 HeungKyu Kim1
HeungKyu Kim1 Seongho Min
Seongho Min Hyun Kim
Hyun Kim Yong Sung Cha
Yong Sung Cha Min-Hyuk Kim
Min-Hyuk Kim- 1Department of Psychiatry, Seoul Metropolitan Eunpyeong Hospital, Seoul, Republic of Korea
- 2Wonju Mental Health Center, Wonju, Republic of Korea
- 3Department of Psychiatry, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea
- 4Department of Emergency Medicine, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea
Objectives: This study aimed to identify sex differences in the factors that affect medical lethality in elderly suicide attempters.
Methods: A total of 253 elderly suicide attempters and 351 middle-aged attempters (comparison group) who visited the emergency room at a general hospital were included. The sociodemographic and clinical characteristics of the patients were investigated. The Chi-squared test and logistic regression analysis were performed. And Spearman’s correlation coefficient was calculated.
Results: In older males, the risk of high lethality was lower when attempting suicide due to the loss of family members [adjusted odds ratio (AOR): 0.08]. The risk increased as the intent to die became more certain (some AOR: 11.31, certain AOR: 28.75), and this association became more pronounced with age (rho middle-aged: 0.329; young-old: 0.387; old-old: 0.415). In older females, the risk was lower when employed (AOR: 0.28). The method of suicide attempt also affected lethality (agricultural chemicals AOR: 3.71; psychiatric medication AOR: 0.31).
Conclusion: Sex differences in the factors that affect medical lethality were identified among elderly suicide attempters. In particular, medical lethality can be predicted by the degree of suicide intention in older males. These findings will help to establish more efficient preventive strategies with specific targets.
1 Introduction
Suicide is a global health problem, with around 700,000 people dying from suicide every year (1). In Korea, the suicide rate (24.6/100,000) in 2019 was more than twice the average of that in Organization for Economic Co-operation and Development member countries (11/100,000). In particular, the suicide rate among the elderly (65+ years, average: 17.2/100,000, Korea: 46.6/100,000) has been reported to be higher than that in the general population. Furthermore, the suicide rate in Korea tends to increase with age (60s: 33.7; 70s: 46.2; 80s: 67.4 per 100,000) (2). This may actually be worse due to the underestimation problem of not counting a death as a suicide in the absence of clear evidence, particularly in the elderly population (3, 4). The reason for the high suicide rate among the elderly is likely to be that they are physically more vulnerable than other ages, plan suicide with a stronger will, and attempt suicide in more dangerous ways in harder-to-find places (5, 6). Suicide attempts, even if they do not lead to death, often result in physical damage and disability and are associated with high medical and socioeconomic costs. Therefore, in countries such as Korea, where the elderly population is rapidly increasing (7) and the elderly suicide rate is particularly high, it is necessary to identify related factors so that interventions can be established.
The lethality of a suicide attempt has been previously defined and studied in terms of the severity of the medical condition, severity predicted by the attempter or medical professional, and type of ward used (8–13). These studies reported that lethality was affected by factors such as the method of the attempt, gender, drinking status, rescue potential, help-seeking, medical infrastructure, depression, intent to die, communication ability, and impulsivity. In particular, intent to die has often been found to be related to or is important as a predictor of lethality (9–11, 14). Nevertheless, some studies have shown no association between intent and lethality of attempt (15, 16) or that the relationship disappears over time (9). These varied results may be due to the different compositions of the research groups, the inability to control mediators, or different definitions of terms such as intent and lethality. The degree of physical damage caused by a suicide attempt not only affects treatment duration, cost, and intensity but also has clinical significance in predicting subsequent reattempts or death (12, 13, 17). Understanding the relationship between intent and lethality can provide a basis for determining the type and intensity of interventions when a patient’s suicidal intent is identified.
The characteristics of suicide attempts, including lethality, vary according to sex and age. Medical lethality is associated with rescue potential and suicidal intent in females but not associated with intent in males (8). However, in a study with an elderly population, the relationship between lethality and suicidal intent was significant only in males (14). A suicide prevention program for depressed elderly people in Japan was effective in females but not males (18). Therefore, it is important to distinguish subgroups when studying the lethality caused by suicide attempts. This would help in the establishment of specific prevention strategies that work effectively in each subgroup, enable the appropriate allocation of medical resources, and the creation of efficient suicide prevention policies. However, there is still insufficient research on lethality that distinguishes the subgroups. This study aimed to identify sex differences in the factors that affect medical lethality in elderly suicide attempters and to verify whether the relationship between intent to die and lethality varies according to sex.
2 Methods
2.1 Participants
This study was conducted from 2009 to 2015 on elderly (60+ years) and middle-aged suicide attempters (45–59 years) who visited the emergency room of a hospital in Wonju City, South Korea (19). This is the only tertiary general hospital in the area with sufficient diagnostic and therapeutic resources for injuries caused by suicide attempts, to which most suicide attempters requiring medical intervention are transferred. Only the first suicide attempt was included in the study for cases that reattempted suicide during the study period.
