
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 07 March 2024
Sec. Anxiety and Stress Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1293935
 Kinga Grochowalska1*†
Kinga Grochowalska1*† Marcin Ziętkiewicz1†
Marcin Ziętkiewicz1† Katarzyna Nowicka-Sauer2
Katarzyna Nowicka-Sauer2 Mariusz Topolski3
Mariusz Topolski3 Ewa Więsik-Szewczyk4Aleksandra Matyja-Bednarczyk5
Ewa Więsik-Szewczyk4Aleksandra Matyja-Bednarczyk5 Katarzyna Napiórkowska-Baran6Zbigniew Zdrojewski1
Katarzyna Napiórkowska-Baran6Zbigniew Zdrojewski1Background: Patients with inborn errors of immunity (IEI) experience recurrent infections, autoimmunity, and malignancies. Owing to repeated medical procedures, the need for constant treatment and surveillance, and the unpredictable course of the disease, patients with IEI are prone to develop mental health disorders, including anxiety. In this study, we aimed to assess the prevalence and level of anxiety symptoms in adult Polish patients with IEI and explore the determinants of anxiety in this group of patients.
Methods: Data from 105 Polish patients with IEI were collected via the hospital anxiety and depression scale (HADS), brief illness perception questionnaire (B-IPQ), illness cognition questionnaire (ICQ), Pittsburgh sleep quality index (PSQI), and a questionnaire on general health and demographic data. For statistical analyses of data, the normality of distribution of quantitative data was assessed, and internal consistency of tests was investigated using Cronbach’s alpha coefficient; moreover, we performed the analysis of correlations and between-group differences, and path analysis to explore causal relationships. Significance was considered at p < 0.050.
Results: Thirty-eight (36.2%) patients had anxiety symptoms (HADS-A ≥ 8); 14 (13.3%) patients had severe anxiety (score ≥ 11), and 24 (22.9%) had moderate anxiety (score of 8–10). Patients with poor sleep quality, higher pain frequency, younger age, and no fixed income had higher anxiety scores than others. Emotional and cognitive representations of illness were positively correlated with anxiety levels. Intense anxiety was related to more negative illness perception, higher helplessness, lower illness acceptance, and lower perceived benefits.
Discussion: Anxiety is common in patients with IEI. However, results indicate that it is not related to a more severe course of IEI or several comorbidities, whereas, pain frequency and poor sleep quality were identified to be important clinical factors for anxiety. Because anxiety was related to negative illness perception, psychological therapy may apply to this group of patients.
Inborn errors of immunity (IEI) comprise a heterogeneous group of inherited disorders affecting the immune system (1). Previously, IEI were known as primary immunodeficiency disorders. The clinical manifestations of IEI include increased susceptibility to infections, autoimmunity, autoinflammatory diseases, allergies, and malignancies (2). Patients with IEI experience a deterioration in their physical condition owing to chronic patterns and recurrent infections. Furthermore, owing to repeated medical procedures, the need for constant treatment and surveillance, the threat of malignancy, and the unpredictable course of the disease; patients are prone to developing mental health disorders, including anxiety and depression (3).
Patient-reported outcomes (PROs) are a type of outcomes that are used to assess the subjective health status from the patients’ perspective without physicians’ interpretation (4). PROs constitute an essential component of psychological mental health assessment because they capture a patient’s subjective experience of the disease or intervention, which may not be reflected in clinical endpoints (5). The implementation of PROs is faced with many obstacles in daily clinical practice (6). Nevertheless, they should be integrated into the clinical routine.
Anxiety is a mental state characterized by excessive fear and concern about potential situations (7). It may be caused by external or internal factors (8). Although anxiety is common in chronic diseases (9), it is not routinely assessed and is rarely treated (10). Recent scientific reports have revealed an increased level of anxiety in patients with IEI (11). However, to the best of our knowledge, the determinants of anxiety have not yet been investigated.
Illness perception defines patients’ beliefs about their disease. According to the Common Sense Model theory, each patient experiencing a disease creates his or her own representation of a condition (12). It comprises of cognitive and emotional representations (13). Cognitive representation comprises five dimensions: identity (patient’s description of illness), consequences (how an illness impacts patient’s life), cause (patient’s beliefs regarding the cause of a disease), timeline (length of the disease in patient’s belief), and cure or control (patient’s belief about the effectiveness of treatment and perceived control of the disease) (14). Emotional representation comprises concerns and negative emotions related to a disease. In addition, this model involves the patient’s understanding of a disease (15).
Illness perception influences emotional reactions in patients and how they cope with daily situations (16). In recent years, interest in the assessment of illness perception has increased. As a potentially modifiable aspect of chronic diseases, illness perception may improve clinical outcomes, or vice versa, leading to even higher mortality (17, 18).
Patients with chronic diseases may experience a range of negative emotions, including anxiety, depression, irritation, and anger, which can interfere (19). In this study, we aimed to investigate these problems in our patients. Previously, patients with IEI were mainly assessed for the prevalence of depression. However, some studies revealed that anxiety is potentially more prevalent than depression among patients with IEI (20), and it is often overlooked in clinical practice. In our previous study (3), which included a part of the current study (n=92), anxiety symptoms were frequent. Therefore, we expanded our sample (n=105) and considered anxiety as a dependent variable to perform a more precise analysis of factors, including anxiety levels, the association of anxiety levels with sleeping disorders, and pain. Moreover, we have evaluated the frequency of pain to determine whether chronic pain is associated with increased anxiety levels.
Anxiety disorders and high levels of anxiety are related to sleeping problems, leading to altered sleep quality. Sleep disorders are common among patients with chronic medical conditions (21). Many longitudinal studies revealed bidirectional correlations between sleep quality and anxiety (22). Previously (3), using a multiple linear regression model, we identified anxiety symptoms as an important predictor of poor sleep quality. Therefore, we decided to further analyze the association between anxiety and sleep quality in the current manuscript.
In this study, we assessed the prevalence of anxiety symptoms and anxiety levels in adult Polish patients with IEI. We also explored the clinical, sociodemographic, and psychological determinants of anxiety in this patient group. To the best of our knowledge, this is the first study to assess illness perception in patients with IEI.
