 Dandan Ma
Dandan Ma Jinya Cao
Jinya Cao Jing Wei
Jing Wei Jing Jiang
Jing Jiang- Department of Psychological Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Objective: This study aimed to analyze the patterns of life events (LEs) and defense mechanisms in outpatients with depression and investigate the mediating role of defense mechanisms in the association between LEs and depressive symptoms in a psychosomatic outpatient sample in China.
Materials and methods: All of 2,747 outpatients (aged 18–65) from psychosomatic department were investigated in this study. LEs, depressive symptoms, and defense mechanisms were assessed by the Life Events Scale (LES), Patient-Health-Questionnaire-9 (PHQ-9), and the Defense Style Questionnaire (DSQ), respectively.
Results: Based on the optimal cut-off point of PHQ-9, 1840 (67.0%) patients had a PHQ-9 score of 10 or higher (depression group), and 907 (33.0%) had a score below 10 (non-depression group). The scores of Negative Life Events (NLEs), immature and intermediate defense mechanisms in the depression group were significantly higher than those in the non-depression group, while the scores of mature defense mechanisms were the opposite (p < 0.001). NLEs was directly related to depressive symptoms (b = 0.010, p < 0.001), and significant indirect effect via immature defense mechanisms (b = 0.008, p < 0.001) was observed.
Conclusion: Immature defense mechanisms play an important mediating role in the relationship between NLEs and depressive symptoms. Helping patients improving defense mechanisms and dealing with NLEs may be of great help in the treatment of relevant patients.
1 Introduction
Depression is one of the most common psychiatric disorders characterized by persistent feelings of sadness, helplessness, hopelessness, reduced energy or fatigue, and considerable difficulty functioning in dealing with daily life (1). In the past decade, the prevalence of depression among young people has risen dramatically (2). Previous work has noticed the complexity of the etiology of depression (3, 4), and focusing solely on factors in a single field cannot understand the occurrence of depression. Today, it is a trend to understand depression from the perspective of biopsychosoical interactions (5, 6), and one most concerned environmental factors in this regard are life events (LEs) (7).
A severe independent event is sufficient to trigger depression (8). Studies have shown that LEs play an important role in the onset, remission, recurrence, persistence, and prognosis of depression (9, 10). LEs include negative life events (NLEs, e.g., bereavement; divorce) and positive life events (PLEs, e.g., marriage) (11). The impacts of NLEs on the development of depressive symptoms have consistently been documented (12). Mazure et al. reviewed previous case–control studies and found that depressed patients report higher rates of at least one severe NLEs than control group in both clinical and non-clinical samples (13). In addition, PLEs may also influence the depressive symptoms, yet there is no consensus. Shahar et al. (14) tested a 603 adolescent sample and found that PLEs are both protective and harmful factors. On the one hand, PLEs share an event-related aspect with NLEs, and on the other hand, PLEs can buffer the impact of NLEs on distress. Some studies have suggested that PLEs are related with lower depressive symptoms (15, 16), whereas others failed to show this relationship (17). According to diathesis-stress theories, vulnerable individuals more likely depressed when confront stressful LEs (18). There is a consensus that LEs are associated with depressive symptoms, but the underlying mechanisms between them has not been fully explored.
A growing body of literature has suggested that psychological factors play an important role in the onset of depression, depressed patients use more immature defense mechanisms (19). The concept of defense mechanism was first proposed by Freud in 1894 (20). Defense mechanism is defined as an automatic psychological process that can protect individuals from excessive anxiety and distress caused by internal or external dangers or stressors by distorting their perception of threatening events, thus maintaining psychological balance (21). Defense mechanisms can be grouped into three types: immature, intermediate, and mature defense mechanisms. Mature defense mechanisms indicate that individuals have a greater ability to adapt to reality and deal with social and emotional conflicts without distorting reality. Immature defense mechanisms indicate maladaptation to internal and external conflicts, which is related to severe psychopathology (22). Accumulating studies has confirmed that immature defense mechanisms predict greater severity of depression, poor treatment adherence, and unsatisfactory therapeutic outcomes (23, 24). Whereas, mature defense mechanisms are associated with less severity of depression and satisfactory treatment outcomes (25). Theoretically, the development of individual defenses is influenced by both biological and environmental factors (26). The relationship between defense mechanisms and LEs has also been explored. The increasing stressful LEs, the more use of immature defense mechanisms (27).
Further, previous studies suggested that immature defense mechanisms may play a mediate role in the relationship between childhood NLEs (such as childhood physical or psychological abuse) and psychopathological symptoms (28, 29). In the present study, we primarily tested the hypothesis that defensive mechanisms mediate the relationship between LEs and depressive symptoms. In addition, we also explored the characteristics of LEs and defensive mechanisms in outpatients with depression. We hope to provide more effective strategies for the treatment of patients with depressive symptoms.
2 Materials and methods
2.1 Participants
We recruited all the outpatients who attended the Department of Psychological Medicine of Peking Union Medical College Hospital from June, 2020 to April, 2023 and completed the following self-report questionnaires. The inclusion criteria were as follows: the age ranged from 18 to 65 years old, sufficient command of Chinese and cognitive capability to understand the self-report questionnaires. The exclusion criteria were adults with language barriers and unable to complete all the questionnaires. Anxiety disorders, depression disorders, obsessive-compulsive disorder, somatic symptom disorders, insomnia comprise the most common diagnosis in our outpatients. The project was approved by the Ethics Committees of Peking Union Medical College Hospital.
