 Agnieszka Kułak-Bejda1*
Agnieszka Kułak-Bejda1* Andrei Shpakou2Natallia Khvoryk3Liudmila Hutsikava3
Andrei Shpakou2Natallia Khvoryk3Liudmila Hutsikava3 Ilknur Aydin Avci4Dilek Celik Eren4
Ilknur Aydin Avci4Dilek Celik Eren4 Lambrini Kourkouta5
Lambrini Kourkouta5 Areti Tsaloglidou5
Areti Tsaloglidou5 Konstantinos Koukourikos5
Konstantinos Koukourikos5 Napoleon Waszkiewicz1
Napoleon Waszkiewicz1- 1Department of Psychiatry, Medical University of Białystok, Białystok, Poland
- 2Department of Integrated Medical Care, Medical University of Białystok, Białystok, Poland
- 3Department of Obstetrics and Gynecology, Grodno State Medical University, Grodno, Belarus
- 4Department of Nursing, Faculty of Health Sciences, Ondokuz Mayıs University, Samsun, Türkiye
- 5Department of Nursing, International Hellenic University, Thessaloniki, Greece
Introduction: Life optimism is an inseparable element accompanying every human being. It takes different values depending on the life situation. The present study aimed to measure the level of dispositional optimism in postpartum and pregnant women, compared to women who are not pregnant and have never given birth in Poland, Greece, Turkey, Belarus, and Russia, depending on the level of life satisfaction, risk of depression and mental health.
Materials and methods: A case–control study was carried out among 2017 women, including 584 pregnant women, 528 postpartum women, and 906 women who had never been pregnant and had never given birth (control group) from Poland, Greece, Turkey, Belarus, and Russia.
The study used the LOT-R Life Orientation Test, the Beck Depression Scale (BDI), the Satisfaction With Life Scale (SWLS), the GHQ- 28, and the Edinburgh Postnatal Depression Scale (EPDS) – only in the postpartum group.
Results: Women from the control group showed an average level of optimism, obtaining an average of 16 points in Belarus, 13.4 points in Poland, 13.3 points in Greece, 13.5 points in Turkey, and Russia – 16.3 points. Pregnant women from Belarus had a high level of optimism (17 points), and in other countries, an average level of optimism was in Poland – 14.5 points, Greece – 14.0 points, Turkey – 14.3 points, and Russia – 16.5 points. Women after childbirth had a high level of optimism in Belarus (17.4 points) and Russia (17.2 points), and in other countries had the average level of optimism. In these countries, the lowest level of optimism was found in non-pregnant women. No significant correlation between age and life optimism was found in any group. In Poland, life optimism increased with age in women who had never been pregnant, and in Turkey, in women who were pregnant and after childbirth.
Conclusion: Pregnant women from Belarus had a higher level of optimism than other countries. Non-pregnant women had an average level of optimism. Future studies should include larger groups of women and consider other factors that may additionally contribute to dispositional optimism.
Introduction
Several terms and gradations of pessimism and optimism may be found in the literature (1–6). Pessimism is a mental attitude in which an undesirable outcome is anticipated from a given situation. Pessimists tend to focus on the negatives of life in general (7).
Optimism is an attitude reflecting a belief or hope that the outcome of some specific endeavor, or outcomes in general, will be positive, favorable, and desirable. For example, the concept of ‘dispositional optimism’, is understood as a way of perceiving the world that involves expecting more positive outcomes (8). They consider it to be a fixed personality trait rather than a variable dependent on the current situation. As such, it can be regarded as an important factor involved in the choice of a goal and in the way it is achieved, determining the effort put into achieving it (8). The terms’ defensive pessimism’ and ‘strategic optimism’ are also distinguished (9, 10).
The development of the above trait is influenced by biological factors (heredity and temperament), and, according to Seligman (11), also by environmental factors (influence of parents, teachers, and early life experiences). Research findings in recent years prove that variables traditionally considered cognitive (self-esteem, satisfaction with life, and optimism) share a common genetic basis (12, 13).
It is worth remembering that life optimism is an intrinsic component that accompanies every human being, although it takes on different magnitudes depending on the life situation and psychological predispositions (5, 11, 12). It determines a person’s behavior, shapes one’s attitude toward oneself, builds high self-esteem and attitudes toward others, determines one’s self- efficacy, and motivates one to take new initiatives. In difficult situations, it reduces tension and stress, facilitates solving difficulties effectively, and triggers adaptive strategies focused on emotions (11). It also facilitates rapid decision-making in a difficult situation for the individual (8). Study results suggest that high levels of dispositional optimism are significantly associated with physical and mental health, life expectancy, high motivation in one’s tasks (even when faced with growing obstacles), positive emotions, more self-efficacy, higher perceived quality of life, resistance to stress, preference for active coping strategies, and a less severe negative impact of stress (8, 14, 15).
The perinatal period, from pregnancy to the first year postpartum, is a transitional period that can result in anxiety and stress for some women. Perinatal anxiety and stress can adversely impact women and children’s physical and psychological health. Understanding these problems is essential to support women better (16).
Numerous studies have been published on the well-known effects of depression during pregnancy and the postpartum period (13, 17, 18). In contrast, the relationship between obstetrical outcomes and dispositional optimism is still debated.
Life satisfaction can be reduced by lower optimism. For example, it is suggested that increasing optimism could reduce the negative consequences of activities of daily living limitations on life satisfaction among middle-aged older adults (19).
Patients’ optimism is correlated with a lower risk of depression and anxiety. A study by Rodrigues et al. (20) demonstrated that high anxiety and depression are correlated with poor optimism and quality-of-life scores.
Antenatal depression is a debilitating experience for many women with significant personal and familial sequelae. Optimism is inversely correlated with depression and directly correlated with improved birth outcomes (21).
Optimism is a potentially modifiable variable that could be used to design antenatal prevention and treatment programs. There are few studies on dispositional optimism in postpartum and pregnant women in Poland (22). Moreover, no similar studies were conducted in Belarus, Greece, Turkey, or Russia. Therefore, we wanted to compare the impact of pregnancy and the postpartum period on dispositional optimism in relation to life satisfaction, risk of depression, and mental health between these different countries with different cultures.
Aim of the study
The study was designed to measure the level of dispositional optimism in postpartum and pregnant women, compared to women who were not pregnant at the time of the survey and had never given birth in Poland, Greece, Turkey, Belarus, or Russia in relation to satisfaction with life, risk of depression and mental health status.
The research hypotheses were that (1) postpartum and pregnant women, compared to women who are not pregnant and have never given birth (control group), show higher levels of optimism; (2) in all study groups/countries, women who had higher optimism levels also had higher satisfaction with life, lower risk of depression, and better mental health.
Materials and methods
A case–control study was carried out among 2017 women surveyed, including 584 pregnant women, 528 postpartum women, and 906 nulliparous women (the control group) from Poland, Greece, Turkey, Belarus, and Russia. The sample selection was purposive. A purposive sample is a non-probability sample selected based on population characteristics and the study’s objective. Purposive sampling differs from convenience sampling and is also known as judgmental, selective, or subjective sampling. The pregnant women were recruited from Obstetrics Departments, the postpartum women were from GP clinics, and the control group included women students and workers of the Universities from the studied countries. Written informed consent for participation in the study was obtained from all participants. The study was retrospective, and participation was voluntary and anonymous. Women were included in the study if they were over 18 years of age, willing to give informed consent, and could communicate in the mother language. The questionnaires were given to the participants by the authors of the study. The authors from Belarus, Russia, Greece, and Turkey have sent the filled questionnaires in their native languages to Poland. Next, the data was then entered into a spreadsheet by a statistician. All the question-and-answer numbers were the same in all five countries. This made the statistician able to analyze the results easily.