2.2 Data collection and measurement
Psychiatric residents and research assistants (nurses, social workers) familiar with the research objectives and evaluation methods collected information from the suicide attempters and their caregivers after arriving at the emergency room and filled in a Crisis Management and Evaluation Record. This document included sociodemographic characteristics such as age, sex, education, marital status, employment, income, and religion; clinical characteristics such as acute/chronic illness and disability, diagnosis according to the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision), current psychiatric treatment, and psychiatric history; suicide attempt-related characteristics such as suicide attempt history, family history of suicide, drinking status, motivation, method, intent to die, suicide note, medical lethality and help-seeking. As there are no commonly accepted criteria for defining acute and chronic illness and disability, these were initially classified according to clinical judgment, and the suitability of this classification was reviewed at a case conference. “Intent to die” was classified into three levels (little, some, certain) based on the attempter’s report, and the caregiver’s report was also considered. Medical lethality was classified into three levels (mild, moderate, and severe) based on the clinical judgment of an emergency medicine physician, considering the physical damage and the intensity of medical treatment required.
In situations where the suicide attempter was unable to provide information (e.g., unconsciousness or due to medical treatment), information was obtained from a caregiver, and the suicide attempter was interviewed later. In cases where the reports from the informants did not match, the attempters’ reports were given priority. A weekly case conference was held during the study period to review all records and improve measurement accuracy and interrater reliability. The conference involved two psychiatric specialists, residents, and research assistants who conducted the interviews. Inaccurate or insufficient records were revised through additional interviews and a review of the medical records. This study was approved by the Research Ethics Committee of Yonsei University Wonju College of Medicine, and the requirement for written consent was waived (YMRS-15-09-097).
2.3 Statistical analyses
A Chi-square test was performed to identify the variables associated with medical lethality due to suicide attempts. For statistically significant variables in the elderly group, a logistic regression analysis was performed and adjusted for education and monthly income. When medical lethality was classified into three categories, the severe group was relatively small, and there were many cases in which the value of a specific variable became zero, making regression analysis impossible. Therefore, the moderate and severe groups were combined into a mod/sev group and compared with the mild group. “Intent to die” and “medical lethality,” which showed prominent association, were analyzed using Spearman’s correlation coefficient. The age of the elderly attempters was grouped (Young-old: 60–74 years; Old-old: 75+). A p < 0.05 was considered statistically significant. The statistical analysis was performed using IBM SPSS Statistics (version 23.0; Armonk, NY, United States).
3 Results
A total of 604 suicide attempters (288 males and 316 females) were included in the analysis, of whom 253 were elderly (139 males and 114 females) and 351 were middle-aged (149 males and 202 females) (Table 1). Males ranged in age from 45 to 92 years with an average of 61.7 ± 11.9 (elderly: 60–92, 72.4 ± 7.7; middle-aged: 45–59, 51.8 ± 4.0), and females ranged in age from 45 to 98 years with an average of 59.1 ± 12.1 (elderly: 60–98, 73.1 ± 8.6; middle-aged: 45–59, 51.2 ± 3.9). The mild, moderate, and severe groups (medical lethality) included 39 (28.1%), 64 (46.0%), and 36 (25.9%) older males, and 37 (32.5%), 62 (54.4%), and 15 (13.2%) older females, respectively. In middle-aged males, it was 55 (36.9%), 77 (51.7%), and 17 (11.4%), and in middle-aged females, it was 95 (47.0%), 91 (45.0%), and 16 (7.9%), respectively. The proportion of high lethality (mod/sev) was higher in the elderly group than in the middle-aged group for both sexes (middle-aged males: 63.1%; older males: 71.9%; middle-aged females: 53%; and older females: 67.5%).
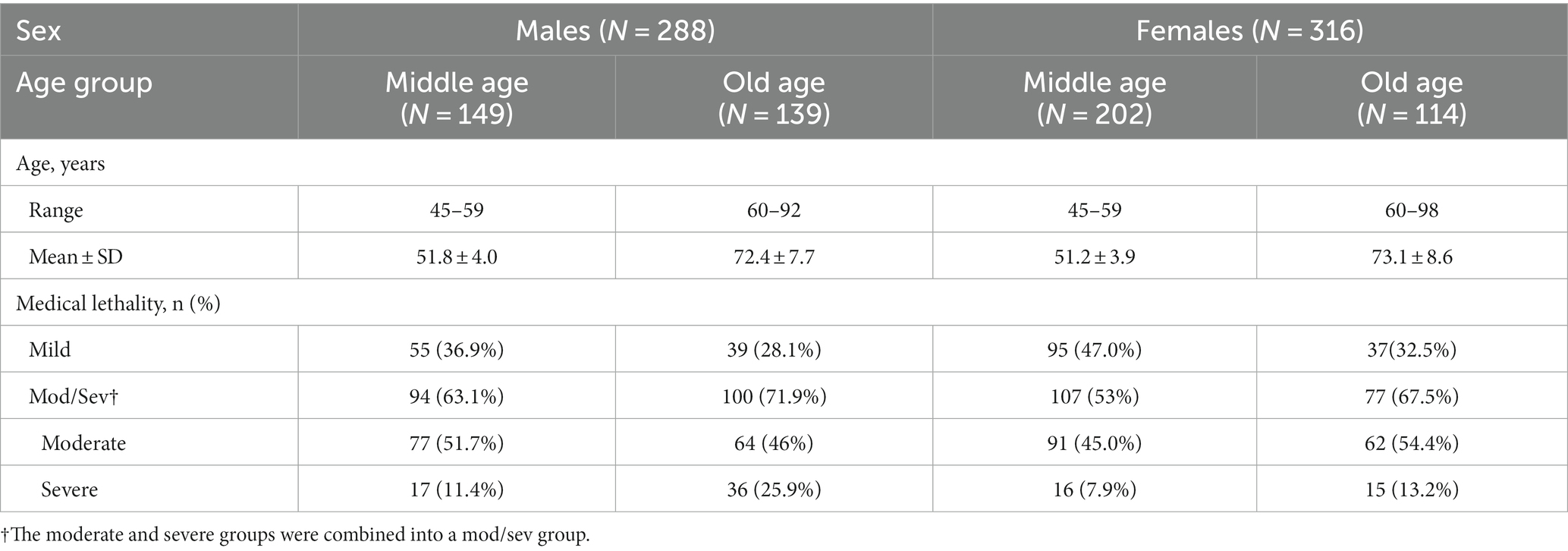
Table 1. Age distribution and medical lethality of subgroups.
