 Lars-Olov Lundqvist1*†
Lars-Olov Lundqvist1*† Patrik Rytterström2†
Patrik Rytterström2† Mikael Rask3†
Mikael Rask3† David Brunt3†
David Brunt3† Tabita Sellin1†
Tabita Sellin1† Katarina Grim4†
Katarina Grim4† Ingrid Rystedt5†
Ingrid Rystedt5† Agneta Schröder1,6†
Agneta Schröder1,6†- 1University Health Care Research Center, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
- 2Division of Nursing Sciences and Reproductive Health, Department of Health, Medicine and Caring Sciences, Linköping University, Norrköping, Sweden
- 3School of Health and Caring Sciences, Linnaeus University, Växjö, Sweden
- 4Department of Social and Psychological Studies, Karlstad University, Karlstad, Sweden
- 5Division of Society and Health, Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
- 6Department of Nursing, Faculty of Health, Care and Nursing, Norwegian University of Science and Technology (NTNU), Gjövik, Norway
Objective: To investigate the relationship between perceived mental health service provision and quality of life (QoL) as perceived by patients in psychiatric outpatient care.
Methods: A total of 373 adult patients registered at 15 psychiatric outpatient clinics in three regions in central and southern Sweden were included in the study. Survey data were collected using a questionnaire on mental health service provision, symptom severity, recovery, clinical diagnosis, sociodemographics (serving as independent variables) and QoL (serving as the dependent variable). Three aspects of mental health service provision were used: patients’ perceived quality of care, perceived staff-patient interaction, and patient reported psychiatric treatments. Structural equation modelling was used to model the relationship among the variables.
Results: Variables in mental health service provision showed few direct associations with patients’ perceived QoL. Instead, the associations of mental health service provision on QoL were mainly mediated through symptom severity and recovery. These relationships were retained after adjusting for sociodemographic variables and clinical diagnoses. The final model achieved excellent goodness of fit (χ2 = 49.502, p = 0.230, RMSEA = 0.020, CFI = 0.997 and a SRMR = 0.024).
Conclusion: This study shows that mental health service provision is associated with patients’ perceived QoL; however, this association is mostly indirect and mediated by reduced symptom severity and increased recovery. This finding can help inform the design of future interventions to enhance service provision to improve patients’ QoL.
1 Introduction
Psychiatric outpatient care is designed to offer comprehensive, continuous treatment and support for individuals to cope with mental health conditions to enabling them to sustain their everyday lives within their community (1). A primary goal of the provided care is to improve patients’ quality of life (QoL) (2–6), which encompasses their perceptions of life circumstances within their cultural context, considering their aspirations, expectations, and concerns (7). However, beyond psychiatric clinical symptoms (3, 8–11), various sociodemographic, social, occupational, and financial factors may contribute to patients’ QoL. For instance, studies have indicated that older age (12, 13), female gender (12, 14), relationship problems (11, 12), lower education levels (10, 13, 15), and unemployment (11, 13, 16–18) are associated with lower QoL in patients with mental illness.
However, the multitude of variables linked to QoL makes the research in this area fragmented and challenging to comprehend (19). While attempts have been made to propose models demonstrating the relationships between various variables and QoL (20–22), explicit models that effectively guide the understanding of how mental health service provision impacts QoL are still lacking. The relationship between mental health service provision and patients’ perceived QoL is intricate and may not be adequately explained solely through simple correlations. Employing more complex modelling techniques, such as mediation analysis (23, 24), can help elucidate the complex relationships, where an intermediate (mediating) variable or factor may clarify the connection between the quality of mental health services and patients’ perceived QoL.
Upon reviewing existing literature, it becomes evident that while numerous factors influence QoL, only a selected few have been thoroughly investigated as potential mediators impacting QoL. For instance, studies have delved into variables such as recovery (21, 25) and symptom severity (22, 25–27) but have yet to explore many others in depth. Within the scope of recovery, notable components encompass empowerment, agency, and hope (21, 25, 28). This emphasis on recovery has spurred a growing body of research over the past three decades, prompting mental health systems globally to advocate for recovery-oriented services. These services encourage active involvement and choice for individuals seeking treatment and support (29).
While the concept of recovery from mental illness traditionally involved symptom absence and restoration to a pre-illness state, the contemporary viewpoint extends beyond this notion. Modern perspectives emphasize personal growth and development, surpassing the adverse effects of mental illness to establish a fulfilling and meaningful life (30). Therefore, recovery encompasses more than mere symptom remission or a return to prior functioning levels. Interestingly, a meta-analysis of 20 articles highlights that individuals with schizophrenia can experience personal recovery despite persisting symptoms of psychosis (31). Consequently, recovery and symptom severity may function as partially independent markers of mental health status.
Building upon the findings of prior research, a conceptual model (Figure 1) has been proposed. According to this model, variables within mental health services can directly influence QoL or operate via mental health status variables that directly impact QoL. Additionally, sociodemographic variables directly influence QoL alongside patients’ clinical diagnoses.