Adult patients (≥ 18 years) diagnosed with IEI according to the diagnostic criteria of the European Society for Immunodeficiencies (23) were recruited from four Polish clinical centers in Bydgoszcz, Gdańsk, Kraków, and Warszawa between February 2021 and December 2022. In total, 120 eligible individuals were selected for this study. Eight patients refused to participate in the study. Seven individuals were excluded because they did not complete the questionnaires. Finally, 105 participants, including 55 women (52.4%) and 50 men (47.6%) with a mean age of 42.16 ± 14.1 years were recruited in this study.
In this cross-sectional observational study, data were collected via the hospital anxiety and depression scale (HADS), brief-illness perception questionnaire (B-IPQ), illness cognition questionnaire (ICQ), and Pittsburgh sleep quality index (PSQI).
Additionally, the survey included demographic questions regarding age, sex, professional activity, and residential status, and clinical data, including comorbidities and type of treatment, with special emphasis on immunoglobulin replacement therapy.
To describe pain, we assessed its frequency with the following questions: How often did you experience pain during the last 3 months? Possible answers were: “not at all”, “for a few days”, “more than 30 days”, or “almost every day”.
To determine the disease activity, we evaluated the following variables: the number of infections in the last 3 months, antibiotic administration in the last 3 months, and hospitalizations (excluding those for immunoglobulin administration) in the last 3 months.
All patients provided written informed consent before the study. The study design was approved by the Independent Bioethics Commission for Research of the Medical University of Gdańsk (Number: 422/2017).
The HADS consists of 14 questions, including seven for the anxiety subscale (HADS-A), and seven for the depression subscale (HADS-D), which are rated on a 0–3 response Likert scale. The maximum score for each subscale is 21 points; scores < 8 indicate a normal result, whereas, 8–10 points indicate moderate anxiety or depressive symptoms, and ≥ 11 presents severe depressive or anxiety symptoms (24). In the present study, we used a modified version of HADS since we sought to assess a wider range of emotions and modified HADS allows to assess irritability. HADS-M contains the following items: (I) “It happened that during the last week, I exploded with anger”; (II) “It happened that I got upset internally”. Patients assess their irritability level using a Likert scale with scores ranging from 0 (“not at all”) to 6 points (“frequently”), where a higher score indicated a higher level of irritability. The modified HADS has satisfactory psychometric properties (19). In this study, Cronbach’s alpha coefficients for depression, anxiety, and irritability subscales of HADS were 0.86, 0.82, and 0.84, respectively.
The B-IPQ is widely used to measure cognitive and emotional representations of illnesses in patients with various chronic diseases. It consists of eight items rated on a 0-to-10 response scale. Additionally, it includes an open-ended question regarding patient-perceived causes of the disease (13, 14). Each of the eight items refers to one of the following illness perception dimensions: consequences, timeline, personal control, treatment control, identity, coherence, concern, and emotional response. Moreover, emotional and cognitive representations scores can be calculated. A higher total B-IPQ score indicates a more negative illness perception (13, 14). A previous study, conducted among patients with chronic somatic diseases, validated the psychometric properties of the Polish version of the B-IPQ (13). In the present study, Cronbach’s alpha was 0.75.
The ICQ is an 18-item instrument that measures three dimensions of illness cognition: helplessness, acceptance, and perceived benefits (25, 26). Helplessness indicates the degree of powerlessness and hopelessness experienced by patients regarding their condition and its consequences in their lives. Acceptance refers to the degree of adaptation and integration of a condition into reality. Perceived benefits indicate the degree of positive outcomes or opportunities that patients perceive in their conditions. Each item is rated on a 4-point Likert scale ranging from 1 (not at all) to 4 (completely). The points for each subscale are added and range from 6 to 24 (25, 27). Higher subscale scores indicate higher, helplessness, acceptance, and perceived benefits. In the original study (25), Cronbach’s alpha ranged from 0.84 to 0.90. The current study involving patients with IEI exhibited satisfactory internal consistency of all three subscales (Cronbach’s alpha coefficients: 0.88 for helplessness, 0.87 for acceptance, and 0.83 for perceived benefits).
The PSQI is a self-rated questionnaire that measures sleep quality and disturbances over one month (28). It comprises 19 items grouped into seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Each domain is scored from 0 to 3, with higher scores indicating poorer sleep quality or more sleep-associated problems. The sum of the seven domain scores yields the global PSQI score, which ranges from 0 to 21. A global PSQI score ≥5 indicates poor sleep quality (29). The internal consistency of the PSQI assessed using Cronbach’s alpha coefficient was 0.83 (28). The Polish version of the scale was used in a study that involved Polish patients with systemic lupus erythematosus (SLE) (30). In the present study, Cronbach’s alpha was 0.82.
Descriptive statistics (mean, standard deviation, median, maximal, and minimal value for quantitative variables, and number and percentage for categorical variables) were analysed to summarize the study outcomes. The internal consistency of the scales was verified using the Cronbach’s alpha coefficient. The normality of the distribution of the variables was verified using the Shapiro–Wilk test. Continuous variables were analyzed using Student’s t-, Mann–Whitney U, and Kruskal–Wallis tests with post-hoc Dunn analysis, in case of multiple comparisons. Associations between anxiety and categorical variables were assessed via between-group comparisons. Categorical variables were analyzed using the chi-square or Fisher exact tests. The associations between anxiety level and quantitative independent variables were assessed using Spearman’s rho correlation coefficient. Path analysis was used to examine both direct effects, which are the direct influences of one variable on another, and indirect effects, which result from the path between two variables through one or more other variables. In the diagram, the variables are represented as nodes and the directional relationships between them are represented with arrows. The path analysis was conducted using the AMOS package. Significance was considered at p < 0.050. Statistical analysis was performed using the STATISTICA software (version 13; TIBCO Software Inc., Palo Alto, CA, USA).
In the statistical analysis, descriptive statistics were first calculated for categorical variables (Table 1) and quantitative variables (Table 2).
