 Guodong Xu
Guodong Xu Lian Li
Lian Li Lijuan Yi1
Lijuan Yi1- 1Ningbo Medical Center Lihuili Hospital, Zhejiang, China
- 2Department of Psychiatry, Ningbo Kangning Hospital & Affiliated Mental Health Centre, Ningbo University, Zhejiang, China
Background: Previous studies examining trends in sleep loss among adolescents have mainly focused on single countriy and region. This study aims to analyze temporal trends in the prevalence of anxiety-induced sleep loss among adolescents from 29 countries in five regions.
Methods: This study used data from the Global School-based Student Health Survey 2003–2018, which surveyed 215,380 adolescents from 29 countries with at least two cross-sectional surveys per country. The weighted country-specific prevalence of anxiety-induced sleep loss and trends across the survey years were evaluated. Random- or fixed-effects meta-analyses were used to calculate pooled prevalence and temporal trends across 29 countries.
Results: Temporal variations in anxiety-induced sleep loss across countries were identified. Increasing (Suriname, Vanuatu, and Myanmar), decreasing (Namibia, Jamaica, the Philippines, Samoa, and Indonesia), and stable (all other countries) trends in anxiety-induced sleep loss were noted. The pooled weighted prevalence of anxiety-induced sleep loss was 11.35 and 10.67% in the first and last surveys, respectively. There was no meaningful change in the propensity to have anxiety-related sleep disorders over time, with the reduction and OR of these two surveys being 0.54 (−0.53–1.61) and 0.98 (0.88–1.10). For subgroup analyses, no significant differences in pooled anxiety-induced sleep loss trends were seen between the two surveys for different sexes, regions, incomes, survey years in the first wave, survey periods, or number of surveys.
Conclusion: Trends in the prevalence of anxiety-induced sleep loss in adolescents varied significantly across different countries. Generally, a stable trend was observed in 21 of the 29 countries surveyed. Our study provides data that can aid policymakers in establishing country-specific strategies for reducing anxiety-induced sleep loss in adolescents.
1. Introduction
Sleep is extremely important to health, especially for adolescents, who are in a formative period of development, with both their brains and bodies experiencing rapid growth. For adolescents, sufficient and good-quality sleep plays a vital role in mental, physical, and emotional development (1). Unfortunately, research indicates that many adolescents have poor quality and insufficient sleep (2), which can harm their physical growth. Anxiety has been consistently cited as one of the main causes of sleep loss (3), which can manifest as trouble in falling asleep, staying asleep, or waking up too early. Harvey’s cognitive model of insomnia supports this, as excessively negative cognitive activities, such as anxiety, are strongly associated with the initiation and persistence of sleep loss (4). Indeed, large studies have reported that anxiety is positively associated with sleep problems in both adolescents (5) and adults (6).
A population-based study of 82 countries reported the prevalence of anxiety-induced sleep loss to be 10% in adolescents aged 12–17 years (7). A 10-year time-trend analysis in Brazil showed that the prevalence of adolescents’ lost sleep from worry increased from 9.4% in 2006 to 9.6% in 2011 and then significantly increased to 13.3% in 2016 (8). The prevalence of daily difficulties falling asleep in Denmark adolescents increased from 7.0 to 13.4% in 1991–2018 (9). In addition, a large international study reported that 28 of 33 (84.8%) European countries/regions surveyed had an increasing prevalence of sleeping difficulties in adolescents (10). A decreasing trend in the prevalence of anxiety-induced sleep loss was reported in the Philippines from 2003 to 2011 (11) and in Lebanon from 2005 to 2017 (12). Besides, stable trends were noted from 2005/2006 to 2016 in the United Arab Emirates (12) and Morocco (13). A study in Korea suggested that the prevalence of individual meeting recommendations sleep guidelines were stable, and from 9.7% in 2013 to 10.3% in 2018 (14). However, most of these studies focused on single country or region, with pooled trends in the prevalence of adolescents’ anxiety-induced sleep loss in global being rarely studied.
Therefore, the aim of this study was to describe the trends in the prevalence of anxiety-induced sleep loss among adolescents using nationally representative datasets from 29 countries, and then examine the pooled trends across them. The findings of this study provide invaluable evidence for the development and implementation of relevant policies and programs in worldwide to address this issue.
2. Methods
The Global School-based Student Health Survey (GSHS) is a multi-country, repeated, cross-sectional survey that was conducted by the World Health Organization and the US Centers for Disease and Control and Prevention. The core aim of this survey was to investigate the prevalence of, and trends in, healthy and unhealthy behaviors and major noncommunicable diseases among school-aged adolescents worldwide. The multi-survey data were obtained from the GSHS. The specific questionnaires used in the survey are available on the WHO1 and CDC2 websites. Briefly, 12–15-year-old adolescents in education were selected using two-stage cluster sampling for each survey (15). In the first stage of the cluster sampling, schools were randomly selected from a list of all schools in the country using the probability proportionate to size method. In the second stage of the sampling process, several classrooms that included high proportions of students of the target age were selected for inclusion from within each of the participating schools, and all students in the selected classes were included in the sampling frame. To allow direct comparisons to be made between each country, the standardized questionnaire modules used were those for which test–retest reliability had already been established (16) and that had been translated into the appropriate languages with no changes in the questions. All data collection was performed during regular class time using computer-scannable sheets. All surveys conducted as part of the GSHS worldwide were approved by the ministry of health or education and an institutional review board or ethics committee in each country. Adolescents voluntarily took part in the GSHS, and verbal or written consent was obtained from each adolescent and their parents or guardians.
From the publicly available GSHS data, we identified countries that participated in at least two nationally representative surveys from 2003 to 2018 and whose datasets included anxiety-induced sleep loss as a variable.
Ultimately, data from 29 countries were included in our study (Supplementary Figure S1). Information relating to anxiety-induced sleep loss was obtained with the question “During the past 12 months, how often have you been so worried about something that you could not sleep at night?” (13) with response options of 1 (never), 2 (rarely), 3 (sometimes), 4 (most of the time), and 5 (always) with scores coded as 1–3 = 0 and 4–5 = 1, The adolescents who were identified as having anxiety-induced sleep loss were coded as 1. Confounding variables included sex, age, and hunger. Hunger was evaluated with the question “How often did you go hungry because there was not enough food in your home during the past 30 days?” with the same response options of 1 (never) to 5 (always).