2.2 Measurements
2.2.1 Depression
Depression was evaluated using the Patient-Health-Questionnaire-9 (PHQ-9) (30). PHQ-9 is a 4-point Likert scale used to describe the severity of depressive symptoms in the past two weeks. The total score of PHQ-9 ranging from 0 to 27, and the higher score indicates more severe depressive symptoms. PHQ-9 is an effective tool for monitoring patients with major depression in China, and the optimal cutoff point for detecting depression is 10 (31). In the present study, the Cronbach alpha value was 0.89.
2.2.2 Life events
LEs were measured by the Life Events Scale (LES). LES is a self-report questionnaire consists of 48 items used to assess negative and positive LEs in terms of family life, work and social interactions. The purpose is to evaluate the nature and quantity of LEs to reflect perceived stress. Stimulation of a certain event = the severity of influence × the duration of influence × the number of occurrences. The total stimulus of LEs is the sum of the total stimulus of positive events and the total stimulus of negative events. Higher scores of the total stimulus of LEs represents greater stress perceived. LES has been widely used in China (32, 33). In the present study, the Cronbach alpha value was 0.82.
2.2.3 Defense mechanism
Defense mechanism was assessed by the defense style questionnaire (DSQ) (34). DSQ includes 88 items, which can be divided into 4 factors. Factor I: immature defense mechanisms (e.g., projection, passive aggression); Factor II: mature defense mechanisms (e.g., sublimation, humor); Factor III: intermediate defense mechanisms (e.g., reaction formation, undoing); and Factor IV: concealment factor. It is a 9-point Likert scale, with ratings ranging from 1 (strongly disagree) to 9 (strongly agree) for each item. The closer to 9, the more frequently this defense mechanism is applied (35, 36). In the present study, the Cronbach alpha value was 0.91.
2.3 Data analysis
IBM SPSS Statistics 25.0 and PROCESS were used for statistical analysis.
Continuous variables and categorical variables were expressed as mean ± standard deviation (x ± s) and percentage, respectively. Based on the score of PHQ-9, all participants were divided into two groups. The comparison between the two groups was conducted using t-test for continuous variables and chi square test for categorical variables.
Characteristics with significant inter group differences (p < 0.05) were considered as potential predictive variables for depression and included in binary logistic regression using the ENTER procedure (total score of LES, score of negative LEs, score of family life, score of work, score of social interactions, score of immature defense mechanism, score of mature defense mechanism, and score of intermediate defense mechanism).
The correlation between NLEs and defense mechanisms was tested by the Pearson correlation coefficient.
Using the Bootstrap method with 5,000 samples, the mediating role of defense mechanisms (immature defense mechanisms, mature defense mechanisms and intermediate defense mechanisms) in the relationship between NLEs and depressive symptoms was tested through SPSS PROCESS (Model 4) (37). Gender (code: male = 1, female = 2), age and diagnosis (code: anxiety disorders = 1, depression disorders = 2, obsessive-compulsive disorders = 3, somatic symptom disorders = 4, insomnia = 5, and others = 6) were included as covariates to control for potential demographic impacts.
3 Results
3.1 Clinical features of patients with depression
In total, 2,747 outpatients were enrolled in the study. Based on the optimal cut-off point of PHQ-9, all participants were divided into two groups. Among them, 1840 (67.0%) patients had a PHQ-9 score of 10 or higher (depression group), and 907 (33.0%) had a score below 10 (non-depression group).
The age and percentage of male in the depression group were significantly lower than those in the non-depression group (p < 0.001).
The total LEs score of the depression group was significantly higher than that of the non-depression group (p < 0.001). Specifically, the scores of NLEs, family LEs, work related events and social related events in the depression group were significantly higher than those in the non-depression group (p < 0.001). However, no difference was found in the score of PLEs between the two groups (p = 0.181).
The scores of immature and intermediate defense mechanisms in the depression group were significantly higher than those in the non-depression group, while the scores of mature defense mechanisms were the opposite (p < 0.001) (see Supplementary Table S1 and Table 1).
