present review
To the best of our knowledge, this is the first systematic review to summarize evidence on the efficacy of eHealth interventions specifically targeted at the treatment of individuals with obesity to reduce depression symptoms. This work was conducted in accordance with the PRISMA guideline for systematic reviews (44). Only RCTs were included, as this is the golden standard for efficacy research. We used broad search terms and searched several large databases, which still resulted in a small number of studies included in this review. The studies included in this systematic review are heterogeneous and disparate, which puts several limitations on the summarized findings. Generally speaking, only English studies were included in the study. On top of that, there are few eHealth interventions that focus on depression symptoms the mental health in individuals with obesity. The focus in this review was specified on individuals with obesity and depression symptoms, resulting in a limited amount of studies that could have been included in this review. This limits the generalizability of the present findings and obstructs the performance of a meta-analysis. In addition, approximately three-quarters of the samples in the reported studies consisted of women. Next to this, each study included in this review made use of a different depression assessment instrument. Thus, there is a lack of standardized measurement instruments among different studies. Therefore, the way depression symptoms was measured in the N = 2371 participants included in this review is not uniform which could lead to deviations.
Conclusion
The evidence on interventions designed for individuals with obesity and depression symptoms as a primary outcome is very limited, only a small number of randomized controlled intervention studies have been published. The findings of this systematic literature review emphasize that eHealth interventions, targeting depression symptoms in individuals with obesity should be multidimensional. Furthermore, eHealth interventions that target both mental health, more specifically depression symptoms and physical health using interactive strategies are needed for better efficacy in meeting the needs of individuals with obesity. Especially eHealth interventions that included CBT modules or techniques and have integrated guided self-help approaches and digital tools seemed to have potentially high acceptance and efficacy in reducing depression symptoms. Hence, it can be concluded that future eHealth interventions that target depression symptoms in individuals with obesity should integrate CBT tools and techniques in combination with guided self-help approaches in order to enhance the efficacy of such interventions in reducing depression symptoms.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
DK: Writing – original draft. AB: Writing – original draft. TS: Writing – original draft. JBK: Writing – original draft. SG: Writing – original draft. E-MS: Writing – original draft. MT: Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1296433/full#supplementary-material
Abbreviations
BMI, Body Mass Index; DSM-V, Diagnostic and Statistical Manual of Mental Disorders; COVID-19, coronavirus disease 19; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta Analyses.
References
1. World Health Organization. Obesity and overweight (2021). Available online at: https://www.who.int/newsroom/fact-sheets/detail/obesity-and-overweight (Accessed 12.12.2021).
2. Eurostat. Over half of adults in the EU are overweight (2021). Available online at: https://ec.europa.eu/eurostat/de/web/products-eurostat-news/-/ddn-20210721-2 (Accessed 15.12.2021).
3. Dai H, Alsalhe TA, Chalghaf N, Riccò M, Bragazzi NL, Wu J. The global burden of disease attributable to high body mass index in 195 countries and territories, 1990-2017: An analysis of the Global Burden of Disease Study. PloS Med. (2020) 17:e1003198. doi: 10.1371/journal.pmed.1003198
4. Puigdomenech Puig E, Robles N, Saigi-Rubio F, Zamora A, Moharra M, Paluzie G, et al. Assessment of the efficacy, safety, and effectiveness of weight control and obesity management mobile health interventions: Systematic review. JMIR Mhealth Uhealth. (2019) 7:e12612. doi: 10.2196/12612
5. Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, Lee A, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. (2017) 377:13–27. doi: 10.1056/NEJMoa1614362
