
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Psychiatry , 18 December 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1307277
This article is part of the Research Topic Community Series In Mental-Health-Related Stigma and Discrimination: Prevention, Role, and Management Strategies, volume II View all 23 articles
 Leila Kamalzadeh1
Leila Kamalzadeh1 Renato de Filippis2†
Renato de Filippis2† Samer El Hayek3
Samer El Hayek3 Mohsen Heidari Mokarar4
Mohsen Heidari Mokarar4 Chonnakarn Jatchavala5
Chonnakarn Jatchavala5 Eugene Boon Yau Koh6
Eugene Boon Yau Koh6 Amine Larnaout7,8
Amine Larnaout7,8 Isa Multazam Noor9,10
Isa Multazam Noor9,10 Margaret Isioma Ojeahere11
Margaret Isioma Ojeahere11 Laura Orsolini12
Laura Orsolini12 Mariana Pinto da Costa13,14
Mariana Pinto da Costa13,14 Ramdas Ransing15Mohammad Amin Sattari4
Ramdas Ransing15Mohammad Amin Sattari4 Mohammadreza Shalbafan16*†
Mohammadreza Shalbafan16*†In the realm of mental health care, the placement and organization of facilities have long been intrinsically linked to prevailing societal and cultural attitudes and the persistent stigma surrounding mental illness (1). Psychiatric hospitals, known as “asylums”, were often located in remote areas due to safety concerns, driven in part by misconceptions and stigma (2). The mid-twentieth century marked the emergence of the deinstitutionalization movement, aimed to reintegrate patients with mental illnesses into the community by placing mental health facilities within or close to urban areas and providing community mental health care (3). Despite these positive movements, traces of stigma continue to influence the geographical positioning and structure of mental care