The Bioethics Committee APK.002.587.2021 approved the Medical University of Białystok, Poland study. Surveys were collected between November 2021 and December 2022. The study used the following questionnaires:
Beck Depression Inventory (BDI) to assess the presence and severity of depressive symptoms (23) – all groups. It is used to self-assess the presence and severity of depression symptoms. The scale consists of 21 points rated according to the intensity of symptoms, from 0 to 3. For each point, the respondent should select one answer that, in his opinion, best describes his condition in the indicated period (before the doctor asks the patient to complete the scale, he should specify what period the answers should refer to – a month, a week or the last 24 h)—obtaining from 0 to 11 points indicates no depression, 12–26 points with a mild depressive episode, 27–49 points - with a moderate depressive episode and 50–63 points – a major depressive episode. The discriminatory power coefficients (corrected item-scale correlation coefficients) of the items were: in the control group from 0.48 to 0.70 (M = 0.59, Me = 0.61) and in the clinical group from 0.38 to 0.79 (M = 0.66, Me = 0.69). The Cronbach’s alpha coefficient was 0.93 and 0.95 for the entire scale, respectively.
Edinburgh Postnatal Depression Scale – EPDS (24) – a group of postpartum women.
The Edinburgh Postnatal Depression Scale was developed to assist health professionals in detecting mothers suffering from postpartum depression, a distressing disorder more prolonged than the “blues” (which can occur in the first week after delivery). The scale consists of 10 questions, each with—four ready-made answers. The woman is asked to read each statement and choose the one that best reflects how she has felt over the past 7 days. The maximum number of points is 30. Mothers scoring above 12 or 13 are likely to be suffering from depression and should seek medical attention, sensitivity, and specificity at the level of 84.2–93.9% and 75.2–76.7%, and Cronbach’s alpha – 0.87–0.88%.
Satisfaction With Life Scale – SWLS (25, 26) – all groups. The scale contains five statements. The respondent assessed the extent to which each of them related to his/her life so far, where: 1 – meant – I completely disagree, 2 – I do not agree, 3 – I rather disagree, 4 – I neither agree nor disagree, 5 – I rather agree, 6 – I agree and 7 – I completely agree. The obtained ratings were added up, and the overall result indicated satisfaction with one’s own life. The range of results could be from 5 to 35 points, and the higher the result, the greater the sense of satisfaction with life: 5–9 points. – a person dissatisfied with their life, 10–14 points, a person very dissatisfied with their life, 15–19 points. – person rather dissatisfied with their life, 20 points. – person neither satisfied nor dissatisfied with their life, 21–25 points. – person rather satisfied with their life, 26–30 points. – a person very satisfied with their life, 31–35 points. – a person satisfied with their life. Results between 1 and 4 sten were treated as low results, and between 7 and 10 sten as high results. Results within 5 and 6 sten are considered average. The reliability index (Cronbach’s alpha) of the SWLS, established in a study of 371 adults, is 0.81. The scale constancy index, determined by testing a group of 30 people twice with an interval of 6 weeks, was 0.86.
General Health Questionnaire GHQ-28 (27) – all groups. The scale is used to assess the state of mental health and allows for the identification of people whose mental state has undergone a temporary or long-term breakdown as a result of experienced difficulties, problems, or as a result of mental illness and those who are at significant risk of mental health disorders. The questionnaire consists of 28 questions measuring four symptom areas: somatic disorders (A), anxiety (B), functional disorders (C), and depression (D). Theoretical scores for the scales range from 7 to 28 points; the higher the score, the greater the difficulties experienced. Cronbach’s alpha coefficients are 0.955, 0.956, 0.945, and 0.926, respectively. The GHQ-28 scale examines four dimensions of mental state: A – somatic symptoms (Cronbach’s alpha for the study group = 0.876), B – anxiety and insomnia (alpha = 0.916), C – social functioning disorders (alpha = 0.933), D – symptoms of depression (alpha = 0.941), which together give an overall score.
Life Orientation Test-Revised LOT-R (25) – all groups. Life Orientation Test-Revised (LOT- R), developed by Scheier, Carter, and Bridges in the Polish adaptation of Poprawa and Juczynski (25), is used to measure dispositional optimism expressing generalized expectations concerning positive events. It is intended for healthy and unhealthy people. It consists of 10 statements, six of which have a diagnostic value for dispositional optimism. The overall test result is the sum of the evaluation of six statements, including three positive and three negative. Possible results are in the range of 0–24 points. The higher the score, the higher the level of optimism. The reliability determined by Cronbach’s alpha coe_cient is 0.78 for the original version and 0.76 for the Polish version.
Statistical analysis
The Statistica 13.0 PL program was used for statistical calculations. The Spearman’s rank correlation coefficient was used for the analysis, and the analysis was done by country and group concerning being pregnant or postpartum. Due to the large number of correlations analyzed (the analysis was done by country and study group), the exact p-values of the test probabilities were omitted, only denoting the level of statistical significance of a given correlation with the symbol *. The tables use a color scheme to facilitate interpretation of the results. Due to the normal distribution of the LOT-R measure, the t-test for independent samples was used in the analysis. Statistical significance was evaluated at p < 0.05.
Results
Table 1 illustrates a summary of the demographics of the respondents by status: not pregnant, pregnant, or postpartum. Among the surveyed women, the group of pregnant (8.1%) and postpartum women from Russia were very low (9.1%) and the highest from Poland (29.6 and 30.9% respectively). Significant differences were found in the residence structure of surveyed women from different countries, which probably depends on the geographical region where the surveys were conducted. Therefore, it seems that it can be assumed that in the 21st century, the place of residence does not significantly determine the quality of life, and the influence of this factor should not be considered further.