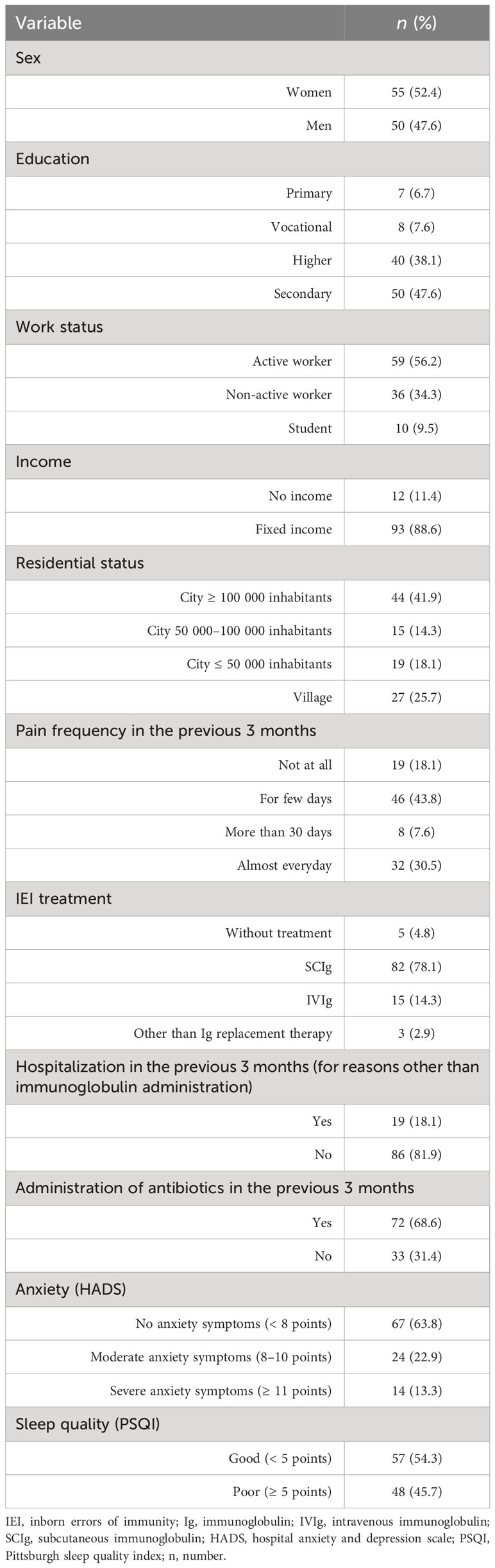
Table 1 Frequency and percentage statistics for categorical variables in the studied sample of patients with inborn errors of immunity (n=105).
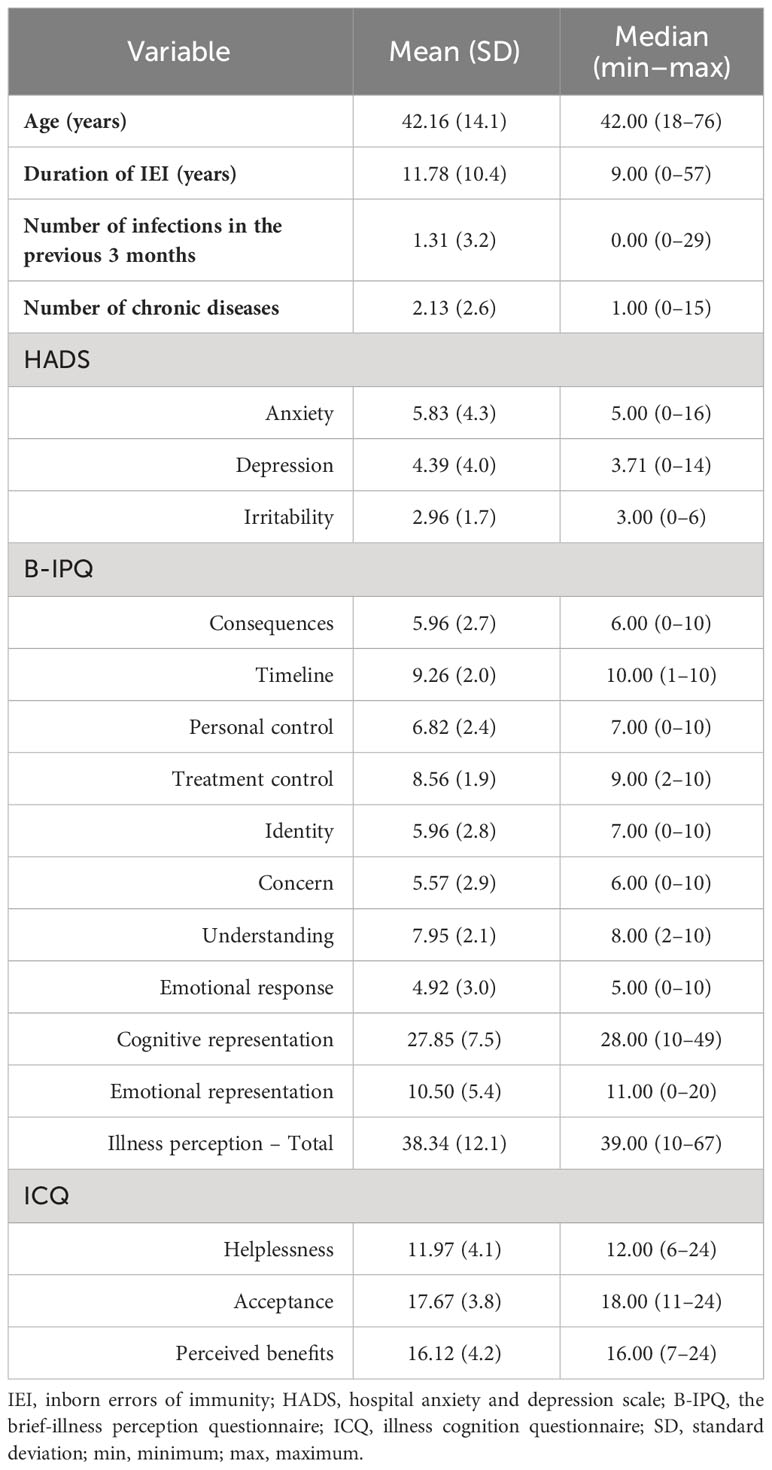
Table 2 Descriptive statistics for quantitative variables in the studied sample of patients with inborn errors of immunity (n=105).
Anxiety symptoms (HADS-A ≥ 8) were detected in 38 (36.2%) patients; 14 (13.3%) patients reported a score ≥ 11 indicating severe anxiety symptoms, and 24 (22.9%) patients had moderate anxiety symptoms (Table 1).
PSQI-based analysis revealed that 57 patients (54.3%) had good sleep quality, whereas, 48 patients (45.7%) reported poor sleep quality (Table 1). The majority of patients (n=86, 81.9%) experienced general pain. Only 18.1% of patients (n = 19) did not report pain in the previous 3 months, whereas 30.5% of the patients (n = 32) reported pain almost every day (Table 1).