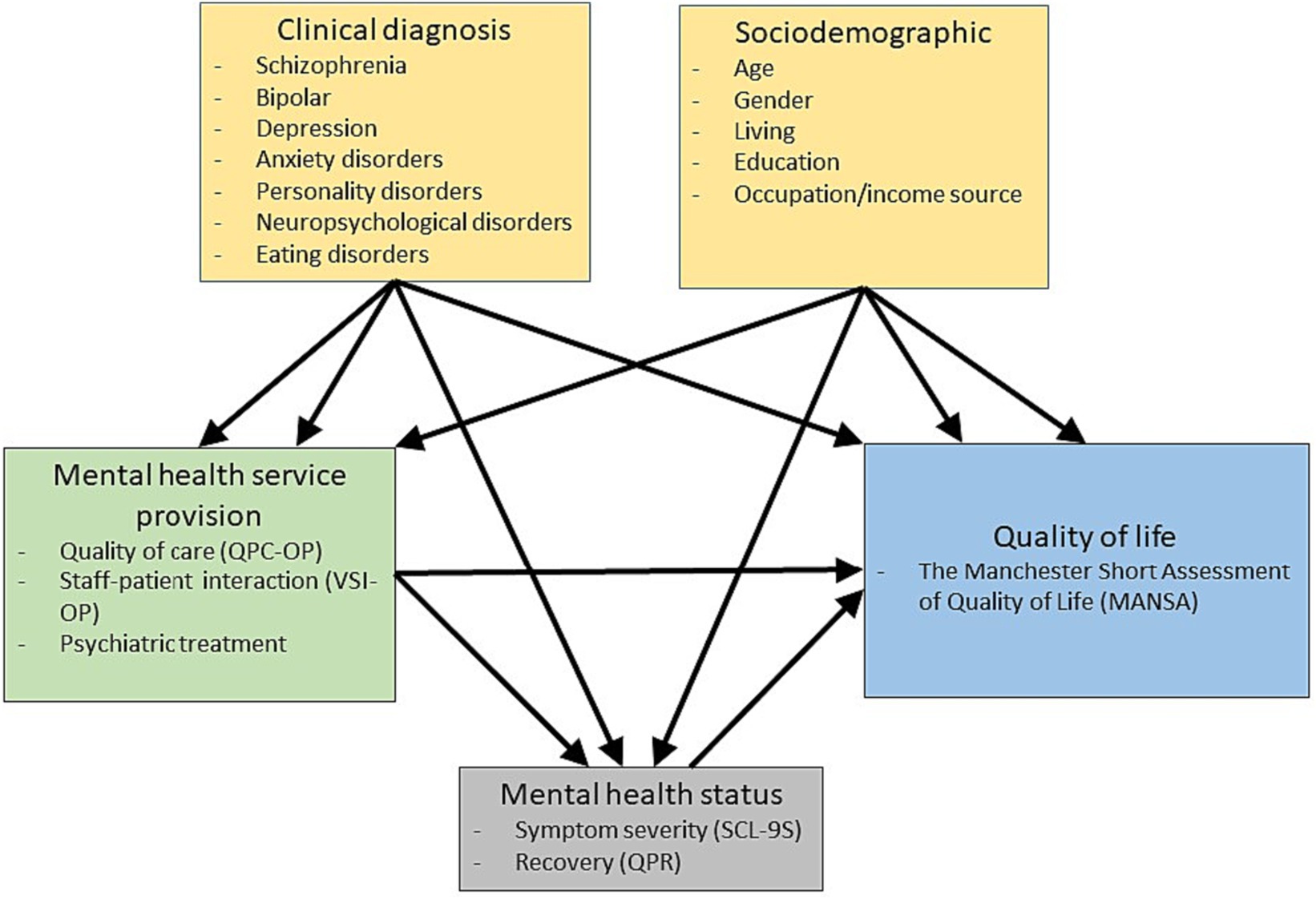
Figure 1. Conceptual model of mental healthcare service provision impact on patients’ perception on quality of life.
1.1 Aim
The aim is to examine the relationship between perceived mental health service provision and QoL among patients in psychiatric outpatient care.
2 Methods
2.1 Participants and procedure
The sample used in this study originated from 15 of totally 17 psychiatric outpatient clinics in three regions in central and southern Sweden (Region Kronoberg, Region Värmland, and Region Örebro län) including approximately 795,000 inhabitants. The clinics serve both the urban and the rural population. They are staffed by multi-professional teams. Patients with different mental illnesses can be admitted to the clinic by self-referral or by referral from other caregivers. A questionnaire containing five standardised instruments (described below) and questions concerning sociodemographic characteristics, diagnoses, and psychiatric treatments was distributed to the 15 outpatient clinics. Inclusion criteria for participants encompassed being 18 years of age or older, being able to understand and read Swedish, and cognitively able to answer the questionnaire. Patients eligible for participation were informed orally and in writing by a designated member of staff, who also ensured that the patients were able to answer the questionnaire in a valid way. Those who gave oral consent were asked to complete the questionnaire anonymously prior to leaving the clinic. A total of 706 questionnaires were returned; however, 333 questionnaires were discarded due to 15% or more missing items in any of the instruments included in the questionnaire. The final sample thus comprised 373 patient questionnaires. The patients were between 18 and 87 years old with a mean age of approximately 35 years. The majority of patients were women, had upper secondary education but only one in five patients was working. Characteristics of the study participants are shown in Table 1.
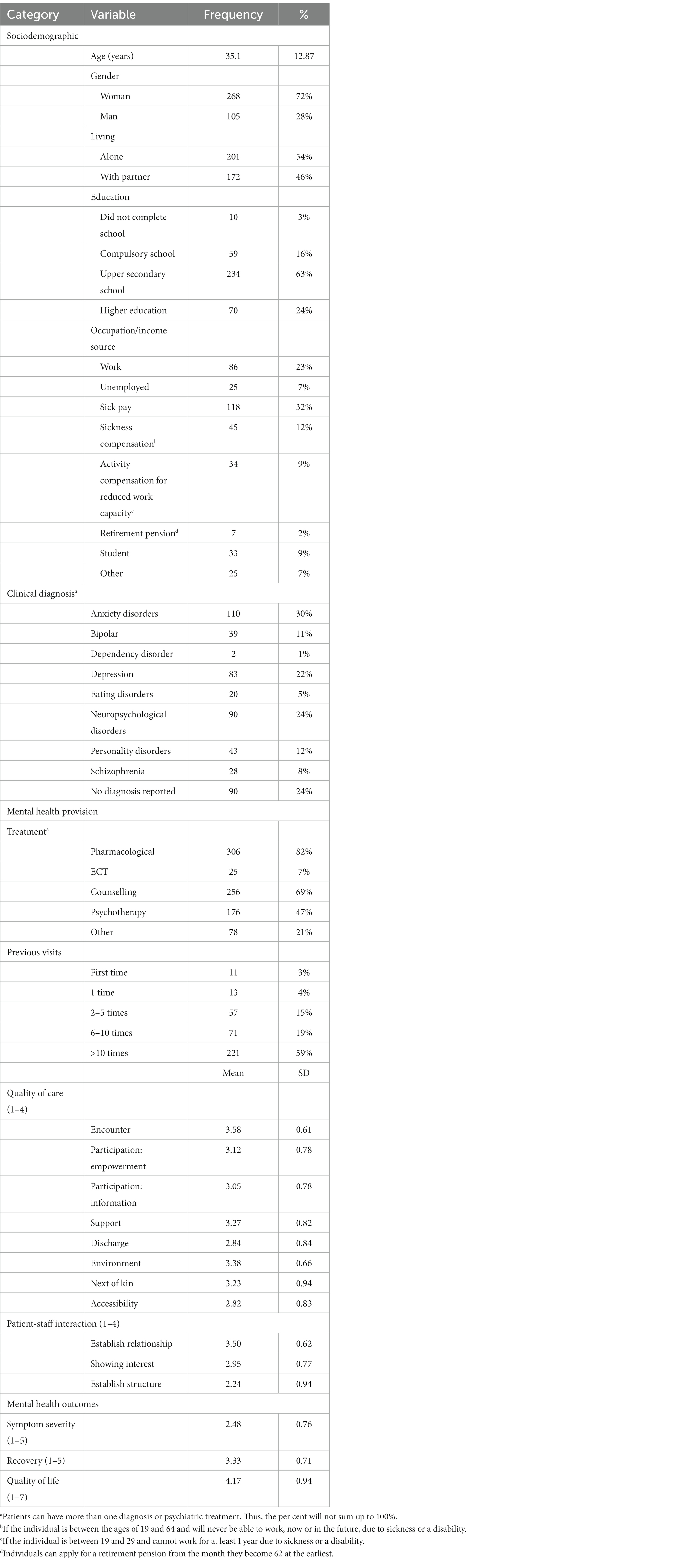
Table 1. Participant characteristics (N = 373).