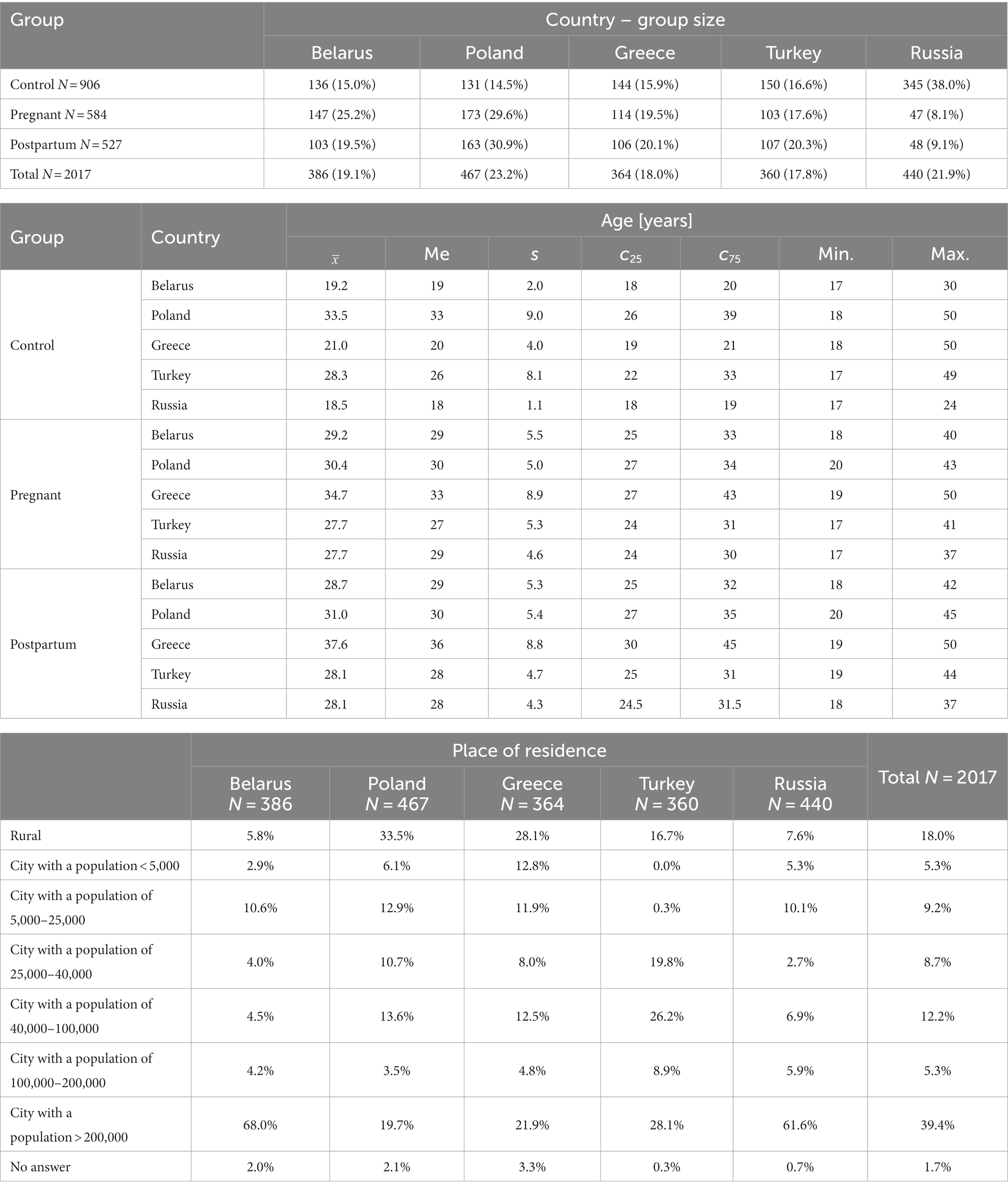
Table 1. Demographics of the respondents by status: not pregnant, pregnant, postpartum.
In Poland, respondents with a master’s degree dominated (201 people), and in Turkey with a bachelor’s degree (155 people). Most respondents from Belarus (114 people), Greece (116 people), and Russia (262 people) were students. The results are shown in Table 2.
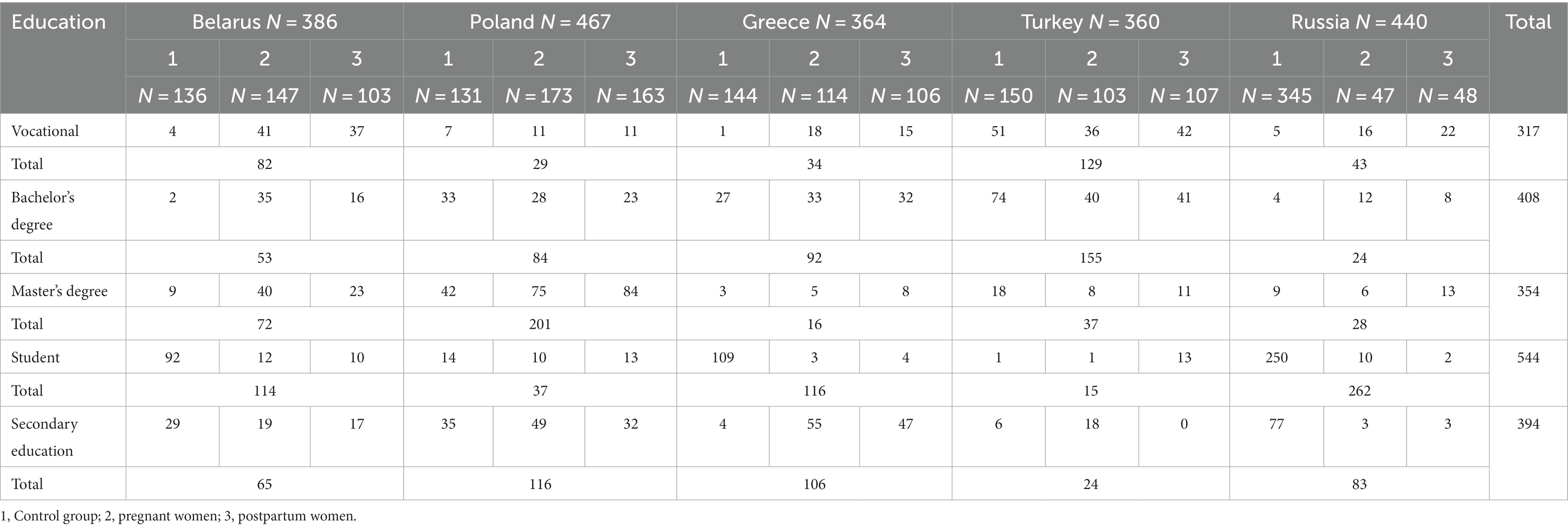
Table 2. Educational background of respondents.
The study used the Life Orientation Test (LOT-R) to assess how women’s optimism varied by status pregnant, postpartum, not pregnant, and the control group across different countries. Pregnant, postpartum, and non-pregnant women had average or medium optimism. We observed the differences in the scoring optimism between the studied countries. Women from Belarus and Russia were more optimistic than other countries.
Women in the control group showed average optimism, scoring 16 points in Belarus, 13.4 points in Poland, 13.3 points in Greece, 13.5 points in Turkey, and 16.3 points in Russia. Pregnant women from Belarus showed high optimism, at 17 points on average, and other countries showed medium optimism, scoring 14.5 points in Poland, 14.0 points in Greece, 14.3 points in Turkey, and 16.5 points in Russia. In contrast, postpartum women showed high optimism in Belarus, at 17.4 points on average, and Russia, at 17.2 points on average. The average optimism in the other countries was Poland at 14.1 points, Greece at 14.5 points, and Turkey at 14.0 points.
It only occurred in Russia that being pregnant or giving birth did not affect optimism. In the remaining countries, differences were statistically significant (in Belarus, marginally above the significant score limit: p = 0.0594). Analysis of the mean or median values revealed that in each of these countries, the lowest optimism was characterized by women who were not pregnant (Table 3 and Figure 1).
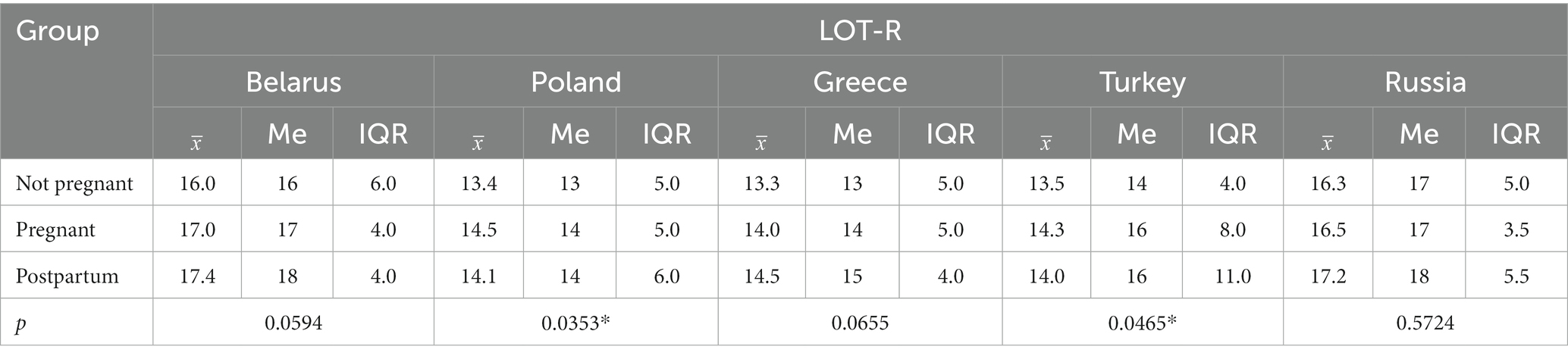
Table 3. Assessment of the study groups using the Life Orientation Test LOT-R.
