 Julia Fahrer1,2*
Julia Fahrer1,2* Philipp Doebler3
Philipp Doebler3 Klara Hagelweide4
Klara Hagelweide4 Pius Kern1
Pius Kern1 Nora Nonnenmacher5
Nora Nonnenmacher5 Vanessa Seipp2
Vanessa Seipp2 Corinna Reck6
Corinna Reck6 Christina Schwenck2
Christina Schwenck2 Sarah Weigelt4
Sarah Weigelt4 Anna-Lena Zietlow5,7
Anna-Lena Zietlow5,7 Hanna Christiansen1
Hanna Christiansen1- 1Clinical Child- and Adolescent Psychology, Department of Psychology, University of Marburg, Marburg, Germany
- 2Special Needs Educational & Clinical Child and Adolescent Psychology, Department of Psychology, Justus Liebig University Giessen, Gießen, Germany
- 3Department of Statistical Methods in the Social Sciences, Technical University Dortmund, Dortmund, Germany
- 4Department of Vision, Visual Impairments & Blindness, Faculty of Rehabilitation Science, Technical University Dortmund, Dortmund, Germany
- 5Center for Psychosocial Medicine, Heidelberg University Hospital, Institute of Medical Psychology, Heidelberg, Germany
- 6Department of Clinical Child and Adolescent Psychology, Faculty of Psychology, Ludwig-Maximilians-University München, Munich, Germany
- 7Clinical Child- and Adolescent Psychology, Department of Psychology, Technical University Dresden, Dresden, Germany
Studies using observational measures often fail to meet statistical standards for both reliability and validity. The present study examined the psychometric properties of the Coding Interactive Behavior (CIB) System within a German sample of parent–child dyads. The sample consisted of 149 parents with and without a mental illness and their children [n experimental group (EG) = 75, n control group (CG) = 74] who participated in the larger Children of Mentally Ill Parents at Risk Evaluation (COMPARE) study. The age of the children ranged from 3 to 12 years (M = 7.99, SD = 2.5). Exploratory factor analysis supported a five-factor model of the CIB with items describing 1) parental sensitivity/reciprocity, 2) parental intrusiveness, 3) child withdrawal, 4) child involvement, and 5) parent limit setting/child compliance. Compared to international samples, the model was reduced by two independent dyadic factors. Testing for predictive validity identified seven items with predictive power to differentiate parental group membership. The CIB factors did not seem to be sufficiently sensitive to illustrate differences in interaction within a sample of parents with various mental illnesses. To apply the CIB to the described sample or similar ones in the future, additional measurement instruments may be necessary.
1 Introduction
Interactive behaviors are the central communication between parents and their children from birth onward (1). Visual contact, a friendly smile, or an affectionate touch from the parent usually builds a child’s first social experiences. The Coding Interactive Behavior (CIB) is a widely used tool for measuring parental, child, and dyadic interactive behavior (2). Especially in infancy and early childhood, children depend on their parents’ intuitive ability to recognize their behavioral signals and to respond to them promptly and appropriately (3–5). Therefore, the interactive behavior of parents with their children is of paramount importance for the development of the child (6). The content of the interaction must be adapted to the child’s cognitive, motor, and socioemotional developmental stages (1). Repeatedly, experienced parental behaviors are internalized by the child and contribute to the child’s perception of safety, empathy, emotion regulation, and moral development (1, 7). Parental interactive style within interactions is stable over time and should be foreseeable for the child (Feldman, 2010 (8)).
Parental sensitivity is a widely used construct to measure parental responsiveness to infant needs (9, 10) and is the core concept within the environment that promotes an infant’s attachment security (11). It consists of supportive parental behaviors such as parental receptivity, responsiveness, contingent reactions, and age-adapted stimulation, involvement, and communication to children’s signals and appears to be a core parental behavioral factor for both infant and child development (8, 12).
As children become more active in their interactions with their parents, dyadic reciprocity becomes an important behavioral expression alongside parental sensitivity. Dyadic reciprocity describes an interactive coordination of gaze, affect, vocalization, and touch of both partners within the interaction. The mutual regulation of affect in reciprocal interaction is necessary for the development of a child’s regulatory skills (13). In later childhood, the content of the dyadic interaction shifts from play to verbal dialogue.
Parental behavior is influenced by the respective culture of the interactive partners and their temperament and may be affected by possible parental illness, especially mental disorders (1). Sensitive maternal behavior toward offspring, whether infants, children, or adolescents, predicts socioemotional development, adaption (14, 15), and cognitive development (14, 16). A high amount of maternal warmth, low levels of punishing disciplinary actions, appropriate limit setting, and dyadic reciprocity within the interaction are associated with improved child self-regulation (17, 18) and resilience (13).
Given the central role of parent–child interactions in child development, it is clear that contextual factors such as cultural influences and parental mental health play an important role in shaping these interactions. Recognizing this, our study seeks to account for these influences by examining the psychometric properties of the CIB tool, thereby enhancing our understanding of parent–child interactions across contexts and ensuring the robustness of our research findings.
2 Background
2.1 Parent–child interaction in the context of parental mental illness
Parental interactive behavior can be impaired when a parent has a mental illness and may appear different from that of parents without a mental illness. The model of the transgenerational transmission of mental disorders (TTMDs) identifies parental hostility, rejection, low involvement, abuse, neglect, and lack of sensitivity as well as reduced child responsiveness and imitation as potential mechanisms of disorder transmission under the broad category of parent–child interaction (19, 20). A meta-analysis by Rodrigues et al. (21) points out that low parental sensitivity and child behavior problems are mutually reinforcing, with a stronger effect in older children. The parental ability to recognize the child’s behavioral signals and to respond promptly and adequately can be impaired by experiences of violence, abuse (22, 23), war (24), and different parental mental illnesses (25–29).
For instance, mothers with depression show more disengagement, are less responsive to their offspring’s distress and social signals, talk less with their children, tend to avoid eye contact, and are more easily irritated (30, 31). They also provide less affectionate touch, need more time to react to shifts in the child’s behavior, have difficulty in determining an appropriate level of stimulation for the child, and prevail less reciprocity in the interaction (30, 31). For parents with an anxiety disorder, findings appear to be more heterogeneous regarding low parental sensitivity due to methodological issues in primary studies (e.g., different anxiety disorders, no clinical interviews, and different paradigms) (29, 32, 33). Parents with anxiety disorders show increased controlling behavior and intrusiveness, and interactions appear to be driven by the parent’s agenda and plans rather than the child’s. In addition, it appears that parents with anxiety disorders have difficulty estimating the adequate intensity of the interaction, tend to overstimulate their children, and thus disregard the child’s signals (1, 30). Mothers with schizophrenia show less sensitivity, increased intrusive behaviors, more self-centeredness, and withdrawal behavior, and their behavior appears to be even more impaired than that of mothers with bipolar disorder or depression (34). Mothers with post-traumatic stress disorder (PTSD) show less supportive behavior and sensitivity and have difficulty recognizing their child’s affective state and behavior. They respond inadequately, and, as a result, their children show more withdrawing behavior (24, 35, 36).
The stated findings offer a brief overview of the many existing studies on parental, especially maternal, interactive behavior, predominantly using the Coding Interactive Behavior when a parent has a mental illness. While most studies focus on maternal mental illness in early childhood, little is known about its effect across the age span of middle childhood (37). A recent meta-analysis of parent–child interactions (38) reported that the mean age of the children was 44 months, and 94% of the primary studies assessed maternal interactive behavior. Cross-lagged analyses show that sensitivity plays an important role in middle childhood and adolescence as well (12). Both mothers and fathers are primary caregivers within a family, but parent–child interactions have been studied primarily in mother–child dyads (39). Moreover, most studies examining the impact of parental mental illness look at one specific disorder rather than various mental illnesses. This raises the question of whether a specific parental mental illness exhibits a unique behavioral profile or whether parents with a mental illness present a similar clinical picture across diagnostic categories and in contrast to parents without a mental illness. Parental interactive behavior appears to be of great importance for child development and is influenced by parental mental illness. The composition of constructs describing interactive behavior is also influenced by culture.
2.2 Parent–child interaction and cultural sensitivity
Every culture has its own set of shared values, norms, beliefs, and behaviors that are considered normative in one culture or society, but not necessarily in another. Cultural beliefs and specific behaviors appear to be stable over time and are communicated to new members of a culture. This accounts for parenting behavior as well, as it maintains cultural conceptions (40). Parental behavior has a direct impact on infant behavior through repeated exchanges and interpersonal relatedness of experiences (30). During the postpartum period, parental behavior appears to be more similar across societies but becomes more diverse and culturally sensitive as children grow up (1). Cultural norms and attitudes shape a parent’s behavior to be consistent with overarching cultural goals and values (41).
For instance, European and American mothers use more suggestions than commands to structure their child’s behavior, in contrast to Puerto Rican mothers who use more immediate cues such as commands, physical manipulation, positioning, and restrictions to attract and draw their child’s attention and guide their play (42). German parents are often characterized by a more distal parental style (43). Verbal communication and focused attention are more prevalent than physical contact. German parents encourage their child’s curiosity and creativity to promote autonomy, independence, and cognitive competencies (44) and perceive their child as an equal interactive partner (45). Furthermore, physical manipulation of children is an indicator of relationship disturbances in Western societies when observed in mother–child interactions with children older than 1 year. However, it can also be observed in father–child interactions and is considered normal because it is categorized as “rough-and-tumble” play that promotes the father–child bond (1, 46, 47). In summary, there are cultural and gender differences in the occurrence of parental behaviors in interactions. In addition, there appears to be a need for an objectifiable tool to classify behavior as well as a valid, comprehensive measurement model.
2.3 The Coding Interactive Behavior system
The CIB is an observable, macro-analytic measure of parent–child interactive behavior. The CIB is a global coding scheme for “free-play” interactions in dyads that takes into account the behavior of both interacting partners. The CIB uses developmental goal-adapted paradigms, such as free play for infants and preschoolers or a joint discussion of a pre-defined topic (e.g., planning a fun day together) at school-aged children, to assess human behavior. Depending on the age of the child, it comprises up to 42 items (Appendix A), of which 21 address the parent’s behavior, 16 assess the child’s behavior, five are dyadic codes, and two are additional overall codes (44 in total). Behaviors are rated on 9-point Likert-type scales, where 5 is a strong expression of behavior and 1 is a weak expression (2). The CIB codes are comprised of eight factors, sometimes called composites: parental sensitivity, intrusiveness, and limit setting; child engagement–involvement, withdrawal, and compliance; dyadic reciprocity; and negative states. Further, the CIB contains items that are central to a construct and other items that are part of a construct in some cultures but not in others or at certain stages of development. Parental acknowledgment is an important component of the parental sensitivity construct across ages and cultures, whereas parental affectionate touch is an essential component of the sensitivity construct in some cultures (1, 2). The interrater reliability of the CIB appears to be substantial (48), and the internal consistency of the different composites ranges between adequate and good (α = 0.72–0.95) in different samples (1, 2, 6, 48).
The CIB is a widely used tool, including samples of premature infants and their mothers (49), clinically referred infants (50), parents with a mental illness (51), and biological and socioemotional risk factors (6, 52). The CIB has been used in Western societies, such as Israel (53), Germany (23, 29), France (54), and Denmark (55), and in non-Western societies, including Palestinian families in Ramallah and the West Bank (41); the CIB appears to be sensitive toward cultural variation (53).
The psychometric properties are reported in several studies stating measures of reliability (6, 48, 56), but information on factorial validity is often lacking (57). In line with Steenhoff et al. (55), we were not able to identify any validation of the CIB within a sample of fathers, with the exception of the study conducted by the respective authors (55, 57). The postulated factor structure has only been validated and verified in a French sample of newborns and their mothers (54) and for the three parental factors within a well-resourced Danish sample of 5-year-olds and their parents without mental illness (55). The Danish study was able to identify the three parental factors for mothers and five paternal factors based on a reduced set of items. To our knowledge, there has been no independent validation and verification of either the measurement model or the factorial structure of the CIB in addition to the two studies mentioned. As the paper by Viaux-Savelon et al. (54) focused on newborns and the paper by Steenhoff et al. (55) on 5-year-olds, a validation of the factorial structure within a sample of German mothers and fathers with and without mental disorders and their children across a broader age range is lacking. Moreover, the former paper (55) only reported Cronbach’s alpha, missing further measures to assert the factorial structure.
