 Kun-Zhe Tsai1,2,3†
Kun-Zhe Tsai1,2,3† Pang-Yen Liu4
Pang-Yen Liu4 Yen-Po Lin5Chen-Chih Chu4
Yen-Po Lin5Chen-Chih Chu4 Wei-Chun Huang6
Wei-Chun Huang6 Xuemei Sui7
Xuemei Sui7 Carl J. Lavie8
Carl J. Lavie8 Gen-Min Lin1,4*†
Gen-Min Lin1,4*†- 1Department of Medicine, Hualien Armed Forces General Hospital, Hualien, Taiwan
- 2Department of Stomatology of Periodontology, Mackay Memorial Hospital, Taipei, Taiwan
- 3Department of Dentistry, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
- 4Department of Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
- 5Department of Critical Care Medicine, Taipei Tzu Chi Hospital, New Taipei City, Taiwan
- 6Department of Critical Care Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
- 7Department of Exercise Science, Arnold School of Public Health, University of South Carolina, Columbia, SC, United States
- 8Ochsner Clinical School, John Ochsner Heart and Vascular Institute, The University of Queensland School of Medicine, New Orleans, LA, United States
Backgrounds: This study aimed to clarify the association of American guideline-based leisure time physical activity (PA) level with mental health in 4,080 military personnel in Taiwan.
Methods: The moderate intensity PA level was assessed according to the total running time per week (wk) reported in a self-administered questionnaire over the previous 6 months and was categorized into PA level <150, 150–299, and ≥300 min/wk. Mental stress was assessed by the Brief Symptom Rating Scale (BSRS)-5 for which ≥15 points were classified as great mental stress. Suicide ideation (SI) was graded as 1 for mild, 2 for moderate, and 3 or 4 for severe. Multivariable logistic regression analysis was employed to determine the association between PA and mental health while adjusting for demographics, smoking, alcohol intake, betel nut chewing, and obesity.
Results: As compared to participants with a PA level of <150 min/wk., those with PA levels 150–299 min/wk. and ≥ 300 min/wk. had a lower possibility of SI ≥1 [odds ratios (ORs) and 95% confidence intervals (CIs): 0.58 (0.40–0.83) and 0.23 (0.14–0.36), respectively] and SI ≥1 and/or BSRS-5 ≥ 15 [ORs: 0.55 (0.39–0.79) and 0.21 (0.13–0.34), respectively]. The possibilities were more significantly lower for SI ≥2 [ORs: 0.37 (0.20–0.68) and 0.10 (0.04–0.26), respectively] and SI ≥2 and/or BSRS-5 ≥ 15 [ORs: 0.35 (0.20–0.62) and 0.10 (0.04–0.25), respectively].
Conclusion: Our findings indicate that participating in moderate-intensity leisure time PA level for ≥150 min/wk. may have a positive effect on mental health among military personnel. The impact appears to be even more significant when engaging in a higher PA level of ≥300 min/wk.
Introduction
Mental health disorder, manifesting as psychological distress, is a leading cause of the global health burden (1). One in eight individuals worldwide encounters a mental health disorder, and nearly half of all individuals experience such a disorder at some point in their life (1). For military personnel, exposure to combat and rescue, witnessing traumatic events, and the military culture, characterized by strict hierarchies, long deployments, and a sense of duty, can lead to a range of mental health issues, e.g., suicidality, insomnia, anxiety, hostility, depression, and interpersonal sensitivity (2). Suicidality is a serious issue that has not declined appreciably in several decades, and there is no accurate predictor of increased risk for suicide (3). Previous reports have shown that nearly 24 out of every 100,000 soldiers in the US died by suicide (4, 5). Although several studies have been done in the armed forces of the US in the past decade and recently in 2020–21, when the suicide rate in the armed forces reduced approximately 15%, the suicide rate again increased rapidly in the first quarter of 2023 (6, 7). With this alarming trend, mental health promotion has been a critical agenda for the armed forces.
Physical activity (PA) forms an integral part of military life because physical training is designed to improve physical fitness and is always encouraged and even required. The newly published World Health Organization (WHO) guidelines report that frequent PA has a beneficial impact on cardiometabolic as well as cardiovascular disease (CVD) risk, and is also therapeutic for people with psychological distress (8). The effect of PA is even comparable to that of anti-depressants and psychotherapy in some cases (9). We have shown very marked improvements in psychological distress, including depression, anxiety, and hostility, in patients with CVD following a formal PA/cardiac rehabilitation program that improves levels of cardiorespiratory fitness (CRF) (10–15). Despite growing recognition of the importance of frequent PA to improve mental health (8), these investigations did not provide a specific threshold. The American guideline recommends a moderate-intensity leisure time PA level, e.g., running ≥150 min/week (wk) for civilian adults (8, 16). However, it is unclear whether the guideline-based PA level also benefits mental health for military personnel. Therefore, this study aimed to examine the association between moderate-intensity PA levels during leisure time and mental health in a large sample of military subjects in Taiwan.
