
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 21 August 2023
Sec. Psychopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1210155
This article is part of the Research Topic Insights on Cannabinoid Translational Science and Medicine: The Endocannabinoidome as a Target for Clinical Practice View all 5 articles
 Patrícia Soares Silva Montagner1†
Patrícia Soares Silva Montagner1† Wesley Medeiros2†
Wesley Medeiros2† Leandro Cruz Ramires da Silva3,4Clarissa Nogueira Borges5
Leandro Cruz Ramires da Silva3,4Clarissa Nogueira Borges5 Joaquim Brasil-Neto6
Joaquim Brasil-Neto6 Vinícius de Deus Silva Barbosa7,8
Vinícius de Deus Silva Barbosa7,8 Fabio V. Caixeta2
Fabio V. Caixeta2 Renato Malcher-Lopes2*
Renato Malcher-Lopes2*Autism Spectrum Disorders (ASD) may significantly impact the well-being of patients and their families. The therapeutic use of cannabis for ASD has gained interest due to its promising results and low side effects, but a consensus on treatment guidelines is lacking. In this study, we conducted a retrospective analysis of 20 patients with autistic symptoms who were treated with full-spectrum cannabis extracts (FCEs) in a response-based, individually-tailored dosage regimen. The daily dosage and relative proportions of cannabidiol (CBD) and tetrahydrocannabinol (THC) were adjusted based on treatment results following periodic clinical evaluation. Most patients (80%) were treated for a minimum of 6 months. We have used a novel, detailed online patient- or caregiver-reported outcome survey that inquired about core and comorbid symptoms, and quality of life. We also reviewed patients’ clinical files, and no individual condition within the autistic spectrum was excluded. This real-life approach enabled us to gain a clearer appraisal of the ample scope of benefits that FCEs can provide for ASD patients and their families. Eighteen patients started with a CBD-rich FCE titrating protocol, and in three of them, the CBD-rich (CBD-dominant) FCE was gradually complemented with low doses of a THC-rich (THC-dominant) FCE based on observed effects. Two other patients have used throughout treatment a blend of two FCEs, one CBD-rich and the other THC-rich. The outcomes were mainly positive for most symptoms, and only one patient from each of the two above-mentioned situations displayed important side effects one who has used only CBD-rich FCE throughout the treatment, and another who has used a blend of CBD-Rich and THC-rich FCEs. Therefore, after FCE treatment, 18 out of 20 patients showed improvement in most core and comorbid symptoms of autism, and in quality of life for patients and their families. For them, side effects were mild and infrequent. Additionally, we show, for the first time, that allotriophagy (Pica) can be treated by FCEs. Other medications were reduced or completely discontinued in most cases. Based on our findings, we propose guidelines for individually tailored dosage regimens that may be adapted to locally available qualified FCEs and guide further clinical trials.
Autism spectrum disorders (ASD) are neurodevelopmental conditions characterized by two main symptom domains: (1) restricted or repetitive behaviors and (2) impairment in language/communication and social skills (1–11). ASD is commonly linked to a high burden of comorbid disorders. Symptoms presented by patients in the spectrum vary widely in severity, and may require either minor, substantial, or very substantial support for the patient’s everyday needs (5, 12). Besides the core symptomatic domains associated to ASD, people in the spectrum frequently present co-morbidities and neurodevelopmental disabilities. These include intellectual deficits (13, 14), behavioral problems (15), emotion regulation impairment (16), ingestion of nonfood substances (allotriophagy or PICA) (17–19), among others. All these conditions have considerable impact the patient’s and their families’ quality of life.
A recent systematic review investigated the ASD prevalence from 1993 to 2019, and found that it is currently around 0.8% in Europe, 0.95% in North America and 1.12% in Oceania, indicating a worldwide increase over the last 25 years (20). A more recent study done between 2019 and 2022 revealed a prevalence of 0,33% (1:30) among children and adolescents aged 3 to 17 years old in the United States (21). The continuous demand for a variety of treatments and the frequent lack of independence of severe ASD patients result in significant economic effects. This economic burden affects families of children and adults with ASD, the community in general, and their governments (22). The mental health of parents and caregivers is also impacted, often leading to enduring mood disorders (23).
Conventional treatments for ASD have limited benefits over symptoms related to social interaction, communication, motor function and intellectual development (23, 24). The first line of treatment consists of behavioral therapy and pharmacological interventions with anxiolytics, antidepressants, antipsychotics, mood stabilizers, alfa−2-agonists and psychostimulants (16, 25–38). Those medications may entail severe side effects, such as metabolic and endocrine dysregulation (resulting in weight gain, gynecomastia, and sexual dysfunction), plus extrapyramidal and cardiac side effects (30, 39–46). The only two medications specifically approved by FDA for ASD treatment, Risperidone and Aripiprazole, are antipsychotics indicated for management of aberrant behaviors (47). According to recent systematic reviews, both are effective for the short-term treatment of emotional dysregulation and irritability, but both are also frequently associated with important metabolic side effects (48, 49).
The endocannabinoid system plays a key role in ASD (50–71). Accordingly, recent prospective and retrospective studies of cannabinoid treatment in humans have shown promising results, with some improvements in most core ASD symptoms, as well as in several comorbid symptoms, and infrequent mild side effects (61, 72–78). The number of patients who benefit from the treatment and the level of improvement varies considerably between studies; this might be due to sample diversity and differences in the Cannabis extracts used, posology, outcome evaluation methodology, and treatment time.
The relative composition of cannabidiol (CBD) and Δ9-tetrahydrocannabinol (THC) present in the whole Cannabis sativa oil extracts, also known as full-spectrum Cannabis extracts (FCE) employed, is likely to be another relevant factor for treatment outcome. However, full-spectrum Cannabis extracts have complex and diverse compositions, not unlike the varied forms in which ASD conditions manifest. Henceforth, it is reasonable to speculate that most individual conditions within the autistic spectrum may benefit from a particular Cannabis extract composition and posology–even though some individuals may not benefit from it at all.
While some researchers believe that CBD-rich or pure CBD (CBD-CE) extracts may be the most beneficial for treating core symptoms of ASD (79–81), available data do not conclusively support this, and parameters for the clinical use of cannabinoids in ASD are yet to be established in the scientific literature. To the best of our knowledge, most studies have employed standardized Full-spectrum (whole) Cannabis Extracts (FCE), some with CBD to THC ratio as high as 75:1 (76), and others as low as 6:1 (72), producing some level of symptomatic improvements in both extremes. Studies using intermediary proportions, such as 20:1 (72–75) and 9:1 (78) have also promoted some amelioration of symptoms. It is important to notice, though, that the treatment with higher THC proportion (6:1) resulted in good outcomes for some cases, but led to a higher frequency of cases showing important behavioral side effects (72).
Recently it has been shown that a suitable way to overcome the lack of a well-defined posology is titrating the dosage according to the patient’s response, starting with a very low dose and adjusting it as the effects are observed (77). One study in particular has shown clinical improvements in patients using a varied range of dosages and CBD to THC proportions. In all cases these improvements were confirmed by Cannabis-responsive biomarkers, that moved toward normal, neurotypical values (82). Altogether, these results indicate that some patients may improve with CBD-rich, full-spectrum extracts containing very low THC levels, while others may benefit from a small increase of THC. However, it seems that CBD should be always present in an amount high enough to prevent the psychotomimetic effects of THC, whereas increase of THC, if deemed necessary, should be very slow and limited to the lower effective dose.
In the Brazilian real-life context, due to persistent lack of proper regulatory systems for production, commercialization and access to Cannabis-derived medicine, patients have organized themselves into dozens of civil societies. Those organizations have taken the lead in the process of securing access to Cannabis-based medicine for patients, especially to those who cannot afford the industrial Cannabis-based products currently available in Brazil. Those are either imported as a finished product, or produced in Brazil from imported concentrated extracts, which become very expensive to most of the community. Some of these nonprofit organizations (NPO) have then established their own production of full-spectrum Cannabis extracts with quality control and standardized composition (78).
Here we describe an open label, real-life study with 20 patients who were treated with individualized dose schemes, using one FCE or a blend of two different FCEs of standardized compositions produced by three Brazilian patient societies. Patients received FCE prescription and were treated under the clinical supervision of two authors of this article (P.M. and L.R.). For most patients, the treatment’s dosage followed the same standardized protocol adapted from the current literature and the clinicians’ previous experience, adjusting FCE’s proportions of CBD and THC to find the combination best suited to each patient.
Effects were evaluated using a retrospective outcome survey with parents of patients in the spectrum that assessed the perceived effect of FCE treatment on both core and comorbid symptoms, in a more comprehensive manner than previously reported in the literature. We have evaluated the effects of Cannabis treatment on 10 main different groups of symptoms, plus 9 specific subcategories for abnormal behavior symptoms and 7 specific subcategories for communication and social interaction problems. We also included five additional questions regarding positive mood improvement, side effects, changes in medication use, and general quality of life for both the patients and their families. As such, we hoped to provide a more comprehensive report of FCE’s impact over autism symptoms, accounting for different ASD conditions and extract parameters.
The studies involving human participants were reviewed and approved by the Ethics Committee on Human Research of the Health Sciences College of the University of Brasília (Universidade de Brasília–UnB), under the protocol number CAAE 54241721.5.0000.0030. Written informed consent to participate in this study was provided by every participant and its legal guardian/next of kin. Written informed consent for publishing of data obtained in this study was provided by the participants’ legal guardian/next of kin.
Treatment with FCE was conducted by two of the authors (PM and LS) in the clinical setting. Either during or after the end of each patient’s treatment, parents, or participants (according to the better convenience in each case) were invited to take part in this study. Twenty participants diagnosed with ASD agreed to participate and were enrolled. We are interested in evaluating the benefits of FCE treatment for any condition within the autistic spectrum, therefore the inclusion criterion was ASD diagnosis (ICD 10 = F84.0) previously received by the patients, or given after clinical evaluation by the authors PM or LS. ASD patients treated with FCE for at least 3 months were included. Participation consisted of allowing the disclosure of patient’s clinical records and answering a detailed survey (Supplementary material S1).
In Table 1 we indicate participant’s weights, genders and details of cannabinoid concentrations consumed daily and per kilo. Patients’ gender is identified as male (m) or female (f) numbers throughout the text and figures. In total, 118 families were initially invited to take part in the research, and 24 of those families answered the survey. Out of those, one participant was removed because he had been under less than 3 months of FCE treatment, one participant was removed due to faulty survey answers, and two others were removed because they used CEs that deviated from the scope of this paper. Of note, three of the enrolled patients chose to interrupt the treatment of their own accord: one (2 m) due to worsening of symptoms and two due to financial limitations (7 m, 19 m), but all treatments lasted 3 months or more, and their data was maintained in the analysis. Patient 16 m used a non-full-spectrum, pure CBD product. This was the only case treated throughout with a purified CBD formulation, which was eventually supplemented with THC-rich FCE.
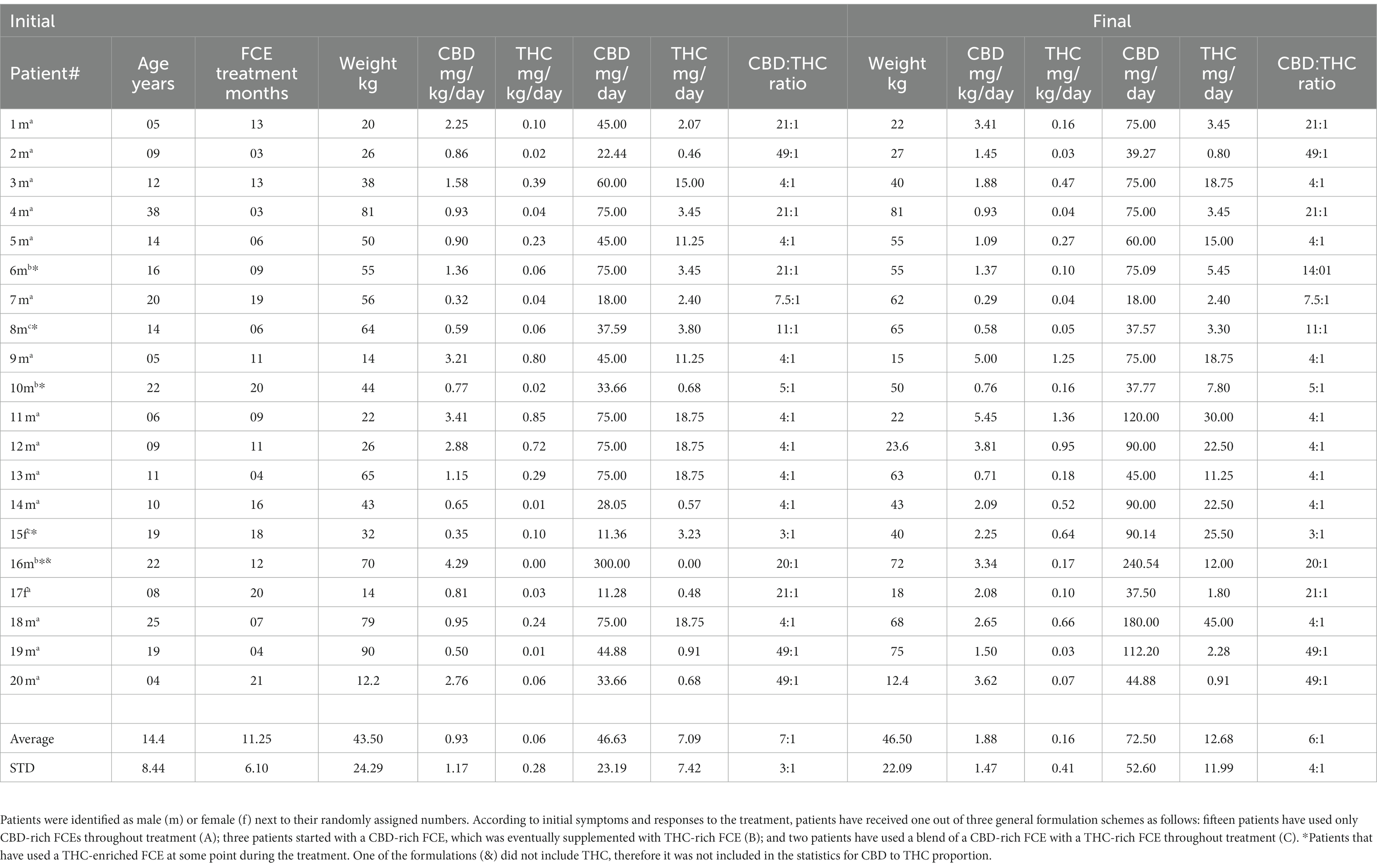
Table 1. Cohort description, weight, and FCE dosage for each patient at the beginning and at the end of treatment.