Tables 2, 3 show the sociodemographic, clinical, and suicide attempt-related characteristics and their association with the dependent variable, medical lethality. In older females, lethality was associated with employment status (χ2 = 4.71, p = 0.03), with 24.3% of the mild lethality group being unemployed compared to 45.5% of the mod/sev group. In older males, lethality was lower when the motivation for the suicide attempt was bereavement (χ2 = 4.47; p = 0.04). Most older adults (>80%) attempted suicide by poisoning, with more use of psychiatric medication (χ2 = 4.82, p = 0.03) in the mild group and more use of pesticides and herbicides (χ2 = 5.12, p = 0.02) in the mod/sev group in older females. However, these substances were not associated with lethality in older males, and pesticide and herbicide use were the most common in both lethality groups (>50%). The association between intent to die and lethality was significant in middle-aged males (χ2 = 14.95, p < 0.01), middle-aged females (χ2 = 22.55, p < 0.01), and older males (χ2 = 28.99, p < 0.01), but not in older females (χ2 = 4.42, p = 0.11).
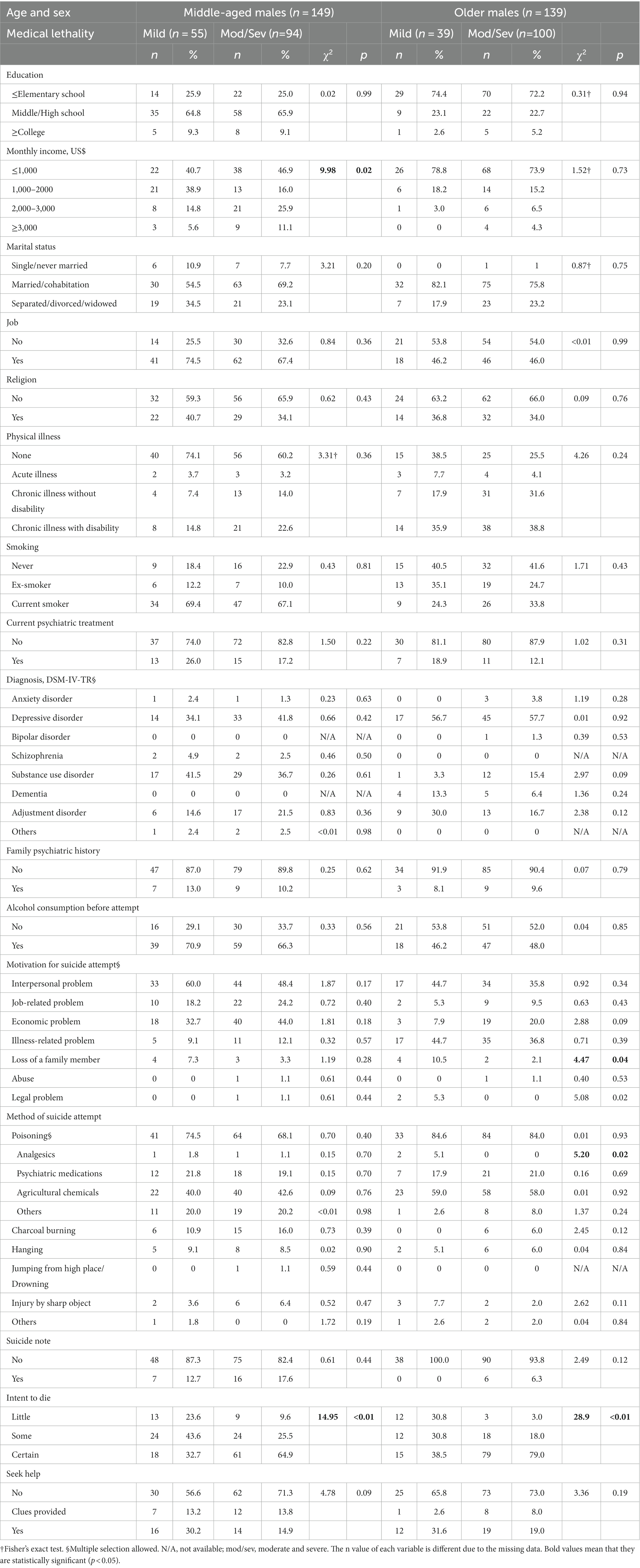
Table 2. Sociodemographic and clinical characteristics of the males.