2.4 Aims
In order to analyze group differences between parents with and without a mental illness, it is important to assess whether the theoretically formulated constructs can be identified within the present sample. Further, it is important to assess how the constructs are composed depending on the specific culture and the age range of the children. Finally, comparing the interactive behavior of parents with different mental illnesses to healthy controls is an important step in understanding the impact of mental illness on parenting behavior and child outcomes and in developing interventions to support families affected by mental illness.
This study is the first to examine the psychometric properties of the CIB within a sample of German parents with different mental disorders as well as healthy control parents and their children aged 3 to 12 years. Specifically, the aims were to investigate a) the item properties and b) the construct validity, with an emphasis on exploring the dimensional structure of the postulated composites. In this regard, exploratory factor analysis was conducted to investigate whether the latent factor structures of parents replicated the postulated CIB parenting constructs. Further, we aimed to investigate c) the reliability and d) the interrater reliability of the instrument. The present study aims to provide the psychometric properties to enable further substantive analysis.
3 Method
The Children of Mentally Ill Parents at Risk Evaluation (COMPARE)-family study is a prospective multicenter, confirmatory, randomized controlled phase III trial with two parallel arms (58), funded by the German Federal Ministry of Education and Research (BMBF), providing cognitive behavioral therapy for parents with a mental illness. For more information, see Stracke et al. (58), Christiansen et al. (19), and Zietlow et al. (59). The present COMPARE-interaction study within the COMPARE-family project is a subproject of the larger COMPARE-interaction (59) and COMPARE-family projects (19).
3.1 Participants
The participants in the interaction study consisted of a subsample of parent–child dyads recruited for the larger COMPARE-family study (19, 58) and a control group (CG) without mental illness. Families met the inclusion criteria for the interaction study if a) parent and child agreed to participate in a videotaped, semi-structured play paradigm; b) children were between the ages of 3 and 12; c) families had sufficient knowledge of the German language; and d) parents were seeking treatment and met diagnostic criteria for a mental disorder according to DSM-5 and children did not have a mental disorder requiring urgent treatment to meet the inclusion criteria for the experimental group (EG). If the families who participated in the COMPARE-family study did not provide their consent to be videotaped, they were not able to participate in the interaction study. To meet the inclusion criteria for the CG, both parent and child were required not to present with any mental illness, and parents were required to report that they had never been treated for or diagnosed with a mental illness. Participants were assessed between 2018 and 2021 at Philipps University Marburg, Justus Liebig University Giessen, and Technical University Dortmund.
Data were collected on 75 children and 60 parents in the EG and 74 children and 59 parents in the CG. An overview of the sociodemographic characteristics is provided in Table 1. In the EG, 46 parents participated with one child, 13 with two children, and one parent with three children. In the CG, 48 parents participated with one child, seven parents with two children, and four parents with three children.
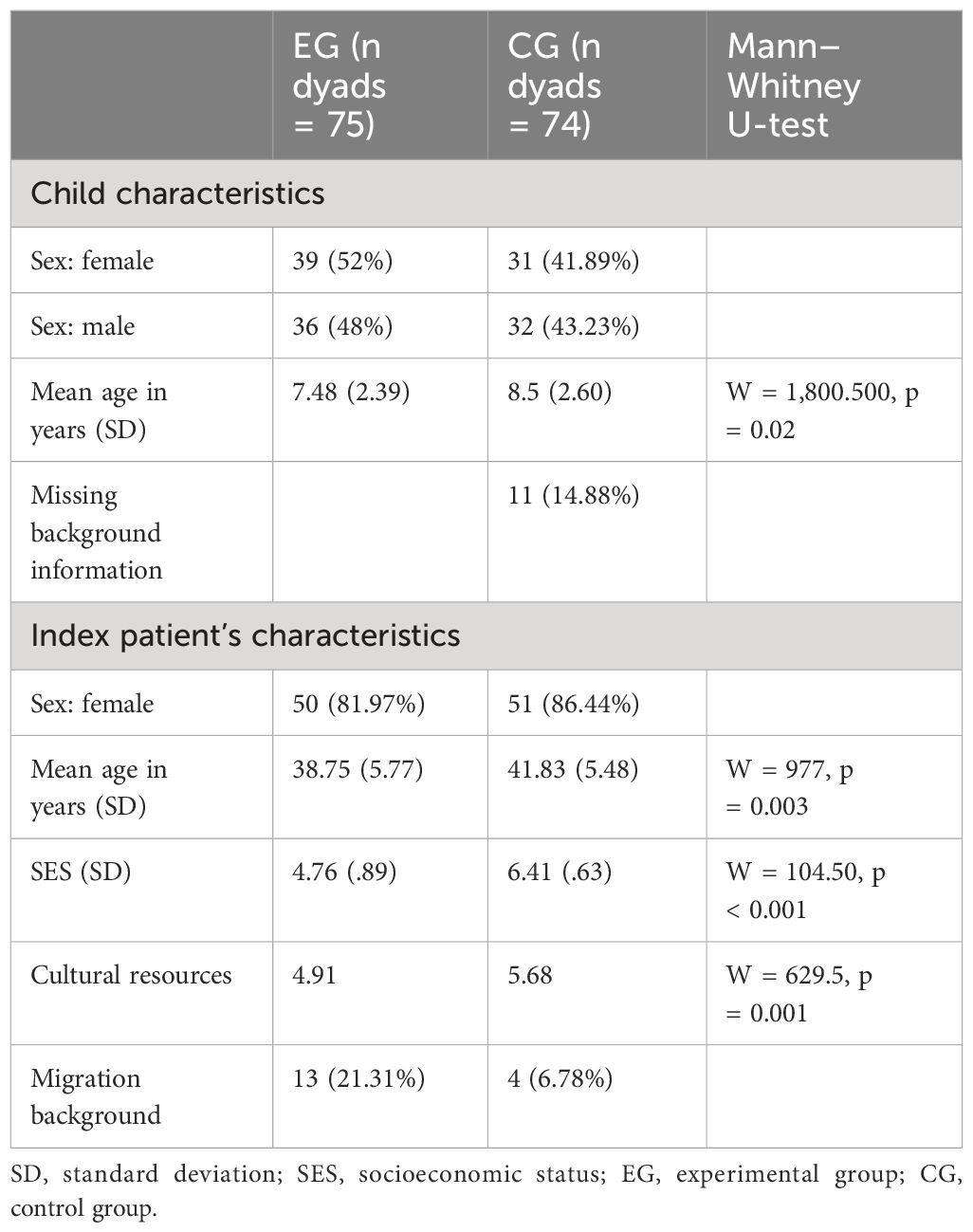
Table 1 Demographics of EG and CG.
The Shapiro–Wilk test was carried out to control for the distribution of demographic variables (60), and the Mann–Whitney test was used to control for group comparability regarding background characteristics and symptom severity (61). Furthermore, the socioeconomic status (SES) of children of parents with a mental illness was lower than that of controls (W = 104.50, p < 0.001). However, when looking at representative data of children and adolescents in Germany, the SES of both groups can be classified as low (62). To assess the SES of both groups, occupational status and net household income were converted into numbers between 1 and 7 according to the scales used in the second wave of the KiGGS study (62), and the mean of both values was calculated. Families with a migrant background were underrepresented in the study in both the EG and the CG (63). Children in the EG showed higher scores on the internalizing subscale of the Child Behavior Checklist (CBCL), and parents in the EG showed higher Brief Symptom Inventory–Global Severity Index (BSI–GSI) scores (see Table 2 for an overview of parent and child group differences). Participation in the study was voluntary for both groups, with families in the CG receiving a financial incentive. Families in the EG received gold standard CBT treatment according to the COMPARE-family protocol (58). Additional information on parental diagnosis is provided in the Appendix.
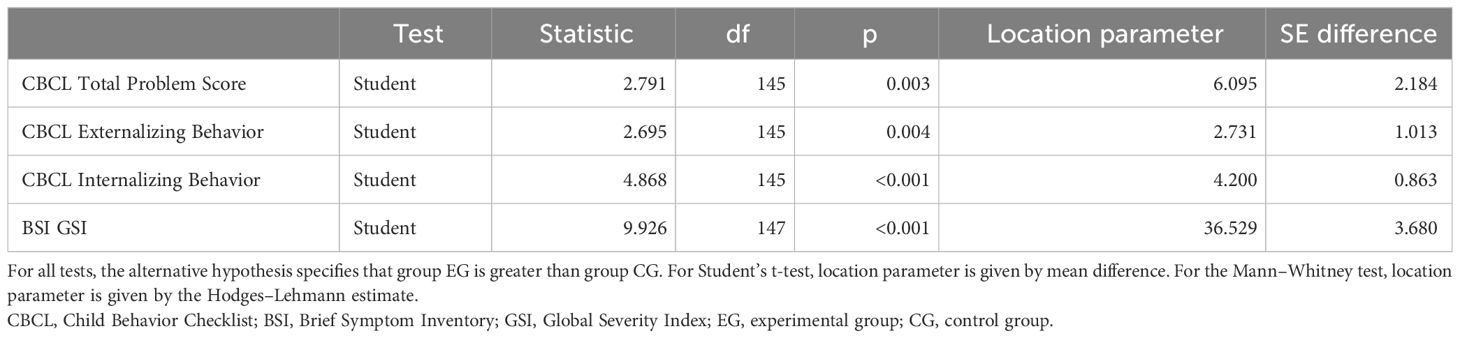
Table 2 Independent samples t-test of CBCL and BSI.
3.2 Measure
In the EG, parental diagnosis as well as potential child disorders were assessed using the Diagnostic Interview of Mental Disorders for parents and children (DIPS and Kinder-DIPS) (62, 64) and the Structured Interview for Preschool Ages (SIVA) (65) for children under the age of 6. In both the EG and the CG, parental psychopathology was assessed using the BSI (66), and child psychopathology was assessed using the German version of the CBCL-parent version (67). Due to the comparability of the groups, only BSI and CBCL scores are reported in the present article.
3.2.1 Child Behavior Checklist
The CBCL/6-18 (parent report) (68) was used to describe internalizing and externalizing behaviors in children age 6 years and older. The CBCL/11/2-5 (parent report) (69) was used to characterize internalizing and externalizing behaviors in children under 6 years of age. The standardized behavior scales quantify children’s and adolescents’ emotional and behavioral difficulties over the past 6 months. The CBCL/6-18 comprises 118 items, and the CBCL/11/2-5 comprises 99 items, each rated on a 3-point Likert-type scale ranging from 0 (never or not true) to 2 (often or very true). Items referring to rule-breaking and aggressive behavior were aggregated into an externalizing subscale. Items describing anxious/depressed, withdrawn/depressed, and somatic components were aggregated into an internalizing subscale. The CBCL has shown high test–retest reliability, criterion, and construct validity (70, 71). In the present study, the internal consistency of the total scale was α = 0.75.
3.2.2 The Brief Symptom Inventory
The BSI (66) is a self-report questionnaire for adolescents and adults that assesses the subjective impairment concerning somatic and psychological symptoms (66). It comprises 53 items, rated on 5-point Likert-type scales ranging from 0 (not at all) to 4 (very much). The items refer to nine primary symptom scales and three global indices that depict the global burden, such as the GSI. The internal consistency of the total scales for our sample was α = 0.91.
