
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 24 October 2023
Sec. Mood Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1291176
This article is part of the Research Topic Treatment Resistant Depression (TRD): epidemiology, clinic, burden and treatment View all 23 articles
 Emiliana Mancuso
Emiliana Mancuso Gaia SampognaAlessia BoianoBianca Della Rocca
Gaia SampognaAlessia BoianoBianca Della Rocca Matteo Di VincenzoMaria Vita Lapadula
Matteo Di VincenzoMaria Vita Lapadula Flavia MartinelliFederico Lucci
Flavia MartinelliFederico Lucci Mario Luciano*
Mario Luciano*Introduction: Many patients fail to respond to multiple antidepressant interventions, being defined as “treatment-resistant depression” (TRD) patients. TRD is usually associated with increased severity and chronicity of symptoms, increased risk of comorbidity, and higher suicide rates, which make the clinical management challenging. Efforts to distinguish between TRD patients and those who will respond to treatment have been unfruitful so far. Several studies have tried to identify the biological, psychopathological, and psychosocial correlates of depression, with particular attention to the inflammatory system. In this paper we aim to review available studies assessing the full range of biomarkers in TRD patients in order to reshape TRD definition and improve its diagnosis, treatment, and prognosis.
Methods: We searched the most relevant medical databases and included studies reporting original data on possible biomarkers of TRD. The keywords “treatment resistant depression” or “TRD” matched with “biomarker,” “inflammation,” “hormone,” “cytokine” or “biological marker” were entered in PubMed, ISI Web of Knowledge and SCOPUS databases. Articles were included if they included a comparison with healthy controls (HC).
Results: Of the 1878 papers identified, 35 were included in the present study. Higher plasma levels of IL-6 and TNF-α were detected in TRD patients compared to HC. While only a few studies on cortisol have been found, four papers showed elevated levels of C-reactive protein among these patients and four articles focused on immunological cells. Altered kynurenine metabolism in TRD patients was reported in two studies, while contrasting results were found with regard to BDNF.
Conclusion: Only a few biological alterations correlate with TRD. TNF-α seems to be the most relevant biomarker to discriminate TRD patients from both HC and treatment-responsive MDD patients. Moreover, several discrepancies among studies have been found, due to methodological differences and the lack of a standardized diagnostic definition of TRD.
Major Depressive Disorder (MDD) is a heterogeneous severe mental disorder, deriving from the interplay between genetic, environmental and psychological factors (1). More than 280 million people suffer from MDD, which is the primary cause of disability worldwide (2) and of significant impairment in daily functioning and quality of life (3, 4). At least 80% of patients with MDD experience work difficulties, problematic social interactions, and impaired daily life activities, making difficult the achievement of a full functional recovery (5, 6). Several effective pharmacological and psychosocial interventions are available for MDD, but many patients fail to respond to multiple antidepressant interventions, being defined as “treatment-resistant depression” (TRD) patients (7).
The first conceptualization of TRD dates back to 1970s as an attempt to overcome the limitation of the construct of “refractory depression” (8). Subsequently, Ban (9) argued that failure to respond to pharmacological treatment in patients with depression might reflect a different neurobiological substrate of depressive symptoms, compared to those patients who responded adequately to antidepressants. Accordingly, resistance to antidepressants would define for a distinct clinical subtype of depression. The first clinical definition of TRD was provided only in the late 90s by Thase and Rush (10), who described a sample of depressed patients who had not responded to at least two adequate trials of antidepressant medications, revitalizing the concept of TRD. Since then, the concept of TRD has been constantly refined (11, 12).
Currently, different definitions of TRD are available. The European Medicines Agency (EMA) defined resistance as a “failure to produce significant clinical results with a treatment of at least two different antidepressants (of the same or different classes) administered at the right doses and for an adequate amount of time, with verified patients’ compliance to treatment,” and is widely adopted as a standard definition of TRD in research settings (13). According to the Maudsley Staging Method, TRD is defined by five domains: time-course, severity, number of drugs, augmentative strategies, and use of ECT, with a maximum score of 15 (14). However, despite efforts, the definition of treatment resistant depression still presents several critical issues. In fact, some authors pointed out that the resistance construct can lead to a sense of nihilism in both patients and mental health professionals (15), and the construct of Difficult-To-Treat Depression (DTTD) would be preferable: while TRD focuses on a trial-and-error approach to find the right treatment, DTTD recognizes the importance of tailoring treatment to the needs of individual patients and considers a more comprehensive evaluation of patient’s medical history, lifestyle, and other subjective variables (16, 17). However, more complex and accurate definitions are poorly represented in clinical trials (18).
The difficulties in increasing knowledge about epidemiology, clinical management, and treatment of TRD are partially due to the lack of a univocal definition of this syndrome, which is highly needed. In fact, resistance to antidepressants is associated with greater symptom severity and chronicity, increased risk of comorbid physical (19, 20) and mental disorders, and higher suicide rates (21). Thus, TRD might represent a distinct clinical subtype of depression, yet one of the more severe, with unique treatment challenges and implications (22, 23), or a more severe form of MDD at the extreme of the affective continuum.
In order to gain deeper insights into the presence of a distinct clinical phenotype of TRD with discernible biological foundations, in this paper we have investigated biomarkers, specifically those previously documented in the literature for their associations with TRD. Biomarker can be defined as “A defined characteristic that is measured as an indicator of normal biological processes, pathogenic processes or responses to an exposure or intervention” (24). Biomarkers, as measurable molecular or cellular indicators, hold the potential to unravel the intricate interplay between genetic, physiological, and environmental factors that contribute to the manifestation of unique clinical profiles. These biomarkers serve as invaluable tools, facilitating the characterization, diagnosis, and understanding of the underlying biological mechanisms associated with a specific clinical phenotype. In the field of psychiatry, the practical application of biomarkers remains notably absent in clinical practice, primarily due to the limited supporting evidence in the literature. Biomarkers have demonstrated their transformative impact in various branches of medicine, including neurology and immunology, where they have facilitated early diagnosis, disease subtyping, treatment monitoring, prognosis assessment, and drug development.