Most patients received individualized treatments based on a titration protocol, which started with low doses of a CBD-rich FCE. According to the clinical evaluation of observed effects, the dose was slowly increased and could be gradually supplemented by low doses of a THC-rich FCE to improve the results. We define “CBD-rich” FCEs as those in which CBD amount is higher than THC, and “THC-rich” FCEs as those in which THC is the more abundant cannabinoid. The CBD-rich FCEs had a proportion of either 4: 1, 21: 1, 49: 1 or 7: 1 (CBD: THC), whereas THC-rich FCEs had a proportion of either 1: 22 or 1: 4 (CBD: THC, rounded to whole numbers). One exceptional case started treatment with a purified, industrial grade CBD extract (identified in Table 1), but eventually added a FCE rich in THC. Two patients presenting refractory severe behavioral symptoms have used a blend of CBD-rich and THC-rich extracts since the beginning of the treatment. These extracts were produced by three patient organizations, and the specific extracts used by each patient depended on their choice of affiliation to a specific NPO. All extracts were administered orally via drops. Thus, daily doses were varied, changed according to symptoms and side effects presented by the patient during treatment, and eventually stabilized after reaching a consensus between physician and family.
Patients were evaluated monthly for a trimester. Upon symptoms stabilization, they were reevaluated every 6 months. In rare cases weekly reassessments/adjustments were made. Criteria employed for CBD-rich FCE dosage change, or supplementation with THC-rich FCE were: (1) severe cases of psychomotor agitation and aggression with little response to CBD; (2) persistence of complaints regarding sleep pattern and appetite despite otherwise satisfactory response to CBD (More details in Figure 1). Average concentrations at the beginning of treatment were 45 mg/day: 1.94 mg/day (CBD: THC) and 75 mg/day: 2.32 mg/day at the end of treatment, normally administered in two or three daily doses.
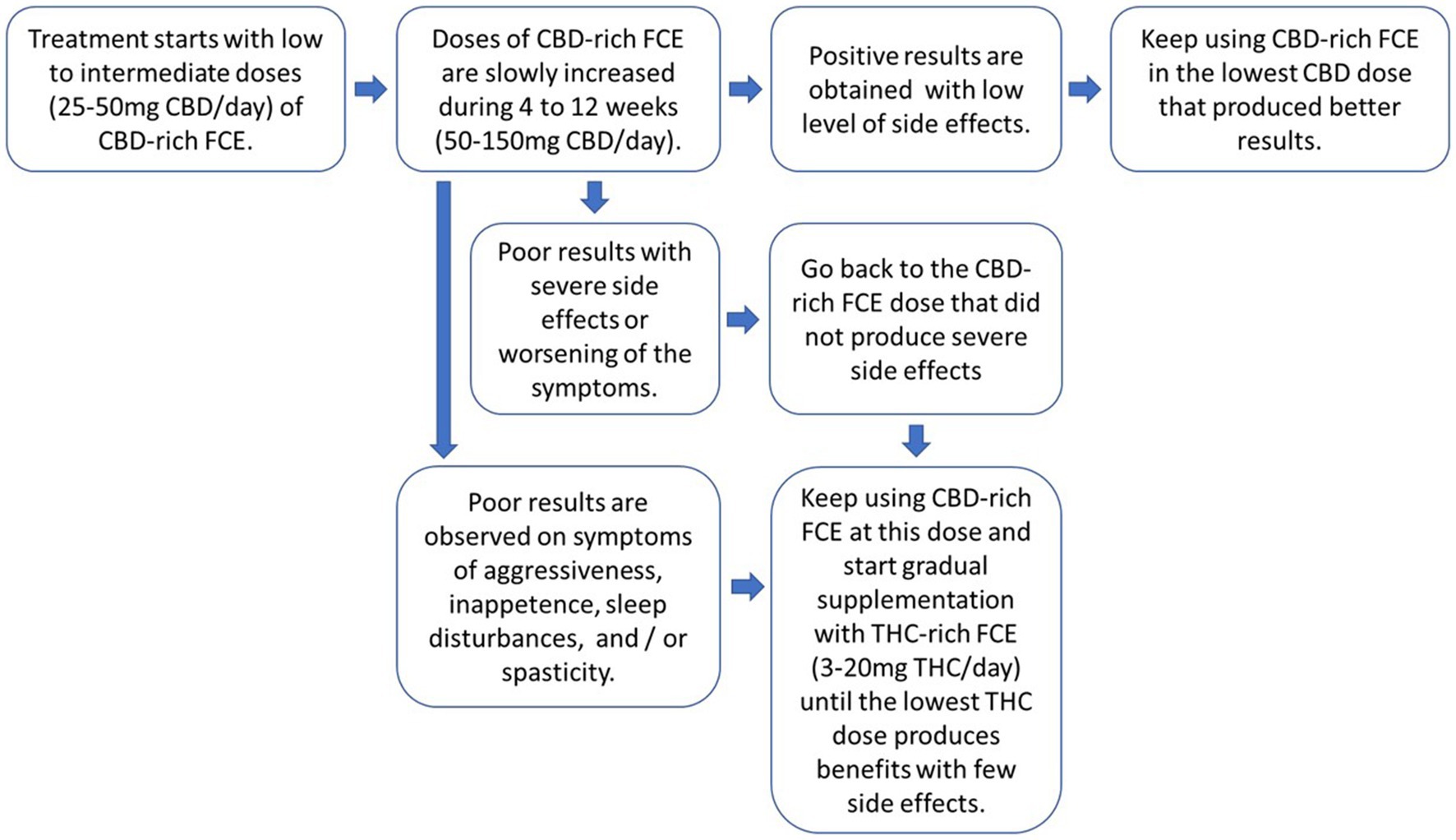
Figure 1. General guidelines for individual tailoring of FCE posology and CBD to THC proportions. The protocol should aways start with low doses of CBD-rich FCEs for all patients and doses should be slowly increased until improvements are observed. Doses can be divided in two or three daily administrations. If improvements are not observed and/or side-effects begin to occur, return to the dosage of the CBD-rich FCE that showed no side effects and start supplementing it with a THC-rich FCE, gradually increasing the final the proportion of THC resulting from the blend of the two FCEs.
Cannabis extracts were produced and distributed to all the patients in the study by three Brazilian patient NPOs, the Brazilian Society of Medicinal Cannabis Patients (also known as AMAME) the Cannabic Society in Defense of Life (also known as Maria Flor) and the Brazilian Support Society Cannabis Hope (also known as ABRACE). The quality and composition of cannabis extract samples were assessed by high-performance liquid chromatography (HPLC) analysis performed at certified laboratories.
The treatment reported here resulted from an adaptation of available clinical data to the Brazilian reality, but it was not originally intended to produce scientific data. Therefore, the approach used by each clinician contributing to this report to assess baseline clinical indicators of the ASD patients was not the same, which precluded us from using a before-vs-after approach. Thus, we have used a structured, caregiver-reported single-assessment retrospective outcome survey sent by e-mail to the patients and their families (Supplementary material). The questionnaire was adapted from the methodology previously used by Fleury and colleagues (76). Thus, we have employed a Likert-like scale (83) composed of six options to evaluate the perceived outcome of the treatment for 10 main symptom categories, 16 specific sub-categories for abnormal behavior and communication/social interaction impairments, and five additional non-symptomatic aspects. Parents were explicitly asked to report the difference observed since FCE treatment onset. The options for each question were: “Does Not Apply,” “Considerable Worsening,” “Moderate Worsening,” “No Change,” “Moderate Improvement” and “Considerable Improvement.”
In addition, responders were asked to describe in their own words the changes observed for each symptom category to ensure that the responder properly understood the meaning of each category and that they were scoring the Likert-like scale in a consistent way throughout the study. If discrepancies were detected, the responders were contacted by telephone or text messages to further discuss the definition of that specific symptom, and then they were asked whether they wished to reconsider their answers. These open-ended questions also helped to elucidate more practical and subjective impacts of the treatment (see discussion). The parents were invited to answer the survey from March 2022 to August 2022. Clinical charts of each patient were also assessed to obtain details of the treatment, such as weight, doses and use of other medications.
The 10 main symptom categories and five non-symptomatic aspects evaluated in the survey were chosen after reviewing their prevalence in the literature, adapting some of the available instruments (mainly the Autism Treatment Evaluation Checklist, ATEC), and considering the clinical experience of the physicians and ASD patient’s parents. Symptom categories used are as follows: (1) Attention deficit and hyperactivity disorder; (2) Abnormal behaviors; (3) Sadness, melancholy, bad moods; (4) Impaired motor development and motor coordination; (5) Lack of independence for daily activities; (6) Impaired communication and personal interactions (verbal and non-verbal); (7) Intellectual and cognitive deficits; (8) Sleep issues; (9) Seizures; (10) Avoidance and/or restrictions to food intake; (11) Positive mood states; (12) Overall patient’s quality of life; (13) Adverse effects due to treatment; (14) Use of other medications; (15) Overall family’s quality of life.
In the main group of categories, concerning Abnormal behavior, and Impaired communication and verbal interactions, each survey responder is likely to evaluate the outcome in each of these two categories considering their own reality regarding the intensity and scope of behavioral and communication problems of the patient. Further outcome details regarding these aspects were collected in two separated groups. Thus, the category “abnormal behaviors” was further subdivided into nine specific aspects as follows: (1) Stereotypies; (2) Aggressiveness Toward Others; (3) Self-Aggressiveness; (4) Autistic Meltdown Crisis/Temper Tantrum; (5) Screams and Random Sounds; (6) Obsessive Compulsive Behaviors; (7) Eating Non-Foods; (8) Discomfort in Noisy/Crowded Places; (9) Excessive Appetite.
In Communication and Social Interactions, we also analyzed specific related features, as follows: (1) Impaired Verbal Communication; (2) Impaired Visual Contact; (3) Impaired Response to Their Own Name; (4) Impaired Attention to Receptive Direct Verbal Communication; (5) Production of Sounds or Isolated Words with Communicative Function; (6) Impaired Written Communication; (7) Use of Alternative Forms of Communication (gestures, signals, cards, software applications, and other systems with images).
Adverse effects and Use of other medications were not evaluated using the above-mentioned scale, but by questions with open written answers, multiple-choice questions and by consulting patients’ medical records.
To generate descriptive outcome scores suitable for interpatient comparisons and statistical analysis, numeric labels were assigned to each of the five possible outcome answers seen in the Parents Outcome Survey. Namely, −2; −1; 0; 1; 2 for the scale of effects, and the # label was assigned when the patient did not present the specific symptom evaluated. The total number of patients for each symptom or aspect is equal to our cohort number minus the number of people who answered “Did Not Apply” (20 – #). Numbers in Figures 2–4 are shown as percentages of the whole cohort that presented each symptom or non-symptomatic aspect, plotted using MATLAB R2022a (Figures 2–4). Three outcome scores were generated, namely: General Outcome Score (GOS), an average of the scores from categories 1 to 11; Abnormal Behaviors Outcome Score (ABOS), an average of the scores from abnormal behavior sub-categories; and Communication and Interaction Outcome Score (CIOS), an average of the scores from communication and interaction sub-categories. Each score includes only the symptoms or categories presented by each patient, and each symptom or category present has the same weight.
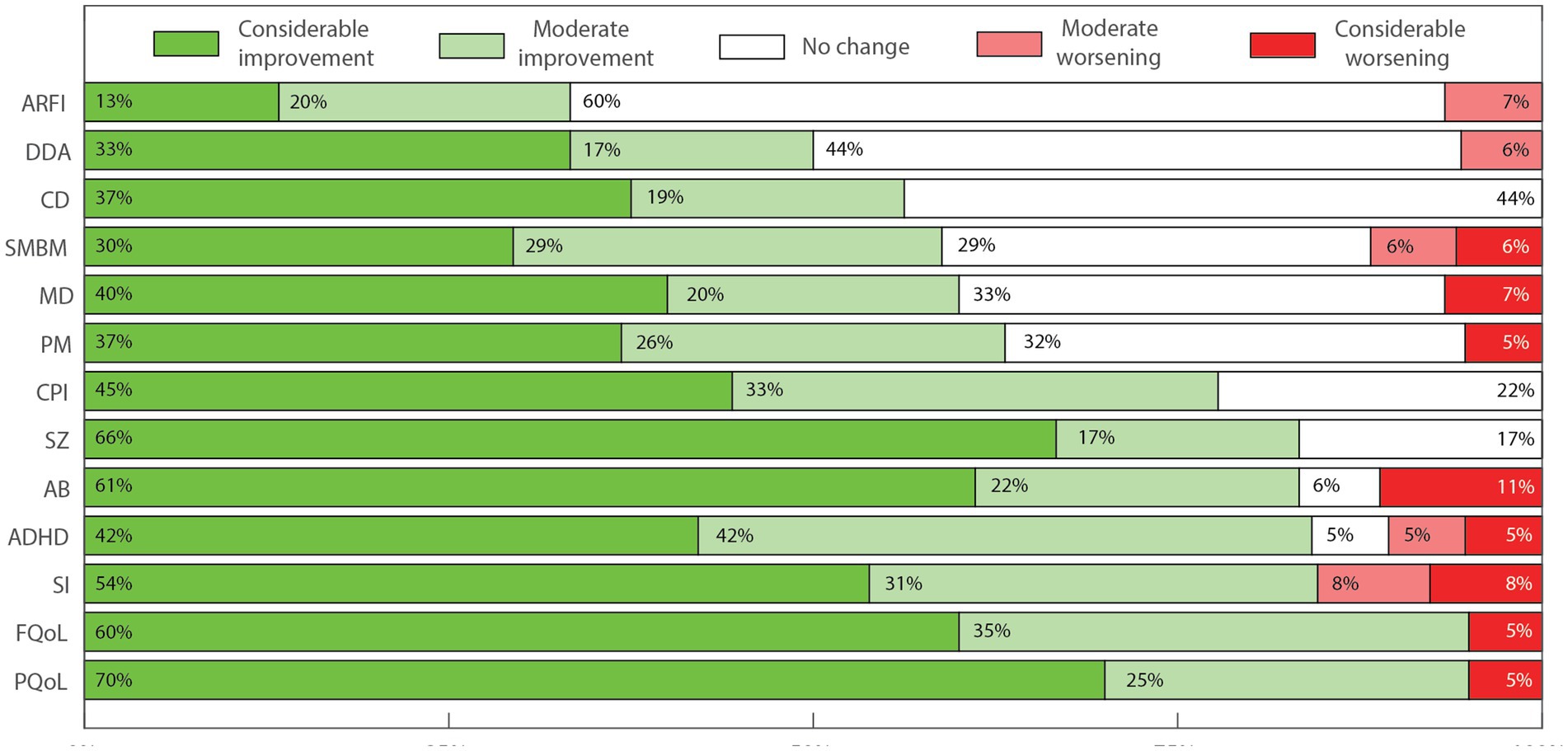
Figure 2. Perceived effects of FCE treatment over main symptom categories and aspects of ASD as percentages of the cohort. Percentages were rounded to whole numbers for clarity. Avoidance and/or restrictions of food intake (ARFI, n = 15); Lack of independence for daily activities (DDA, n = 18); Intellectual and cognitive performance deficits (CD, n = 16); Sadness, melancholy and bad moods (SMBM, n = 17); Impaired motor development and motor coordination (MD, n = 15); Positive mood states (PM, n = 19); Impaired communication and personal interactions (verbal and non-verbal; CPI, n = 18); Seizures (SZ, n = 6); Abnormal behaviors in general (AB, n = 18); Attention deficits/ hyperactivity disorder (ADHD, n = 19); Sleep issues (SI, n = 13); Overall family’s quality of life (FQoL, n = 20); Overall patient’s quality of life (PQoL, n = 20).
