 Aviv M. Weinstein
Aviv M. Weinstein
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 27 October 2023
Sec. Addictive Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1230760
This article is part of the Research Topic Insights in Addictive Disorders: 2023 View all 7 articles
There is increased risk of psychosis associated with cannabis use disorder and the interaction of THC with dopamine neurotransmission is complex. It is important to investigate the recovery from cannabis-induced psychosis and its effects on the brain’s dopamine neurotransmission. This study was to evaluate dopamine receptor D2 availability in the striatum (caudate/putamen) in recently abstinent cannabis dependent users after recovery from psychosis in comparison with abstinent MDMA “ecstasy” abusers and healthy control participants. Participants were eight abstinent ex cannabis-dependent users who were treated for cannabis-induced psychosis with anti-psychotic medication and psychosocial support for 4 months in an inpatient treatment center for drug users. They were compared with nine abstinent ex MDMA “ecstasy” abusers who received medication and psycho-social treatment for 4 months at the same treatment facility and eight healthy control participants. All participants were scanned with bolus and constant infusion of [123I] Iodobenzamide (IBZM) in Single Photon Computed Tomography (SPECT). Cannabis abstinent users who were treated for cannabis-induced psychotic episodes showed no difference in dopamine D2 receptor availability in the caudate compared with abstinent MDMA “ecstasy” abusers and healthy control participants. This finding indicates minimal effects of cannabis-induced psychosis on dopamine reward mechanisms. There is evidence for reduced D2 receptor availability measures in the right putamen (uncorrected) which may indicate a residual effect of anti-psychotic medication.
There is growing evidence of high rates (40–50%) of substance use disorders among individuals with psychotic illness especially in young adolescents where it can be up to 70% (1, 2).
Cannabis use is a risk factor for developing schizophrenia although the issue is controversial (3, 4). A prospective study of cannabis use showed that cannabis use increased the risk for psychotic symptoms in young people (aged 14–24 years), particularly in individuals who are predisposed for psychosis (5). Pre-clinical studies showed that acute administration of Δ-9 tetrahydrocannabinol (THC) activated dopamine in the meso-limbic dopamine system and release of acetylcholine in the hippocampus and prefrontal cortex (6). Repeated daily administration of THC for 7 or 14 days reduced dopamine turnover in the medial prefrontal cortex (7). Consistent with this evidence, brain-imaging studies showed THC-induced dopamine release in the Striatum and limbic regions (8, 9). This evidence supports the notion of psychotogenic properties of THC and the hypothesis of dopamine over-activity in schizophrenia (10).
Laboratory experiments studied the relationship between cannabis and psychosis [see reviews by Radhakrishnan et al. (1), Ranganathan et al. (2), Sherif et al. (11), Volkow et al. (12), Hindley et al. (13)]. D’Souza et al. (14) showed that THC induced positive symptoms of schizophrenia. Morrison et al. (15) reported similar effects of 2.5 mg i.v of THC in healthy participants. Hindley et al. (13) have reviewed eligible studies on the acute administration of THC and four studies on CBD with THC administration. They have reported that THC increased total psychiatric symptom severity, positive symptom severity and negative symptom severity with a large effect sizes.
There is consistent evidence that THC acutely induces psychotic symptoms via CB1 receptor partial agonism and that heavy long-term cannabis use during adolescence exacerbates the risk of psychosis (16). Individuals with high risk for psychosis had high endocannabinoid levels in peripheral blood (17). Those with prodromal psychotic symptoms of a pre-psychotic phase or attenuated psychosis syndrome showed high activity of endocannabinoids during the beginning of the disorder (18). There is further evidence that chronic cannabis use leads to CB1 receptor down-regulation similarly to medication naive cannabis-free patients with schizophrenia (19). Furthermore, peripheral endocannabinoid anandamide (endogenous CB1 receptor agonist) is elevated in individuals with schizophrenia (20).
Cannabis exacerbates psychotic symptoms among individuals with schizophrenia (21) and there is evidence showing an association between psychosis and dopamine, thus elevated striatal dopamine synthesis and release capacity has been found in people with genetic and/or clinical high risk for schizophrenia in some studies (22). THC affects dopaminergic transmission with some consistent and complex findings (23), which merit further investigation.
Very few brain imaging studies investigated the link between cannabis use and psychosis. Delta-9-THC induced psychotic symptoms but no significant dopamine release in healthy volunteers, suggesting that dopamine release in the striatum is not responsible for cannabis-induced psychosis (24). This evidence is contrary to the argument that enhanced cannabis-induced dopamine release may give rise to delusions and hallucinations (10).
Regular cannabis users after abstinence and recovery display dopamine D2 measures of availability that is not different from healthy control participants (25–27). These findings indicate normal levels of dopamine function after recovery. However, recovery as result of treatment cannot be ascertained because baseline measures of dopamine D2 availability were not taken in these studies. Furthermore, it is not known whether recovery from cannabis-induced psychosis is associated with normal measures of dopamine D2 receptor availability. The increased risk of cannabis-induced psychosis and the complex interaction of THC with dopamine neurotransmission, merits an investigation on the effects of cannabis-induced psychosis on the brain’s dopamine neurotransmission mechanisms after recovery.
Previous studies have investigated the relationship between striatal dopamine function and symptoms in psychotic disorders, and they have measured the whole striatum (28–30). A recent study has measured spatial variability in dopamine synthesis capacity and psychotic symptoms combining 18F-DOPA in positron emission tomography (PET) and resting-state magnetic resonance imaging in patients with first-episode psychosis and healthy control participants (31). Although no subdivision relationships were found when using anatomical divisions, dopamine function in striatal areas connected to the default mode network correlated with negative symptoms. These findings suggest that individual differences in the topography of dopamine dysfunction within the striatum contribute to psychotic symptoms.
The aim of this study was to evaluate dopamine receptor D2 availability in the striatum (caudate/putamen) in abstinent cannabis users after recovery from cannabis-induced psychosis. We have also included a control group pf recently abstinent MDMA ‘ecstasy” abusers after 4–6 months of recovery and healthy control participants. The rationale for using this group is that MDMA or “ecstasy” abuse is associated with chronic effects on the brains serotonin 5-HT system but its effects on the brain’s dopamine neurotransmission during drug abuse and recovery is unknown. Due to difficulty in imaging cannabis and psycho-stimulant dependent individuals with history of psychosis under medication treatment, no baseline imaging measures were taken. These patients underwent psychiatric assessment and brain imaging after treatment. We hypothesized that abstinent cannabis users after recovery from cannabis-induced psychosis would show comparable dopamine D2 availability in the striatum to abstinent MDMA “ecstasy” abusers after 4–6 months of recovery and healthy control participants.
Seventeen in-patient and 8 control participants were recruited for this study. This study was approved by the Institutional Review Board of Tel Aviv Sourasky Medical Center in Israel and informed consent was obtained from all participants. Participants were excluded for psychiatric disorders such as attention deficit hyperactivity disorder, taking medications that affect the CNS, neurological damage, infection that might the affect CNS (HIV, syphilis, and herpes), pregnancy or age under 18 years. All participants fulfilled the criterion of drinking less than 2 standard units of alcohol a day, drinking less than 3 cups of coffee a day and having a body mass index between 18.5 and 25, based on self-reports.