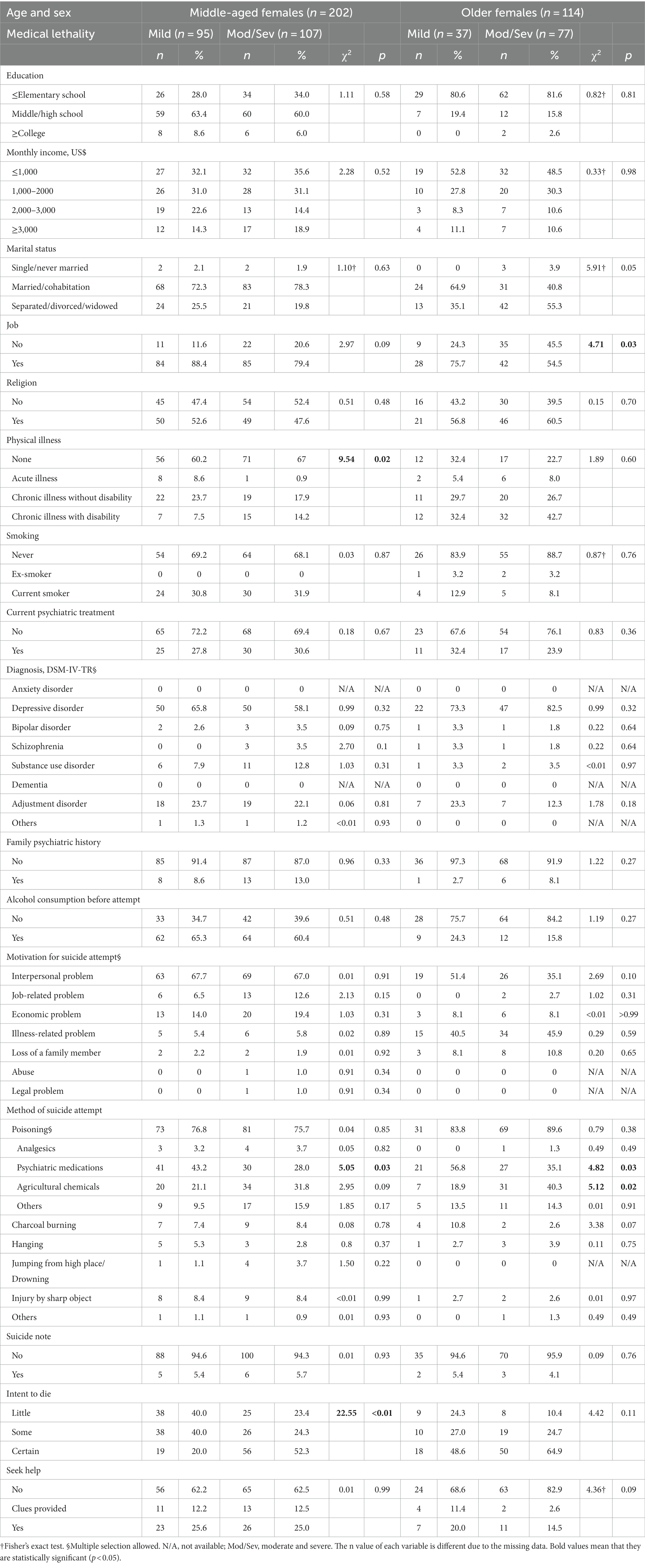
Table 3. Sociodemographic and clinical characteristics of the females.
Table 4 presents the odds ratios (OR) and confidence intervals (CI) for higher lethality in elderly individuals. In elderly males, the risk of higher lethality was lower when the motivation for the suicide attempt was the loss of a family member (OR: 0.18, CI: 0.03–1.04; Adjusted OR (AOR): 0.08, CI: 0.01–0.74), while increased risk was observed when the intent was “some” (OR: 6.00, CI: 1.39–25.86; AOR: 11.31, CI: 1.88–68.25) or “certain” (OR: 21.07, CI: 5.31–83.77; AOR: 28.75, CI: 5.17–160.78). In older females, the risk of higher lethality was lower when employed (OR: 0.39, CI: 0.16–0.93; AOR: 0.28, CI: 0.11–0.75) and when attempting suicide with psychiatric medication (OR: 0.41, CI: 0.19–0.92; AOR: 0.31, CI: 0.12–0.78), whereas the risk was higher when attempting suicide with pesticides or herbicides (OR: 2.89, CI: 1.13–7.40; AOR: 3.71, CI: 1.31–10.49). In elderly females, an increased risk was observed when the intent was “certain”; however, this was not significant after adjusting for education and monthly income (OR: 3.13, CI: 1.05–9.33; AOR: 2.68, CI: 0.84–8.54).