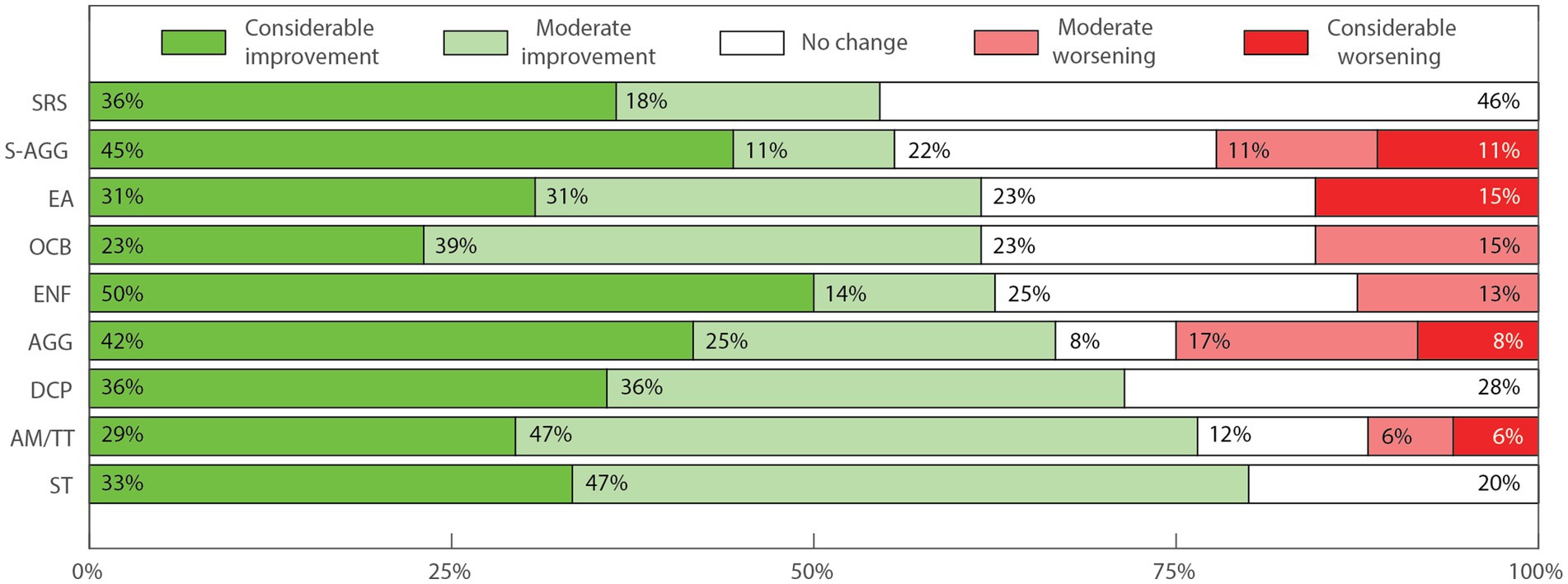
Figure 3. Perceived change in sub aspects of abnormal behaviors. Percentages were rounded to whole numbers for clarity. Screams and Random Sounds (SRS, n = 11); Self-Aggressiveness (S-AGG, n = 9); Excessive Appetite (EA, n = 13); Obsessive compulsive behaviors (OCB, n = 13); Eating non-foods (ENF, n = 8); Aggressiveness toward others (AGG, n = 12); Discomfort in noisy/crowded places (DCP, n = 14); Autistic Meltdown crisis/temper tantrum (AM/TT, n = 17); Stereotypies (ST, n = 20). Percentages were rounded to whole numbers for clarity.
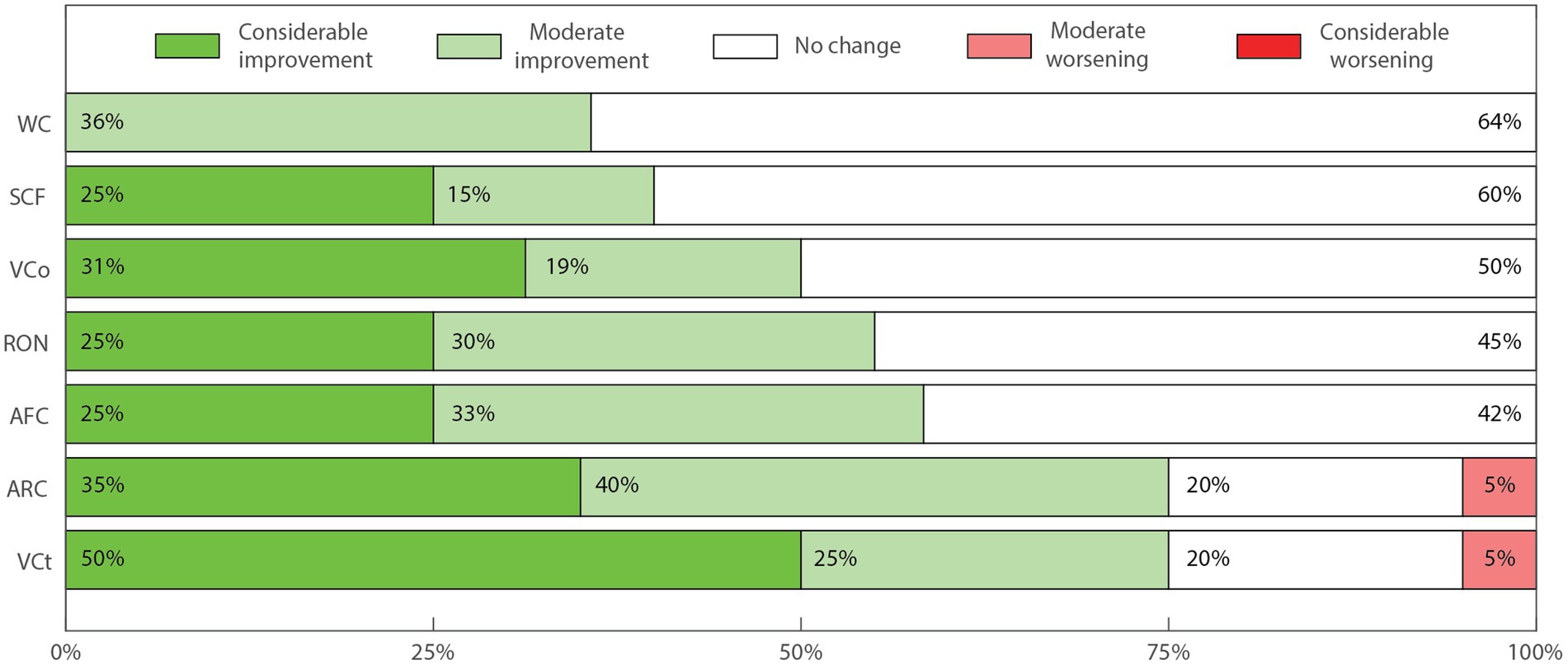
Figure 4. Perceived change in sub-categories of communication and interaction impairments. Impaired written communication (WC, n = 14); Production of sounds or isolated words with communicative function (SCF, n = 20); Impaired verbal communication (VCo, n = 16); Impaired response to their own name (RON, n = 20); Use of alternative forms of communication (AFC, n = 12); Impaired attention to receptive direct verbal communication (ARC, n = 20); Impaired visual contact (VCt, 20).
Concerning the dosage/formulation scheme, among the patients who answered the survey, 15 patients have used only CBD-rich FCEs throughout treatment (a); three patients started with a CBD-rich FCE, which was eventually supplemented with THC-rich FCE (b); and two patients have used a blend of a CBD-rich FCE with a THC-rich FCE throughout treatment (c). This may reflect a similar distribution pattern present in the whole treated population, but it actually emerged as a direct result of who chose to answer the survey or not. Among the predominant group who exclusively used CBD-rich FCEs throughout the treatment, only one patient, 2 m, showed a negative GOS (−1.1), whereas the other 14 showed positive GOS. All three patients who started with only CBD-rich FCE and eventually supplemented it with a THC-rich FCE, showed positive GOS. One of the two patients who used a blend of CBD-rich and THC-rich FCEs since the beginning, 8 m, showed positive GOS (1.0), while the other, 15f, showed a slightly negative GOS (−0,3). Overall, only 2 patients did not show positive GOS. This is a very high proportion of improvement, even though we cannot know whether this reflects the reality of the whole treated population, or the result of some bias, which, for instance, could have motivated parents who perceived better results to be more willing to answer the very detailed survey used here. Out of the 20 patients included in the study, 16 (80%) were treated with FCE for 6 months or more, and the average FCE treatment duration was 11.25 (± 6.1 SD) months. Average age was 14 years old (5–38) at the moment of the survey, being 18 males and 2 females. Average doses CBD changed from 46.63 (± 23.19 SD) mg/day at the beginning to 72.50 (± 37.82 SD) mg/day at the end, while the average dose of THC changed from 7.09 (± 7.42 SD) mg/day to 12.68 (± 12.31 SD) mg/day, representing an increase of average dose/day of 25.87 mg and 5.59 mg, respectively. The average final doses per weight were 1.88 (± 1.47 SD) mg/kg/day of CBD and 0.16 (± 0.41 SD) mg/kg/day of THC. The average final CBD to THC proportion was 5.71 (± 3.07 SD):1.
In Tables 2 3 and 4 we show the raw data from the survey answers of all participants regarding perceived effects on the main symptoms and on the symptoms subcategories. In cases when a given symptom/aspect did not apply to that patient, response was marked with a hashtag (#). Adverse Effects and Use of Other Medication are shown in Table 5 due to their particular type of answer (see Supplementary material).
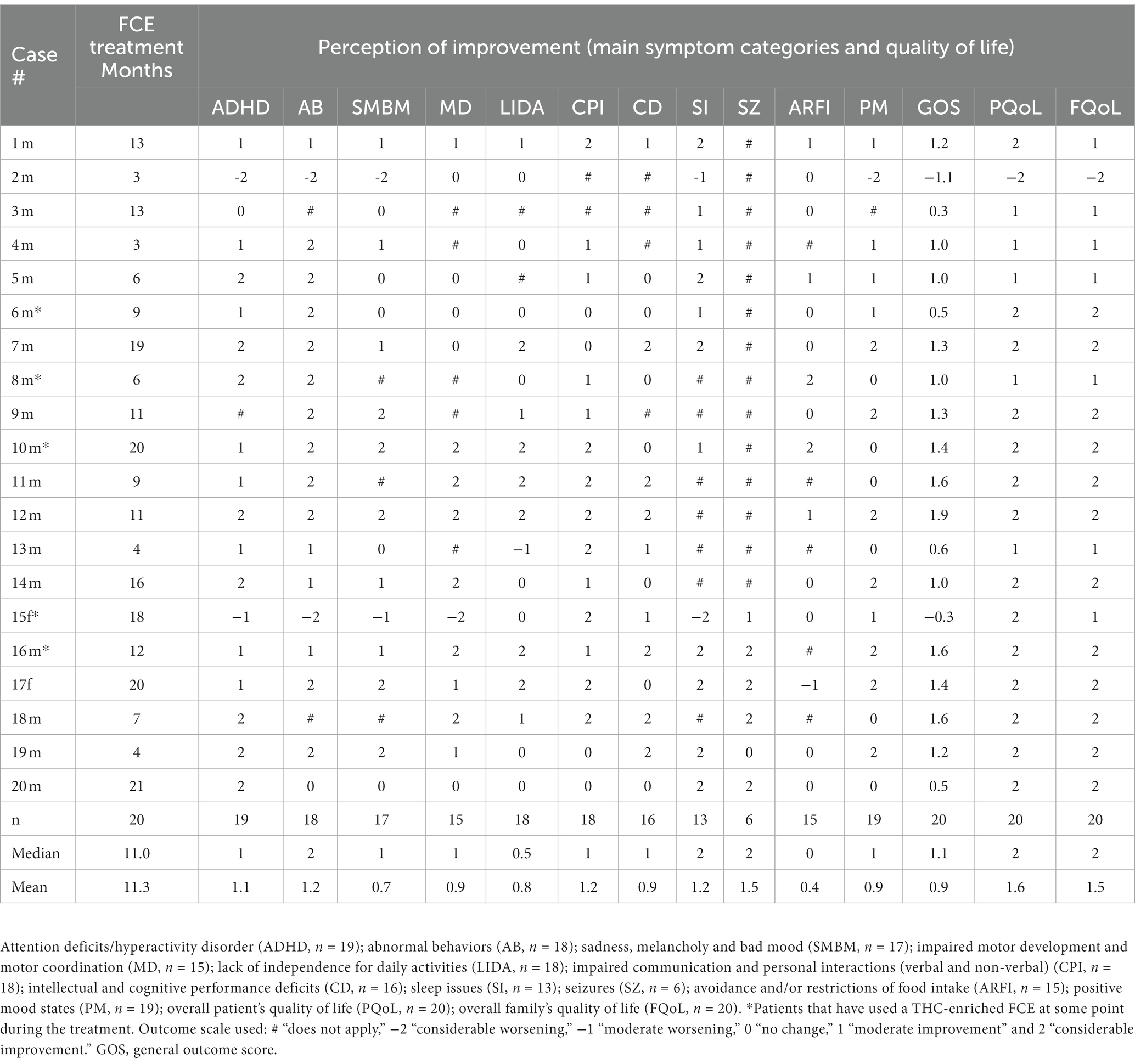
Table 2. Perceived improvement of symptoms and non-symptomatic aspects after FCE treatment for each patient.