2.2 Measurements
2.2.1 Quality of life
The Swedish version (32) of the Manchester Short Assessment of Quality of Life (MANSA (33)) was used to assess the perceived QoL. The MANSA contains 12 items on global life satisfaction, job, financial situation, friendships, leisure activities, accommodation, personal safety, people that the person lives with, family and health. Items are scored on a 7-point scale from 1 (could not be worse) to 7 (could not be better). A higher score indicates perceived better QoL. The Swedish version has a satisfactory internal consistency with a Cronbach’s alpha of 0.81 (32).
2.2.2 Mental health service provision
The Quality in Psychiatric Care – Outpatient (QPC-OP (34)) instrument was used to assess patients’ perception of the quality of care. The QPC-OP consists of 30 items covering 8 dimensions: encounter (6 items), participation-empowerment (3 items), participation-information (5 items), discharge (3 items), support (4 items), environment (3 items), next of kin (2 items), and accessibility (4 items). Each item begins with the wording “I experience that…” and is scored on a 4-point Likert-type scale from 1 (totally disagree) to 4 (totally agree) with a ‘not applicable option.’ A higher score represents perceived better quality of care. The QP-OP has an excellent internal consistency with a Cronbach’s alpha of 0.95 (34).
The Verbal and Social Interaction questionnaire for Psychiatric Outpatient Care (VSI-OP (35)) was used to assess the patients’ perceptions of the patient-staff relationship. The VSI-OP contains 17 items covering 3 dimensions: relationship (inviting the patient to establish a relationship, 6 items), interest (showing interest in the patients’ feelings, experiences, and behaviour, 6 items) and helping (helping the patients to establish structure and routines in their everyday life, 5 items). The items are scored on 4-point Likert-type scales from 1 (not at all) to 4 (very high degree). A higher score reflects a perceived better patient-staff relationship. The internal consistency for VSI-OP is satisfactory, with a Cronbach’s alpha of 0.81.
Psychiatric treatment. Patients were asked to report which psychiatric treatments they received from the outpatient clinic, e.g., pharmacological, electroconvulsive therapy, counselling, psychotherapy, and other psychiatric treatment. Patients could report having more than one treatment.
2.2.3 Mental health status
The Symptom Checklist 9 short index (SCL-9S (36)) was used to measure general psychological distress of patients. The SCL-9S is a unidimensional measure that comprises the nine items most indicative of each of the nine subscales of the Symptom Checklist-90-R (37). Each item is scored on a five-point Likert-type scale from 1 (not at all) to 5 (very much). The internal consistency for SCL-9S is satisfactory, with a Cronbach’s alpha of 0.75 (36).
Questionnaire about the Process of Recovery (QPR). The Swedish 16-item one-factor version (28) of the original 22-item two-factor version (38) was used. Each item is scored using a five-point Likert-type scale from 1 (disagree strongly) to 5 (agree strongly). The Cronbach’s alpha internal consistency of the QPR was excellent, with a Cronbach’s alpha of 0.92 (28).
2.2.4 Sociodemographic characteristics
The following sociodemographic variables were used: age, gender, living with partner, education level, and occupation/income source.
2.2.5 Self-reported clinical diagnoses
The patients reported their diagnoses in free text on the questionnaire. The diagnoses were then categorised into eight categories: anxiety, bipolar, dependency disorder, depression, eating disorders, neuropsychological disorders, personality disorders, and schizophrenia. Patients could report having more than one diagnosis.
2.3 Data analysis
IBM SPSS 27 and AMOS 25.0 were used to analyse the data. The 333 questionnaires with 15% or more missing items were discarded prior to analysis. Imputation of missing values was performed for the remaining 373 questionnaires using the SPSS expectation-maximisation procedure. We used structural equation modelling to test the proposed model because of greater flexibility in model specification and estimation options, such as simultaneously testing the full model (24, 39). To examine direct and indirect associations we used bootstrapping because it does not make assumptions about the distribution of the variables, which circumvents deviations from multivariate normality (39).
Based on the conceptual model (Figure 1), we specified a testable model and analysed it stepwise. First, we tested the model for the association of variables in mental health care service provision with mental health status variables and QoL. We used an iterative process by deleting non-significant variables and modifying the model according to the modification indices until no more improvements could be made. Once the relationships were established, sociodemographic variables and clinical diagnoses were entered into the model to evaluate whether they still hold when adjusted for these variables.
Model adequacy was assessed with different fit indexes, including the chi-square test, the comparative fit index (CFI), the standardised root mean square residual (SRMR), and the root mean square error of approximation (RMSEA). A non-significant chi-square reflects agreement between the model and the data. CFI values ≥0.90 and ≥0.95 and SRMR and RMSEA values ≤0.08 and ≤0.05 were considered adequate and excellent levels of goodness of fit, respectively (23).
Differences between the goodness-of-fit indexes of the models were analysed to determine which model better fitted the data. Differences no greater than 0.01 between the CFI values (0.030 for the SRMR and 0.015 between the RMSEA values) were considered irrelevant when comparing the models (40). In such cases we chose the model that accomplished the desired level of explanation with as few parameters or predictor variables as possible.
3 Results
Twenty significant relationships were found after the iterative testing procedure (Table 2), and we reached a final mediation model (Table 3) that received excellent goodness of fit for all evaluated goodness-of-fit indices. The non-significant chi-square shows that the model did not deviate significantly from observed data. The R2 indicates that the model explained 55% of the variance in quality of life, which was deemed adequate. Adjustment of the model with sociodemographic and diagnosis variables had a small and non-significant effect on the model fit (Δχ2 = 17.04 with a Δdf = 21 giving a p = 0.71, a ΔRMSEA = 0.011, and a ΔCFI = 0.001), demonstrating that the associations between the variables in mental health service provision and QoL were not affected by the observed socioeconomic or diagnosis variables.