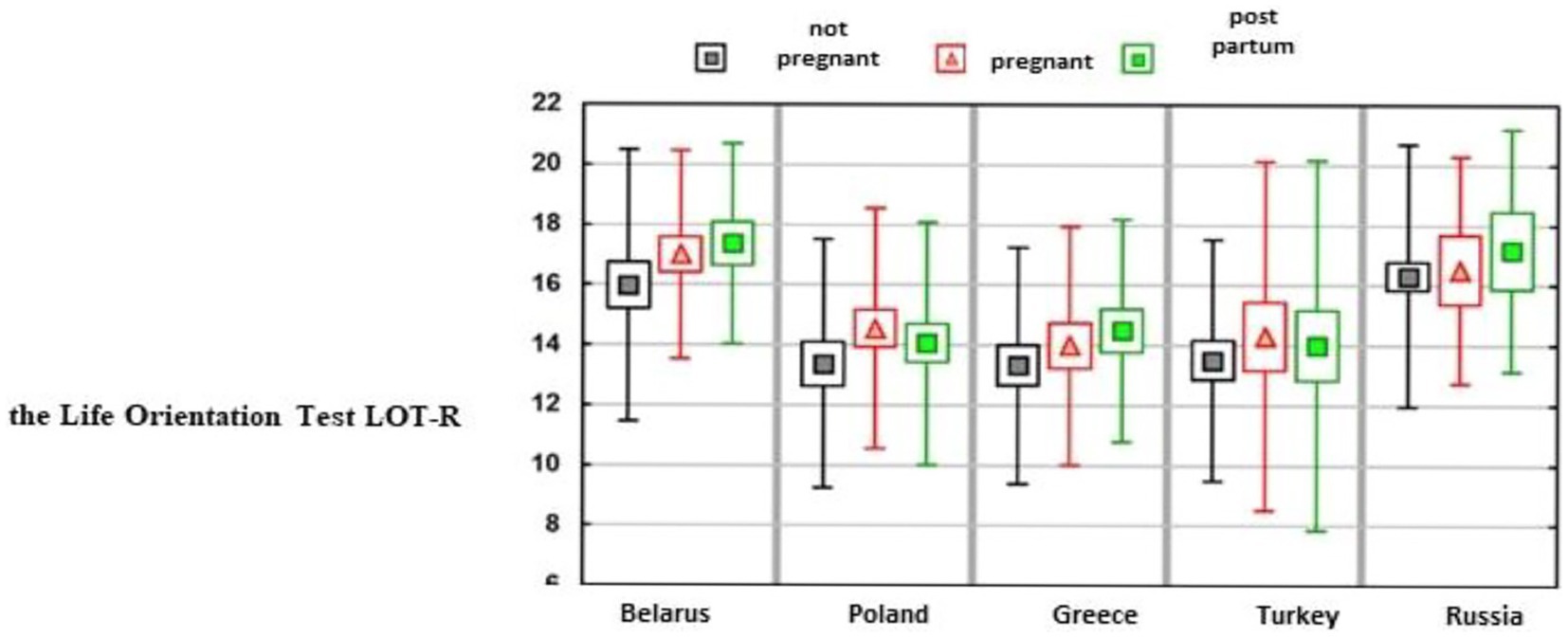
Figure 1. Assessment of the study groups using the Life Orientation Test LOT-R.
Correlations between optimism by the LOT-R scale and depressive symptoms, life satisfaction, and mental health were examined (Table 4). Generally, we found positive correlations between optimism and life satisfaction and negative correlations between optimism and depressive symptoms and mental health in the studied women. In detail, in the non-pregnant women’s group – LOT-R was positively correlated with life satisfaction and negatively correlated with depressive symptoms and mental health. However, most correlations were at a weak or average level. Among pregnant women, similar correlations were only found in Turkey. The correlations in the other countries are much weaker, and in Russia and Belarus, the LOT-R measures only correlated with life satisfaction. The correlations analyzed in postpartum women were similar, except they were significantly stronger in Turkey.
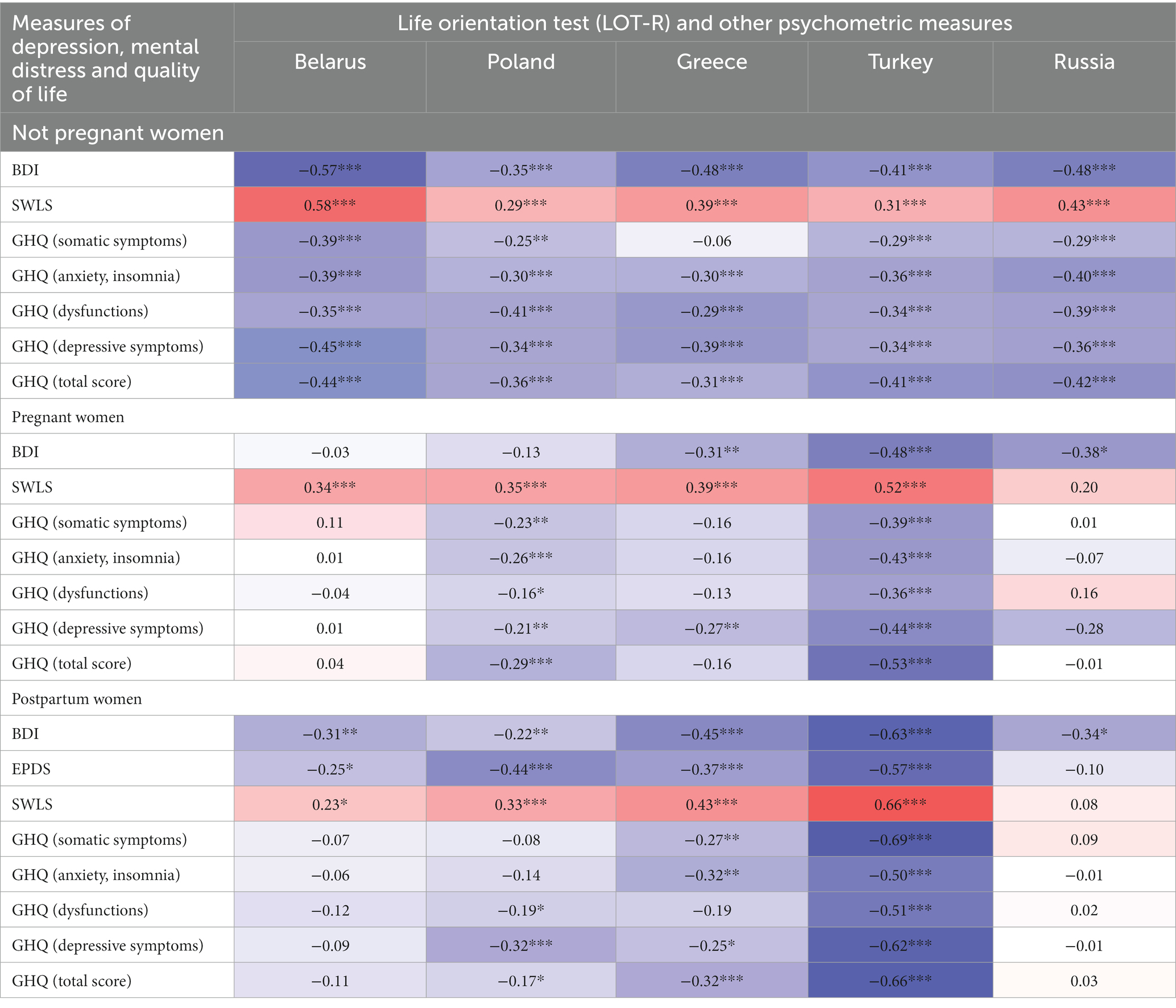
Table 4. Correlations of LOT-R measures with BDI, EPDS, SWLS and GHQ-28 measures.