The mean age was 42.16±14.1 years, the mean IEI duration was 11.78 ± 10.4 years; the mean number of chronic disease was recorded to be 2.13 ± 2.6. (Table 2).
The correlation analysis was performed to explore the association between anxiety levels and quantitative variables (Table 3). Age and number of chronic diseases were not significantly correlated with anxiety levels (Table 3). Moreover, disease-related factors, such as IEI duration and the number of infections in the previous 3 months, were not correlated with anxiety levels (Table 3).
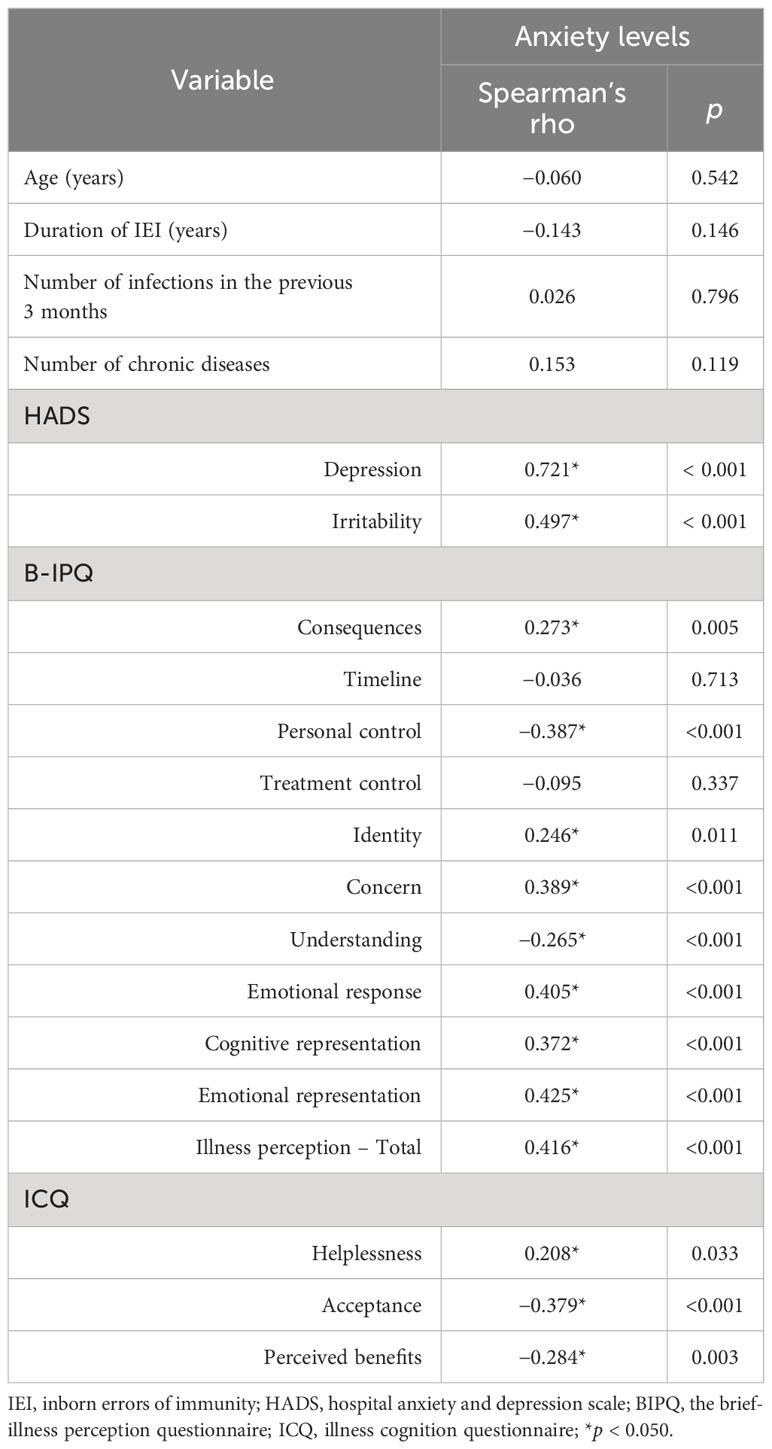
Table 3 Matrix of Spearman’s rho correlation coefficients between the anxiety level (dependent variable) and independent variables in the studied sample of patients with inborn errors of immunity (n=105).
B-IPQ revealed that, among the illness perception dimensions, statistically significant positive correlations were detected between anxiety and consequences (r = 0.273; p = 0.005), identity (r = 0.246; p = 0.011), concern (r = 0.389; p < 0.001), and emotional response (r = 0.405; p < 0.001). Significant negative correlations were found between anxiety and personal control (r = −0.387; p < 0.001), as well as understanding (r = −0.265; p < 0.001); whereas emotional representation (r = 0.425; p < 0.001), cognitive representation (r = 0.372; p < 0.001), and total illness perception score (r = 0.416; p < 0.001) showed significant positive correlation with anxiety (Table 3).
In the ICQ results, we noted a positive correlation between anxiety and helplessness (r = 0.208; p = 0.033), and a negative correlation between anxiety and acceptance (r = −0.379; p < 0.001) and perceived benefits (r = −0.284; p = 0.003) (Table 3).
Significant positive correlations of anxiety with depression (r = 0.721; p < 0.001), irritability (r = 0.497; p < 0.001) were detected (Table 3).
The analysis of relationship between anxiety and categorical variables was performed using group comparisons (Table 4).
