 Kerstin Paschke1*
Kerstin Paschke1* Silke Diestelkamp1
Silke Diestelkamp1 Antonia Zapf2
Antonia Zapf2 Katharina Busch1
Katharina Busch1 Nicolas Arnaud1
Nicolas Arnaud1 Alexander Prehn-Kristensen3
Alexander Prehn-Kristensen3 Olaf Reis4Maria Stark2Jan-Ole Cloes1Anna-Lena Schulz1
Olaf Reis4Maria Stark2Jan-Ole Cloes1Anna-Lena Schulz1 Hannah Brauer3Thomas Krömer5Rainer Thomasius1
Hannah Brauer3Thomas Krömer5Rainer Thomasius1  the Res@t Consortium
the Res@t Consortium- 1German Center for Addiction Research in Childhood and Adolescence (DZSKJ), University Medical Center Hamburg-Eppendorf (UKE), Hamburg, Germany
- 2Institute of Medical Biometry and Epidemiology (IMBE), University Medical Center Hamburg-Eppendorf (UKE), Hamburg, Germany
- 3Institute of Child and Adolescent Psychiatry, Center for Integrative Psychiatry, School of Medicine, Christian-Albrecht University Kiel, Kiel, Germany
- 4Department for Child and Adolescent Psychiatry and Neurology, Rostock University Medical Center, Rostock, Germany
- 5Collaborative Practice for Child and Adolescent Psychiatry, Psychotherapy and Psychosomatics, Hamburg, Germany
Background: Digital media-use disorders (DMUD) in adolescents are a rising phenomenon associated with psychological distress, comorbid mental disorders, and high burden on affected families. Since the ICD-11 introduced criteria for gaming disorder, these can now be transferred to describe additional DMUD associated with social media platforms and streaming services. Most evidence for effective treatments comes from cognitive-behavioral therapy (CBT). However, interventions based on theoretical models for adolescents and their parents are widely missing, leading to a significant clinical gap.
Methods: Res@t digital (Resource-Strengthening Training for Adolescents with Problematic Digital-Media Use and their Parents) is the app-based translation of the first model-based digital intervention for adolescents with DMUD and their parents based on CBT. It comprises separate but content-related modules for adolescents (Res@t–A) and parents (Res@t–P), applying multimodal techniques. The effectiveness of Res@t will be evaluated within a multicenter cluster-randomized controlled evaluator-blinded pre–post follow-up trial with the waitlist control group (CG). In addition to the Res@t program in the intervention group, both groups will receive treatment as usual within primary child and adolescent psychiatric/psychotherapeutic healthcare. The primary outcome addresses DMUD symptom reduction after 10 weeks. Secondary outcomes are related to a reduction in psychological and family-related problems and an increase in parental self-efficacy. All outcomes will be assessed using standardized self-report measures. A total of 1,334 participating adolescent–parent dyads from a large clinical network throughout Germany are planned to be included in the primary analyses based on an intention-to-treat approach, applying linear mixed models.
Discussion: Assuming superiority of Res@t over the control condition, the intervention has the potential to provide evidence-based treatment for a significant number of help-seeking families, supporting local healthcare structures and resources. It is a promising program for practicable implementation and flexible use in different settings.
Clinical trial registration: https://drks.de, DRKS00031043.
1 Introduction
The digital entertainment and media market industries belong to the fastest-growing businesses in the world (1). In 2022, revenue from digital games amounted to 184 billion U.S. dollars with mobile games accounting for 50% of the global gaming market (2). During the last decades, improved design mechanisms and broad availability led to increased usage frequency and duration worldwide over all age groups (3). During the COVID-19 pandemic, this development was fostered by contact restrictions, quarantines, and the closure of schools and leisure facilities, especially for children and adolescents (4–6). The majority of German children and adolescents use digital media on a regular basis from several times a week to daily, including social media (SM, more than 90%), video streaming (VS) services (more than 80%), and digital games (more than 70%) (7).
For some users, frequent digital media use as a leisure activity can turn into problematic patterns, resulting in severe negative personal, family, social, educational, and work-related sequelae with significant subsequent costs to healthcare and economic systems (8). Recent meta-analyses estimated the worldwide prevalence of problematic gaming between 3.1 and 3.3% (9, 10) and problematic SM use at 5% (11) with a peak during adolescence. Much less research has been conducted on problematic VS, although similar addiction-promoting mechanisms are applied to increase user bonding (12). Most associated research has focused on binge-watching, i.e., the consumption of several (television) series episodes in a row (13, 14). However, the series resembles only a small subentity of VS services. A representative study on German adolescents estimated the prevalence of pathologic VS at 4.7% in frequent (at least weekly) VS users (15).
Adolescents are particularly at risk for behavioral addictions including problematic gaming due to neuronal remodeling processes with a mature reward system, on the one hand, and a cognitive-control system that is still in development on the other hand (16, 17).
As the first behavioral addiction purely associated with digital media, problematic (online or offline) gaming has been included in the current (11th) version of the International Classification of Diseases (ICD-11) as Gaming Disorder (GD, 6C51) (18). Four criteria have been defined for diagnosing GD which must usually be present for the past 12 months: loss of control over the temporal and situational use of digital games, increased prioritization of digital gaming over alternative activities, continued or increased gaming despite negative consequences, and the occurrence of significant impairments in important areas of functioning. At the current state, other digital-media-related disorders (DMUD), such as Social Media Use Disorder (SMUD) or Video Streaming Disorder (VSD), can be classified under the umbrella Other specific disorders due to addictive behaviors (GC5Y), applying comparable criteria as for GD (19). Affected individuals who do not (yet) fulfill all criteria of addiction can be classified under Hazardous Gaming (HG, QE22) or problems with other specified health-related behaviors (QE2Y). The latter can include Hazardous Social Media Use (HSMU) and Hazardous Video Streaming (HVS). Disordered or hazardous usage patterns can be summarized as Problematic Gaming (PG), Problematic Social Media Use, or Problematic Video Streaming (PVS).
The etiology of DMUD can, e.g., be described by the Triad Model of Addiction by Kielholz & Ladewig (20). This biopsychosocial model describes an interaction of personal, social, and agent-related factors. It employs mechanisms of learning, stress management (21), and information processing and can be comprehensively applied to DRMD in adolescents. For more details, please refer to the study by Paschke et al. (22).
If DMUD remains untreated, there will be a high risk of chronicity with severe psychological consequences, repeated hospitalizations, and failure to fulfill necessary developmental tasks (e.g., no school qualifications, no education) with negative effects on the mental and physical health of the affected person and high costs for society. The best effects on symptom reduction have been shown for cognitive-behavioral therapy (CBT) (23). However, model-based and evidence-based treatment programs, addressing adolescents and their parents, are currently not available (24–26).
1.1 Aim of the study and hypotheses
The present study aims to evaluate the effectiveness of a new model-based standardized online intervention program, the Resource-Strengthening Training for Adolescents with Problematic Digital-Media Use, and their Parents (Res@t digital) in an outpatient setting. The Res@t digital intervention group (IG) will be compared with a waiting control group (CG). The IG will receive the Res@t digital intervention, and both groups will receive treatment as usual (TAU) during the study period. The waitlist CG will be offered access to the intervention after individual data collections are completed. It is hypothesized that Res@t digital + TAU is superior to TAU only and will lead to a decrease in adolescent DMUD (i.e., GD, SMUD, or VSD) symptoms. In the case of an adolescent being affected by more than one DMUD or hazardous use pattern, the clinician will identify the most prominent phenomenon that will be focused on within the targeted intervention. Moreover, Res@t digital will reduce mental-health-related problems in adolescents and increase parental self-efficacy.
There are three primary hypotheses structured hierarchically which address the one most prominent DMUD or hazardous use pattern in the individual adolescent identified by the clinician (i.e., PG, PSMU, or PVS). This is referred to the term “specific” DMUD:
First primary hypothesis: Res@t + TAU reduces symptoms of specific DMUD in adolescents compared with TAU, measured as change from screening to post-intervention. Second primary hypothesis: Res@t + TAU reduces symptoms of specific DMUD in adolescents assessed by their parents compared with TAU, measured as change from screening to post-intervention. Third primary hypothesis: Res@t + TAU reduces symptoms of specific DMUD in adolescents assessed by their treating clinicians compared with TAU, measured as change from screening to post-intervention.
To the best of our knowledge, although positive effects of online interventions have been repeatedly suggested to fill substantial treatment gaps for mental health issues in adults (27–29) and adolescents (30–32) including addictive behavior (33–35), no comparable intervention for adolescents with DMUD and their parents is available yet. Therefore, Res@t strives to close a significant void.
2 Methods and analysis
2.1 Study design
The current study is a multicenter, prospective, cluster randomized-controlled, observer-blind clinical trial on the effectiveness of Res@t regarding symptom reduction in adolescents with DMUD. A two-arm study design will be applied with an IG and a waitlist CG with pre–post follow-up assessments. All patients will receive surveillance by a child and adolescent psychiatrist and psychotherapist who offers TAU in regular treatment parallel to the study.
2.2 Study sample and setting
Adolescents aged 10 to 19 years (based on the WHO definition of adolescence) and their respective parents, i.e., caregivers, will be recruited for the study by their child and adolescent psychiatrists and/or psychotherapists. Recruitment sites will include 10 outpatient departments of participating clinics (five university hospitals, five large care clinics) and approximately 40 practices throughout Germany (coordinated via the Professional Association for Child and Adolescent Psychiatry, Psychosomatics, and Psychotherapy in Germany e.V., BKJPP).
All eligible recruitment sites will be assigned randomly to IG or CG. Sites randomized to CG will have the opportunity to use Res@t after study recruitment and follow-up are completed.