However, efforts to distinguish between patients who will respond to treatment and those who will not have been unfruitful so far (25). Several studies have tried to identify the biological, psychopathological, and psychosocial correlates of depression, with particular attention to the dysfunction of the inflammatory system (26). Compared to patients with major depression who respond to pharmacological treatments, TRD patients have increased levels of proinflammatory cytokines, which indirectly reduce serotonin availability in the central nervous system (27) and the efficacy of antidepressant medications (28). Moreover, TRD is also associated with alterations in the hypothalamic-pituitary-adrenal (HPA) axis (29). A systematic review investigating the role of C-reactive protein (CRP) as a biomarker for MDD showed a low grade of inflammation was found in a percentage of MDD patients who were less responsive to treatment, suggesting that this could represent a subgroup of depressed patients with a different etiopathogenesis (30). Another studied biomarker is the brain-derived neurotrophic factor (BDNF), whose levels are significantly reduced in TRD patients compared to MDD, suggesting that the decreased levels of BDNF may be associated with biological resistance to traditional antidepressant treatments (31).
Taken together, available data suggest that chronic neuroinflammation might be implicated in the pathogenesis of MDD, with lower evidence about possible biomarkers of TRD (32). The identification of biomarkers of TRD holds relevant implications at clinical and research level. TRD biomarker could be used in clinical practice to identify in advance patients who are at higher risk to develop treatment resistance, facilitating the early detection of difficult to treat patients. Moreover, from a clinical perspective the availability of reliable biomarkers of TRD would be useful to assess a more precise prognosis of MDD patients, and to identify personalized and integrated treatments (which include psychotherapy and other psychosocial interventions) in order to reduce the risk of treatment resistance. At research level the identification of reliable biomarkers for TRD would be useful in order to develop new treatments strategies to be used in patients with TRD.
In this paper we review available studies assessing the full range of biomarkers compared to healthy controls in order to reshape TRD definition and improve its diagnosis, treatment, and prognosis.
The keywords “treatment resistant depression” OR “TRD” matched with “biomarker,” “inflammation,” “hormone,” “cytokine” or “biological marker” were entered in the PubMed, ISI Web of Knowledge and SCOPUS databases for papers published from inception until April 6, 2023. Studies were included in the review if they: (1) included patients with a diagnosis of TRD; (2) assessed any biological marker for TRD; (3) included a control group of healthy subjects; (4) were written in English. Studies including other subsamples of patients (i.e., those with bipolar disorder) were included only if it was possible to extrapolate data on patients with unipolar TRD. We included only papers assessing biological markers in the review. Markers of different nature, such as those based on imaging, genetics and clinical evaluations were excluded from our analysis. Moreover, articles not providing a clear definition or utilizing ambiguous terminology for TRD were excluded. Only original articles were considered for the review. Additionally, the reference lists of all included papers were checked for the identification of other possible studies (Figure 1). The full reports of potentially relevant studies were obtained, and content of each paper was extracted.
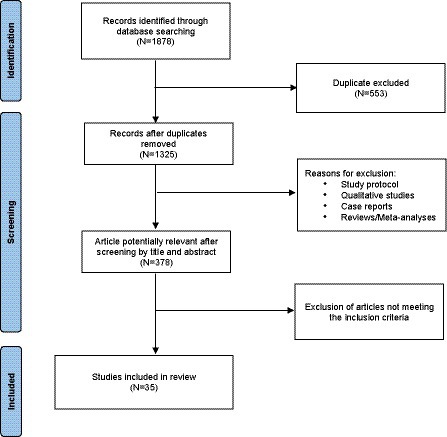
Figure 1. PRISMA flow diagram of selection of studies for inclusion in the review.
For each paper, data on study design, sample characteristics, age range of recruited patients, biomarkers detected, psychopathological and psychosocial characteristics, TRD definition, and main results were independently extracted by four authors; discrepancies were resolved by discussion.
Entering the keywords in the relevant databases, 1,878 papers were identified; 553 were duplicates and excluded. 947 further papers were eliminated after reading the abstracts because they did not meet the inclusion criteria. After reading full-text papers, 212 more papers were excluded. Therefore, our review consists of 35 papers, grouped in the following five categories according to the main investigated biological correlates: studies on cytokines; other inflammatory markers; kynurenine; Brain-Derived Neurotrophic Factor (BDNF); and other clinical parameters (Table 1).

Table 1. Summary of studies included in the review.
With respect to IL-1, available data are still inconsistent. In fact, while Uint et al. (62) found higher IL-1b plasma levels in TRD compared to HC, Zincir et al. (67) and Wu et al. (65) found lower IL-1b levels of in TRD patients.
All available studies found increased plasma levels of IL-6 in TRD patients compared to HC (28, 49, 54, 65).
Seven studies addressed the correlation between TNF-α and TRD. Sanchez-Carro et al. (55) provided data supporting the role of TNF-α in discriminating between TRD and HC using a machine learning approach. These findings were replicated in a case–control cross-sectional study on elderly TRD patients, where TNF-α levels were significantly higher in TRD than in the HC group (65). In addition, in a double-blind, randomized, placebo-controlled trial, Strawbridge et al. (59) found that the baseline pro-inflammatory proteins, including TNF-α, were significantly higher in TRD patients than in HC, after controlling for gender, age, childhood adversity and BMI. On the other hand, one study found no difference in the production of lipopolysaccharide induced-TNF-α in peripheral blood mononuclear cells (34), while other reports (61, 67) found decreased TNF-α levels in TRD compared to HC. Interestingly, one study reported higher serum concentrations of TNF-α receptor subtype 1 (TNF-α R1) titers in TRD patients compared to HC (44).
In a randomized controlled trial, Zincir et al. (67) found higher levels of IL-10 in TRD compared to HC, while another study found no difference between TRD patients and healthy controls (59).
Other cytokines which have been explored as potential biomarkers of TRD include IL-12, IL-5, Interferon gamma (IFN-gamma), IL-8 and IL-4. Szałach et al. (61) reported lower levels of serum IL-12 and higher levels of IL-8 in TRD patients vs. HC. Strawbridge et al. (60) found higher levels of IL-8 in TRD patients compared to controls, associated with elevated titers of IL-5. Moreover, IL-4 blood levels were significantly higher in TRD than in the control group (67), while no difference in phytohemagglutinin (PHA)-induced IL-2 production has been found between patients and controls (34). One study found higher IFN-gamma titers in TRD than in the control group (67).
Despite consolidated evidence on cortisol levels in MDD, only a few studies have been carried out in patients with TRD. Markopoulou et al. (51) and Wu et al. (65) found higher cortisol serum levels in TRD vs. HC. Interestingly, Juruena et al. (45) found an impaired activity of glucocorticoid receptors (GRs) in TRD group compared to HC. de Menezes Galvão et al. (40) carried out a RCT on the effect of ayahuasca on the hypothalamic-pituitary-adrenal axis (HPA) and found that at baseline TRD patients exhibit blunted awakening salivary cortisol response and hypocortisolemia compared to HC.