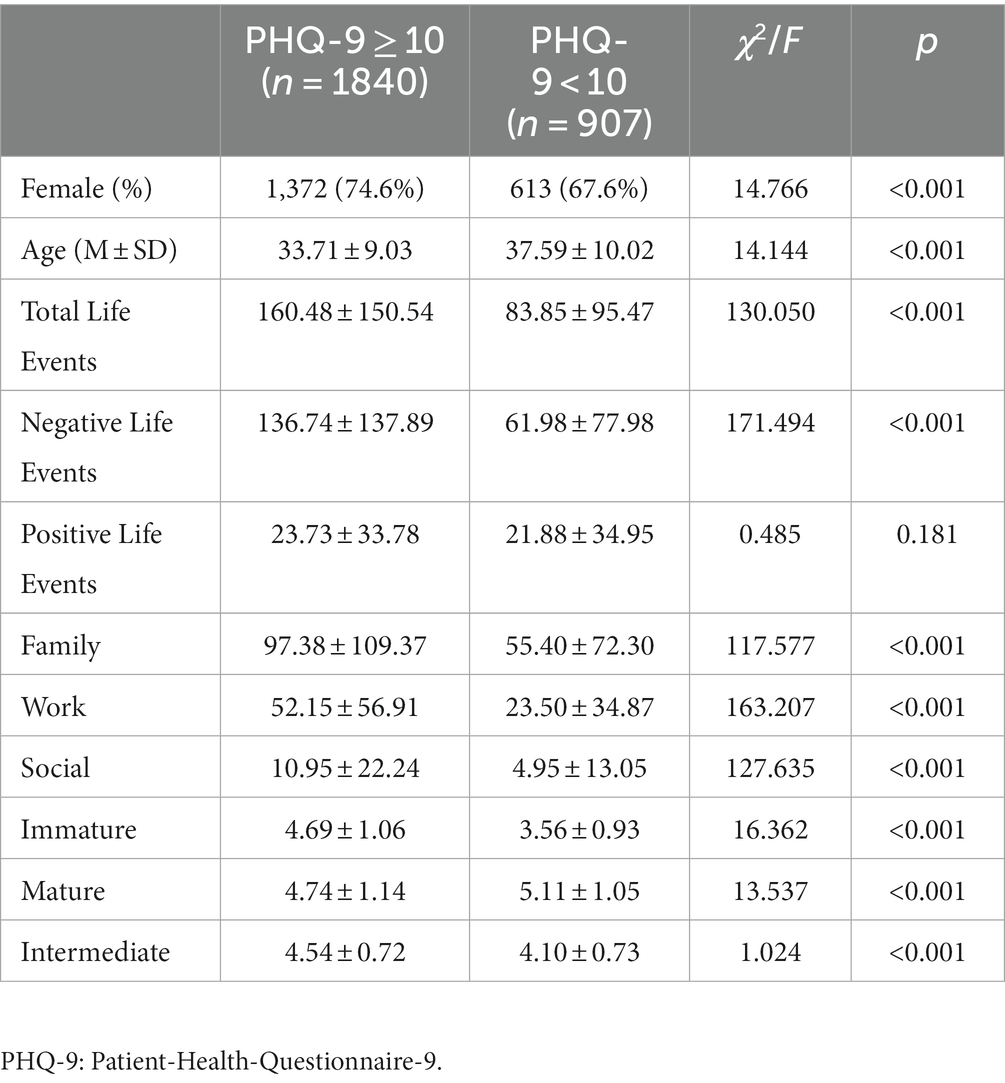
Table 1. Clinical features of patients with depression.
3.2 Predictor variables of depression
In binary logistic regression, NLEs, immature defense mechanisms, mature defense mechanisms and intermediate defense mechanisms were found to be predictor variables of a depression diagnosis. The explained variance was Nagelkerke R2 = 0.39 (see Table 2).
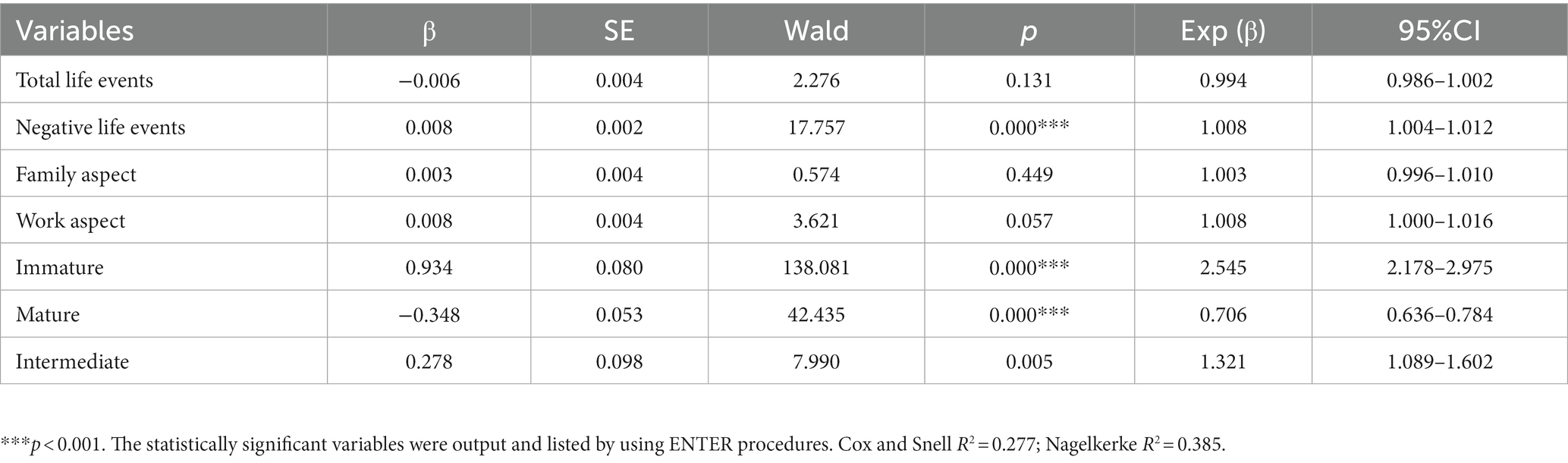
Table 2. Logistic regression analyses to predict depression.
3.3 Correlations between NLEs and DSQ
Pearson correlation analysis showed that the score of NLEs was significantly and positively correlated with immature defense mechanisms (r = 0.363, p < 0.05), intermediate defense mechanisms (r = 0.187, p < 0.05), and negatively with mature defense mechanisms (r = −0.061, p < 0.05) (see Table 3).
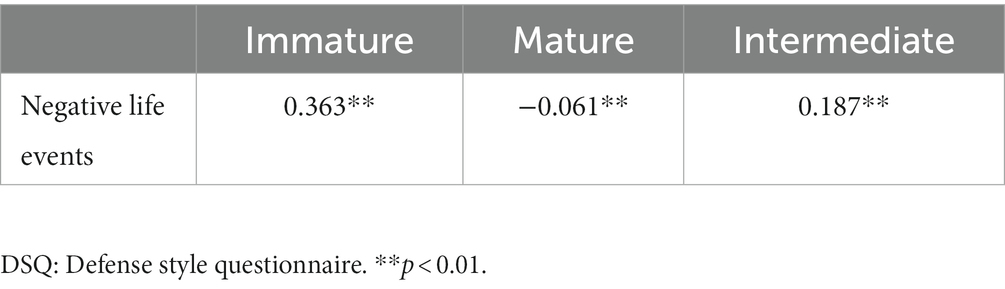
Table 3. Correlations between negative life events and DSQ.