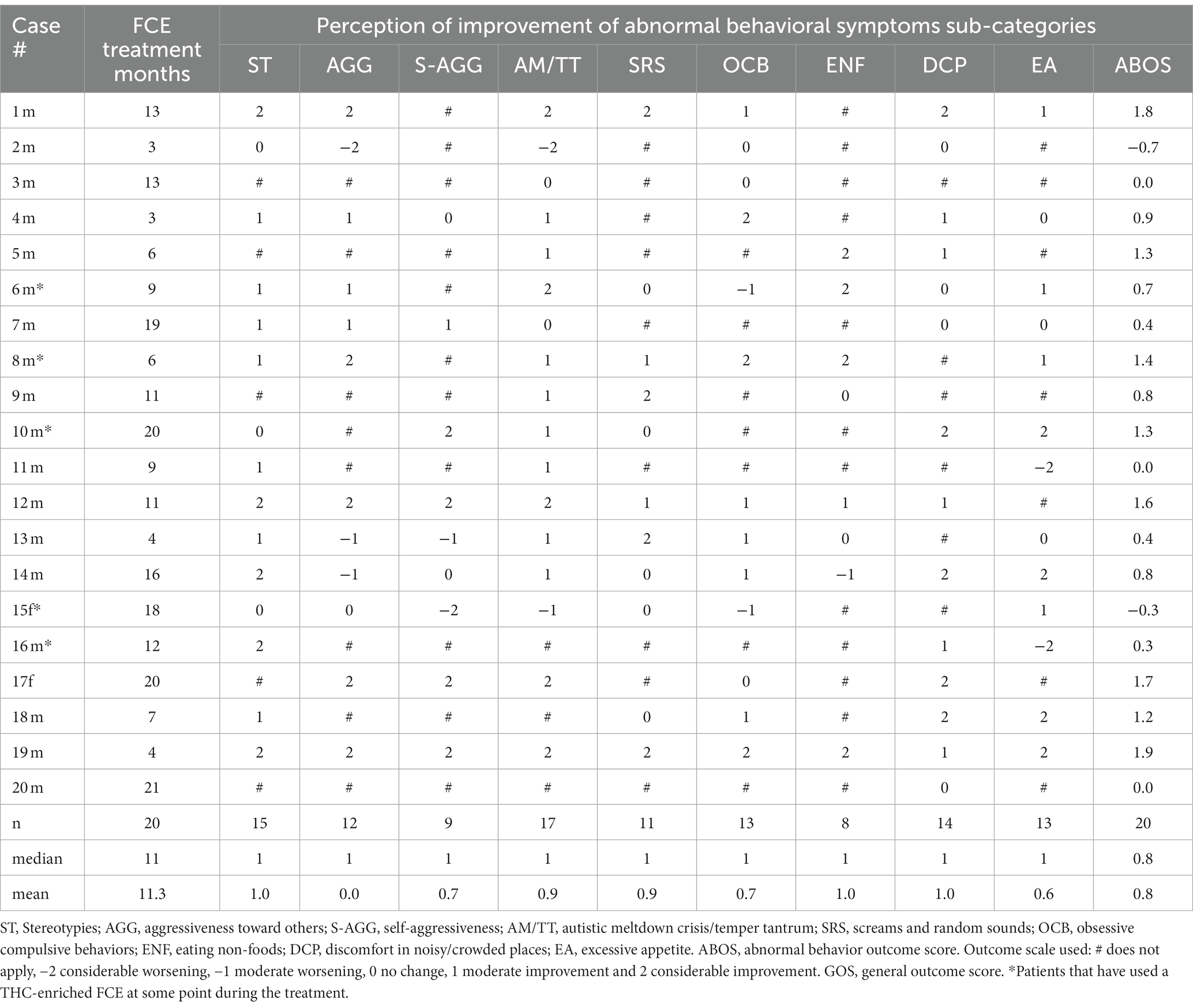
Table 3. Perceived improvement of abnormal behavior sub-aspects after FCE treatment for each patient.
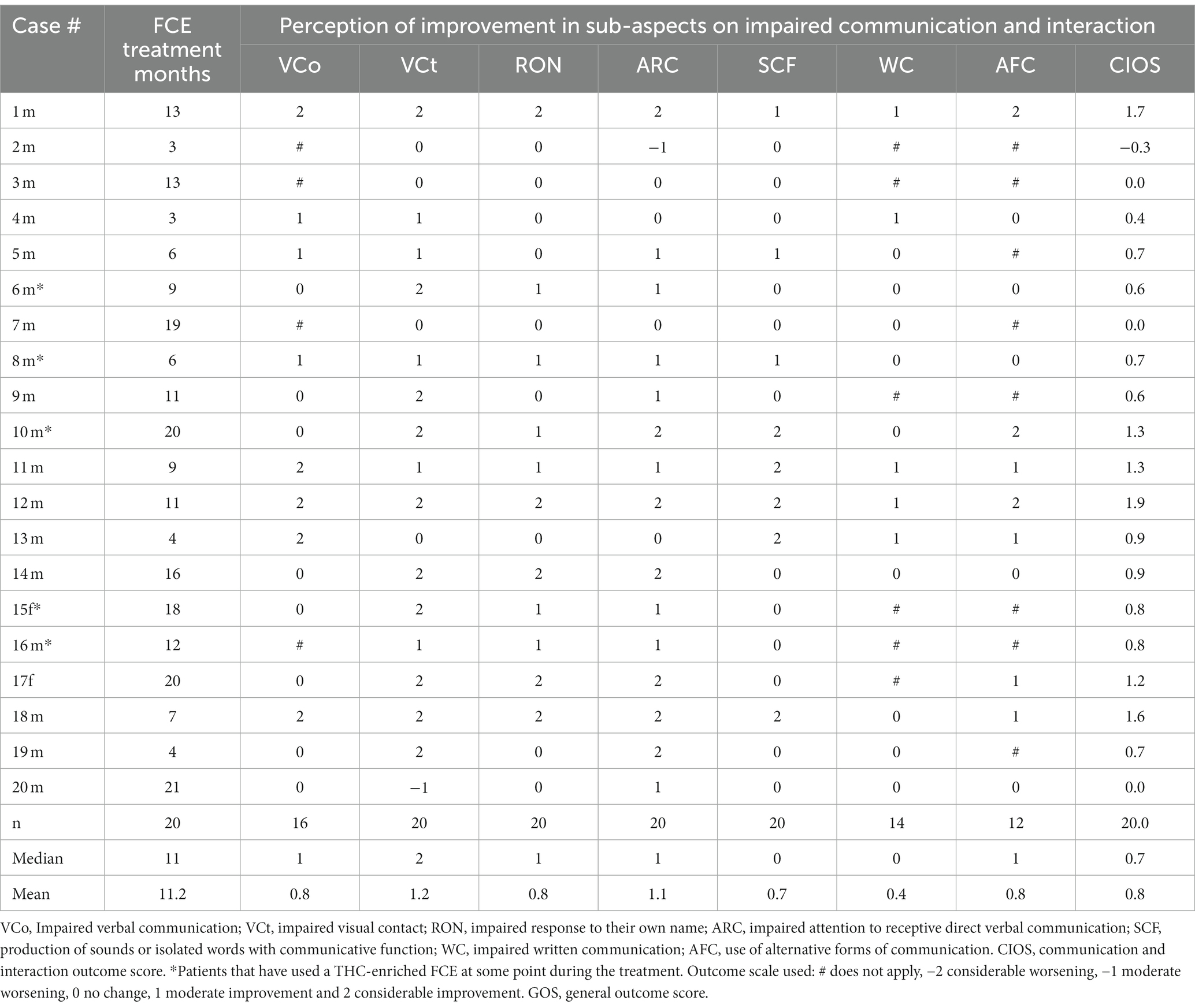
Table 4. Perception of improvement in sub-aspects on impaired communication and interaction after FCE treatment for each patient.
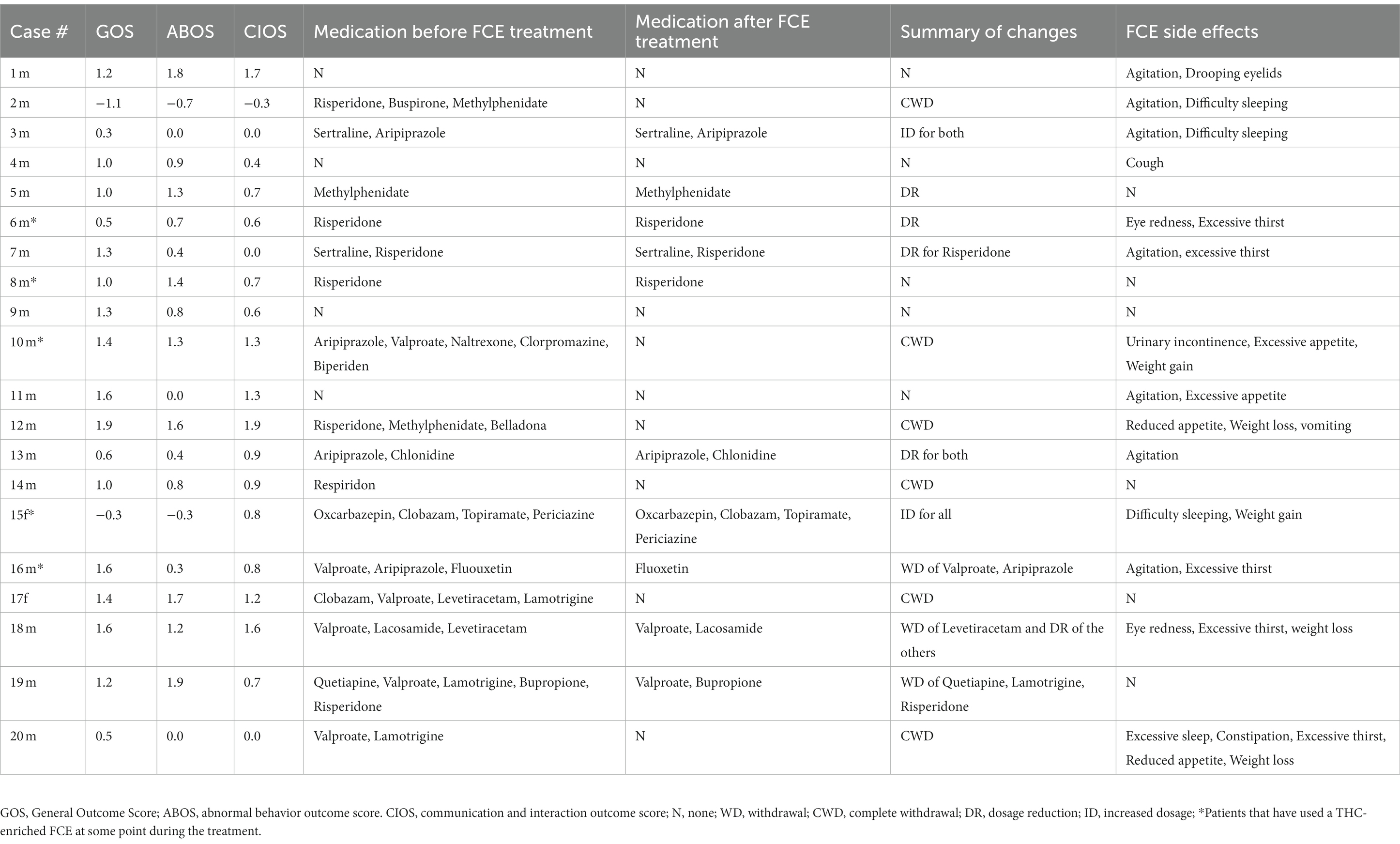
Table 5. Medications other than FCE used by the patients, and untoward effects observed during treatment with FCE.
There was a general perception of improvement for all 10 main symptom categories and 3 non-symptomatic aspects analyzed (Figure 2). Some features improved more frequently than others. While “avoidance and/or restrictions to food intake” improved in approximately 30% of cases, ADHD symptoms, “behavioral disorders,” “communication and social interaction deficits,” “sleep disorders,” “seizures,” “patient’s quality of life” and “family’s quality of life” improved in at least 77% of cases. General improvement in “intellectual and cognitive performance” were observed in 57% of the cases, which is very striking since there is no other pharmacological treatment known to improve this impactful and recurrent aspect of severe ASD.
Benefits from using FCE were observed in 84% of seizure cases, in general accordance with many other reports from the literature (84). Considerable improvement was equal or more frequent than 33% in 12 out of the 13 main categories (Table 2 and Figure 2). Remarkably, “patient’s quality of life” and “family’s quality of life” improved in 95 and 83% of cases, respectively. Only two patients, 2 m and 15f presented an overall worsening or no change in the main symptom categories (GOS equal to −0,3 and − 1.1, respectively).