In addition to introducing the study in regular appointments, advertisements will be carried out via five health insurance companies and the German Society for Child and Adolescent Psychiatry, Psychosomatics, and Psychotherapy (DGKJP) who support the study. Adolescents and parents who are interested in the study will be referred to participating clinics and practices, an appointment for screening and diagnosis will be made, and they will be informed about study details.
Screening for DMUD will take place for all patients within regular child and adolescent psychiatric diagnostics. If a DMUD is confirmed during clinical examination, adolescents and parents will be informed verbally and in writing about the study purpose and procedure including intervention, assessments, and recruitment-site-associated randomized group allocation. Further information concerns confidentiality and data protection procedures including pseudonymization, anonymous data storage at the study center (German Center for Addiction Research in Childhood and Adolescence, DZSKJ, University Clinic Hamburg-Eppendorf, UKE) for 10 years after study completion, possible advantages and disadvantages of participation, and the option to withdraw from the study at any time and without any given reason. Before study enrolment, adolescents and parents give their informed consent and receive all necessary documents on the study.
Since all participants are patients in regular treatment, they will not be financially compensated. However, patients will be offered a voucher for a large selection of online shops as incentive for full questionnaire completion with graded values according to assessment points.
Patient recruitment (first patient in to last patient out) is planned from January 2024 to May 2025. This includes a recruitment period of 12 months and a treatment and follow-up period of 17 months in total.
2.3 Eligibility criteria
Recruitment sites have been selected based on the following criteria:
• They are either approved outpatient departments of clinics for child and adolescent psychiatry and psychotherapy,
• Medical care centers for child and adolescent psychiatry and psychotherapy, or
• Practices for child and adolescent psychiatry and/or psychotherapy listed with the local Association of Statutory Health Insurance Physicians or Chamber of Psychotherapists.
• Local healthcare providing professionals need to be experienced with child and adolescent psychiatry and/or psychotherapy. They will comprise specialists for child and adolescent psychiatry, registrars in training as child and adolescent psychiatrists, psychologists, certified psychotherapists for children and adolescents, or psychotherapists for children and adolescents in training.
• All sites will be supervised by a certified experienced child and adolescent psychiatrist and/or psychotherapists.
• The sites are located in Germany.
Participants will be included in the study if they:
• Are between 10 and 19 years old (WHO definition of adolescence);
• Reach the cutoff values for hazardous or pathological use on the Gaming Disorder, Social Media Use Disorder or Streaming Disorder Scale for Adolescents or Parents (GADIS-A/-P, SOMEDIS-A/-P, STREDIS-A/P);
• Fulfill the ICD-11 criteria of disordered or hazardous gaming, social media use, or streaming based on clinical examination;
• Have sufficient German language skills;
• Give written informed consent (for adolescents <16 years with additional informed consent of legal guardians).
OR
• Are a parent, i.e., caregiver, of a patient fulfilling the criteria above.
Participants will be excluded from the study if they:
• Show symptoms of an acute psychosis;
• Are acute suicidal;
• Are substance intoxicated or fulfill criteria of substance use disorder (alcohol, illegal substances, and non-prescribed medication);
• Show a severe reduction in literacy and/or intelligence;
• Have no access to the Internet or are not able to operate on a smartphone, tablet, or computer.
2.4 Sample size calculation
The sample size was computed with the procedure tests for Two Means in a Cluster-Randomized Design in PASS 16.0.4 (NCSS, LLC. Kaysville, Utah, United States). A small standardized mean difference (Cohen’s d = 0.2) between IG and CG in symptom reduction measured as change from baseline to post-intervention is assumed. The number of study centers is assumed to be 50, each recruiting 27 patients on average. This leads to a feasible sample size of 667 per group. The coefficient of variation of the cluster sizes is set to 0.4 because recruitment is assumed to be heterogeneous due to the different sizes of the study sites. The intra-cluster correlation (ICC) is set to 0.005. With the achievable sample size of 667 patients with respective parents in each of the two groups (Ndyads = 667) and a two-sided type I error of 5%, the power will be 77%. A dropout rate of 40% before post-intervention assessment (10 weeks) and 20% before follow-up (20 weeks) is assumed. The sample size calculation refers to the three primary hypotheses, taking into account the hierarchical structure. A drop-out rate of 40% before post-intervention assessment (week 10) is considered. With an estimated proportion of adolescents in the outpatient setting with hazardous or disordered digital media use of 20% and a participation rate of 50%, N = 13,340 patients must be initially screened. Due to the novelty of the study, conservative estimates were chosen for the assumed effect size and drop-out and participation rates. Digital CBT-based intervention studies with comparable adolescent age groups reported small to medium effect sizes regarding the reduction in depression and anxiety symptoms (36, 37).
Three nuisance parameters (drop-out rate, coefficient of variation, and intraclass correlation coefficient) enter the sample size planning, the assumptions of which are not known with certainty. Therefore, a blinded interim analysis will be performed after the collection of post-intervention data from half of the planned patients (200 per group, 400 total) to estimate the nuisance parameters and possibly adjust the sample size.
2.5 Randomization
A stratified cluster randomization will be employed, resulting in each recruitment site (outpatient department or practice) being randomly allocated to the intervention or waitlist control. Stratification is performed according to recruitment site size (annual patient number ≤ 600, > 600 and ≤ 1,600, and > 1,600) and location (urban or rural). An independent statistician at the Institute of Medical Biometry and Epidemiology (IMBE) at the University Medicine Hamburg-Eppendorf will randomly allocate recruitment sites using computerized random number generations within each stratum to IG or CG based on internal standard operating procedures, without knowledge of the identity of recruitment sites (with variable block length). Cluster randomization will be applied to avoid contamination between IG and CG conditions regarding TAU. Based on the resulting allocation, the intervention will be made available immediately (IG) or after the recruitment phase and follow-up data collection is completed (CG).
2.6 Assessment and data collection
Clinical assessments with the adolescents and respective parents will be realized at screening, baseline, week 10 (post-intervention), and week 20 (follow-up). By the latter, the durability of the treatment effect should be estimated. Screening and baseline visits should not be apart by more than 4 weeks, otherwise a clinical reevaluation will become necessary. In addition to clinical diagnosis and post-treatment evaluation, all assessments are performed digitally via standardized questionnaires, which are provided on an online platform without the involvement of the clinician. They will be automatically presented to the participants at the time points according to the study protocol. Participants will receive e-mail reminders just before and during the scheduled time frame. All data will be initially stored in a patient dossier on the ISO-certified e-mental health platform run by Embloom1 before pseudonymization and secure transfer to the central study center. Regular visits with the clinician will take place within TAU. These should support compliance and adherence to keep the drop-out rate as low as possible. Figure 1 shows all study phases including assessment time points. Table 1 shows all questionnaires and items used in the current study. Table 2 shows the schedule of the questionnaire application.
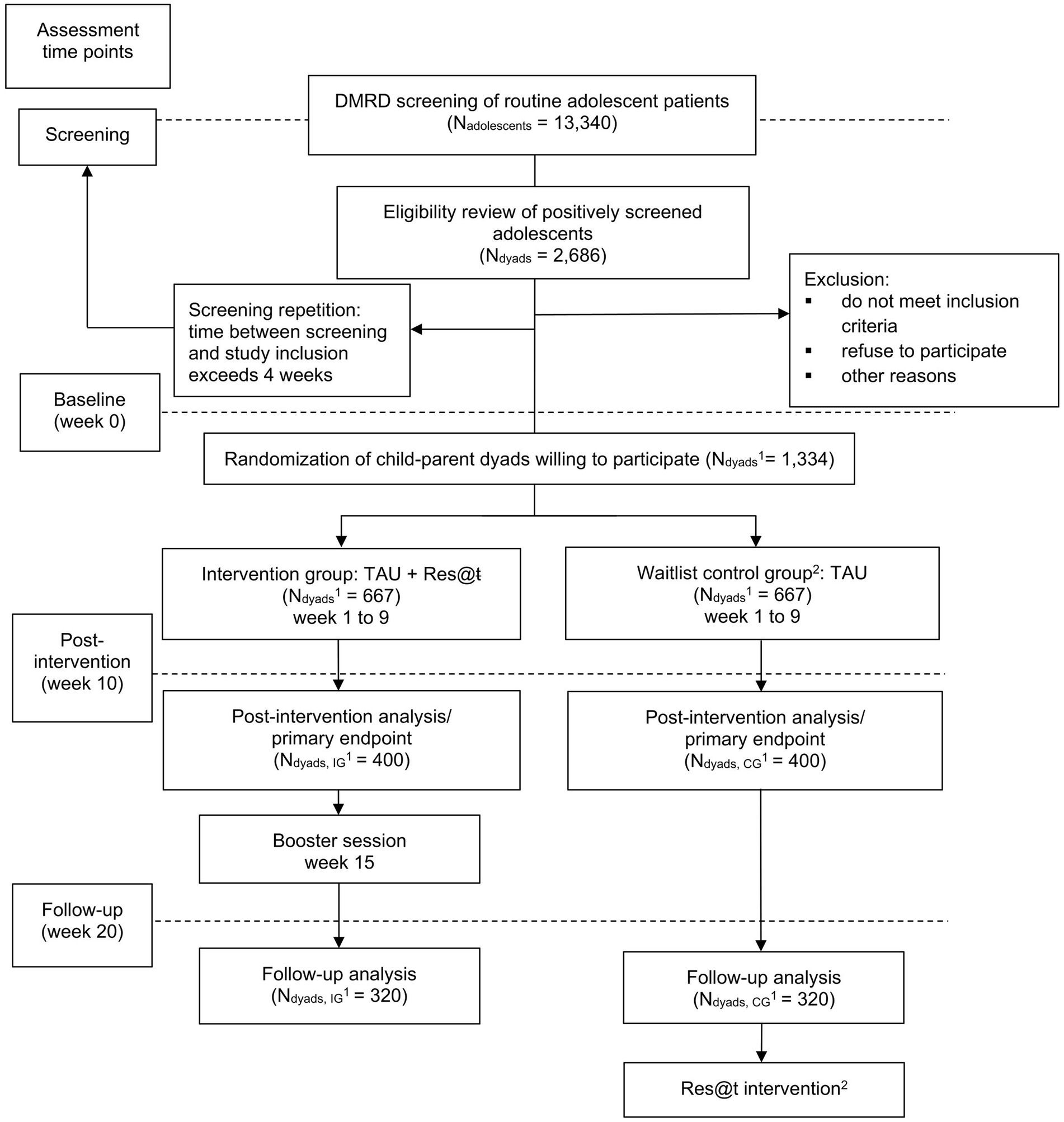
Figure 1. Flow chart of the study. 1Total number of adolescent–parent dyads; 2Participants of the waitlist control group will be offered the Res@t intervention after data collection is completed. DMUD, digital-media use disorders; TAU, treatment as usual; IG, intervention group; CG, control group.