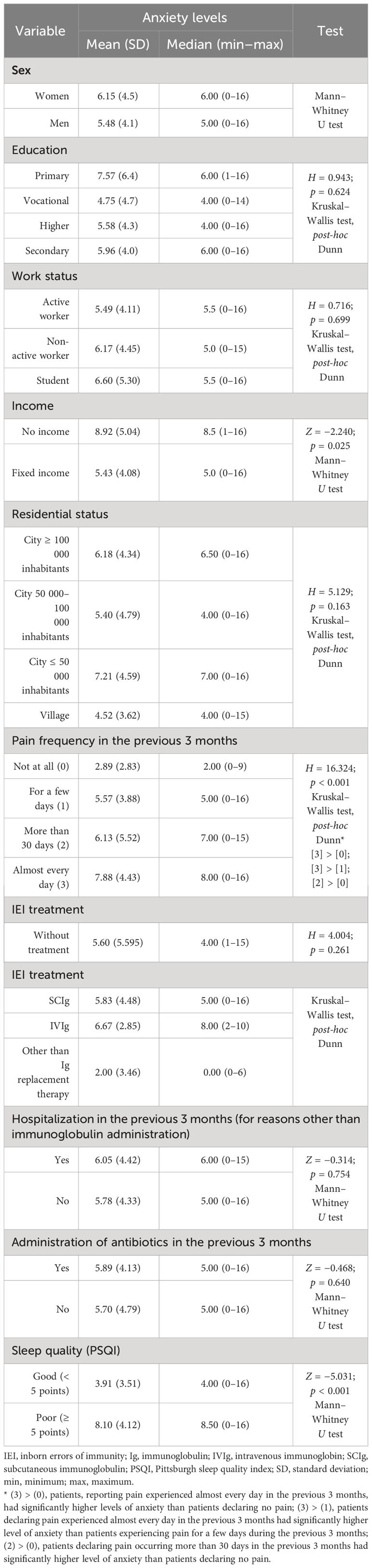
Table 4 Differences in anxiety levels in relation to independent categorical variables in the studied sample of patients with inborn errors of immunity (n=105).
Among the sociodemographic factors, only income exhibited a correlation with anxiety; patients with no income had significantly higher anxiety levels compared to those with fixed incomes (scores of 8.92 ± 5.04 vs. 5.43 ± 4.08; p = 0.025). Sex, education, professional activity, and domicile were not associated with anxiety (Table 4).
Among clinical features, only pain frequency was related to anxiety levels. Patients with a higher pain frequency had a higher anxiety score (p < 0.001). Hospitalization in the previous 3 months, antibiotic administration, and IEI treatment were not related to anxiety (Table 4).
Patients with poor sleep quality had a higher score for anxiety than those with good sleep quality (8.10 ± 4.12 vs. 3.91 ± 3.51; p < 0.001) (Table 4). The majority of patients (n = 41, 82.0%) with good sleep quality did not experience anxiety.
To explore the causal relationship between studied variables, path analysis was performed. The obtained value of the root mean square error of approximation (RMSEA) parameter (0.038; p < 0.050), indicated a well-fitting model and was statistically significant. Higher scores for irritability (Beta = 0.615), depression (Beta = 0.598), and emotional representation (Beta = 0.446), as well as lower scores for personal control (Beta = −0.198), higher treatment control (Beta = 0.271), lower perceived benefits (Beta = −0.214), and lower timeline (Beta = −0.218), were associated with higher anxiety scores. This model explains 70.3% of the variance. These results were further reinforced by moderator A, which consists of the following relationships: higher likelihood of poor sleep quality (p = 0.759) and lower acceptance (Beta = −0.219), higher frequency of pain (“at least 1 month in previous 3 months” and “almost every day in previous 3 months”; p = 0.638), younger age (Beta = −0.218), and lower number of infections (Beta = −0.174). These relationships enhance the association between construct B and the dependent variable by approximately 14%. On the contrary, construct A alone explained 30.9% of the total variance in anxiety (Figure 1).
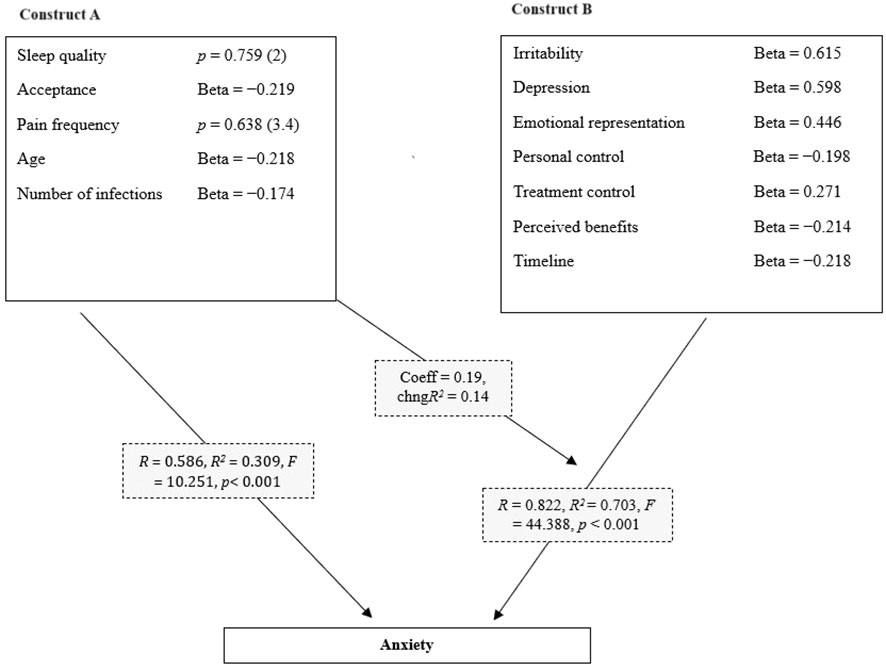
Figure 1 Path analysis of potential causal relationships between anxiety level and independent variables in the studied sample of patients with inborn errors of immunity (n=105). (RMSEA = 0.038; CFI = 0.951; CMIN = 44.287; p < 0.01). The following statistics were used in the moderation analysis. ;R: Correlation before moderation; R2: Coefficient of determination before moderation; Change in R2: Change in the coefficient of determination due to moderation; Coeff - coefficient of moderation analysis; p: significance of the moderator’s influence on the model; RMSEA: Model fit index.
Patients with chronic diseases might be affected by psycho-emotional disorders. They may experience psychological distress, such as fear, anger, helplessness, powerlessness, and a range of negative affective states. In current attempts to provide the highest compliance, there has been a constant improvement in medical therapies and treatment protocols. Hence, assessing patient-related outcomes, including emotional state and illness perception could be indispensable.
The subjective image of a disease is reported to be more relevant to the patient than the measured disease severity (31). While exploring other factors related to the well-being of patients with IEI, we decided to evaluate the frequency and level of anxiety and the factors associated with enhanced levels of anxiety.