2.1. Statistical analysis
The prevalence of anxiety-induced sleep loss was reported by weighted prevalence and 95% confidence intervals (CIs) using the SAS software PROC SURVEYMEANS procedure. We added weights, strata, and a primary sampling unit to every set of school-aged adolescents to reflect the weighting process and the two-stage sampling design. The pooled estimates of prevalence and the differences between countries were calculated by fixed−/random-effects meta-analysis using STATA and the Higgins’s I2 statistic was used to estimate between-country heterogeneity. An I2 value <25% was considered as negligible heterogeneity and a fixed-effects meta-analysis was performed. Otherwise, we used a random-effects meta-analysis for analysis. After adjusting for sex, age and hunger, the between-survey differences and country-specific estimated odds ratio (OR) for the prevalence of anxiety-induced sleep loss were estimated using the SAS software PROC SURVEYREG and PROC SURVEYLOGISTIC procedure (17, 18). Subgroup analyses were stratified by sex (males vs. females), WHO region [Africa (AFR), Americas (AMR), Eastern Mediterranean (EMR), Western Pacific (WPR) and South-East Asia (SEAR)], World Bank income level (low, lower-middle, upper-middle and high), survey year in first wave (<2008 and ≥ 2008), inter-survey period (≤ 7 years and > 7 years) and number of surveys (2 and > 2). Sensitivity analyses were conducted to determine the stability of the pooled estimates after excluding each study in turn. Meta-regression analysis was used to explore the sources of heterogeneity. SAS version 9.4 (SAS Institute, Cary, NC, United States) and STATA version 12.0 (Stata Corporation, College Station, TX) were used to perform statistical analyses. A two-sided p values less than 0.05 were considered statistically significant.
3. Results
Of the countries included in this study, three were in AFR, ten were in AMR, four were in EMR, seven were in WPR and five were in SEAR (Table 1). Three countries were low-income, eight were lower middle-income, eleven were upper middle-income and seven were high income. The initial survey in each country was conducted from 2003 to 2011, and the last surveys were conducted from 2010 to 2018. The median inter-survey period was 7 years. The response rates ranged from 96.76% in Kuwait (2015) to 100% in Benin and the Cook Islands (2009) (Table 1).
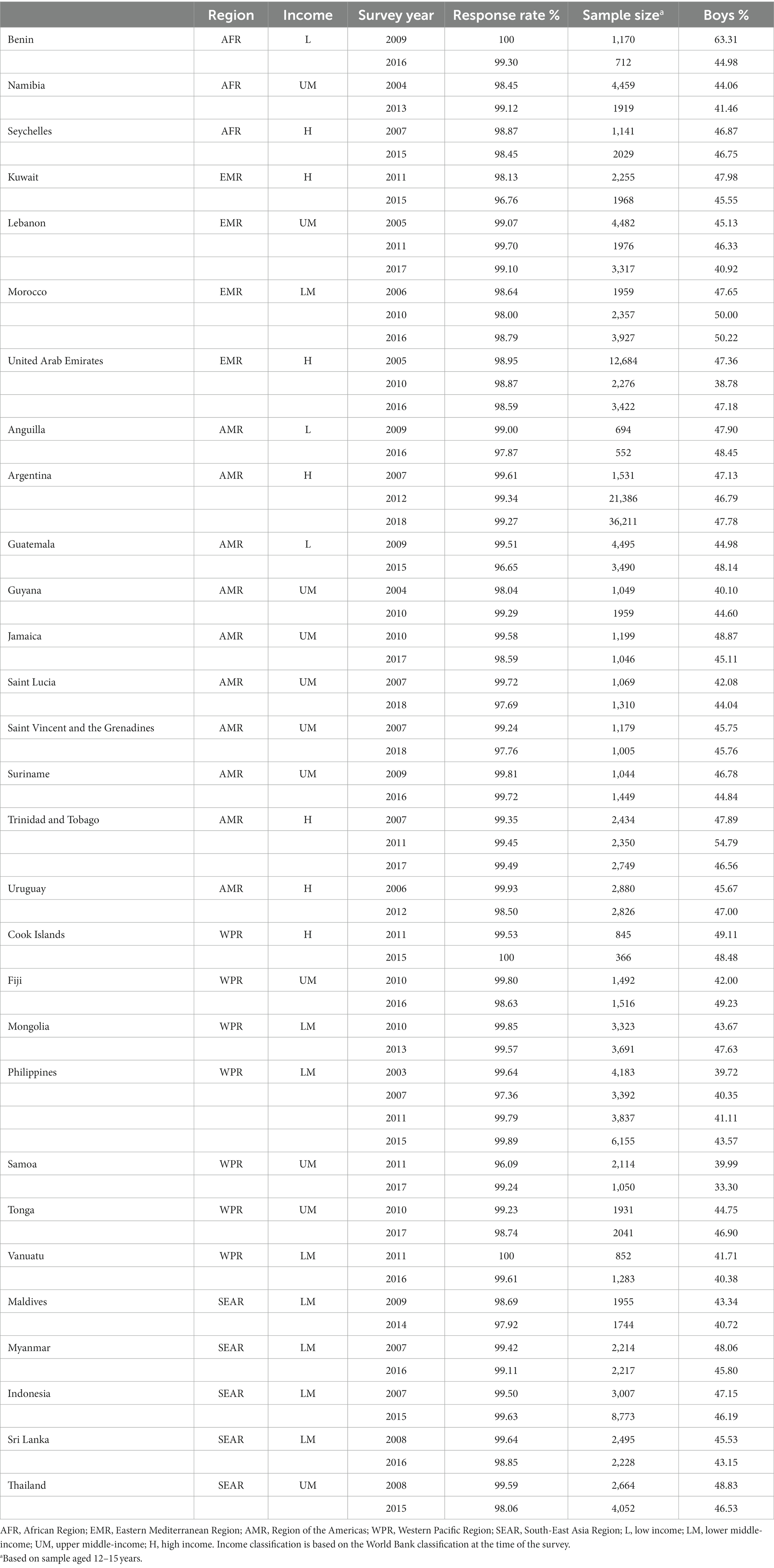
Table 1. Survey characteristics.
The country-specific and pooled estimates of anxiety-induced sleep loss prevalence, and their trends, are shown in Figure 1 and Supplementary Table S1. In the initial survey, the prevalence of anxiety-induced sleep loss ranged from 1.75% (1.05–2.45%) in Myanmar to 27.44% (23.87–31.02%) in Samoa (Supplementary Table S1 and Figure 1). On a regional scale, prevalence ranged from 6.56% (3.54–9.58%) in SEAR to 15.58% (10.47–20.69%) in AFR (Table 2). In the last survey, the prevalence of anxiety-induced sleep loss ranged from 3.59% (2.79–4.39%) in Myanmar to 18.31% (14.80–21.82%) in Kuwait (Supplementary Table S1 and Figure 1) and ranged from 10.03% (7.45–12.62%) in WPR to 14.20% (12.28–16.11%) in EMR (Table 2). The reduction in the prevalence of anxiety-induced sleep loss between the first and last surveys ranged from −2.88% (−5.52−−0.24%) in Suriname to 18.35% (14.57–22.13%) in Samoa (Figure 2 and Supplementary Table S1).