Materials and methods
Study population
Individuals for this cross-sectional study were included from the main study of the cardiorespiratory fitness and health in the armed forces (CHIEF) in Taiwan (17). All participants underwent regular annual whole-body health examinations in the Hualien Armed Forced General Hospital, the only military referral hospital in East Taiwan in 2014. Only the participants who completed the available questionnaire on leisure time PA levels and psychological distress assessment were recruited for this study (18, 19). The Institutional Ethics Committee approval (No. 16-05-008) from the Mennonite Christian Hospital in Taiwan was obtained at the beginning of the study, and all participants gave informed consent.
Clinical and biochemical assessment
Each participant responded to a questionnaire regarding their personal information and substance use experience (cigarette smoking, alcohol drinking, and betel nut chewing). Anthropometric parameters for waist circumference, body height, and body weight were further measured in a standing position. The body mass index (BMI) was calculated as body weight (kilograms) divided by the square of body height (meters). General obesity was defined as BMI ≥27 kg/m2, and abdominal obesity was defined as a waist circumference ≥90 cm in men and ≥80 cm in women (20–22).
The hemodynamic information about systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse rate was obtained from the right upper arm, using the automatic blood pressure monitoring machine (Parama-Tech Co Ltd., Fukuoka, Japan). Serum metabolic biomarkers, including total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride, fasting glucose (FPG), serum uric acid (SUA), blood urea nitrogen (BUN), and creatinine, and blood cells information about white blood cell count (WBC), red blood cell count (RBC), hemoglobin, and platelet count were obtained from participants’ overnight fasting blood samples (17, 23).
Mental health assessment
Mental health was assessed using one question on suicide ideation (SI) and the 5-item Brief Symptom Rating Scale (BSRS-5) scores (24–26), which comprised trouble falling asleep (insomnia), feeling tense (anxiety), feeling easily annoyed or irritated (hostility), feeling low in mood (depression), and feeling inferior to others (interpersonal sensitivity). The scoring of each domain of the BSRS-5 and SI used a five-point Likert-type scale, where 0 = not at all, 1 = mild, 2 = moderate, 3 = severe, and 4 = extremely severe. Traditionally, normal, slight, moderate, and great psychological distress has been defined by the sum of BSRS-5 scores ≤5, 6–9, 10–14, and ≥ 15, respectively. Internal consistency (Cronbach alpha) coefficients for the BSRS-5 score ranged between 0.77 and 0.90. The test–retest reliability coefficient was 0.82 (24). In this study, those with SI ≥2 and the BSRS-5 ≥ 15 were considered to have great psychological distress, which was the main outcome in this study. The secondary outcomes in this study were the psychological distress separately assessed by various degrees of SI, the BSRS-5 scores >5, ≥10, and ≥ 15, and each domain of the BSRS-5 ≥ 2 (over moderate degree).
Moderate intensity PA level
Through a questionnaire, the moderate-intensity PA level of each participant was assessed by weekly total running time on average during leisure time in the past 6 months based on the 2018 American guideline, with <150, 150–299, and ≥300 min/wk. considered as low, adequate and high levels, respectively (16).
Statistical analysis
The demographic and clinical characteristics were expressed as numbers (%) for categorical data, and mean ± standard deviation (SD) for continuous data. The chi-square test was used to compare categorical variables, and the analysis of variance (ANOVA) test was used to compare continuous variables between those with and without psychological distress. Multiple logistic regression analysis was used to determine the odds ratio (OR) and 95% confidence interval (CI) of psychological distress. We conducted two stages of analysis. In the first stage, the univariate analysis model, only the guideline-based PA levels were entered as a predictor. In the second stage, the multinomial analysis model, we entered potential confounders in the regression analysis and then tested if there was a significant change in the association. Age was treated as a continuous variable, and sex, specialty, cigarette smoking, alcohol drinking, betel nut chewing, and general and abdominal obesity were treated as categorical variables. The possibility of any suicide ideation (≥1) with and without BSRS-5 scores >5, ≥10, and ≥15 was, respectively, analyzed, and the possibility of moderate or more severe (≥2) suicide ideation with and without BSRS-5 scores >5, ≥10, and ≥15 was also analyzed. The software SPSS 26.0 (IBM Corp., Armonk, NY, United States) was used to establish a database and for subsequent statistical analysis. A two-sided p-value of less than 0.05 was considered to indicate statistical significance.
Results
In total, 4,080 individuals with complete data on leisure time PA levels, as well as mental health information, were included in this study for analysis. The demographics and characteristics of the study population are shown in Table 1. Their average age was approximately 29.2 years, and 89.9% of them were males. A higher prevalence of alcohol consumption and betel nut chewing was observed in those with any suicide ideation or BSRS ≥15. Furthermore, those without SI and BSRS <15 had higher PA levels.