facilities (4). We synthesized the viewpoints of some Early Career Psychiatrists (ECPs) Section members from the World Psychiatric Association (WPA) (5), who were within the age bracket of 30–47 years. Our inquiry aimed to examine the influence of stigma on the location and configuration of mental health establishments, as well as its effects on the professional identities and levels of job satisfaction among psychiatrists. This exploration spanned across 10 distinct national contexts, including: India, Indonesia, Iran, Italy, Lebanon, Malaysia, Nigeria, Thailand, Tunisia, and the United Kingdom, as summarized in Tables 1A, B. We also provided recommendations for improving the quality and accessibility of mental health care.
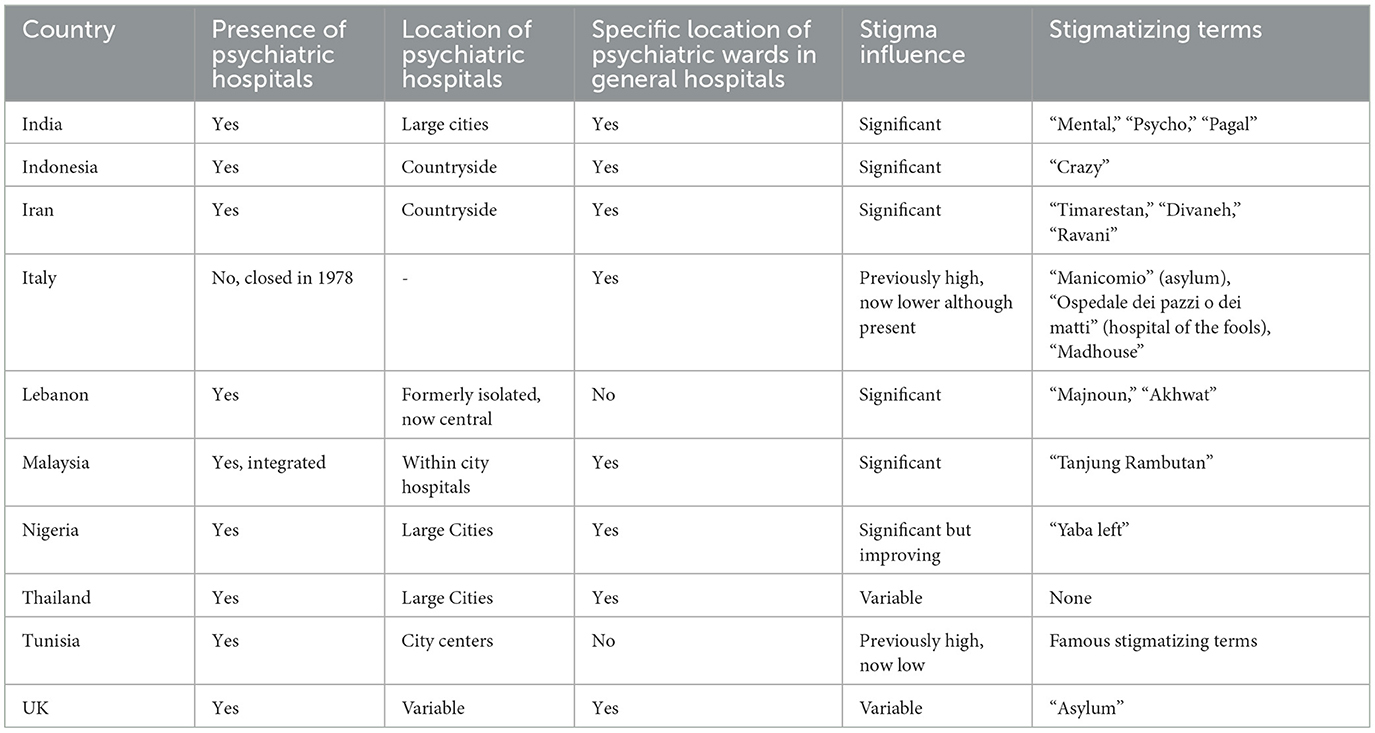
Table 1A. Presence and location of psychiatric facilities and stigma.
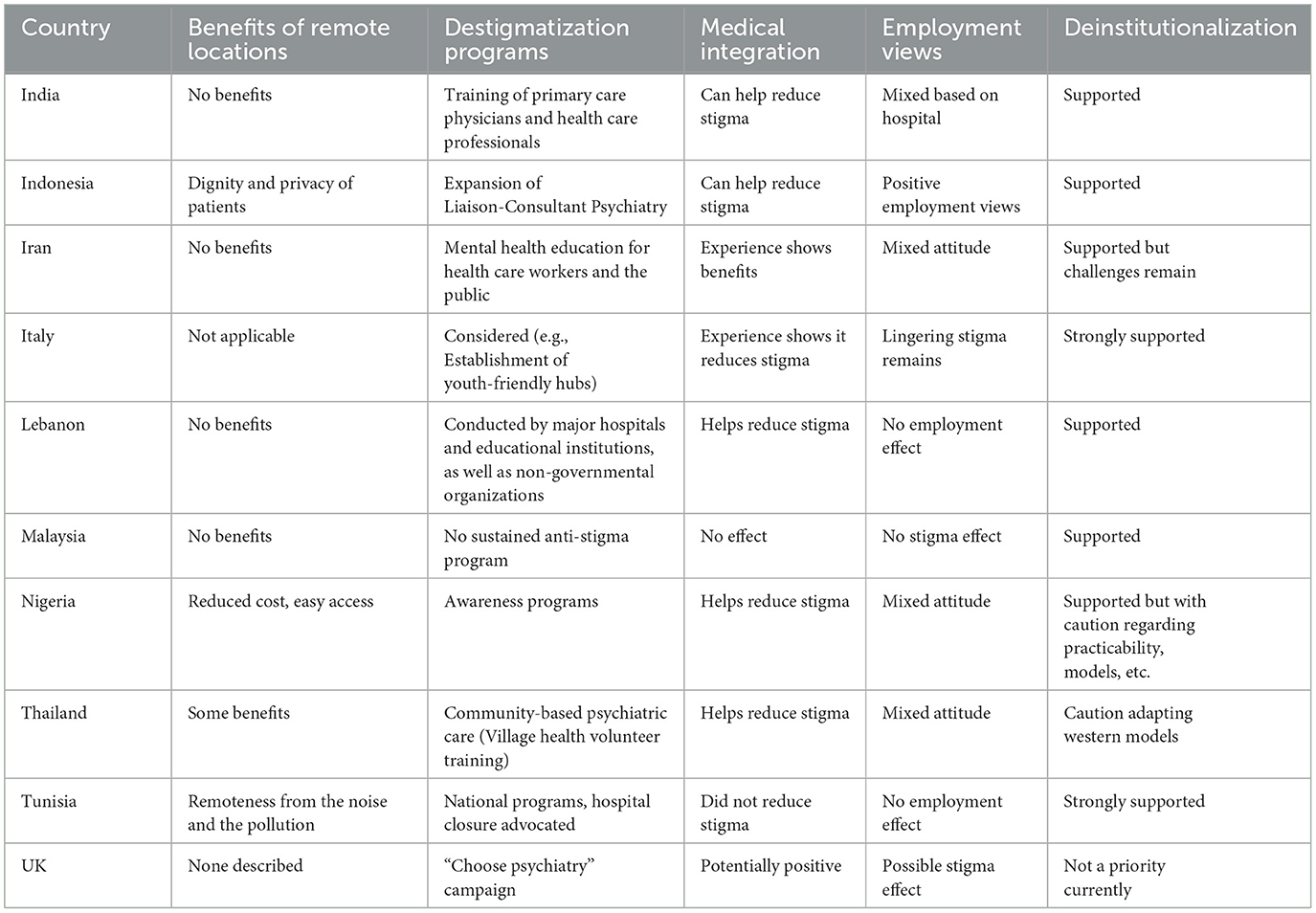
Table 1B. Programs, integration, and views on psychiatric care.
In most of the countries where we collected the views of psychiatrists, standalone psychiatric hospitals still comprise a significant portion of psychiatric beds, with diverse geographical distribution patterns influenced by factors such as population density, urbanization, and healthcare infrastructure. However, the specter of stigma noticeably affects the geographic placement of psychiatric facilities in various nations. For instance, Indonesia and Iran have predominantly located their psychiatric hospitals in the countryside. This choice stems from misconceptions about mental illness, with the assumption that remote locations with stringent security measures will prevent patients from wandering or posing threats to the community (6, 