Four studies (38, 39, 41, 59) found elevated levels of C-reactive protein (CRP) in TRD patients compared to HC, two studies reported no differences between cases and controls (44, 62), while Sanchez-Carro et al. (55) found that CRP does not discriminate between the two groups.
Four studies investigated immunological cells populations in TRD patients compared to HC. In particular, two studies found no differences in lymphocyte proliferation (34) and central populations of T cells between TRD patients and HC (61). However, in a large trial by Lauden et al. (46) on 570 TRD patients and 2,850 HC, higher levels of blood WBC, lymphocytes and platelets were found in the TRD group. Another study on lymphocyte sensitivity to dexamethasone (DEX) intake found that changes in cell redistribution after DEX administration were more prominent in TRD patients than in controls, but the effects of DEX were dependent on DEX-induced suppression of cortisol secretion (35).
We found three studies on the kynurenine pathway in TRD. Zhou et al. (66) found lower serum concentrations of tryptophan (TRP), kynurenic acid (KYNA) and the KYNA/kynurenine (KYN) ratio, and a higher KYN/TRP ratio in TRD patients compared to HC. Also, Schwieler et al. (57) found an altered kynurenine metabolism in TRD patients, in particular decreased plasma levels of KYNA and significantly increased quinolinic acid/kynurenine ratio. However, one study found no difference between TRD and HC in the plasma levels of tryptophan, KYNA, and quinolinic acid (QUIN).
Four studies have explored the role of BDNF in TRD. In a randomized double-blinded placebo-controlled trial using a parallel-arm design of ayahuasca vs. placebo, no correlation was found between plasma levels of BDNF and TRD (41). Two studies reported lower levels of BDNF in TRD compared to HC (33, 53), while Uint et al. (62) found opposite results.
Several other hematological parameters have been investigated in TRD patients. In particular, lower serum albumin levels were found in TRD patients compared to controls (64), while no significant difference in the levels of basal Thyroid Stimulating Hormone (TSH) and T4 were detected between major depressed patients with or without TRD and non-TRD (46, 63). One study showed lower vascular endothelial growth factor (VEGF) titers in TRD patients compared to HC (53). One study found reduced baseline levels of enzyme cofactor biopterin (involved in the synthesis of neurotransmitters like serotonin, dopamine, and norepinephrine) in TRD patients compared to HC (43). Significantly decreased serum levels of acetylating molecule acetyl-L-carnitine (LAC) were observed in TRD patients compared to HC (52). Another study reported higher serum levels of oxytocin (OXT) in a sample of adolescents with TRD compared to age-matched HC (56).
Gur et al. (42) found that TRD patients are more frequently seronegative to Aquaporin-4 (an astrocyte water channel protein) autoantibodies (AQP4-IgG) compared to HC. However, another study reported no statistical difference in the expression of AQP4 gene between TRD and HC (37).
Interestingly, two studies assessed zinc (Zn) serum levels: Maes et al. (48) found significantly lower levels of serum Zn in TRD than in HC, which were inversely correlated with IL-6 titers (49). The same authors showed a significantly lower serum activity of dipeptidyl peptidase IV (DPP IV), a serine protease with a role in cytokine production, in TRD than in HC (47), and significantly lower levels of the antioxidant Coenzyme Q10 compared to responsive-MDD patients (50). Sanchez-Carro et al. (55) reported that glutathione and 4-hydroxynonenal (HNE) could serve as variables to discriminate between TRD patients and HC. Moreover, one study investigated the role of stress-related neuropetide Substance P (SP) in the central nervous system (CNS), by means of standard lumbar puncture techniques (36). Authors reported that TRD patients taking psychotropic medications had significantly lower mean cerebrospinal fluid SP concentration than HC (53).
The underlying biological mechanisms that contribute to development and maintenance of TRD are not yet elucidated. The identification of reliable biomarkers would allow an early identification, proper diagnosis and treatment of TRD, improving the chance of a successful outcome (68). However, only a small number of biological alterations seem to correlate with TRD, in particular some cytokines, the kynurenine pathway catabolites, CRP, BDNF and cortisol.
The role of inflammation, and in particular of cytokines, in the pathophysiology of mental disorders has been recently highlighted (69), following a new wave of studies using modern biological techniques (70, 71). While several evidence shows an involvement of the immunological systems in MDD, suggesting that the communication between immune and brain systems might be mediated by increased cytokine levels (72, 73), only a limited number of studies investigating the role of inflammation and of cytokine alteration in TRD have been found, despite the presence of low-grade neuroinflammation has been reported to be more frequently in patient with treatment resistant major depression, rather than in responders and healthy controls (74, 75).
Available evidence has reported that TNF-α, whose blood concentration has shown a significant improvement after treatments with antidepressants, is the most relevant biomarker to discriminate TRD patients from both to HC and to treatment-responsive MDD patients (55, 74). In the Central Nervous System (CNS) TNF-α promotes serotonin metabolism and enhances the serotonin transporter’s activity (76). In particular, reduced levels of TNF-α could be associated to a reduced activity of serotonin transporter, thus influencing the effectiveness antidepressants, like selective serotonin reuptake inhibitors (SSRIs) (76). Consequently, the assessment of TNF-α levels could have potential clinical relevance for TRD patients who have experienced several unsuccessful trials of antidepressant treatments (77).
Two studies found increased levels of IL-8 in TRD patients compared to healthy controls. IL-8 is produced by monocytes, macrophages, and neutrophils and exerts a pro-inflammatory action, by facilitating neutrophil migration. It is also synthetized in SNC by microglia can synthesize IL-8 in response to proinflammatory stimuli; it has also been reported that anti-inflammatory cytokines can downregulate its production and release in the SNC (20). IL-8 levels have been found to be consistently elevated in TRD patients also when they are compared to MDD responsive individuals, suggesting that this cytokine could be a potential biomarker for TRD. However, this hypothesis needs to be confirmed by further larger longitudinal studies, with standardized diagnostic criteria and treatment-specific analyzes. Additionally, a more comprehensive understanding of the role of IL-8 in TRD might come from multi-modal research approaches, integrating genetic, imaging, and clinical data. Reviewed studies are insufficient to draw any other firm consideration about the role of the other cytokines, such as IL-2, IL-5, and IL-12, in TRD pathophysiology.