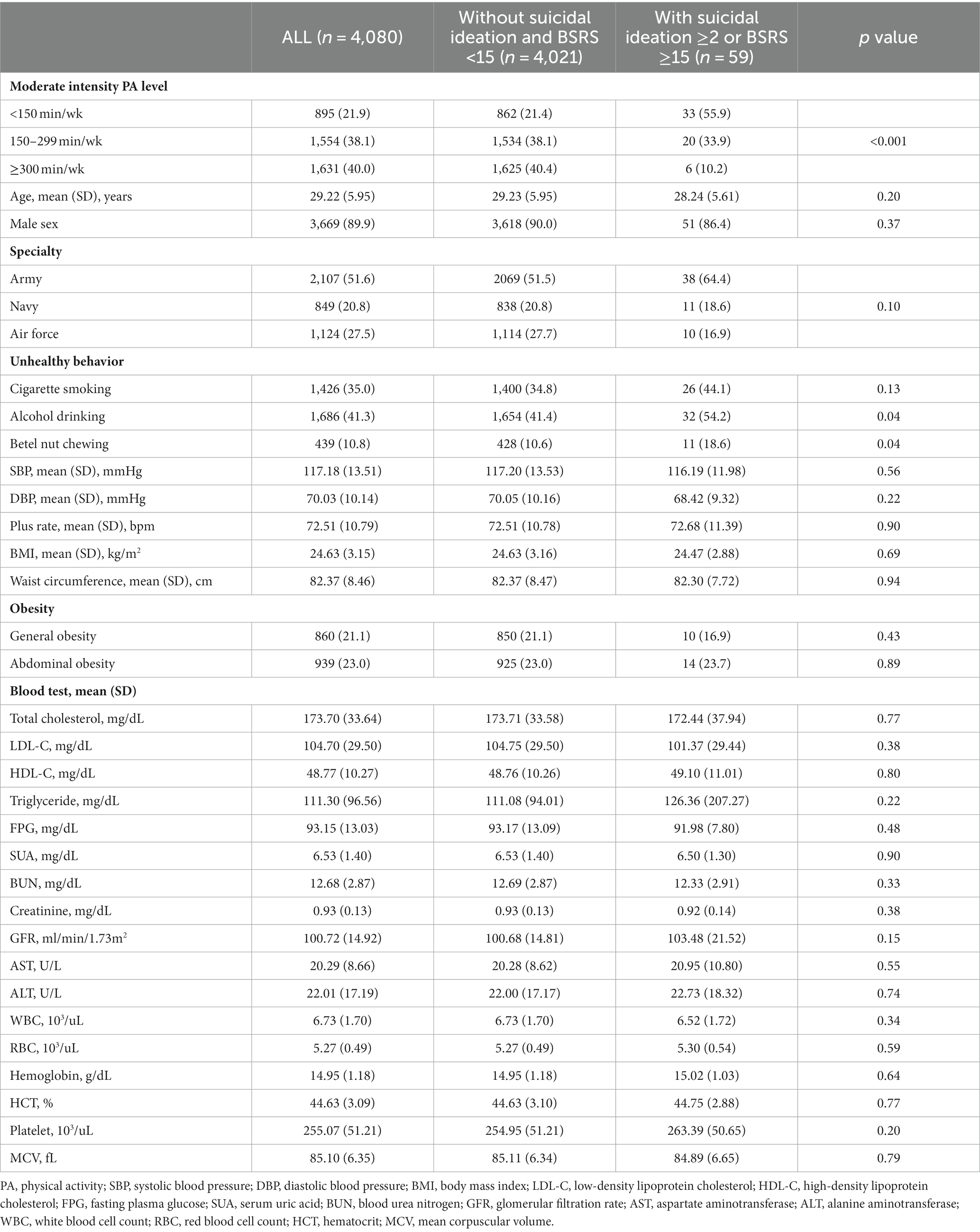
Table 1. Characteristics of the study participants.
The results of multiple logistic regression analysis for the association between guideline-based moderate-intensity PA levels and psychological distress items are shown in Table 2. As compared to those with a PA level of <150 min/wk., those with a PA level of 150–299 min/wk. had lower odds of suffering from moderate or more severe depression [OR and 95% CI: 0.67 (0.49–0.91)] and interpersonal sensitivity [OR: 0.67 (0.47–0.96)]. In addition, those with a PA level of ≥300 min/wk. had lower odds of suffering from moderate or more severe insomnia, anxiety, hostility, depression, and interpersonal sensitivity [ORs: 0.48 (0.36–0.65), 0.31 (0.21–0.45), 0.47 (0.34–0.65), 0.29 (0.20–0.43), and 0.43 (0.29–0.64), respectively]. With regard to the BSRS-5 score (Supplementary Table S1), there was a tendency for those with a PA level of ≥300 min/wk. to have lower odds of BSRS-5 ≥ 15 [OR: 0.21 (0.04–1.04)], BSRS-5 ≥ 10 [OR: 0.38 (0.21–0.69)], and BSRS-5 > 5 [OR: 0.41 (0.31–0.55)], as compared to those with a PA level of <150 min/wk.