3.4 The mediating role of defense mechanisms
The overall model accounted for a significant 40.2% of the variance in depressive symptoms, F (7, 2,739) = 262.680, p < 0.001, R2 = 0.402.
NLEs was directly related to depressive symptoms (b = 0.010, p < 0.001), and significant indirect effect via immature defense mechanisms (b = 0.008, p < 0.001), mature defense mechanisms (b = 0.001, p < 0.001) and intermediate defense mechanisms (b = 0.001, p < 0.001) were observed. The mediate effect of immature defense mechanisms was significantly higher than that of mature defense mechanisms and intermediate defense mechanisms. But there is no significant difference in mediating effect between mature defense mechanisms and intermediate defense mechanisms (see Figure 1 and Table 4).
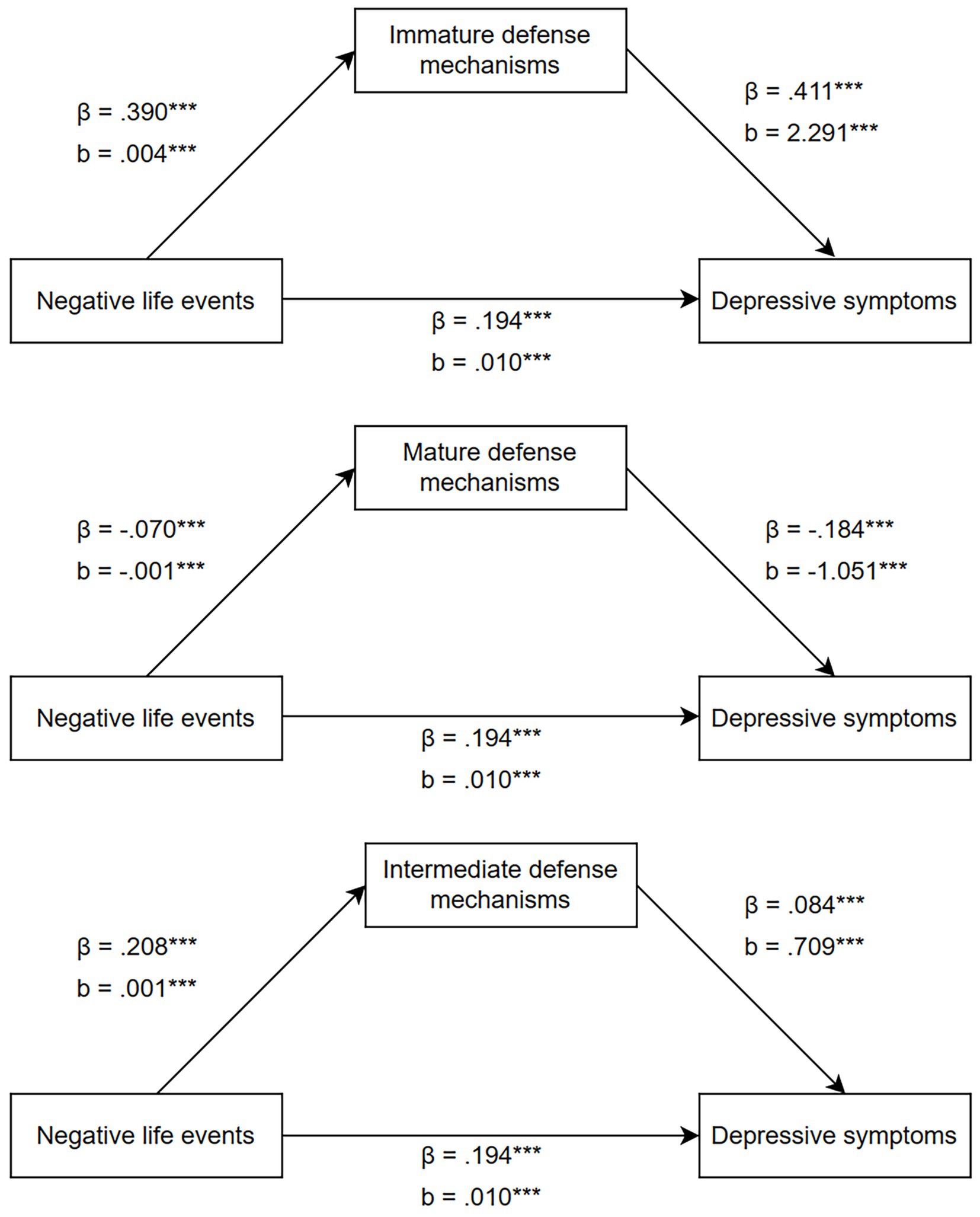
Figure 1. A structural equation model with direct and indirect effects between negative life events, defense mechanisms, and depressive symptoms. The effects of gender, age and diagnosis were controlled in the model. β: Standardized beta regression coefficient; b: Unstandardized beta regression coefficient. *** p < 0.001.