The BDNF has also been assessed as a biomarker in the pathophysiology of TRD. The BDNF belongs to the family of neurotrophins, a group of growth factors that support the survival, development, and function of neurons in the brain and peripheral nervous system (78). Inflammation, which is associated with increased cytokines production, affects BDNF expression, although the exact biological pathway is not fully elucidated (79). Chronic stress induces a reduction in BDNF concentration (80), but studies analyzing serum BDNF levels in TRD conveyed conflicting results (81). In fact, while some studies reported a reduction of BDNF concentration (53, 64), others found an increase of BDNF levels (62) or no difference between TRD and healthy controls. The inconsistency of these results might be due to the fact that serum analysis of BDNF concentrations is variable and scarcely reliable, unless Polymerase Chain Reaction (PCR) is used.
Many studies reported increased cortisol levels in TRD patients (51, 65), suggesting an alteration in HPA axis. One hypothesis regarding cortisol modulation in depression indicates a form of HPA axis fatigue with an underlying hypocortisolism both in salivary and plasma samples (34, 40). In fact, chronic low levels of cortisol can cause weakness, loss of appetite and immunological dysfunctions, which are symptoms commonly associated to depression (82, 83). However, the inconsistency of results reported in studies included in the present review can be explained by the fact that antidepressant treatments can alter HPA axis functions. Therefore, in order to fully understand the role of cortisol in depression, studies comparing medicated vs. non medicated patients are needed (84).
Several studies found alterations in the number of blood immune cells. Evidence shows that TRD patients can have increased leucocytes and possibly platelets; however, the role of immune cells in TRD should be better investigated. In fact, studies including a higher number of participants reported an increase in immunological cells, such as neutrophils and platelets in TRD patients vs. healthy controls; however, these differences were not statistically significant when comparing MMD and TRD, challenging the view that they can represent different pathologies along the affective spectrum (46).
In the present review, an alteration in the kynurenine pathway (KP) has been reported in several studies. This result is of particular relevance, since the vast majority (~95%) of tryptophan (TRP) is metabolized via KP in kynurenine (KYN), quinolinic acid (QUIN) and kynuretic acid (KYNA), while only a small part of TRR is used to synthetize monoamines, implicated in the pathophysiology of MDD, including noradrenaline and serotonin (85). Enzymes of the KP, can be activated by pro-inflammatory cytokines, which may lead to TRP depletion (86). Results of the present review confirm this hypothesis, despite they need to be replicated in larger samples.
Treatment-resistant depression represents a significant challenge in mental health care, making a priority the need to identify the etiological pathways of this complex mental disorder. Numerous additional biological pathways, including biopterin, acetyl-L-carnitine, oxytocin, zinc, glutathione, nesfatin-1, and dipeptidyl peptidase IV, have been investigated in TRD. In particular, biopterin, a critical cofactor in neurotransmitter synthesis, has shown potential relevance in TRD (87). Alterations in biopterin metabolism have been associated with the dysregulation of serotonin, dopamine, and norepinephrine systems, all of them being implicated in depression (88). Similarly, Acetyl-L-carnitine, an endogenous compound involved in cellular energy metabolism and neuroprotection, has demonstrated antidepressant effects in clinical studies, indicating its potential as a therapeutic target for TRD (89). While the studies on pathways of biopterin and acetyl-L-carnitine seem promising to enhance our understanding of major depression and of TRD, others - including aquaporin-4, vascular endothelial growth factor (VEGF), and thyroid-stimulating hormone (TSH) - have yield fewer compelling results. However, the current level of evidence for these pathways is still low, and any consideration about the potential role in TRD remains speculative.
The existing literature on the biological correlates of TRD is explored by numerous studies, but the comparability of their findings and methods often proves challenging mainly due to methodological disparities and clinical characterization differences. These variations encompass the utilization of diverse laboratory techniques and the incorporation of inclusion criteria grounded in distinct conceptual definitions. As a consequence, the synthesis of this body of research faces obstacles in drawing definitive conclusions about the underlying biological mechanisms of TRD.
In the analysis of the selected articles conflicting outcomes have emerged. Nevertheless, certain cytokines, such as IL-6 and TNF-α, have demonstrated a more extensive body of supporting evidence. A significant proportion of the examined cytokines, however, lacked a sufficient number of studies for meaningful cross-comparisons, rendering the available evidence insufficient to derive preliminary conclusions. Moreover, notwithstanding the presence of evidentiary support in other domains of psychiatric pathologies, the cortisol pathway exhibited incongruent findings in the context of TRD. Additionally, the available data regarding BDNF appear challenging to compare due to methodological disparities in the analysis, which may account for the incongruity of the results.
This review is subject to several limitations, that are hereby acknowledged. First and foremost, a significant challenge in our synthesis of findings is the inconsistency in the definition of treatment-resistant depression across studies. The lack of a standardized and universally accepted definition hampers the possibility to draw definitive conclusions regarding biomarkers associated with this specific depressive phenotype. Additionally, methodological limitations within included studies, such as variations in sample collection and processing techniques, assay methodologies, and data analysis approaches, introduce potential sources of bias, reducing the comparability and generalizability of results. Another common limitation observed in available studies is represented by the relatively small sample sizes, which may limit the statistical power of studies. Therefore, caution is needed when interpreting the findings of this review, and further well-designed studies with larger and more homogeneous samples are warranted to overcome these limitations and provide more robust evidence regarding biomarkers of TRD.
In conclusion, although the notion of TRD lacks coherence and standardization (90, 91), some evidence suggests a biological alteration in TRD. However, the future perspectives for research on the biological correlates of TRD are both promising and challenging (92). To advance our understanding of TRD’s biological underpinnings, it is imperative to establish a more robust conceptual framework for TRD, which include the resistance to psychotherapeutic interventions, also. Additionally, future studies should aim to include well-characterized, medication-naïve patient samples and adopt longitudinal designs to assess biomarker variations over time. Based on the findings of this review, it becomes evident that prioritizing the analysis of biomarker panels, rather that single biomarkers, is imperative. Finding a biosignature of TRD, coming from a panel of biomarkers, not only enables a more comprehensive understanding of biological processes underlying mental disorder but also offers an opportunity to develop targeted treatments able to influence it and to modify the long-term outcome of TRD. Lastly, future studies should include strategies to identify patient with pseudoresistance to pharmacological treatments (23), due to poor compliance to pharmacological treatments.
EM: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. GS: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Supervision. AB: Writing – review & editing, Data curation. BD: Data curation, Writing – review & editing. MD: Data curation, Writing – review & editing. MVL: Methodology, Writing – review & editing. FM: Methodology, Writing – review & editing. FL: Data curation, Writing – review & editing. ML: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Boschloo, L , Hieronymus, F , and Cuijpers, P, ICECA Work Group . Clinical response to SSRIs relative to cognitive behavioral therapy in depression: a symptom-specific approach. World Psychiatry. (2022) 21:152–3. doi: 10.1002/wps.20944
2. World Health Organization . Depression (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/depression (Accessed April 25, 2023).