The group consisted of eight cannabis-dependent users, six males and two females with mean age 23 years and 4 months (S.D = 1.03) fulfilling DSM-IV (32) with diagnosis of substance-induced psychotic disorder (SIPD). They were treated with anti-psychotic medication and psychosocial support for 4 months in an inpatient treatment center. Their psychosis lasted on average for 1 month (S.D = 0.53). All participants used cannabis regularly before their psychosis. Five of them have also occasionally used psycho-stimulants such as MDMA, LSD and psilocybin but according to self-reports, they have not used psycho-stimulants during the month before their psychosis. All participants were in remission from substance induced psychosis. Psychotic symptoms were measured by a Psychiatrist. They were scanned between 2012 and 2016.
Nine abstinent ex MDMA “ecstasy” abusers, eight males and one female with mean age 25 years (S.D = 3.5). They fulfilled DSM-IV (32) diagnosis of substance abuse and dependence without substance-induced psychotic disorder (SUD). The abstinent MDMA “ecstasy” abusers took part in our earlier study (33) and underwent the same recruitment and assessment procedure as the main group of cannabis users who recovered from cannabis-induced psychosis and the same imaging procedure in the same scanner SPECT (Hawkeye, GE Healthcare). All participants used MDMA “ecstasy” regularly before treatment. According to their self-report they also used LSD, psilocybin, amphetamines and inhalants but they have not regularly used cocaine or heroin (see Table 1). They were not taking medication during scanning.
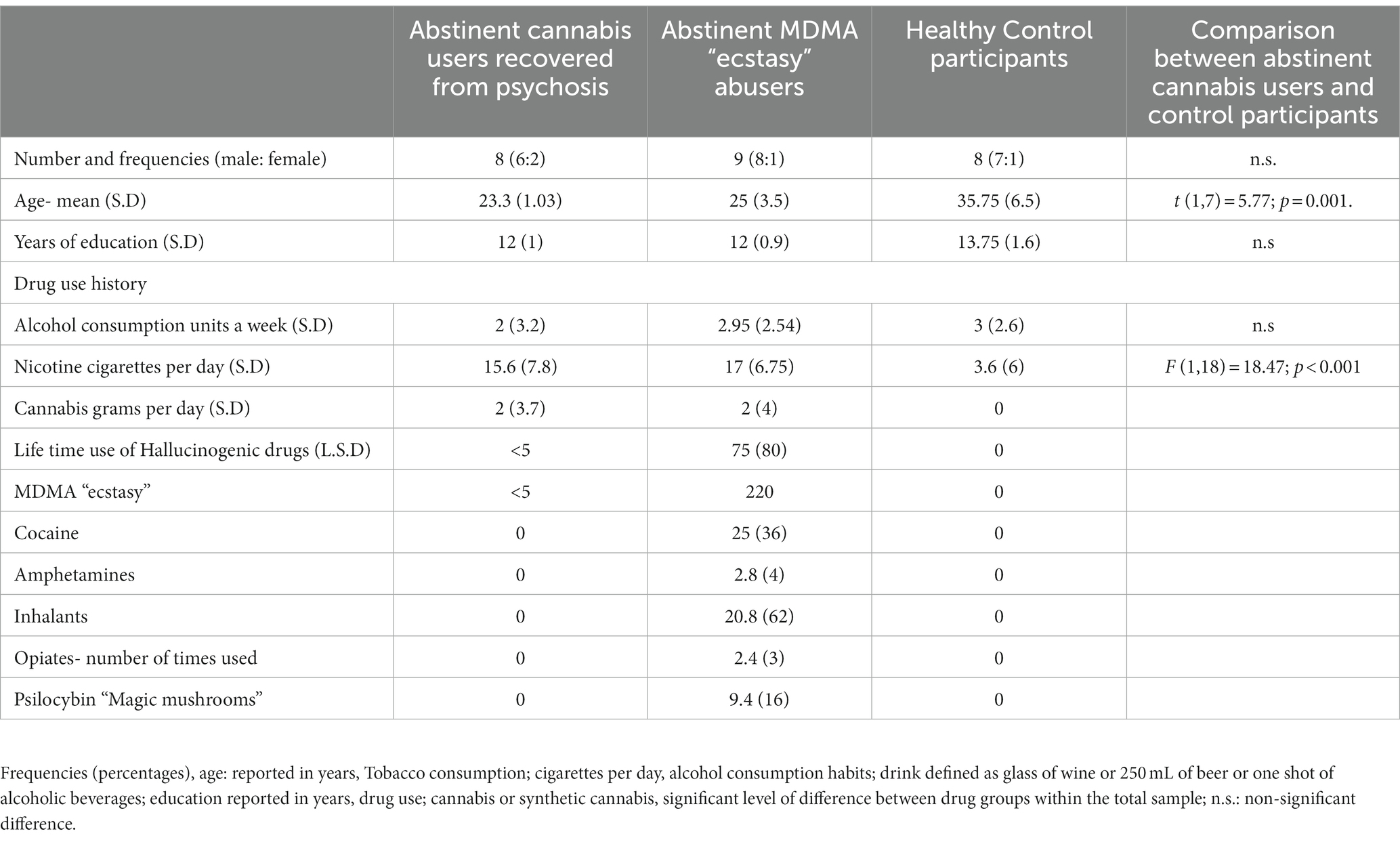
Table 1. Demographic and participants characteristics for each group.
The control group consisted of eight healthy drug-free (based on self-report) participants, seven males and one female with mean age 35 years and 9 months (S.D = 6.5). They took part in our earlier study (33) and underwent the same recruitment and assessment procedure as the main group of cannabis users who recovered from cannabis-induced psychosis and the same imaging procedure in the same scanner SPECT (Hawkeye, GE Healthcare).
The demographic questionnaire included items on education level, age, and gender, use of psychoactive substances like cannabis and MDMA “ecstasy,” LSD and psilocybin, as well as tobacco, and alcohol.
The Beck Depression Inventory (BDI) is a self-reported inventory measuring symptoms of depression (34). The inventory includes 21 items, each item is rated on a scale from 0 to 4 and a total score is computed by summing the items. The BDI demonstrates high internal consistency, with Cronbach internal reliability of α = 0.86 and 0.81 for psychiatric and non-psychiatric populations, respectively (35).
The Spielberger State–Trait Anxiety Inventory (STAI) is self-reported 40 items questionnaire; 20 items of trait anxiety inventory (A- Trait) and 20 items of state anxiety inventory (A-State) (36). Scores on a Likert scale range from 1 “not at all” to 4 “agree very much.” Total score is computed by summing the items, higher scores indicate greater trait or state anxiety. The STAI had been validated with average Cronbach internal reliability of α =0.88 (36).
Treatment of the main group included two sessions a week of individual psychotherapy, one family therapy session a week and daily sessions of group psychotherapy.
Cannabis users who were treated for cannabis-induced psychosis received pharmacological treatment by a Psychiatrist. They were treated with anti-psychotic medication- Risperidone 3–4 mg per day, Olanzapine 20 mg per day, 1 patient received Lithium 300–600 mg per day, and 2 patients received Clonazepam 0.5 mg per day. Medication was reduced gradually during treatment in accordance with patients’ recovery. A month after cessation of anti-psychotic medication the SPECT scan was performed. Time since last use of cannabis was between 4 and 6 months. Five of the abstinent MDMA “ecstasy” abusers were treated with antidepressant medication (Sertraline, Venlafaxine, Fluoxetine and Escitalopram) and six of them were treated with relaxants (Clonazepam and Diazepam). They were treated with medication and psychosocial support for 4 months in an inpatient treatment centers for drug users. All patients were scanned a month after treatment when they were not taking medication and they were abstinent from drugs based on urine samples. The month after treatment time-point was in order to ensure that there are no residual medication effects that may affect scanning. The patients were not symptomatic at the time of scanning and that was verified by a Psychiatrist.