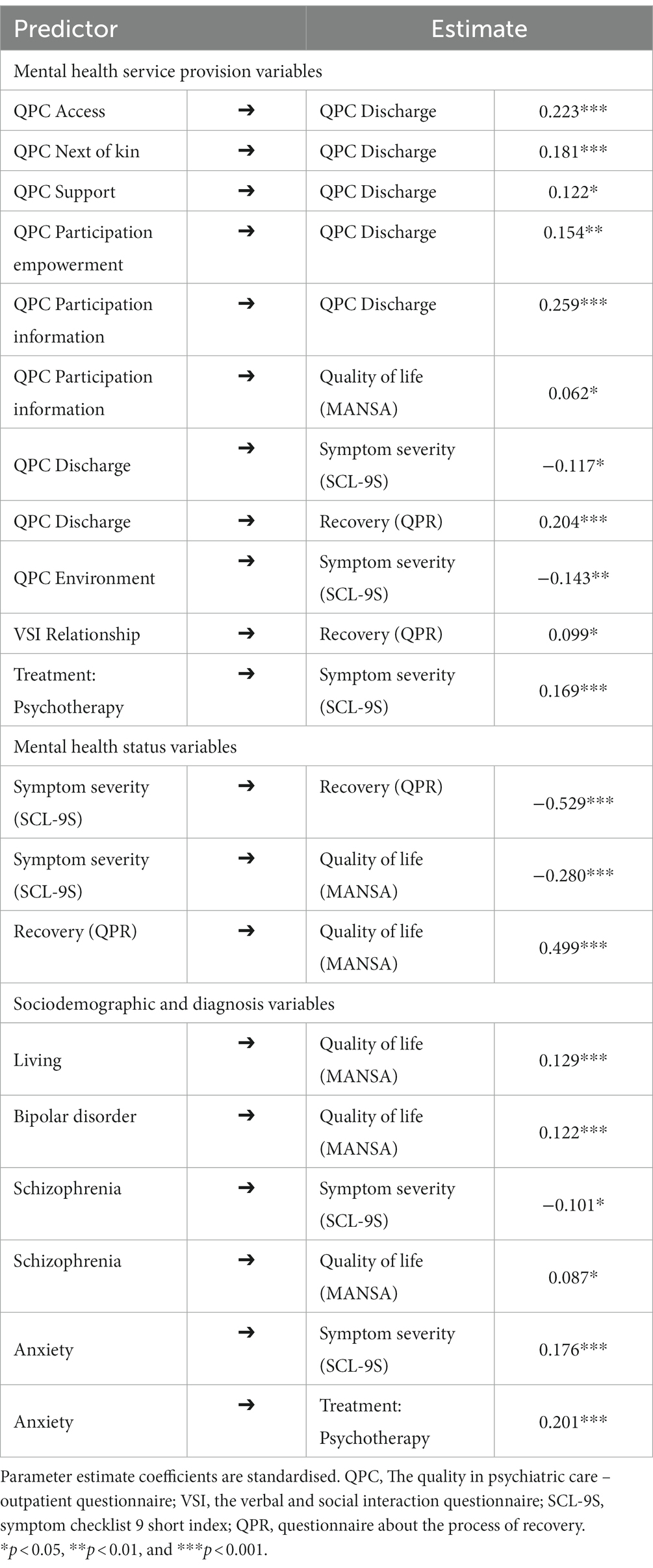
Table 2. Standardised regression weights.
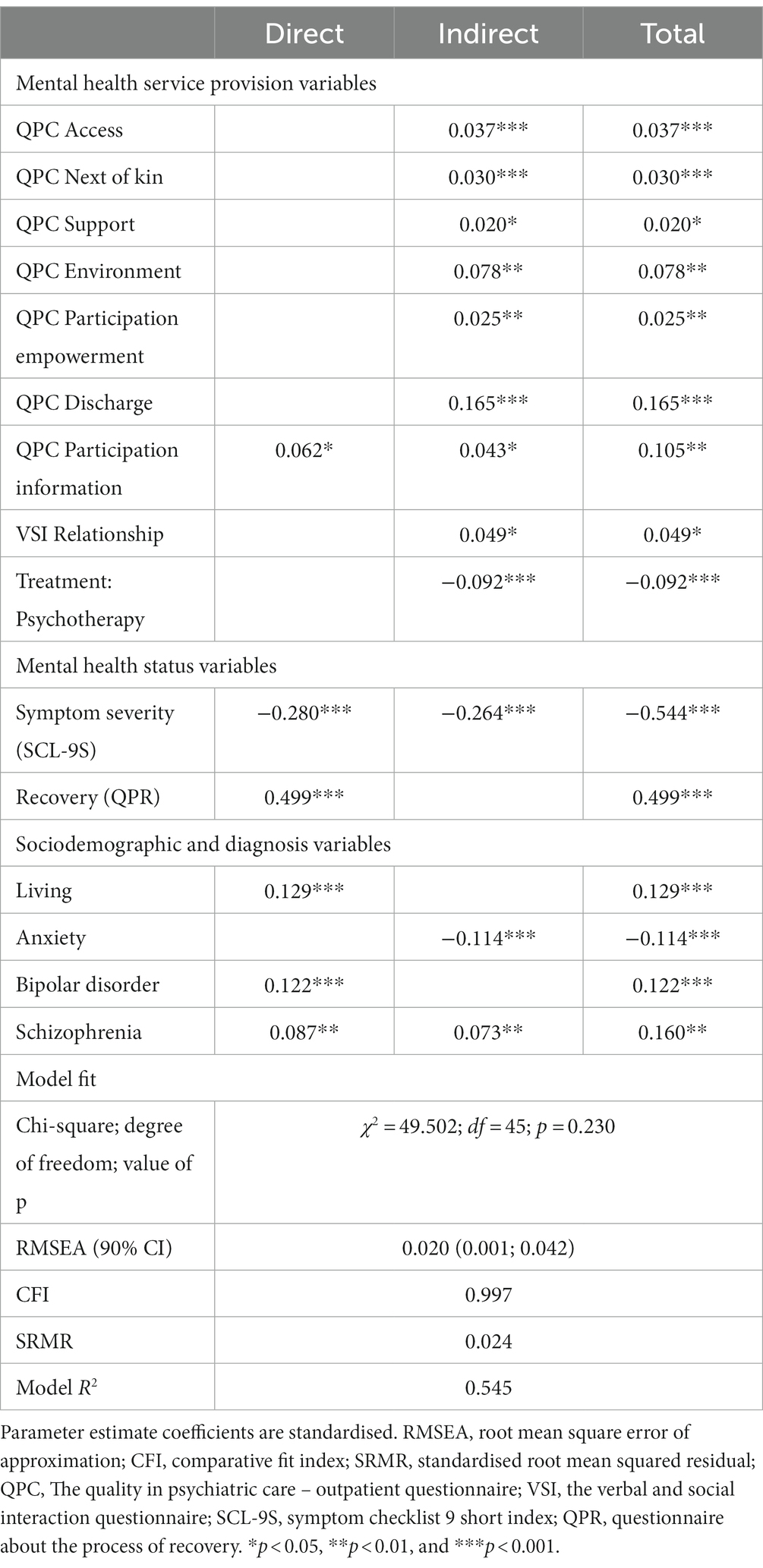
Table 3. Final mediation model of direct, indirect, and total effects on quality of life.