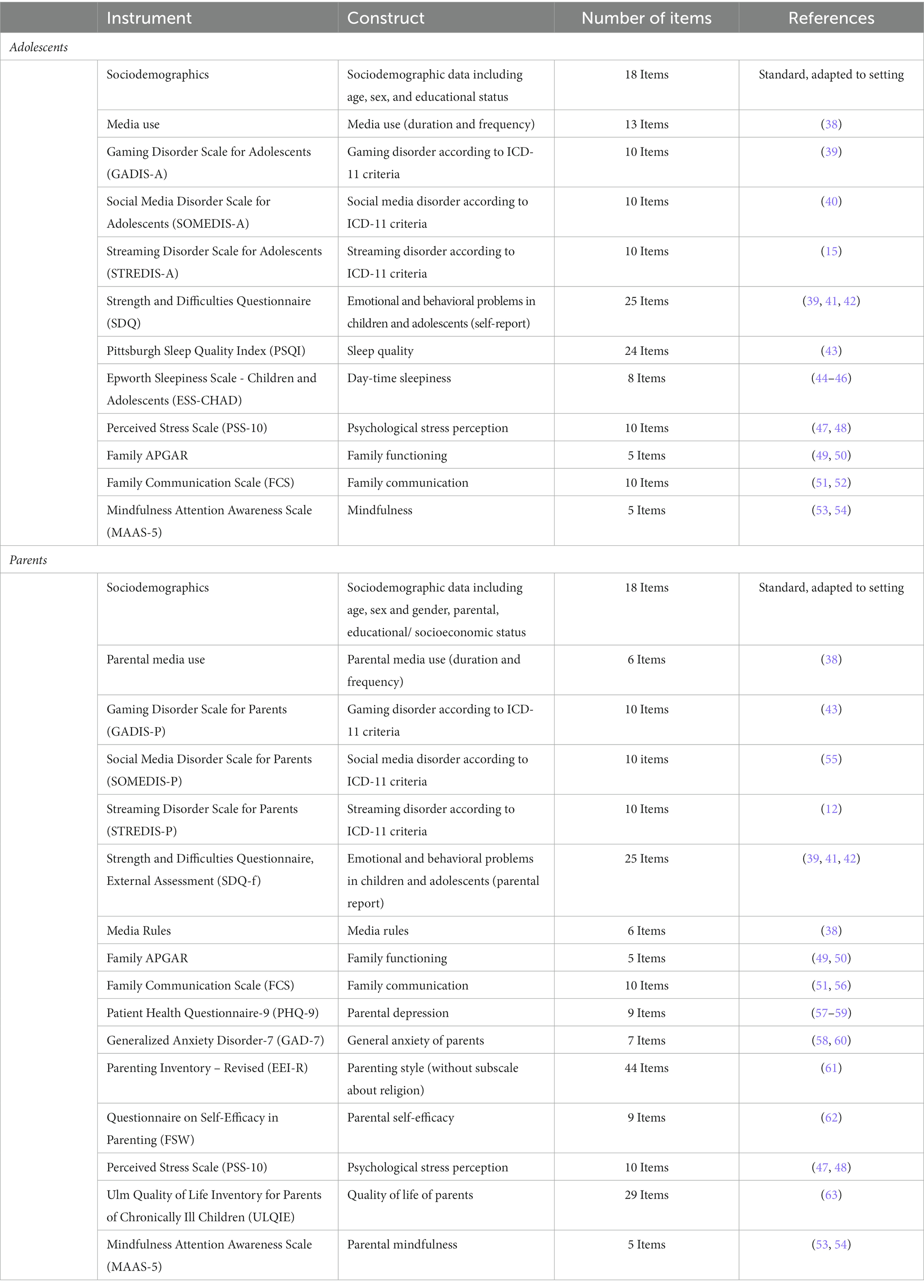
Table 1. Overview of study questionnaires for adolescents and their parents.
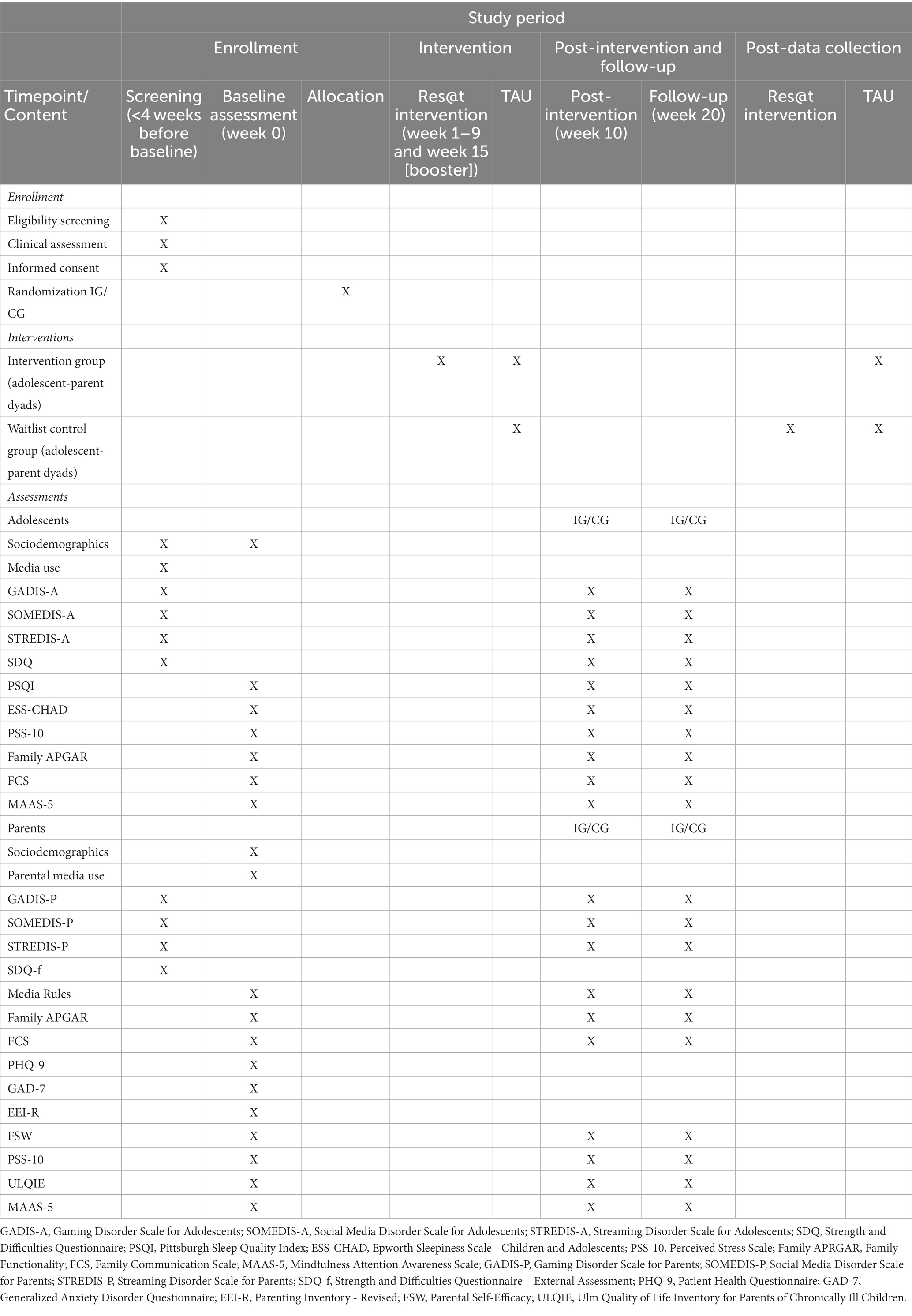
Table 2. Diagram of trial activities and measurement time points.
2.7 Blinding
Practitioners will be informed whether their recruitment site has been assigned to IG or CG at the beginning of the study. Once a patient has been identified to be eligible for study participation and the family gave informed consent to participate, the practitioner will individually inform about the assignment to IG or CG. Evaluating data analysists at IMBE will be blinded and will receive blinded datasets only.
2.8 Compliance
Compliance and adherence will be fostered by the treating clinician who observes the participants regularly within the context of normal treatment. Moreover, automatic reminders will be presented via the online app to the participating adolescents and parents. To all participants in the CG, the Res@t intervention will be offered after the completion of study recruitment. Incentives are planned for participants and clinicians to compensate for additional effort. These measures should increase study motivation and reduce drop-out rates.