7). Conversely, in places like India, Tunisia, Lebanon, and Nigeria, psychiatric hospitals are predominantly situated in large urban centers. Malaysia initially constructed psychiatric hospitals in suburban areas but later shifted them to city centers with urban expansion. The UK and Thailand exhibit variable rural and urban placement patterns, while Italy underwent significant transformations due to anti-stigma efforts initiated by “Basaglia's Law” in 1978, resulting in the closure of psychiatric asylums (usually located in peripheral areas), the organization of psychiatric assistance through the creation of territorial psychiatry departments and the integration of psychiatry wards (with a limited number of bed seats) for the management of acute phases of psychiatric diseases, within general hospitals in medium and large cities (8).
On a more positive note, some psychiatrists highlighted potential benefits of locating psychiatric hospitals in areas distant from urban centers. These benefits include reduced exposure to urban noise and pollution and reduced transport costs for individuals residing in rural areas. Additionally, the case of the Aro Village Project in Nigeria was mentioned. This innovative initiative, led by Prof. Thomas Adeoye Lambo, established a community-based mental health care system that prioritized affordability, accessibility, and cultural appropriateness. The project involved villagers in the accommodation and treatment of psychiatric patients, integrating family members and traditional healers into the care process. This initiative transformed social perceptions of madness and evolved from a rural mental hospital into a community situated in an urban center (9).