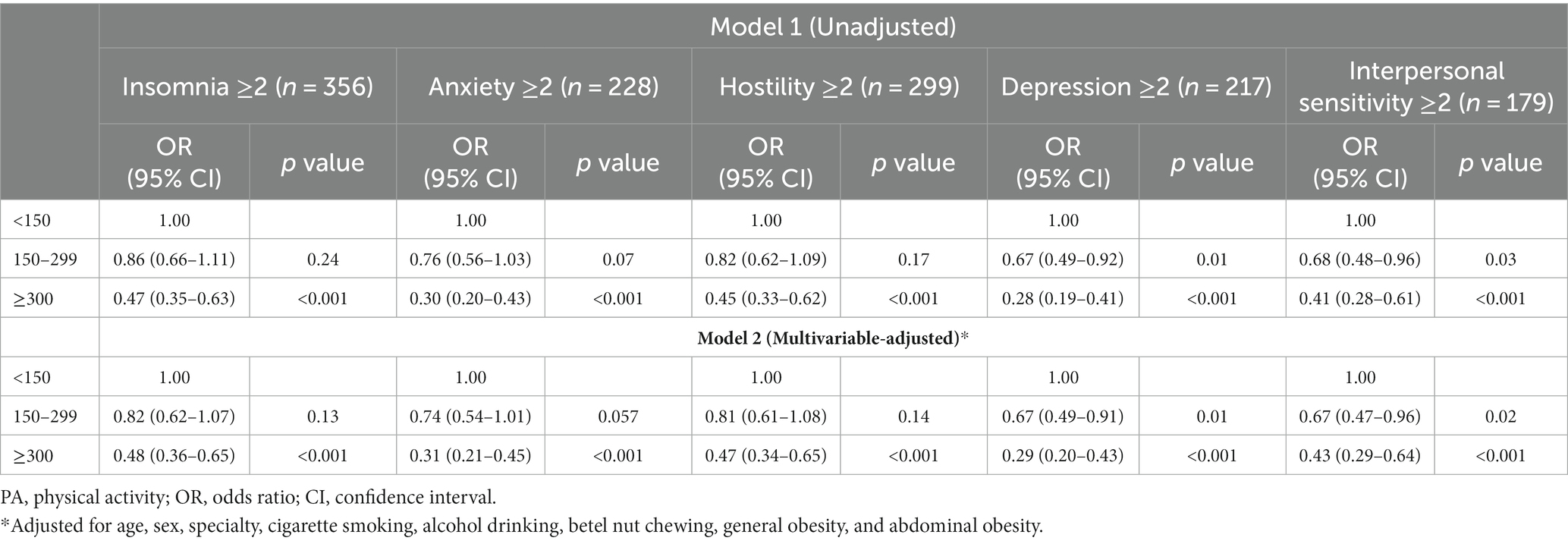
Table 2. Association of physical activity levels with various moderate to extremely severe psychological distress.
Table 3 reveals the results of multiple logistic regression analysis of American guideline-based moderate-intensity PA levels for SI and/or various grades of psychological distress. For SI ≥1, an inverse dose–response relationship was found between PA levels and SI with psychological distress. As compared to those with a PA level of <150 min/wk., those with a PA level of 150–299 min/wk. and a PA level of ≥300 min/wk. were observed to be less likely to have any SI [ORs: 0.58 (0.40–0.83) and 0.23 (0.14–0.36), respectively], any SI and/or BSRS-5 ≥ 15 [ORs: 0.55 (0.39–0.79) and 0.21 (0.13–0.34), respectively], any SI and/or BSRS-5 ≥ 10 [ORs: 0.63 (0.45–0.87) and 0.27 (0.18–0.41), respectively], and any SI and/or BSRS-5 > 5 [OR: 0.72 (0.57–0.91) and 0.37 (0.29–0.49), respectively]. For moderate or more severe SI (≥2), such an inverse dose–response relationship still existed and became more obvious. As compared to those with a PA level of <150 min/wk., those with a PA level of 150–299 min/wk. and a PA level of ≥300 min/wk. were observed to be less likely to have an SI ≥2 [OR: 0.37 (0.20–0.68) and 0.10 (0.04–0.26), respectively], an SI ≥2 and/or BSRS-5 ≥ 15 [OR: 0.35 (0.20–0.62) and 0.10 (0.04–0.25), respectively], an SI ≥2 and/or BSRS-5 ≥ 10 [OR: 0.52 (0.34–0.79) and 0.24 (0.14–0.40), respectively], and an SI ≥2 and/or BSRS-5 > 5 [OR: 0.69 (0.54–0.89) and 0.36 (0.27–0.48), respectively].