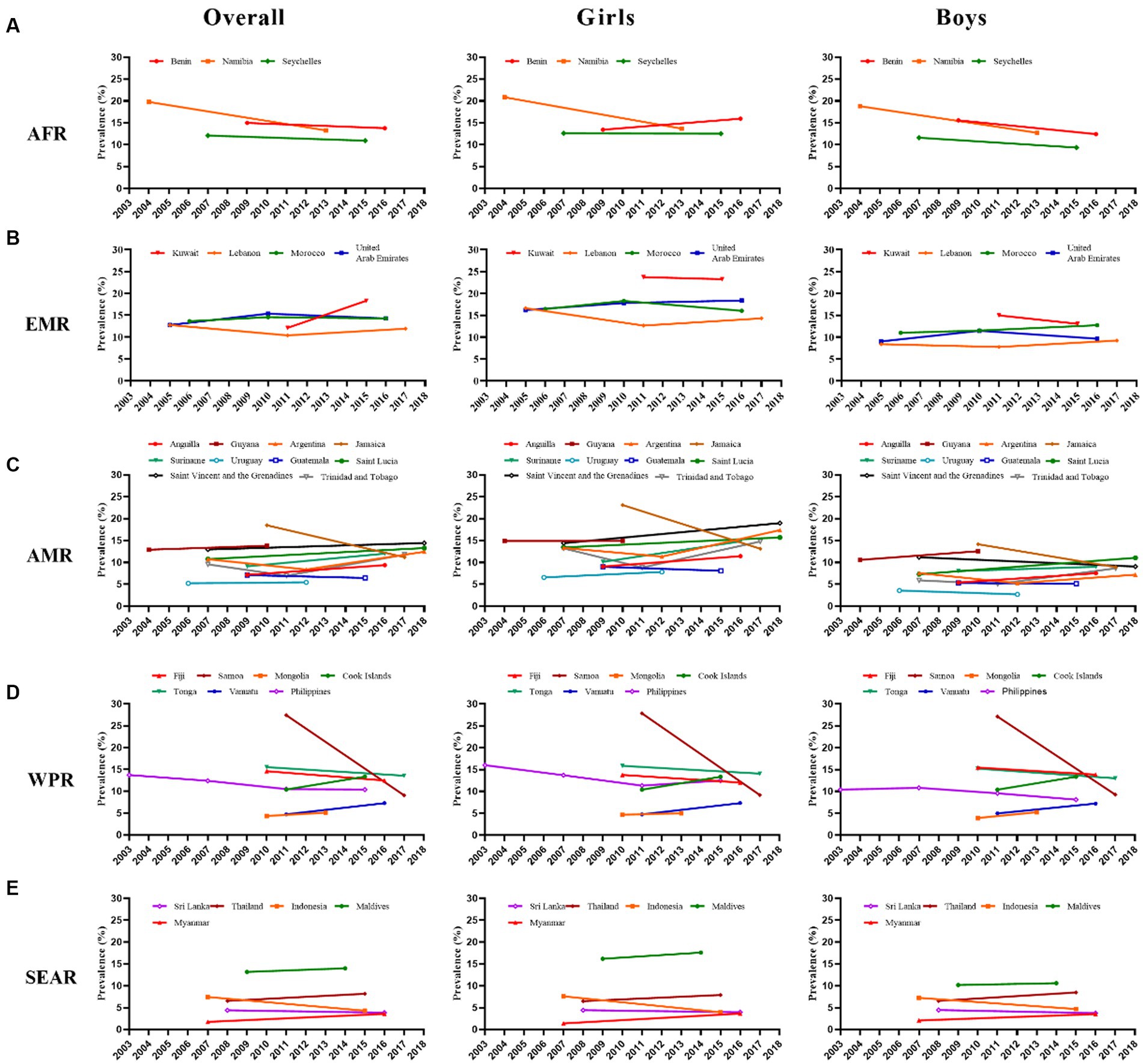
Figure 1. Trends in prevalence (%) of anxiety-induced sleep loss by country, region, and sex. (A) African Region (AFR), (B) Eastern Mediterranean Region (EMR), (C) Region of the Americas (AMR), (D) Western Pacific Region (WPR), (E) South-East Asia Region (SEAR).
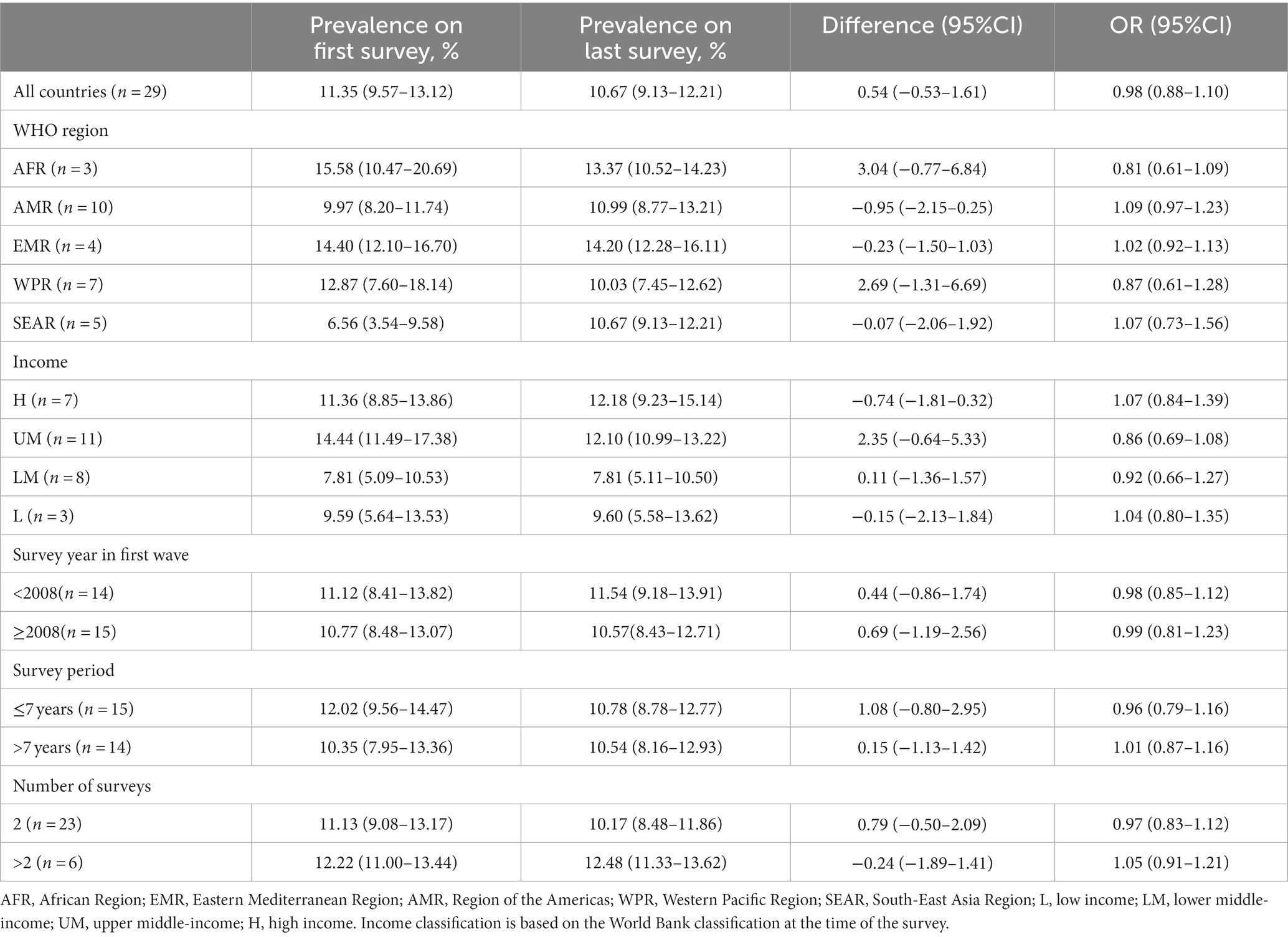
Table 2. Subgroup prevalence and trend of anxiety based on 29 countries from the global school-based student health surveys.