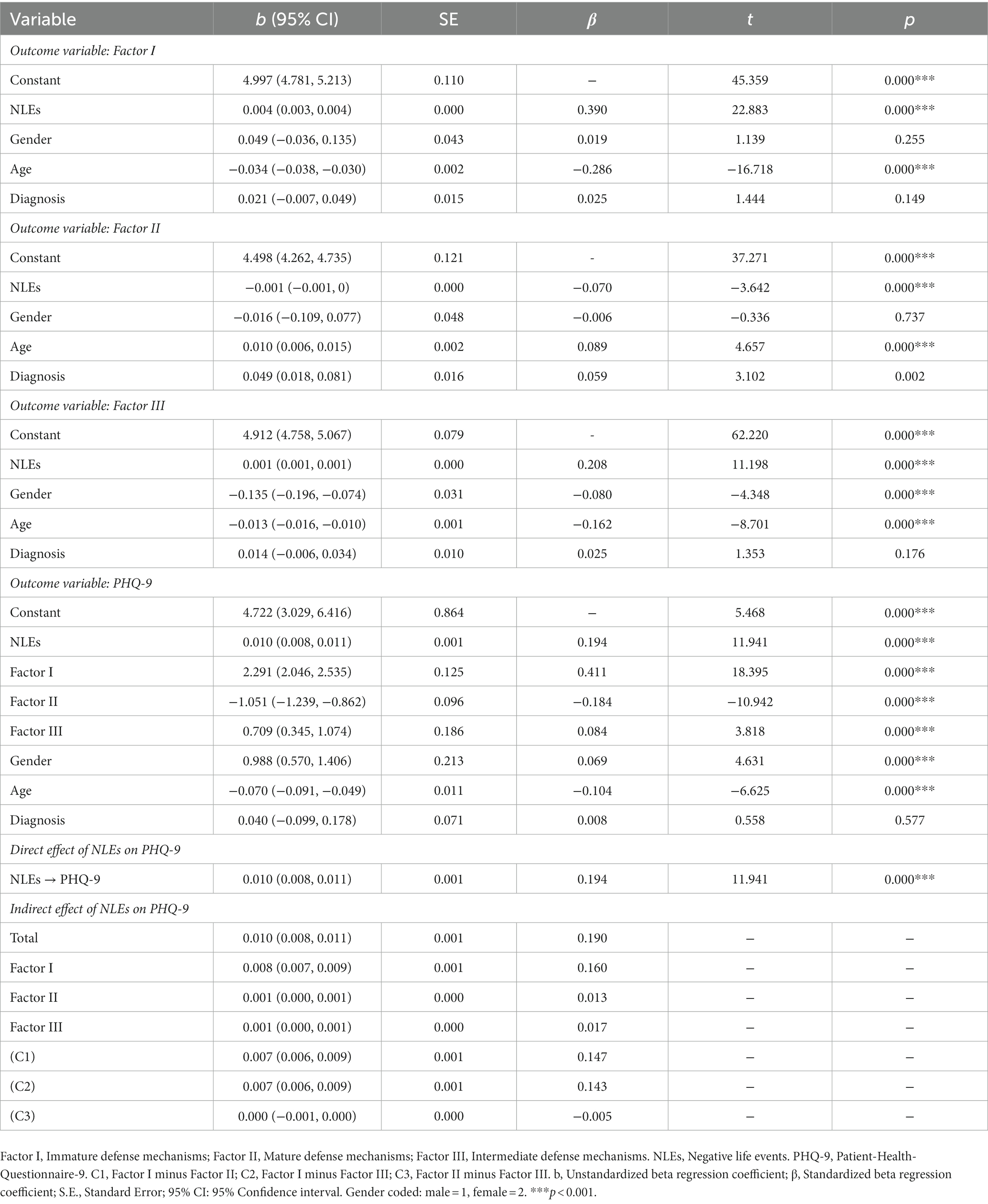
Table 4. Unstandardized and standardized coefficients for all variables in the tested models.
4 Discussion
In 2019, one paper published in JAMA had illustrated the ability of PHQ-9 to screen for and monitor depression, and the most common recommended positive case threshold was 10 points (38). Xiong et al. (31) found that the optimal cutoff point for detecting depression with PHQ-9 in the Chinese population is 10. In the present study, we divided all participants into two groups (depression group and non-depression group) according to the 10 score of PHQ-9. Our results showed that depression is more common among young women. This is consistent with the findings of an epidemiological study of DSM-5 major depressive disorder in adults in the United States (39).
4.1 LEs and depression
We observed that the LEs total scores and all LEs sub-scores (except for PLEs) were associated with depression. Logistic regression also showed that the NLEs score was the predictor of depression. Previous studies have consistently documented the impact of NLEs on the onset, remission, and recurrence of depression (16, 40, 41). Few studies have focused on the impact of PLEs on depressive symptoms, and the evidence is inconsistent (11, 16). One view has suggested that PLEs can directly or indirectly reduce depressive symptoms by buffering the effects of NLEs (42), while another view posits that PLEs themselves are also a source of stress (14, 43). In our present study, we did not find significant differences in PLEs between depressed and non-depressed patients. According to the content of the event, LEs can be divided into three dimensions: family life; work and study; social and other aspects. Similar to findings of other studies, we found all these three dimensions of LEs were related to depression (13, 44).
4.2 Defense mechanisms and depression
Our finding suggested that patients with depression are more likely to use immature and intermediate defense mechanisms, and less likely to use mature defense mechanisms, which is consistent with the case–control study by Peng et al. (45) conducted in populations with depression and non-suicidal self-injury. Accumulating literatures suggest that depressed patients mainly tend to use immature defense mechanisms (46, 47). As the symptoms of depression improve, patients show an increase in adaptive and a decrease in immature defenses (25). This suggest the influence of depression on defense mechanisms.