All participants have filled in a consent form a week before the study. They have fasted for 2 h in the morning before scanning. In the morning of the study they have received Iodine (Lugol). Participants have been admitted to the hospital ward at 10 am. They were not allowed to eat or drink anything but water and they were allowed to go to the bathroom when needed. Starting at 10:30 a.m., they received a bolus injection of 5–6 mCi of [123I] IBZM in Single Photon Computed Tomography (SPECT) (Hawkeye, GE Healthcare), followed by constant infusion of 5–6 mCi of [123I] IBZM (1.7–2 mCi/h). for 3 hours while resting on a hospital bed and another 50 min during baseline scan following procedure described by Laruelle et al. (37).
[123I] IBZM with specific activity >5,000 Ci/mmol and radiochemical purity >95% supplied by Eldan Medical equipment. [123I] IBZM is a dopamine D2 antagonist radiotracer for imaging dopamine in vivo in SPECT. The protocol of administration (bolus plus constant infusion) induces a state of sustained binding equilibrium in the absence of pharmacological or behavioral challenge (38). After a baseline SPECT scan in which constant infusion was maintained they returned to their room and were released from the study.
All groups of participants underwent the same image analysis procedure reported by Weinstein (33). A measure of dopamine receptor availability binding potential (BPND) can be calculated by the equation BPND = (S−O)/O where S and O are activity concentrations in the striatum and occipital cortex, respectively, under equilibrium conditions (37). All images were registered and normalized to an IBZM template (39) using the pre-processing tools of Statistical Parametric Mapping (SPM),1 implemented on a Matlab platform. Volume of interest (VOI) analysis image comparisons were performed using the MarsBaR tool within SPM2 described in Tzourio-Mazoyer et al. (40). VOIs, including the putamen, caudate nucleus, and the occipital lobe of each image were defined on the decay-corrected [123IBZM] images. For each scan acquisition, alignment of the image frames was checked. Since only minimal head movements were observed over the acquisitions, no correction for movement was performed. The binding potential (BPND) described above was then calculated for right and left side caudate and putamen for each patient scan.
A second volume of interest (VOI) analysis was performed using the Xeleris software of GE. SPECT data were analyzed blind to the diagnosis. Count projections were pre-filtered using the Wiener 0.5 filter. The four slices with the highest striatal uptake were summed and were attenuation-corrected using the Chang method of attenuation correction. Standard region of interest templates of the striatum and occipital cortex were used as described by Lokkegaard et al. (41). Striatal specific binding was calculated as the ratio described earlier. Since the results using SPM were more accurate and reproducible the second analysis of VOI will not be presented here.
[123I] IBZM SPECT imaging using the bolus injection and a single scan at 90 min post injection is a reproducible method showing acceptable test–retest variability and reliability (42). A comparison of striatal D2 receptor occupancy measured by [123I] IBZM SPECT or [11C] raclopride binding potential in treated schizophrenic patients showed that although anatomical resolution was superior in PET, D2 availability almost perfectly correlated between both methods (43).
Measures of BPND for right and left side caudate and putamen for each scan were calculated using paired one-way ANOVA tests.
One female patient who recovered from psychosis was excluded from analysis due to abnormally low binding potential BPND measures. Table 1 describes demographic data and drug use history in all participants.
Abstinent cannabis users scored on STAI (A- Trait) = 38.13 (SD = 10.92), STAI (A- State) = 37.88 (S.D = 12.25) BDI = 7.88 (S.D = 7.86). Control participants scored on STAI (A- Trait) = 37.88 (S.D = 12.25) STAI (A- State) = 34.25 (S.D = 8.06) BDI = 3.25 (S.D = 4.72). There was no significant difference between the abstinent cannabis users and the healthy control participants group in STAI t (1, 14) = 1.61; p = n.s SSAI t (1, 14) = 0.855; p = n.s or BDI scores t (1, 14) = 1.6; p = N.S. There was no significant difference between the abstinent cannabis users and abstinent “ecstasy” abusers in STAI t (1, 14) = 0.68; p = 0.52 SSAI t (1, 14) = 0.976; p = 0.36 or BDI scores t (1, 14) = 1.17; p = 0.28. The groups showed no significant difference in alcohol consumption measures but both abstinent groups smoked nicotine cigarettes per day more than control participants.
Table 2 shows binding potential BPND measures in all participants.
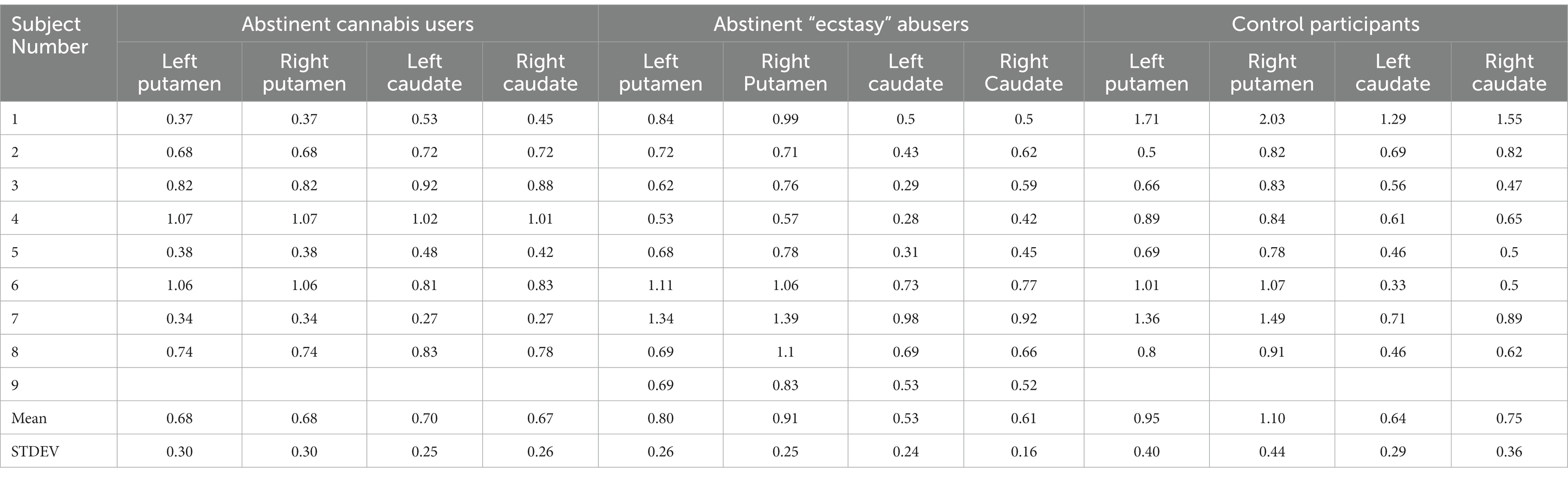
Table 2. Dopamine D2 receptor binding potential (BPND) measures in abstinent cannabis users, abstinent MDMA “ecstasy” abusers and healthy control participants.