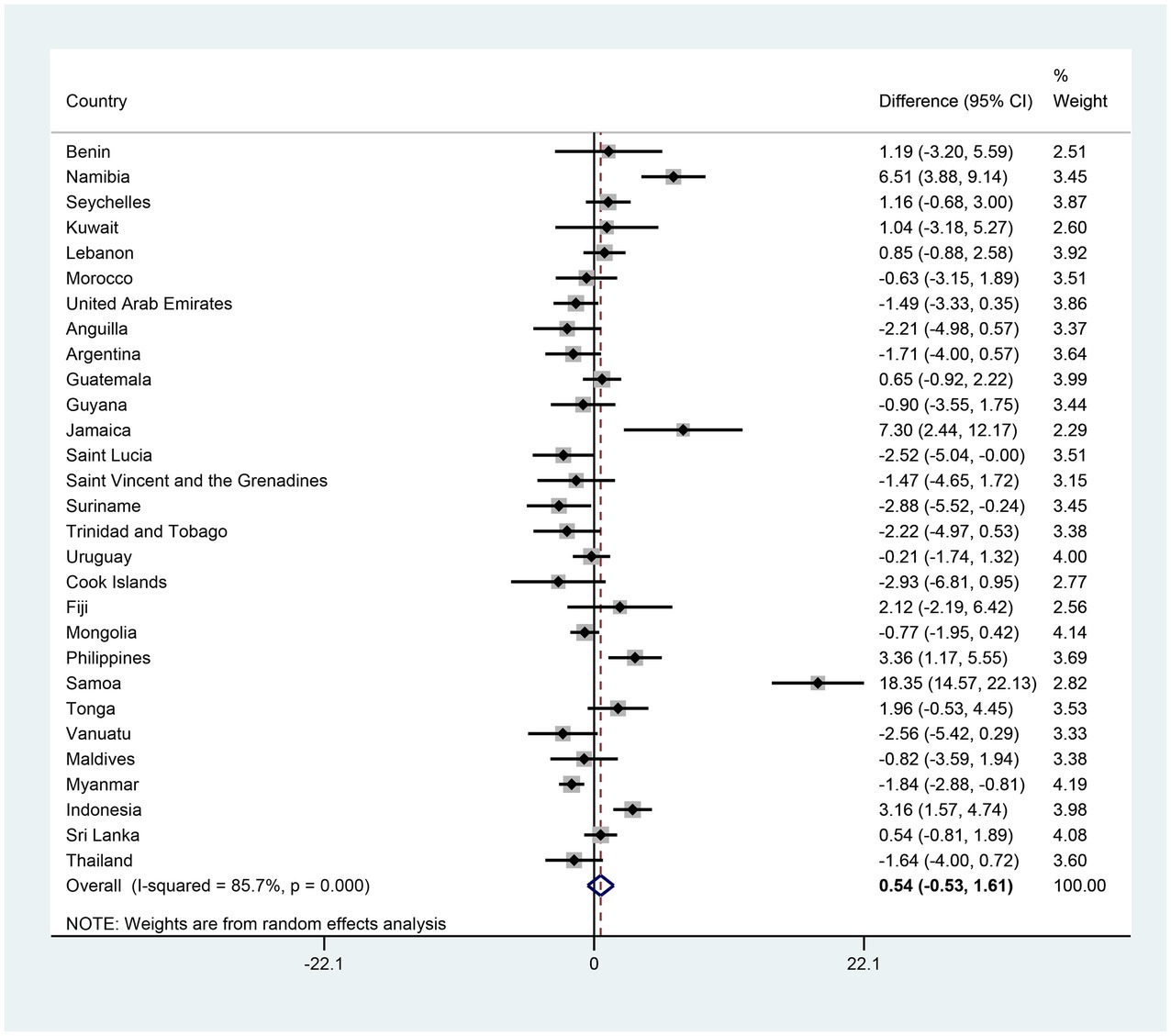
Figure 2. The country-specific and pooled difference of anxiety-induced sleep loss. The black diamonds and horizontal line represent the difference and their 95% confidence interval (CI), the gray box size represents the weight of the country, and the bottom diamond represents the pooled difference and 95% CI.
The pooled estimates of anxiety-induced sleep loss prevalence were 11.35 and 10.67% in the first and the last survey, respectively; however, the adjusted reduction and adjusted OR (AOR) for the two surveys was 0.54 (−0.53–1.61) and 0.98 (0.88–1.10), suggesting that there was no significant trend in the prevalence of anxiety-induced sleep loss between the first and last surveys in adolescents (Figures 2, 3 and Supplementary Table S1). In terms of countries, five countries (Namibia, Jamaica, the Philippines, Samoa and Indonesia) exhibited significant decreases in the prevalence of anxiety-induced sleep loss over the study period, with AORs ranging from 0.30 in Samoa to 0.76 in the Philippines (Figure 3 and Supplementary Table S1). In contrast, the prevalence of anxiety-induced sleep loss significantly increased in three countries (Suriname, Vanuatu, and Myanmar), with AORs ranging from 1.36 in Suriname to 2.23 in Myanmar (Figure 3 and Supplementary Table S1). In the other 21 countries, the prevalence of anxiety-induced sleep loss remained stable over the study period (Figure 3 and Supplementary Table S1).