3.2.3 The Coding Interactive Behavior
The CIB is a global coding scheme for the analysis of behavior observations of dyads (2). The CIB enables the rating of specific behaviors and affective states of each interaction partner within a dyad, as well as an overall dyadic impression (2). The CIB appears to be sensitive to cultural variation (53), parental mental illness (51), biological and socioemotional risk factors (6, 52), and the effects of interventions (48, 72). The CIB is used from the newborn stage to adolescence with adapted coding manuals for the different age groups, providing manuals for newborns (2–36 months), preschoolers (3–6 years), school-aged children (6–12 years), and adolescents (2). The CIB is a 44-item global coding scheme that provides eight theoretically derived composites (48, 52, 53, 73–76), of which three composite scores with 22 items depict parental behaviors and affective states: Parent Sensitivity, Parent Intrusiveness, and Parent Limit Setting. Another three composites of 16 items are child-related: Child Social Involvement, Withdrawal, and Compliance to Parent. Two additional composites of five items refer to the dyadic behaviors and states: Dyadic Reciprocity and Dyadic Negative States (1, 2). Feldman (1) reported a sufficient model fit for the composites Parent Sensitivity, Parent Intrusiveness, Child Social Involvement, and Child Negative Affect [χ2 = 56.12, p = 0.18, goodness-of-fit index (GFI) = 0.94, adjusted goodness-of-fit index (AGFI) = 0.93, normed fit index (NFI) = 0.92, root mean square error of approximation (RMSEA) = 0.03].
3.3 Procedure
This study was approved by the Ethical Committees of Philipps University Marburg, Justus Liebig University Giessen, and Technical University Dortmund, Germany. The recruitment for the EG consisted of electronic and paper flyers as well as posters that were distributed in clinics and private practices, mental health hospitals, schools, bus commercials, topic-related readings, and Facebook. Furthermore, the research team contacted almost every local youth care institution that supports families and children in order to raise awareness of the project and to request that information about the project be forwarded to suitable families. The families in the CG were recruited as a convenience sample with electronic and paper flyers as well as posters that were distributed at schools, flea markets, and private practices and on Facebook.
All participating parents and children of school age gave their written informed consent prior to or on the date of the assessment. In the case of shared child custody, both parents provided written informed consent. Parents completed the CBCL and BSI questionnaires online. Parent–child interaction observations were carried out and videotaped by graduate students and undergraduate assistants at the respective universities in laboratory settings. The semi-structured play paradigm invited the parents to spend time together with their children as they usually do. Therefore, a set of several toys for free play situations was provided. Videos were pseudonymized afterward and exchanged between reliable raters to ensure the blindness of the raters toward group allocation and parental diagnosis. A subset of 21 videos was blindly coded by all reliable raters enrolled in a Ph.D. or postdoctoral program.
3.4 Data analysis
3.4.1 Item properties
Data from 149 dyads were used for the analysis of the item properties. The means and standard deviation of every item of the CIB were assessed. Table 3 shows all items as they are traditionally assigned to the original factors according to Feldman’s model (training provided by Ruth Feldman in 2020). For the items child Fatigue and Parent Depressed Mood, this was performed in their original form as well as after reversing them as suggested in the training provided by the research group of Feldman. In order to investigate how well the items differentiate between individuals in our sample, their discriminatory power was analyzed.
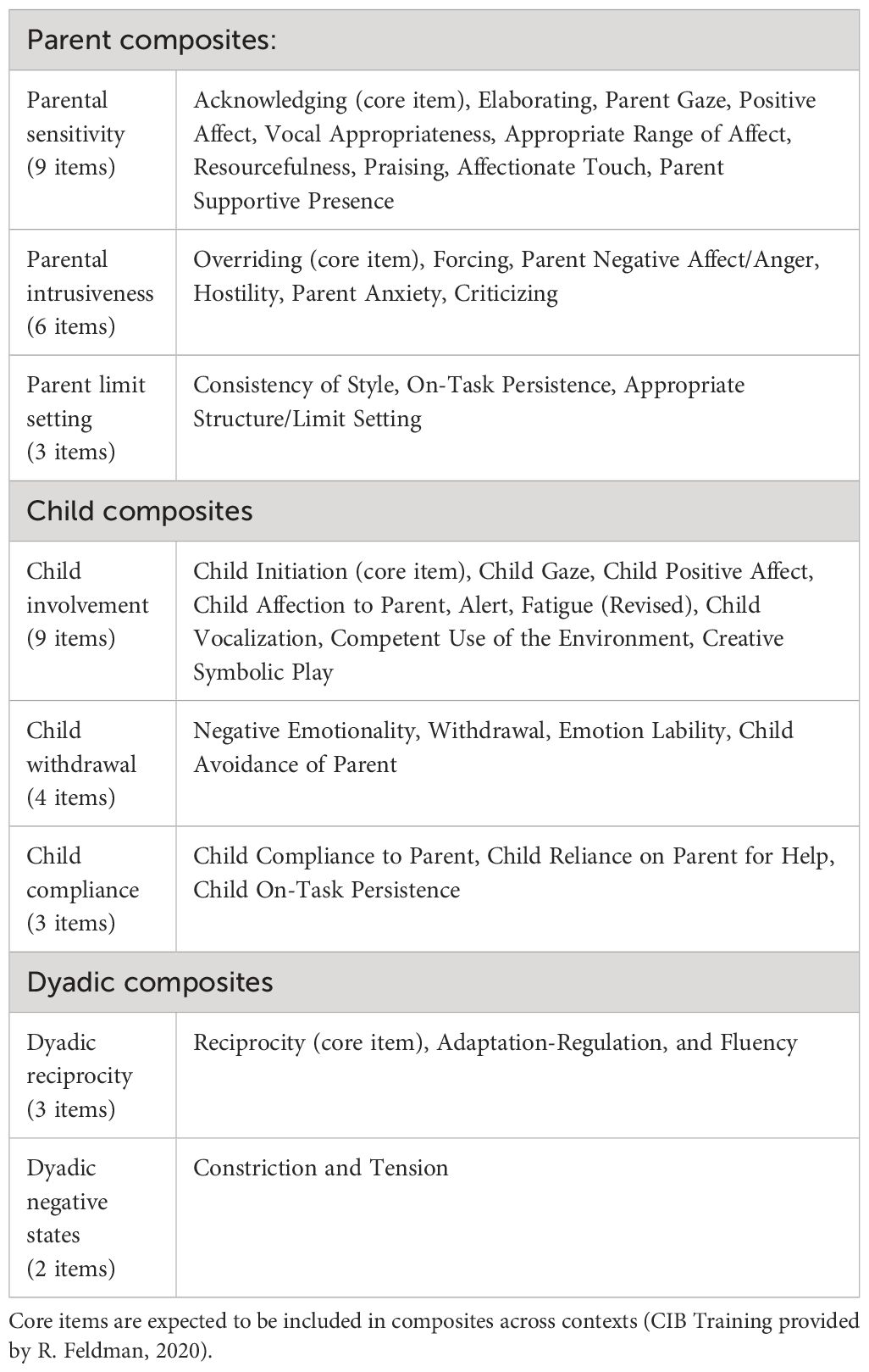
Table 3 Original theoretical model.
The item discrimination and reliability were reported based on our newly specified model. The item child Fatigue was inverted as suggested by the research group of Ruth Feldman within the training they provided in 2020. Regarding the item properties, an item difficulty of Pi of between 5 and 95 appears to be achievable if one aims to depict the whole spectrum of characteristic features and even wants to differentiate between persons with extreme expressions of characteristic values. Furthermore, discriminatory power >0.4 to 0.7 was considered good (77).
3.4.2 Construct validity
In the current study, we conducted an exploratory factor analysis (EFA) with the whole sample consisting of both the CG and EG.
3.4.2.1 Model adaption
We performed an EFA (78) using the R software package EFAtools [version 0.3.1 (79)]. The minimum and maximum number of factors to be extracted must be specified. We based this decision on a scree test (80) and a parallel analysis (81). In line with Preacher and MacCallum (82), we considered factor loadings smaller than 0.30 to be too small to be relevant and dropped them from further analysis. Therefore values .3 and above are displayed in bold letters. We assumed that the identified factors would correlate, as composites have been found to correlate in previous research (8). We decided to start with an EFA, as this is the first study examining the dimensional structure of the CIB within a sample of parents with various mental illnesses as well as including the item Parent Depressed Mood, and we aimed to explore the data without making any prior assumptions. We performed the EFA with the total sample of 149 dyads using oblimin, promax, and bifactor rotations and a minimal residual resolution (minres) using principal axis factoring (PAF) to calculate the model fit.
An EFA can provide evidence of whether current CIB practice mostly based on samples of dyads with infants from diverse cultural backgrounds is justified in a sample of preschool and school-age German-speaking children–parent dyads. Further, it can especially help to approach the question of dimensionality. By using several rotations, we can sketch avenues for further work on an appropriate measurement model, which would need to be based on a larger sample. For applications with relatively pure scores for subscales, we employed promax, oblimin, and bifactor (83).
3.4.3 Predictive validity
Since the CIB items have repeatedly been demonstrated to be indicative of group differences, especially in the context of mental health, item scores and EFA factor scores were validated based on the CG and the EG. Two different methods were employed: (1) three multivariate analyses of variance (MANOVAs), each with the factor group (CG vs. EG) based on the factor scores of oblimin, promax, and oblique bifactor. The scores were deemed predictive if the MANOVAs were significant, indicating some latent mean group differences. For an appropriate test procedure, Friedrich and Pauly’s (84) MANOVA for heteroscedastic data was used. (2) A logistic regression with a (relaxed) least absolute shrinkage and selection operator (LASSO) was used to predict group membership. All factor scores and all item scores were used. Tuning of the LASSO was by 10-fold cross-validation. Based on a recent critical review of labeling conventions of area under the curve (AUC) values by de Hond et al. (85), the AUC was interpreted.
3.4.4 Reliability
Cronbach’s alpha was used to calculate the internal consistency of the different composites presented in the factor analysis. A minimum value of 0.80 was considered good. Nevertheless, the number of items included was taken into account when interpreting the alpha coefficient (86).
3.4.5 Interrater reliability
Reliable raters were trained to code with a substantial agreement of at least 80%. In order to achieve this, training was first provided by the research group of Ruth Feldman, and in a next step within the group of raters. A subset of 27 videos out of the 149 parent–child interactions was chosen for reliability training, with the aim of covering all age groups present in the study, as the initial training predominantly covered children of newborn and infant age. Videos were individually coded by each rater, and discrepancies in the ratings were solved through discussion to achieve a deep, shared understanding of the postulated items within the research group.
To calculate interrater agreement, a subset of 20% of the videos was randomly chosen and coded by four raters at the different study centers. The intraclass correlation coefficient (ICC) was calculated using a one-way random-effects model for multiple raters, and the average of k ratings was selected for absolute agreement (87) using the R psych software package [version 2.1.3 (88)]. Absolute agreement for the items Compliance to Parent, Reliance on Parent for Help, Child Fatigue Recoded, Alert, Parent Anxiety, and Parent Appropriate Range of Affect was moderate (0.50–0.75). The ICC for all remaining 38 items was good (0.75–0.90) to excellent (>0.90).
4 Results
4.1 Item properties
First, the analysis of the item properties was performed based on the model suggested by Feldman and her research group. However, the EFA of the CIB scales revealed a different five-factor structure. Therefore, the analyses were re-run using this revised model. The report of the results regarding item properties was restricted to these second analyses.
4.1.1 Parental scales
The item difficulty of all parental items ranged from Pi = 20.13 (Forcing) to Pi = 92.62 (Consistency of Style and Parental Depression Recoded). Only the Parent Anxiety item achieved an item difficulty greater than Pi = 95 and was therefore excluded from further analysis.
The means of the items of the postulated Sensitivity scale ranged from M = 1.18 (SD = 0.5; Affectionate Touch) to M = 4.37 (SD = 0.68; Parent Gaze), with a possible maximum of 5. The discriminatory powers ranged from rit(i) = −0.02 (Affectionate Touch) to rit(i) = 0.68 (Elaborating and Acknowledging). The discriminatory power of all items was considered good (>0.40), except for the items Praising and Affectionate Touch, which were considered poor (<0.20).