4.3 The mediate effect of defense mechanisms
Although the relationship between depression and NLEs has been established, the mediators of the link were not clear. Based on the above findings, we hypothesized that defense mechanisms may play a mediating role between NLEs and depressive symptoms. We found that immature defense mechanisms play a predominant mediating role. Similar to previous studies, Wang et al. (28) found that immature defense mechanisms had a significant mediate effect on the onset of bipolar disorder through childhood trauma in 86 patients with bipolar disorder and 43 healthy controls. In the study by Finzi-Dottan et al. (29) with 196 undergraduate students, immature defense mechanisms played a mediating role in the association between childhood emotional abuse and psychopathological symptoms. We also found the mediate effect of mature defense mechanisms and intermediate defense mechanisms in the relationship between NLEs and depressive symptoms, but significantly lower than that of immature defenses.
A study conducted by Araujo et al. (27) among 87 female adolescent patients found that immature defense mechanisms are related to life stressors. More sources of life stress are significantly positively correlated with an increase in the use of immature defense mechanisms. Accumulating evidence has converged to suggest that the increasing usage of immature defenses mechanisms may be associated with the severity of depression, increased risk of suicide attempts, reduced treatment compliance, and more treatment related adverse responses (48–50). Excessive use of immature defenses may cause serious damage to interpersonal and professional relationships, leading to severe psychological pain and worsening of psychopathological symptoms (25, 51). NLEs reflects perceived stressfulness, and the use of immature defense mechanisms reflects individual maladaptation.
From a psychodynamic perspective of view, defense mechanisms can be seen as part of ego function. Ego function has a basic level and can be influenced by other factors, such as psychopathology and stress, which can reduce ego function. But ego function can also mediate one’s ability to deal with stress and influence psychopathology (24). Thus, they have a bidirectional relationship with each other. In psychodynamic therapy, it is important to strengthen ego function in patients with a structural damage (a low basic level of ego function) and in patients with reduced ego function under stress and psychopathology.
In summary, we found that immature defense mechanisms and NLEs might be an important risk factor for depression. And defense mechanisms play a mediating role in the relationship between NLEs and depressive symptoms. These findings confirm the importance of NLEs and defense mechanisms in depression. Helping patients improving defense mechanisms and dealing with NLEs may be of great help in the treatment of relevant patients.
4.4 Limitations
The present study has the following limitations: (1) This study is a cross-sectional study and cannot reflect the causal effects between factors. (2) We used a self-assessment scale to screen patients with depression as a large-scale clinical study. (3) The control group was also patients from the department of psychological medicine, which may be influenced by confounding factors.
5 Conclusion
Immature defense mechanisms play an important mediating role in the relationship between NLEs and depressive symptoms. Helping patients improving defense mechanisms and dealing with NLEs may be of great help in the treatment of relevant patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Peking Union Medical College Hospital (PUMCH). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DM: Writing – original draft. JC: Writing – review & editing. JW: Writing – review & editing. JJ: Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-B-093) and the National Nature Science Foundation of China (T2341003). The supporter had no role in the design, analysis, interpretation, or publication of this study.
Acknowledgments
The authors would like to thank all participants at Peking Union Medical College Hospital for their participation in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1341288/full#supplementary-material
References
1. Barry, MJ, Nicholson, WK, Silverstein, M, Chelmow, D, Coker, TR, Davidson, KW, et al. Screening for depression and suicide risk in adults. JAMA. (2023) 329:2057. doi: 10.1001/jama.2023.9297
2. Thapar, A, Eyre, O, Patel, V, and Brent, D. Depression in young people. Lancet. (2022) 400:617–31. doi: 10.1016/s0140-6736(22)01012-1
3. Rice, F, Sellers, R, Hammerton, G, Eyre, O, Bevan-Jones, R, Thapar, AK, et al. Antecedents of new-onset major depressive disorder in children and adolescents at high familial risk. JAMA Psychiatry. (2017) 74:153–60. doi: 10.1001/jamapsychiatry.2016.3140