2.9 Res@t digital intervention
Res@t digital is the app-based translation of a manualized CBT-based treatment package comprising offline programs for adolescents with GD (Res@t–A offline) and their parents (Res@t–P offline (64)). A detailed description of the original program package and its further development can be found in a recent publication by Paschke et al. (22). For better readability, a short summary is given by:
Res@t was created within the theoretical framework of the Trias model of addiction (20) based on clinical experiences and up-to-date research findings on the etiology of DMUD and potentially effective treatment components. During the developmental process, qualitative interviews and focus groups had been conducted with clinical experts, affected adolescents, and their parents on needs and program requirements (26, 64). The findings were considered for the final Res@t version. Original content was adapted to fit digital demands, and specific elements for the treatment of SMUD and VSD have been added. Res@t digital is comprised of nine weekly sessions and one booster session in week 15 of approximately 20 min processing time each. Additionally, participants are encouraged to complete a daily calendar on usage times, non-digital activities, mood, and sleep.
Table 3 gives an overview of the Res@t session contents as offered to adolescents and parents. Modules with adaption to address the type of DMUD are indicated.
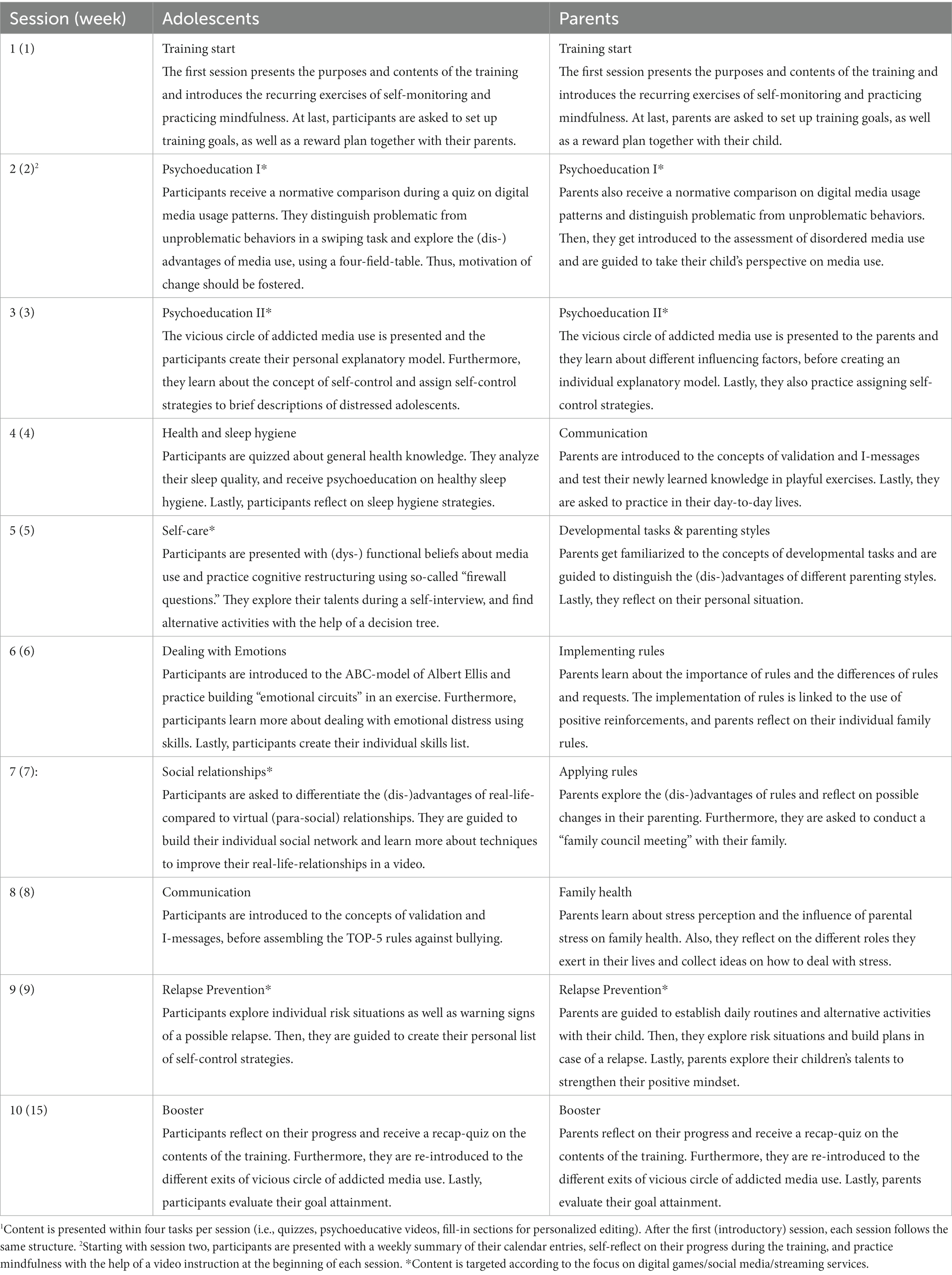
Table 3. Intervention modules1 in Res@t app training for adolescents and their parents.
The digital application in the adolescent and the parental versions will be made available via app stores. It is hosted in the secure Embloom platform environment. Based on the study arm allocation, the app, i.e., the intervention content, will be made available directly (for IG) or after individual data collection is completed (for CG). Figure 2 shows examples of the Res@t digital interface (in German language).
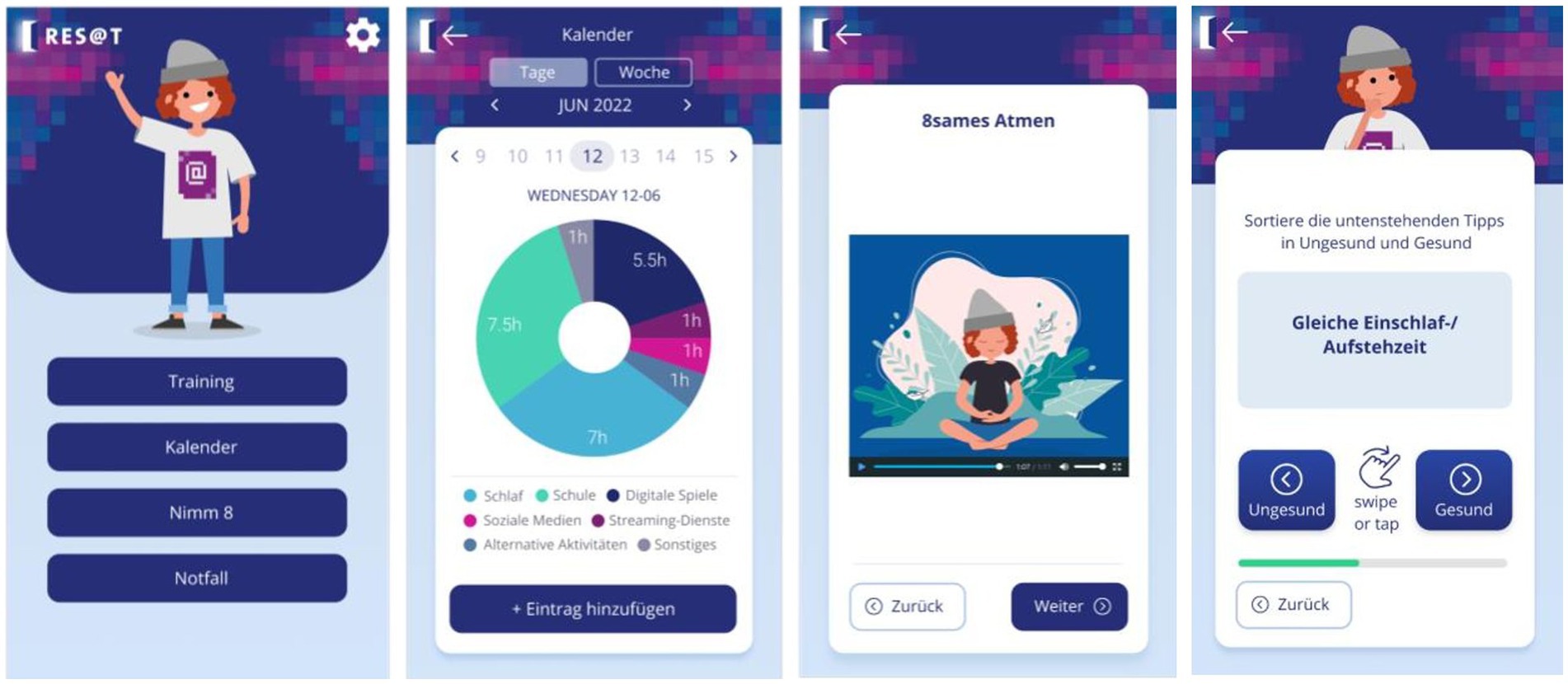
Figure 2. Res@t digital dashboard. The dashboard of the German Res@t application includes an overview of weekly sessions and their completion. It organizes access to the diary, individual sessions, mindfulness exercises, and an emergency button with skills for acute stress reduction and contact numbers of the treating child and adolescent psychiatrist and psychotherapist as well as local emergency departments (left frame). The middle-left frame represents the graphical feedback of diary entries on the duration of digital media use, sleep, and other activities. A mindfulness exercise is shown in the middle right frame. The right frame depicts an example of a swiping task within a quest.
2.10 Outcome measures
2.10.1 Primary outcome
The primary outcome is the reduction of specific DMUD (GD, PSMU, or VSD) symptoms assessed by the DMUD test battery for adolescents and parents based on differential scores in pre–post comparison.