The final model indicated that the relationship between the variables in mental health service provision and the patient’s perceived QoL is relatively complex. As shown in Figure 2, QoL was directly associated with six variables, whereas only one, participation information, was a service provision variable. Most service provision variables were mediated by the mental health status variables (symptom severity and recovery) mediating QoL. Among the quality-of-care variables, all but one were mediated by the discharge variable. Moreover, the patient-staff relationship, measured by the VSI, had an indirect association with QoL and a significant direct association with recovery. One treatment variable, psychotherapy, had a significant association with QoL, i.e., a mediated association via symptom severity and recovery, resulting in a total negative association with QoL.
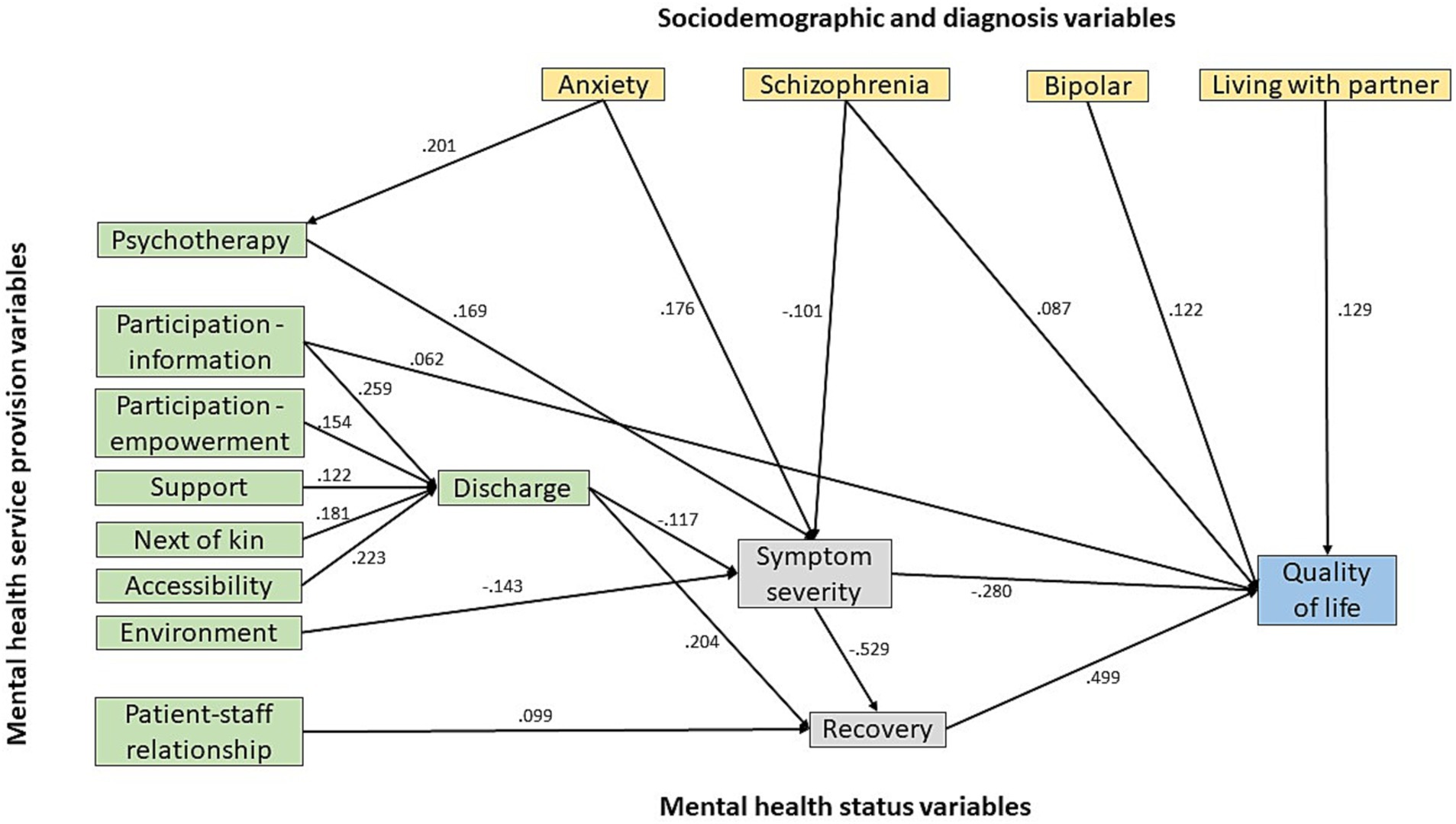
Figure 2. Final mediation model of the impact of mental health service provision on psychiatric outpatients’ perception of quality of life. Coefficients are standardised.
Although sociodemographic and diagnosis variables had no significant effects on the model fit, some relationships with QoL were significant. Living with partner had a significant and direct positive association with QoL. For clinical diagnosis, bipolar disorder, schizophrenia, and anxiety had a significant positive association with QoL. Notably, the relationship between patients’ anxiety and QoL was somewhat complex. Patients with anxiety were more likely than those with other diagnoses to receive psychotherapy. Those receiving psychotherapy (whether or not with anxiety) perceived slightly more severe symptoms and less QoL than those receiving other psychiatric treatments, resulting in a negative association between anxiety and QoL. In contrast, patients diagnosed with schizophrenia and bipolar disorders reported better QoL than patients with other diagnoses.
4 Discussion
This study examined the relationship between perceived mental health service provision and QoL among patients in psychiatric outpatient care. The final model achieved excellent goodness of fit, showing that variables in mental health service provision mainly had an indirect effect on patients’ perceived QoL and that this effect was mediated by symptom severity and recovery.
This result is consistent with research indicating that service provision variables have a minor direct association with perceived QoL, suggesting that other factors beyond mental health care service are more impactful (5, 31, 40). Moreover, the results correspond to studies using complex mediator models. For instance, Fleury and colleagues (21) found that sociodemographic variables (gender and living) and clinical diagnosis variables (mood disorders and substance use disorders) were directly related to patients’ perceived QoL but that only two of the service provision variables (service continuity and adequacy of help) were directly associated with QoL. Similarly, the present study shows that recovery serves as an important mediator but that symptom severity, which was not assessed by Fleury and colleagues (21), also acts as a mediator and has a similar magnitude of association with QoL, suggesting that both recovery and symptom severity have a vital role for patients’ perceived QoL. However, in this study the association of symptom severity with QoL is primarily mediated by recovery, which correspond with findings by Saavedra and colleagues (24), suggesting that the symptom severity and QoL association may depend on the presence of recovery, which aligns with previous research (e.g., (30)). The present results thus suggest that symptom relief is unnecessary for recovery, but in relation to QoL, the absence of symptom relief will reduce recovery, resulting in a negative association with QoL. Hence, the model indicates that recovery would have less impact on patients’ perceived QoL if there was no symptom relief.