There was improvement in at least 54% of cases in all 9 sub-categories of abnormal behaviors, as indicated in Table 3. A graphic representation of these results is presented in Figure 3. The frequency of patients presenting overall improvement in each of the specific subcategories of abnormal behavior was as follows: “stereotypies” 80%; “autistic meltdown crisis/temper tantrum” 76%; “discomfort in noisy/crowded places” 72%; “aggressiveness toward others” 67%; “eating non-foods” 63%; “excessive appetite” 62%; “obsessive compulsive behaviors” 62%; “self-aggressiveness” 56%; and “screams and random sounds” 54%. The frequency of “considerable improvement” perception was above 30% for 8 out of the 9 sub-categories, and ranged from 23% for “obsessive compulsive behavior” to 50% for “eating non-foods.”
Worsening of one or more abnormal behavior sub-categories was perceived in 7 out of the 20 patients (35%), with 3 out of 12 (25.0%) reporting worsening in “aggressiveness toward others”; 2 out of 9 (22.2%) in “self-aggressiveness,” 2 out of 17 (11.8%) in “meltdown crisis/temper tantrum,” 2 out of 13 (15.4%) in “obsessive compulsive behaviors,” 1 out of 8 (12.5%) in “eating non-foods” and 2 out of 13 (15.4%) in “excessive appetite.” “Considerable worsening” was perceived in 5 out of 20 patients (25.0%) in four sub-categories, with 1 out of 12 (83.3%) reporting considerable worsening in “aggressiveness toward others,” 1 out of 9 (11.1%) in “self-aggressiveness,” 1 out of 17 (5.8%) in “meltdown crises/temper tantrums” and 2 out of 13 (15.3%) in “excessive eating.” Nevertheless, only two patients, 2 m and 15f presented an overall worsening in abnormal behavior sub-categories (ABOS equal to −0.3 and − 0.7, respectively).
There was consistent improvement in all communication and social interaction sub-categories. We highlight that “attention to receptive direct verbal communication” improved in 17 out of 20 (85%), while “visual contact” and “attention to conversation” improved in 15 out of 20 (75%) of cases. “Verbal communication” improved in 8 out of 16 (50%) of cases, “response to their own name” improved in 11 out of 20 (55%) of cases, “written communication” improved in 5 out of 14 (35.7%) of cases and “alternative forms of communication” improved in 7 out of 12 (58%) of cases. Actual worsening of cases was found only in one case for “visual contact” and in one case for “attention to receptive direct verbal communication.” Only patient 2 m presented an overall worsening in communication and interaction sub-categories (CIOS equal to −0.3).
Medications other than the FCE used by the patients are indicated in Table 5. As FCE treatment progressed, out of the 16 patients receiving other neuropsychiatric medications, four (25%) reduced the dosage for at least one type of medication, nine (56%) discontinued at least one type of medication, and six (37%) discontinued all medication. Therefore, out of 16 patients, 13 (81%) have reduced or discontinued neuropsychiatric medications after using FCE. Only two patients increased the doses of medications other than FCE during treatment, and one patient’s medications remained unaltered.
The adverse effects reported in our cohort of patients are also shown in Table 5. In most cases, adverse effects were mild and temporary. The most frequent adverse effects were agitation (6), difficulty sleeping (3), excessive thirst (3), eye redness (2), excessive appetite (2), weight gain (2), reduced appetite (2), weight loss (2). Only one patient (2 m) abandoned the treatment due to worsening of symptoms.
In this manuscript we present the perceived improvements of ASD patients and their families over the course of 3–21 months of treatment with FCE, using a titration protocol that resulted in personalized CBD and THC dosages, resulting in individually tailored CBD to THC proportions ranging from 49:1 to 1:22. Our sample consisted of 20 patients of varied ages and ASD severities. Parents reported improvement in all aspects evaluated. Side effects observed during FCE treatment were mild, as well as untoward interactions with other medications. As treatment evolved, most of other medications had their doses reduced or were completely removed during FCE treatment, which is consistent with the subjective perception of general improvement after FCE treatment. Patients’ and their families’ quality of life improved in 19 out of the 20 cases.
Difficulties in language and social interaction from a young age can result in behavioral issues, poor social skills and the consequent impacts over the quality of life of ASD patients (85). An overall perception of improvement in the main category “impaired communication and personal interactions” (CPI) was perceived in 78% of the patients (Figure 2). Accordingly, our analysis of the sub-categories of communication and interaction yielded a positive average communication and interaction outcome score (CIOS) of 0.8 (Table 4). The positive results were mostly driven specifically by benefits in speech, visual contact, and attention (Figure 4). In their open answers to our control questions (see Supplementary material), parents often reported feeling happy to see their children actively engaging with them, as well as with colleagues in the school setting during FCE treatment. This reinforces the increasing amount of data supporting the use of FCE to treat some of the most impactful core aspects of ASD (8), which are not effectively treated by any of the currently available medications.
Here we also provide a more detailed account on the effect of FCE treatment for the well-being of people with autism and the nuances of non-core symptoms. The generally positive outcome in social interaction, cognition and behavioral abnormalities seems to have had very impacting effects over quality of life of both families and patients, which are of particular interest, reflecting the benefits of FCE in a more comprehensive way. Open-answer questions provided some insight on how those improvements impacted on day-to-day situations; decrease of “aggressiveness toward others,” “discomfort in crowded places,” and “autistic meltdown crises / temper tantrums,” for example, allowed families to have less stressful situations and more relaxed moments of joy at home and in outdoor activities. Ninety-five percent of families of patients using FCE in our study reported improvement in their quality of life, which must be considered by any kind of therapeutical intervention for autism (23). Given the variety of symptoms and comorbidities associated with ASD (86), THC-rich and CBD-rich FCEs may be useful for managing different core symptoms of ASD and its comorbidities. Although impairments in sleep quality, appetite and motor development are not central to ASD diagnosis (i.e., non-core symptoms), they are frequent in the spectrum and their improvements are crucial to the well-being of people with ASD and their families.
We have also included in our outcome survey the category “eating non-foods,” which corresponds to the behavioral condition known as allotriophagy or Pica, characterized by the recurrent ingestion of nonfood substances or objects, lacking nutritional value, in an age incompatible with such behavior, according to the DSM 5 (87). In our sample, 8 out of 20 patients (40%) presented this condition. Although its general prevalence in ASD patients is not well established, it seems to be relatively frequent and regularly neglected as an important comorbidity of the spectrum, even though every so often it may lead to important health problems, such as choking, gastrointestinal obstructions or perforations, parasitic infections and poisoning (17–19, 87–90). ASD-associated Pica is generally refractory to medications, and the most effective treatment involves behavioral modeling by applied behavioral analysis therapy (ABA) (87). There is one case report of a female ASD patient who started engaging in coprophagy while in risperidone treatment, which was completely resolved when the medication was changed for aripiprazole (18).
Our results showed that, out of the 8 ASD patients who present Pica, 1 showed moderate worsening, 2 showed no change, 1 showed moderate improvement and 4 showed considerable improvement after FCE treatment. To the best of our knowledge, this is the first time a cannabinoid-based treatment showed such effectiveness for the treatment of Pica in ASD patients. Pica’s etiology may be associated to nutritional deficiencies, related to metabolic or ingestion issues (difficulties on mastication, for instance), to mental conditions, such as psychosis and impaired emotional regulation or a combination of these factors (17, 19, 87). The frequent association of Pica with the ASD populations may be a consequence of comorbid genetic conditions, intestinal inflammatory processes, or food selectivity, for instance. The improvements observed here may be due, therefore, to improvement of absorptive function by reducing intestinal inflammatory processes (91–98) often associated with ASD, and /or by improving emotional regulation. It cannot be ruled out, however, that the whole cannabis extract can also contribute supplementing nutrients (95, 99, 100) absent in the individual’s normal diet.
On a sidenote, we want to address our decisions regarding some symptom categories and subcategories. It is important to stress out that hyperactivity and attention deficit are not necessarily linked, and may, therefore, respond differently to cannabinoids (101–104). Nonetheless, here they are conjugated in one single category because that combination is frequent among ASD patients (102, 103, 105, 106), and further detailing of the specific effect of cannabinoids in each one could broaden too much the scope of the present study. The categories “abnormal behaviors” and “impaired communication and personal interactions” are important to access the core aspects of ASD. However, they are multifaceted and vary widely in specificity and severity among people in the spectrum. For this reason, we have included these categories in the group of main symptomatic categories, and have created two other outcome groups to analyze the specificities for both these categories.
Regarding the importance of using whole extracts as opposed to purified phytocannabinoids, it is worth noting that in one of the best controlled studies, published by Aran and colleagues in 2021, the treatment with full-spectrum extract containing both CBD and THC has yielded slightly better results than the mixture of pure CBD and THC in proportion equivalent to the whole extract, even though the difference was not statistically significant (73). Besides, a metanalysis study has shown that the use of full-spectrum, CBD-rich extracts has yielded better clinical results than the use of pure CBD for the treatment of infantile syndromes associated with refractory epilepsy and regressive autism (84). Finally, there is one case report showing significant outcome improvements when CBD was combined with selected terpenes for the behavioral treatment of an adolescent ASD patient (107).
Studies that followed the standard 12 weeks period of clinical evaluation and used more restrictive, homogeneous samples (73, 78), may have been too short to assess specific changes in ASD behavioral symptoms, which depend on slow neurochemical, structural and cognitive adjustments. Hopefully, our real-life study design was able to better capture such changes. These more rigorous and well controlled prospective studies have mostly used a single formulation with a CBD to THC proportion of 20: 1 (72–75). Nevertheless, published studies have altogether used a diverse range of full-spectrum cannabis extracts (72–74, 76–79, 82, 108) with comparable results.
Since these studies also varied considerably in terms of sample heterogeneity, treatment time and outcome evaluating method, it is very difficult to compare the results among them. However, most of them presented some level of improvement in both core ASD symptoms and comorbidities, with a varied range of specific benefits and proportion of patients with positive outcomes. Another trend across the studies was the occurrence of mostly mild and infrequent adverse effects. Therefore, we may say that, altogether, these studies indicate that FCE-based treatment of ASD symptoms has yielded some level of positive results, regardless of sample heterogeneity, outcome evaluating method or proportion of CBD to THC dosages. However, when high THC formulations are used, the frequency of behavioral side-effects is higher (72). Hence, it is reasonable to speculate that, even though some patients may not benefit at all from cannabinoid treatment, there might exist a CBD-to-THC formulation range and cannabinoids dosage better suited to each specific condition in the ASD spectrum. The mostly beneficial results demonstrated here support this hypothesis, since our titration protocol used combinations of extracts with different CBD to THC proportions, resulting in individually tailored CBD to THC proportions. Among the 20 patients enrolled in this study, 15 have used CBD-rich formulations throughout treatment and 3 have started with CBD-rich FCEs, and eventually supplemented it with THC-rich FCEs. Among these 18 patients, only one, who belongs to the first group, showed a negative GOS. On the other hand, among the 2 patients who have used a blend of CBD-rich FCE and THC rich FCEs since the beginning, one (8 m) showed a positive result (GOS = 1), while the other (15f) showed a slightly negative score (GOS = −0,3), which resulted from some worsening in behavioral symptoms. Patient 15f was also the only one who did not follow any kind of parallel support activities like psychotherapy or sports (see Supplementary File S1), which may have had some influence over its GOS score. Among the remaining 19 patients, which displayed predominantly positive GOS scores, the most common activities reported were Inclusive Regular Schooling (60% of cases), Psychotherapy (50% of cases), Occupation Therapy and Speech Therapy (45% of cases each) and Special Schooling and Physical Activities (30% of cases each). When proposing a tailored dose FCE treatment, physicians should also observe for the possible relevance of support activities in potentializing the effects of Cannabis treatment.
Regardless of our generally small sample size, our data strongly suggests that the effective range of cannabinoid dosage and CBD to THC proportions in ASD treatment may be wide and flexible, but it is safer to start with CBD-rich FCEs, even though some good results may be obtained by starting with a blend of CBD-rich and THC-rich FCEs. Thus, our results allow us to propose safe guidelines for a dosage scheme protocol, as illustrated in Figure 1: (1) low doses of CBD-rich FCEs should be employed at first for all patients as a standard care; (2) CBD doses should be slowly increased until improvements are observed; (3) if improvements are not observed and/or side-effects begin to occur, return to the dosage that has shown no side effects and start supplementing the first CBD-rich FCE with a second THC-rich FCE, gradually increasing in the final proportion of THC to CBD. Of course, these guidelines will need to be further tested with larger and more diverse sample sizes in order to be fully validated.
Cannabinoids are considered potential treatment option for various neurodevelopmental disorders, such as schizophrenia (109–111) and autism. ASD patients have been shown to possess abnormal neuronal activation and connectivity (61, 112, 113), probably due to deficient regulation in synapses. This is a feature reminiscent of mechanisms involved in epilepsy (61). Further, there is higher incidence of epilepsy among autism patients (114, 115) and EEG records of epileptiform activity have been recorded from non-epileptic ASD children (116). Epilepsy symptoms have been successfully treated using Cannabis extracts, especially due to CBD and THC’s ability to reduce epileptiform activity (117–119), reinforcing the use of both as a possible treatment for ASD. Indeed, people on the spectrum present modified expression of cannabinoid receptors (120) and of the endocannabinoid anandamide (121), just like in animal models of autism (122). CBD might further promote ASD symptom improvement through its anti-inflammatory effects (123), as ASD symptoms has been linked to neuroinflammation (124–126). This research background guided our choice of full spectrum Cannabis extracts instead of purified ones, and we believe it plays a part on achieving the benefits reported above.