The means of the items on the postulated Intrusiveness scale ranged from M = 1.01 (SD = 0.06; Forcing) to M = 1.63 (SD = 0.83; Overriding), with a possible minimum of 1 and maximum of 5.0. The discriminatory powers ranged from rit(i) = 0.0 (Forcing) to rit(i) = 0.98 (Overriding). The items Parent Negative Affect and Hostility showed weak discriminatory power (<0.40), and the items Forcing and Parent Anxiety even displayed poor discriminatory power close to 0. The remaining items of the Intrusiveness Scale showed good discriminatory power.
The means of the items on the postulated Limit Setting scale ranged from M = 4.61 (SD = 0.7; Appropriate Structure) to M = 4.63 (SD = 0.61; Consistency of Style), with a possible maximum of 5.0. The discriminatory powers ranged from rit(i) = 0.34 (Parent On-Task Persistence) to rit(i) = 0.64 (Parent Appropriate Structure). The discriminatory power was weak (<0.40) for one item (Parent On-Task Persistence) and good for the remaining items.
4.1.2 Child scales
The item difficulty of all child items ranged from Pi = 22.55 (Child negative affect and Withdrawal) to Pi = 94.77 (Child Gaze). Only the item Fatigue Recoded achieved an item difficulty above Pi = 95 (p = 98.46) and was therefore excluded from further analysis.
Means of the items of the postulated Child Involvement Scale ranged from M = 2.16 (SD = 1.38; Creative–Symbolic Play) to M = 4.28 (SD = 0.68; Competent Use of the Environment), excluding Fatigue M = 1.08 (SD = 0.3) and Fatigue Recoded M = 4.92 (SD = 0.3). The discriminatory powers ranged from rit(i) = 0.47 (Child Gaze) to rit(i) = 0.73 (Child Positive Affect). The discriminatory power was good, except for the item Fatigue Recoded, which showed weak discriminative power rit(i) = 0.16.
The means of the items of the postulated Withdrawal Scale ranged from M = 1.09 (SD = 0.29; Avoidance of Parent) to M = 1.14 (SD = 0.34; Withdrawal). The item difficulty and discriminatory powers ranged from Pi = 1.08, rit(i) = 0.07 (Avoidance of Parent) to Pi = 1.14, rit(i) = 0.27 (Withdrawal). All items on the scale showed weak discrimination.
Means of the items of the postulated Compliance to Parent scale ranged from M = 1.69 (SD = 0.82; Reliance on Parent for Help) to M = 4.72 (SD = 0.48; On-Task Persistence). The discriminatory powers ranged from weak rit(i) = 0.01 (Reliance on Parent for Help) to good rit(i) = 0.63 (Compliance to Parent).
4.1.3 Dyadic scales
Item difficulty of all dyadic items was within the spectrum of 5 ≤ Pi ≤ 20, e.g., 80 ≤ 95.
Means of the items of the postulated Dyadic Reciprocity scale ranged from M = 3.84 (SD = 0.86; Dyadic Reciprocity) to M = 3.94 (SD = 0.74; Adaptation-Regulation). The discriminatory powers ranged from rit(i) = 0.65 (Adaptation-Regulation) to rit(i) = 0.79 (Fluency).
Means of the items of the postulated Dyadic Negative States scale ranged from M = 1.19 (SD = 0.43; Tension) to M = 1.61 (SD = 0.75; Constriction). The discriminatory powers ranged from rit(i) = −0.43 (Tension) to rit(i) = −0.71 (Constriction).
4.2 Construct validity
4.2.1 Preliminary analysis
The data for the assumption of univariate and multivariate normality were tested with respect to skewness and kurtosis. For skewness and kurtosis, the items Parent Depressed Mood and Child Fatigue were imputed in their original form, as recoded items would only result in reversed skewness values. Overall, 26 out of 44 items showed values of skewness greater than I1I, and 23 items showed kurtosis greater than I1I. For all 26 items, skewness was significant, and 23 items showed significant kurtosis.
4.2.2 EFA
Bartlett’s test of sphericity, which tests the significance of the item correlations within a correlation matrix, resulted in χ2 (721) = 4,119.98, p < 0.00, indicating that factor analysis appears appropriate (89). The Kaiser–Meyer–Olkin (KMO) test revealed an overall KMO = 0.87 and was therefore considered meritorious, indicating that the strength of the relationship between the items was high (90). The KMO for the items Praising, Affectionate Touch, On-Task Persistence, Criticizing, child Persistence, and Creative Play were below 0.5. Therefore, they were excluded from further analysis. The empirical Kaiser–Guttman criterion (KGC) suggested the extraction of five factors. The scree plot revealed five eigenvalues before the substantial drop. In the parallel analysis, there were six eigenvalues before the point of intersection of the present data with the data line simulated from random data. However, the sixth eigenvalue was very close to the randomly generated plot. The Velicer MAP test (91, 92) achieved a minimum of 0.02 with six factors, and the empirical Bayesian information criterion (BIC) achieved a minimum of −2,330.4 with five factors when using promax, oblimin, or bifactor rotation. Based on these results, the goodness-of-fit indices of a one-factor baseline model and a five-factor model were compared with the reduced item pool as proposed in the KMO analysis (Table 4) (93, 94).

Table 4 Model fit exploratory factor analysis (minres PAF estimator).
A model fit is considered to be good if χ2/df ≤ 2 or as acceptable if χ2/df ≤ 3 (95). The inspection of the fit indices of the different EFA models indicated that the reduced five-factor solution when removing the items Parent Anxiety, Praising, Affectionate Touch, child Fatigue Recoded, and Reliance on Parent for Help represented the data the best and resulted in a good model fit of χ2/df = 1.88, Tucker–Lewis index (TLI) = 0.80 appeared mediocre (TLI ≥ 0.8), and RMSEA = 0.08 appeared to be acceptable (RMSEA ≤ 0.08). It was decided to continue with the reduced five-factor model. Table 5 shows the factor loadings of the generated model using promax rotation. Please compare the Appendix for the EFA using oblimin and bifactor rotations.
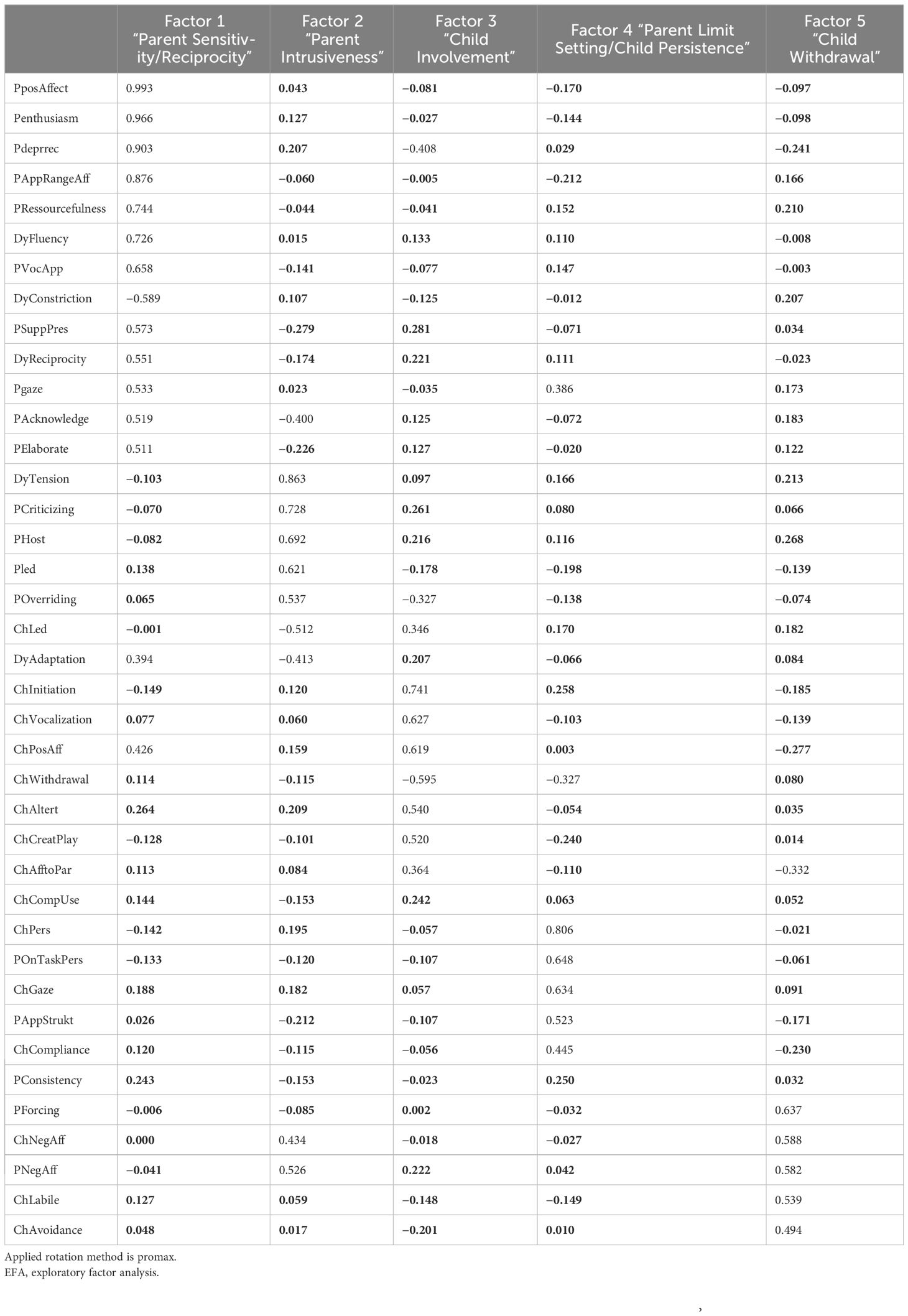
Table 5 Factor loadings on the 5-factor EFA model (promax) (n = 149).
In contrast to Feldman’s postulated eight-factor model, our EFA revealed a five-factor model. We identified factors related to traditional factors such as Parental Sensitivity/Reciprocity, Parental Intrusiveness, Child Involvement, Parent Limit Setting/Child Compliance, and Child Withdrawal, as shown in Table 5. However, the EFA model did not identify separate factors associated with the individual for parental, child, and dyadic behaviors. Within the EFA using bifactor rotation, we were able to identify a main factor. This was related to parental sensitivity, dyadic reciprocity, and child involvement. The other four factors were Parent Sensitivity, Parent Intrusiveness, Child Withdrawal, and Parent Limit Setting/Child Compliance (see Appendix).
In this study, we conducted EFA using promax, oblimin, and bifactor rotations to explore the underlying structure of the observed variables. Factors related to Parental Sensitivity/Reciprocity, Parental Intrusiveness, Child Involvement, Parent Limit Setting/Child Compliance, and Child Withdrawal were identified in both analyses (see Table 6). The Appendix presents the factor loadings, the proportion of variance explained, and factor correlations obtained from the oblimin rotation.