Among the patients included in this study, 36.2% had anxiety symptoms according to HADS, with 13.3% and 22.9% having severe and moderate levels of anxiety, respectively. A review of the literature reveals a strong association between anxiety and chronic diseases (32). However, anxiety is frequently overlooked and inadequately managed; therefore, appropriate diagnosis and intervention are required. Owing to a lack of awareness and underestimation of the prevalence of anxiety, many patients do not receive proper treatment. Anyfanti et al. studied 514 patients with rheumatic disease and noted anxiety and depression in 30.8% and 21.8% of the patients, respectively. However, anti-anxiety medications were prescribed to only 12.1% of the patients with anxiety symptoms (10).
Improper treatment of anxiety and depressive symptoms may lead to the failure of somatic disease treatment. Matcham et al. conducted a longitudinal study to investigate the association between symptoms of anxiety and depression, and the response to prednisolone. Interestingly, patients with symptoms of anxiety or depression at the baseline also showed a 50% reduction in the effects of prednisolone treatment compared to patients with no symptoms of anxiety or depression at the baseline (33). Owing to the worsening mental health and diminishing treatment efforts, anxiety and depression are associated with increased mortality in patients with rheumatoid arthritis (34), chronic obstructive pulmonary disease, and heart failure (35). Hence, studies exploring the determinants of negative emotionality, especially the modifiable ones, are crucial, since they allow for the implementation of targeted and effective interventions.
Only a few studies on anxiety in patients with IEI have been reported. In a pilot study, Heath et al. detected that anxiety was more frequent in patients with IEI (n = 33) than in the general population. Risk factors for significantly elevated anxiety include poor health and a lack of refreshing sleep (11).
Sower et al. identified significantly higher anxiety scores in 292 patients with IEI compared to the normative values. Besides enhanced anxiety and depression, patients with IEI exhibited a greater degree of perceived memory impairment or brain fog (36). Previously, we revealed that 38% of patients with IEI had anxiety symptoms, which were more frequent than depression symptoms (3).
In this study, no correlations were detected between the activity of the disease and the anxiety levels. Pain was considered the only important clinical feature. Thus, clinical data alone are insufficient for determining the anxiety levels. Among sociodemographic variables, only age and income status were related to anxiety levels.
In our group, patients who had fewer infections and did not receive antibiotics in the previous 3 months, a sign of a more benign course of IEI, had higher levels of anxiety. Anxiety level was not related to disease duration, number of comorbidities, or number of hospitalizations. The only significant clinical variable was pain frequency. Patients with higher pain frequency had higher levels of anxiety. Smith et al. conducted an 11-week study to examine the influence of anxiety and depression on pain in women with arthritis. They revealed that both anxiety and depression predicted higher levels of pain in the same and the following weeks; however, the impact of anxiety was stronger than that of depression (37). Contrarily, Kosson et al. examined 1025 patients treated in pain clinics and revealed that the level of anxiety can be determined by pain intensity. A higher pain intensity was associated with higher anxiety levels (38). Although the causal relationship between pain and anxiety remains unclear, it appears to be bidirectional. Further longitudinal studies are required to determine the direction of this association. According to the findings described above, it is crucial to assess the anxiety status of patients experiencing pain.
Our study revealed that patients with poor sleep quality had higher anxiety scores than those with good sleep quality. Our results are consistent with those reported by Heath et al. who revealed that a lack of refreshing sleep was a risk factor for significantly elevated anxiety in patients with IEI (11).
The current study revealed significant associations between anxiety and several psychological variables in both the correlation and path analyses. More intense anxiety was associated with higher levels of depression and irritability, indicating a more complex multidimensional picture of negative emotionality. Moreover, more negative emotional and cognitive representations of illness, including perceived severe consequences and symptoms, perceived personal uncontrollability of the disease and lower understanding as well as higher helplessness, lower acceptance of the disease and lower perceived benefits related to the disease, were significantly associated with heightened levels of anxiety. Despite the high perceived treatment effectiveness and low frequency of infections, patients had a very high average score (9.2) in the timeline dimension, with a median score of 10 points. These results indicate patients’ awareness of the chronic course of their disease.
A perusal of the literature provides insights into the association between illness perception and anxiety in many chronic conditions (18). The results of the present study are comparable to previous reports that revealed that a more negative perception of illness is associated with higher anxiety (39). Similarly, an association of helplessness with anxiety and depression was reported in patients with systemic lupus erythematosus (40). In a study conducted among patients with type 1 diabetes, those who perceived disease benefits had more positive illness perception and lower levels of depression, anxiety, and irritability (41).
Furthermore, the impact of illness perception on emotional states, including depression, anxiety, and mental well-being, was reported in patients with heart failure (42, 43), fibromyalgia (44), and unruptured intracranial aneurysm (45).
The results of the present study indicate that targeted interventions focusing on maladaptive illness perception are potentially important. Cognitive behavioral therapy resulted in a more positive illness perception and less anxiety in patients with unruptured intracranial aneurysms (45). The strong association between the cognitive model of illness and its emotional dimensions observed in our study justifies the suggestion that psychological therapies should address both cognitive illness representation and regulation of emotions (43, 44). Hence, interventions focused on illness perception should be considered as a part of a holistic medical approach that leads to improved health outcomes (18, 36).
Despite careful planning, this study had some limitations. Anxiety symptoms were assessed using the HADS and were not verified according to the DSM-5 classification. Psychiatric examination is the best method to evaluate mental disorders. However, conducting a psychiatric examination for every patient would be difficult. Therefore, primary screening with the usage of standardized questionnaires seems justified in search for patients at higher risk of a mental disorder.
Furthermore, the patients were asked to provide their chronic disease information; however, we did not investigate mental disorders other than those mentioned by the patients. Patients provided data concerning general health and medication administration, which were not further verified. Nearly one-third of the patients did not name the administrated medicines; therefore, this variable was excluded from the analysis. Unlike a longitudinal study, this observational study did not support the observation of progression; however, the conducted path analysis led to preliminary conclusions about a causal relationship. Prospective, further interventional studies can shed more light on this topic.
Our study revealed that anxiety is common in patients with IEI. Anxiety was not related to a more severe course of IEI or the number of comorbidities, whereas pain and poor sleep quality were important clinical factors associated with high anxiety levels. Therefore, proper assessment and subsequent treatment of pain and sleep disorders may be beneficial.