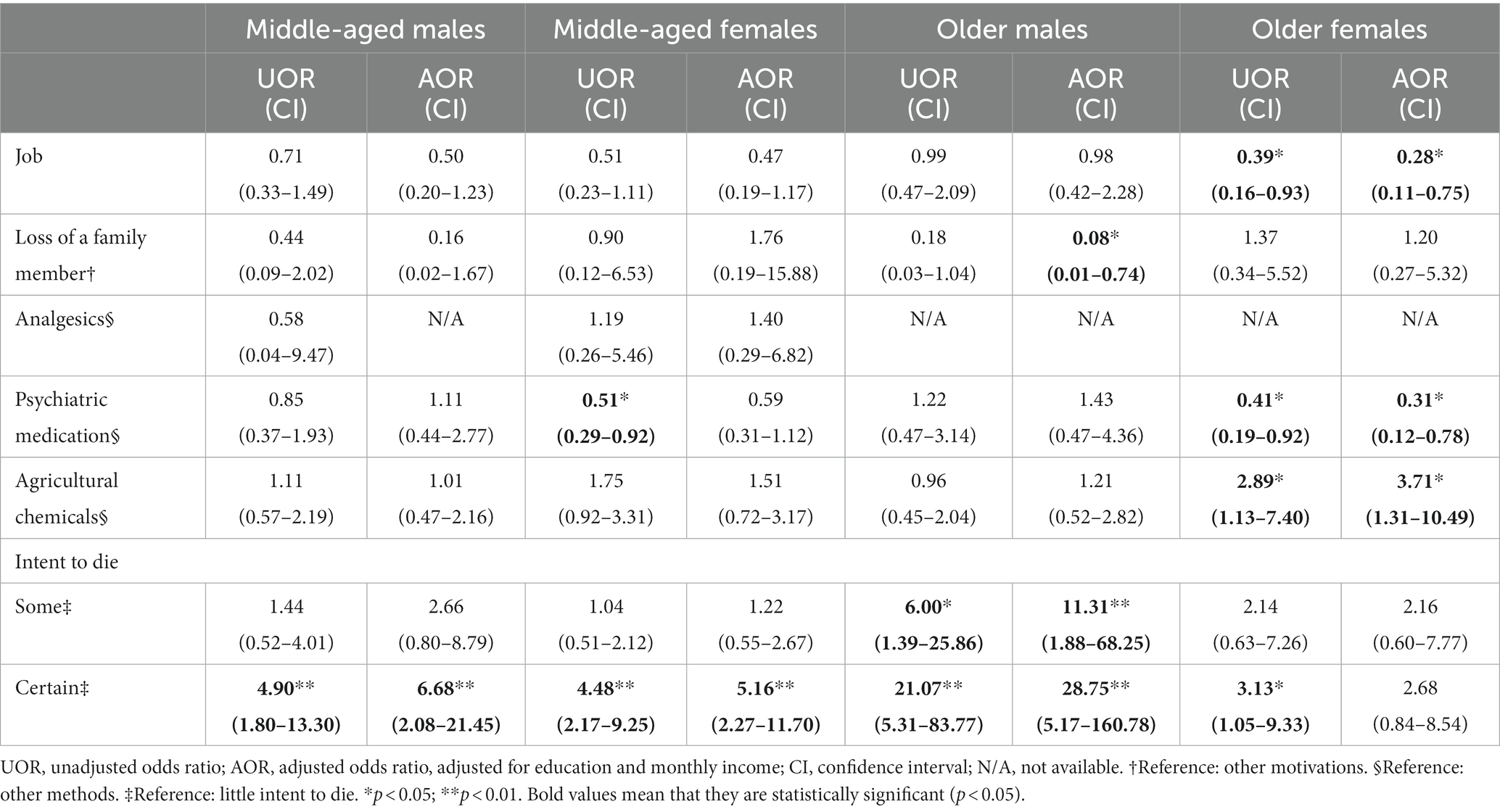
Table 4. Factors that affect medical lethality.
Figure 1 shows that the relationship between “intent to die” and “medical lethality” changes with age and that there are sex differences in these changes. In males, as intent increases (i.e., little, some, certain), the proportion of mild lethality decreases, and the proportion of severe lethality increases. Furthermore, this phenomenon becomes more pronounced in older age groups. In females, no such trend was observed with increasing age. Figure 1C shows the correlation between “intent to die” and “medical lethality” through Spearman’s correlation coefficient (rho). In males, the correlation between the two variables was significant at all ages, and the correlation coefficient increased as age increased (rho: middle age: 0.323, young old: 0.387, old-old: 0.415). However, in females, a significant correlation (rho: 0.329) was shown only in middle age.
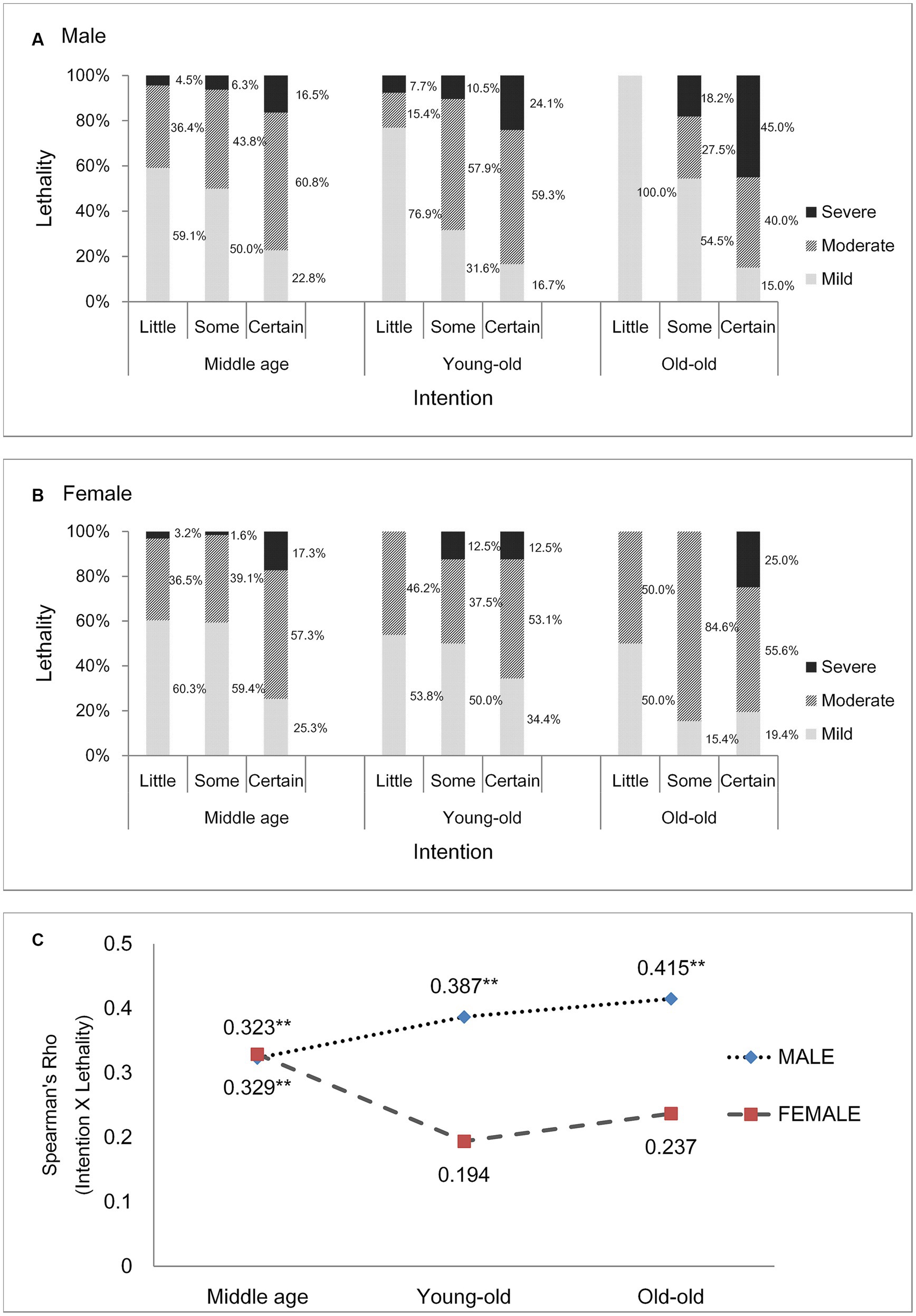
Figure 1. Correlation between intent to die and lethality. (A) Males, (B) females (bar: proportion of each lethality), (C) Spearman’s correlation coefficient. The symbol ** means it is statictically significant (p < 0.01).
4 Discussion
This study aimed to identify the factors that affect medical lethality in elderly suicide attempters and to verify whether the relationship between “intent to die” and “medical lethality” differs by sex. We found that in older males, the risk of lethality was lower when attempting suicide due to the loss of a family member compared to other motivations. The risk increased as intent became more definite, and this association became more pronounced with age. In older females, the risk was lower when employed or when attempting suicide with psychiatric medication and higher when using agricultural chemicals. Physical condition or help-seeking, which were expected to be closely related to lethality, were not significant in either sex.
The association between the intent to die and lethality was significant and increased with age in males. This association was similar in middle-aged females but was no longer present in older females. Factors such as the attempt method, ability to execute the attempt accurately, avoiding detection, time taken for transport, and physical health affect the course from intention to physical damage. However, sufficient research has not yet been conducted on how these factors differ by sex. Dombrovski et al. suggested that hormonal changes from aging affect the frontal cortex and executive function differently by sex, causing older males to be better at acting out their suicidal intent, leading to more significant physical damage (14). They also reported that prefrontal functions, such as reward delay and planning, are associated with lethality (20). It can also be speculated that physical vulnerability in older males allows for damage proportional to the intent to die. The shorter life expectancy of older males indirectly supports their higher vulnerability (21, 22). However, this does not explain why the association between intent and lethality observed in middle-aged females disappears in physically weaker, older females. This finding suggests that suicidal intent should be actively explored in older males, particularly in the older age groups. When a high level of intent is identified, treatment for psychopathology and preventive interventions for suicide should be initiated immediately. However, in older females, even if they are reported to have low suicidal intentions, caution is needed because the damage cannot be expected to be small.