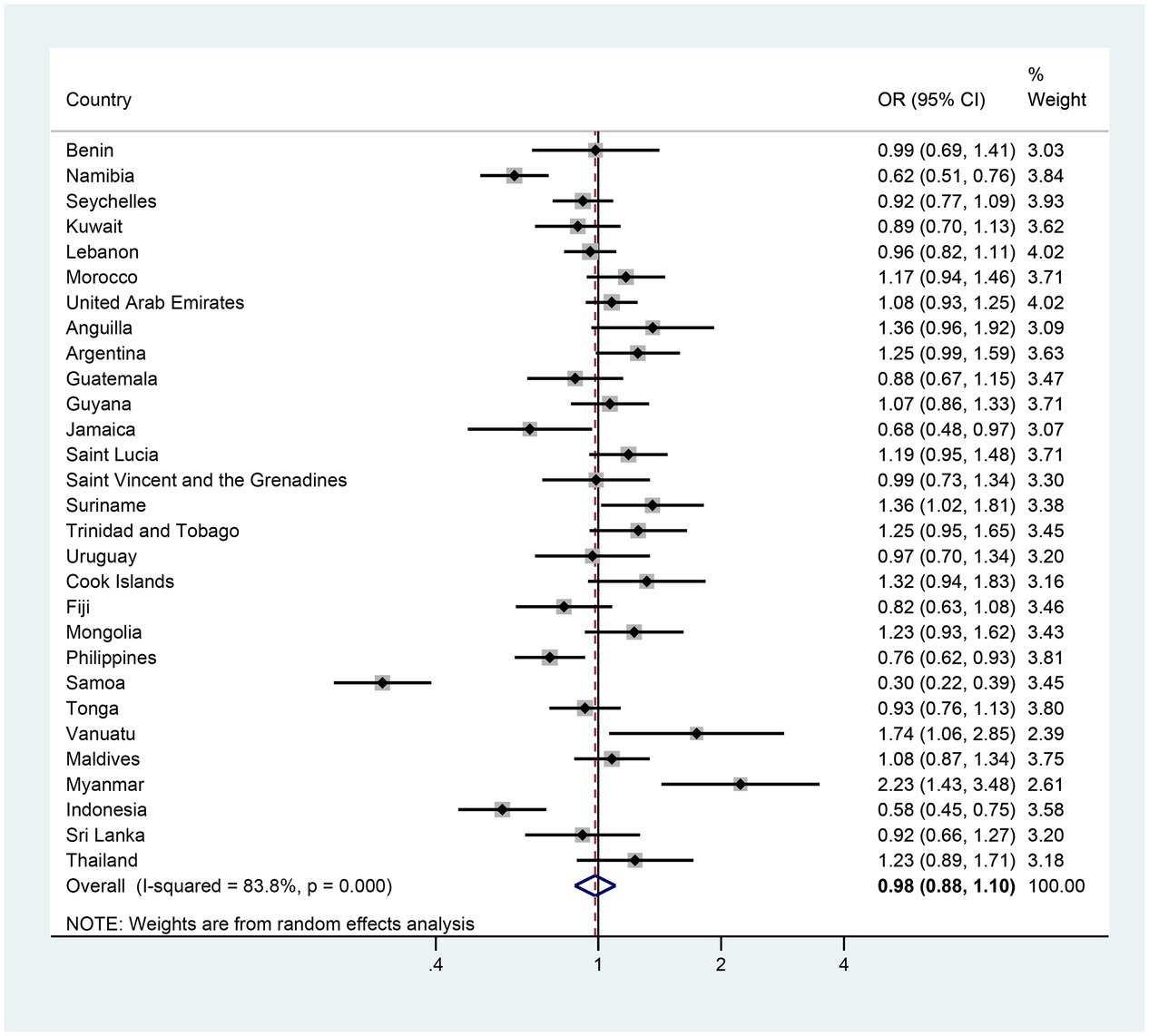
Figure 3. The country-specific and pooled estimated trend of anxiety-induced sleep loss. The black diamonds and horizontal line represent the OR and their 95% confidence interval (CI), the gray box size represents the weight of the country, and the bottom diamond represents the pooled OR and 95% CI.
In girls specifically, 7 of the 29 countries demonstrated significant changes in the prevalence of anxiety-induced sleep loss between the first and last surveys. Five countries (Namibia, Jamaica, the Philippines, Samoa and Indonesia) exhibited a significant decrease in prevalence, with AORs was ranging from 0.30 in Samoa to 0.74 in the Philippines (Figure 4 and Supplementary Table S2). In contrast, two countries (Argentina and Myanmar) experienced a significant increase, with AORs of 1.41 and 2.92 (Figure 4 and Supplementary Table S2). The remaining 22 countries showed a stable trend in the prevalence of anxiety-induced sleep loss (Figure 4 and Supplementary Table S2). In boys, three countries (Namibia, Samoa and Indonesia) experienced significant decreases in the prevalence of anxiety-induced sleep loss, with AORs ranging from 0.30 in Samoa to 0.65 in Indonesia (Figure 5 and Supplementary Table S3). Conversely, two countries (Vanuatu and Myanmar) displayed significant increases in prevalence, with AORs of 2.28 and 1.70, respectively (Figure 5 and Supplementary Table S3). The remaining 24 countries had a stable trend (Figure 5 and Supplementary Table S3).

Figure 4. The country-specific and pooled estimated trend of anxiety-induced sleep loss in girls. The black diamonds and horizontal line represent the OR and their 95% confidence interval (CI), the gray box size represents the weight of the country, and the bottom diamond represents the pooled OR and 95% CI.