A partial confirmation of the hypotheses was obtained. A series of graphs shows the correlations between BDI and LOT-R for each country and each woman’s status. It examined how the level of life optimism is related to selected factors. First, the influence of age on the level of life optimism was analyzed – the analysis was carried out taking into account the specificity of the country and belonging to a group.
The results turned out to be quite varied, the most important being that:
• In none of the groups of women from Belarus, Greece, and Russia, a statistically significant relationship between age and the level of life optimism found;
• Among the Polish women, the level of life optimism increased with age, only in women who had never been pregnant;
• Age was also a factor causing an increase in optimism in life in Turkey, and the correlations concerned pregnant women, especially after childbirth (r = 0.50, so the correlation here is at an average level). The results are presented in Table 5.
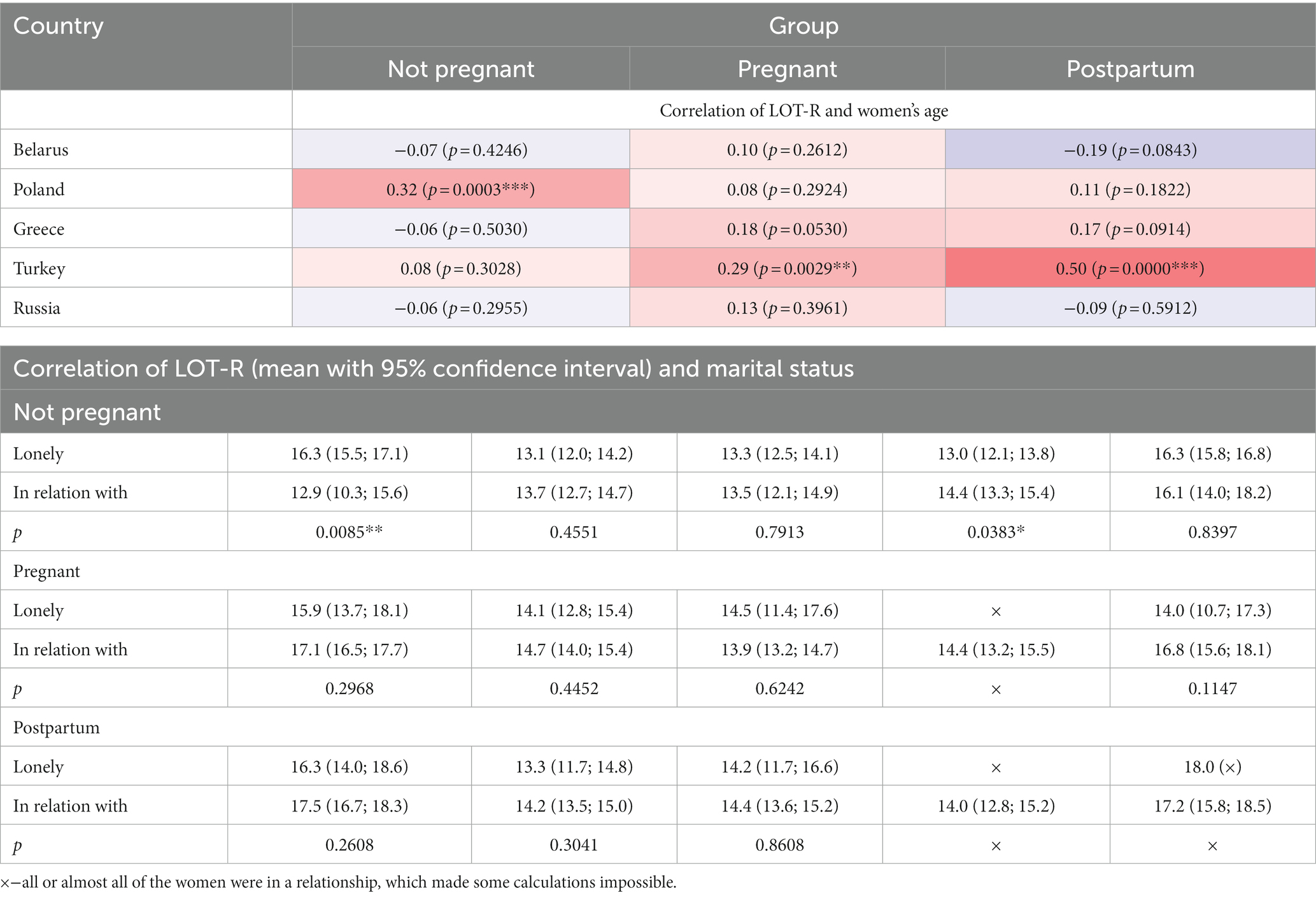
Table 5. Correlations of LOT-R measures with age and marital status of women.
Married and unmarried women dominated the surveyed population, and the remaining groups were much smaller; therefore, to ensure the appropriate size of the compared groups, the groups of single and married women were combined, and the analysis was conducted in such a system. Due to the normal distribution of the LOT-R measure, the t-test for independent samples was used in the analysis.
In the group of pregnant and postpartum women, in those countries where a comparison was possible (because, for example, in Turkey, and partly also in Russia, all or almost all women were in a relationship), no significant differences in optimism were found. On the other hand, in the group of non-pregnant women from Belarus, single people had a significantly higher level of optimism. A statistically significant difference was also found among Turkish women who were not pregnant but in favor of women in a relationship who had a slightly higher level of life optimism.
Another analysis concerned the level of life optimism depending on having children. In none of the countries, having children by pregnant women did not affect their current level of life optimism (Table 6).

Table 6. Correlations of LOT-R measures with the fact of having children.
The analysis was also performed considering the number of children already had, using Spearman’s rank correlation analysis. However, the correlation analysis also showed no relationship between pregnant women’s level of life optimism and the number of children they had.
The type of childbirth did not influence the level of life optimism significantly. The level of optimism of pregnant women with a natural or artificial miscarriage did not differ significantly from those of other women. The only difference concerned pregnant women from Turkey – those with a natural miscarriage had a significantly lower level of life optimism (11.9 vs. 15.9 points; p = 0.0392*). The results are shown in Table 7.