In our study, both male and female elderly attempters most frequently used poison, especially psychiatric medications and agricultural chemicals (pesticides and herbicides), to attempt suicide. Self-poisoning was also the most common method used by elderly attempters in other countries (23, 24). The most frequently used substance is a psychiatric medication that is relatively less harmful than other substances. However, the use of agricultural chemicals is generally low except in a few countries, such as Korea and China (25, 26). In Korea, suicide attempts using agricultural chemicals are more common than in Taiwan and Japan, which have similar economic and sociocultural backgrounds (27, 28), because of limitations in the enactment and implementation of laws that restrict access to such substances (29). In addition, because the elderly population engaged in agriculture in the study area was considerable, it was not difficult for elderly attempters to obtain information about the chemicals and to access and acquire them. This implies that Korea needs to overhaul its laws restricting access and strengthening assessment of suicidality when older people buy agricultural chemicals. It remains unclear why this method, which can directly affect the degree of damage, was not associated with lethality in elderly males. Other aspects, such as the dose of the ingested substance or the intensity of the implementation, should be investigated in future studies. The importance of ascertaining the suicidal intention of older males is further emphasized in that the main determinant of lethality is suicidal intention rather than the method of the attempt.
Unemployment and job loss generally increase male suicide risk; however, the association increases in females with longer follow-up periods and older age (30–32). Similarly, in our study, lethality was low among older employed females. Deterioration in employment status may indirectly affect physical impairment in older adults through reduced self-esteem, depression, and hopelessness. Conversely, having a job may reflect that they are in good health condition. However, there is still no plausible explanation as to why this phenomenon occurs only in females. It is hoped that follow-up studies will shed light on how occupation has a sex-specific effect on these mediators and, eventually, physical damage.
A few studies reported that the impact of spousal death on suicidal behavior is greater in older males, while older females tend to become more affected over time (33, 34). However, this difference could not be confirmed in this study because bereavement, separation, and divorce were grouped into one category of marital status. Our results showed that the risk of high lethality was lower when the motivation for suicide attempt is the loss of a family member in older males. We did not examine whether the lost family member was the spouse. In addition, there were very few participants whose motivation for suicide was the loss of a family member. These altogether hinder us from explaining the results. Further study is needed to replicate our results.