It includes the Gaming Disorder Scale for Adolescents/Parents (GADIS-A/-P), the Social Media Disorder Scale for Adolescents/Parents (SOMEDIS-A/-P), and the Streaming Disorder Scale for Adolescents/Parents (STREDIS-A/-P). All 10-item scales are identical except for the initial explanation and continuous naming of the specific digital medium of interest (digital games, social media platforms, and video-streaming services) and address either the potentially affected adolescent (self-rating version) or the respective parent (external-rating version). The whole test battery is based on the ICD-11 criteria of GD and has been adapted for SMUD and VSD accordingly. It has been validated in large nationally representative adolescent–parent samples and showed profound psychometrical properties with good to excellent internal consistency, criterion validity, and discriminatory power (12, 15, 40, 55, 65, 66). Accordance between self-rating and parental rating was moderate. Moreover, GADIS-A has been evaluated with Persian and Russian adolescents with good to very good internal consistency and adequate to very good retest reliability (67, 68). Adolescents and parents indicate their agreement with nine statements on a five-point Likert scale (strongly disagree [0]–strongly agree [4]) under consideration of the past 12 months with higher total scale scores resembling more problems. The 10th item reflects the frequency of problems, conflicts, or difficulties due to the digital medium and is answered by choosing one out of four response options (not at all [0]–nearly daily [3]). The questionnaires can be used for a categorical assessment of the DMUD. Accordingly, a score of ≥2 is considered significant regarding the ICD-11 criteria. Moreover, factor analyses confirmed two underlying scale factors, one for cognitive-behavioral symptoms (CBS) of problematic media usage and one for negative consequences (NC) of the media usage pattern. Cutoffs between scales are comparable, although slightly differing. For GADIS-A and GADIS-P, these are >9 (CBS) and > 5 (NC), for SOMEDIS-A and SOMEDIS-p > 8 (CBS) and > 6 (NC), and for STREDIS-A and SOMEDIS-p > 6 (CBS) and > 11 (NC).
Children and adolescents will be classified as disordered if the cutoffs for both factors are reached and the time criterion is met. Reaching the cutoff of CBS only suggests hazardous media use. In the clinical context, the DMUD test battery has been regularly used and could prove to be helpful in assessing potential symptom changes during therapy.
Additionally, each treating clinician will assess symptom expression, rate fulfillment of the ICD-11 criteria (based on criteria of GD), and diagnosis of a potential specific DMUD. They will be provided with a digital criterion checklist including examples to enhance interpretation based on ICD-11 suggestions, the clinical interview guideline of the Gaming Disorder and Hazardous Gaming Scale (GDHGS) (69), and clinical expert experience.
In the case of the diagnosis of more than one DMUD, the clinically most prominent one (i.e., by total rating scores and clinical evaluation) will be defined as the main DMUD. This will be addressed during intervention and used as a primary outcome, which was assessed during enrollment, at post-intervention, and follow-up. The differences between screening and post-intervention total scale scores will be investigated primarily.
2.10.2 Secondary outcomes
Secondary outcomes can be divided into psychological, media-associated, parental, and family-associated factors and are assessed with the participating adolescents and parents separately (Table 1). For adolescents, these include adolescent emotional and behavioral problems (based on self-rating and parental rating), sleep-associated aspects, mindfulness, and psychological stress perception, media usage times, and family communication/functioning. For the parents, these comprise mindfulness, quality of life, parental media usage, media rules, parental self-efficacy, and family communication/functioning.
2.10.3 Additional variables
Additional variables that will be included as covariates cover sociodemographic information (age, sex/gender, region of living, and parental status), parental mental distress, and parenting style (Table 1). Moreover, data on media usage and app usage patterns, i.e., media usage time as well as number of app usage sessions, days, weeks, quests started, quests completed, mindfulness exercises observed, and calendar entries, as well as the relative completion of modules and complete training will be collected.
2.11 Data collection and management
All data will be collected on an ongoing basis via the Res@t application and stored within the ISO-certified Embloom platform on secure servers with regular backups. Data will be pseudonymized before transferring it in an encrypted form to the secure UKE server. Sensitive participant data will be accessible only to the treating practitioner within individual digital patient folders (within the recruitment center) and authorized admins of Embloom (across the recruitment centers). The latter will have the primary responsibility for verifying the integrity of the database and securing pseudonymized data transfer. A statistician at the UKE who is independent of the evaluation team will monitor trial conduct and data collection manually in addition to automatic monitoring of data completeness by the software. Moreover, pseudonymized data will be reprocessed to fit all structural requirements for the analyses. The principal study center at the DZSKJ will be responsible for managing and archiving the transferred database after analysis. All participant data will be always handled confidentially and in accordance with the General Data Protection Regulation (GDPR).
2.12 Data analysis
Data will be analyzed by the independent statisticians at the IMBE with sophisticated experience in multicenter therapy studies. Descriptive statistics will be presented with respect to both the entire sample and group-wise. The primary analysis is based on the intention-to-treat (ITT) approach with all randomized patients. The significance level will be set at 5% (two-sided). All three primary hypotheses are structured hierarchically. The second primary hypothesis will only be evaluated in a confirmatory way if the first primary hypothesis leads to a significant test result. The third primary hypothesis will only be evaluated in a confirmatory way if the second primary hypothesis leads to a significant test result. For the analysis of each primary hypothesis, a linear mixed model with implicit maximum likelihood correction of missing values under the missing-at-random assumption will be calculated, respectively. The change in DMUD symptoms from baseline to post-treatment will be used as an outcome variable, randomization group, type of DMUD (social media, gaming, streaming), recruitment site size and location as fixed effects, individual recruitment site and patient nested within site as random effects, and the baseline DMUD score as a covariate. The interaction between the randomization group and media usage pattern (hazardous vs. pathological) as well as effects of incomplete dyads will be tested within secondary analyses.
To examine the impact of missing values on the outcome of the primary analysis, sensitivity analyses will be performed using multiple imputation methods to replace missing values. The primary endpoint at follow-up and the secondary endpoints will be investigated exploratorily using analogous methods, which are adequate for the scale type. The following subgroup analyses are planned: severity of DMUD, sex, education, and socioeconomic status. Qualitative assessments of treatment provider satisfaction will be supplemented. Details of the analysis will be specified in a statistical analysis plan. The analysis will be performed with the latest version of the software package R (70).
2.13 Quality assurance and monitoring
All recruitment sites will be supervised by and stay in close contact with the principal study center at UKE during the complete course of the study.
At the beginning of the recruitment, a Data Safety Monitoring Board (DSMB) will be implemented with meetings during initiation, regular monitoring visits, and after study closeout. The DSMB will be comprised of experienced scientists not otherwise involved in the study. Members will be independent of the investigarors and the trial sponsor and will have no conflicts of interests. The DSMB will frequently oversee trial processes and data collection based on the requirements of Good Clinical Practice. These include monitoring of study and recruitment progress, considering adherence to the inclusion criteria, study procedure, recruitment rate, completeness of study documents, protocol deviations, loss-to-follow-up data, serious adverse events (SAEs), adverse events (AEs), and/or newly emerged evidence of potential harmful effects of the intervention, and all potential study problems. Meetings will be held in closed and open manner. The latter includes the discussion of management issues with the coordinating investigator at the principal study center. Recommendations on study continuation, necessary design changes, or the end of the trial will be given by the DSMB without the involvement of the coordinating investigator.
2.14 Safety
Data safety is secured via confirmation with the Information Security Management System Standard (ISO/IEC 27001:2013y) in accordance with the Declaration of Applicability v 2.0 d.d. 22/10/2019. This certificate is valid within the scope of information security related to the development and management of e-health applications for healthcare providers and the purpose of measuring, monitoring, and treating psychological and physical symptoms. Data collection, transfer, and storage are described within a data protection concept, which has been approved by the data protection officer at the UKE.
Participant safety, especially the safety of minor-aged patients, is secured primarily by the clinicians during regular treatment. They will continuously monitor adverse events (AEs) and serious adverse events (SAEs) and report these as an (S)AE comment within the case report form of Embloom software. (S)AEs will be rated based on the NCI Common Terminology Criteria for Adverse Events (71). They will be carefully monitored, documented, and reported to the coordinating investigator and the Data Safety Monitoring Board (DSMB) members within 1 week of the initial observation. DSMB experts will comment on potential causal study relations to identify serious study-related events (SSREs), to determine benefit–risk of trial continuation and adequate participant support. SSREs might include suicidal ideation and behavior, self-harming behavior, worsening of general wellbeing, mental distress, or psychiatric comorbidities with an indication for hospitalization. SAEs and SSREs will be reported to the local ethics committees.
2.15 Clinical trial registry
The trial is registered on the German Clinical Trials Register (DRKS00031043, https://drks.de).
3 Discussion
Given the rising prevalence of DMUD, especially during the vulnerable period of adolescence, and a severe lack of evidence-based treatment options, especially for this age group and their parents, Res@t digital aims to close a significant gap. Res@t is the first model-based manualized training program to reduce DMUD symptoms that specifically includes adolescents and parents. It has been applied and pilot-tested in different settings and translated into a digitalized version. Within a large clinical consortium, the effectiveness of Res@t digital will be independently evaluated in a multicenter cluster RCT study in the clinical context. This setting was chosen to investigate a novel intervention for those in urgent need and secure safety of mostly minor patients. In the case of a positive evaluation, Res@t digital can be applied quickly and support potentially limited local medical care structures by providing evidence-based treatment content. The reliable screening for and treatment of DMUD can prevent aggravation and chronification of symptoms. Res@t digital might be used to bridge waiting time and support patients who initially avoid face-to-face interventions due to factors such as lack of motivation, logistic, time, or financial problems. Accordingly, a recent systematic review and meta-analysis could not find differences between the treatment effectiveness of face-to-face intervention and digital intervention in the context of anxiety disorders (72).
In addition, applying the Res@t app with its up-to-date treatment material within a blended therapy context might enrich and facilitate face-to-face interventions and allow multiple self-guided repetitions to consolidate content. Reviews suggest positive effects of such an approach across age groups including adolescent patients (73, 74) with evidence of beneficial effects of guided (versus unguided) digital interventions (75). Moreover, the beneficial effects of additional face-to-face interventions are assumed to vary according to the reachability of adolescents with DMUD. Therefore, within a subproject of the Res@t digital consortium, it will be investigated how much face-to-face contact is required to guide affected adolescents through the Res@t digital intervention. These adolescents will be supported by the youth welfare system but will not yet be involved in outpatient care.