4. Weavers, B, Heron, J, Thapar, AK, Stephens, A, Lennon, J, Bevan Jones, R, et al. The antecedents and outcomes of persistent and remitting adolescent depressive symptom trajectories: a longitudinal, population-based English study. Lancet Psychiatry. (2021) 8:1053–61. doi: 10.1016/s2215-0366(21)00281-9
5. Warrier, V, Kwong, ASF, Luo, M, Dalvie, S, Croft, J, Sallis, HM, et al. Gene-environment correlations and causal effects of childhood maltreatment on physical and mental health: a genetically informed approach. Lancet Psychiatry. (2021) 8:373–86. doi: 10.1016/s2215-0366(20)30569-1
6. Rutter, M. Some of the complexities involved in gene-environment interplay. Int J Epidemiol. (2015) 44:1128–9. doi: 10.1093/ije/dyv054
7. Yarrington, JS, Metts, AV, Zinbarg, RE, Nusslock, R, Wolitzky-Taylor, K, Hammen, CL, et al. The role of positive and negative aspects of life events in depressive and anxiety symptoms. Clin Psychol Sci. (2023) 11:910–20. doi: 10.1177/21677026221141654
8. Kendler, KS, Karkowski, LM, and Prescott, CA. Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry. (1999) 156:837–41. doi: 10.1176/ajp.156.6.837
9. Buckman, JEJ, Saunders, R, Arundell, LL, Oshinowo, ID, Cohen, ZD, O'Driscoll, C, et al. Life events and treatment prognosis for depression: a systematic review and individual patient data meta-analysis. J Affect Disord. (2022) 299:298–308. doi: 10.1016/j.jad.2021.12.030
10. Horesh, N, Klomek, AB, and Apter, A. Stressful life events and major depressive disorders. Psychiatry Res. (2008) 160:192–9. doi: 10.1016/j.psychres.2007.06.008
11. Blonski, SC, Conradi, HJ, Oldehinkel, AJ, Bos, EH, and de Jonge, P. Associations between negative and positive life events and the course of depression. J Nerv Ment Dis. (2016) 204:175–80. doi: 10.1097/nmd.0000000000000445
12. Ruan, H, Shen, K, and Chen, F. Negative life events, social ties, and depressive symptoms for older adults in China. Front Public Health. (2021) 9:774434. doi: 10.3389/fpubh.2021.774434
13. Mazure, CM. Life stressors as risk factors in depression. Clin Psychol Sci Pract. (1998) 5:291–13. doi: 10.1111/j.1468-2850.1998.tb00151.x
14. Shahar, G, and Priel, B. Positive life events and adolescent emotional distress: in search of protective-interactive processes. J Soc Clin Psychol. (2002) 21:645–68. doi: 10.1521/jscp.21.6.645.22798
15. Khazanov, GK, Ruscio, AM, and Swendsen, J. The "brightening" effect: reactions to positive events in the daily lives of individuals with major depressive disorder and generalized anxiety disorder. Behav Ther. (2019) 50:270–84. doi: 10.1016/j.beth.2018.05.008
16. Spinhoven, P, Elzinga, BM, Hovens, JGFM, Roelofs, K, van Oppen, P, Zitman, FG, et al. Positive and negative life events and personality traits in predicting course of depression and anxiety. Acta Psychiatr Scand. (2011) 124:462–73. doi: 10.1111/j.1600-0447.2011.01753.x
17. Davidson, L, Shahar, G, Lawless, MS, Sells, D, and Tondora, J. Play, pleasure, and other positive life events: “non—specific” factors in recovery from mental illness? Psychiatry. (2006) 69:151–63. doi: 10.1521/psyc.2006.69.2.151
18. Colodro-Conde, L, Couvy-Duchesne, B, Zhu, G, Coventry, WL, Byrne, EM, Gordon, S, et al. A direct test of the diathesis-stress model for depression. Mol Psychiatry. (2018) 23:1590–6. doi: 10.1038/mp.2017.130
19. Jun, JY, Lee, YJ, Lee, SH, Yoo, SY, Song, J, and Kim, SJ. Association between defense mechanisms and psychiatric symptoms in north Korean refugees. Compr Psychiatry. (2015) 56:179–87. doi: 10.1016/j.comppsych.2014.10.001
20. Freud, S. The neuro-psychosis of defense (the standard edition of the complete psychological works of Sigmund Freud). London: The Hogarth Press and the Institute of Psycho-Analysis (1894).
21. Association AP. Diagnostic and statistical manual of mental disorders, DSM-IV. 4th ed. Washington, DC: American Psychiatric Association (1994).
22. Bond, M. Empirical studies of defense style: relationships with psychopathology and change. Harv Rev Psychiatry. (2004) 12:263–78. doi: 10.1080/10673220490886167
23. Babl, A, Grosse Holtforth, M, Perry, JC, Schneider, N, Dommann, E, Heer, S, et al. Comparison and change of defense mechanisms over the course of psychotherapy in patients with depression or anxiety disorder: evidence from a randomized controlled trial. J Affect Disord. (2019) 252:212–20. doi: 10.1016/j.jad.2019.04.021
24. da Silva, MR, Vieira, IS, Scaini, C, Molina, ML, Barbosa, LP, da Silva, GDG, et al. Ego-defense mechanisms and brief psychotherapies for the management of major depressive disorder in adults: a longitudinal and quasi-experimental study. J Affect Disord. (2023) 330:291–9. doi: 10.1016/j.jad.2023.02.141
25. Babl, A, Berger, T, Grosse Holtforth, M, Taubner, S, Caspar, F, and Gómez Penedo, JM. Disentangling within- and between-patient effects of defensive functioning on psychotherapy outcome using mixed models. Psychother Res J Soc Psychother Res. (2020) 30:1088–00. doi: 10.1080/10503307.2019.1690714
26. Dorpat, T. L the development of defense mechanisms: theory, research, and assessment by Phebe Cramer New York: springer-Verlag, 1991, xiii+. J Psychoanalytic Books. (1993) 4:405–7.