Table 3 shows comparisons between in D2 binding potential BPND measures in the caudate and putamen in all participants. There were no differences in dopamine D2 receptor availability in the caudate between abstinent cannabis users compared with abstinent MDMA “ecstasy” abusers and healthy control participants. Using a simple comparison with one-way ANOVA, abstinent cannabis users had lower right putamen BPND measures compared with control participants F (1, 14) = 4.80, *p = 0.046. When comparing abstinent cannabis users with abstinent MDMA “ecstasy” abusers and healthy control participants using one-way ANOVA with Bonferroni corrections the difference has become non-significant F (2, 23) = 2.91 p = 0.076. When comparing the cannabis group with abstinent MDMA “ecstasy” abusers and healthy control participants using one-way ANOVA with Bonferroni corrections none of the other areas have shown significant group differences: Left putamen F (2, 23) = 1.345, p = 0.28, Left caudate F (2, 23) = 0.86, p = 0.44, Right caudate F (2, 23) = 0.497, p = 0.62.
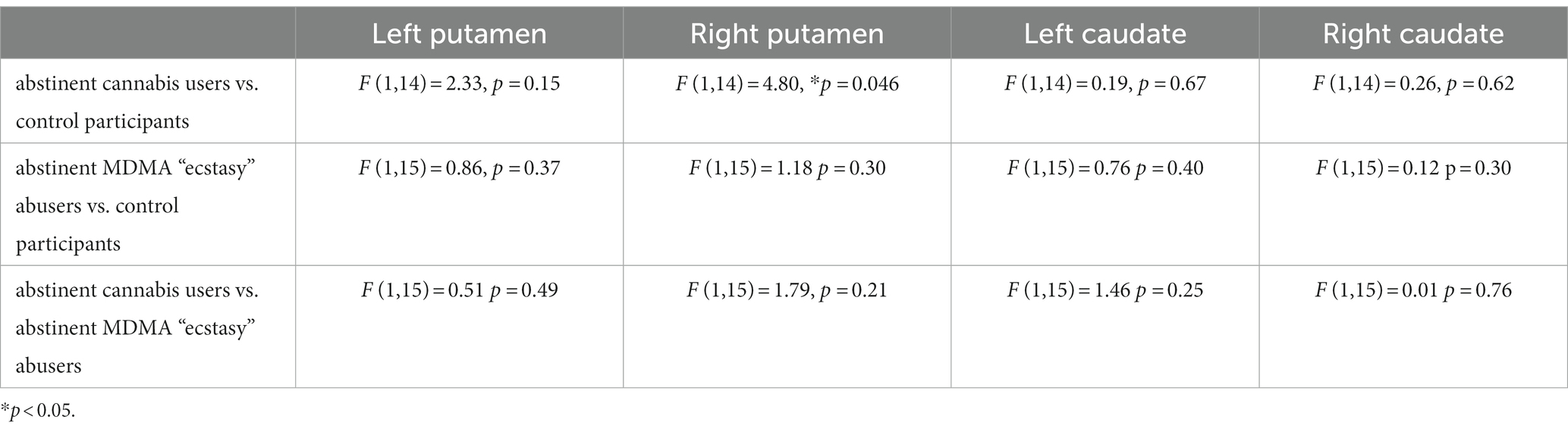
Table 3. A comparison of D2 binding potential BPND measures in the Caudate and putamen (left and right) between abstinent cannabis users after recovery from psychosis, abstinent drug users and healthy control participants (one-way ANOVA).
Dopamine D2 availability was within normal range of 0.3–2.5 (44).
Figure 1 shows D2 binding potential BPND measures in the striatum (left and right caudate and putamen) in all participants.
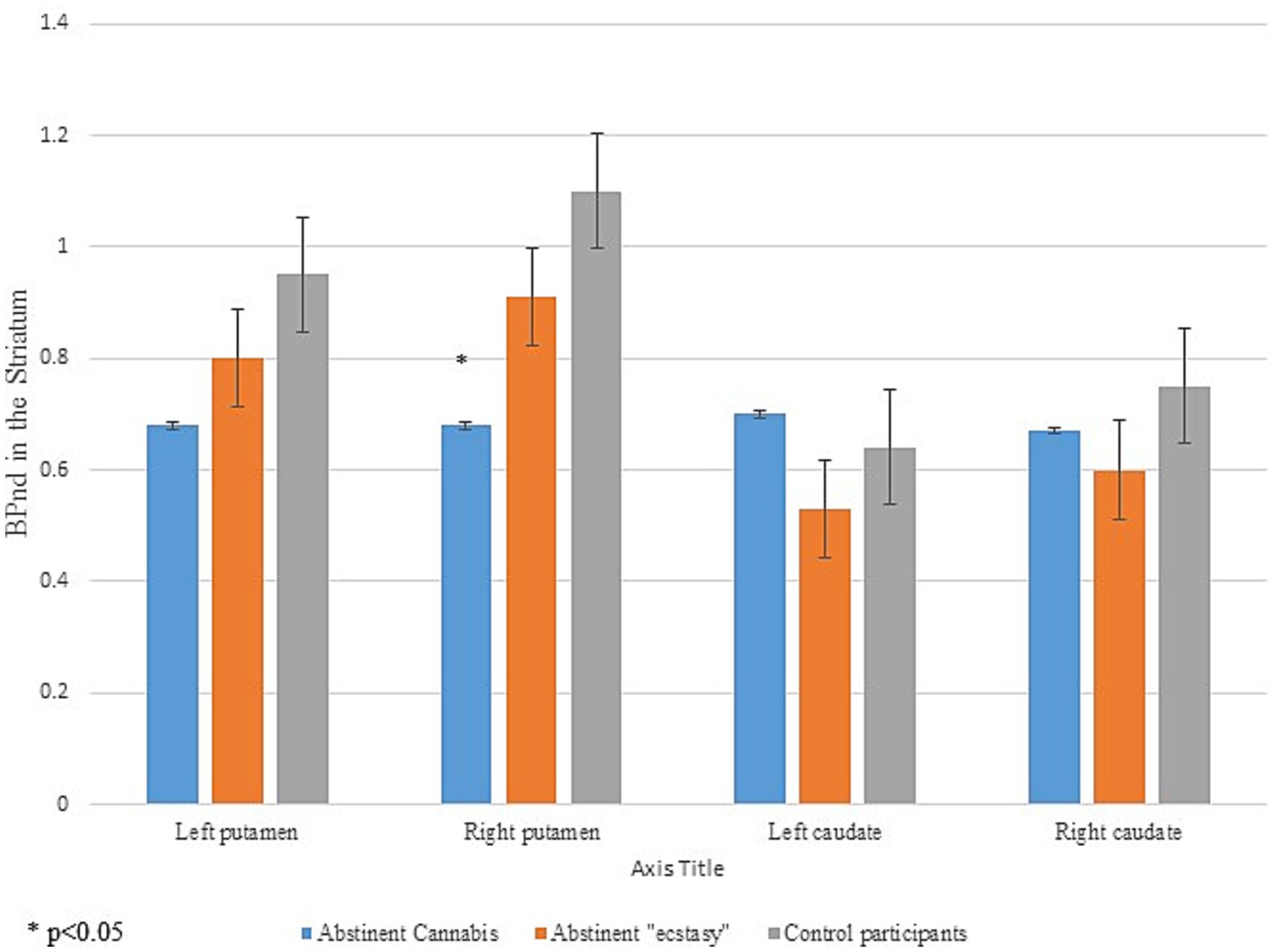
Figure 1. Dopamine receptor D2 binding potentials in the striatum in all participants.