3. Miguel, C , Karyotaki, E , Cuijpers, P , and Cristea, IA . Selective outcome reporting and the effectiveness of psychotherapies for depression. World Psychiatry. (2021) 20:444–5. doi: 10.1002/wps.20900
4. Trivedi, MH . Major depressive disorder: remission of associated symptoms. J Clin Psychiatry. (2006) 67:27–32.
5. Greenberg, PE , Fournier, AA , Sisitsky, T , Simes, M , Berman, R , Koenigsberg, SH, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). PharmacoEconomics. (2021) 39:653–65. doi: 10.1007/s40273-021-01019-4
6. Steger, MF . Meaning in life is a fundamental protective factor in the context of psychopathology. World Psychiatry. (2022) 21:389–90. doi: 10.1002/wps.20916
7. Furukawa, TA , Shinohara, K , Sahker, E , Karyotaki, E , Miguel, C , Ciharova, M, et al. Initial treatment choices to achieve sustained response in major depression: a systematic review and network meta-analysis. World Psychiatry (2021) 20:387–96. doi: 10.1002/wps.20906
8. Murphy, JA , Sarris, J , and Byrne, GJ . A review of the conceptualisation and risk factors associated with treatment-resistant depression. Depress Res Treat. (2017) 2017:4176825–10. doi: 10.1155/2017/4176825
9. Ban, TA . Prolegomenon to the clinical prerequisite: psychopharmacology and the classification of mental disorders. Prog Neuro-Psychopharmacol Biol Psychiatry. (1987) 11:527–80. doi: 10.1016/0278-5846(87)90019-4
10. Thase, ME , and Rush, AJ . When at first you don’t succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry. (1997) 58:23–9.
11. Ventriglio, A , Bhugra, D , Sampogna, G , Luciano, M , De Berardis, D , Sani, G, et al. From dysthymia to treatment-resistant depression: evolution of a psychopathological construct. Int Rev Psychiatry. (2020) 32:471–6. doi: 10.1080/09540261.2020.1765517
12. Cuijpers, P , Quero, S , Noma, H , Ciharova, M , Miguel, C , Karyotaki, E, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types. World Psychiatry (2021) 20:283–93. doi: 10.1002/wps.20860
13. European Medicines Agency . Guideline on clinical investigation of medicinal products for the treatment of depression. (2013). Available at: https://www.ema.europa.eu/en/news/european-medicines-agency-publishes-guideline-clinical-investigation-medicines-depression (Accessed April 25, 2023).
14. Fekadu, A , Wooderson, S , Donaldson, C , Markopoulou, K , Masterson, B , Poon, L, et al. A multidimensional tool to quantify treatment resistance in depression: the Maudsley staging method. J Clin Psychiatry. (2009) 70:177–84. doi: 10.4088/jcp.08m04309
15. McIntyre, RS , Filteau, MJ , Martin, L , Patry, S , Carvalho, A , Cha, DS, et al. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affect Disord. (2014) 156:1–7. doi: 10.1016/j.jad.2013.10.043
16. Rush, AJ , Sackeim, HA , Conway, CR , Bunker, MT , Hollon, SD , Demyttenaere, K, et al. Clinical research challenges posed by difficult-to-treat depression. Psychol Med. (2022) 52:419–32. doi: 10.1017/S0033291721004943
17. Stein, DJ , Shoptaw, SJ , Vigo, DV , Lund, C , Cuijpers, P , Bantjes, J, et al. Psychiatric diagnosis and treatment in the 21st century: paradigm shifts versus incremental integration. World Psychiatry. (2022) 21:393–414. doi: 10.1002/wps.20998
18. Anderson, IM . We all know what we mean by treatment-resistant depression - don't we? Br J Psychiatry. (2018) 212:259–61. doi: 10.1192/bjp.2018.56
19. Meng, R , Yu, C , Liu, N , He, M , Lv, J , Guo, Y, et al. Association of Depression with all-Cause and Cardiovascular Disease Mortality among Adults in China. JAMA Netw Open. (2020) 3:e1921043. doi: 10.1001/jamanetworkopen.2019.21043
20. Kim, H , Turiano, NA , Forbes, MK , Kotov, R , Krueger, RF , Eaton, NR, et al. Internalizing psychopathology and all-cause mortality: a comparison of transdiagnostic vs. diagnosis-based risk prediction. World Psychiatry. (2021) 20:276–82. doi: 10.1002/wps.20859
21. Bergfeld, IO , Mantione, M , Figee, M , Schuurman, PR , Lok, A , and Denys, D . Treatment-resistant depression and suicidality. J Affect Disord. (2018) 235:362–7. doi: 10.1016/j.jad.2018.04.016
22. Möller, HJ , Seemüller, F , Schennach, R , and Gupta, RK . Treatment-resistant depression: a separate disorder – a new approach In: S Kasper and S Montgomery, editors. Treatment-resistant depression. London: Willey Blackwell (2013). 21–41. doi: 10.1002/9781118556719.ch2
23. Leichsenring, F , Steinert, C , Rabung, S , and Ioannidis, JPA . The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry. (2022) 21:133–45. doi: 10.1002/wps.20941
24. FDA-NIH Biomarker Working Group . BEST (biomarkers, EndpointS, and other tools) resource. Silver spring (MD): Food and Drug Administration (US); Bethesda (MD): National Institutes of Health (US). (2006). Available at: www.ncbi.nlm.nih.gov/books/NBK326791/.