The Res@t application ensures highest quality standards and has the potential to reduce health care costs. As with other e-health interventions, it might help reaching a broader patient group (76), not only for affected German adolescents but potentially worldwide. By involving primary healthcare providers in the evaluation process, this study is settled within direct healthcare research, mirroring immediate realities of life and high practical relevance.
Based on our current knowledge, Res@t digital has the potential of an effective, safe, and cost-efficient treatment option for a significant number of adolescent patients and their parents. In the future, new modules could be added or current modules could be altered and tested to fit the demands of different settings, such as schools, youth, and counseling services, or expand to additional age groups such as young adults or younger children.
4 Limitations
A cluster-randomized design was chosen to exclude contamination effects on TAU within IG and CG. However, by involving practitioners actively in the study and providing structured diagnostic tools for the assessment of DMUD, it cannot be ruled out that TAU is altered by an increased awareness of the clinicians. This effect might be stronger in recruitment sites that are allocated to CG as child, and adolescent psychiatrists and psychotherapists strive to address detected problems, where no immediate additional support is available. More attention to the CG compared with the IG would result in a potential reduction in the overall outcome effect. Measures taken against this will include proper instruction of recruiting practitioners. Moreover, the cluster-randomized design does not allow initial sample stratification, e.g., regarding the type of DMUD, sex, age, and single versus dyad study participation. However, the number of recruitment sites is aimed to be so high that these variables should be distributed randomly. Another potential drawback of cluster randomization is that the waiting CG will get access to the intervention after their individual data collection but not after full data collection. Based on the feedback from recruiting clinicians, waiting times of several months up to a year in that case would not have been acceptable. Clinicians will be instructed to not to alter TAU based on their experiences with Res@t digital. However, contamination effects on TAU cannot be ruled out.
A potential risk for project realization could be that recruiting a significant number of parent–child dyads are more challenging than expected. Therefore, a large clinical consortium has been established. The heterogeneity of the consortium might induce additional variance (TAU, support of study). However, measures are being taken to control this effect. These include clear recruitment instructions, attractive remuneration for successful recruiting, including recruitment site size into the stratification process of randomization and recruitment site itself as a nested factor into the multilevel model analyses. Participant dropout has been estimated conservatively but is especially challenging since parent–child dyads are addressed. Hence, dropout could be higher than expected. Rates should be kept as low as possible by personal contacts and motivation via practitioner, reminders, app visualization of progress, fostering parent–child interaction during the intervention process, and family incentives in the case of full assessment completion. Moreover, separate analyses will be performed on incomplete dyads.
The evaluation of the primary outcome includes self-rating, parental rating, and expert rating in a hierarchical order. The use of different ratings for diagnosis and monitoring is highly common in clinical practice. On the one hand, it can be observed that affected adolescents might show a tendency to understate present symptoms due to feelings of shame and social desirability (77), lowered introspective abilities (78), self-regulatory and executive control functions (79), or denial and concealment typical for addictive disorders (80). On the other hand, parents’ worries often lead to a focus on (potentially) negative consequences of problematic behavioral patterns of their children. This could result in a more critical symptom evaluation or even exaggeration (81–83). The clinician tries to integrate all available information and applies diagnostic criteria for evaluation. Consequently, diverging symptom estimates might occur which need to be considered when interpreting the evaluation results.
Moreover, since the aim is a large sample, no objective measures can be applied to evaluate intervention effectiveness for the complete sample, even though these would be highly appreciated. Hence, a second subproject within the Res@t consortium focusing on DMUD-associated sleep–wake alterations will apply neuropsychological and physiological measures including actigraphy in a subsample.
5 Conclusion
Res@t digital is the first model-based and app-based intervention that addresses the vulnerable group of adolescents with DMUD or hazardous use patterns and a respective parent in order to reduce symptoms and negative sequelae, prevent chronification, and foster the mastering of developmental tasks. After standardized diagnosis, treatment effectiveness will be evaluated by applying a multicenter cluster-randomized pre–post follow-up waitlist control group design with evaluator blinding within the primary clinical care setting. It will be tested if Res@t digital is feasible for and effective in outpatients who receive the intervention in addition to TAU compared with the control group with TAU only. By selecting a study setting within primary clinical care, optimal patient security can be assured, blended-therapy approaches are made possible, and important implementation factors can be accounted for to increase acceptance and accessibility from the very beginning. If effectiveness is shown, Res@t will be made available for long-term perpetuation, considering practicability and potential independence of local care structures and cost-effectiveness.
Ethics statement
The study was approved by the Ethics Committee of the Medical Board Hamburg. The study will be conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study will be provided by the participants and their legal guardians/next of kin.
Author contributions
KP and RT acquired the funding for the trial. KP contributed to the conceptualization, intervention content, study design and methodology, and prepared the original draft. AZ provided guidance on the study design and statistical issues. KB contributed to manuscript preparation including editing and visualization. SD and TK contributed to project implementation. SD, NA, AP-K, and OR served as scientific advisors. J-OC and A-LS contributed to the intervention content. RT contributed to the resources and supervision. All authors contributed to the article and approved the submitted version.
Funding
The study is funded by the German Innovation Fund of the Federal Joint Committee (G-BA Innovationsfond: 01NVF20011). The funding source have no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
Acknowledgments
RT is the coordinator and KP is the co-coordinator of the Res@t consortium. The consortium comprises two subprojects. Subproject leaders are Alexander Prehn-Kristensen and Olaf Reis. Clinical consortium partners are: Hubertus Adam (Martin Gropius Hospital GmbH Eberswalde), Martin Holtmann and Tanja Legenbauer (LWL-University Clinic Hamm), Marianne Klein, Claas van Aaken, and Birgit Rudnicki (Clinic Weissenhof/ Center for Psychiatry Weinsberg), Martina Pitzer (Vitos Rheingau gGmbH), Beate Reinders and Günther Stratmann (Pfalzklinikum for Psychiatry and Neurology AdöR). Consortium partners representing four German statutory health insurances companies are Sibel Vildan Altin and Olaf Beckmann (AOK Rheinland/Hamburg), Jennifer Lenz & Sophia Rocabado (DAK), Frank Liedtke & Jessica Stohri (Barmer Hamburg), Johanna Kampmann (TK) and one statutory health insurance company as a cooperation partner Thomas Marks & Katrin Meißner (BKK Regional Association NORDWEST). Further members of the consortium are (in alphabetical order): Nicolas Arnaud, Hannah Brauer, Ivo Buil, Katharina Busch, Jan-Ole Cloes, Silke Diestelkamp, Marco Essed, Nicole Fangerau, Fabian Flaßkamp, Anne-Katrin Gerber, Sylvia Hansen, Julian Harbs, Martin Hoff, Jaimy Kerstges, Thomas Krömer, Oliver, Labrenz Susanne Lezius, Manuel Munz, Johanna Philippi, Sarah Runge, Ina Schloss, Clara Marie Schreiber, Anna-Lena Schulz, Katharina Stahlmann, Bart van Viggen, Christina Wacker, Felix von Warburg and Antonia Zapf. We thank Stanni Otten and Frank Visser for visualizations and Uta Wittekind for voice overs as well as Nele Fritsch, Lucie Nike Könnecke and Miriam Rabels. Additionally, we thank the Professional Association for Child and Adolescent Psychiatry, Psychosomatics, and Psychotherapy in Germany e.V. and the German Society for Child and Adolescent Psychiatry, Psychosomatics, and Psychotherapy for supporting the project, and all committed clinical partners for participant recruitment.
Conflict of interest
AP-K received funding and HB consulting fees by mementor by ResMed.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. PWC . Global Entertainment and Media Outlook. (2023). Available at: https://www.pwc.com/gx/en/industries/tmt/media/outlook/outlook-perspectives.html (Accessed January 13, 2023)
2. Statista . Video Game Market Revenue Worldwide in 2022. (2023). Available at: https://de.statista.com/statistik/daten/studie/196642/umfrage/abonnenten-von-netflix-quartalszahlen/ (Accessed January 13, 2023)
3. Zendle, D, Flick, C, Halgarth, D, Ballou, N, Demediuk, S, and Drachen, A. Cross-cultural patterns in mobile playtime: an analysis of 118 billion hours of human data. Sci Rep. (2023) 13:386. doi: 10.1038/s41598-022-26730-w
4. Medrano, M, Cadenas-Sanchez, C, Oses, M, Arenaza, L, Amasene, M, and Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: a longitudinal analysis from the MUGI project. Pediatr Obes. (2021) 16:e12731. doi: 10.1111/ijpo.12731
5. Schmidt, SCE, Anedda, B, Burchartz, A, Eichsteller, A, Kolb, S, Nigg, C, et al. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: a natural experiment. Sci Rep. (2020) 10:21780. doi: 10.1038/s41598-020-78438-4
6. Paschke, K, Austermann, MI, Simon-Kutscher, K, and Thomasius, R. Adolescent gaming and social media usage before and during the COVID-19 pandemic: interim results of a longitudinal study. SUCHT. (2021) 67:13–22. doi: 10.1024/0939-5911/a000694
7. Feierabend, S, Rathgeb, T, Kheredmand, H, and Glöckler, S. JIM-Studie 2021 Medien - Basisstudie zum Medienumgang 12- bis 19-Jähriger in Deutschland. Medienpädagogischer Forschungsverbund Südwest (MPFS). Stuttgart: Medienpädagogischer Forschungsverbund Südwest (2021).