There is a controversy whether using cannabis regularly is posing a risk for psychotic disorders. Adolescent cannabis use was associated with psychosis in a longitudinal study (5). This association could be explained by causality, interactions between genes and environment, shared etiology, or self-medication (45, 46). The age of the beginning of cannabis use correlated with the age at onset of psychosis (45, 47, 48). Also, individuals who used cannabis frequently during adolescence were at greater risk for psychosis and schizophrenia (47, 49–53). Cannabis use is estimated to increase the risk of schizophrenia particularly among those using high THC potency (49, 54).
There are several possible biological mechanisms that may underlie cannabis induced-psychosis. The dopaminergic system has been for a long time considered to play an important role in psychotic disorders, but there is increasing evidence that the cannabinoid system may also be involved. High levels of anandamide, an endogenous cannabinoid agonist, were detected in the cerebrospinal fluid of persons with schizophrenia (55). Additionally, persons with schizophrenia had a greater density of CB1 receptors in the prefrontal cortex than control participants (55). Cannabis use interacts with the dopamine catechol-O-methyl transferase (COMT) Val158Met polymorphism (56). Finally, regular cannabis use exacerbated the symptoms among recent onset cases of schizophrenia (57, 58). However, most cannabis users do not develop schizophrenia. Cannabis may initiate psychotic symptoms in individuals with genetic vulnerability and family history of mental illness, and this may cause concern among healthcare professionals.
We report the first study to the best of our knowledge that has assessed dopamine D2 receptor availability in abstinent cannabis dependent individuals who recovered from cannabis-induced psychosis. Their measures of D2 receptor availability in the caudate were not different between abstinent MDMA “ecstasy” abusers and healthy control participants. This evidence is compatible with previous studies measuring D2 receptor availability in recovered cannabis-dependent users. The length of abstinence of participants was 15 weeks (25), 4 weeks (27) and 18 months (26). Most of the imaging evidence (dopamine imaging and other methods) points to normalization of function following abstinence and so these findings are entirely in keeping with that literature. However, we have used a different methodology from previous studies by using a different radio ligand and scanner (IBZM in SPECT vs. [11C] raclopride in PET). Furthermore, our patients were tested after recovery from cannabis-induced psychosis whereas previous studies included current cannabis users.
The lack of differences in D2 receptor availability may be due to abstinence and the adaptive changes that occur after a prolonged period of abstinence. Stokes et al. (59) argued that cannabis use history is not related to changes in striatal dopamine D2 receptor availability. Urban et al. (27) maintained that the effects of THC are mediated by the endocannabinoid system and that striatal DA neurotransmission is not changed in cannabis dependence. This is supported by evidence for a reversal or normalization of CB1 receptor within a few weeks of abstinence in chronic cannabis users, using the novel CB1 receptor-selective radio ligand [18F] FMPEP-d2 in PET (60). Alternatively, differences in striatal DA transmission in cannabis users compared with healthy control participants may have resolved during the abstinence phase as shown in our study.
Our findings are compatible with those reported by Bloomfield et al. (61) of no association between cannabis-induced psychotic symptoms and dopamine synthesis capacity. Furthermore, striatal dopamine release was reduced after amphetamine challenge in cannabis users (62, 63), although these studies reported reduced dopamine release in active cannabis users. Likewise, Leroy et al. (64) reported reduced DAT availability in cannabis users and Albrecht et al. (65) showed that D2 receptor availability was associated with current cannabis use. These findings as well suggest that reduced dopamine activity depends on active cannabis use.
Barkus et al. (24) showed that positive and general symptoms on the Positive and Negative Syndrome Scale (PANSS) increased at 30 min following THC administration THC has not induced dopamine release in the striatum measured with 123I-iodobenzamide ([123I] IBZM) in SPECT. Secondly, positive psychotic symptoms and DA release were unrelated. They argued that their findings do not support a central role for striatal DA in THC-elicited psychosis. Their results are contrary to the results of two studies that showed significant dopamine release following THC ingestion in healthy volunteers. THC reduced [11C] raclopride binding the ventral striatum and the pre-commissural dorsal putamen but not in other striatal sub-regions in healthy participants in PET (9). THC administration also induced a significant reduction in [11C] raclopride binding in the limbic striatum in a large group of healthy volunteers (8). Although THC induces an increase in dopamine release in the striatum, it is not known precisely how cannabis induces psychotic symptoms. It is plausible that these symptoms are a result of cannabis-induced dopamine dysregulation (10) or its effects on CB1 receptors, Glutamate or GABA.
Previous studies showed the effects of anti-psychotic treatment on the putamen. Farde et al. (66) reported that clinically effective doses of chemically distinct neuroleptic drugs result in 85 to 90 percent occupancy of D2 dopamine receptors in the putamen of schizophrenic patients using [11C] raclopride in PET. These findings indicate that the effects of anti-psychotic medication during treatment of cannabis-induced psychosis may have been evident in the putamen. It is plausible that these effects extended beyond the 3 months of treatment and hence the reduced availability of D2 in the right putamen after recovery in our study.
This study also showed comparable D2 availability in the caudate and putamen measures in abstinent MDMA “ecstasy” abusers and healthy control participants. MDMA (“ecstasy”) operates through its binding affinity to the serotonin receptors (67). MDMA also binds to the serotonin transporter (SERT), thus prolonging signaling at the synapses. Little is known about the effects of chronic MDMA ‘ecstasy” use on the dopamine reward mechanisms in humans.
Recent studies have shown that use of highly potent and rewarding novel psychoactive substances (NPS) is associated with high rates of psychosis and 25% of first-episode psychoses are substance-induced psychosis (68). Ricci et al. (69) have reported that first-episode psychotic patients (FEPp) using cannabis showed higher levels of positive symptoms, dissociative experiences and worse function than their non-user counterpart, which persist after 8 months. Ricci et al. (70) have reported that THC-users, especially synthetic cannabinoid users (SCs) showed more severe positive symptoms than non-users and worse recovery after 9 months. Martinotti et al. (68) have proposed a new diagnosis of substance-related exogenous psychosis (SREP) which refers to both transient and persistent psychoses associated with substance use which is distinct from schizophrenia. Finally, there is evidence that rTMS can be effective in the treatment of addiction, with promising results in treatment of cocaine, and cannabis use disorder (71). Future studies could examine the use of rTMS in treatment of patients with cannabis use disorder and those with cannabis-induced psychosis.