This study had several limitations. First, objective comparison with other studies was challenging since a standardized scale was not used, and the interrater reliability may be low. Changes in cognitive function which are important in geriatric study were not evaluated using an objective scale such as the Mini-Mental Status Examination (MMSE). However, due to time limitations in the emergency department, the use of time-consuming assessment tools for suicide research could not be performed. Second, suicidal intent or related features may have been overreported which would have received less attention prior to the suicide attempt. Cohort studies can compensate for this problem; however, they are expensive due to the low suicide attempt rates within a general cohort. Third, it is difficult to generalize the study results to all older people for several reasons. First, this study had a relatively small sample size and was conducted at a single center. Second, both extremes of the lethality continuum, death and non-transfer, were excluded from the study. Nevertheless, this study was conducted over a long period at a hospital where most suicide attempters requiring medical intervention are transferred within a wide administrative area.
5 Conclusion
The suicidal intent reported by older males is closely related to lethality; therefore, appropriate measures are required that increase in importance with age. However, the lethality of suicide attempts in older females cannot be expected to be low, even if their intent is reported to be low; therefore, caution is needed. Compared with other suicidal motivations, bereavement of a family member has a lower risk of lethality in older males. In older females, the risk is lower when employed or attempting suicide with psychiatric medication and higher when attempting suicide with agricultural chemicals. Due to the lack of related studies, providing a sufficient evidence-based explanation for the influencing factors and sex-specific effects is challenging. Further studies with larger sample sizes and cases at both ends of the lethality continuum are needed to enable more detailed analysis.
Data availability statement
The datasets presented in this article are not readily available because the datasets for this article are not publicly available due to concerns regarding participant/patient anonymity. Requests to access the datasets should be directed to the corresponding author. Requests to access the datasets should be directed to M-HK, bWhraW0wOUB5b25zZWkuYWMua3I=.
Ethics statement
The studies involving humans were approved by the Research Ethics Committee of Yonsei University Wonju College of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
HKK: Investigation, Writing – review & editing, Formal analysis, Writing – original draft. SM: Writing – review & editing, Conceptualization, Project administration, Supervision. J-SA: Writing – review & editing, Investigation. HK: Investigation, Writing – review & editing, Data curation, Methodology. YC: Data curation, Investigation, Methodology, Writing – review & editing. JL: Data curation, Investigation, Methodology, Writing – review & editing, Resources, Validation. M-HK: Investigation, Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Suicide data. Available at: https://www.who.int/teams/mental-health-and-substance-use/data-resaerch/suicide-data (Accessed June 11, 2023).
2. World Health Organization. WHO mortality database. Available at: https://www.who.int/data/data-collection-tools/who-mortality-database (Accessed June 11, 2023).
3. Williams, RF, Doessel, DP, Sveticic, J, and De Leo, D. Accuracy of official suicide mortality data in Queensland. Aust NZ J Psychiatry. (2010) 44:815–22. doi: 10.3109/00048674.2010.483222
4. DeLeo, D, and Arnautovska, U. Prevention and treatment of suicidality in older adults In: R O’Connor and J Pirkis, editors. International handbook of suicide prevention research, policy and practice. Chichester: Wiley Blackwell (2016). 323–45.
5. Conwell, Y, Duberstein, PR, Cox, C, Herrmann, J, Forbes, N, and Caine, ED. Age differences in behaviors leading to completed suicide. Am J Geriatr Psychiatry. (1998) 6:122–6. doi: 10.1097/00019442-199805000-00005
6. Miller, M. Geriatric suicide: the Arizona study. Gerontologist. (1978) 18:488–95. doi: 10.1093/geront/18.5_Part_1.488
7. OECD: Fiscal challenges and inclusive growth in ageing societies. Available at: https://www.oecd.org/economy/ageing-inclusive-growth (Accessed June 11, 2023).
8. Choo, CC, Harris, KM, and Ho, RC. Prediction of lethality in suicide attempts: gender matters. Omega. (2019) 80:87–103. doi: 10.1177/0030222817725182
9. Gjelsvik, B, Heyerdahl, F, Holmes, J, Lunn, D, and Hawton, K. Is there a relationship between suicidal intent and lethality in deliberate self-poisoning? Suicide Life Threat Behav. (2017) 47:205–16. doi: 10.1111/sltb.12277
10. Horesh, N, Levi, Y, and Apter, A. Medically serious versus non-serious suicide attempts: relationships of lethality and intent to clinical and interpersonal characteristics. J Affect Disord. (2012) 136:286–93. doi: 10.1016/j.jad.2011.11.035
11. Haw, C, Hawton, K, Houston, K, and Townsend, E. Correlates of relative lethality and suicidal intent among deliberate self-harm patients. Suicide Life Threat Behav. (2003) 33:353–64. doi: 10.1521/suli.33.4.353.25232