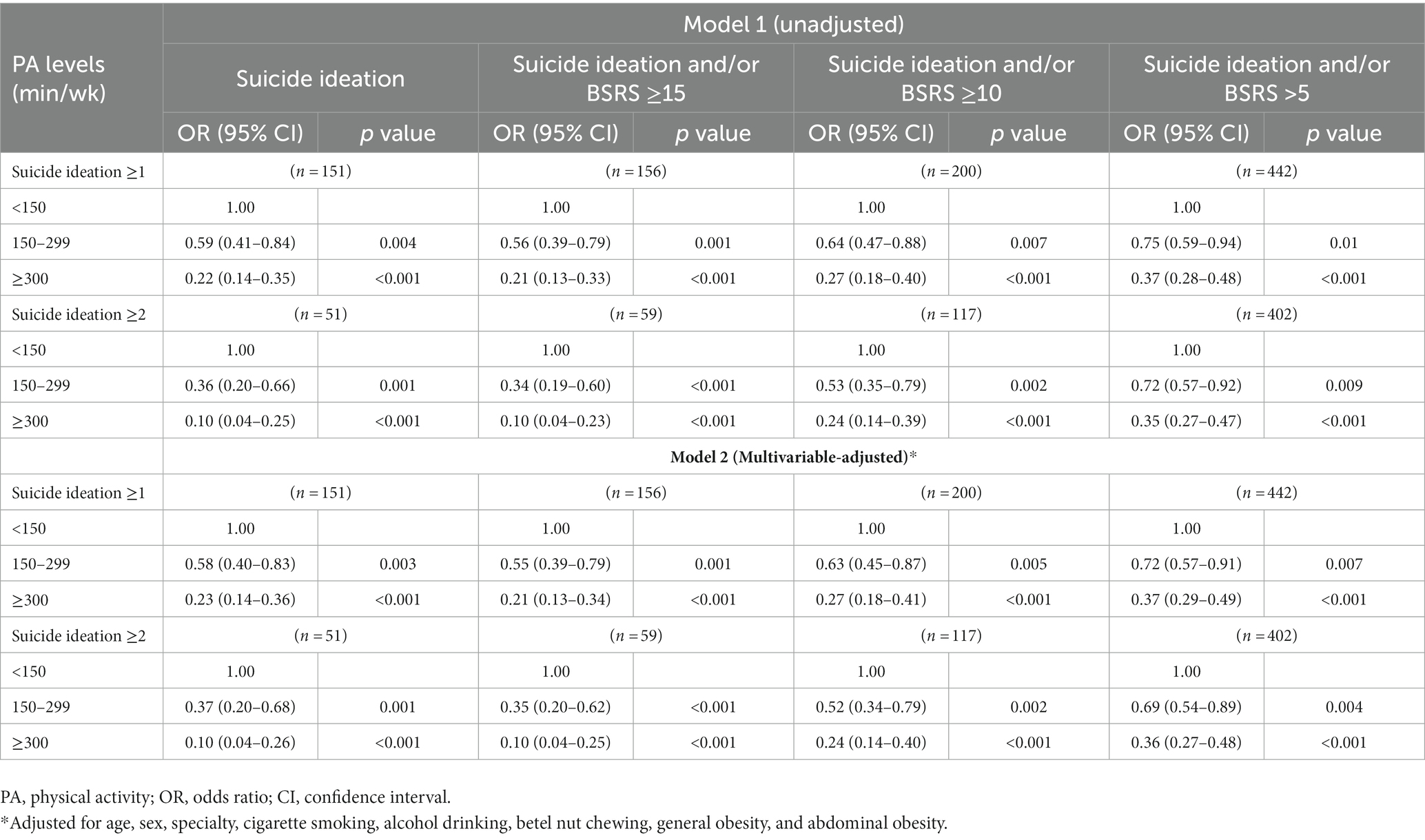
Table 3. Association of physical activity levels with suicidal ideation and different grades of psychological distress.
Discussion
Our findings suggested that military personnel engaging in a moderate intensity PA level of >150 min/wk. in leisure time might have lower psychological distress, particularly in depression and interpersonal sensitivity, and be protected from any SI. Moreover, adhering to the highest PA level that the guideline recommended, ≥300 min/wk., may provide additional benefits for mental health in the military.