The specific side effects observed in both patients who were receiving multiple medications and patients who only had used FCE varied considerably, but were mostly mild. Patients 15f and 2 m were the two with the lowest general outcome scores (GOS equal to −0.3 and − 1.1, respectively). Both were using many neuropsychiatric medications and perceived worsening in more symptomatic categories and subcategories than all other patients. The patient with the lowest GOS of all, 2 m, has unilaterally decided to completely withdraw at once both FCE treatment and all other medications after presenting behavioral worsening. He is the only one among all patients who has discontinued FCE treatment in consequence of worsening. He is also the only one, among the six patients who discontinued all previously used medications, who presented negative GOS. In his case, the precocious, unadvised discontinuation of all medications at once precluded us from trying to adjust the doses and have a clear understand of what may have caused the worsening. Medication interactions did not seem to have caused problems in other patients, but it is a possible cause of worsening in this case. Most of the other five patients who discontinued all other medications under clinical supervision did not present negative outcome scores in any of the 10 main symptomatic categories. The only exception was patient 17f, who presented worsening in only one main symptom category (“avoidance and/or restrictions of food intake”), but still had a relatively high outcome score (GOS equal to 1.4).
All the four patients who were not using any other medications since the beginning of the FCE treatment (namely 1 m, 4 m, 9 m and 11 m) presented GOS equal or above 1.0. Concomitant use of FCE and other psychiatric medications was mostly well tolerated across participants, supporting the use of FCE both as an adjuvant and as a single pharmacological approach for ASD treatment. There is, however, significant concern about the important side effects related to polypharmacy of psychotropic medications used by people in the spectrum (26, 27, 30, 34, 35, 38, 41, 42, 44–46, 127–139), prevalent in 19% in adults (138) going as high as 81% in children (136, 137). This may reflect the considerable range of non-core ASD symptoms still untreated by conventional clinical protocols for ASD (86).
Discontinuation and/or dose reduction of other medications, as we observed in a considerable number of cases in this work, may significantly reduce the patient’s array of side effects associated to other medicines (26, 27, 30, 34, 35, 38, 41, 42, 44–46, 127, 129–135, 139). Furthermore, in the long run, such a wide range of benefits may also significantly alleviate the family’s economic burden (22).
Although the proposed FCE dosage regimen was developed as a result of clinical experience with over a hundred ASD patients, few patients effectively provided all data necessary to be included in the analysis. As a retrospective study, our cohort is also a convenience sample. The cohort we analyzed is composed of patients who already possessed an ASD diagnosis, often referred from other doctors. As the original evaluation of symptoms and diagnosis was obtained, in some cases, years before the start of Cannabis treatment, records of it were difficult to obtain. The clinicians involved in this study evaluated each person according to DSM-V criteria to perform adequate treatment. Furthermore, one must acknowledge that a patient-reported outcome survey, although valid as a source of clinical information, is not the most objective tool to inform about aspects such as cognitive and motor improvement. Finally, as an open-labeled study with no control group, a possible wishful thinking effect on parents’ answers to the outcome survey must be taken in account, especially in cases of short time treatment and in those were there was no change in previously used medication.
In sum, this work reinforces the benefits of the full spectrum Cannabis extract for treatment of people in the autistic spectrum, and proposes individually-tailored, response-based dosage regimen guidelines for this population. Both the patient’s and their family’s quality of life improved significantly after treatment. Our study expands the scientific data demonstrating that clinical use of Cannabis extracts is a safe intervention with promising and valuable effects over many core and comorbid aspects of autism, that are not achieved by conventional medications. In addition, we have shown, for the first time, that allotriophagy (Pica), another important comorbidity relatively frequent in ASD, may also be effectively treated by Cannabis extracts. Side effects from FCE were mild and mostly did not preclude treatment. Further studies with larger samples will be necessary to confirm our overall positive results as well as to further validate our suggested dosage guidelines and new patient/parents-reported outcome questionnaire for ASD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee on Human Research of the Health Sciences College of the University of Brasilia (Universidade de Brasília-UnB). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
PM, WM, LS, FC, and RM-L were responsible for study conception and design. PM and LS were responsible for clinical care of the patients. PM, WM, LS, CB, and RM-L were responsible for the elaboration of the patients, parents-reported outcome survey. FC and JB-N provided editing of patients, parents-reported outcome survey. FC was responsible for the ethical aspects of research. WM was responsible for data collection. FC and WM were responsible for data analysis and presentation. PM and RM-L were responsible for the guideline’s graphic presentation. WM and RM-L provided bibliographic revision and wrote the manuscript. JB-N and VB provided critical reading of the manuscript. PM, WM, FC, JB-N, VB, and RM-L provided editing of the manuscript. FC aided in the scientific supervision. RM-L provided general scientific supervision. All authors read and approved the final version of the manuscript.
WM received a grant from WeCann Academy, an international institution for education in endocannabinoid medicine, for data collection and analysis in this work. FC was supported Fundação de Apoio ã Pesquisa do Distrito Federal (FAPDF, grant #30023.128.46472.04012022).
The authors thank the support of the nonprofit organizations AMA+ME, MARIA FLOR and ABRACE, which provided details on extract concentrations for this paper. They also provide relevant social work in Brazil by enabling access to medical Cannabis products, especially for people in a vulnerable social situation, and for that they deserved to be acknowledged.
PM is one of the founders and main clinicians of NeuroVinci, and founded WeCann Academy, an international institution for education in endocannabinoid medicine. WM received a grant from WeCann Academy for data collection and analysis in this work. RM-L has a 0,8% share of the company Grüne Labs, Pando, Uruguay, which plans to commercialize cannabis-based medications in the future.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1210155/full#supplementary-material
1. Arnold, M , Netson, R , and Vyshedskiy, A . Combinatorial language parent-report scores differ significantly between typically developing children and those with autism Spectrum disorders. J Autism Dev Disord. (2022) 2022:5769. doi: 10.1007/s10803-022-05769-8
2. Arutiunian, V , Gomozova, M , Minnigulova, A , Davydova, E , Pereverzeva, D , Sorokin, A, et al. Structural brain abnormalities and their association with language impairment in school-aged children with autism Spectrum disorder. Sci Rep. (2023) 13:1172. doi: 10.1038/s41598-023-28463-w
3. Carter Leno, V , Bedford, R , Chandler, S , White, P , Yorke, I , Charman, T, et al. Callous-unemotional traits in youth with autism spectrum disorder (ASD): replication of prevalence estimates and associations with gaze patterns when viewing fearful faces. Dev Psychopathol. (2021) 33:1220–8. doi: 10.1017/S0954579420000449
4. Gulati, S , Kaushik, JS , Saini, L , Sondhi, V , Madaan, P , Arora, NK, et al. Development and validation of DSM-5 based diagnostic tool for children with autism Spectrum disorder. PLoS One. (2019) 14:e0213242. doi: 10.1371/journal.pone.0213242
5. Hyman, SL , Levy, SE , and Myers, SM, Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics . Executive summary: identification, evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics. (2020) 145:e20193448. doi: 10.1542/peds.2019-3447
6. Ji, Y , Xu, M , Liu, X , Dai, Y , Zhou, L , Li, F, et al. Temporopolar volumes are associated with the severity of social impairment and language development in children with autism spectrum disorder with developmental delay. Front Psych. (2022) 13:1072272. doi: 10.3389/fpsyt.2022.1072272
7. Melo, C , Ruano, L , Jorge, J , Pinto Ribeiro, T , Oliveira, G , Azevedo, L, et al. Prevalence and determinants of motor stereotypies in autism spectrum disorder: a systematic review and meta-analysis. Autism. (2020) 24:569–90. doi: 10.1177/1362361319869118
8. Prelock, PJ , and Nelson, NW . Language and communication in autism: an integrated view. Pediatr Clin. (2012) 59:129–45. doi: 10.1016/j.pcl.2011.10.008
9. Rieth, SR , Haine-Schlagel, R , Burgeson, M , Searcy, K , Dickson, KS , and Stahmer, AC . Integrating a parent-implemented blend of developmental and Behavioral intervention strategies into speech-language treatment for toddlers at risk for autism Spectrum disorder. Semin Speech Lang. (2018) 39:114–24. doi: 10.1055/s-0038-1627483
11. Vats, P , Juneja, M , and Mishra, D . Diagnostic accuracy of international epidemiology network (INCLEN) diagnostic tool for autism Spectrum disorder (INDT-ASD) in comparison with diagnostic and statistical manual of mental Disorders-5 (DSM-5). Indian Pediatr. (2018) 55:482–4. doi: 10.1007/s13312-018-1339-8
12. Hossain, MM , Khan, N , Sultana, A , Ma, P , McKyer, ELJ , Ahmed, HU, et al. Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: an umbrella review of systematic reviews and meta-analyses. Psychiatry Res. (2020) 287:112922. doi: 10.1016/j.psychres.2020.112922
13. Dunn, K , Rydzewska, E , Fleming, M , and Cooper, SA . Prevalence of mental health conditions, sensory impairments and physical disability in people with co-occurring intellectual disabilities and autism compared with other people: a cross-sectional total population study in Scotland. BMJ Open. (2020) 10:e035280. doi: 10.1136/bmjopen-2019-035280
14. Li, YJ , Xie, XN , Lei, X , Li, YM , and Lei, X . Global prevalence of obesity, overweight and underweight in children, adolescents and adults with autism spectrum disorder, attention-deficit hyperactivity disorder: a systematic review and meta-analysis. Obes Rev. (2020) 21:e13123. doi: 10.1111/obr.13123
15. Fombonne, E , Croen, LA , Bulkley, JE , Varga, AM , Daida, YG , Hatch, BA, et al. Emotional and Behavioral problems in youth with autism: high prevalence and impact on functioning. J Dev Behav Pediatr. (2021) 43:140–8. doi: 10.1097/DBP.0000000000001028
16. Beck, KB , Conner, CM , Breitenfeldt, KE , Northrup, JB , White, SW , and Mazefsky, CA . Assessment and treatment of emotion regulation impairment in autism Spectrum disorder across the life span: current state of the science and future directions. Psychiatr Clin North Am. (2021) 44:95–110. doi: 10.1016/j.psc.2020.11.008
17. Fields, VL , Soke, GN , Reynolds, A , Tian, LH , Wiggins, L , Maenner, M, et al. Pica, autism, and other disabilities. Pediatrics. (2021) 147:e20200462. doi: 10.1542/peds.2020-0462
18. Herguner, A , and Herguner, S . Pica in an adolescent with autism Spectrum disorder responsive to aripiprazole. J Child Adolesc Psychopharmacol. (2016) 26:80–1. doi: 10.1089/cap.2015.0184
19. Kinnell, HG . Pica as a feature of autism. Br J Psychiatry. (1985) 147:80–2. doi: 10.1192/bjp.147.1.80
20. Anorson, N , Male, I , Farr, W , and Memon, A . Prevalence of autism in Europe, North America and Oceania, 2000-2020: a systematic review. Eur J Pub Health. (2021) 31:786. doi: 10.1093/eurpub/ckab164.786
21. Li, Q , Li, Y , Liu, B , Chen, Q , Xing, X , Xu, G, et al. Prevalence of autism Spectrum disorder among children and adolescents in the United States from 2019 to 2020. JAMA Pediatr. (2022) 176:943–5. doi: 10.1001/jamapediatrics.2022.1846
22. Hong, M , Lee, SM , Park, S , Yoon, SJ , Kim, YE , and Oh, IH . Prevalence and economic burden of autism Spectrum disorder in South Korea using National Health Insurance Data from 2008 to 2015. J Autism Dev Disord. (2020) 50:333–9. doi: 10.1007/s10803-019-04255-y
23. Schnabel, A , Youssef, GJ , Hallford, DJ , Hartley, EJ , McGillivray, JA , Stewart, M, et al. Psychopathology in parents of children with autism spectrum disorder: a systematic review and meta-analysis of prevalence. Autism. (2020) 24:26–40. doi: 10.1177/1362361319844636