Surprisingly, the discharge dimension was a mediator between most of the other service provision variables and recovery. It is not apparent why discharge has this role. However, visits to outpatient clinics are often intermittent and a regular discharge procedure does not always occur. Thus, the QPC-OP discharge dimension items are mainly about closure and the future. These aspects can be related to findings by Fleury and colleagues (21), who showed that recovery, which included elements found in patients’ experience at discharge, was a mediating factor between service continuity and QoL. Discharge may thus be a significant event and a crucial component of the treatment process. As such, discharge is a creative process that can be customised to meet each patient’s unique needs and comprehensively address them across multiple health systems in a continuous and coordinated manner (41). As mentioned above, the discharge process in outpatient care is less formal, and in this study, it was measured by questions including aspects of closure and the future. These questions encompass parts of the personal agency, an essential factor in understanding the ‘service provision-recovery-quality of life’ relationship (22).
From a clinical perspective, this finding raises questions about whether interventions in outpatient psychiatric care need to focus more on agency rather than providing more support and that it is important to include questions about closure and the future from the start of the care process. Prospects encouraging hope can be positive for perceived QoL (42). The quality-of-service provision may also increase patients’ capacity, allowing them to influence their future (43), potentially affecting their QoL. Our model aligns with the assumption that the experience of controlling and being able to master situations is an important recovery factor for developing a higher level of QoL. In this regard, our findings correspond with a holistic perspective on mental health service providers aiming to support recovery by focusing on both symptom reduction and increased well-being related to hope, self-esteem, social connectedness, and a sense of control of one’s life (35–47). However, the current outcome on the role of the discharge dimension should be taken with caution until it has been replicated in independent studies. Further research is needed to clarify the link between the quality of the service provided and the patients’ view of their future.
In addition to the discharge issues, the present results show that the patient-staff relationship, as measured by the VSI, may have an independent effect on recovery. Among the three elements of the patient-staff relationship measured by the VSI-OP, only Inviting the patient to establish a relationship had an association with QoL. This association was mediated entirely by recovery. In other words, the greater the patient-staff relationship, the greater the recovery and thus better QoL. A good patient-staff relationship has been noted as an important factor that can make a difference in recovery during an episode of mental illness, including involuntary admission (48). Using the VSI-OP, Rask and colleagues (35) showed that patients reported that Inviting the patient to establish a relationship, as well as, Showing interest in patients’ feelings, experiences, and behaviour were rated as the most frequent actions performed by staff. In another study, using VSI for supported housing, the residents rated inviting the patient to establish a relationship as the most frequently performed and the most important facet of the patient-staff interaction (49). These findings confirm Green et al. (50), who reported that patients value a staff perceived as competent, caring, trustworthy, and trusting and that these factors were important for patient recovery. This position is in line with our findings that a positive patient-staff relationship, including staff showing interest in the patients’ thoughts and experiences, is vital for patient recovery.
Concerning clinical diagnoses, schizophrenia and bipolar disorders were directly associated with QoL. The associations were positive, indicating that patients with schizophrenia and bipolar disorder perceived QoL better than patients with other mental diagnoses. In addition, schizophrenia was associated with less symptom severity, leading to a positive indirect association with QoL. This observation aligns with previous findings showing that patients with schizophrenia report higher self-reported QoL than patients with other mental disorders (51). However, our finding differed from the finding of Priebe et al. (51) that schizophrenia is associated with more severe reported symptoms.
Anxiety was not directly associated with QoL. Instead, the association between anxiety and QoL was mediated by psychotherapy and reported symptom severity, indicating that the relationship between anxiety and QoL is complex. Specifically, patients with anxiety reported receiving more psychotherapy compared to patients with other mental diagnoses and receiving psychotherapy was associated with reporting greater symptom severity, suggesting that patients with anxiety in ongoing psychotherapy also struggle with severe symptoms. This circumstance may thus explain why psychotherapy was associated with greater reported symptom severity.
Concerning the sociodemographic variables only one, living with a partner, was positively associated with QoL. Although associations between sociodemographic variables and QoL seem to depend on the study population, similar results have been demonstrated in studies on patients with schizophrenia (52).
4.1 Methodological considerations
The measurement of QoL in mental health services depends on the assessment instrument used. We chose the MANSA because it is an established and widely used instrument for QoL assessment in mental health practice and has good psychometric properties in Swedish patients who receive psychiatric outpatient services. Because QoL instruments may differ in definition and item content, results based on other tools may deviate from those we observed. Yet, our results are largely consistent with comparable results in studies using other QoL measures (e.g., (20, 21, 26)). In addition, the rigorous method of structural equation modelling made it possible to investigate the complex network of mediating variables and to model associations and hypothesised causal mechanisms between service provision and QoL.
This study has some limitations. First, the model hinges on the study variables. We have chosen variables based on previous research, which does not rule out the possibility that other variables may have equal or better predictive values than those we chose. Second, as in any research involving recall, there exists the potential for the results to be influenced by recall bias. Nevertheless, in our study, patients complete the questionnaire immediately upon leaving the clinic. The short duration between their visit/consultation and answering the questionnaire significantly reduces the likelihood of substantial recall bias affecting the outcomes. Third, although the study included patients from several clinics in three regions in Sweden, the results may not be directly generalisable to other countries, especially those with different healthcare systems. Fourth, because the present data are cross-sectional, we cannot determine the temporal and causal relationships of the variables. This model must therefore be assessed in terms of the model matching the observed data, given that the model reflects an existing temporal/causal relationship. Thus, the results do not reflect actual causal relationships. Therefore, longitudinal or experimental studies should be performed to investigate the causality of the effects of mental health service provision on patients’ QoL. In such an effort, the present study can thus be used to scrutinise potential causal relationships more closely.
5 Conclusion
The present study shows that patients’ perception of mental health service provision is positively associated with their perceived QoL; however, this association is mostly indirect and mediated by reduced symptom severity and increased recovery. This finding can help design future interventions to enhance service provision and thus promote patients’ QoL. Further studies are needed to capture a causal path to QoL.
Data availability statement
The datasets presented in this article are not readily available because of ethical restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Swedish Ethical Review Authority. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because the participants gave verbal informed consent to participate.