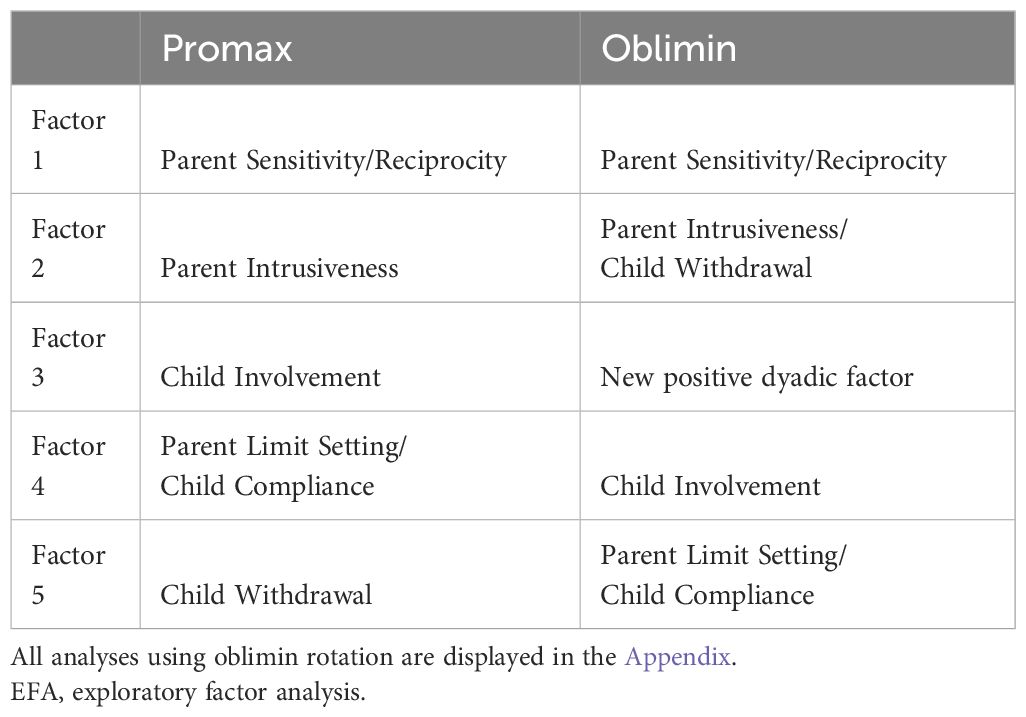
Table 6 Factors identified using different rotations for EFA.
The results of the rotated factor solution using promax rotation provide important insights into the underlying structure of the variables under consideration (Table 7). The proportion of variance explained by each factor provides valuable information about the relative importance of these factors in explaining the variability in the observed data.
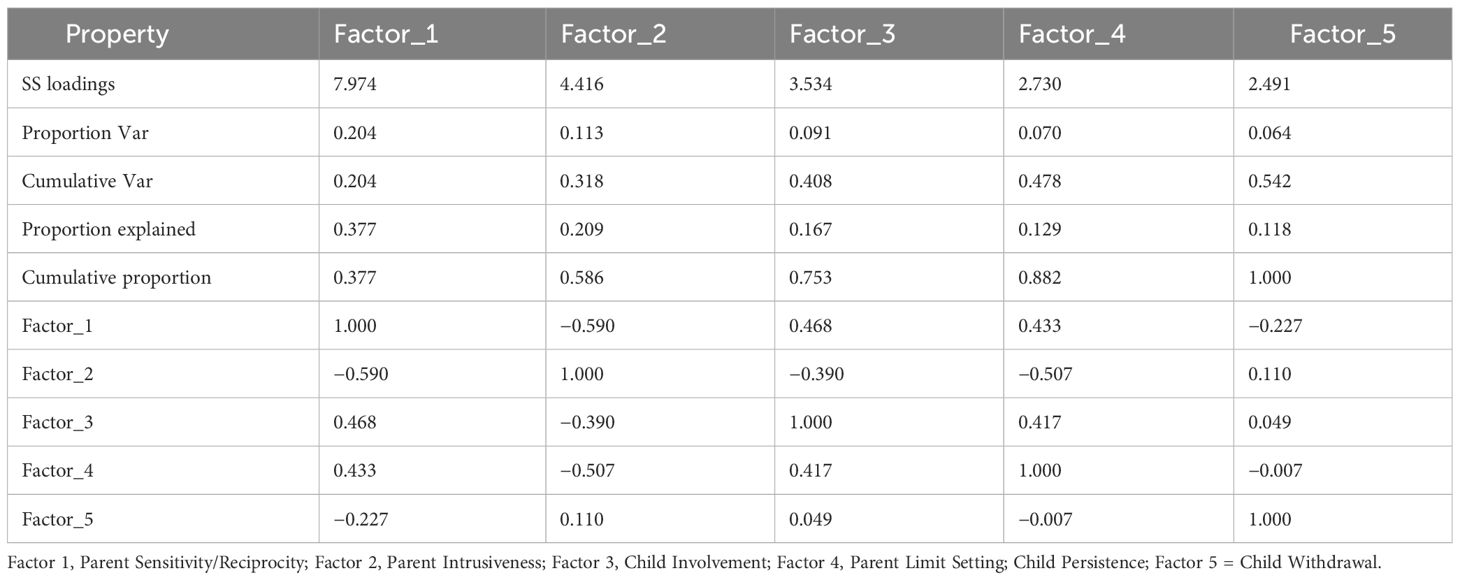
Table 7 Eigenvalues, variance explained, and factor correlations for rotated factor solution using promax rotation.
Factor 1, identified as Parent Sensitivity/Reciprocity, emerged as the most influential factor, explaining 37.7% of the variance in the data, followed by Factor 2, representing Parent Intrusiveness, which explained 20.9% of the variance. Factor 3, which captured Child Involvement, accounted for 16.7% of the variance, while Factors 4 and 5, which represented Parent Limit Setting/Child Persistence and Child Withdrawal, explained 12.9% and 11.8% of the variance, respectively. The cumulative proportion of variance explained by all five factors was 100%, indicating that together they comprehensively accounted for the variability in the observed variables. In addition, the correlations between the factors provide insight into the interrelationships among the underlying constructs. Factors 1 and 3 showed a moderate positive correlation (0.468), suggesting a relationship between Parent Sensitivity/Reciprocity and child involvement. Conversely, Factors 1 and 2 showed a negative correlation (−0.590), suggesting a possible trade-off between Parent Sensitivity/Reciprocity and Parent Intrusiveness.
4.2.3 Predictive validity
None of the three MANOVAs were significant. The logistic regression reached a maximal AUC during cross-validation of approximately 0.67, with seven items—Parent Positive Affect, Parent Depression Recoded, Parent Appropriate Range of Affect, Parent On-Task Persistence, Child Compliance, Child Affection to Parent, and Dyadic Constriction—influencing the prediction. There was, hence, weak evidence of the predictive usefulness of some of the CIB items, but none of the factor scores contributed to the prediction. An AUC value of 0.67 indicated that the model was moderately effective at distinguishing between the two classes, resp. groups.
4.2.4 Reliability
Reliability analysis was based on the original model formulated by Feldman (1998) (2) (Model A) and the newly specified Model B, which lacked the independent dyadic factors Reciprocity and Tension. We computed Cronbach’s α coefficients based on our model as a measure of internal consistency. The results are displayed in Table 8. All α coefficients were slightly better in Model B, except for the α coefficients for the factor Involvement. For Child Withdrawal, internal consistency was questionable with very low values of Cronbach’s α (see Table 8 for details). The identified α coefficients are in contrast to the α coefficients identified by Keren and Feldman (96) in young children, which ranged from 0.85 to 0.95 and were based on the traditional measure model.
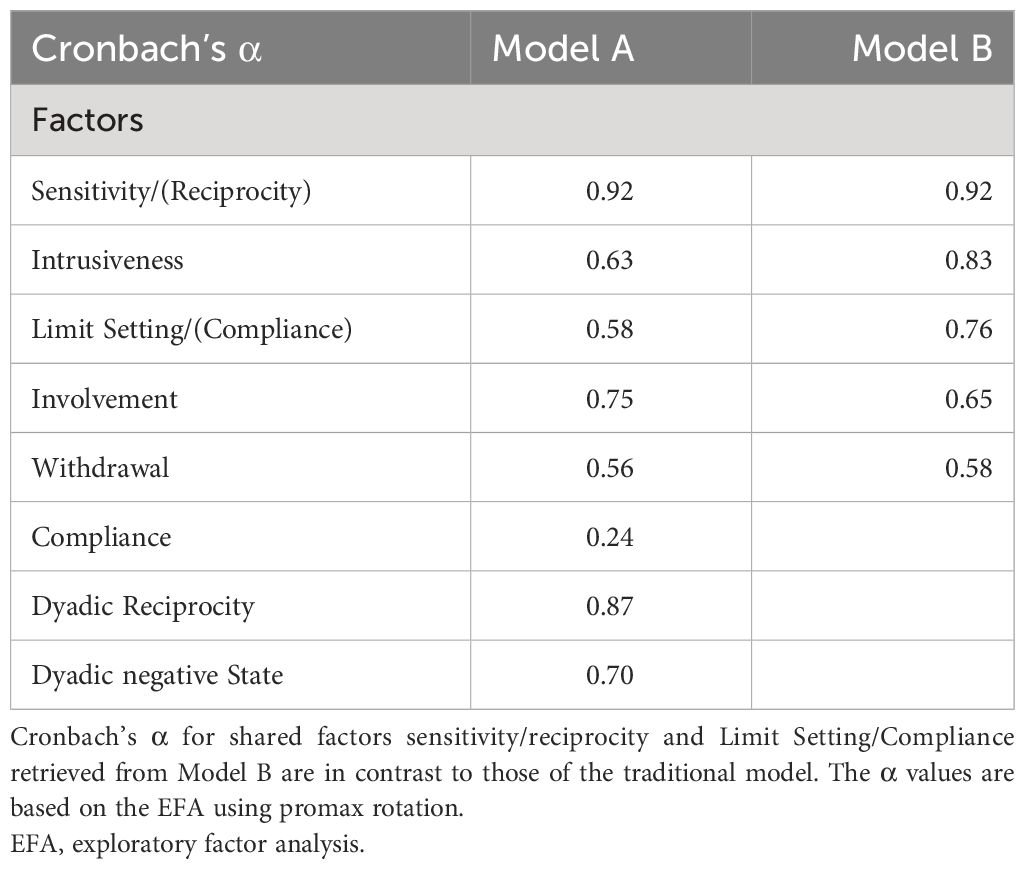
Table 8 Cronbach’s α for the traditional Model A formulated by R. Feldman and the newly specified Model B retrieved from the EFA.
5 Discussion
The present study evaluated the factor structure of the CIB in a sample of German parents with and without a mental illness. The study adds to the previous research by providing a comprehensive analysis of the psychometric properties of the CIB. The authors first considered the item properties, followed by the construct validity, with a focus on examining the dimensional structure, the measure invariance, and the reliability of the instrument. The respective objectives are shown in italics and bold in the following section.
The analysis of the item properties resulted in a 32-item CIB version and suggested the elimination of 10 items within the present sample. The application of the KMO revealed that seven items—Parent Forcing, Praising, Affectionate Touch, On-Task Persistence, Criticizing, child Persistence, and Creative Play—should be removed in order to best represent the data, as they were not fit for factorial analysis (90). These findings are similar to those of Steenhoff et al. (55), who performed the EFA for mothers and fathers separately. The KMO in their study suggested the elimination of the parental items Forcing, Depressed Mood, Praising, Affectionate Touch, and Object Oriented for mothers. For fathers, the KMO indicated the removal of Overriding, Anxiety, Criticizing, and Affectionate Touch.
In our study and based on our sample, the removed items show a few weaknesses: Reliance on Parent for Help, Praising, and Affectionate Touch showed weak discriminatory power in the present sample. Starting with Affectionate Touch, the item showed a low mean, indicating that this behavior was rarely observed. This is not surprising, as Affectionate Touch has been described as a culturally sensitive item (1), and in parenting in Northern and Middle European countries, such as Germany or Denmark, less physical closeness/touching and more distal behaviors are observed (43), compared to countries in Southern Europe or Israel (97, 98), where the instrument was originally developed. Apart from that, parental Affectionate Touch tends to decrease as children grow older (99). According to Keller et al. (44), German parents place great value on a child’s autonomy and cognitive competence, and children are perceived as equal interactive partners from an early age (45). This might also provide an explanation for the weak discrimination of the item Reliance on Parent for Help.
Both the Danish mothers without any mental illness and the parents in our mixed German sample showed little praise for their children’s actions. However, Viaux-Savelon et al. (55) were able to identify maternal praise in their sample of mothers with and without a mental illness and their children up to 2 months of age. It can therefore be concluded that maternal or parental praising can be observed in Central European cultures but seems to be sensitive toward the children’s age, emerging in dyads with very young children.