27. Araujo, K, Ryst, E, and Steiner, H. Adolescent defense style and life stressors. Child Psychiatry Hum Dev. (1999) 30:19–28. doi: 10.1023/a:1022666908235
28. Wang, L, Yin, Y, Bian, Q, Zhou, Y, Huang, J, Zhang, P, et al. Immature defense mechanisms mediate the relationship between childhood trauma and onset of bipolar disorder. J Affect Disord. (2021) 278:672–7. doi: 10.1016/j.jad.2020.10.029
29. Finzi-Dottan, R, and Karu, T. From emotional abuse in childhood to psychopathology in adulthood: a path mediated by immature defense mechanisms and self-esteem. J Nerv Ment Dis. (2006) 194:616–21. doi: 10.1097/01.nmd.0000230654.49933.23
30. Kroenke, K, Spitzer, RL, and Williams, JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
31. Xiong, N, Fritzsche, K, Wei, J, Hong, X, Leonhart, R, Zhao, X, et al. Validation of patient health questionnaire (PHQ) for major depression in Chinese outpatients with multiple somatic symptoms: a multicenter cross-sectional study. J Affect Disord. (2015) 174:636–43. doi: 10.1016/j.jad.2014.12.042
32. Yang, J, Ke, S, Qiao, Z, Yang, X, Qiu, X, Song, X, et al. Interactions between glycogen synthase kinase-3β gene polymorphisms, negative life events, and susceptibility to major depressive disorder in a Chinese population. Front Psych. (2020) 11:503477. doi: 10.3389/fpsyt.2020.503477
33. Xiong, N, Liu, Q, Lv, X, Leonhart, R, Tian, H, et al. Demographic and psychosocial variables could predict the occurrence of major depressive disorder, but not the severity of depression in patients with first-episode major depressive disorder in China. J Affect Disord. (2020) 274:103–11. doi: 10.1016/j.jad.2020.05.065
34. Bond, M, Gardner, ST, Christian, J, and Sigal, JJ. Empirical study of self-rated defense styles. Arch Gen Psychiatry. (1983) 40:333–8. doi: 10.1001/archpsyc.1983.01790030103013
35. Wang, Y-L, Wang, J-R, Huang, B-L, Yang, X-H, Guo, H-R, and Ren, Y-M. Changes in the psychological defense mechanism and clinical features of patients with OCD – a four-year follow-up study. J Affect Disord. (2022) 317:131–5. doi: 10.1016/j.jad.2022.08.031
36. Ma, H, Li, M, Zhang, L, Tao, J, and Zhu, G. Association of Neurotensin Receptor 1 gene polymorphisms with defense mechanisms in healthy Chinese. Front Psych. (2021) 12:762276. doi: 10.3389/fpsyt.2021.762276
37. Hayes, AF. Mediation, moderation, and conditional process analysis. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford Publications (2013).
38. Zimmerman, M. Using the 9-item patient health questionnaire to screen for and monitor depression. JAMA. (2019) 322:2125–6. doi: 10.1001/jama.2019.15883
39. Hasin, DS, Sarvet, AL, Meyers, JL, Saha, TD, Ruan, WJ, Stohl, M, et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. (2018) 75:336–46. doi: 10.1001/jamapsychiatry.2017.4602
40. Monroe, SM, Slavich, GM, and Georgiades, K. The social environment and life stress in depression. J Handb Dep. (2009) 2:340–60.
41. Wardenaar, KJ, van Veen, T, Giltay, EJ, Zitman, FG, and Penninx, BW. The use of symptom dimensions to investigate the longitudinal effects of life events on depressive and anxiety symptomatology. J Affect Disord. (2014) 156:126–33. doi: 10.1016/j.jad.2013.12.004
42. Haeffel, GJ, and Vargas, I. Resilience to depressive symptoms: the buffering effects of enhancing cognitive style and positive life events. J Behav Ther Exp Psych. (2011) 42:13–8. doi: 10.1016/j.jbtep.2010.09.003
43. Madhavan, S, Stewart, LC, Birk, SL, Nielsen, JD, and Olino, TM. Positive and negative life events in association with psychopathology: an examination of sex differences in early adolescence. Child Psychiatry Hum Dev. (2023) 1–10. doi: 10.1007/s10578-023-01509-w
44. Liu, L, Liu, C, Ke, X, and Li, N. Mediating effect of social support on the association between life events and depression. Medicine. (2020) 99:e22627. doi: 10.1097/md.0000000000022627
45. Peng, B, Liao, J, Li, Y, Jia, G, Yang, J, Wu, Z, et al. Personality characteristics, defense styles, borderline symptoms, and non-suicidal self-injury in first-episode major depressive disorder. Front Psychol. (2023) 14:711. doi: 10.3389/fpsyg.2023.989711
46. Martino, G, Caputo, A, Bellone, F, Quattropani, MC, and Vicario, CM. Going beyond the visible in type 2 diabetes mellitus: defense mechanisms and their associations with depression and health-related quality of life. Front Psychol. (2020) 11:267. doi: 10.3389/fpsyg.2020.00267
47. Blaya, C, Dornelles, M, Blaya, R, Kipper, L, Heldt, E, Isolan, L, et al. Do defense mechanisms vary according to the psychiatric disorder? Revista brasileira de psiquiatria. (2006) 28:179–83. doi: 10.1590/s1516-44462006000300007
48. Fitzpatrick, T. Primitive defenses and unilateral termination of psychotherapy: Are the lerner defense scales useful in predicting premature termination in psychotherapy? Duquesne: U.S. Duquesne University (2014).
49. Vaillant, GE. Ego mechanisms of defense: A guide for clinicians and researchers, Washington, DC: U.S. American Psychiatric Pub (1992).
50. Laaksonen, MA, Sirkiä, C, Knekt, P, and Lindfors, O. Self-reported immature defense style as a predictor of outcome in short-term and long-term psychotherapy. J. Brain Behav. (2014) 4:495–03. doi: 10.1002/brb3.190
Keywords: life events, defense mechanisms, depression, mediate, psychosomatic
Citation: Ma D, Cao J, Wei J and Jiang J (2024) Immature defense mechanisms mediate the relationship between negative life events and depressive symptoms. Front. Psychiatry. 14:1341288. doi: 10.3389/fpsyt.2023.1341288
Edited by:
Stephan Zipfel, University of Tübingen, GermanyReviewed by:
Isheeta Zalpuri, Stanford University, United StatesHirofumi Hirakawa, Oita University, Japan
Copyright © 2024 Ma, Cao, Wei and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinya Cao, Y2FvamlueWFAcHVtY2guY24=; Jing Wei, d2VpamluZ0BwdW1jaC5jbg==