Author contributions
L-OL: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. PR: Conceptualization, Writing – review & editing. MR: Conceptualization, Writing – review & editing. DB: Conceptualization, Writing – review & editing. TS: Conceptualization, Writing – review & editing. KG: Conceptualization, Writing – review & editing. IR: Conceptualization, Writing – review & editing. AS: Conceptualization, Funding acquisition, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Fund for Rehabilitation and Medical Research (Fonden för Rehabilitering och Medicin) and the Region Örebro County Research Committee (Forskningskommittén i Region Örebro län).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Björkman, T, Hansson, L, Svensson, B, and Berglund, I. What is important in psychiatric outpatient care? Quality of care from the patient's perspective. Int J Qual Health Care. (1995) 7:355–62. doi: 10.1093/intqhc/7.4.355
2. Gigantesco, A, and Giuliani, M. Quality of life in mental health services with a focus on psychiatric rehabilitation practice. Annali dell’Istituto superiore di sanita. (2011) 47:363–72. doi: 10.4415/ANN_11_04_07
3. Hansson, L . Determinants of quality of life in people with severe mental illness. Acta Psychiatr Scand Suppl. (2006) 113:46–50. doi: 10.1111/j.1600-0447.2005.00717.x
4. Holloway, F, and Carson, J. Quality of life in severe mental illness. Int Rev Psychiatry. (2002) 14:175–84. doi: 10.1080/09540260220145000
5. Petkari, E, and Pietschnig, J. Associations of quality of life with service satisfaction in psychotic patients: a meta-analysis. PLoS One. (2015) 10:e0135267. doi: 10.1371/journal.pone.0135267
6. Fleury, MJ, Grenier, G, Bamvita, JM, Tremblay, J, and Schmitz, N. Predictors of quality of life in a longitudinal study of users with severe mental disorders. Health Qual Life Outcomes. (2013) 11:92. doi: 10.1186/1477-7525-11-92
7. The WHOQoL Group . The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. (1995) 41:1403–9. doi: 10.1016/0277-9536(95)00112-K
8. Cramer, V, Torgersen, S, and Kringlen, E. Mood disorders and quality of life. A community study. Nord J Psychiatry. (2010) 64:58–62. doi: 10.3109/08039480903287565
9. Saarni, SI, Viertio, S, Perala, J, Koskinen, S, and Lonnqvist, J. Quality of life of people with schizophrenia, bipolar disorder and other psychotic disorders. Br J Psychiatry. (2010) 197:386–94. doi: 10.1192/bjp.bp.109.076489
10. Desalegn, D, Girma, S, and Abdeta, T. Quality of life and its association with psychiatric symptoms and socio-demographic characteristics among people with schizophrenia: a hospital-based cross-sectional study. PLoS One. (2020) 15:e0229514. doi: 10.1371/journal.pone.0229514
11. Wilmer, MT, Anderson, K, and Reynolds, M. Correlates of quality of life in anxiety disorders: review of recent research. Curr Psychiatry Rep. (2021) 23:77–9. doi: 10.1007/s11920-021-01290-4
12. Dong, M, Lu, L, Zhang, L, Zhang, YS, and Ng, CH. Quality of life in schizophrenia: a meta-analysis of comparative studies. Psychiatry Q. (2019) 90:519–32. doi: 10.1007/s11126-019-09633-4
13. Cho, Y, Lee, JK, Kim, DH, Park, JH, and Choi, M. Factors associated with quality of life in patients with depression: a nationwide population-based study. PLoS One. (2019) 14:e0219455. doi: 10.1371/journal.pone.0219455
14. Colillas-Malet, E, Prat, G, Espelt, A, and Juvinyà, D. Gender differences in health-related quality of life in people with severe mental illness. PLoS One. (2020) 15:e0229236. doi: 10.1371/journal.pone.0229236
15. Hasan, AA, and Tumah, H. Determinants of quality of life among people diagnosed with schizophrenia at outpatient clinics. Perspect Psychiatr Care. (2019) 55:30–9. doi: 10.1111/ppc.12278
16. Bond, GR, Resnick, SG, Drake, RE, Xie, H, and McHugo, GJ. Does competitive employment improve nonvocational outcomes for people with severe mental illness? J Consult Clin Psychol. (2001) 69:489–501. doi: 10.1037/0022-006X.69.3.489
17. Hsiao, CY, Hsieh, MH, Tseng, CJ, Chien, SH, and Chang, CC. Quality of life of individuals with schizophrenia living in the community: relationship to socio-demographic, clinical and psychosocial characteristics. J Clin Nurs. (2012) 21:2367–76. doi: 10.1111/j.1365-2702.2012.04067.x
18. Eklund, M, Hansson, L, and Bejerholm, U. Relationships between satisfaction with occupational factors and health-related variables in schizophrenia outpatients. Soc Psychiatry Psychiatr Epidemiol. (2001) 36:79–85. doi: 10.1007/s001270050293
19. Bakas, T, McLennon, SM, Carpenter, JS, Buelow, JM, Otte, JL, and Hanna, KM. Systematic review of health-related quality of life models. Health Qual Life Outcomes. (2012) 10:134. doi: 10.1186/1477-7525-10-134
20. Berghöfer, A, Martin, L, Hense, S, Weinmann, S, and Roll, S. Quality of life in patients with severe mental illness: a cross-sectional survey in an integrated outpatient health care model. Qual Life Res. (2020) 29:2073–87. doi: 10.1007/s11136-020-02470-0
21. Fleury, MJ, Grenier, G, and Bamvita, JM. Associated and mediating variables related to quality of life among service users with mental disorders. Qual Life Res. (2018) 27:491–502. doi: 10.1007/s11136-017-1717-z
22. Ho, WW, Chiu, MY, Lo, WT, and Yiu, MG. Recovery components as determinants of the health-related quality of life among patients with schizophrenia: structural equation modelling analysis. Austr New Zealand J Psychiatr. (2010) 44:71–84. doi: 10.3109/00048670903393654
23. Kline, RB . Principles and practice of structural equation modelling. 4th ed. New York: Guilford Publications (2016).
24. Rijnhart, JJ, Lamp, SJ, Valente, MJ, Mac Kinnon, DP, and Twisk, JW. Mediation analysis methods used in observational research: a scoping review and recommendations. BMC Med Res Methodol. (2021) 21:226–17. doi: 10.1186/s12874-021-01426-3
25. Saavedra, J, Brzeska, J, Matías-García, JA, and Arias-Sánchez, S. Quality of life and psychiatric distress in people with serious mental illness, the role of personal recovery. Psychol Psychother Theory Res Pract. (2023) 96:525–41. doi: 10.1111/papt.12451
26. de Beurs, E, Carlier, I, and van Hemert, A. Psychopathology and health-related quality of life as patient-reported treatment outcomes: evaluation of concordance between the brief symptom inventory (BSI) and the short form-36 (SF-36) in psychiatric outpatients. Qual Life Res. (2022) 31:1461–71. doi: 10.1007/s11136-021-03019-5
27. Eklund, M, and Bäckström, M. A model of subjective quality of life for outpatients with schizophrenia and other psychoses. Qual Life Res. (2005) 14:1157–68. doi: 10.1007/s11136-004-2960-7
28. Argentzell, E, Hultqvist, J, Neil, S, and Eklund, M. Measuring personal recovery–psychometric properties of the Swedish questionnaire about the process of recovery (QPR-Swe). Nord J Psychiatry. (2017) 71:529–35. doi: 10.1080/08039488.2017.1346144
29. Mahdanian, AA, Laporta, M, Drew Bold, N, Funk, M, and Puras, D. Human rights in mental healthcare; a review of current global situation. Int Rev Psychiatry. (2023) 35:150–62. doi: 10.1080/09540261.2022.2027348
30. Davidson, L, O’Connell, MJ, Tondora, J, and Lawless, M. Recovery in serious mental illness: a new wine or just a new bottle? Prof Psychol Res Pract. (2005) 36:480.