First, this study is a cross-sectional study hence it is not possible to ascertain directly recovery from cannabis induced psychosis and the effects of medication on the brain’s dopamine D2 receptor availability. Secondly, no baseline measures of D2 receptor availability were taken since cannabis users were admitted in an acute psychotic state when it was not possible for scanning. Although all patients were assessed by a Psychiatrist, during treatment and recovery, no measures of psychotic symptoms are available. Third, both abstinent groups were younger than the control group and smoked more nicotine cigarettes per day and that may have affected the results. Furthermore, there is absence of a qualitative assessment of the study and image realignment correction was not performed. Our analysis methods were not able to use sub-divisions of the striatum for image analysis (apart from caudate-putamen). Finally, this was a relatively small sample of participants due to major difficulties recruiting and scanning patients who were treated for cannabis-induced psychosis and “ecstasy” abusers. According to our power calculations 15 participants in each group would be required in order to provide definite results. Unfortunately, most studies that measured dopamine occupancy in cannabis use disorder have used a smaller number of participants which is a limitation in these kind of studies due to recruitment issues.
This study showed no difference in dopamine D2 receptor availability in the caudate between the abstinent cannabis users after recovery from cannabis-induced psychosis, abstinent MDMA “ecstasy” abusers and healthy control participants indicating minimal effects of cannabis-induced psychosis and chronic MDMA “ecstasy” abuse on dopamine reward mechanisms. Due to the small number of patients there is a possibility of type 2 error and the results should be regarded as preliminary and require further replication in larger samples. The findings suggest that remission of cannabis-induced psychosis is not associated with hyper-dopaminergic activity. This could either be because it has resolved. The lower D2 receptor availability measures in the right putamen (uncorrected) may indicate residual effect of anti-psychotic medication.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Tel Aviv Sourasky Medical Center, Tel Aviv Israel. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
The author confirms being the sole contributor of this work and has approved it for publication.
The study was funded by a grant from the Israeli Anti-Drug Authority to AW.
We would like to thank Nanette Freedman for analyzing the brain imaging data, Einat Even-Sapir and Hedva Lerman from Sourasky Medical Center Tel Aviv in Israel for performing the imaging procedure and clinical responsibility, Omri Frisch from Kfar Izun treatment center Ceasaria Israel for providing access to patients.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Radhakrishnan, R, Wilkinson, ST, and D'Souza, DC. Gone to pot - a review of the association between Cannabis and psychosis. Front Psych, 22. (2014) 5:54. doi: 10.3389/fpsyt.2014.00054. eCollection 2014
2. Ranganathan, M, Skosnik, PD, Gupta, S, Cahill, J, Cortes-Briones, J, Sherif, M, et al. Cannabinoids and psychosis. Curr Pharm Des. (2016) 22:6380–91. doi: 10.2174/1381612822666160826105628
3. Hall, W. Is cannabis use psychotogenic? Lancet. (2006) 367:193–5. doi: 10.1016/S0140-6736(06)68012-4
4. Henquet, C, and Van Os, J. The coherence of the evidence linking cannabis with psychosis. Psychol Med. (2008) 38:461-2; author reply 462-4. doi: 10.1017/S0033291707002279
5. Henquet, C, Krabbendam, L, Spauwen, J, Kaplan, C, Lieb, R, Wittchen, HU, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ. (2005) 330:11. doi: 10.1136/bmj.38267.664086.63
6. Pisanu, A, Acquas, E, Fenu, S, and Di Chiara, G. Modulation of Delta(9)-THC induced increase of cortical and hippocampal acetylcholine release by microopioid and D(1) dopamine receptors. Neuropharmacology. (2006) 50:661–70. doi: 10.1016/j.neuropharm.2005.11.023
7. Verrico, CD, Jentsch, JD, and Roth, RH. Persistent and anatomically selective reduction in prefrontal cortical dopamine metabolism after repeated intermittent cannabinoid administration to rats. Synapse. (2003) 49:61–6. doi: 10.1002/syn.10215
8. Bossong, MG, Mehta, MA, Berckel, BN, Howes, OD, Kahn, RS, and Stokes, PR. Further human evidence for striatal dopamine release induced by administration of ∆9-tetrahydrocannabinol (THC): selectivity to limbic striatum. Psychopharmacol (Berl). (2015) 232:2723–9. doi: 10.1007/s00213-015-3915-0
9. Bossong, MG, van Berckel, BN, Boellaard, R, Zuurman, L, Schuit, RC, Windhorst, AD, et al. Delta 9-tetrahydrocannabinol induces dopamine release in the human striatum. Neuropsychopharmacology. (2009) 34:759–66. doi: 10.1038/npp.2008.138
10. Kuepper, R, Morrison, PD, van Os, J, Murray, RM, Kenis, G, and Henquet, C. Does dopamine mediate the psychosis-inducing effects of cannabis? A review and integration of findings across disciplines. Schizophrenia Res. (2010) 121:107–17. doi: 10.1016/j.schres.2010.05.031
11. Sherif, M, Radhakrishnan, R, D'Souza, DC, and Ranganathan, M. Human laboratory studies on cannabinoids and psychosis. Biol Psychiatry. (2016) 79:526–38. doi: 10.1016/j.biopsych.2016.01.011
12. Volkow, ND, Swanson, JM, Evins, AE, DeLisi, LE, Meier, MH, Gonzalez, R, et al. Effects of Cannabis use on human behavior, including cognition, motivation, and psychosis: a review. JAMA Psychiatry. (2016) 73:292–7. doi: 10.1001/jamapsychiatry.2015.3278
13. Hindley, G, Beck, K, Borgan, F, Ginestet, CE, McCutcheon, R, Kleinloog, D, et al. Psychiatric symptoms caused by cannabis constituents: a systematic review and meta-analysis. Lancet Psychiatry. (2020) 7:344–53. doi: 10.1016/S2215-0366(20)30074-2
14. D'Souza, DC, Perry, E, MacDougall, L, Ammerman, Y, Cooper, T, Wu, YT, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. (2004) 29:1558–72. doi: 10.1038/sj.npp.1300496
15. Morrison, PD, Zois, V, McKeown, DA, Lee, TD, Holt, DW, Powell, JF, et al. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. (2009) 39:1607–16. doi: 10.1017/S0033291709005522
16. Colizzi, M, Ruggeri, M, and Bhattacharyya, S. Unraveling the intoxicating and therapeutic effects of Cannabis ingredients on psychosis and cognition. Front Psychol. (2020) 11:833. doi: 10.3389/fpsyg.2020.00833
17. Appiah-Kusi, E, Wilson, R, Colizzi, M, Foglia, E, Klamerus, E, Caldwell, A, et al. Childhood trauma and being at-risk for psychosis are associated with higher peripheral endocannabinoids. Psychol Med. (2020) 50:1862–71. doi: 10.1017/S0033291719001946
18. Fusar-Poli, P, Borgwardt, S, Bechdolf, A, Addington, J, Riecher-Rössler, A, Schultze-Lutter, F, et al. The psychosis high-risk state: a comprehensive state-of-the-art review. JAMA Psychiatry. (2013) 70:107–20. doi: 10.1001/jamapsychiatry.2013.269