24. Pandina, G , Ring, RH , Bangerter, A , and Ness, S . Current approaches to the pharmacologic treatment of Core symptoms across the lifespan of autism Spectrum disorder. Psychiatr Clin North Am. (2020) 43:629–45. doi: 10.1016/j.psc.2020.08.003
25. Doyle, CA , and McDougle, CJ . Pharmacologic treatments for the behavioral symptoms associated with autism spectrum disorders across the lifespan. Dialogues Clin Neurosci. (2022) 14:263–79. doi: 10.31887/DCNS.2012.14.3/cdoyle
26. Dreifuss, FE , and Langer, DH . Side effects of valproate. Am J Med. (1988) 84:34–41. doi: 10.1016/0002-9343(88)90055-1
27. Hofer, A , Fleischhacker, WW , and Hummer, M . Worsening of psychosis after replacement of adjunctive valproate with topiramate in a schizophrenia patient. J Clin Psychiatry. (2003) 64:1237–1238. doi: 10.4088/jcp.v64n1019c
28. Fitzpatrick, SE , Srivorakiat, L , Wink, LK , Pedapati, EV , and Erickson, CA . Aggression in autism spectrum disorder: presentation and treatment options. Neuropsychiatr Dis Treat. (2016) 12:1525–38. doi: 10.2147/NDT.S84585
29. Fletcher, S , Pawliuk, C , Ip, A , Huh, L , Rassekh, SR , Oberlander, TF, et al. Medicinal cannabis in children and adolescents with autism spectrum disorder: a scoping review. Child Care Health Dev. (2021) 48:33–44. doi: 10.1111/cch.12909
30. Fung, LK , Mahajan, R , Nozzolillo, A , Bernal, P , Krasner, A , Jo, B, et al. Pharmacologic treatment of severe irritability and problem behaviors in autism: a systematic review and Meta-analysis. Pediatrics. (2016) 137:S124–35. doi: 10.1542/peds.2015-2851K
31. Hesami, O , Hosseini, SS , Kazemi, N , Hosseini-Zijoud, S-M , Moghaddam, NB , Assarzadegan, F, et al. Evaluation of ocular side effects in the patients on topiramate therapy for control of migrainous headache. J Clin Diagn Res. (2016) 10:NC01. doi: 10.7860/JCDR/2016/16263.7339
32. Hirota, T , Veenstra-VanderWeele, J , Hollander, E , and Kishi, T . Antiepileptic medications in autism spectrum disorder: a systematic review and meta-analysis. J Autism Dev Disord. (2014) 44:948–57. doi: 10.1007/s10803-013-1952-2
33. Ijff, DM , and Aldenkamp, AP . Cognitive side-effects of antiepileptic drugs in children. Handb Clin Neurol. (2013) 111:707–18. doi: 10.1016/B978-0-444-52891-9.00073-7
34. Koliqi, R , Polidori, C , and Islami, H . Prevalence of side effects treatment with carbamazepine and other antiepileptics in patients with epilepsy. Mater Sociomed. (2015) 27:167. doi: 10.5455/msm.2015.27.167-171
35. Nicolai, J , Smith, S , and Keunen, R . Simultaneous side effects of both clozapine and valproate. Intensive Care Med. (2001) 27:943–3. doi: 10.1007/s001340100937
36. Sahoo, S , Padhy, SK , Singla, N , and Singh, A . Effectiveness of clozapine for the treatment of psychosis and disruptive behaviour in a child with atypical autism: a case report and a brief review of the evidence. Asian J Psychiatr. (2017) 29:194–5. doi: 10.1016/j.ajp.2017.07.012
37. Vasa, RA , Mazurek, MO , Mahajan, R , Bennett, AE , Bernal, MP , Nozzolillo, AA, et al. Assessment and treatment of anxiety in youth with autism Spectrum disorders. Pediatrics. (2016) 137:S115–23. doi: 10.1542/peds.2015-2851J
38. Wood, JR , Nelson-Degrave, VL , Jansen, E , McAllister, JM , Mosselman, S , and Strauss, JF . Valproate-induced alterations in human theca cell gene expression: clues to the association between valproate use and metabolic side effects. Physiol Genomics. (2005) 20:233–43. doi: 10.1152/physiolgenomics.00193.2004
39. Alsayouf, HA , Talo, H , and Biddappa, ML . Core signs and symptoms in children with autism Spectrum disorder improved after starting risperidone and aripiprazole in combination with standard supportive therapies: a large, single-center, retrospective case series. Brain Sci. (2022) 12:50618. doi: 10.3390/brainsci12050618
40. Binici, NC , and Guney, SA . Epistaxis as an unexpected side effect of aripiprazole and risperidone treatment in two children with two different psychiatric diagnosis. J Child Adolesc Psychopharmacol. (2017) 27:759–60. doi: 10.1089/cap.2017.0059
41. Hirsch, LE , and Pringsheim, T . Aripiprazole for autism spectrum disorders (ASD). Cochrane Database Syst Rev. (2016) 2016:CD009043. doi: 10.1002/14651858.CD009043.pub3
42. Kloosterboer, SM , de Winter, BCM , Reichart, CG , Kouijzer, MEJ , de Kroon, MMJ , van Daalen, E, et al. Risperidone plasma concentrations are associated with side effects and effectiveness in children and adolescents with autism spectrum disorder. Br J Clin Pharmacol. (2021) 87:1069–81. doi: 10.1111/bcp.14465
43. Lee, J , Shepperd, R , Smith, M , and Anand, G . Recognising side effects of antipsychotics in children with intellectual disabilities. BMJ Case Rep. (2023) 16:e251974. doi: 10.1136/bcr-2022-251974
44. Mohapatra, S . Extrapyramidal side-effects of low-dose aripiprazole in an 11-year-old child. J Neurosci Rural Pract. (2016) 7:141–2. doi: 10.4103/0976-3147.165355
45. Roke, Y , Buitelaar, JK , Boot, AM , Tenback, D , and van Harten, PN . Risk of hyperprolactinemia and sexual side effects in males 10-20 years old diagnosed with autism spectrum disorders or disruptive behavior disorder and treated with risperidone. J Child Adolesc Psychopharmacol. (2012) 22:432–9. doi: 10.1089/cap.2011.0109
46. Strawn, JR , Mills, JA , Cornwall, GJ , Mossman, SA , Varney, ST , Keeshin, BR, et al. Buspirone in children and adolescents with anxiety: a review and Bayesian analysis of abandoned randomized controlled trials. J Child Adolesc Psychopharmacol. (2018) 28:2–9. doi: 10.1089/cap.2017.0060
47. Ghanizadeh, A , Sahraeizadeh, A , and Berk, M . A head-to-head comparison of aripiprazole and risperidone for safety and treating autistic disorders, a randomized double blind clinical trial. Child Psychiatry Hum Dev. (2014) 45:185–92. doi: 10.1007/s10578-013-0390-x
48. Fieiras, C , Chen, MH , Escobar Liquitay, CM , Meza, N , Rojas, V , Franco, JVA, et al. Risperidone and aripiprazole for autism spectrum disorder in children: an overview of systematic reviews. BMJ Evid Based Med. (2023) 28:7–14. doi: 10.1136/bmjebm-2021-111804
49. Hirota, T , and King, BH . Autism Spectrum disorder: a review. JAMA. (2023) 329:157–68. doi: 10.1001/jama.2022.23661
50. Aran, A , Eylon, M , Harel, M , Polianski, L , Nemirovski, A , Tepper, S, et al. Lower circulating endocannabinoid levels in children with autism spectrum disorder. Mol Autism. (2019) 10:2. doi: 10.1186/s13229-019-0256-6
51. Araujo, DJ , Tjoa, K , and Saijo, K . The endocannabinoid system as a window into microglial biology and its relationship to autism. Front Cell Neurosci. (2019) 13:424. doi: 10.3389/fncel.2019.00424
52. Busquets-Garcia, A , Gomis-Gonzalez, M , Guegan, T , Agustin-Pavon, C , Pastor, A , Mato, S, et al. Targeting the endocannabinoid system in the treatment of fragile X syndrome. Nat Med. (2013) 19:603–7. doi: 10.1038/nm.3127
53. Chakrabarti, B , Persico, A , Battista, N , and Maccarrone, M . Endocannabinoid signaling in autism. Neurotherapeutics. (2015) 12:837–47. doi: 10.1007/s13311-015-0371-9
54. De Pol, M , and Kolla, NJ . Endocannabinoid markers in autism spectrum disorder: a scoping review of human studies. Psychiatry Res. (2021) 306:114256. doi: 10.1016/j.psychres.2021.114256
55. Foldy, C , Malenka, RC , and Sudhof, TC . Autism-associated neuroligin-3 mutations commonly disrupt tonic endocannabinoid signaling. Neuron. (2013) 78:498–509. doi: 10.1016/j.neuron.2013.02.036
56. Fyke, W , Alarcon, JM , Velinov, M , and Chadman, KK . Pharmacological inhibition of the primary endocannabinoid producing enzyme, DGL-alpha, induces autism spectrum disorder-like and co-morbid phenotypes in adult C57BL/J mice. Autism Res. (2021) 14:1375–89. doi: 10.1002/aur.2520
57. Habib, SS , Al-Regaiey, K , Bashir, S , and Iqbal, M . Role of endocannabinoids on Neuroinflammation in autism Spectrum disorder prevention. J Clin Diagn Res. (2017) 11:CE01–3. doi: 10.7860/JCDR/2017/23862.9969
58. Jung, KM , Sepers, M , Henstridge, CM , Lassalle, O , Neuhofer, D , Martin, H, et al. Uncoupling of the endocannabinoid signalling complex in a mouse model of fragile X syndrome. Nat Commun. (2012) 3:1080. doi: 10.1038/ncomms2045
59. Kerr, DM , Downey, L , Conboy, M , Finn, DP , and Roche, M . Alterations in the endocannabinoid system in the rat valproic acid model of autism. Behav Brain Res. (2013) 249:124–32. doi: 10.1016/j.bbr.2013.04.043
60. Krueger, DD , and Brose, N . Evidence for a common endocannabinoid-related pathomechanism in autism spectrum disorders. Neuron. (2013) 78:408–10. doi: 10.1016/j.neuron.2013.04.030
61. Malcher-Lopes, R . Cannabinoids help to unravel etiological aspects in common and bring hope for the treatment of autism and epilepsy. Rev Biol. (2014) 13:43–59. doi: 10.7594/revbio.13.01.07
62. Pietropaolo, S , Bellocchio, L , Bouzon-Arnaiz, I , and Yee, BK . The role of the endocannabinoid system in autism spectrum disorders: evidence from mouse studies. Prog Mol Biol Transl Sci. (2020) 173:183–208. doi: 10.1016/bs.pmbts.2020.04.016
63. Rubino, T , Zamberletti, E , and Parolaro, D . Endocannabinoids and mental disorders. Handb Exp Pharmacol. (2015) 231:261–83. doi: 10.1007/978-3-319-20825-1_9
64. Speed, HE , Masiulis, I , Gibson, JR , and Powell, CM . Increased cortical inhibition in autism-linked Neuroligin-3R451C mice is due in part to loss of endocannabinoid signaling. PLoS One. (2015) 10:e0140638. doi: 10.1371/journal.pone.0140638
65. Thornton, AM , Humphrey, RM , Kerr, DM , Finn, DP , and Roche, M . Increasing endocannabinoid tone alters anxiety-like and stress coping behaviour in female rats prenatally exposed to Valproic acid. Molecules. (2021) 26:3720. doi: 10.3390/molecules26123720
66. Wei, D , Dinh, D , Lee, D , Li, D , Anguren, A , Moreno-Sanz, G, et al. Enhancement of anandamide-mediated endocannabinoid signaling corrects autism-related social impairment. Cannabis Cannabinoid Res. (2016) 1:81–9. doi: 10.1089/can.2015.0008
67. Wu, HF , Lu, TY , Chu, MC , Chen, PS , Lee, CW , and Lin, HC . Targeting the inhibition of fatty acid amide hydrolase ameliorate the endocannabinoid-mediated synaptic dysfunction in a valproic acid-induced rat model of autism. Neuropharmacology. (2020) 162:107736. doi: 10.1016/j.neuropharm.2019.107736
68. Yeh, ML , and Levine, ES . Perspectives on the role of endocannabinoids in autism Spectrum disorders. OBM Neurobiol. (2017) 1:5. doi: 10.21926/obm.neurobiol.1702005
69. Zamberletti, E , Gabaglio, M , and Parolaro, D . The endocannabinoid system and autism Spectrum disorders: insights from animal models. Int J Mol Sci. (2017) 18:1916. doi: 10.3390/ijms18091916
70. Zamberletti, E , Gabaglio, M , Woolley-Roberts, M , Bingham, S , Rubino, T , and Parolaro, D . Cannabidivarin treatment ameliorates autism-like behaviors and restores hippocampal endocannabinoid system and glia alterations induced by prenatal Valproic acid exposure in rats. Front Cell Neurosci. (2019) 13:367. doi: 10.3389/fncel.2019.00367
71. Zou, M , Liu, Y , Xie, S , Wang, L , Li, D , Li, L, et al. Alterations of the endocannabinoid system and its therapeutic potential in autism spectrum disorder. Open Biol. (2021) 11:200306. doi: 10.1098/rsob.200306
72. Aran, A , Cassuto, H , Lubotzky, A , Wattad, N , and Hazan, E . Brief report: Cannabidiol-rich Cannabis in children with autism Spectrum disorder and severe Behavioral problems-a retrospective feasibility study. J Autism Dev Disord. (2019) 49:1284–8. doi: 10.1007/s10803-018-3808-2
73. Aran, A , Harel, M , Cassuto, H , Polyansky, L , Schnapp, A , Wattad, N, et al. Cannabinoid treatment for autism: a proof-of-concept randomized trial. Mol Autism. (2021) 12:6. doi: 10.1186/s13229-021-00420-2
74. Bar-Lev Schleider, L , Mechoulam, R , Saban, N , Meiri, G , and Novack, V . Real life experience of medical Cannabis treatment in autism: analysis of safety and efficacy. Sci Rep. (2019) 9:200. doi: 10.1038/s41598-018-37570-y
75. Barchel, D , Stolar, O , De-Haan, T , Ziv-Baran, T , Saban, N , Fuchs, DO, et al. Oral cannabidiol use in children with autism spectrum disorder to treat related symptoms and co-morbidities. Front Pharmacol. (2019) 9:1521. doi: 10.3389/fphar.2018.01521
76. Fleury-Teixeira, P , Caixeta, FV , Ramires da Silva, LC , Brasil-Neto, JP , and Malcher-Lopes, R . Effects of CBD-enriched Cannabis sativa extract on autism Spectrum disorder symptoms: an observational study of 18 participants undergoing compassionate use. Front Neurol. (2019) 10:1145. doi: 10.3389/fneur.2019.01145
77. Hacohen, M , Stolar, OE , Berkovitch, M , Elkana, O , Kohn, E , Hazan, A, et al. Children and adolescents with ASD treated with CBD-rich cannabis exhibit significant improvements particularly in social symptoms: an open label study. Transl Psychiatry. (2022) 12:375. doi: 10.1038/s41398-022-02104-8
78. Silva, EADJ , Medeiros, WMB , Santos, J , Sousa, JMM , Costa, FBD , Pontes, KM, et al. Evaluation of the efficacy and safety of cannabidiol-rich cannabis extract in children with autism spectrum disorder: randomized, double-blind and controlled placebo clinical trial. Trends Psychiatry Psychother. (2022) 2022:44. doi: 10.47626/2237-6089-2021-0396