Additionally, Parent Anxiety and Child Fatigue Recoded achieved weak discrimination and a high item difficulty, suggesting that they were too difficult. The poor discriminatory power and high item difficulty of Parent Anxiety are surprising, as one might expect to observe various expressions of anxious behaviors in the present sample. This is in contrast to the Danish study, which was able to keep the item in the model for mothers but not for fathers (55), and the French study for clinically and non-clinically referred mothers (54). One might assume a gender difference when aiming to investigate parental anxious behavior, which should be further investigated. Another possible explanation may be that one might expect multidimensionality, which calls for factorial analysis when items present with poor discriminatory power (77). Unlike the study by Steenhoff et al. (55), the items Depressed Mood, Overriding, and Critique were suitable to enter factorial analysis in our sample. This may be caused by the sample composition of parents with and without a mental illness.
The analysis of construct validity resulted in a five-factor model with the following factors: Parental Sensitivity/Reciprocity, Parental Intrusiveness, Child Involvement, Parental Limit Setting/Child Compliance, and Child Withdrawal. The analyses indicated that parent limit setting merges with the factor of child compliance and parental sensitivity merges with dyadic reciprocity. This is not surprising, as strong associations between the two factors have been described in the previous research. According to the paper by Stuart et al. (100), we were also unable to identify isolated dyadic factors. For example, sensitivity and reciprocity were loaded on a common factor. When utilizing the bifactor model, we identified a general dyadic factor that represents positive aspects of parent–child interactions and is associated with sensitivity.
The bifactor model provides a clearer understanding of the underlying structure of the CIB data by decomposing variance into general and specific factors. One potential future direction is to differentiate between dyads using the dyadic main factor from the bifactor model. However, further research is necessary to investigate the differences and possible advantages of a general factor model and the traditional eight-factor model.
Additionally, this raises the question of whether parental sensitive behavior within an interaction can be assessed independently of dyadic behavior and thus also of the child’s behavior. This statistical inseparability at the factor level raises exciting questions for future research projects, and possible practical implications should be investigated in more detail.
Previous studies identified intrusive behavior to be more prevalent within the interactions of parents with anxiety disorders (1, 30) and schizophrenia (34). We were able to identify a strong factor depicting intrusiveness with a good internal consistency (α = 0.80). As disregarding a child’s signals and needs, overriding parental behavior, has been described to be more prevalent in parents with a mental illness (1), an imputation of not only the factor Intrusiveness but also the item parental Overriding might be of interest in future analyses. Overriding is the main aspect of the factor Intrusiveness, and the single item can be used as an index of intrusive parenting behavior (101). Another possibility to capture negative aspects of interactions in families of parents with a mental illness may be to measure the absence of sensitivity rather than the presence of intrusiveness. The results of various studies of parental depression, anxiety disorders (30), and PTSD (24, 35, 36) emphasized low levels of sensitivity. As evidence of factorial validity is only reported in very few studies on behavior observation instruments (57), the assessment of the dimensionality of the theoretically driven composites using factor analysis is a special highlight of the present article.
The consistency of the five factors across both rotation methods enhances the robustness and generalizability of our findings, providing confidence in the stability of the identified factor structure. The use of both rotation methods provides a comprehensive examination of the data and allows for a robust interpretation of the factor structure. This approach enhances the validity and reliability of the findings and facilitates a deeper understanding of the relationships between the variables under study.
As observational studies often fail to meet statistical standards for both reliability and validity (102), a major advantage of the present study is to first examine the validity of the instrument used before considering other observation-specific components (e.g., reliability, task, and setting) (57, 103). The Child Withdrawal factor showed poor internal consistency. Unlike the study by Steenhoff et al. (2019) (55), which reported moderate internal consistency reliability for Parent Limit Setting, we were able to obtain alpha values above acceptable. Low alpha values can be caused by a small number of items, poor inter-relatedness, or heterogeneous constructs (104). Apart from the Danish study by Steenhoff et al. (55), which only assessed the parental constructs, this is the first independent study to present the internal consistency of the theoretically derived factors of the CIB within a sample of children aged 3 to 12 years, indicating that the factor Child Withdrawal should be used and interpreted with caution when studying the respective sample.
We depicted a strong interdependence between parental sensitivity and child involvement in the factor correlations. These factors have been associated with protective behavioral factors that promote child wellbeing (17, 18) and resilience (13) in previous studies.
The statistical analyses provide insights into the predictive validity of the CIB items in parent–child interactions. Although the three MANOVA tests were not significant, the logistic regression model showed a moderate AUC. This indicates a moderate level of effectiveness in distinguishing between the two groups or classes under consideration. Notably, seven specific items emerged as influential predictors in the logistic regression model: Parent Positive Affect, Parent Depression (recoded), Parent Appropriate Range of Affect, Parent On-Task Persistence, Child Compliance, Child Affection to Parent, and Dyadic Constriction. Against the background of various parental mental illnesses, the parental items all seem to address parental affect and appear to be able to distinguish well between the group affiliations within the present sample. This finding is of particular importance, as the present sample is the first with the various parental mental illnesses. The items Child Compliance and Child Affection to Parent are likely important aspects of parent–child interactions during middle childhood that can differentiate between the two groups. These items are developmentally significant and can provide valuable insight into the parent–child relationship. At the same time, it should be noted that children’s behavior is not solely determined by their own actions but also influenced by the behavior of their parents. Therefore, it can be assumed that parental and child effects within the interaction mutually influence each other. However, it must be said at this point that these findings cannot be generalized to other populations.
Although these findings suggest weak evidence of the predictive utility of some CIB items, it is important to note that none of the factor scores derived from exploratory factor analysis made a significant contribution to the prediction. Therefore, while the logistic regression model demonstrates moderate discriminative ability, the lack of significant contribution from factor scores implies a nuanced relationship between CIB items and predictive outcomes. These findings emphasize the intricate nature of interactions between parents and children and emphasize the necessity for additional research to clarify the specific mechanisms that underlie predictive validity in this area. The CIB factors did not seem to be sufficiently sensitive to illustrate differences in interaction within a sample of parents with various mental illnesses. Given that the CIB has historically been utilized for particular disorders, this discovery appears to be novel. To apply the CIB to the described sample or similar ones in the future, additional measurement instruments may be necessary.
To substantiate the robustness of our findings and further establish the reliability of the instrument, future research efforts should prioritize the expansion of the participant pool to capture a larger sample. Furthermore, the inclusion of additional psychometric quality criteria such as test–retest stability and the assessment of convergent and divergent validity will contribute to a more comprehensive validation framework for the instrument and thus improve its reliability and applicability in different contexts.
6 Limitations
The present study was mainly limited by the small sample size. According to Kline (105), the sample should comprise at least five participants per model parameter for factor analyses, which was not met by the present data. Observational studies require significant resources for data acquisition, compared to questionnaire studies. In the context of observational studies, our sample size is quite considerable. The present analysis therefore provides a first attempt to investigate the factorial validity of the CIB given the limitations of such observational tools. Additionally, the sample was not representative of the German population, such that, for example, few fathers participated in the present study. Similar challenges regarding the sample size, parental gender, and representativity have been reported by Steenhoff et al. (55), and future studies should aim for larger sample sizes, emphasizing the recruitment of fathers to enable group comparisons across parental gender. Within the CIB, two different coding manuals are used for children under and over the age of 6. Although this approach takes developmental differences into account, it introduces a potential confounding factor that can significantly affect the validity of the study. The presence of different manuals raises concerns about the generalizability and comparability of results across different age groups, which could affect the robustness of the validation study. Future research efforts in this area should explore methods that ensure more homogeneous age groups to improve the internal validity and reliability of the observed parent–child interactions.
The confirmatory factor analysis (CFA) and subsequent assessments of measure invariance were compromised by the challenging model fits ranging from poor to satisfactory. However, achieving a good model fit in a large model based on small samples has been described as challenging because common fit indices are sensitive to sample sizes (106). Most studies using behavior observations are limited by small sample sizes and often do not report model fit indices. This association should be assessed more precisely in further studies.
We included multiple children within one family in our study, resulting in a nested data structure, but did not perform multilevel analysis. This is a serious limitation of the present study. Ignoring this nested structure can lead to underestimation of the variability within the higher-level units and overestimation of the variability within the lower-level units. Further, we did not analyze associations between the specific parental diagnoses and interactive behavior, as this is beyond the scope of the present article. These various statistical possibilities should be exhausted in future analyses.
7 Conclusion
In conclusion, this study systematically evaluated the factor structure and psychometric properties of the CIB in a sample of German parents, both with and without a mental illness. The comprehensive analysis encompassed item properties, construct validity, and model fit in the context of confirmatory and exploratory factor analyses. The findings revealed the need for refinement in the CIB instrument, with the elimination of specific items that demonstrated weak discriminatory power or were culturally sensitive, reflecting nuances in parenting practices across different regions. Moreover, the identification of a statistical inseparability at the factor level raised intriguing questions for future research and emphasized the necessity of exploring these nuances for an improved understanding of parent–child interactions. While the study offered valuable insights into the factor structure and validity of the CIB, it also acknowledged limitations, including a relatively small sample size and challenges in achieving optimal model fits, which are common in observational studies.
In conclusion, this research contributes to the ongoing refinement of the CIB instrument and underscores the importance of cultural context, parental mental illness, and developmental considerations in understanding parent–child interactions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics committee Philipps-University Marburg. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
JF: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. VS: Writing – review & editing, Investigation. KH: Writing – review & editing, Investigation. NN: Writing – review & editing, Conceptualization. CR: Writing – review & editing, Conceptualization. CS: Conceptualization, Writing – review & editing, Funding acquisition, Methodology. SW: Writing – review & editing, Funding acquisition. A-LZ: Writing – review & editing, Conceptualization. HC: Writing – review & editing, Conceptualization, Funding acquisition, Methodology, Supervision. PD: Writing – review & editing, Formal analysis. PK: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study is entirely funded by the Federal Ministry of Education and Research (BMBF) (01GL1748B).
Acknowledgments
We thank all the families who participated in the current study on mothers’ and fathers’ parenting behavior.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AD declared a past co-authorship with one of the authors HC to the handling editor.
The reviewer AT declared a past co-authorship with the author(s) to the handling editor.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1266383/full#supplementary-material
References
1. Feldman R. Parenting behavior as the environment where children grow. Cambridge Handb Environ Hum Dev. (2012), 535–67. doi: 10.1017/cbo9781139016827.031
2. Feldman R. Coding interactive behavior manual. Israel: Unpublished Manual; Bar-Ilan University (1998).
3. Cierpka M. Frühe Kindheit 0-3 Jahre. Berlin, Heidelberg: Springer (2014). doi: 10.1007/978-3-662-45742-9
4. Papoušek H, Papoušek M. Intuitives elterliches Verhalten im Zwiegespräch mit dem Neugeborenen. Sozialpäd. Prax. Klin. (1981) 3:229–38.
5. Papousek M. Intuitive elterliche Kompetenzen. Eine Ressource in der präventiven Eltern-Säuglings-Beratung und-Psychotherapie. Berlin: Deutsche Liga für das Kind (2001). pp. 1435–4705.