8. Cho, DJ, Kim, HT, Lee, J, and Park, SH. Economic cost–benefit analysis of the addictive digital game industry. Appl Econ Lett. (2018) 25:638–42. doi: 10.1080/13504851.2017.1355528
9. Stevens, MWR, Dorstyn, D, Delfabbro, PH, and King, DL. Global prevalence of gaming disorder: a systematic review and meta-analysis. Aust N Z J Psychiatry. (2021) 55:553–68. doi: 10.1177/0004867420962851
10. Kim, HS, Son, G, Roh, E-B, Ahn, W-Y, Kim, J, Shin, S-H, et al. Prevalence of gaming disorder: a meta-analysis. Addict Behav. (2022) 126:107183. doi: 10.1016/j.addbeh.2021.107183
11. Cheng, C, Lau, Y, Chan, L, and Luk, JW. Prevalence of social media addiction across 32 nations: meta-analysis with subgroup analysis of classification schemes and cultural values. Addict Behav. (2021) 117:106845. doi: 10.1016/j.addbeh.2021.106845
12. Paschke, K, Napp, A-K, and Thomasius, R. Parents rate problematic video streaming in adolescents: conceptualization and external assessment of a new clinical phenomenon based on the ICD-11 criteria of gaming disorder. JCM. (2023) 12:1010. doi: 10.3390/jcm12031010
13. Starosta, J, and Izydorczyk, B. Understanding the phenomenon of binge-watching—a systematic review. Int J Environ Res Public Health. (2020) 17:4469. doi: 10.3390/ijerph17124469
14. Flayelle, M, Maurage, P, Di Lorenzo, KR, Vögele, C, Gainsbury, SM, and Billieux, J. Binge-watching: what do we know so far? A first systematic review of the evidence. Curr Addict Rep. (2020) 7:44–60. doi: 10.1007/s40429-020-00299-8
15. Paschke, K, Napp, A-K, and Thomasius, R. Applying ICD-11 criteria of gaming disorder to identify problematic video streaming in adolescents: conceptualization of a new clinical phenomenon (STREDIS-A). JBA. (2022) 11:451–66. doi: 10.1556/2006.2022.00041
16. Casey, BJ, and Jones, RM. Neurobiology of the adolescent brain and behavior: implications for substance use disorders. J Am Acad Child Adolesc Psychiatry. (2010) 49:1189–201. doi: 10.1016/j.jaac.2010.08.017
17. Schettler, L, Thomasius, R, and Paschke, K. Neural correlates of problematic gaming in adolescents: a systematic review of structural and functional magnetic resonance imaging studies. Addict Biol. (2021) 27:e13093. doi: 10.1111/adb.13093
18. WHO . International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision). Geneva, Switzerland: World Health Organization (2018).
19. Rumpf, H-J, Batra, A, Bischof, A, Hoch, E, Lindenberg, K, Mann, K, et al. Vereinheitlichung der Bezeichnungen für Verhaltenssüchte. SUCHT. (2021) 67:181–5. doi: 10.1024/0939-5911/a000720
20. Kielholz, P, and Ladewig, D. Die Abhängigkeit von Drogen. München: Dt. Taschenbuch-Verlag (1973).
21. Lazarus, RS . Psychological stress and coping in adaptation and illness. Int J Psychiatry Med. (1974) 5:321–33. doi: 10.2190/T43T-84P3-QDUR-7RTP
22. Paschke, K, Cloes, J-O, and Thomasius, R. Res@t: resource-strengthening training for adolescents with problematic digital-media use and their parents. SUCHT. (2023) 69:75–85. doi: 10.1024/0939-5911/a000810
23. Stevens, MWR, King, DL, Dorstyn, D, and Delfabbro, PH. Cognitive–behavioral therapy for internet gaming disorder: a systematic review and meta-analysis. Clin Psychol Psychother. (2019) 26:191–203. doi: 10.1002/cpp.2341
24. Bonnaire, C, Liddle, HA, Har, A, Nielsen, P, and Phan, O. Why and how to include parents in the treatment of adolescents presenting internet gaming disorder? J Behav Addict. (2019) 8:201–12. doi: 10.1556/2006.8.2019.27
25. Paschke, K, Holtmann, M, Melchers, P, Klein, M, Schimansky, G, Krömer, T, et al. Media-associated disorders in childhood and adolescence: evidence paper of the joint addiction commision of the German societies and professional associations of child and adolescent psychiatry and psychotherapy. Z Kinder Jugendpsychiatr Psychother. (2020) 48:303–17. doi: 10.1024/1422-4917/a000735
26. Wendt, LM, Austermann, MI, Rumpf, H-J, Thomasius, R, and Paschke, K. Requirements of a group intervention for adolescents with internet gaming disorder in a clinical setting: a qualitative interview study. IJERPH. (2021) 18:7813. doi: 10.3390/ijerph18157813
27. Karyotaki, E, Efthimiou, O, Miguel, C, Bermpohl, FMG, Furukawa, TA, Cuijpers, P, et al. Internet-based cognitive Behavioral therapy for depression: a systematic review and individual patient data network meta-analysis. JAMA Psychiatry. (2021) 78:361–71. doi: 10.1001/jamapsychiatry.2020.4364
28. Lattie, EG, Adkins, EC, Winquist, N, Stiles-Shields, C, Wafford, QE, and Graham, AK. Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being among college students: systematic review. J Med Internet Res. (2019) 21:e12869. doi: 10.2196/12869
29. Tang, Y, Gierc, M, Lam, RW, Liu, S, and Faulkner, G. The effectiveness of internet-guided self-help interventions to promote physical activity among individuals with depression: systematic review. JMIR Ment Health. (2022) 9:e38049. doi: 10.2196/38049
30. Thabrew, H, Stasiak, K, Hetrick, SE, Wong, S, Huss, JH, and Merry, SN. E-health interventions for anxiety and depression in children and adolescents with long-term physical conditions. Cochrane Database Syst Rev. (2018) 2018:CD012489. doi: 10.1002/14651858.CD012489.pub2
31. Aguirre Velasco, A, Cruz, ISS, Billings, J, Jimenez, M, and Rowe, S. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? A systematic review. BMC Psychiatry. (2020) 20:293. doi: 10.1186/s12888-020-02659-0
32. Liverpool, S, Mota, CP, Sales, CMD, Čuš, A, Carletto, S, Hancheva, C, et al. Engaging children and young people in digital mental health interventions: systematic review of modes of delivery, facilitators, and barriers. J Med Internet Res. (2020) 22:e16317. doi: 10.2196/16317
33. Gainsbury, S, and Blaszczynski, A. A systematic review of internet-based therapy for the treatment of addictions. Clin Psychol Rev. (2011) 31:490–8. doi: 10.1016/j.cpr.2010.11.007
34. Hutton, A, Prichard, I, Whitehead, D, Thomas, S, Rubin, M, Sloand, E, et al. mHealth interventions to reduce alcohol use in young people: a systematic review of the literature. Compr Child Adolesc Nurs. (2020) 43:171–202. doi: 10.1080/24694193.2019.1616008
35. Kazemi, DM, Li, S, Levine, MJ, Auten, B, and Granson, M. Systematic review of smartphone apps as a mHealth intervention to address substance abuse in adolescents and adults. UJAN. (2021) 32:180–7. doi: 10.1097/JAN.0000000000000416
36. Calear, AL, Christensen, H, Mackinnon, A, Griffiths, KM, and O’Kearney, R. The YouthMood project: a cluster randomized controlled trial of an online cognitive behavioral program with adolescents. J Consult Clin Psychol. (2009) 77:1021–32. doi: 10.1037/a0017391
37. Venturo-Conerly, KE, Osborn, TL, Alemu, R, Roe, E, Rodriguez, M, Gan, J, et al. Single-session interventions for adolescent anxiety and depression symptoms in Kenya: a cluster-randomized controlled trial. Behav Res Ther. (2022) 151:104040. doi: 10.1016/j.brat.2022.104040
38. DAK-Gesundheit . DAK Study: Gaming, Social-Media & Corona. (2020). Available at: https://www.dak.de/dak/gesundheit/dak-studie-gaming-social-media-und-corona-2295548.html#/ (Accessed January 22, 2021)
39. Lohbeck, A, Schultheiss, J, Petermann, F, and Petermann, U. The German self-report version of the strengths and difficulties questionnaire (SDQ-Deu-S): psychometric properties, factor structure, and critical values. Diagnostica. (2015) 61:222–35. doi: 10.1026/0012-1924/a000153
40. Paschke, K, Austermann, MI, and Thomasius, R. ICD-11-based assessment of social media use disorder in adolescents: development and validation of the social media use disorder scale for adolescents. Front Psych. (2021) 12:661483. doi: 10.3389/fpsyt.2021.661483
41. Goodman, R . The strengths and difficulties questionnaire: a research note. J Child Psychol & Psychiat. (1997) 38:581–6. doi: 10.1111/j.1469-7610.1997.tb01545.x
42. Altendorfer-Kling, U, Ardelt-Gattinger, E, and Thun-Hohenstein, L. Der Selbstbeurteilungsbogen des SDQ anhand einer österreichischen Feldstichprobe. Z Kinder Jugendpsychiatr Psychother. (2007) 35:265–71. doi: 10.1024/1422-4917.35.4.265
43. Buysse, DJ, Reynolds, CF, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
44. Johns, MW . A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. (1991) 14:540–5. doi: 10.1093/sleep/14.6.540
45. Janssen, KC, Phillipson, S, O’Connor, J, and Johns, MW. Validation of the Epworth sleepiness scale for children and adolescents using Rasch analysis. Sleep Med. (2017) 33:30–5. doi: 10.1016/j.sleep.2017.01.014
46. Pilcher, JJ, Switzer, FS, Munc, A, Donnelly, J, Jellen, JC, and Lamm, C. Psychometric properties of the Epworth sleepiness scale: a factor analysis and item-response theory approach. Chronobiol Int. (2018) 35:533–45. doi: 10.1080/07420528.2017.1420075
47. Cohen, S, and Williamson, G. Perceived stress in a probability sample of the United States In: S Spacapan and S Oskamp (editors). The social Psychology of Health. The Claremont Symposium on Applied Social Psychology. Thousand Oaks, CA, US: Sage Publications, Inc (1988). 31–67.