19. Borgan, F, Laurikainen, H, Veronese, M, Marques, TR, Haaparanta-Solin, M, Solin, O, et al. In vivo availability of cannabinoid 1 receptor levels in patients with first-episode psychosis. JAMA Psychiatry. (2019) 76:1074–84. doi: 10.1001/jamapsychiatry.2019.1427
20. Borgan, F, Kokkinou, M, and Howes, O. The cannabinoid CB1 receptor in schizophrenia. Biol Psychiatry: Cogn Neurosci Neuroimaging. (2021) 6:646–59. doi: 10.1016/j.bpsc.2020.06.018
21. D'Souza, DC, Sewell, RA, and Ranganathan, M. Cannabis and psychosis/schizophrenia: human studies. Eur Arch Psychiatry Clin Neurosci. (2009) 259:413–31. doi: 10.1007/s00406-009-0024-2
22. Howes, OD, and Shatalina, E. Integrating the neurodevelopmental and dopamine hypotheses of schizophrenia and the role of cortical excitation-inhibition balance. Biol Psychiatry. (2022) 92:513. doi: 10.1016/j.biopsych.2022.06.017
23. Bloomfield, MA, Ashok, AH, Volkow, ND, and Howes, OD. The effects of Δ9-tetrahydrocannabinol on the dopamine system. Nature. (2016) 539:369–77. doi: 10.1038/nature20153
24. Barkus, E, Morrison, PD, Vuletic, D, Dickson, JC, Pilowsky, LS, Brenneisen, R, et al. Does intravenous Δ9-tetrahydrocannabinol increase dopamine release? A SPET study. J Psychopharmacol. (2011) 25:1462–8. doi: 10.1177/0269881110382465
25. Sevy, S, Smith, GS, Ma, Y, Dhawan, V, Chaly, T, Kingsley, PB, et al. Cerebral glucose metabolism and D2/D3 receptor availability in young adults with cannabis dependence measured with positron emission tomography. Psychopharmacol (Berlin). (2008) 197:549–56. doi: 10.1007/s00213-008-1075-1
26. Stokes, PR, Mehta, MA, Curran, HV, Breen, G, and Grasby, PM. Can recreational doses of THC produce significant dopamine release in the human striatum? NeuroImage. (2009) 48:186–90. doi: 10.1016/j.neuroimage.2009.06.029
27. Urban, NB, Slifstein, M, Thompson, JL, Xu, X, Girgis, RR, Raheja, S, et al. Dopamine release in chronic cannabis users: a [(11)C] raclopride positron emission tomography study. Biol Psychiatry. (2012) 71:677–83. doi: 10.1016/j.biopsych.2011.12.018
28. Abi-Dargham, A, Gil, R, Krystal, J, Baldwin, RM, Seibyl, JP, Bowers, M, et al. Increased striatal dopamine transmission in schizophrenia: confirmation in a second cohort. Am J Psychiatry. (1998) 155:761–7. doi: 10.1176/ajp.155.6.761
29. Demjaha, A, Murray, RM, McGuire, PK, Kapur, S, and Howes, OD. Dopamine synthesis capacity in patients with treatment-resistant schizophrenia. Am J Psychiatry. (2012) 169:1203–10. doi: 10.1176/appi.ajp.2012.12010144
30. Jauhar, S, Veronese, M, Nour, MM, Rogdaki, M, Hathway, P, Turkheimer, FE, et al. Determinants of treatment response in first-episode psychosis: an 18F-DOPA PET study. Mol Psychiatry. (2019) 24:1502–12. doi: 10.1038/s41380-018-0042-4
31. McCutcheon, RA, Jauhar, S, Pepper, F, Nour, MM, Rogdaki, M, Veronese, M, et al. The topography of striatal dopamine and symptoms in psychosis: an integrative positron emission tomography and magnetic resonance imaging study. Biol Psychiatry Cogn Neurosci Neuroimaging. (2020) 5:1040–51. doi: 10.1016/j.bpsc.2020.04.004
32. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association (1994).
33. Weinstein, A. Computer and video game addiction. Am J Drug Alcohol Abuse. (2010) 36:268–76. doi: 10.3109/00952990.2010.491879
35. Beck, AT, Steer, RA, and Garbin, MG. Psychometric properties of the Beck depression inventory: twenty-five years of evaluation. Clin Psychol Rev. (1988) 8:77–100. doi: 10.1016/0272-7358(88)90050-5
36. Spielberger, CD, Gorsuch, RL, Lushene, R, Vagg, PR, and Jacobs, GA. Manual for the state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologists Press (1983).
37. Laruelle, M, Abi-Dargham, A, Van Dyck, CH, Rosenblatt, W, Zea-Ponce, Y, Zoghbi, SS, et al. SPECT imaging of striatal dopamine release after amphetamine challenge. J Nucl Med. (1995) 36:1182–90.
38. Laruelle, M, Abi-Dargham, A, Van Dyck, CH, Gil, R, D’Souza, CD, Erdos, J, et al. Single photon emission computerised tomography imaging of amphetamine-induced dopamine release in drug-free schizophrenic subjects. Proc Natl Acad Sci U S A. (1996) 93:9235–40. doi: 10.1073/pnas.93.17.9235
39. Buchert, R, Berding, G, Wilke, F, Martin, B, von Borczyskowski, D, Mester, J, et al. IBZM tool: a fully automated expert system for the evaluation of IBZM SPECT studies. Eur J Nuc Med Mol Imaging. (2006) 33:1073–83. doi: 10.1007/s00259-006-0067-9
40. Tzourio-Mazoyer, N, Landeau, B, Papathanassiou, D, Crivello, F, Etard, O, Delcroix, N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. NeuroImage. (2002) 15:273–89. doi: 10.1006/nimg.2001.0978
41. Lokkegaard, A, Werdelin, LM, and Friberg, L. Clinical impact of diagnostic SPET investigations with a dopamine re-uptake ligand. Eur J Nucl Med. (2002) 29:1623–9. doi: 10.1007/s00259-002-0938-7
42. Catafau, AM, Bullich, S, Danús, M, Penengo, MM, Cot, A, Abanades, S, et al. Test-retest variability and reliability of 123I-IBZM SPECT measurement of striatal dopamine D2 receptor availability in healthy volunteers and influence of iterative reconstruction algorithms. Synapse. (2008) 62:62–9. doi: 10.1002/syn.20465
43. Catafau, AM, Suarez, M, Bullich, S, Llop, J, Nucci, G, Gunn, RN, et al. Within-subject comparison of striatal D2 receptor occupancy measurements using [123I]IBZM SPECT and [11C]Raclopride PET. NeuroImage. (2009) 46:447–58. doi: 10.1016/j.neuroimage.2009.02.005
44. Wulff, S, Pinborg, LH, Svarer, C, Jensen, LT, Nielsen, MØ, Allerup, P, et al. Striatal D(2/3) binding potential values in drug-Naïve first-episode schizophrenia patients correlate with treatment outcome. Schizophr Bull. (2015) 41:1143–52. doi: 10.1093/schbul/sbu220
45. Large, M, Sharma, S, Compton, MT, Slade, T, and Nielssen, O. Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Arch Gen Psychiatry. (2011) 68:555–61. doi: 10.1001/archgenpsychiatry.2011.5
46. Miettunen, J, Törmänen, S, Murray, GK, Jones, PB, Mäki, P, Ebeling, H, et al. Association of cannabis use with prodromal symptoms of psychosis in adolescence. Br J Psychiatry. (2008) 192:470–1. doi: 10.1192/bjp.bp.107.045740
47. Di Forti, M, Sallis, H, Allegri, F, Trotta, A, Ferraro, L, Stilo, SA, et al. Daily use, especially of high-potency cannabis, drives the earlier onset of psychosis in cannabis users. Schizophr Bull. (2014) 40:1509–17. doi: 10.1093/schbul/sbt181
48. Galvez-Buccollini, JA, Proal, AC, Tomaselli, V, Trachtenberg, M, Coconcea, C, Chun, J, et al. Association between age at onset of psychosis and age at onset of cannabis use in non-affective psychosis. Schizophr Res. (2012) 139:157–60. doi: 10.1016/j.schres.2012.06.007
49. Andréasson, S, Allebeck, P, Engström, A, and Rydberg, U. Cannabis and schizophrenia: a longitudinal study of Swedish conscripts. Lancet. (1987) 2:1483–6.