6. Feldman R, Eidelman AI. Biological and environmental initial conditions shape the trajectories of cognitive and social-emotional development across the first years of life. Dev Sci. (2009) 12:194–200. doi: 10.1111/j.1467-7687.2008.00761.x
7. Bowlby J. Attachment and Loss, Vol. 1: Attachment. Attachment and Loss. New York: Basic Books (1969).
8. Feldman R. The relational basis of adolescent adjustment: trajectories of mother-child interactive behaviors from infancy to adolescence shape adolescents’ adaptation. Attach Hum Dev. (2010) 12:173–92. doi: 10.1080/14616730903282472
9. Gibson FL, Ungerer JA, McMahon CA, Leslie GI, Saunders DM. The mother-child relationship following in vitro fertilisation (IVF): Infant attachment, responsivity, and maternal sensitivity. J Child Psychol Psychiatry. (2000) 41:1015–23. doi: 10.1017/S0021963099006472
10. Atkinson L, Niccols A, Paglia A, Coolbear J, H. Parker KC, Poulton L, et al. A meta-analysis of time between maternal sensitivity and attachment assessments: Implications for internal working models in infancy/toddlerhood. J Soc Pers Relat. (2000) 17:791–810. doi: 10.1177/0265407500176005
11. Ainsworth MD, Blehar M, Waters E, Wall S. Patterns of attachment. Hillsdale nj: erlbaum. (1978). doi: 10.4324/9781315802428
12. Zvara BJ, Sheppard KW, Cox M. Bidirectional effects between parenting sensitivity and child behavior: A cross-lagged analysis across middle childhood and adolescence. J Family Psychol. (2018) 32:484–95. doi: 10.1037/fam0000372
13. Feldman R. Social behavior as a transdiagnostic marker of resilience. Annu Rev Clin Psychol. (2021) 17:153–80. doi: 10.1146/annurev-clinpsy-081219-102046
14. Page M, Wilhelm MS, Gamble WC, Card NA. A comparison of maternal sensitivity and verbal stimulation as unique predictors of infant social–emotional and cognitive development. Infant Behav Dev. (2010) 33:101–10. doi: 10.1016/j.infbeh.2009.12.001
15. Shumow L, Lomax R. Parental efficacy: predictor of parenting behavior and adolescent outcomes. Parenting: Sci Pract. (2002) 2:127–50. doi: 10.1207/S15327922PAR0202_03
16. Lemelin J-P, Tarabulsy GM, Provost MA. Predicting preschool cognitive development from infant temperament, maternal sensitivity, and psychosocial risk. Merrill-Palmer Q. (2006) 52:779–804. doi: 10.1353/mpq.2006.0038
17. Colman RA, Hardy SA, Albert M, Raffaelli M, Crockett L. Early predictors of self-regulation in middle childhood. Infant Child Dev. (2006) 15:421–37. doi: 10.1002/(ISSN)1522-7219
18. Lengua LJ, Honorado E, Bush NR. Contextual risk and parenting as predictors of effortful control and social competence in preschool children. J Appl Dev Psychol. (2007) 28:40–55. doi: 10.1016/j.appdev.2006.10.001
19. Christiansen H, Reck C, Zietlow A-L, Otto K, Steinmayr R, Wirthwein L, et al. Children of mentally III parents at risk evaluation (COMPARE): design and methods of a randomized controlled multicenter study-part I. Front Psychiatry. (2019) 10:128. doi: 10.3389/fpsyt.2019.00128
20. Reck C, Tietz A, Müller M, Seibold K, Tronick E. The impact of maternal anxiety disorder on mother-infant interaction in the postpartum period. PloS One. (2018) 13:e0194763. doi: 10.1371/journal.pone.0194763
21. Rodrigues M, Sokolovic N, Madigan S, Luo Y, Silva V, Misra S, et al. Paternal sensitivity and children’s cognitive and socioemotional outcomes: A meta-analytic review. Child Dev. (2021) 92:554–77. doi: 10.1111/cdev.13545
22. Kress S, Cierpka M, Möhler E, Resch F. Mütterliche Affektabstimmung von Müttern mit Missbrauchserfahrungen in der Mutter-Kind-Interaktion. Praxis Der Kinderpsychologie Und Kinderpsychiatrie (2012) 61:271–285. doi: 10.23668/psycharchives.9737
23. Bödeker K, Fuchs A, Führer D, Kluczniok D, Dittrich K, Reichl C, et al. Impact of maternal early life maltreatment and maternal history of depression on child psychopathology: mediating role of maternal sensitivity? Child Psychiatry Hum Dev. (2019) 50:278–90. doi: 10.1007/s10578-018-0839-z
24. Feldman R, Vengrober A. Posttraumatic stress disorder in infants and young children exposed to war-related trauma. J Am Acad Child Adolesc Psychiatry. (2011) 50:645–58. doi: 10.1016/j.jaac.2011.03.001
25. Crockenberg SC, Leerkes EM. Parental acceptance, postpartum depression, and maternal sensitivity: mediating and moderating processes. J Family Psychol. (2003) 17:80. doi: 10.1037//0893-3200.17.1.80
26. Herrera E, Reissland N, Shepherd J. Maternal touch and maternal child-directed speech: effects of depressed mood in the postnatal period. J Affect Disord. (2004) 81:29–39. doi: 10.1016/j.jad.2003.07.001
27. Malphurs JE, Raag T, Field T, Pickens J, Pelaez-Nogueras M. Touch by intrusive and withdrawn mothers with depressive symptoms. Early Dev Parenting: Int J Res Pract. (1996) 5:111–5. doi: 10.1002/(SICI)1099-0917(199606)5:2111::AID-EDP122>3.0.CO;2-#
28. Feldman R. Maternal versus child risk and the development of parent–child and family relationships in five high-risk populations. Dev Psychopathol. (2007) 19:293–312. doi: 10.1017/S0954579407070150
29. Zietlow A-L, Nonnenmacher N, Reck C, Ditzen B, Müller M. Emotional stress during pregnancy–associations with maternal anxiety disorders, infant cortisol reactivity, and mother–child interaction at pre-school age. Front Psychol. (2019) 10:2179. doi: 10.3389/fpsyg.2019.02179
30. Feldman R. Parent–infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. J Child Psychol Psychiatry. (2007) 48:329–54. doi: 10.1111/j.1469-7610.2006.01701.x
31. Lovejoy MC, Graczyk PA, O’Hare E, Neuman G. Maternal depression and parenting behavior: A meta-analytic review. Clin Psychol Rev. (2000) 20:561–92. doi: 10.1016/S0272-7358(98)00100-7
32. Ulmer-Yaniv A, Djalovski A, Yirmiya K, Halevi G, Zagoory-Sharon O, Feldman R. Maternal immune and affiliative biomarkers and sensitive parenting mediate the effects of chronic early trauma on child anxiety. psychol Med. (2018) 48:1020–33. doi: 10.1017/S0033291717002550
33. Feldman R, Granat AD, Pariente C, Kanety H, Kuint J, Gilboa-Schechtman E. Maternal depression and anxiety across the postpartum year and infant social engagement, fear regulation, and stress reactivity. J Am Acad Child Adolesc Psychiatry. (2009) 48:919–27. doi: 10.1097/CHI.0b013e3181b21651
34. Deneke C, Lüders B. Besonderheiten der Interaktion zwischen psychisch kranken Eltern und ihren kleinen Kindern. Praxis Der Kinderpsychologie Und Kinderpsychiatrie. (2003) 52:172–181.
35. Halevi G, Djalovski A, Kanat-Maymon Y, Yirmiya K, Zagoory-Sharon O, Koren L, et al. The social transmission of risk: Maternal stress physiology, synchronous parenting, and well-being mediate the effects of war exposure on child psychopathology. J Abnormal Psychol. (2017) 126:1087. doi: 10.1037/abn0000307
36. Levy J, Yirmiya K, Goldstein A, Feldman R. Chronic trauma impairs the neural basis of empathy in mothers: relations to parenting and children’s empathic abilities. Dev Cogn Neurosci. (2019) 38:100658. doi: 10.1016/j.dcn.2019.100658
37. Priel A, Djalovski A, Zagoory-Sharon O, Feldman R. Maternal depression impacts child psychopathology across the first decade of life: Oxytocin and synchrony as markers of resilience. J Child Psychol Psychiatry. (2019) 60:30–42. doi: 10.1111/jcpp.12880
38. Cooke JE, Deneault A-A, Devereux C, Eirich R, Fearon RM, Madigan S. Parental sensitivity and child behavioral problems: A meta-analytic review. Child Dev. (2022) 93:1231–48. doi: 10.1111/cdev.13764
39. Lucassen N, Tharner A, van IJzendoorn MH, Bakermans-Kranenburg MJ, Volling BL, Verhulst FC, et al. The association between paternal sensitivity and infant–father attachment security: A meta-analysis of three decades of research. J Family Psychol. (2011) 25:986. doi: 10.1037/a0025855
40. Bornstein MH. Cultural approaches to parenting. Parenting: Sci Pract. (2012) 12:212–21. doi: 10.1080/15295192.2012.683359
41. Feldman R, Masalha S. Parent–child and triadic antecedents of children’s social competence: Cultural specificity, shared process. Dev Psychol. (2010) 46:455. doi: 10.1037/a0017415
42. Harwood RL, Schoelmerich A, Schulze PA, Gonzalez Z. Cultural differences in maternal beliefs and behaviors: A study of middle-class Anglo and Puerto Rican mother-infant pairs in four everyday situations. Child Dev. (1999) 70:1005–16. doi: 10.1111/1467-8624.00073
43. Keller H, Kärtner J, Borke J, Yovsi R, Kleis A. Parenting styles and the development of the categorical self: A longitudinal study on mirror self-recognition in Cameroonian Nso and German families. Int J Behav Dev. (2005) 29:496–504. doi: 10.1177/01650250500147485
44. Keller H, Völker S, Yovsi RD. Conceptions of parenting in different cultural communities: The case of West African Nso and Northern German women. Soc Dev. (2005) 14:158–80. doi: 10.1111/j.1467-9507.2005.00295.x
45. Keller H. Socialization for competence: Cultural models of infancy. Hum Dev. (2003) 46:288–311. doi: 10.1159/000071937
46. Yogman MW. Games fathers and mothers play with their infants. Infant Ment Health J. (1981) 2:241–8. doi: 10.1002/(ISSN)1097-0355
47. Lamb ME. Father-infant and mother-infant interaction in the first year of life. Child Dev. (1977) 48(1):167–81. doi: 10.2307/1128896
48. Feldman R, Weller A, Sirota L, Eidelman AI. Testing a family intervention hypothesis: The contribution of mother-infant skin-to-skin contact (kangaroo care) to family interaction, proximity, and touch. J Family Psychol. (2003) 17:94–107. doi: 10.1037/0893-3200.17.1.94
49. Feldman R, Eidelman AI. Direct and indirect effects of breast milk on the neurobehavioral and cognitive development of premature infants. Dev Psychobiology: J Int Soc Dev Psychobiology. (2003) 43:109–19. doi: 10.1002/dev.10126
50. Keren M, Feldman R, Tyano S. Diagnoses and interactive patterns of infants referred to a community-based infant mental health clinic. J Am Acad Child Adolesc Psychiatry. (2001) 40:27–35. doi: 10.1097/00004583-200101000-00013
51. Priel A, Zeev-Wolf M, Djalovski A, Feldman R. Maternal depression impairs child emotion understanding and executive functions: The role of dysregulated maternal care across the first decade of life. Emotion. (2020) 20:1042–58. doi: 10.1037/emo0000614
52. Feldman R, Eidelman AI, Rotenberg N. Parenting stress, infant emotion regulation, maternal sensitivity, and the cognitive development of triplets: a model for parent and child influences in a unique ecology. Child Dev. (2004) 75:1774–91. doi: 10.1111/j.1467-8624.2004.00816.x
53. Feldman R, Masalha S, Nadam R. Cultural perspective on work and family: Dual-earner Israeli Jewish and Arab families at the transition to parenthood. J Family Psychol. (2001) 15:492–509. doi: 10.1037/0893-3200.15.3.492
54. Viaux-Savelon S, Leclere C, Aidane E, Bodeau N, Camon-Senechal L, Vatageot S, et al. Validation de la version française du Coding Interactive Behavior sur une population d’enfants à la naissance et à 2 mois. Neuropsychiatrie l’Enfance l’Adolescence. (2014) 62:53–60. doi: 10.1016/j.neurenf.2013.11.010
55. Steenhoff T, Tharner A, Væver MS. Mothers’ and fathers’ observed interaction with preschoolers: Similarities and differences in parenting behavior in a well-resourced sample. PloS One. (2019) 14:e0221661. doi: 10.1371/journal.pone.0221661
56. Dollberg D, Feldman R, Keren M. Maternal representations, infant psychiatric status, and mother-child relationship in clinic-referred and non-referred infants. Eur Child Adolesc Psychiatry. (2010) 19:25–36. doi: 10.1007/s00787-009-0036-5
57. Lotzin A, Lu X, Kriston L, Schiborr J, Musal T, Romer G, et al. Observational tools for measuring parent–infant interaction: A systematic review. Clin Child Family Psychol Rev. (2015) 18:99–132. doi: 10.1007/s10567-015-0180-z
58. Stracke M, Gilbert K, Kieser M, Klose C, Krisam J, Ebert DD, et al. COMPARE family (Children of mentally ill parents at risk evaluation): A study protocol for a preventive intervention for children of mentally ill parents (Triple P, evidence-based program that enhances parentings skills, in addition to gold-standard CBT with the mentally ill parent) in a multicenter RCT-part II. Front Psychiatry. (2019) 10:54. doi: 10.3389/fpsyt.2019.00054
59. Zietlow A-L, Woll CF, Nonnenmacher N, Müller M, Labonte V, Ditzen B, et al. Study protocol of the COMPARE-Interaction study: the impact of maternal comorbid depression and anxiety disorders in the peripartum period on child development. BMJ Open. (2022) 12:e050437. doi: 10.1136/bmjopen-2021-050437
60. Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika. (1965) 52:591–611. doi: 10.1093/biomet/52.3-4.591
61. Mann HB, Whitney DR. On a Test of Whether one of Two Random Variables is Stochastically Larger than the Other. Ann Math Statist. (1947) 18:50–60. doi: 10.1214/aoms/1177730491
62. Margraf J, Cwik JC, Suppiger A, Schneider S. DIPS Open Access: Diagnostisches Interview bei psychischen Störungen (DIPS). Bochum: Forschungs- und Behandlungszentrum für psychische Gesundheit, Ruhr-Universität Bochum (2017).