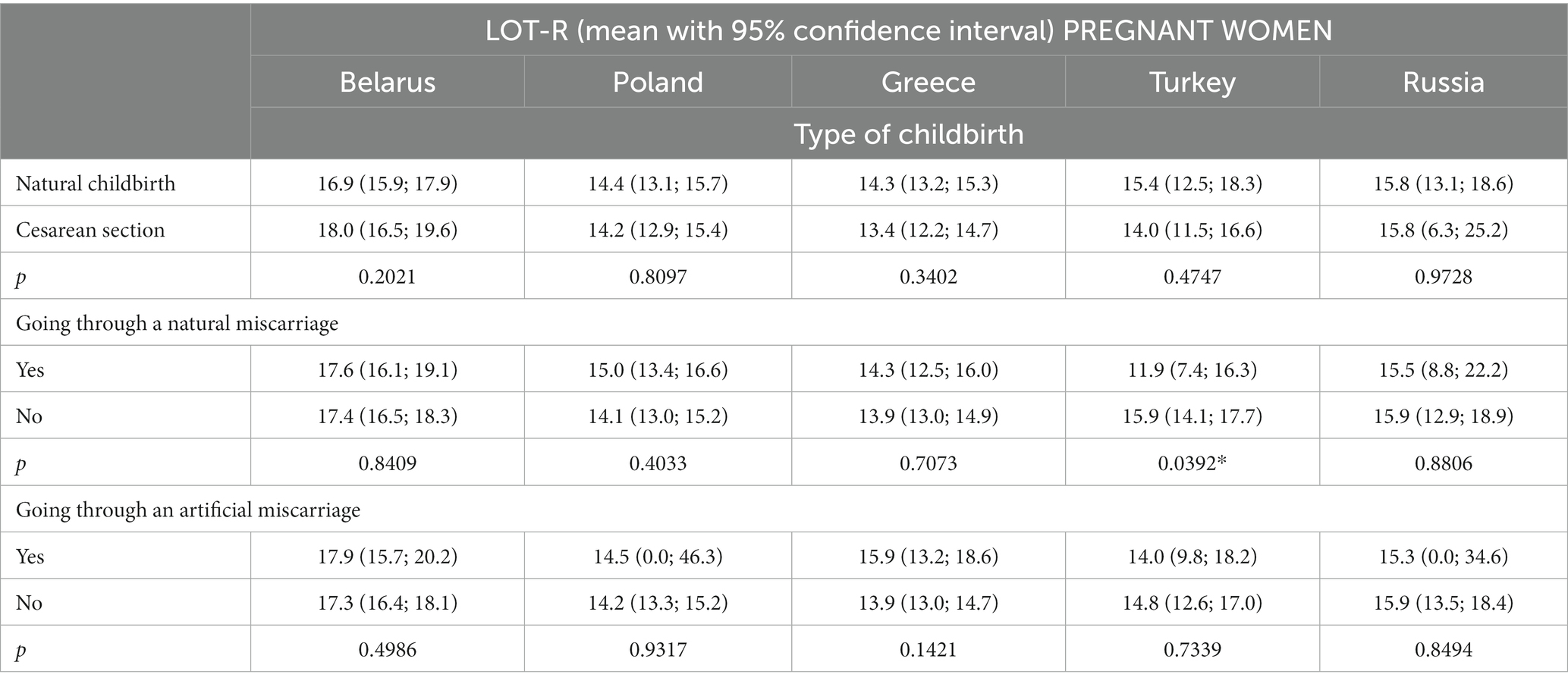
Table 7. Correlations of LOT-R measures in the group of pregnant women with the type of delivery and miscarriage.
Discussion
Our study contributes new knowledge about dispositional optimism in pregnant and non-pregnant women from five different cultural countries: Poland, Belarus, Greece, Russia, and Turkey.
Women in the control group showed average optimism. Similar results have been obtained in pregnant and postpartum women except for women from Belarus who had high optimism. The dispositional optimism in the LOT-R scale was positively correlated with life satisfaction in the studied and the control group. In contrast, dispositional optimism was negatively correlated with depressive, somatic, and anxiety symptoms. The dispositional optimism was positively correlated with age among Polish and Turkish women. Having children does not affect the level of optimism.
Our findings are in agreement with previous results (21, 22, 28).
Niewiadomska et al. (22) determined the role of dispositional optimism in the relationship between health locus of control and self-efficacy in pregnant women with threatened preterm labor. For women with a high-risk pregnancy, dispositional optimism was a significant resource for coping with their problems. Optimistic pregnant women maintained a positive outlook, even when confronted with difficult, negative experiences such as threatened preterm labor.
In a study from New Zealand, women in hospital and community groups completed a battery of questionnaires on pregnancy and health history, life events, anxiety, optimism, coping, and relationship factors (28). The groups did not differ on life events, optimism, and coping self-efficacy. Predictors of acute anxiety differed across the groups: for hospitalized women, anxiety was predicted by the rating of their health and their dispositional optimism; for women in the community, anxiety was predicted by stressful life events, dispositional optimism, and coping self-efficacy.
In a prospective cohort study (29) completed between 5/2019-2/2022, nulliparous pregnant women completed a validated assessment of dispositional optimism at <20 weeks’ gestation and were followed until delivery. The authors demonstrated that lower early- pregnancy ispositional optimism was associated with significantly higher odds of adverse maternal outcomes.
Italian, Canadian, German, and Japanese studies confirm that positive orientation can be considered a ‘good functioning syndrome’ that correlates positively with the health status assessment (30). Dispositional optimism has been associated with protection against depressive symptoms and reduced negative affect in multiple contexts (31).
The transition to motherhood is a time of elevated risk for clinical depression. Dispositional optimism may be protective against depressive symptoms; however, the arrival of a newborn causes numerous challenges that may contribute to depressed mood. Robakis et al. (32) explored the relative contributions of antenatal and postnatal optimism regarding maternity to depressive symptoms in the postnatal period. Pregnant women underwent clinician interviews in the third trimester to record psychiatric history and antenatal depressive symptoms and administer a novel measure of optimism toward maternity. The authors concluded that antenatal optimism is the approach that is most protective against postnatal depressive symptoms and that this is true irrespective of either mood disorder history or parity.
Kazmierczak et al. (33) analyzed risk factors for perinatal mental disorders and assessed dispositional optimism in women at 37 weeks pregnant and 6 weeks after giving birth. The authors demonstrated that the main predictors of perinatal mental disorders were the variables: mental health disorders before pregnancy, subjectively reported decreased mood in pregnancy, the lack of social support, and the tendency to pessimism.
The literature emphasizes that optimism affects human health in multiple ways (34, 35). Firstly, it improves the functioning of the immune system (when one has a negative disposition toward the world, negative emotions tend to dominate one’s life, resulting in lower levels of catecholamines and endorphins, which translates into a weaker immune system and greater susceptibility to infection). Secondly, people who are positive believe that they have control over their lives and are more willing to take various actions that promote good health. Thirdly, it reduces the risk of developing diseases, as pessimists are much more likely than optimists to contract various types of diseases. Fourthly, it reduces the negative effects of stress, which is one of the main factors in the development of many diseases, including circulatory system diseases. Optimists are less likely to develop these diseases because they cope much better with stress and have much lower levels of cortisol (the stress hormone) (36–49).
Future studies should include larger groups of women and consider other factors that may additionally contribute to dispositional optimism.
Conclusion
In general, we have found differences in the dispositional optimism between women from Poland, Belarus, Greece, Turkey, and Russia The studied women, had average and medium levels of dispositional optimism. More optimistic women were pregnant from Belarus and Russia. The dispositional optimism in pregnant women negatively correlated with depressive symptoms and mental health. In the control group, dispositional optimism positively correlated with life satisfaction. In none of the countries, having children by pregnant women and the type of last delivery affected their current level of life optimism.
Limitations of the study
We did not calculate the sample size.
The study was conducted during the COVID-19 pandemic, which could impact the optimism levels among the studied women.
The participants in this study were not random. This can lead to a biased sample that is not representative of the studied populations.