25. Owen, MJ , and Williams, NM . Explaining the missing heritability of psychiatric disorders. World Psychiatry. (2021) 20:294–5. doi: 10.1002/wps.20870
26. Fisher, AJ , Song, J , and Soyster, PD . Toward a systems-based approach to understanding the role of the sympathetic nervous system in depression. World Psychiatry. (2021) 20:295–6. doi: 10.1002/wps.20872
27. Miller, AH , Maletic, V , and Raison, CL . Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. (2009) 65:732–41. doi: 10.1016/j.biopsych.2008.11.029
28. Liu, JJ , Wei, YB , Strawbridge, R , Bao, Y , Chang, S , Shi, L, et al. Peripheral cytokine levels and response to antidepressant treatment in depression: a systematic review and meta-analysis. Mol Psychiatry. (2020) 25:339–50. doi: 10.1038/s41380-019-0474-5
29. Markopoulou, K , Fischer, S , Papadopoulos, A , Poon, L , Rane, LJ , Fekadu, A, et al. Comparison of hypothalamo-pituitary-adrenal function in treatment resistant unipolar and bipolar depression. Transl Psychiatry. (2021) 11:1–8. doi: 10.1038/s41398-021-01343-5
30. Orsolini, L , Pompili, S , Tempia Valenta, S , Salvi, V , and Volpe, U . C-reactive protein as a biomarker for major depressive disorder? Int J Mol Sci. (2022) 23:1616. doi: 10.3390/ijms23031616
31. Watson, D , Levin-Aspenson, HF , Waszczuk, MA , Conway, CC , Dalgleish, T , Dretsch, MN, et al. Validity and utility of hierarchical taxonomy of psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry. (2022) 21:26–54. doi: 10.1002/wps.20943
32. Marrie, RA , and Bernstein, CN . Psychiatric comorbidity in immune-mediated inflammatory diseases. World Psychiatry. (2021) 20:298–9. doi: 10.1002/wps.20873
33. Allen, AP , Naughton, M , Dowling, J , Walsh, A , Ismail, F , Shorten, G, et al. Serum BDNF as a peripheral biomarker of treatment-resistant depression and the rapid antidepressant response: a comparison of ketamine and ECT. J Affect Disord. (2015) 186:306–11. doi: 10.1016/j.jad.2015.06.033
34. Bauer, ME , Papadopoulos, A , Poon, L , Perks, P , Lightman, SL , Checkley, S, et al. Altered glucocorticoid immunoregulation in treatment resistant depression. Psychoneuroendocrinology. (2003) 28:49–65. doi: 10.1016/s0306-4530(02)00009-4
35. Bauer, M , Papadopoulos, A , Poon, L , Perks, P , Lightman, S , Checkley, S, et al. Dexamethasone-induced effects on lymphocyte distribution and expression of adhesion molecules in treatment-resistant depression. Psychiatry Res. (2002) 113:1–15. doi: 10.1016/s0165-1781(02)00243-3
36. Carpenter, LL , Bayat, L , Moreno, F , Kling, MA , Price, LH , Tyrka, AR, et al. Decreased cerebrospinal fluid concentrations of substance P in treatment-resistant depression and lack of alteration after acute adjunct vagus nerve stimulation therapy. Psychiatry Res. (2008) 157:123–9. doi: 10.1016/j.psychres.2007.04.016
37. Cattaneo, A , Ferrari, C , Turner, L , Mariani, N , Enache, D , Hastings, C, et al. Whole-blood expression of inflammasome- and glucocorticoid-related mRNAs correctly separates treatment-resistant depressed patients from drug-free and responsive patients in the BIODEP study. Transl Psychiatry. (2020) 10:232. doi: 10.1038/s41398-020-00874-7
38. Chamberlain, SR , Cavanagh, J , de Boer, P , Mondelli, V , Jones, DNC , Drevets, WC, et al. Treatment-resistant depression and peripheral C-reactive protein. Br J Psychiatry. (2019) 214:11–9. doi: 10.1192/bjp.2018.66
39. Congio, AC , Norcia, M , Urbano, MR , Verri, WA , and Vargas Nunes, SO . Association of clinical features and biomarkers with treatment-resistant depression. Neurol Psychiatry Brain Res. (2020) 36:32–8. doi: 10.1016/j.npbr.2020.02.004
40. de Menezes Galvão, AC , de Almeida, RN , Silva, EADS , Freire, FAM , Palhano-Fontes, F , Onias, H, et al. Cortisol modulation by Ayahuasca in patients with treatment resistant depression and healthy controls. Front Psych. (2018) 9:185. doi: 10.3389/fpsyt.2018.00185
41. Galvao-Coelho, NL , de Menezes Galvao, AC , de Almeida, RN , Palhano-Fontes, F , Braga, IC , Soares, BL, et al. Changes in inflammatory biomarkers are related to the antidepressant effects of Ayahuasca. J Psychopharmacol. (2020) 34:1125–33. doi: 10.1177/0269881120936486
42. Gur, S , Taler, M , Bormant, G , Blattberg, D , Nitzan, U , Vaknin-Dembinsky, A, et al. Lack of association between unipolar or bipolar depression and serum aquaporin-4 autoantibodies. Brain Behav Immun. (2020) 88:930–4. doi: 10.1016/j.bbi.2020.05.001
43. Hoekstra, R , Van den Broek, WW , Fekkes, D , Bruijn, JA , Mulder, PGH , and Pepplinkhuizen, L . Effect of electroconvulsive therapy on biopterin and large neutral amino acids in severe, medication-resistant depression. Psychiatry Res. (2001) 103:115–23. doi: 10.1016/s0165-1781(01)00282-7
44. Huang, MH , Chen, MH , Tu, PC , Bai, YM , Su, TP , Yang, BH, et al. Elevated tumor necrosis factor-alpha receptor subtype 1 and the association with abnormal brain function in treatment-resistant depression. J Affect Disord. (2018) 235:250–6. doi: 10.1016/j.jad.2018.04.037
45. Juruena, MF , Pariante, CM , Papadopoulos, AS , Poon, L , Lightman, S , and Cleare, AJ . The role of mineralocorticoid receptor function in treatment-resistant depression. J Psychopharmacol. (2013) 27:1169–79. doi: 10.1177/0269881113499205
46. Lauden, A , Geishin, A , Merzon, E , Korobeinikov, A , Green, I , Golan-Cohen, A, et al. Higher rates of allergies, autoimmune diseases and low-grade inflammation markers in treatment-resistant major depression. Brain Behav Immun Health. (2021) 16:100313. doi: 10.1016/j.bbih.2021.100313
47. Maes, M , de Meester, I , Verkerk, R , de Medts, P , Wauters, A , Vanhoof, G, et al. Lower serum dipeptidyl peptidase IV activity in treatment resistant major depression: relationships with immune-inflammatory markers. Psychoneuroendocrinology. (1997) 22:65–78. doi: 10.1016/s0306-4530(96)00040-6
48. Maes, M , Vandoolaeghe, E , Neels, H , Demedts, P , Wauters, A , Meltzer, HY, et al. Lower serum zinc in major depression is a sensitive marker of treatment resistance and of the immune/inflammatory response in that illness. Biol Psychiatry. (1997) 42:349–58. doi: 10.1016/S0006-3223(96)00365-4
49. Maes, M , Bosmans, E , De Jongh, R , Kenis, G , Vandoolaeghe, E , and Neels, H . Increased serum IL-6 and IL-1 receptor antagonist concentrations in major depression and treatment resistant depression. Cytokine. (1997) 9:853–8. doi: 10.1006/cyto.1997.0238
50. Maes, M , Mihaylova, I , Kubera, M , Uytterhoeven, M , Vrydags, N , and Bosmans, E . Lower plasma coenzyme Q10 in depression: a marker for treatment resistance and chronic fatigue in depression and a risk factor to cardiovascular disorder in that illness. Neuro Endocrinol Lett. (2009) 30:462–9.