We cannot infer the level of anxiety based on clinical data, as subjective illness perception has proven to be the most crucial factor. Our study revealed that anxiety is related to negative illness perception and, therefore, psychological therapy can be beneficial to patients with IEI. Future studies with a larger group of patients could further reveal the relationship between negative emotionality, illness representation, and clinical features of immunodeficiencies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Independent Bioethics Commission for Research of the Medical University of Gdańsk (Number: 422/2017). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
KG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. MZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. KNS: Conceptualization, Supervision, Writing – original draft. MT: Methodology, Writing – review & editing. EWS: Data curation, Writing – review & editing. AM: Data curation, Writing – review & editing. KN-B: Data curation, Writing – review & editing. ZZ: Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We thank the patients for their time and support during the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pieniawska-Śmiech K, Pasternak G, Lewandowicz-Uszyńska A, Jutel M. Diagnostic challenges in patients with inborn errors of immunity with different manifestations of immune dysregulation. J Clin Med. (2022) 11. doi: 10.3390/jcm11144220
2. Zhang SY, Jouanguy E, Zhang Q, Abel L, Puel A, Casanova JL. Human inborn errors of immunity to infection affecting cells other than leukocytes: from the immune system to the whole organism. Curr Opin Immunol. (2019) 59:88–100. doi: 10.1016/j.coi.2019.03.008
3. Grochowalska K, Ziętkiewicz M, Więsik-Szewczyk E, Matyja-Bednarczyk A, Napiórkowska-Baran K, Nowicka-Sauer K, et al. Subjective sleep quality and fatigue assessment in Polish adult patients with primary immunodeficiencies: A pilot study. Front Immunol. (2023) 13:1028890. doi: 10.3389/fimmu.2022.1028890
4. Rivera SC, Kyte DG, Aiyegbusi OL, Slade AL, McMullan C, Calvert MJ. The impact of patient-reported outcome (PRO) data from clinical trials: A systematic review and critical analysis. Health Qual Life Outcomes. (2019) 17:1–19. doi: 10.1186/s12955-019-1220-z
5. Cruz Rivera S, McMullan C, Jones L, Kyte D, Slade A, Calvert M. The impact of patient-reported outcome data from clinical trials: perspectives from international stakeholders. J Patient-Rep Outcomes. (2020) 4(1):51. doi: 10.1186/s41687-020-00219-4
6. Nelson EC, Eftimovska E, Lind C, Hager A, Wasson JH, Lindblad S. Patient reported outcome measures in practice. BMJ. (2015) 350:1–3. doi: 10.1136/bmj.g7818
7. Saviola F, Pappaianni E, Monti A, Grecucci A, Jovicich J, De Pisapia N. Trait and state anxiety are mapped differently in the human brain. Sci Rep. (2020) 10:1–11. doi: 10.1038/s41598-020-68008-z
8. Steimer T. The biology of fear- and anxiety-related behaviors. Dialogues Clin Neurosci. (2002) 4:231–49. doi: 10.31887/DCNS.2002.4.3/tsteimer
9. Clarke DM, Currie KC. Depression, anxiety and their relationship with chronic diseases: A review of the epidemiology, risk and treatment evidence. Med J Aust. (2009) 190:S54-S60. doi: 10.5694/j.1326-5377.2009.tb02471.x
10. Anyfanti P, Gavriilaki E, Pyrpasopoulou A, Triantafyllou G, Triantafyllou A, Chatzimichailidou S, et al. Depression, anxiety, and quality of life in a large cohort of patients with rheumatic diseases: common, yet undertreated. Clin Rheumatol. (2016) 35:733–9. doi: 10.1007/s10067-014-2677-0
11. Heath J, Lehman E, Saunders EFH, Craig T. Anxiety and depression in adults with primary immunodeficiency: How much do these patients experience and how much do they attribute to their primary immunodeficiency? Allergy Asthma Proc. (2016) 37:409–15. doi: 10.2500/aap.2016.37.3977
12. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. (2016) 39:935–46. doi: 10.1007/s10865-016-9782-2
13. Nowicka-Sauer K, Banaszkiewicz D, Staskiewicz I, Kopczynski P, Hajduk A, Czuszynska Z, et al. Illness perception in Polish patients with chronic diseases: Psychometric properties of the Brief Illness Perception Questionnaire. J Health Psychol. (2016) 21:1739–49. doi: 10.1177/1359105314565826
14. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. (2006) 60:631–7. doi: 10.1016/j.jpsychores.2005.10.020
15. Basu S, Poole J. The brief illness perception questionnaire. Occup Med (Chic Ill). (2016) 66:419–20. doi: 10.1093/occmed/kqv203
16. Luca M, Eccles F, Perez Algorta G, Patti F. Illness perceptions and outcome in multiple sclerosis: A systematic review of the literature. Mult Scler Relat Disord. (2022) 67:104180. doi: 10.1016/j.msard.2022.104180
17. Chilcot J. The importance of illness perception in end-stage renal disease: Associations with psychosocial and clinical outcomes. Semin Dial. (2012) 25:59–64. doi: 10.1111/j.1525-139X.2011.00987.x
18. Breland JY, Wong JJ, McAndrew LM. Are Common Sense Model constructs and self-efficacy simultaneously correlated with self-management behaviors and health outcomes: A systematic review. Heal Psychol Open. (2020) 7(1):1–13. doi: 10.1177/2055102919898846
19. Majkowicz M. Praktyczna ocena efektywności opieki paliatywnej – wybrane techniki badawcze. In: de Walden-Galuszko K, Majkowicz M, editors. Ocena jakości opieki paliatywnej w teorii i praktyce. Medical University of Gdańsk, Gdańsk (2000). p. 21–42.