Regarding the placement of psychiatric units or wards within general hospitals, over half of the respondents reported that psychiatric wards in their respective countries were situated in specific locations, such as separate buildings, lower floors, or isolated wings. These wards often feature specialized facilities, security measures, and unique ward architecture, including closed walls and security guards. While these security measures primarily aim to ensure patient safety and prevent suicides, this segregation inadvertently perpetuates stigma by communicating separation between physical and mental healthcare. Patients' restricted access to outdoor spaces due to security concerns fosters feelings of isolation and marginalization. Moreover, disparities in resource allocation are observed, with specialists from other fields often exhibiting a negative view or even fear of psychiatric patients. In some cases, these specialists refuse to accept patients with psychiatric disorders into their departments.
Many countries still use stigmatizing terms for psychiatric hospitals, wards, or locations. Terms like “crazy” and “psycho” label patients, while references to “asylums” further perpetuate institutional stigma. For example, “Tanjung Rambutan” is the location of Malaysia's first psychiatric hospital, but it is also used as a derogatory and discriminatory term for someone who is not accepted and should be locked up in an asylum. Similarly, some countries, like Thailand, consistently use “neuro” instead of “psycho” (or neuro-psycho) in official terms, hospitals, and institutes (10). Such stigmatizing terminology may reflect and reinforce societal prejudice (11).
Opinions on the establishment of medical inpatient wards or outpatient clinics of various specialties, such as neurology, internal medicine, or emergency care, within psychiatric hospitals as means to reduce stigma diverged. Some believed that such integration reduced stigma by fostering frequent interactions between psychiatrists and non-psychiatry practitioners, challenging stereotypes and discrimination. However, others argued that stigma persisted across various fields, often stemming from professionals' own understanding of mental illness.
Perspectives varied on how stigma associated with psychiatric hospitals affects psychiatrists' employment choices. Some observed willingness among younger generations to foster positive change through such positions. However, stigma appears to deter others from these career paths. Improved infrastructure can increase desirability of psychiatric hospital employment. Overall, individual attitudes likely involve multiple factors like past training experiences and job availability.
Psychiatrists also highlighted the implementation of destigmatization initiatives in their regions. These efforts encompassed the expansion of Liaison-Consultant Psychiatry, the establishment of off-site centers for adolescents with mental distress, the training of primary care physicians and specialists from various fields, the introduction of CBT-based anti-stigma programs for caregivers of psychiatric patients, and initiatives to raise awareness about mental health issues among children, and youths. Additionally, community-based psychiatric care programs involving Village Health Volunteers (VHVs) were mentioned. However, despite these endeavors, the absence of comprehensive, sustainable, and long-term destigmatization programs, coupled with financial constraints and inadequate support from authorities, remains a significant challenge in this regard.
Respondents' opinions on the deinstitutionalization movement also vary. Many express supports for deinstitutionalization, citing reasons such as reducing stigma, increasing access to care, respecting patient preferences, enhancing family and social support, and saving costs. Some mention that modern mental health hospitals offering high-quality services may render deinstitutionalization less urgent. Others emphasize the importance of considering social welfare and contextual culture when implementing deinstitutionalization.
In summary, despite notable advancements in the deinstitutionalization movement and the incorporation of mental health care into mainstream healthcare systems, the enduring impact of stigma continues to shape the placement and structure of psychiatric facilities. It is crucial to acknowledge and actively address these persistent stigmatizing influences to ensure comprehensive and inclusive healthcare for individuals with psychiatric disorders, thereby enhancing their wellbeing and alleviating the societal burden of mental illness. Future research and policy endeavors should prioritize the dismantling of these barriers and the cultivation of a more compassionate and integrated approach to mental health care. A balanced strategy is recommended: (1) Foster the development of accessible community-based care by allocating adequate resources and implementing anti-stigma initiatives; (2) In cases where psychiatric hospitals are still deemed necessary, introduce internal destigmatization programs while concurrently devising transitional plans to gradually shift toward community-based models when sustainability allows.