6. Avila C, Holloway AC, Hahn MK, Morrison KM, Restivo M, Anglin R, et al. An overview of links between obesity and mental health. Curr Obes Rep. (2015) 4:303–10. doi: 10.1007/s13679-015-0164-9
7. Lobner M, Stein J, Rost T, Förster F, Dorow M, Keller J, et al. [Innovative E-health approaches for comorbid depression in patients with obesity: Patient and expert perspectives on user acceptance]. Psychiatr Prax. (2017) 44:286–95. doi: 10.1055/s-0043-107471
8. Rajan TM, Menon V. Psychiatric disorders and obesity: A review of association studies. J Postgrad Med. (2017) 63:182–90. doi: 10.4103/jpgm.JPGM_712_16
9. Pereira-Miranda E, Costa PRF, Queiroz VAO, Pereira-Santos M, Santana MLP. Overweight and obesity associated with higher depression prevalence in adults: A systematic review and meta-analysis. J Am Coll Nutr. (2017) 36:223–33. doi: 10.1080/07315724.2016.1261053
10. Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. (2010) 67:220–9. doi: 10.1001/archgenpsychiatry.2010.2
11. Kinzl JF, Maier C and Bosch A. [Morbidly obese patients: psychopathology and eating disorders. Results of a preoperative evaluation]. Neuropsychiatr. (2012) 26:159–65. doi: 10.1007/s40211-012-0036-4
12. Scarpina F, Varallo G, Castelnuovo G, Capodaglio P, Molinari E, Mauro A. Implicit facial emotion recognition of fear and anger in obesity. Eat Weight Disord. (2021) 26:1243–51. doi: 10.1007/s40519-020-01010-6
13. Sanders RH, Han A, Baker JS, Cobley S. Childhood obesity and its physical and psychological co-morbidities: a systematic review of Australian children and adolescents. Eur J Pediatr. (2015) 174:715–46. doi: 10.1007/s00431-015-2551-3
14. Taylor VH, Forhan M, Vigod SN, McIntyre RS, Morrison KM. The impact of obesity on quality of life. Best Pract Res Clin Endocrinol Metab. (2013) 27:139–46. doi: 10.1016/j.beem.2013.04.004
15. Schwartz MB, Brownell KD. Obesity and body image. Body Image. (2004) 1:43–56. doi: 10.1016/S1740-1445(03)00007-X
16. Muller-Riemenschneider F, Reinhold T, Berghofer A, Willich SN. Health-economic burden of obesity in Europe. Eur J Epidemiol. (2008) 23:499–509. doi: 10.1007/s10654-008-9239-1
17. von Lengerke T, Krauth C. Economic costs of adult obesity: a review of recent European studies with a focus on subgroup-specific costs. Maturitas. (2011) 69:220–9. doi: 10.1016/j.maturitas.2011.04.005
18. Hoare E, Skouteris H, Fuller-Tyszkiewicz M, Millar L, Allender S. Associations between obesogenic risk factors and depression among adolescents: a systematic review. Obes Rev. (2014) 15:40–51. doi: 10.1111/obr.12069
19. Kivimaki M, Lawlor DA, Singh-Manoux A, Batty GD, Ferrie JE, Shipley MJ, et al. Common mental disorder and obesity: insight from four repeat measures over 19 years: prospective Whitehall II cohort study. BMJ. (2009) 339:b3765. doi: 10.1136/bmj.b3765
20. Marcus MD, Wildes JE. Obesity: is it a mental disorder? Int J Eat Disord. (2009) 42:739–53. doi: 10.1002/eat.20725
21. Volkow N, O'Brien C. Issues for DSM-V: Should obesity be included as a brain disorder? Am J Psychiatry. (2007) 164:708–10. doi: 10.1176/ajp.2007.164.5.708
22. Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognit Ther Res. (2012) 36:427–40. doi: 10.1007/s10608-012-9476-1
23. Cattivelli R, Guerrini Usubini A, Manzoni GM, Vailati Riboni F, Pietrabissa G, Musetti A, et al. ACTonFood. Acceptance and commitment therapy-based group treatment compared to cognitive behavioral therapy-based group treatment for weight loss maintenance: An individually randomized group treatment trial. Int J Environ Res Public Health. (2021) 18:9558. doi: 10.3390/ijerph18189558
24. Guerrini Usubini A, Cattivelli R, Bertuzzi V, Varallo G, Rossi AA, Volpi C, et al. The ACTyourCHANGE in teens study protocol: An acceptance and commitment therapy-based intervention for adolescents with obesity: A randomized controlled trial. Int J Environ Res Public Health. (2021) 18:6225. doi: 10.3390/ijerph18126225
25. Bacon L, Keim NL, Van Loan MD, Derricote M, Gale B, Kazaks A, et al. Evaluating a 'non-diet' wellness intervention for improvement of metabolic fitness, psychological well-being and eating and activity behaviors. Int J Obes Relat Metab Disord. (2002) 26:854–65. doi: 10.1038/sj.ijo.0802012
26. Foster GD, McGuckin BG. Estimating resting energy expenditure in obesity. Obes Res. (2001) 9 Suppl 5:367S–72S. doi: 10.1002/oby.2001.9.s5.367.