31. Van Eck, RM, Burger, TJ, Vellinga, A, Schirmbeck, F, and de Haan, L. The relationship between clinical and personal recovery in patients with schizophrenia spectrum disorders: a systematic review and meta-analysis. Schizophr Bull. (2018) 44:631–42. doi: 10.1093/schbul/sbx088
32. Björkman, T, and Svensson, B. Quality of life in people with severe mental illness. Reliability and validity of the Manchester short assessment of quality of life (MANSA). Nord J Psychiatry. (2005) 59:302–6. doi: 10.1080/08039480500213733
33. Priebe, S, Huxley, P, Knight, S, and Evans, S. Application and results of the Manchester short assessment of quality of life (MANSA). Int J Soc Psychiatry. (1999) 45:7–12. doi: 10.1177/002076409904500102
34. Schröder, A, Ahlström, G, Wilde-Larsson, B, and Lundqvist, LO. Psychometric properties of the quality in psychiatric care–outpatient (QPC–OP) instrument. Int J Ment Health Nurs. (2011) 20:445–53. doi: 10.1111/j.1447-0349.2011.00741.x
35. Rask, M, Lundqvist, L-O, Schröder, A, and Brunt, D. Psychometric properties of the verbal and social interaction questionnaire for psychiatric outpatient care (VSI-OP), staff and patient versions. Issues Ment Health Nurs. (2022) 43:936–43. doi: 10.1080/01612840.2022.2072549
36. Lundqvist, LO, and Schröder, A. Evaluation of the SCL-9S, a short version of the symptom checklist-90-R, on psychiatric patients in Sweden by using Rasch analysis. Nord J Psychiatry. (2021) 75:538–46. doi: 10.1080/08039488.2021.1901988
37. Derogatis, LR . SCL-90-R, administration, scoring and procedures manual-II for the R (evised) version and other instruments of the psychopathology rating scale series. Townson: Clinical Psychometric Research (1992).
38. Neil, ST, Kilbride, M, Pitt, L, Nothard, S, and Welford, M. The questionnaire about the process of recovery (QPR): a measurement tool developed in collaboration with service users. Psychosis. (2009) 1:145–55. doi: 10.1080/17522430902913450
39. Preacher, KJ, and Hayes, AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
40. Chen, FF . Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Model Multidiscip J. (2007) 14:464–504. doi: 10.1080/10705510701301834
41. Alghzawi, HM . Psychiatric discharge process. Int Schol Res Not. (2012) 2012:638943. doi: 10.5402/2012/638943
42. Laranjeira, C, and Querido, A. Hope and optimism as an opportunity to improve the positive mental health demand. Front Psychol. (2022) 13:827320. doi: 10.3389/fpsyg.2022.827320
43. Pinfold, V, Sweet, D, Porter, I, Quinn, C, and Byng, R. Improving community health networks for people with severe mental illness: a case study investigation. Health Serv Delivery Res. (2015) 3:1–234. doi: 10.3310/hsdr03050
44. Hansson, L, and Björkman, T. Are factors associated with subjective quality of life in people with severe mental illness consistent over time? – a 6-year follow-up study. Qual Life Res. (2007) 16:9–16. doi: 10.1007/s11136-006-9119-7
45. James, K, and Quirk, A. The rationale for shared decision making in mental health care: a systematic review of academic discourse. Ment Health Rev J. (2017) 22:152–65. doi: 10.1108/MHRJ-01-2017-0009
46. Onken, SJ, Craig, CM, Ridgway, P, Ralph, RO, and Cook, JA. An analysis of the definitions and elements of recovery: a review of the literature. Psychiatr Rehabil J. (2007) 31:9–22. doi: 10.2975/31.1.2007.9.22
47. Slade, M . Personal recovery and mental illness: a guide for mental health professionals. Cambridge: Cambridge University Press (2009).
48. Wyder, M, Bland, R, Blythe, A, Matarasso, B, and Crompton, D. Therapeutic relationships and involuntary treatment orders: service users’ interactions with healthcare professionals on the ward. Int J Ment Health Nurs. (2015) 24:181–9. doi: 10.1111/inm.12121
49. Brunt, D, and Rask, M. Resident and staff perceptions of the content of their relationship in supported housing facilities for people with psychiatric disabilities. J Multidiscip Healthc. (2018) 11:673–81. doi: 10.2147/JMDH.S179322
50. Green, CA, Polen, MR, Janoff, SL, Castleton, DK, and Wisdom, JP. Understanding how clinician-patient relationships and relational continuity of care affect recovery from serious mental illness: STARS study results. Psychiatr Rehabil J. (2008) 32:9–22. doi: 10.2975/32.1.2008.9.22
51. Priebe, S, Reininghaus, U, McCabe, R, Burns, T, Eklund, M, and Hansson, L. Factors influencing subjective quality of life in patients with schizophrenia and other mental disorders: a pooled analysis. Schizophr Res. (2010) 121:251–8. doi: 10.1016/j.schres.2009.12.020
Keywords: mediator model, mental health, outpatient psychiatric care, service provision, structural equation modelling, quality of life
Citation: Lundqvist L-O, Rytterström P, Rask M, Brunt D, Sellin T, Grim K, Rystedt I and Schröder A (2024) Influence of mental health service provision on the perceived quality of life among psychiatric outpatients: associations and mediating factors. Front. Psychiatry. 14:1282466. doi: 10.3389/fpsyt.2023.1282466
Edited by:
Jing Wei, Peking Union Medical College Hospital (CAMS), ChinaReviewed by:
Jose Antonio Matias-Garcia, Sevilla University, SpainMatteo Monzio Compagnoni, University of Milano-Bicocca, Italy
Copyright © 2024 Lundqvist, Rytterström, Rask, Brunt, Sellin, Grim, Rystedt and Schröder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lars-Olov Lundqvist, bGFycy1vbG92Lmx1bmRxdmlzdEBvcnUuc2U=