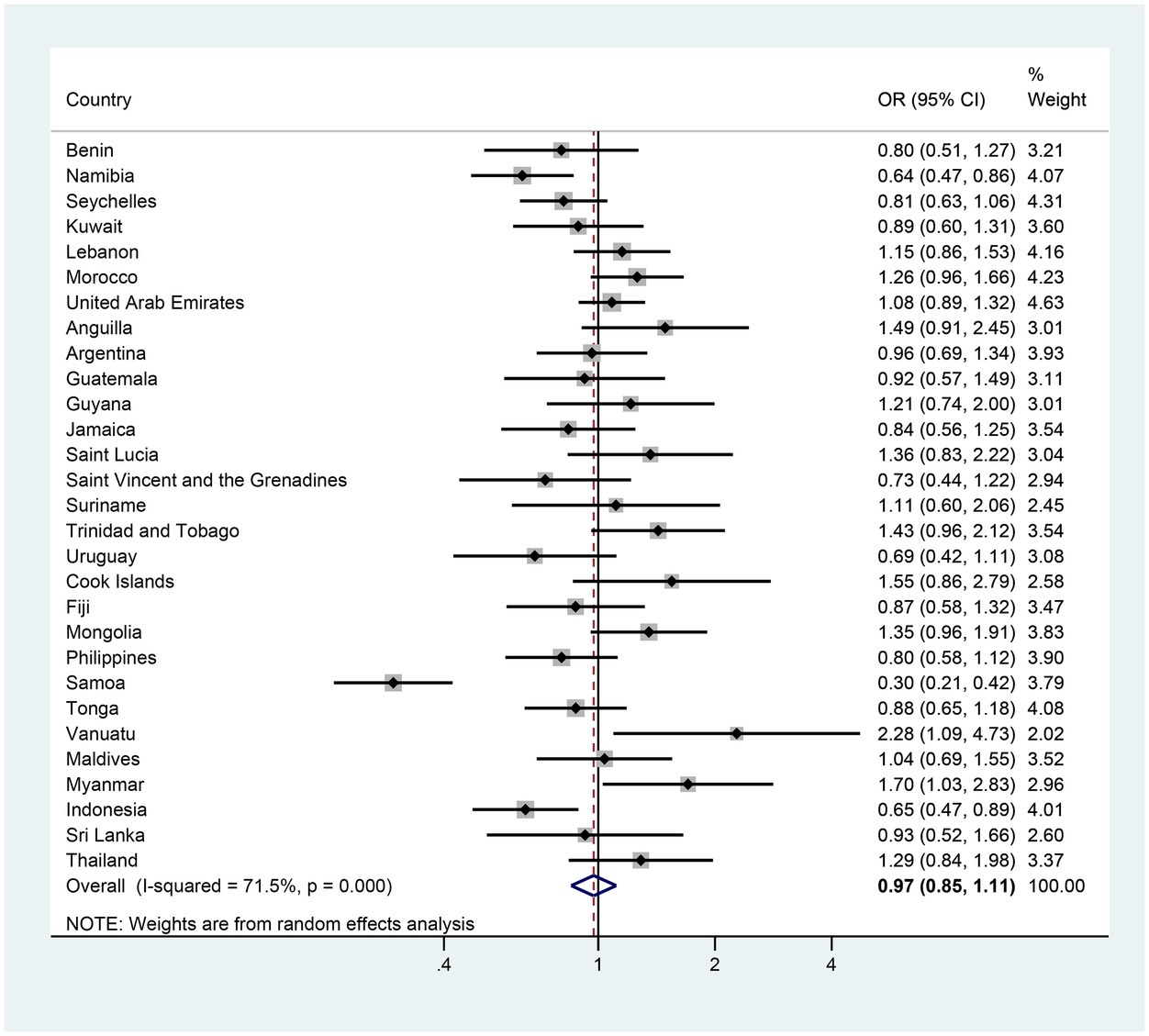
Figure 5. The country-specific and pooled estimated trend of anxiety-induced sleep loss in boys. The black diamonds and horizontal line represent the OR and their 95% confidence interval (CI), the gray box size represents the weight of the country, and the bottom diamond represents the pooled OR and 95% CI.
After adjusting for sex, age and hunger, no significant changes were identified in the prevalence of anxiety-induced sleep loss between the first and last surveys for different regions, income levels, survey year in first wave, lengths of survey period or number of surveys (Table 2). Sensitivity analyses did not alter any of these global trends in the prevalence of anxiety-induced sleep loss (Supplementary Figure S4) and the result of meta-regression also confirmed it (p = 0.902).
4. Discussion
This study found that the prevalence of anxiety-induced sleep loss varied widely across the 29 countries, with most countries having high prevalence of such anxiety-induced sleep loss. We also described plateauing, increasing, and decreasing trends in the prevalence of anxiety-induced sleep loss across different countries and regions.
A previous global study of 82 countries reported the prevalence of sleep loss over anxiety to be 10% in 12–17-year-old adolescents (7). Given that sleep loss significantly correlates with suicidal ideation, plans and attempts (19), it is extremely important to address sleep loss in children. In our study, the pooled weighted prevalence of anxiety-induced sleep loss was 11.35 and 10.67% in the first and last surveys and the OR of these two surveys was 0.98 (0.88–1.10), suggesting a plateauing trend in the prevalence of anxiety-induced sleep loss in adolescents in 29 countries. The high prevalence of anxiety-induced sleep loss might be due to environmental factors, social inequality (9) or policy (7). Based on the GSHS data, smoking (2), bullying and victimization (20), reduced fruit intake (21) and sedentary behavior (22) are all related to increased prevalence of anxiety-induced sleep loss in adolescents. Unfortunately, numerous studies have found that such behaviors have remained common in adolescents over time (23), with some even increasing in prevalence, such as sedentary behavior (24). In addition, a previous study conducted in GSHS reported that nearly one in three of these countries had no specific mental health policy (7), suggesting significant neglection of mental health and a shortage of appropriate health services in those countries.
We noted a consistently higher prevalence of anxiety-induced sleep loss in girls than in boys in Supplementary Tables S2, S3, which aligns with studies carried out in Canada (25), the United States (26) and Brazil (8). Indeed, sex inequality in the prevalence of anxiety-induced sleep loss has long been reported (26), suggesting that a tendency for severe anxiety in females has not abated. Females are more likely to be both anxious and stressed than males, potentially due to higher estrogen and progesterone levels in their bodies (27). Moreover, females tend to experience mistreatment more often and have been reported to internalize their distress more than their male counterparts (28). In fact, suicidal ideation and anxiety were both higher in females than their male counterparts (7). As such, more attention should be paid to the mental status of females. However, plateauing trends of the two surveys in the prevalence of anxiety-induced sleep loss were both shown in boys and girls, which further suggested the clinically meaningful of reducing anxiety-induced sleep loss. In addition, the prevalence is greater in higher income countries, which was consisted with the pervious study (2), however, in another study (7) conducted in GSHS showed low-income countries have the highest prevalence of anxiety-induced sleep loss, the difference may be due to varied country were included.