The impacts of PA on mental health are incredibly extensive and beneficial for physical or mental illness regardless of age stratum. Higher intensity PA levels have been associated with greater improvements in psychological symptoms (1). In addition, aerobic PA is found to be an important protective factor against health-threatening reactions to acute psychosocial stress (27), which can enhance the consolidation and subsequent recall of fear extinction learning (28). Consistent with our findings, a prior study conducted in the Brazilian Army highlighted the dose–response association between greater leisure time PA levels and lower psychological distress, while occupational PA may have detrimental effects on mental health (29). Notably, this study was the first report that greater leisure time PA may prevent the development of SI, particularly moderate or more severe SI, for military subjects. This finding was also noted in the general population (30). Additionally, our findings in patients with cardiovascular diseases following cardiac rehabilitation exercise and improvements in CRF showed reductions in psychological distress, anxiety, hostility, and especially depression as well as psychological distress-associated increased mortality (10–15).
Regular exercise regulates the activity of the hypothalamic–pituitary–adrenal axis (31), and exerts anti-inflammation effects by increasing the release of peroxisome proliferator-activated receptor gamma coactivator 1 (PGC1)-α (32). Numerous clinical and translational studies have revealed an association between psychological distress and elevated pro-inflammatory cytokines (33–35). In addition, higher PA levels elevate serotonin and norepinephrine concentrations (36), and enhance the release of neurotrophin (31). These bioactive molecules can cross the blood–brain barrier (BBB), enhance brain-derived neurotrophic factor (BDNF) signaling, and positively contribute to mental health (37–40).
This study has several limitations. First, the cross-sectional design employed in this study could not establish a causal relationship between psychological distress and PA levels. Second, the focus on military subjects in this study restricts the generalizability of the findings to the general population. Third, the PA levels in this study were assessed by running time while the effect of strength exercises on mental stress was unclear. Finally, since psychological distress involves various factors that can affect outcomes, it was not feasible to account for all potential confounding factors in this study. However, this study had some strengths. First, the living environment and medical support in the military were similar, possibly reducing the unmeasured confounding effects. Second, this study focused on leisure-time PA instead of training-related PA, which was correlated to rank in the military, and those with lower rank were likely to have higher psychological distress.
Conclusion
Engaging in moderate-intensity PA during leisure time based on American guidelines was associated with better mental health in the military in this study. It is worth noting a dose–response phenomenon was observed in the association of greater moderate-intensity aerobic PA levels with better mental health, e.g., SI among military personnel. Further prospective longitudinal studies are needed to clarify the temporal association between PA levels and mental health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Institutional Ethics Committee approval (No. 16-05-008) from the Mennonite Christian Hospital in Taiwan was obtained at the beginning of the study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
K-ZT: Data curation, Formal analysis, Investigation, Resources, Software, Visualization, Writing – original draft. P-YL: Investigation, Supervision, Visualization, Writing – review & editing. Y-PL: Investigation, Supervision, Validation, Visualization, Writing – review & editing. C-CC: Investigation, Supervision, Writing – review & editing. W-CH: Investigation, Supervision, Writing – review & editing. XS: Investigation, Supervision, Validation, Writing – review & editing. CL: Investigation, Supervision, Writing – review & editing. G-ML: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by the Medical Affairs Bureau Ministry of National Defense (MND-MAB-D-113200).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1255516/full#supplementary-material
References
1. Singh, B, Olds, T, Curtis, R, Dumuid, D, Virgara, R, Watson, A, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. (2023) 57:1203–9. doi: 10.1136/bjsports-2022-106195