27. Beleigoli AM, Andrade AQ, Cancado AG, Paulo MN, Diniz MFH, Ribeiro AL, et al. Web-based digital health interventions for weight loss and lifestyle habit changes in overweight and obese adults: Systematic review and meta-analysis. J Med Internet Res. (2019) 21:e298. doi: 10.2196/jmir.9609
28. Mead E, Brown T, Rees K, Azevedo LB, Whittaker V, Jones D, et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst Rev. (2017) 6:CD012651. doi: 10.1002/14651858.CD012651
29. World Health Organization. Using e-health and information technology to improve health (2022). Available online at: https://www.who.int/westernpacific/activities/using-e-health-andinformationtechnology-to-improve-health (Accessed 02.07.2022).
30. Jamal A, McKenzie K and Clark M. The impact of health information technology on the quality of medical and health care: a systematic review. Health Inf Manag. (2009) 38:26–37. doi: 10.1177/183335830903800305
31. Davalos ME, French MT, Burdick AE, Simmons SC. Economic evaluation of telemedicine: review of the literature and research guidelines for benefit-cost analysis. Telemed J E Health. (2009) 15:933–48. doi: 10.1089/tmj.2009.0067
32. Bauerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health (Oxf). (2020) 42:672–8. doi: 10.1093/pubmed/fdaa106
33. Bauerle A, Graf J, Jansen C, Musche V, Schweda A, Hetkamp M, et al. E-mental health mindfulness-based and skills-based 'CoPE It' intervention to reduce psychological distress in times of COVID-19: study protocol for a bicentre longitudinal study. BMJ Open. (2020) 10:e039646. doi: 10.1136/bmjopen-2020-039646
34. Arem H, Irwin M. A review of web-based weight loss interventions in adults. Obes Rev. (2011) 12:e236–243. doi: 10.1111/j.1467-789X.2010.00787.x
35. Hutchesson MJ, Rollo ME, Krukowski R, Ells L, Harvey J, Morgan PJ, et al. eHealth interventions for the prevention and treatment of overweight and obesity in adults: a systematic review with metaanalysis. Obes Rev. (2015) 16:376–92. doi: 10.1111/obr.12268
36. Neve M, Morgan PJ, Jones PR, Collins CE. Effectiveness of web-based interventions in achieving weight loss and weight loss maintenance in overweight and obese adults: a systematic review with meta-analysis. Obes Rev. (2010) 11:306–21. doi: 10.1111/j.1467-789X.2009.00646.x
37. Stinson J, Wilson R, Gill N, Yamada J, Holt JA. A systematic review of internet-based selfmanagement interventions for youth with health conditions. J Pediatr Psychol. (2009) 34:495–510. doi: 10.1093/jpepsy/jsn115
38. Ma J, Rosas LG, Lv N, Xiao L, Snowden MB, Venditti EM, et al. Effect of integrated behavioral weight loss treatment and problem-solving therapy on body mass index and depressive symptoms among patients with obesity and depression: The RAINBOW randomized clinical trial. JAMA. (2019) 321:869–79. doi: 10.1001/jama.2019.0557
39. Hutchesson MJ, Tan CY, Morgan P, Callister R, Collins C. Enhancement of self-monitoring in a web- based weight loss program by extra individualized feedback and reminders: Randomized trial. J Med Internet Res. (2016) 18:e82. doi: 10.2196/jmir.4100
40. Young MD, Morgan PJ. Effect of a gender-tailored eHealth weight loss program on the depressive symptoms of overweight and obese men: Pre-post study. JMIR Ment Health. (2018) 5:e1. doi: 10.2196/mental.8920
41. Ryan K, Dockray S and Linehan C. A systematic review of tailored eHealth interventions for weight loss. Digit Health. (2019) 5:2055207619826685. doi: 10.1177/2055207619826685
42. Young MD, Drew RJ, Kay-Lambkin F, Collins CE, Callister R, Kelly BJ, et al. Impact of a self-guided, eHealth program targeting weight loss and depression in men: A randomized trial. J Consult Clin Psychol. (2021) 89:682–94. doi: 10.1037/ccp0000671
43. Hoare E, Fuller-Tyszkiewicz M, Skouteris H, Millar L, Nichols M, Allender S. Systematic review of mental health and well-being outcomes following community-based obesity prevention interventions among adolescents. BMJ Open. (2015) 5:e006586. doi: 10.1136/bmjopen-2014-006586
44. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PloS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