LK: Conceptualization, Data curation, Investigation, Project administration, Writing—original draft. RdF: Conceptualization, Data curation, Writing—review & editing. SE: Conceptualization, Data curation, Writing—review & editing. MH: Data curation, Writing—review & editing. CJ: Data curation, Writing—review & editing. EK: Data curation, Writing—review & editing. AL: Data curation, Writing—review & editing. IN: Data curation, Writing—review & editing. MO: Data curation, Writing—review & editing. LO: Data curation, Writing—review & editing. MP: Conceptualization, Data curation, Supervision, Writing—review & editing. RR: Data curation, Writing—review & editing. MAS: Data curation, Writing—review & editing. MS: Conceptualization, Data curation, Investigation, Project administration, Supervision, Writing—review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bil JS. Stigma and architecture of mental health facilities. Br J Psychiatry. (2016) 208:499–500. doi: 10.1192/bjp.208.5.499b
2. Reports. Joint Action on Mental Health and Welbeing: Towards Community-based and Socially Inclusive Mental Health Care. Lisbon: Saúde Mental (2015). p. 1–341. Available online at: http://www.app.com.pt/relatorio-nacional-e-u-joint-action-mental-health-versao-portuguesa
3. George P, Jones N, Goldman H, Rosenblatt A. Cycles of reform in the history of psychosis treatment in the United States. SSM Mental Health. (2023) 3:100205. doi: 10.1016/j.ssmmh.2023.100205
4. Fulone I, Barreto JOM, Barberato-Filho S, Bergamaschi CC, Silva MT, Lopes LC. Improving care for deinstitutionalized people with mental disorders: experiences of the use of knowledge translation tools. Front Psychiatry. (2021) 12:575108 doi: 10.3389/fpsyt.2021.575108
5. Pinto da Costa M. Early career psychiatrists – history, 2020 and beyond. World Psychiatry. (2020) 19:127–8. doi: 10.1002/wps.20712
6. Hartini N, Fardana NA, Ariana AD, Wardana ND. Stigma toward people with mental health problems in Indonesia. Psychol Res Behav Manag. (2018) 11:535–41. doi: 10.2147/PRBM.S175251
7. Taghva A. Strategies to reduce the stigma toward people with mental disorders in Iran based on stakeholders view: a qualitative study. Eur Psychiatry. (2017) 17:17. doi: 10.1186/s12888-016-1169-y
8. Foot J. Franco Basaglia and the radical psychiatry movement in Italy, 1961–78. Crit Radic Soc Work. (2014) 2:235–49. doi: 10.1332/204986014X14002292074708
9. Nabel E. Advancing clinical care and medical understanding in a resource-limited setting: lessons from the aro village project in the wake of the affordable care act. Am J Psychiatry Resid J. (2017) 12:5–7. doi: 10.1176/appi.ajp-rj.2017.120602
10. Jatchavala C. Discourse and stigmatization of psychiatric disorder in Thailand. J Sociol Anthropol. (2013) 1:93–113.
Keywords: mental health, mental disorders, psychiatry, art, social stigma, health facilities, psychiatric hospital
Citation: Kamalzadeh L, de Filippis R, El Hayek S, Heidari Mokarar M, Jatchavala C, Koh EBY, Larnaout A, Noor IM, Ojeahere MI, Orsolini L, Pinto da Costa M, Ransing R, Sattari MA and Shalbafan M (2023) Impact of stigma on the placement of mental health facilities: insights from early career psychiatrists worldwide. Front. Psychiatry 14:1307277. doi: 10.3389/fpsyt.2023.1307277
Received: 04 October 2023; Accepted: 08 November 2023;
Published: 18 December 2023.
Edited by:
Ricardo Gusmão, University of Porto, PortugalReviewed by:
Gaia Sampogna, University of Campania “L. Vanvitelli”, ItalyCopyright © 2023 Kamalzadeh, de Filippis, El Hayek, Heidari Mokarar, Jatchavala, Koh, Larnaout, Noor, Ojeahere, Orsolini, Pinto da Costa, Ransing, Sattari and Shalbafan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammadreza Shalbafan, c2hhbGJhZmFuLm1yQGl1bXMuYWMuaXI=
†ORCID: Renato de Filippis orcid.org/0000-0001-6928-1224
Mohammadreza Shalbafan orcid.org/0000-0002-4536-3441
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.