12. Suokas, J, and Lönnqvist, J. Outcome of attempted suicide and psychiatric consultation: risk factors and suicide mortality during a five-year follow-up. Acta Psychiatr Scand. (1991) 84:545–9. doi: 10.1111/j.1600-0447.1991.tb03191.x
13. Beautrais, AL. Further suicidal behavior among medically serious suicide attempters. Suicide Life Threat Behav. (2004) 34:1–11. doi: 10.1521/suli.34.1.1.27772
14. Dombrovski, AY, Szanto, K, Duberstein, P, Conner, KR, Houck, PR, and Conwell, Y. Sex differences in correlates of suicide attempt lethality in late life. Am J Geriatr Psychiatry. (2008) 16:905–13. doi: 10.1097/JGP.0b013e3181860034
15. Hjelmeland, H, and Grøholt, B. A comparative study of young and adult deliberate self-harm patients. Crisis. (2005) 26:64–72. doi: 10.1027/0227-5910.26.2.64
16. Brown, GK, Henriques, GR, Sosdjan, D, and Beck, AT. Suicide intent and accurate expectations of lethality: predictors of medical lethality of suicide attempts. J Consult Clin Psychol. (2004) 72:1170–4. doi: 10.1037/0022-006X.72.6.1170
17. Blumenthal, SJ, and Kupfer, DJ. Overview of early detection and treatment strategies for suicidal behavior in young people. J Youth Adolesc. (1988) 17:1–23. doi: 10.1007/BF01538721
18. Oyama, H, Koida, J, Sakashita, T, and Kudo, K. Community-based prevention for suicide in elderly by depression screening and follow-up. Community Ment Health J. (2004) 40:249–63. doi: 10.1023/B:COMH.0000026998.29212.17
19. Kim, H, Ahn, JS, Kim, H, Cha, YS, Lee, J, Kim, MH, et al. Sociodemographic and clinical characteristics of old-old suicide attempters compared with young-old and middle-aged attempters. Int J Geriatr Psychiatry. (2018) 33:1717–26. doi: 10.1002/gps.4976
20. Dombrovski, AY, Szanto, K, Siegle, GJ, Wallace, ML, Forman, SD, Sahakian, B, et al. Lethal forethought: delayed reward discounting differentiates high- and low-lethality suicide attempts in old age. Biol Psychiatry. (2011) 70:138–44. doi: 10.1016/j.biopsych.2010.12.025
21. Gordon, EH, Peel, NM, Samanta, M, Theou, O, Howlett, SE, and Hubbard, RE. Sex differences in frailty: a systematic review and meta-analysis. Exp Gerontol. (2017) 89:30–40. doi: 10.1016/j.exger.2016.12.021
22. World Health Organization. Life expectancy at age 60. Available at: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/life-expectancy-at-age-60-(years) (Accessed June 11, 2023).
23. Nowers, M. Deliberate self-harm in the elderly: a survey of one London borough. Int J Geriatr Psychiatry. (1993) 8:609–14. doi: 10.1002/gps.930080713
24. Hawton, K, and Fagg, J. Deliberate self-poisoning and self-injury in older people. Int J Geriatr Psychiatry. (1990) 5:367–73. doi: 10.1002/gps.930050604
25. Ticehurst, S, Carter, GL, Clover, KA, Whyte, IMG, Raymond, J, and Fryer, J. Elderly patients with deliberate self-poisoning treated in an Australian general hospital. Int Psychogeriatr. (2002) 14:97–105. doi: 10.1017/S1041610202008311
26. Chiu, HFK, Lam, LCW, Pang, AHT, Leung, CM, and Wong, CK. Attempted suicide by Chinese elderly in Hong Kong. Gen Hosp Psychiatry. (1996) 18:444–7. doi: 10.1016/S0163-8343(96)00063-1
27. Wu, KC-C, Chen, Y-Y, and Yip, PSF. Suicide methods in Asia: implications in suicide prevention. Int J Environ Res Public Health. (2012) 9:1135–58. doi: 10.3390/ijerph9041135
28. Kim, S, Kim, M-H, Kawachi, I, and Cho, Y. Comparative epidemiology of suicide in South Korea and Japan: effects of age, gender and suicide methods. Crisis. (2011) 32:5–14. doi: 10.1027/0227-5910/a000046
29. Cha, ES, Khang, Y-H, and Lee, WJ. Mortality from and incidence of pesticide poisoning in South Korea: findings from national death and health utilization data between 2006 and 2010. PLoS One. (2014) 9:e95299–9. doi: 10.1371/journal.pone.0095299
30. Kposowa, AJ. Unemployment and suicide: a cohort analysis of social factors predicting suicide in the US national longitudinal mortality study. Psychol Med. (2001) 31:127–38. doi: 10.1017/S0033291799002925
31. Qin, P, Agerbo, E, and Mortensen, PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register–based study of all suicides in Denmark, 1981–1997. Am J Psychiatry. (2003) 160:765–72. doi: 10.1176/appi.ajp.160.4.765
32. Corcoran, P, and Arensman, E. Suicide and employment status during Ireland’s Celtic tiger economy. Eur J Pub Health. (2011) 21:209–14. doi: 10.1093/eurpub/ckp236
33. Erlangsen, A, Jeune, B, Bille-Brahe, U, and Vaupel, JW. Loss of partner and suicide risks among oldest old: a population-based register study. Age Ageing. (2004) 33:378–83. doi: 10.1093/ageing/afh128
Keywords: sex difference, old age, suicide attempt, lethality, suicide intent
Citation: Kim H, Min S, Ahn J-S, Kim H, Cha YS, Lee J and Kim M-H (2023) Sex differences in the factors that affect medical lethality in elderly suicide attempters. Front. Psychiatry. 14:1260295. doi: 10.3389/fpsyt.2023.1260295
Edited by:
Gonzalo Martinez-Ales, Columbia University, United StatesReviewed by:
Yari Gvion, Bar-Ilan University, IsraelS. M. Yasir Arafat, Enam Medical College, Bangladesh
Copyright © 2023 Kim, Min, Ahn, Kim, Cha, Lee and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min-Hyuk Kim, bWhraW0wOUB5b25zZWkuYWMua3I=