2. Lin, GM, Nagamine, M, Yang, SN, Tai, YM, Lin, C, and Sato, H. Machine learning based suicide ideation prediction for military personnel. IEEE J Biomed Health Inform. (2020) 24:1907–16. doi: 10.1109/JBHI.2020.2988393
3. Franklin, JC, Ribeiro, JD, Fox, KR, Bentley, KH, Kleiman, EM, Hung, X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
4. Schoenbaum, M, Kessler, RC, Gilman, SE, Colpe, LJ, Heeringa, SG, Stein, MB, et al. Predictors of suicide and accident death in the Army study to assess risk and resilience in servicemembers (Army STARRS): results from the Army study to assess risk and resilience in servicemembers (Army STARRS). JAMA Psychiatry. (2014) 71:493–503. doi: 10.1001/jamapsychiatry.2013.4417
5. Zuromski, KL, Dempsey, CL, Ng, THH, Riggs-Donovan, CA, Brent, DA, Heeringa, SG, et al. Utilization of and barriers to treatment among suicide decedents: results from the Army study to assess risk and resilience among servicemembers (Army STARRS). J Consult Clin Psychol. (2019) 87:671–83. doi: 10.1037/ccp0000400
8. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
9. Stubbs, B, Vancampfort, D, Hallgren, M, Firth, J, Veronese, N, Solmi, M, et al. EPA guidance on physical activity as a treatment for severe mental illness: a meta-review of the evidence and position statement from the European psychiatric association (EPA), supported by the International Organization of Physical Therapists in mental health (IOPTMH). Eur Psychiatry. (2018) 54:124–44. doi: 10.1016/j.eurpsy.2018.07.004
10. Lavie, CJ, Menezes, AR, De Schutter, A, Milani, RV, and Blumenthal, JA. Impact of cardiac rehabilitation and exercise training on psychological risk factors and subsequent prognosis in patients with cardiovascular disease. Can J Cardiol. (2016) 32:S365–73. doi: 10.1016/j.cjca.2016.07.508
11. Kachur, S, Menezes, AR, De Schutter, A, Milani, RV, and Lavie, CJ. Significance of comorbid psychological stress and depression on outcomes after cardiac rehabilitation. Am J Med. (2016) 129:1316–21. doi: 10.1016/j.amjmed.2016.07.006
12. Lavie, CJ, Sui, X, and Milani, RV. Emotional distress after myocardial infarction: importance of cardiorespiratory fitness. Eur J Prev Cardiol. (2018) 25:906–9. doi: 10.1177/2047487318770516
13. Hughes, JW, Serber, ER, and Kuhn, T. Psychosocial management in cardiac rehabilitation: current practices, recommendations, and opportunities. Prog Cardiovasc Dis. (2022) 73:76–83. doi: 10.1016/j.pcad.2021.12.006
14. Lavie, CJ, Zhang, I, Yang, D, and Liu, M. Improving fitness through exercise will improve our heart and mind. Heart Mind. (2023) 7:49–51. doi: 10.4103/hm.hm_59_22
15. O'Keefe, EL, O'Keefe, JH, and Lavie, CJ. The intersection of exercise, cognition, and cardiovascular disease. Heart Mind. (2023) 7:3–4. doi: 10.4103/hm.hm_5_23
16. Piercy, KL, Troiano, RP, Ballard, RM, Carlson, SA, Fulton, JE, Galuska, DA, et al. The physical activity guidelines for Americans. JAMA. (2018) 320:2020–8. doi: 10.1001/jama.2018.14854
17. Lin, GM, Li, YH, Lee, CJ, Shiang, JC, Lin, KH, Chen, KW, et al. Rationale and design of the cardiorespiratory fitness and hospitalization events in armed forces study in eastern Taiwan. World J Cardiol. (2016) 8:464–71. doi: 10.4330/wjc.v8.i8.464
18. Lin, KH, Su, FY, Yang, SN, Liu, MW, Kao, CC, Nagamine, M, et al. Body mass index and association of psychological stress with exercise performance in military members: the cardiorespiratory fitness and hospitalization events in armed forces (CHIEF) study. Endocr Metab Immune Disord Drug Targets. (2021) 21:2213–9. doi: 10.2174/1871530321666210427090550
19. Su, FY, Wang, SH, Lu, HH, and Lin, GM. Association of tobacco smoking with physical fitness of military males in Taiwan: the CHIEF study. Can Respir J. (2020) 2020:1–6. doi: 10.1155/2020/5968189
20. Hwang, LC, Bai, CH, and Chen, CJ. Prevalence of obesity and metabolic syndrome in Taiwan. J Formos Med Assoc. (2006) 105:626–35. doi: 10.1016/S0929-6646(09)60161-3
21. Lin, YK, Tsai, KZ, Han, CL, Lin, YP, Lee, JT, and Lin, GM. Obesity phenotypes and electrocardiographic characteristics in physically active males: CHIEF study. Front Cardiovasc Med. (2021) 8:738575. doi: 10.3389/fcvm.2021.738575
22. Wang, SH, Chung, PS, Lin, YP, Tsai, KZ, Lin, SC, Fan, CH, et al. Metabolically healthy obesity and physical fitness in military males in the CHIEF study. Sci Rep. (2021) 11:9088. doi: 10.1038/s41598-021-88728-0
23. Chung, PS, Tsai, KZ, Lin, YP, Lin, YK, and Lin, GM. Association between leukocyte counts and physical fitness in male military members: the CHIEF study. Sci Rep. (2020) 10:6082. doi: 10.1038/s41598-020-63147-9
24. Lee, MB, Liao, SC, Lee, YJ, Wu, CH, Tseng, MC, Gau, SF, et al. Development and verification of validity and reliability of a short screening instrument to identify psychiatric morbidity. J Formos Med Assoc. (2003) 102:687–94.