51. Markopoulou, K , Papadopoulos, A , Juruena, MF , Poon, L , Pariante, CM , and Cleare, AJ . The ratio of cortisol/DHEA in treatment resistant depression. Psychoneuroendocrinology. (2009) 34:19–26. doi: 10.1016/j.psyneuen.2008.08.004
52. Nasca, C , Bigio, B , Lee, FS , Young, SP , Kautz, MM , Albright, A, et al. Acetyl-l-carnitine deficiency in patients with major depressive disorder. Proc Natl Acad Sci U S A. (2018) 115:8627–32. doi: 10.1073/pnas.1801609115
53. Pisoni, A , Strawbridge, R , Hodsoll, J , Powell, TR , Breen, G , Hatch, S, et al. Growth factor proteins and treatment-resistant depression: a place on the path to precision. Front Psych. (2018) 9:386. doi: 10.3389/fpsyt.2018.00386
54. Rengasamy, M , McClain, L , Gandhi, P , Segreti, AM , Brent, D , Peters, D, et al. Associations of plasma interleukin-6 with plasma and cerebrospinal fluid monoamine biosynthetic pathway metabolites in treatment-resistant depression. Neurol Psychiatry Brain Res. (2018) 30:39–46. doi: 10.1016/j.npbr.2018.05.001
55. Sánchez-Carro, Y , de la Torre-Luque, A , Leal-Leturia, I , Salvat-Pujol, N , Massaneda, C , de Arriba-Arnau, A, et al. Importance of immunometabolic markers for the classification of patients with major depressive disorder using machine learning. Prog Neuro-Psychopharmacol Biol Psychiatry. (2023) 121:110674. doi: 10.1016/j.pnpbp.2022.110674
56. Sasaki, T , Hashimoto, K , Oda, Y , Ishima, T , Yakita, M , Kurata, T, et al. Increased serum levels of oxytocin in 'Treatment resistant depression in adolescents (TRDIA)' group. PLoS One. (2016) 11:e0160767. doi: 10.1371/journal.pone.0160767
57. Schwieler, L , Samuelsson, M , Frye, MA , Bhat, M , Schuppe-Koistinen, I , Jungholm, O, et al. Electroconvulsive therapy suppresses the neurotoxic branch of the kynurenine pathway in treatment-resistant depressed patients. J Neuroinflammation. (2016) 13:51. doi: 10.1186/s12974-016-0517-7
58. Sowa-Kucma, M , Styczen, K , Siwek, M , Misztak, P , Nowak, RJ , Dudek, D, et al. Lipid peroxidation and immune biomarkers are associated with major depression and its phenotypes, including treatment-resistant depression and melancholia. Neurotox Res. (2018) 33:448–60. doi: 10.1007/s12640-017-9835-5
59. Strawbridge, R , Jamieson, A , Hodsoll, J , Ferrier, IN , McAllister-Williams, RH , Powell, TR, et al. The role of inflammatory proteins in anti-glucocorticoid therapy for treatment-resistant depression. J Clin Med. (2021) 10:784. doi: 10.3390/jcm10040784
60. Strawbridge, R , Hodsoll, J , Powell, TR , Hotopf, M , Hatch, SL , Breen, G, et al. Inflammatory profiles of severe treatment-resistant depression. J Affect Disord. (2019) 246:42–51. doi: 10.1016/j.jad.2018.12.037
61. Szałach, ŁP , Cubała, WJ , and Lisowska, KA . Changes in T-cell subpopulations and cytokine levels in patients with treatment-resistant depression-a preliminary study. Int J Mol Sci. (2022) 24:479. doi: 10.3390/ijms24010479
62. Uint, L , Bastos, GM , Thurow, HS , Borges, JB , Hirata, TDC , França, JID, et al. Increased levels of plasma IL-1b and BDNF can predict resistant depression patients. Rev Assoc Med Bras. (2019) 65:361–9. doi: 10.1590/1806-9282.65.3.361
63. Vandoolaeghe, E , Maes, M , Vandevyvere, J , and Neels, H . Hypothalamic-pituitary-thyroid-axis function in treatment resistant depression. J Affect Disord. (1997) 43:143–50. doi: 10.1016/s0165-0327(96)01426-7
64. Van Hunsel, F , Wauters, A , Vandoolaeghe, E , Neels, H , Demedts, P , and Maes, M . Lower total serum protein, albumin, and beta-and gamma-globulin in major and treatment-resistant depression: effects of antidepressant treatments. Psychiatry Res. (1996) 65:159–69. doi: 10.1016/s0165-1781(96)03010-7
65. Wu, X , Dai, B , Yan, F , Chen, Y , Xu, Y , Xia, Q, et al. Serum cortisol, Nesfatin-1, and IL-113: potential diagnostic biomarkers in elderly patients with treatment-resistant depression. Clin Interv Aging. (2022) 17:567–76. doi: 10.2147/CIA.S361459
66. Zhou, Y , Zheng, W , Liu, W , Wang, C , Zhan, Y , Li, H, et al. Antidepressant effect of repeated ketamine administration on kynurenine pathway metabolites in patients with unipolar and bipolar depression. Brain Behav Immun. (2018) 74:205–12. doi: 10.1016/j.bbi.2018.09.007
67. Zincir, S , Öztürk, P , Bilgen, AE , Izci, F , and Yükselir, C . Levels of serum immunomodulators and alterations with electroconvulsive therapy in treatment-resistant major depression. Neuropsychiatr Dis Treat. (2016) 12:1389–96. doi: 10.2147/NDT.S106652
68. Kendler, KS . Incremental advances in psychiatric molecular genetics and nosology. World Psychiatry. (2022) 21:415–6. doi: 10.1002/wps.20999
69. Penninx, BWJH . Psychiatric symptoms and cognitive impairment in "long COVID": the relevance of immunopsychiatry. World Psychiatry. (2021) 20:357–8. doi: 10.1002/wps.20913
70. Keshavan, MS . Characterizing transdiagnostic premorbid biotypes can help progress in selective prevention in psychiatry. World Psychiatry. (2021) 20:231–2. doi: 10.1002/wps.20857
71. Wakefield, JC . Klerman’s “credo” reconsidered: neo-Kraepelinianism, Spitzer’s views, and what we can learn from the past. World Psychiatry. (2022) 21:4–25. doi: 10.1002/wps.20942