63. Statisches Bundesamt. Bevölkerung und Erwerbstätigkeit. Bevölkerung mit Migrationshintergrund-Ergebnisse des Mikrozensus. (2019).
64. Schneider S, Pflug V, In-Albon T, Margraf J. Kinder-DIPS Open Access: Diagnostisches Interview bei psychischen Störungen im Kindes-und Jugendalter. Bochum: Forschungs- und Behandlungszentrum für psychische Gesundheit, Ruhr-Universität Bochum (2017).
65. Bolten M, Equit M, von GA, In-Albon T. SIVA: 0-6. Das Strukturierte Interview für das Vorschulalter [Verfahrensdokumentation, Interviewleitfaden mit den Modulen 0-16, Handbuch, Zuordnung Module und Interview und Diagnoseblatt]. In Leibniz-Institut für Psychologie (ZPID) (Hrsg.), Open Test Archive. Trier: ZPID (2021). doi: 10.23668/psycharchives.4365
66. Derogatis LR. BSI: Brief Symptom Inventory. Deutsche Fassung. Frankfurt am Main: Pearson Deutschland GmbH (2017).
67. Döpfner M, Plück J, Kinnen C, Achenbach TM. Deutsche Schulalter-Formen der Child Behavior Checklist von Thomas M. Achenbach: CBCL/6-18R-TRF/6-18R-YSR/11-18R; Elternfragebogen über das Verhalten von Kindern und Jugendlichen (CBCL/6-18R), Lehrerfragebogen über das Verhalten von Kindern und Jugendlichen (TRF/6-18R), Fragebogen für Jugendliche (YSR/11-18R). Göttingen: Hogrefe (2014).
68. Achenbach TM, La Rescorla. Manual for the ASEBA school-age forms and profiles. In: Research Center for Children, Youth, and Families. University of Vermont, Burlington, VT (2001).
69. Achenbach TM, Rescorla LA. Manual for the ASEBA preschool forms and profiles. Burlington, VT: University of Vermont, Research center for children, youth (2000).
70. Achenbach TM, Dumenci L, Rescorla LA. Ratings of relations between DSM-IV diagnostic categories and items of the CBCL/6-18. TRF YSR. (2001).
72. Ferber SG, Feldman R, Kohelet D, Kuint J, Dollberg S, Arbel E, et al. Massage therapy facilitates mother–infant interaction in premature infants. Infant Behav Dev. (2005) 28:74–81. doi: 10.1016/j.infbeh.2004.07.004
73. Feldman R. Parents’ convergence on sharing and marital satisfaction, father involvement, and parent-child relationship at the transition to parenthood. Infant Ment Health J. (2000) 21:176–91. doi: 10.1002/1097-0355(200007)21:3<176:AID-IMHJ3>3.0.CO;2-4
74. Feldman R, Eidelman AI, Sirota L, Weller A. Comparison of skin-to-skin (kangaroo) and traditional care: parenting outcomes and preterm infant development. Pediatrics. (2002) 110:16–26. doi: 10.1542/peds.110.1.16
75. Feldman R, Greenbaum CW, Mayes LC, Erlich SH. Change in mother-infant interactive behavior: Relations to change in the mother, the infant, and the social context. Infant Behav Dev. (1997) 20:151–63. doi: 10.1016/s0163-6383(97)90018-7
76. Feldman R, Klein PS. Toddlers’ self-regulated compliance to mothers, caregivers, and fathers: implications for theories of socialization. Dev Psychol. (2003) 39:680–92. doi: 10.1037/0012-1649.39.4.680
77. Moosbrugger H, Kelava A. Testtheorie und Fragebogenkonstruktion: Mit 66 Abbildungen und 41 Tabellen. Berlin, Heidelberg: Springer (2020). p. 770.
78. Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. psychol Methods. (1999) 4:272. doi: 10.1037//1082-989X.4.3.272
79. Steiner M, Grieder S. EFAtools: An R package with fast and flexible implementations of exploratory factor analysis tools. JOSS. (2020) 5:2521. doi: 10.21105/joss.02521
80. Cattell RB. The scree test for the number of factors. Multivariate Behav Res. (1966) 1:245–76. doi: 10.1207/s15327906mbr0102_10
81. Horn JL. A rational and test for the number of factors in factor analysis. Psychometrika. (1965) 30:179–85. doi: 10.1007/BF02289447
82. Preacher KJ, MacCallum RC. Repairing Tom Swift’s electric factor analysis machine. Understanding Stat. (2003) 2:13–43. doi: 10.1207/S15328031US0201_02
83. Hendrickson AE, White PO. Promax: A quick method for rotation to oblique simple structure. Br J Stat Psychol. (1964) 17:65–70. doi: 10.1111/j.2044-8317.1964.tb00244.x
84. Friedrich S, Pauly M. MATS: Inference for potentially singular and heteroscedastic MANOVA. J Multivar Anal. (2017) 165:166–79. doi: 10.1016/j.jmva.2017.12.008
85. de Hond AA, Steyerberg EW, Van calster B. Interpreting area under the receiver operating characteristic curve. Lancet Digit Health. (2022). doi: 10.1016/S2589-7500(22)00188-1
86. Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. (1993) 78:98. doi: 10.1037//0021-9010.78.1.98
87. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropractic Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
89. Bartlett MS. The statistical conception of mental factors. Br J Psychol Gen Section. (1937) 28:97–104. doi: 10.1111/j.2044-8295.1937.tb00863.x
90. Kaiser HF, Rice J. Little jiffy, mark IV. Educ psychol measurement. (1974) 34:111–7. doi: 10.1177/001316447403400115
91. Velicer WF. Determining the number of components from the matrix of partial correlations. Psychometrika. (1976) 41:321–7. doi: 10.1007/BF02293557
92. Velicer WF, Eaton CA, Fava JL. Construct explication through factor or component analysis: A review and evaluation of alternative procedures for determining the number of factors or components. Problems solutions Hum Assess. (2000), 41–71. doi: 10.1007/978-1-4615-4397-8_3
93. Clark DA, Bowles RP. Model fit and item factor analysis: Overfactoring, underfactoring, and a program to guide interpretation. Multivariate Behav Res. (2018) 53:544–58. doi: 10.1080/00273171.2018.1461058
94. Finch WH. Using fit statistic differences to determine the optimal number of factors to retain in an exploratory factor analysis. Educ psychol measurement. (2020) 80:217–41. doi: 10.1177/0013164419865769
95. Gäde JC, Schermelleh-Engel K, Brandt H. Konfirmatorische faktorenanalyse (CFA). In: Testtheorie und Fragebogenkonstruktion. Berlin, Heidelberg: Springer (2020). p. 615–59.
96. Keren M, Feldman R. Le rôle de l’évaluation des interactions lors du repas dans l’évaluation psychopathologique usuelle du jeune enfant. Devenir. (2002) 14:5. doi: 10.3917/dev.021.0005
97. Lustig MW, Koester J, Halualani R. Intercultural competence: Interpersonal communication across cultures. Pearson/A B Boston. (2006).
98. Sussman NM, Rosenfeld HM. Influence of culture, language, and sex on conversational distance. J Pers Soc Psychol. (1982) 42:66. doi: 10.1037//0022-3514.42.1.66
99. Ferber SG, Feldman R, Makhoul IR. The development of maternal touch across the first year of life. Early Hum Dev. (2008) 84:363–70. doi: 10.1016/j.earlhumdev.2007.09.019
100. Stuart AC, Egmose I, Smith-Nielsen J, Reijman S, Wendelboe KI, Væver MS. Coding interactive behaviour instrument: mother-infant interaction quality, construct validity, measurement invariance, and postnatal depression and anxiety. J Child Family Stud. (2023) 32:1839–54. doi: 10.1007/s10826-023-02584-2
101. Feldman R, Bamberger E, Kanat-Maymon Y. Parent-specific reciprocity from infancy to adolescence shapes children’s social competence and dialogical skills. Attach Hum Dev. (2013) 15:407–23. doi: 10.1080/14616734.2013.782650
102. Gridley N, Blower S, Dunn A, Bywater T, Whittaker K, Bryant M. Psychometric properties of parent–child (0–5 years) interaction outcome measures as used in randomized controlled trials of parent programs: A systematic review. Clin Child Family Psychol Rev. (2019) 22:253–71. doi: 10.1007/s10567-019-00275-3
103. Munson LJ, Odom SL. Review of rating scales that measure parent-infant interaction. Topics Early Childhood Special Educ. (1996) 16:1–25. doi: 10.1177/027112149601600104
104. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. (2011) 2:53–5. doi: 10.5116/ijme.4dfb.8dfd
105. Reinecke J. Strukturgleichungsmodelle in den sozialwissenschaften. Gruyter Oldenbourg. (2014). doi: 10.1524/9783486854008
Keywords: parent-child interaction, Coding Interactive Behavior, CIB, parents with a mental illness, factorial structure, behavior observation, factor analysis, psychometric properties
Citation: Fahrer J, Doebler P, Hagelweide K, Kern P, Nonnenmacher N, Seipp V, Reck C, Schwenck C, Weigelt S, Zietlow A-L and Christiansen H (2024) Parent–child interactive behavior in a German sample of parents with and without a mental illness: model replication and adaption of the Coding Interactive Behavior system. Front. Psychiatry 15:1266383. doi: 10.3389/fpsyt.2024.1266383
Received: 24 July 2023; Accepted: 23 February 2024;
Published: 30 April 2024.
Edited by:
Geneviève Piché, University of Quebec in Outaouais, CanadaReviewed by:
Abigail Lucy Dunn, University of Surrey, United KingdomAnne Amalie Elgaard Thorup, Copenhagen University Hospital, Denmark
Anne Stuart, University of Copenhagen, Denmark
Copyright © 2024 Fahrer, Doebler, Hagelweide, Kern, Nonnenmacher, Seipp, Reck, Schwenck, Weigelt, Zietlow and Christiansen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Fahrer, anVsaWEtZmFocmVyQHdlYi5kZQ==