In our study, 6 of the 29 countries examined had conducted more than two surveys. However, only the Philippines exhibited a decreasing trend in the prevalence of anxiety-induced sleep loss. Such improvements might be due to the existence of school-based mental health education and other public health strategies in the Philippines (29, 30). Indeed, multiple surveys suggesting a stable high prevalence of anxiety-induced sleep loss should warrant the attention of state authorities in other countries. The findings of the GSHS have important implications for curbing the stable high prevalence of anxiety-induced sleep loss. Effective policies (e.g., rational emotive behavioral education and social emotional learning) should be implemented to mitigate anxiety-induced sleep loss in school-aged adolescents (31). Furthermore, healthy lifestyles that could effectively reduce anxiety in adolescents should be advocated (32). Parental and peer relationships have strong association with adolescent anxiety (7). Thus, parents and educators should maintain parental and peer relationships with adolescents. Additionally, adolescents should be taught coping mechanisms for dealing with sleep loss, such as going to bed at a consistent time and reducing the use of electronic devices, especially in the hour before bedtime (33). Finally, excessive use of electronic devices has been associated with both anxiety and insomnia (34, 35), especially when used at bedtime. It is worth noting that the long-term frequent use of electronic devices has become more prevalent in recent years in many countries (36), which may be contributing to insomnia.
This is the first study of global trends in the prevalence of anxiety-induced sleep loss in adolescents. Using GSHS data provides this study with the strength of standardized data collection and a regular data collection time. Moreover, the survey data collected for each country was nationally representative, due to a large random sample drawn from a wide variety of geographic and cultural settings. However, some limitations also need to be acknowledged. First, only 29 countries had at least two survey waves, which limits the generalizability of our findings to worldwide. Second, only school-attending adolescents aged 12–15 years were included in our study, and thus, selection bias may exist within the samples due to low school attendance in some countries. It is possible that the characteristics of school-attending adolescents changed over the study period, resulting in an additional influence on the temporal trends observed in our study. Therefore, future studies of temporal trends in the prevalence of anxiety-induced sleep loss should also include non-school-attending adolescents, to represent the entire adolescent population. Third, anxiety-induced sleep loss was measured using a single self-report item, which may have resulted in bias being introduced into this study. Fourth, the various surveys included in this study were conducted in different years and had different survey period. Therefore, the temporal trends identified are not comparable across countries. However, the results did not differ significantly stratified by the median of the year of the first survey (2008) or survey period (7 years). In addition, high heterogeneity was found across countries, and random-effects model ws used to reduce the effect. Finally, given that some countries provided more survey data, the accuracy of our findings may vary between countries.
In conclusion, our study reports that the trends in the prevalence of anxiety-induced sleep loss vary significantly across countries, with a stable prevalence of anxiety-induced sleep loss seen across 29 countries. These findings highlight the need to develop specific interventions to mitigate anxiety-induced sleep loss in adolescents. Our study provides data that policymakers can use to establish country-specific strategies for reducing anxiety-induced sleep loss in adolescent populations.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the all surveys conducted as part of the GSHS worldwide were approved by the ministry of health or education and an institutional review board or ethics committee in each country. Adolescents voluntarily took part in the GSHS, and verbal or written consent was obtained from each adolescent and their parents or guardians. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
GX: Writing – original draft, Writing – review & editing. LL: Investigation, Methodology, Writing – original draft. LY: Investigation, Methodology, Writing – original draft. TL: Data curation, Writing – original draft. QC: Data curation, Writing – original draft. JZ: Writing – original draft, Writing–review–&–editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1259442/full#supplementary-material
Footnotes
References
1. Tarokh, L, Saletin, JM, and Carskadon, MA. Sleep in adolescence: physiology, cognition and mental health. Neurosci Biobehav Rev. (2016) 70:182–8. doi: 10.1016/j.neubiorev.2016.08.008
2. Wang, Q. Tobacco use and sleep loss over worry among adolescents aged 12-15 years: a population-based study of 38 countries. J Glob Health. (2020) 10:020427. doi: 10.7189/jogh.10.020427
3. Dregan, A, Lallukka, T, and Armstrong, D. Potential pathways from biopsychosocial risk factors to sleep loss due to worry: a population-based investigation. J Public Ment Health. (2013) 12:43–50. doi: 10.1108/17465721311304230
4. Harvey, AG. A cognitive model of insomnia. Behav Res Ther. (2002) 40:869–93. doi: 10.1016/S0005-7967(01)00061-4
5. Kim, H, Kim, SH, Jang, SI, and Park, EC. Association between sleep quality and anxiety in Korean adolescents. J Prev Med Public Health. (2022) 55:173–81. doi: 10.3961/jpmph.21.498
6. McGowan, SK, Behar, E, and Luhmann, M. Examining the relationship between worry and sleep: a daily process approach. Behav Ther. (2016) 47:460–73. doi: 10.1016/j.beth.2015.12.003
7. Biswas, T, Scott, JG, Munir, K, Renzaho, AMN, Rawal, LB, Baxter, J, et al. Global variation in the prevalence of suicidal ideation, anxiety and their correlates among adolescents: a population based study of 82 countries. EClinicalMedicine. (2020) 24:100395. doi: 10.1016/j.eclinm.2020.100395
8. Dos Santos, AT, Soares, FC, Lima, RA, Dos Santos, SJ, Silva, CRM, Bezerra, J, et al. Violence and psychosocial stress: a 10-year time trend analysis. J Affect Disord. (2021) 295:116–22. doi: 10.1016/j.jad.2021.08.011
9. Holstein, BE, Ammitzboll, J, Damsgaard, MT, Pant, SW, Pedersen, TP, and Skovgaard, AM. Difficulties falling asleep among adolescents: social inequality and time trends 1991-2018. J Sleep Res. (2020) 29:e12941. doi: 10.1111/jsr.12941
10. Ghekiere, A, Van Cauwenberg, J, Vandendriessche, A, Inchley, J, Gaspar de Matos, M, Borraccino, A, et al. Trends in sleeping difficulties among European adolescents: are these associated with physical inactivity and excessive screen time? Int J Public Health. (2019) 64:487–98. doi: 10.1007/s00038-018-1188-1
11. Peltzer, K, and Pengpid, S. Health risk behaviour among in-school adolescents in the Philippines: trends between 2003, 2007 and 2011, a cross-sectional study. Int J Environ Res Public Health. (2015) 13:73. doi: 10.3390/ijerph13010073
12. Pengpid, S, and Peltzer, K. Trends in the prevalence of twenty health indicators among adolescents in United Arab Emirates: cross-sectional national school surveys from 2005, 2010 and 2016. BMC Pediatr. (2020) 20:357. doi: 10.1186/s12887-020-02252-0
13. Pengpid, S, and Peltzer, K. Trends of 20 health risk behaviours among adolescents in Morocco: results of three National Cross-Sectional School Surveys of 2006, 2010 and 2016. Int J Gen Med. (2021) 14:1611–9. doi: 10.2147/IJGM.S283137
14. Lee, EY, Khan, A, Uddin, R, Lim, E, and George, L. Six-year trends and intersectional correlates of meeting 24-hour movement guidelines among south Korean adolescents: Korea youth risk behavior surveys, 2013-2018. J Sport Health Sci. (2023) 12:255–65. doi: 10.1016/j.jshs.2020.11.001
15. Han, L, You, D, Gao, X, Duan, S, Hu, G, Wang, H, et al. Unintentional injuries and violence among adolescents aged 12-15 years in 68 low-income and middle-income countries: a secondary analysis of data from the global school-based student health survey. Lancet Child Adolesc Health. (2019) 3:616–26. doi: 10.1016/S2352-4642(19)30195-6
16. Brener, ND, Collins, JL, Kann, L, Warren, CW, and Williams, BI. Reliability of the youth risk behavior survey questionnaire. Am J Epidemiol. (1995) 141:575–80. doi: 10.1093/oxfordjournals.aje.a117473
17. Lee, SW. Regression analysis for continuous independent variables in medical research: statistical standard and guideline of life cycle committee. Life Cycle. (2022) 2:2. doi: 10.54724/lc.2022.e3
18. SAS/STAT User’s Guide. Introduction to Survey Sampling and Analysis Procedures: The Survey Procedures. Available at: https://documentation.sas.com/doc/en/pgmsascdc/9.4_3.5/statug/titlepage.htm (Accessed July 2, 2022).