Due to the differences in the residence structure of female respondents from different countries, depending on the geographical region where the surveys were conducted, it was assumed that in the 21st century, the place of residence does not significantly determine the quality of life and the influence of this factor should not be considered further.
In Russia and Belarus, and to a slightly lesser extent in Greece, the surveys for non- pregnant women were conducted mainly among young people, which may have significantly influenced the results.
The strength of the study
Our study contributes new knowledge about the dispositional optimism in pregnant and non- pregnant women from five different cultural countries: Poland, Belarus, Greece, Russia, and Turkey. We have compared the dispositional optimism in pregnant, post-partum, and non- pregnant women. We have analyzed the dispositional optimism in women with correlation with life satisfaction, depressive symptoms, and mental health.
Implications
There is a need for physicians and nurses/midwives to become more involved in the health education of pregnant women regarding a health-promoting lifestyle. This education should consider patients’ resources, especially the level of dispositional optimism, as a factor that strengthens motivation and consistency in following medical recommendations. It is important to strengthen women’s reservoirs of dispositional optimism, even though it is a relatively fixed attribute. After all, it cannot be ruled out that in a difficult situation such as pregnancy, fear of childbirth and childbirth may, on the one hand, decrease and, on the other, intensify under the influence of health educators’ actions. These findings may have important implications for pregnant and postpartum women. Perinatal screening for depression is common, but monitoring the level of optimism is not used in clinical practice. We suggest there is also a need to assess the level of optimism in primary care antenatal services. Moreover, we have found dispositional optimism in the LOT-R scale generally was positively correlated with life satisfaction and negatively correlated with mental health, depressive symptoms, anxiety, and somatic disorders. We suggest that knowing the importance of optimism in pregnant and post-pregnant women can facilitate a more elevated detection of women’s mental health disorders.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee APK.002.587.2021, Medical University of Białystok, Poland. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AK-B: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. AS: Data curation, Investigation, Writing – review & editing. NK: Data curation, Investigation, Writing – review & editing. LH: Data curation, Investigation, Writing – review & editing. IA: Data curation, Investigation, Writing – review & editing. DC: Data curation, Investigation, Writing – review & editing. LK: Data curation, Investigation, Writing – review & editing. AT: Data curation, Investigation, Writing – review & editing. KK: Data curation, Investigation, Writing – review & editing. NW: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Carroll, PJ, Sweeny, K, and Shepperd, JA. Forsaking optimism. Rev Gen Psychol. (2006) 10:56–73. doi: 10.1037/1089-2680.10.1.56
2. Norem, JK, and Chang, EC. A very full glass: adding complexity to our thinking about the implications and applications of optimism and pessimism research. In EC Chang, Ed. Optimism and pessimism: Implications for theory, research, and practice. Washington, DC: American Psychological Association. (2001) 347–367.
3. Norem, JK, and Chang, EC. The positive psychology of negative thinking. J Clin Psychol. (2002) 58:993–1001. doi: 10.1002/jclp.10094
5. Arbel, R, Segel-Karpas, D, and Chopik, W. Optimism, pessimism, and health biomarkers in older couples. Br J Health Psychol. (2020) 25:1055–73. doi: 10.1111/bjhp.12466
6. Stach, R. Optymizm. Badania nad optymizmem jako mechanizmem adaptacyjnym. Kraków: Wyd. Uniwersytetu Jagiellońskiego (2006) (Polish).
7. Dienstag, JF. Pessimism: philosophy, ethic, spirit. Princeton, New Jersey: Princeton University Press (2009).
8. Carver, CS, and Scheier, MF. Dispositional optimism. Trends Cogn Sci. (2014) 18:293–9. doi: 10.1016/j.tics.2014.02.003
9. Ferradás Canedo, MM, Freire Rodríguez, C, Regueiro Fernández, B, and Valle, AA. Defensive pessimism, self-esteem and achievement goals: a person-centered approach. Psicothema. (2018) 30:53–8. doi: 10.7334/psicothema2017.199
10. Thomas, SP. In defense of defensive pessimism. Issues Ment Health Nurs. (2011) 32:1. doi: 10.3109/01612840.2011.535350
11. Seligman, MEP. Optymizmu można się nauczyć, Jak zmienić swoje myślenie i swoje życie. Poznań: Media Rodzinna (2005) (Polish).
12. Pilch, T. Optymizm i pesymizm – dwie orientacje życia indywidualnego i dwie strategie budowania świata społecznego. Pedagogika Społeczna. (2016) 15:9–25. (Polish)
13. Caprara, GV, Vecchione, M, Capanna, C, and Mebane, M. Perceived political self-efficacy: theory, assessment, and applications. Eur J Soc Psychol. (2009) 39:1002–20. doi: 10.1002/ejsp.604
14. Scheier, MF, and Carver, CS. Dispositional optimism and physical health: a long look back, a quick look forward. Am Psychol. (2018) 73:1082–94. doi: 10.1037/amp0000384
15. Giangiordano, I, Sahani, H, Di Mascio, D, Saccone, G, Bellussi, F, Berghella, A, et al. Optimism during pregnancy and obstetrical outcomes: a systematic review. Eur J Obstet Gynecol Reprod Biol. (2020) 248:95–101. doi: 10.1016/j.ejogrb.2020.03.029
16. McCarthy, M, Houghton, C, and Matvienko-Sikar, K. Women's experiences and perceptions of anxiety and stress during the perinatal period: a systematic review and qualitative evidence synthesis. BMC Pregnancy Childbirth. (2021) 21:811. doi: 10.1186/s12884-021-04271-w
17. Mukherjee, S, Trepka, MJ, Pierre-Victor, D, Bahelah, R, and Avent, T. Racial/ethnic disparities in antenatal depression in the United States: a systematic review. Matern Child Health J. (2016) 20:1780–97. doi: 10.1007/s10995-016-1989-x
18. Klawetter, S, McNitt, C, Hoffman, JA, Glaze, K, Sward, A, and Frankel, K. Perinatal depression in low- income women: a literature review and innovative screening approach. Curr Psychiatry Rep. (2020) 22:1. doi: 10.1007/s11920-019-1126-9
19. Cheng, KJG, McMaughan, DJD, and Smith, ML. The role of optimism on the relationship between activity limitations and life satisfaction among middle-aged and older adults in the United States: a growth curve model of changes over time. J Appl Gerontol. (2022) 41:993–1001. doi: 10.1177/07334648211056638
20. Rodrigues, MF, Vianna, R, Galdino, MK, Nardi, AE, Appolinário, JC, and Levitan, MN. Could dispositional optimism impair panic disorder and depression outcomes? J Nerv Ment Dis. (2021) 209:459–62. doi: 10.1097/NMD.0000000000001317
21. Evans, EC, and Bullock, LF. Optimism and other psychosocial influences on antenatal depression: a systematic review. Nurs Health Sci. (2012) 14:352–61. doi: 10.1111/j.1442-2018.2012.00700.x
22. Niewiadomska, I, Bień, A, Rzońca, E, and Jurek, K. The mediating role of dispositional optimism in the relationship between health locus of control and self-efficacy in pregnant women at risk of preterm delivery. Int J Environ Res Public Health. (2022) 19:6075. doi: 10.3390/ijerph19106075
23. Zawadzki, B, Popiel, A, and Pragłowska, E. Charakterystyka psychometryczna polskiej adaptacji Kwestionariusza Depresji BDI-II Aarona T. Becka (Psychometric Properties of the Polish Version of the Aaron T. Beck’s Depression Inventory BDI-II). psychologia – etologia – genetyka. (2009) 71–95.