48. Klein, EM, Brähler, E, Dreier, M, Reinecke, L, Müller, KW, Schmutzer, G, et al. The German version of the perceived stress scale – psychometric characteristics in a representative German community sample. BMC Psychiatry. (2016) 16:159. doi: 10.1186/s12888-016-0875-9
49. Smilkstein, G, Ashworth, C, and Montano, D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. (1982) 15:303–11.
50. Wartberg, L, Zieglmeier, M, and Kammerl, R. Accordance of adolescent and parental ratings of internet gaming disorder and their associations with psychosocial aspects. Cyberpsychol Behav Soc Netw. (2019) 22:264–70. doi: 10.1089/cyber.2018.0456
51. Olson, DH, Gorall, DM, and Tiesel, JW. Faces IV Package: Administration Manual. Minneapolis, MN: Life Innovations (2004).
52. Akhlaq, A, Malik, NI, and Khan, NA. Family communication and family system as the predictors of family satisfaction in adolescents. Sci J Psychol. (2013) 2013:1–6. doi: 10.7237/sjpsych/258
53. Brown, KW, and Ryan, RM. The benefits of being present: Mindfulness and its role in psychological well-being. J Pers Soc Psychol (2009). 84:822–48. doi: 10.1037/0022-3514.84.4.822
54. Michalak, J, Heidenreich, T, Ströhle, G, and Nachtigall, C. Die deutsche Version der Mindful Attention and Awareness Scale (MAAS) Psychometrische Befunde zu einem Achtsamkeitsfragebogen. Z Klin Psychol Psychother. (2008) 37:200–8. doi: 10.1026/1616-3443.37.3.200
55. Paschke, K, Austermann, MI, and Thomasius, R. International classification of Diseases-11-based external assessment of social media use disorder in adolescents: development and validation of the social media use disorder scale for parents. Cyberpsychol Behav Soc Netw. (2022) 25:518–26. doi: 10.1089/cyber.2022.0020
56. Rivadeneira, J, and López, MA. Family communication scale: validation in Chilean. Acta Colombiana de Psicología. (2017) 20:127–37. doi: 10.14718/ACP.2017.20.2.6
57. Kroenke, K, Spitzer, RL, and Williams, JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
58. Kroenke, K, Spitzer, RL, Williams, JBW, and Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. (2010) 32:345–59. doi: 10.1016/j.genhosppsych.2010.03.006
59. Löwe, B, Kroenke, K, Herzog, W, and Gräfe, K. Measuring depression outcome with a brief self-report instrument: sensitivity to change of the patient health questionnaire (PHQ-9). J Affect Disord. (2004) 81:61–6. doi: 10.1016/S0165-0327(03)00198-8
60. Löwe, B, Müller, S, Brähler, E, Kroenke, K, Albani, C, and Decker, O. Validierung und Normierung eines kurzen Selbstratinginstrumentes zur Generalisierten Angst (GAD-7) in einer repräsentativen Stichprobe der deutschen Allgemeinbevölkerung. Psychother Psych Med. (2007) 57:970669. doi: 10.1055/s-2007-970669
61. Satow, L. Eltern-Erziehungsstil-Inventar (EEI): Test-und Skalendokumentation; (2013). Available at: http://www.drsatow.de (Accessed September 22, 2021)
62. Kliem, S, Kessemeier, Y, Heinrichs, N, Döpfner, M, and Hahlweg, K. Der Fragebogen zur Selbstwirksamkeit in der Erziehung (FSW) [Parenting self-efficacy questionnaire]. Diagnostica. (2014) 60:35–45. doi: 10.1026/0012-1924/a000107
63. Goldbeck, L, and Storck, M. Das Ulmer Lebensqualitäts-Inventar für Eltern chronisch kranker Kinder (ULQIE). Z Klin Psychol Psychother. (2002) 31:31–9. doi: 10.1026/0084-5345.31.1.31
64. Hülquist, J, Fangerau, N, Thomasius, R, and Paschke, K. Resource-strengthening training for parents of adolescents with problematic gaming (Res@t-P): a clinical pilot study. IJERPH. (2022) 19:9495. doi: 10.3390/ijerph19159495
65. Paschke, K, Austermann, MI, and Thomasius, R. Assessing ICD-11 gaming disorder in adolescent gamers: development and validation of the gaming disorder scale for adolescents (GADIS-A). JCM. (2020) 9:993. doi: 10.3390/jcm9040993
66. Paschke, K, Austermann, MI, and Thomasius, R. Assessing ICD-11 gaming disorder in adolescent gamers by parental ratings: development and validation of the gaming disorder scale for parents (GADIS-P). J Behav Addict. (2021) 10:159–68. doi: 10.1556/2006.2020.00105
67. Mazaherizadeh, A, Taherifar, Z, and Farahani, H. Psychometric properties of the Farsi version of the gaming disorder scale for adolescents (GADIS-A). BMC Psychol. (2022) 10:195. doi: 10.1186/s40359-022-00899-1
68. Nazari, N, Shabbir, MS, Sevbitov, AV, Sadeghi, M, and Griffiths, MD. Psychometric evaluation of the Russian version of the gaming disorder scale for adolescents. Curr Psychol. (2022) 42:13754–68. doi: 10.1007/s12144-021-02575-w
69. Balhara, YPS, Singh, S, Saini, R, Kattula, D, Chukkali, S, and Bhargava, R. Development and validation of Gaming Disorder and Hazardous Gaming Scale (GDHGS) based on the WHO framework (ICD-11 criteria) of disordered gaming. Asian J Psychiatr. (2020) 54:102348. doi: 10.1016/j.ajp.2020.102348
70. R Core Team . R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2019).
71. GBG . NCI Common Terminology Critera for Adverse Events (CTCAE) – GBG. (2020). Available at: https://www.gbg.de/de/rechner/ctcae.php (Accessed September 13, 2021).
72. Pauley, D, Cuijpers, P, Papola, D, Miguel, C, and Karyotaki, E. Two decades of digital interventions for anxiety disorders: a systematic review and meta-analysis of treatment effectiveness. Psychol Med. (2021) 53:1–13. doi: 10.1017/S0033291721001999
73. Erbe, D, Eichert, H-C, Riper, H, and Ebert, DD. Blending face-to-face and internet-based interventions for the treatment of mental disorders in adults: systematic review. J Med Internet Res. (2017) 19:e306. doi: 10.2196/jmir.6588
74. Rasing, SPA . Blended treatment for depressive disorders in youth: a narrative review. J Cogn Ther. (2021) 14:47–58. doi: 10.1007/s41811-020-00088-1
75. Baumeister, H, Reichler, L, Munzinger, M, and Lin, J. The impact of guidance on internet-based mental health interventions — a systematic review. Internet Interv. (2014) 1:205–15. doi: 10.1016/j.invent.2014.08.003
76. Postel, MG, de Jong, CAJ, and de Haan, HA. Does E-therapy for problem drinking reach hidden populations? AJP. (2005) 162:2393:2393. doi: 10.1176/appi.ajp.162.12.2393
77. Moshagen, M, Musch, J, Ostapczuk, M, and Zhao, Z. Brief report: reducing socially desirable responses in epidemiologic surveys: an extension of the randomized-response technique. Epidemiology. (2010) 21:379–82. doi: 10.1097/EDE.0b013e3181d61dbc
78. Weil, LG, Fleming, SM, Dumontheil, I, Kilford, EJ, Weil, RS, Rees, G, et al. The development of metacognitive ability in adolescence. Conscious Cogn. (2013) 22:264–71. doi: 10.1016/j.concog.2013.01.004
79. Zhou, Z, Zhou, H, and Zhu, H. Working memory, executive function and impulsivity in internet-addictive disorders: a comparison with pathological gambling. Acta Neuropsychiatr. (2016) 28:92–100. doi: 10.1017/neu.2015.54
80. Schneider, LA, King, DL, and Delfabbro, PH. Maladaptive coping styles in adolescents with internet gaming disorder symptoms. Int J Ment Health Addiction. (2018) 16:905–16. doi: 10.1007/s11469-017-9756-9
81. Vadlin, S, Åslund, C, Rehn, M, and Nilsson, KW. Psychometric evaluation of the adolescent and parent versions of the gaming addiction identification test (GAIT). Scand J Psychol. (2015) 56:726–35. doi: 10.1111/sjop.12250
82. De Los, RA, and Kazdin, AE. Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull. (2005) 131:483–509. doi: 10.1037/0033-2909.131.4.483
Keywords: digital media-use disorders, e-health, digital intervention, cognitive-behavioral therapy, adolescents, parents
Citation: Paschke K, Diestelkamp S, Zapf A, Busch K, Arnaud N, Prehn-Kristensen A, Reis O, Stark M, Cloes J-O, Schulz A-L, Brauer H, Krömer T and Thomasius R the Res@t Consortium (2024) An app-based training for adolescents with problematic digital-media use and their parents (Res@t digital): protocol for a cluster-randomized clinical trial. Front. Psychiatry. 14:1245536. doi: 10.3389/fpsyt.2023.1245536
Reviewed by:
Shimin Zhu, Hong Kong Polytechnic University, Hong Kong SAR, ChinaEser Ercil, Independent Researcher, Lisbon, United States
Copyright © 2024 Paschke, Diestelkamp, Zapf, Busch, Arnaud, Prehn-Kristensen, Reis, Stark, Cloes, Schulz, Brauer, Krömer and Thomasius. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kerstin Paschke, ay5wYXNjaGtlQHVrZS5kZQ==