19. Wong, MM, Brower, KJ, and Craun, EA. Insomnia symptoms and suicidality in the National Comorbidity Survey – adolescent supplement. J Psychiatr Res. (2016) 81:1–8. doi: 10.1016/j.jpsychires.2016.06.004
20. Hasan, MM, Fatima, Y, Smith, SS, Tariqujjaman, M, Jatrana, S, and Mamun, AA. Geographical variations in the association between bullying victimization and sleep loss among adolescents: a population-based study of 91 countries. Sleep Med. (2022) 90:1–8. doi: 10.1016/j.sleep.2021.12.014
21. Liu, MW, Chen, QT, Towne, SD Jr, Zhang, J, Yu, HJ, Tang, R, et al. Fruit and vegetable intake in relation to depressive and anxiety symptoms among adolescents in 25 low- and middle-income countries. J Affect Disord. (2020) 261:172–80. doi: 10.1016/j.jad.2019.10.007
22. Zhang, Y, Chen, S, Wang, C, Zhang, X, Zou, L, Chi, X, et al. Does more sedentary time associate with higher risks for sleep disorder among adolescents? A pooled analysis. Front Pediatr. (2021) 9:603177. doi: 10.3389/fped.2021.603177
23. Fan, H, and Zhang, X. Prevalence of and trends in the co-existence of obesogenic Behaviors in adolescents from 15 countries. Front Pediatr. (2021) 9:664828. doi: 10.3389/fped.2021.664828
24. Iannotti, RJ, and Wang, J. Trends in physical activity, sedentary behavior, diet, and BMI among US adolescents, 2001-2009. Pediatrics. (2013) 132:606–14. doi: 10.1542/peds.2013-1488
25. Gariepy, G, and Elgar, FJ. Trends in psychological symptoms among Canadian adolescents from 2002 to 2014: gender and socioeconomic differences. Can J Psychiatr. (2016) 61:797–802. doi: 10.1177/0706743716670130
26. Mojtabai, R, and Jorm, AF. Trends in psychological distress, depressive episodes and mental health treatment-seeking in the United States: 2001–2012. J Affect Disord. (2015) 174:556–61. doi: 10.1016/j.jad.2014.12.039
27. Hoyt, LT, and Falconi, AM. Puberty and perimenopause: reproductive transitions and their implications for women's health. Soc Sci Med. (2015) 132:103–12. doi: 10.1016/j.socscimed.2015.03.031
28. Altemus, M, Sarvaiya, N, and Neill, EC. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. (2014) 35:320–30. doi: 10.1016/j.yfrne.2014.05.004
29. Bonito, SR, Westergaard, LS, and Velayudhan, R. Philippines In: CE Aldinger and C Vince Whitman, editors. Case studies in global school health promotion. New York, NY: Springer (2009). 337–48.
30. Villaverde, M, and Vergeire, M. (2012). Socorro de los Santos M. health promotion and non-communicable diseases in the Philippines current status and priority policy interventions and actions. Available at: http://www.ateneo.edu/sites/default/files/ASoG-HJ%20Health%20Promotion%20Study%202012_0.pdf (Accessed July 2, 2022).
31. Ahinkorah, BO, Aboagye, RG, Arthur-Holmes, F, Hagan, JE Jr, Okyere, J, Budu, E, et al. A multi-country analysis of prevalence of anxiety-induced sleep disturbance and its associated factors among in-school adolescents in sub-Saharan Africa using the global school-based health survey. Healthcare. (2021) 9:234. doi: 10.3390/healthcare9020234
32. Otsuka, Y, Kaneita, Y, Spira, AP, Mojtabai, R, Itani, O, Jike, M, et al. Trends in sleep problems and patterns among Japanese adolescents: 2004 to 2017. Lancet Reg Health West Pac. (2021) 9:100107. doi: 10.1016/j.lanwpc.2021.100107
33. Gradisar, M, Wolfson, AR, Harvey, AG, Hale, L, Rosenberg, R, and Czeisler, CA. The sleep and technology use of Americans: findings from the National Sleep Foundation's 2011 sleep in America poll. J Clin Sleep Med. (2013) 9:1291–9. doi: 10.5664/jcsm.3272
34. Lange, K, Cohrs, S, Skarupke, C, Gorke, M, Szagun, B, and Schlack, R. Electronic media use and insomnia complaints in German adolescents: gender differences in use patterns and sleep problems. J Neural Transm. (2017) 124:79–87. doi: 10.1007/s00702-015-1482-5
35. Harbard, E, Allen, NB, Trinder, J, and Bei, B. What's keeping teenagers up? Prebedtime Behaviors and actigraphy-assessed sleep over School and vacation. J Adolesc Health. (2016) 58:426–32. doi: 10.1016/j.jadohealth.2015.12.011
Keywords: adolescents, prevalence, trends, anxiety-induced sleep loss, difference
Citation: Xu G, Li L, Yi L, Li T, Chai Q and Zhu J (2023) A pooled analysis of temporal trends in the prevalence of anxiety-induced sleep loss among adolescents aged 12–15 years across 29 countries. Front. Psychiatry. 14:1259442. doi: 10.3389/fpsyt.2023.1259442
Edited by:
Nirinjini Naidoo, University of Pennsylvania, United StatesReviewed by:
Brendan T. Keenan, University of Pennsylvania, United StatesDong Keon Yon, Kyung Hee University, Republic of Korea
Copyright © 2023 Xu, Li, Yi, Li, Chai and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junyang Zhu, NTY5MDc3MzU5QHFxLmNvbQ==
†These authors have contributed equally to this work