45. Chang MW, Nitzke S and Brown R. Mothers In Motion intervention effect on psychosocial health in young, low-income women with overweight or obesity. BMC Public Health. (2019) 19:56. doi: 10.1186/s12889-019-6404-2
46. Jones RA, Mueller J, Sharp SJ, Vincent A, Duschinsky R, Griffin SJ, et al. The impact of participant mental health on attendance and engagement in a trial of behavioural weight management programmes: secondary analysis of the WRAP randomised controlled trial. Int J Behav Nutr Phys Act. (2021) 18:146. doi: 10.1186/s12966-021-01216-6
47. Kim M, Kim Y, Go Y, Lee S, Na M, Lee Y, et al. Multidimensional cognitive behavioral therapy for obesity applied by psychologists using a digital platform: open-label randomized controlled trial. JMIR Mhealth Uhealth. (2020) 8:e14817. doi: 10.2196/14817
48. Marcus BH, Hartman SJ, Larsen BA, Pekmezi D, Dunsiger SI, Linke S, et al. Pasos Hacia La Salud: a randomized controlled trial of an internet-delivered physical activity intervention for Latinas. Int J Behav Nutr Phys Act. (2016) 13:62. doi: 10.1186/s12966-016-0385-7
49. Welzel FD, Bar J, Stein J, Löbner M, Pabst A, Luppa M, et al. Using a brief web-based 5A intervention to improve weight management in primary care: results of a cluster-randomized controlled trial. BMC Fam Pract. (2021) 22:61. doi: 10.1186/s12875-021-01404-0
50. Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
51. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. (2001) 52:1–26. doi: 10.1146/annurev.psych.52.1.1
52. Rentrop V, Damerau M, Schweda A, Steinbach J, Schüren LC, Niedergethmann M, et al. Predicting acceptance of e-mental health interventions in patients with obesity by using an extended unified theory of acceptance model: Cross-sectional study. JMIR Form Res. (2022) 6:e31229. doi: 10.2196/31229
53. Burley C, Anderson D, Brownlee A, Lafer G, Luong T, McGowan M, et al. Increasing engagement in eHealth interventions using personalization and implementation intentions. In: 2020 Systems and Information Engineering Design Symposium (SIEDS), Charlottesville, VA, USA (2020). p. 1–5.
54. Gustafson DH Sr, Kornfield R, Mares ML, Johnston DC, Cody OJ, Yang EF, et al. Effect of an eHealth intervention on older adults' quality of life and health-related outcomes: a randomized clinical trial. J Gen Intern Med. (2022) 37:521–30. doi: 10.1007/s11606-021-06888-1
55. Kim EK, Kwak SH, Jung HS, Koo BK, Moon MK, Lim S, et al. The effect of a smartphone-based, patient- centered diabetes care system in patients with type 2 diabetes: A randomized, controlled trial for 24 weeks. Diabetes Care. (2019) 42:3–9. doi: 10.2337/dc17-2197
56. Mummah SA, Mathur M, King AC, Gardner CD, Sutton S. Mobile technology for vegetable consumption: A randomized controlled pilot study in overweight adults. JMIR Mhealth Uhealth. (2016) 4:e51. doi: 10.2196/mhealth.5146
57. Turner-McGrievy GM, Hales SB, Schoffman DE, Valafar H, Brazendale K, Weaver RG, et al. Choosing between responsivedesign websites versus mobile apps for your mobile behavioral intervention: presenting four case studies. Transl Behav Med. (2017) 7:224–32. doi: 10.1007/s13142-016-0448-y
58. Andersson G. Internet-delivered psychological treatments. Annu Rev Clin Psychol. (2016) 12:157–79. doi: 10.1146/annurev-clinpsy-021815-093006.21
Keywords: e-mental health, depression, eHealth intervention, obesity, mental health
Citation: Kocol D, Bäuerle A, Schadendorf T, Geiger S, Krakowczyk JB, Skoda E-M and Teufel M (2024) Efficacy of eHealth interventions to reduce depression symptoms in individuals with obesity: a systematic review of randomized controlled trials. Front. Psychiatry 15:1296433. doi: 10.3389/fpsyt.2024.1296433
Received: 18 September 2023; Accepted: 07 February 2024;
Published: 07 March 2024.
Edited by:
Heleen Riper, VU Amsterdam, NetherlandsReviewed by:
Nami Mohammadian Khonsari, Alborz University of Medical Sciences, IranGiorgia Varallo, University of Parma, Italy
Copyright © 2024 Kocol, Bäuerle, Schadendorf, Geiger, Krakowczyk, Skoda and Teufel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dilara Kocol, ZGlsYXJhLmtvY29sQGx2ci5kZQ==
†These authors have contributed equally to this work