50. Arseneault, L, Cannon, M, Poulton, R, Murray, R, Caspi, A, and Moffitt, TE. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. (2002) 325:1212–3. doi: 10.1136/bmj.325.7374.1212
51. Di Forti, M, Marconi, A, Carra, E, Fraietta, S, Trotta, A, Bonomo, M, et al. Proportion of patients in South London with first-episode psychosis attributable to use of high potency cannabis: a case-control study. Lancet Psychiatry. (2015) 2:233–8. doi: 10.1016/S2215-0366(14)00117-5
52. Di Forti, M, Morgan, C, Dazzan, P, Pariante, C, Mondelli, V, Marques, TR, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry. (2009) 195:488–91. doi: 10.1192/bjp.bp.109.064220
53. Zammit, S, Allebeck, P, Andreasson, S, Lundberg, I, and Lewis, G. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. (2002) 325:1199. doi: 10.1136/bmj.325.7374.1199
54. van Os, J, Bak, M, Hanssen, M, Bijl, RV, de Graaf, R, and Verdoux, H. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. (2002) 156:319–27. doi: 10.1093/aje/kwf043
55. Dean, B, Sundram, S, Bradbury, R, Scarr, E, and Copolov, D. Studies on [3H]CP-55940 binding in the human central nervous system: regional specific changes in density of cannabinoid-1 receptors associated with schizophrenia and cannabis use. Neuroscience. (2001) 103:9–15. doi: 10.1016/s0306-4522(00)00552-2
56. Caspi, A, Moffitt, TE, and Cannon, M. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry. (2005) 57:1117–27. doi: 10.1016/j.biopsych.2005.01.026
57. Degenhardt, L, Tennant, C, and Gilmour, S. The temporal dynamics of relationships between cannabis, psychosis and depression among young adults with psychotic disorders: findings from a 10-month prospective study. Psychol Med. (2007) 37:927–34. doi: 10.1017/S0033291707009956
58. Hides, L, Dawe, S, Kavanagh, DJ, and Young, RM. Psychotic symptom and cannabis relapse in recent-onset psychosis. Prospective study. Br J Psychiatry. (2006) 189:137–43. doi: 10.1192/bjp.bp.105.014308
59. Stokes, PR, Egerton, A, Watson, B, Reid, A, Lappin, J, Howes, OD, et al. History of cannabis use is not associated with alterations in striatal dopamine D2/D3 receptor availability. J Psychopharmacol. (2012) 26:144–9. doi: 10.1177/0269881111414090
60. Hirvonen, J, Goodwin, RS, Li, CT, Terry, GE, Zoghbi, SS, Morse, C, et al. Reversible and regionally selective downregulation of brain cannabinoid CB1 receptors in chronic daily cannabis smokers. Mol Psychiatry. (2012) 17:642–9. doi: 10.1038/mp.2011.82
61. Bloomfield, MA, Morgan, CJ, Egerton, A, Kapur, S, Curran, HV, and Howes, OD. Dopaminergic function in cannabis users and its relationship to cannabis-induced psychotic symptoms. Biol Psychiatry. (2014) 75:470–8. doi: 10.1016/j.biopsych.2013.05.027
62. van de Giessen, E, Weinstein, JJ, Cassidy, CM, Haney, M, Dong, Z, Ghazzaoui, R, et al. Deficits in striatal dopamine release in cannabis dependence. Mol Psychiatry. (2017) 22:68–75. doi: 10.1038/mp.2016.21
63. Volkow, ND, Wang, GJ, Telang, F, Fowler, JS, Alexoff, D, Logan, J, et al. Decreased dopamine brain reactivity in marijuana abusers is associated with negative emotionality and addiction severity. Proc Natl Acad Sci U S A. (2014) 111:E3149–56. doi: 10.1073/pnas.1411228111
64. Leroy, C, Karila, L, Martinot, JL, Lukasiewicz, M, Duchesnay, E, Comtat, C, et al. Striatal and extrastriatal dopamine transporter in cannabis and tobacco addiction: a high-resolution PET study. Addict Biol. (2012) 17:981–90. doi: 10.1111/j.1369-1600.2011.00356.x
65. Albrecht, DS, Skosnik, PD, Vollmer, JM, Brumbaugh, MS, Perry, KM, Mock, BH, et al. Striatal D(2)/D(3) receptor availability is inversely correlated with cannabis consumption in chronic marijuana users. Drug and Alc Dep. (2013) 128:52–7. doi: 10.1016/j.drugalcdep.2012.07.016
66. Farde, L, Wiesel, FA, Halldin, C, and Sedvall, G. Central D2 dopamine receptor occupancy in schizophrenic patients treated with antipsychotic drugs. Arc Gen Psychiatry. (1988) 45:71–6. doi: 10.1001/archpsyc.1988.01800250087012
67. Liechti, ME, Saur, MR, Gamma, A, Hell, D, and Vollenweider, FX. Psychological and physiological effects of MDMA ("ecstasy") after pretreatment with the 5-HT(2) antagonist ketanserin in healthy humans. Neuropsychopharmacology. (2000) 23:396–404. doi: 10.1016/S0893-133X(00)00126-3
68. Martinotti, G, Miuli, A, Stigliano, G, Stigliano, G, Pettorruso, M, and di Giannantonio, M. Transcranial magnetic stimulation to treat substance use disorders and behavioral addictions: the state of the art. Evid Based Psychiatric Care. (2021) 7:40–6. doi: 10.36180/2421-4469-2021-7
69. Ricci, V, Ceci, F, Di Carlo, F, Lalli, A, Ciavoni, L, Mosca, A, et al. Cannabis use disorder and dissociation: a report from a prospective first-episode psychosis study. Drug Alcohol Depend. (2021) 229:109118. doi: 10.1016/j.drugalcdep.2021.109118
70. Ricci, V, Ceci, F, Di Carlo, F, Di Muzio, I, Ciavoni, L, Santangelo, M, et al. First episode psychosis with and without the use of cannabis and synthetic cannabinoids: psychopathology, global functioning and suicidal ideation and antipsychotic effectiveness. Psychiatry Res. (2023) 320:115053. doi: 10.1016/j.psychres.2023.115053
Keywords: cannabis, psychosis, dopamine, D2, SPECT imaging
Citation: Weinstein AM (2023) A brain imaging study of dopamine receptor D2 availability in cannabis dependent users after recovery from cannabis-induced psychosis. Front. Psychiatry. 14:1230760. doi: 10.3389/fpsyt.2023.1230760
Edited by:
Giovanni Martinotti, University of Studies G. d'Annunzio Chieti and Pescara, ItalyReviewed by:
Francesco Maria Semeraro, University of Studies G. d'Annunzio Chieti and Pescara, ItalyCopyright © 2023 Weinstein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aviv M. Weinstein, YXZpdndlQGFyaWVsLmFjLmls
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.