25. Lin, YP, Fan, CH, Tsai, KZ, Lin, KH, Han, CL, and Lin, GM. Psychological stress and long-term blood pressure variability of military young males: the cardiorespiratory fitness and hospitalization events in armed forces study. World J Cardiol. (2020) 12:626–33. doi: 10.4330/wjc.v12.i12.626
26. Lin, KH, Chen, YJ, Yang, SN, Liu, MW, Kao, CC, Nagamine, M, et al. Association of psychological stress with physical fitness in a military cohort: the CHIEF study. Mil Med. (2020) 185:e1240–6. doi: 10.1093/milmed/usz469
27. Wyss, T, Boesch, M, Roos, L, Tschopp, C, Frei, KM, Annen, H, et al. Aerobic fitness level affects cardiovascular and salivary alpha amylase responses to acute psychosocial stress. Sports Med Open. (2016) 2:33. doi: 10.1186/s40798-016-0057-9
28. Crombie, KM, Adams, TG, Dunsmoor, JE, Greenwood, BN, Smits, JA, Nemeroff, CB, et al. Aerobic exercise in the treatment of PTSD: an examination of preclinical and clinical laboratory findings, potential mechanisms, clinical implications, and future directions. J Anxiety Disord. (2023) 94:102680. doi: 10.1016/j.janxdis.2023.102680
29. Martins, LC, and Lopes, CS. Rank, job stress, psychological distress and physical activity among military personnel. BMC Public Health. (2013) 13:716. doi: 10.1186/1471-2458-13-716
30. Kim, K, Shin, YJ, Nam, JH, Choi, BY, and Kim, MK. A dose-response relationship between types of physical activity and distress. J Korean Med Sci. (2008) 23:218–25. doi: 10.3346/jkms.2008.23.2.218
31. Lopresti, AL, Hood, SD, and Drummond, PD. A review of lifestyle factors that contribute to important pathways associated with major depression: diet, sleep and exercise. J Affect Disord. (2013) 148:12–27. doi: 10.1016/j.jad.2013.01.014
32. Handschin, C, and Spiegelman, BM. The role of exercise and PGC1alpha in inflammation and chronic disease. Nature. (2008) 454:463–9. doi: 10.1038/nature07206
33. Raison, CL, Capuron, L, and Miller, AH. Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol. (2006) 27:24–31. doi: 10.1016/j.it.2005.11.006
34. Weber, MD, Godbout, JP, and Sheridan, JF. Repeated social defeat, neuroinflammation, and behavior: monocytes carry the signal. Neuropsychopharmacology. (2017) 42:46–61. doi: 10.1038/npp.2016.102
35. Nobis, A, Zalewski, D, and Waszkiewicz, N. Peripheral markers of depression. J Clin Med. (2020) 9:3793. doi: 10.3390/jcm9123793
36. Ross, RE, VanDerwerker, CJ, Saladin, ME, and Gregory, CM. The role of exercise in the treatment of depression: biological underpinnings and clinical outcomes. Mol Psychiatry. (2023) 28:298–328. doi: 10.1038/s41380-022-01819-w
37. Khoury, R, and Nagy, C. Running from stress: a perspective on the potential benefits of exercise-induced small extracellular vesicles for individuals with major depressive disorder. Front Mol Biosci. (2023) 10:1154872. doi: 10.3389/fmolb.2023.1154872
38. Sleiman, SF, Henry, J, Al-Haddad, R, Hayek, LE, Haidar, EA, Stringer, T, et al. Exercise promotes the expression of brain derived neurotrophic factor (BDNF) through the action of the ketone body beta-hydroxybutyrate. elife. (2016) 5:e15092. doi: 10.7554/eLife.15092
39. Karnib, N, El-Ghandour, R, El Hayek, L, Nasrallah, P, Khalifeh, M, Barmo, N, et al. Lactate is an antidepressant that mediates resilience to stress by modulating the hippocampal levels and activity of histone deacetylases. Neuropsychopharmacology. (2019) 44:1152–62. doi: 10.1038/s41386-019-0313-z
Keywords: mental health, psychological distress, suicide ideation, leisure time physical activity, military personnel
Citation: Tsai K-Z, Liu P-Y, Lin Y-P, Chu C-C, Huang W-C, Sui X, Lavie CJ and Lin G-M (2023) Do the American guideline-based leisure time physical activity levels for civilians benefit the mental health of military personnel? Front. Psychiatry. 14:1255516. doi: 10.3389/fpsyt.2023.1255516
Edited by:
Meenakshi Shukla, Allahabad University, IndiaReviewed by:
Mehmet Hamdi Örüm, Elazığ Eğitim ve Araştırma Hastanesi, TürkiyeRajendra Prasad Gupta, Tilak Dhari Post Graduate College, India
Copyright © 2023 Tsai, Liu, Lin, Chu, Huang, Sui, Lavie and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gen-Min Lin, ZmFybWVyNTA3QHlhaG9vLmNvbS50dw==
†ORCID: Kun-Zhe Tsai, https://orcid.org/0000-0002-7126-1545
Gen-Min Lin, https://orcid.org/0000-0002-5509-1056