24. Giannakou, M, Roussi, P, Kosmides, M-E, Kiosseoglou, G, Adamopoulou, A, and Garyfallos, G. Adaptation of the Beck depression inventory-II to Greek population. Hell J Psychol. (2013) 10:120–46.
25. Kapci, EG, Uslu, R, Turkcapar, H, and Karaoglan, A. Beck depression inventory II: evaluation of the psychometric properties and cut-off points in a Turkish adult population. Depress Anxiety. (2008) 25:E104–10. doi: 10.1002/da.20371
26. Ponizovsky, A. Beck Depression Inventory - Russian version. Avaible at: https://www.researchgate.net/publication/323995572_Beck_Depression_Inventory_-_Russian_version (2018) (Accessed October 1, 2023).
27. Cox, JL, Holden, JM, and Sagovsky, R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
28. Vivilaki, VG, Dafermos, V, Kogevinas, M, Bitsios, P, and Lionis, C. The Edinburgh postnatal depression scale: translation and validation for a Greek sample. BMC Public Health. (2009) 9:329. doi: 10.1186/1471-2458-9-329
29. Aydin, N, Inandi, T, Yigit, A, and Hodoglugil, NN. Validation of the Turkish version of the Edinburgh Postnatal Depression Scale among women within their first postpartum year. Soc Psych Epid. (2004) 39:483–6. doi: 10.1007/s00127-004-0770-4
30. Yakupova, VA, and Suarez, A. Postpartum depression and birth experience in Russia. Psychol Russ. (2021) 14:28–38. doi: 10.11621/pir.2021.0103
31. Juczyński, Z. Narzędzia pomiaru w promocji i psychologii zdrowia. Warszawa: Ed. Pracownia Testów Psychologicznych (2011) (Polish).
32. Michael Galanakis, M, Lakioti, A, Pezirkianidis, C, and Stalikas, A. Reliability and validity of the satisfaction with life scale (SWLS) in a Greek sample. Int J Human Soc Stud. (2017) 5:120–7.
33. Durak, M, Senol-Durak, E, and Genco, T. Psychometric properties of the satisfaction with life scale among Turkish university students, correctional officers, and elderly adults. Soc Indic Res. (2010) 99:413–29. doi: 10.1007/s11205-010-9589-4
34. Shpakou, A, Naumau, IA, Krestyaninova, TY, Znatnova, AV, Lollini, SV, Surkov, S, et al. Physical activity, life satisfaction, stress perception and coping strategies of university students in Belarus during the COVID-19 pandemic. Int J Environ Res Public Health. (2022) 19:8629. doi: 10.3390/ijerph19148629
35. Zolotareva, AA, Averina, PA, and Timoshina, AL. Satisfaction with life in the third age and its measurement: adaptation of the Russian version of the LSITA-SF. Psychol Sci Educ. (2022) 27:19–28. doi: 10.17759/pse.2022270202
36. Makowska, Z, and Merecz, Z. Polska adaptacja kwestionariuszy ogólnego stanu zdrowia Davida Golberga: GHQ-12 i GHQ-28. Łódź: Instytut Medycyny Pracy (2001) (Polish).
37. Garyfallos, G, Karastergiou, A, Adamopoulou, A, Moutzoukis, C, Alagiozidou, E, Mala, D, et al. Greek version of the general health questionnaire: accuracy of translation and validity. Acta Psychiatr Scand. (1991) 84:371–8. doi: 10.1111/j.1600-0447.1991.tb03162.x
38. Kilic, C, Rezaki, M, Rezaki, B, Kaplan, I, Ozgen, G, Sağduyu, A, et al. General health questionnaire (GHQ12 & GHQ28): psychometric properties and factor structure of the scales in a Turkish primary care sample. Soc Psychiatry Psychiatr Epidemiol. (1997) 32:327–31. doi: 10.1007/BF00805437
39. Ignatyev, Y, Assimov, M, Aichberger, MC, Ivens, S, Mir, J, Dochshanov, D, et al. Psychometric properties of a Russian version of the general health Questionnaire-28. Psychopathology. (2012) 45:252–8. doi: 10.1159/000334918
40. Özden, F, and Tuna, S. The psychometric properties of the Turkish version of the self- regulatory fatigue scale. Perspect Psychiatr Care. (2022) 58:954–60. doi: 10.1111/ppc.12882
41. Lyrakos, GN, Damigos, D, Mavreas, V, Georgia, K, and Dimoliatis, IDΚ. A translation and validation study of the life orientation test revised in the Greek speaking population of nurses among three hospitals in Athens and Ioannina. Soc Indic Res. (2010) 95:129–42. doi: 10.1007/s11205-009-9453-6
42. Barber, CC, and Starkey, NJ. Predictors of anxiety among pregnant New Zealand women hospitalised for complications and a community comparison group. Midwifery. (2015) 31:888–96. doi: 10.1016/j.midw.2015.04.017
43. Ayala, NK, Fain, AC, Cersonsky, TEK, Werner, EF, Miller, ES, Clark, MA, et al. Early- pregnancy dispositional optimism and pregnancy outcomes among nulliparous people. Am J Obstet Gynecol MFM. (2023) 19:101155. doi: 10.1016/j.ajogmf.2023.101155
44. Caprara, GV, Alessandri, G, Trommsdorff, G, Heikamp, T, Yamaguchi, S, and Suzuki, F. Positive orientation across three cultures. J Cross-Cult Psychol. (2012) 43:77–83. doi: 10.1177/0022022111422257
45. Scheier, MF, and Carver, CS. Effects of optimism on psychological and physical well-being: theoretical overview and empirical update. Cogn Ther Res. (1992) 16:201–28. doi: 10.1007/BF01173489
46. Robakis, TK, Williams, KE, Crowe, S, Kenna, H, Gannon, J, and Rasgon, NL. Optimistic outlook regarding maternity protects against depressive symptoms postpartum. Arch Womens Ment Health. (2015) 18:197–208. doi: 10.1007/s00737-014-0446-3
47. Kaźmierczak, M, Gebuza, G, Gierszewska, M, Bannach, M, Mieczkowska, E, Dombrowska-Pali, A, et al. Screening for detection of the risk of perinatal mental disorders among women in Poland. Issues Ment Health Nurs. (2020) 41:438–44. doi: 10.1080/01612840.2019.1677829
48. Alessandri, G, Caprara, GV, and Tisak, J. The unique contribution of positive orientation to optimal functioning: farther explorations. Eur Psychol. (2012) 17:44–54. doi: 10.1027/1016-9040/a000070
Keywords: postpartum, depression, pregnancy, optimism, mental health
Citation: Kułak-Bejda A, Shpakou A, Khvoryk N, Hutsikava L, Aydin Avci I, Celik Eren D, Kourkouta L, Tsaloglidou A, Koukourikos K and Waszkiewicz N (2024) Impact of pregnancy/childbirth on dispositional optimism in the context of risk of depression, mental health status and satisfaction with life. Front. Psychiatry. 14:1271033. doi: 10.3389/fpsyt.2023.1271033
Edited by:
Sami Hamdan, Academic College of Tel Aviv-Yaffo, IsraelReviewed by:
Maheshkumar Kuppuswamy, Government Yoga and Naturopathy Medical College, IndiaChet Kant Bhusal, Universal College of Medical Sciences and Teaching Hospital, Nepal
Copyright © 2024 Kułak-Bejda, Shpakou, Khvoryk, Hutsikava, Aydin Avci, Celik Eren, Kourkouta, Tsaloglidou, Koukourikos and Waszkiewicz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnieszka Kułak-Bejda, YWduaWVzemthLmt1bGFrLmJlamRhQGdtYWlsLmNvbQ==