20. Manusama OR, van Beveren NJM, van Hagen PM, Drexhage HA, Dalm VASH. Psychological symptoms in primary immunodeficiencies: a common comorbidity? J Clin Immunol. (2022) 42:695–8. doi: 10.1007/s10875-022-01207-7
21. Leggett A, Assari S, Burgard S, Zivin K. The effect of sleep disturbance on the association between chronic medical conditions and depressive symptoms over time. Longit Life Course Stud. (2017) 8:138–51. doi: 10.14301/llcs.v8i2.433
22. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep (2013) 36:1059–68. doi: 10.5665/sleep.2810
23. Seidel MG, Kindle G, Gathmann B, Quinti I, Buckland M, van Montfrans J, et al. The European society for immunodeficiencies (ESID) registry working definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract. (2019) 7:1763–70. doi: 10.1016/j.jaip.2019.02.004
24. Stern AF. The hospital anxiety and depression scale. Occup Med. (2014) 64:393–4. doi: 10.1093/occmed/kqu024
25. Evers AW, Kraaimaat FW, van Lankveld W, Jongen PJ, Jacobs JW, Bijlsma JW. Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. J Consult Clin Psychol. (2001) 69:1026–36. doi: 10.1037//0022-006X.69.6.1026
26. Lauwerier E, Crombez G, Van Damme S, Goubert L, Vogelaers D, Evers AWM. The construct validity of the Illness Cognition Questionnaire: The robustness of the three-factor structure across patients with chronic pain and chronic fatigue. Int J Behav Med. (2010) 17:90–6. doi: 10.1007/s12529-009-9059-z
27. Sint Nicolaas SM, Schepers SA, van den Bergh EMM, Evers AWM, Hoogerbrugge PM, Grootenhuis MA, et al. Illness cognitions and family adjustment: psychometric properties of the Illness Cognition Questionnaire for parents of a child with cancer. Support Care Cancer. (2016) 24:529–37. doi: 10.1007/s00520-015-2795-5
28. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
29. Manzar MD, BaHammam AS, Hameed UA, Spence DW, Pandi-Perumal SR, Moscovitch A, et al. Dimensionality of the Pittsburgh Sleep Quality Index: A systematic review. Health Qual Life Outcomes. (2018) 16:9–11. doi: 10.1186/s12955-018-0915-x
30. Hajduk A. Subiektywna jakość snu u chorych na toczeń rumieniowaty układowy. In: Praca doktorska. Gdański Uniwersytet Medyczny, Gdańsk (2015).
31. van Leeuwen NM, Boonstra M, Huizinga TWJ, Kaptein AA, de Vries-Bouwstra JK. Illness perceptions, risk perceptions and worries in patients with early systemic sclerosis: A focus group study. Musculoskeletal Care. (2020) 18:177–86. doi: 10.1002/msc.1453
32. Gerontoukou E-I, Michaelidoy S, Rekleiti M, Saridi M, Souliotis K. Investigation of anxiety and depression in patients with chronic diseases. Heal Psychol Res. (2015) 3. doi: 10.4081/hpr.2015.2123
33. Matcham F, Norton S, Scott DL, Steer S, Hotopf M. Symptoms of depression and anxiety predict treatment response and long-term physical health outcomes in rheumatoid arthritis: Secondary analysis of a randomized controlled trial. Rheumatol (United Kingdom). (2015) 55:268–78. doi: 10.1093/rheumatology/kev306
34. Pedersen JK, Wang L, Risbo N, Pedersen AB, Andersen K, Ellingsen T. Mortality in patients with incident rheumatoid arthritis and depression: A Danish cohort study of 11,071 patients and 55,355 comparators. Rheumatol (Oxford). (2023) kead259. doi: 10.1093/rheumatology/kead259
35. Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: Prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. (2010) 25:1209–21. doi: 10.1002/gps.2463
36. Sowers KL, Gayda-Chelder CA, Galantino ML. Self-reported cognitive impairment in individuals with Primary Immunodeficiency Disease. Brain Behav Immun - Heal. (2020) 9:100170. doi: 10.1016/j.bbih.2020.100170
37. Smith BW, Zautra AJ. The effects of anxiety and depression on weekly pain in women with arthritis. Pain. (2008) 138:354–61. doi: 10.1016/j.pain.2008.01.008
38. Kosson D, Malec-Milewska M, Gałązkowski R, Rzońca P. Analysis of anxiety, depression and aggression in patients attending pain clinics. Int J Environ Res Public Health. (2018) 15:1–10. doi: 10.3390/ijerph15122898
39. Sawyer AT, Harris SL, Koenig HG. Illness perception and high readmission health outcomes. Health Psychology Open. (2019) 6(1):1–11. doi: 10.1177/2055102919844504
40. Nowicka-Sauer K, Hajduk A, Kujawska-Danecka H, Banaszkiewicz D, Czuszyńska Z, Smoleńska Ż, et al. Learned helplessness and its associations with illness perception, depression and anxiety among patients with systemic lupus erythematosus. Fam Med Prim Care Rev. (2017) 19:243–6. doi: 10.5114/fmpcr.2017.69285
41. Rymon Lipińska W, Nowicka-Sauer K. Illness perception and perceived benefits of illness among persons with type 1 diabetes. Heal Psychol Rep. (2023) 11(3):201–12. doi: 10.5114/hpr/153999
42. Lerdal A, Hofoss D, Gay CL, Fagermoen MS. Perception of illness among patients with heart failure is related to their general health independently of their mood and functional capacity. J Patient-Reported Outcomes. (2019) 3:1–7. doi: 10.1186/s41687-019-0142-1
43. Morgan K, Villiers-Tuthill A, Barker M, McGee H. The contribution of illness perception to psychological distress in heart failure patients. BMC Psychol. (2014) 2:1–9. doi: 10.1186/s40359-014-0050-3
44. de Heer EW, Vriezekolk JE, van der Feltz-Cornelis CM. Poor illness perceptions are a risk factor for depressive and anxious symptomatology in fibromyalgia syndrome: A longitudinal cohort study. Front Psychiatry. (2017) 8:217. doi: 10.3389/fpsyt.2017.00217
Keywords: inborn errors of immunity, anxiety, illness perception, depression, sleep quality
Citation: Grochowalska K, Ziętkiewicz M, Nowicka-Sauer K, Topolski M, Więsik-Szewczyk E, Matyja-Bednarczyk A, Napiórkowska-Baran K and Zdrojewski Z (2024) Anxiety in Polish adult patients with inborn errors of immunity: a cross-sectional study. Front. Psychiatry 15:1293935. doi: 10.3389/fpsyt.2024.1293935
Received: 14 September 2023; Accepted: 16 February 2024;
Published: 07 March 2024.
Edited by:
Gaia Sampogna, University of Campania “L. Vanvitelli”, ItalyReviewed by:
Moussa Antoine Chalah, GHU Paris Psychiatrie et Neurosciences, FranceCopyright © 2024 Grochowalska, Ziętkiewicz, Nowicka-Sauer, Topolski, Więsik-Szewczyk, Matyja-Bednarczyk, Napiórkowska-Baran and Zdrojewski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kinga Grochowalska, a2luZ2EuZ3JvY2hvd2Fsc2thOTBAZ3VtZWQuZWR1LnBs
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.