72. Arango, C , Dragioti, E , Solmi, M , Cortese, S , Domschke, K , Murray, RM, et al. Risk and protective factors for mental disorders beyond genetics: an evidence-based atlas. World Psychiatry. (2021) 20:417–36. doi: 10.1002/wps.20894
73. Islam, MR , Sohan, M , Daria, S , Masud, AA , Ahmed, MU , Roy, A, et al. Evaluation of inflammatory cytokines in drug-naïve major depressive disorder: a systematic review and meta-analysis. Int J Immunopathol Pharmacol. (2023) 37:3946320231198828. doi: 10.1177/03946320231198828
74. Lanquillon, S , Krieg, JC , Bening-Abu-Shach, U , and Vedder, H . Cytokine production and treatment response in major depressive disorder. Neuropsychopharmacology. (2000) 22:370–9. doi: 10.1016/S0893-133X(99)00134-7
75. Uher, R , Tansey, KE , Dew, T , Maier, W , Mors, O , Hauser, J, et al. An inflammatory biomarker as a differential predictor of outcome of depression treatment with escitalopram and nortriptyline. Am J Psychiatry. (2014) 171:1278–86. doi: 10.1176/appi.ajp.2014.14010094
76. Zhu, CB , Blakely, RD , and Hewlett, WA . The proinflammatory cytokines interleukin-1beta and tumor necrosis factor-alpha activate serotonin transporters. Neuropsychopharmacology. (2006) 31:2121–31. doi: 10.1038/sj.npp.1301029
77. Haroon, E , Daguanno, AW , Woolwine, BJ , Goldsmith, DR , Baer, WM , Wommack, EC, et al. Antidepressant treatment resistance is associated with increased inflammatory markers in patients with major depressive disorder. Psychoneuroendocrinology. (2018) 95:43–9. doi: 10.1016/j.psyneuen.2018.05.026
78. Krueger, RF , Hobbs, KA , Conway, CC , Dick, DM , Dretsch, MN , Eaton, NR, et al. Validity and utility of hierarchical taxonomy of psychopathology (HiTOP): II. Externalizing superspectrum. World Psychiatry. (2021) 20:171–93. doi: 10.1002/wps.20844
79. de Felice, G , Luciano, M , Boiano, A , Colangelo, G , Catapano, P , Della Rocca, B, et al. Can brain-derived neurotrophic factor be considered a biomarker for bipolar disorder? An analysis of the current evidence. Brain Sci. (2023) 13:1221. doi: 10.3390/brainsci13081221
80. Lydiard, RB . Worried sick: antidepressants, stress, and inflammation. J Clin Psychiatry. (2007) 68:1613–4. doi: 10.4088/jcp.v68n1021
81. Felger, JC , and Lotrich, FE . Inflammatory cytokines in depression: neurobiological mechanisms and therapeutic implications. Neuroscience. (2013) 246:199–229. doi: 10.1016/j.neuroscience.2013.04.060
82. Laugesen, K , Farkas, DK , Vestergaard, M , Jørgensen, JOL , Petersen, I , and Sørensen, HT . Glucocorticoid use and risk of suicide: a Danish population-based case-control study. World Psychiatry. (2021) 20:142–3. doi: 10.1002/wps.20831
83. Feldman, R . What is resilience: an affiliative neuroscience approach. World Psychiatry. (2020) 19:132–50. doi: 10.1002/wps.20729
84. Lee, DH , Lee, JY , Hong, DY , Lee, EC , Park, SW , Lee, YK, et al. Pharmacological treatment for Neuroinflammation in stress-related disorder. Biomedicine. (2022) 10:2518. doi: 10.3390/biomedicines10102518
85. Dinan, TG , and Cryan, JF . Gut microbiota: a missing link in psychiatry. World Psychiatry. (2020) 19:111–2. doi: 10.1002/wps.20726
86. Zádor, F , Joca, S , Nagy-Grócz, G , Dvorácskó, S , Szűcs, E , Tömböly, C, et al. Pro-inflammatory cytokines: potential links between the endocannabinoid system and the kynurenine pathway in depression. Int J Mol Sci. (2021) 22:5903. doi: 10.3390/ijms22115903
87. Cavaleri, D , Bartoli, F , Capogrosso, CA , Guzzi, P , Moretti, F , Riboldi, I, et al. Blood concentrations of neopterin and biopterin in subjects with depression: a systematic review and meta-analysis. Prog Neuro-Psychopharmacol Biol Psychiatry. (2023) 120:110633. doi: 10.1016/j.pnpbp.2022.110633
88. Kalkman, HO , and Feuerbach, D . Antidepressant therapies inhibit inflammation and microglial M1-polarization. Pharmacol Ther. (2016) 163:82–93. doi: 10.1016/j.pharmthera.2016.04.001
89. Veronese, N , Stubbs, B , Solmi, M , Ajnakina, O , Carvalho, AF , and Maggi, S . Acetyl-L-carnitine supplementation and the treatment of depressive symptoms: a systematic review and Meta-analysis. Psychosom Med. (2018) 80:154–9. doi: 10.1097/PSY.0000000000000537
90. Dyck, MJ . Treatment-resistant depression: a critique of current approaches. Aust N Z J Psychiatry. (1994) 28:34–41. doi: 10.3109/00048679409075843
91. Conway, CR , George, MS , and Sackeim, HA . Toward an evidence-based, operational definition of treatment-resistant depression: when enough is enough. JAMA. Psychiatry. (2017) 74:9–10. doi: 10.1001/jamapsychiatry.2016.2586
Keywords: major depression, treatment resistant depression, TRD, biomarker, cytokines, inflammation
Citation: Mancuso E, Sampogna G, Boiano A, Della Rocca B, Di Vincenzo M, Lapadula MV, Martinelli F, Lucci F and Luciano M (2023) Biological correlates of treatment resistant depression: a review of peripheral biomarkers. Front. Psychiatry. 14:1291176. doi: 10.3389/fpsyt.2023.1291176
Edited by:
Vassilis Martiadis, Asl Napoli 1 Centro, ItalyReviewed by:
Pasquale Scognamiglio, ASL Napoli 3 Sud, ItalyCopyright © 2023 Mancuso, Sampogna, Boiano, Della Rocca, Di Vincenzo, Lapadula, Martinelli, Lucci and Luciano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mario Luciano, bWFyaW8ubHVjaWFub0B1bmljYW1wYW5pYS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.