79. Bilge, S , and Ekici, B . CBD-enriched cannabis for autism spectrum disorder: an experience of a single center in Turkey and reviews of the literature. J Cannabis Res. (2021) 3:53. doi: 10.1186/s42238-021-00108-7
80. Crippa, JAS , Zuardi, AW , and Hallak, JE . Therapeutical use of the cannabinoids in psychiatry. Braz J Psychiatry. (2010) 32:556–66. doi: 10.1590/S1516-44462010000500009
81. Mostafavi, M , and Gaitanis, J . Autism Spectrum disorder and medical Cannabis: review and clinical experience. Semin Pediatr Neurol. (2020) 35:100833. doi: 10.1016/j.spen.2020.100833
82. Siani-Rose, M , Cox, S , Goldstein, B , Abrams, D , Taylor, M , and Kurek, I . Cannabis-responsive biomarkers: a Pharmacometabolomics-based application to evaluate the impact of medical Cannabis treatment on children with autism Spectrum disorder. Cannabis Cannabinoid Res. (2021) 8:126–37. doi: 10.1089/can.2021.0129
83. Joshi, A , Kale, S , Chandel, S , and Pal, DK . Likert scale: explored and explained. Br J Appl Sci Technol. (2015) 7:396. doi: 10.9734/BJAST/2015/14975
84. Pamplona, FA , da Silva, LR , and Coan, AC . Potential clinical benefits of CBD-rich Cannabis extracts over purified CBD in treatment-resistant epilepsy: observational data Meta-analysis. Front Neurol. (2018) 9:759. doi: 10.3389/fneur.2018.00759
85. Brignell, A , Chenausky, KV , Song, H , Zhu, J , Suo, C , and Morgan, AT . Communication interventions for autism spectrum disorder in minimally verbal children. Cochrane Database Syst Rev. (2018) 11:CD012324. doi: 10.1002/14651858.CD012324.pub2
86. Jobski, K , Höfer, J , Hoffmann, F , and Bachmann, C . Use of psychotropic drugs in patients with autism spectrum disorders: a systematic review. Acta Psychiatr Scand. (2017) 135:8–28. doi: 10.1111/acps.12644
87. Schnitzler, E . The neurology and psychopathology of Pica. Curr Neurol Neurosci Rep. (2022) 22:531–6. doi: 10.1007/s11910-022-01218-2
88. Fields, VL , Soke, GN , Reynolds, A , Tian, LH , Wiggins, L , Maenner, M, et al. Association between pica and gastrointestinal symptoms in preschoolers with and without autism spectrum disorder: study to explore early development. Disabil Health J. (2021) 14:101052. doi: 10.1016/j.dhjo.2020.101052
89. Matson, JL , Hattier, MA , Belva, B , and Matson, ML . Pica in persons with developmental disabilities: approaches to treatment. Res Dev Disabil. (2013) 34:2564–71. doi: 10.1016/j.ridd.2013.05.018
90. Palimaru, I , Guetta, M , Cravero, C , Fron, C , Cohen, D , and Giannitelli, M . Opioid overdose and serotonin syndrome due to gastric bezoar in a woman with autism and Pica behaviour. Case Rep Psychiatry. (2021) 2021:7334467. doi: 10.1155/2021/7334467
91. Bogale, K , Raup-Konsavage, W , Dalessio, S , Vrana, K , and Coates, MD . Cannabis and Cannabis derivatives for abdominal pain Management in Inflammatory Bowel Disease. Med Cannabis Cannabinoids. (2021) 4:97–106. doi: 10.1159/000517425
92. Carvalho, ACA , Souza, GA , Marqui, SV , Guiguer, EL , Araujo, AC , Rubira, CJ, et al. Cannabis and Canabidinoids on the inflammatory bowel diseases: going beyond misuse. Int J Mol Sci. (2020) 21:2940. doi: 10.3390/ijms21082940
93. Farinon, B , Molinari, R , Costantini, L , and Merendino, N . The seed of industrial hemp (Cannabis sativa L.): nutritional quality and potential functionality for human health and nutrition. Nutrients. (2020) 12:1935. doi: 10.3390/nu12071935
94. Grill, M , Hasenoehrl, C , Storr, M , and Schicho, R . Medical Cannabis and cannabinoids: an option for the treatment of inflammatory bowel disease and Cancer of the Colon? Med Cannabis Cannabinoids. (2018) 1:28–35. doi: 10.1159/000489036
95. Iftikhar, A , Zafar, U , Ahmed, W , Shabbir, MA , Sameen, A , Sahar, A, et al. Applications of Cannabis sativa L. in food and its therapeutic potential: from a prohibited drug to a nutritional supplement. Molecules. (2021) 26:7699. doi: 10.3390/molecules26247699
96. Izzo, AA , Capasso, R , Aviello, G , Borrelli, F , Romano, B , Piscitelli, F, et al. Inhibitory effect of cannabichromene, a major non-psychotropic cannabinoid extracted from Cannabis sativa, on inflammation-induced hypermotility in mice. Br J Pharmacol. (2012) 166:1444–60. doi: 10.1111/j.1476-5381.2012.01879.x
97. Naftali, T , Mechulam, R , Lev, LB , and Konikoff, FM . Cannabis for inflammatory bowel disease. Dig Dis. (2014) 32:468–74. doi: 10.1159/000358155
98. Wallace, JL , Flannigan, KL , McKnight, W , Wang, L , Ferraz, JG , and Tuitt, D . Pro-resolution, protective and anti-nociceptive effects of a cannabis extract in the rat gastrointestinal tract. J Physiol Pharmacol. (2013) 64:167–75. doi: 10.1111/jpn.13557
99. Vastolo, A , Calabro, S , Pacifico, S , Koura, BI , and Cutrignelli, MI . Chemical and nutritional characteristics of Cannabis sativa L. co-products. J Anim Physiol Anim Nutr (Berl) 105 Suppl. (2021) 1:1–9. doi: 10.1111/jpn.13557
100. Zamarripa, CA , Spindle, TR , Surujunarain, R , Weerts, EM , Bansal, S , Unadkat, JD, et al. Assessment of orally administered delta9-tetrahydrocannabinol when coadministered with Cannabidiol on Delta9-tetrahydrocannabinol pharmacokinetics and pharmacodynamics in healthy adults: a randomized clinical trial. JAMA Netw Open. (2023) 6:e2254752. doi: 10.1001/jamanetworkopen.2022.54752
101. Casseus, M , Kim, WJ , and Horton, DB . Prevalence and treatment of mental, behavioral, and developmental disorders in children with co-occurring autism spectrum disorder and attention-deficit/hyperactivity disorder: a population-based study. Autism Res. (2023) 16:855–67. doi: 10.1002/aur.2894
102. Schachar, RJ , Dupuis, A , Arnold, PD , Anagnostou, E , Kelley, E , Georgiades, S, et al. Autism Spectrum disorder and attention-deficit/hyperactivity disorder: shared or unique neurocognitive profiles? Res Child Adolesc Psychopathol. (2023) 51:17–31. doi: 10.1007/s10802-022-00958-6
103. Vaidya, CJ , and Klein, C . Comorbidity of attention-deficit hyperactivity disorder and autism Spectrum disorders: current status and promising directions. Curr Top Behav Neurosci. (2022) 57:159–77. doi: 10.1007/7854_2022_334
104. Zhang, M , Huang, Y , Jiao, J , Yuan, D , Hu, X , Yang, P, et al. Transdiagnostic symptom subtypes across autism spectrum disorders and attention deficit hyperactivity disorder: validated by measures of neurocognition and structural connectivity. BMC Psychiatry. (2022) 22:102. doi: 10.1186/s12888-022-03734-4
105. Antshel, KM , and Russo, N . Autism Spectrum disorders and ADHD: overlapping phenomenology, diagnostic issues, and treatment considerations. Curr Psychiatry Rep. (2019) 21:34. doi: 10.1007/s11920-019-1020-5
106. Visser, JC , Rommelse, NNJ , Lappenschaar, M , Servatius-Oosterling, IJ , Greven, CU , and Buitelaar, JK . Variation in the early trajectories of autism symptoms is related to the development of language, cognition, and behavior problems. J Am Acad Child Adolesc Psychiatry. (2017) 56:659–68. doi: 10.1016/j.jaac.2017.05.022
107. Raz, N , Heller, I , Lombardi, T , Marino, G , Davidson, EM , and Eyal, AM . Terpene-enriched CBD oil for treating autism-derived symptoms unresponsive to pure CBD: case report. Front Pharmacol. (2022) 13:979403. doi: 10.3389/fphar.2022.979403
108. Ma, L , Platnick, S , and Platnick, H . Cannabidiol in treatment of autism Spectrum disorder: a case study. Cureus. (2022) 14:e28442. doi: 10.7759/cureus.28442
109. Di Bartolomeo, M , Stark, T , Maurel, OM , Iannotti, FA , Kuchar, M , Ruda-Kucerova, J, et al. Crosstalk between the transcriptional regulation of dopamine D2 and cannabinoid CB1 receptors in schizophrenia: analyses in patients and in perinatal Delta9-tetrahydrocannabinol-exposed rats. Pharmacol Res. (2021) 164:105357. doi: 10.1016/j.phrs.2020.105357
110. Stark, T , Di Martino, S , Drago, F , Wotjak, CT , and Micale, V . Phytocannabinoids and schizophrenia: focus on adolescence as a critical window of enhanced vulnerability and opportunity for treatment. Pharmacol Res. (2021) 174:105938. doi: 10.1016/j.phrs.2021.105938
111. Stark, T , Ruda-Kucerova, J , Iannotti, FA , D'Addario, C , Di Marco, R , Pekarik, V, et al. Peripubertal cannabidiol treatment rescues behavioral and neurochemical abnormalities in the MAM model of schizophrenia. Neuropharmacology. (2019) 146:212–21. doi: 10.1016/j.neuropharm.2018.11.035
112. Liu, X , Kumar, V , Tsai, NP , and Auerbach, BD . Hyperexcitability and homeostasis in fragile X syndrome. Front Mol Neurosci. (2021) 14:805929. doi: 10.3389/fnmol.2021.805929
113. Markram, K , and Markram, H . The intense world theory - a unifying theory of the neurobiology of autism. Front Hum Neurosci. (2010) 4:224. doi: 10.3389/fnhum.2010.00224
114. Cao, X , and Tabuchi, K . Functions of synapse adhesion molecules neurexin/neuroligins and neurodevelopmental disorders. Neurosci Res. (2017) 116:3–9. doi: 10.1016/j.neures.2016.09.005
115. Kwon, CS , Wirrell, EC , and Jette, N . Autism Spectrum disorder and epilepsy. Neurol Clin. (2022) 40:831–47. doi: 10.1016/j.ncl.2022.03.011
116. Chez, MG , Chang, M , Krasne, V , Coughlan, C , Kominsky, M , and Schwartz, A . Frequency of epileptiform EEG abnormalities in a sequential screening of autistic patients with no known clinical epilepsy from 1996 to 2005. Epilepsy Behav. (2006) 8:267–71. doi: 10.1016/j.yebeh.2005.11.001
117. Costa, AM , Senn, L , Anceschi, L , Brighenti, V , Pellati, F , and Biagini, G . Antiseizure effects of fully characterized non-psychoactive Cannabis sativa L. extracts in the repeated 6-Hz corneal stimulation test. Pharmaceuticals (Basel). (2021) 14:1259. doi: 10.3390/ph14121259
118. do Val-da Silva, RA , Peixoto-Santos, JE , Kandratavicius, L , de Ross, JB , Esteves, I , de Martinis, BS, et al. Protective effects of Cannabidiol against seizures and neuronal death in a rat model of mesial temporal lobe epilepsy. Front Pharmacol. (2017) 8:131. doi: 10.3389/fphar.2017.00131
119. Zirotti Rosenberg, A , Mendez-Ruette, M , Gorziglia, M , Alzerreca, B , Cabello, J , Kaufmann, S, et al. Behavioral and molecular responses to exogenous cannabinoids during Pentylenetetrazol-induced convulsions in Male and female rats. Front Mol Neurosci. (2022) 15:868583. doi: 10.3389/fnmol.2022.868583
120. Siniscalco, D , Sapone, A , Giordano, C , Cirillo, A , de Magistris, L , Rossi, F, et al. Cannabinoid receptor type 2, but not type 1, is up-regulated in peripheral blood mononuclear cells of children affected by autistic disorders. J Autism Dev Disord. (2013) 43:2686–95. doi: 10.1007/s10803-013-1824-9
121. Karhson, DS , Krasinska, KM , Dallaire, JA , Libove, RA , Phillips, JM , Chien, AS, et al. Plasma anandamide concentrations are lower in children with autism spectrum disorder. Mol Autism. (2018) 9:18. doi: 10.1186/s13229-018-0203-y
122. Servadio, M , Melancia, F , Manduca, A , di Masi, A , Schiavi, S , Cartocci, V, et al. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl Psychiatry. (2016) 6:e902. doi: 10.1038/tp.2016.182
123. Martini, S , Gemma, A , Ferrari, M , Cosentino, M , and Marino, F . Effects of Cannabidiol on innate immunity: experimental evidence and clinical relevance. Int J Mol Sci. (2023) 24:3125. doi: 10.3390/ijms24043125
124. Abruzzo, PM , Matte, A , Bolotta, A , Federti, E , Ghezzo, A , Guarnieri, T, et al. Plasma peroxiredoxin changes and inflammatory cytokines support the involvement of neuro-inflammation and oxidative stress in autism Spectrum disorder. J Transl Med. (2019) 17:332. doi: 10.1186/s12967-019-2076-z
125. Li, YJ , Zhang, X , and Li, YM . Antineuroinflammatory therapy: potential treatment for autism spectrum disorder by inhibiting glial activation and restoring synaptic function. CNS Spectr. (2020) 25:493–501. doi: 10.1017/S1092852919001603
126. Roe, K . Autism Spectrum disorder initiation by inflammation-facilitated neurotoxin transport. Neurochem Res. (2022) 47:1150–65. doi: 10.1007/s11064-022-03527-x
127. Akyuz, E , Koklu, B , Ozenen, C , Arulsamy, A , and Shaikh, MF . Elucidating the potential side effects of current anti-seizure drugs for epilepsy. Curr Neuropharmacol. (2021) 19:1865–83. doi: 10.2174/1570159X19666210826125341
128. Espadas, C , Ballester, P , Londoño, AC , Almenara, S , Aguilar, V , Belda, C, et al. Multimorbidity and psychotropic polypharmacy among participants with autism spectrum disorder with intellectual disability. Psychiatry Res. (2020) 292:113321. doi: 10.1016/j.psychres.2020.113321
129. Hellings, JA , Jadhav, M , Jain, S , Jadhav, S , and Genovese, A . Low dose Loxapine: Neuromotor side effects and tolerability in autism Spectrum disorders. J Child Adolesc Psychopharmacol. (2015) 25:618–24. doi: 10.1089/cap.2014.0145
130. Heming, SM , and Olsen, KE . Significant extrapyramidal side effects on low-dose aripiprazole. Prim Care Companion CNS Disord. (2022) 24:21cr03060. doi: 10.4088/PCC.21cr03060
131. Konrad-Bindl, DS , Gresser, U , and Richartz, BM . Changes in behavior as side effects in methylphenidate treatment: review of the literature. Neuropsychiatr Dis Treat. (2016) 12:2635–47. doi: 10.2147/NDT.S114185
132. Lee, J , Grizenko, N , Bhat, V , Sengupta, S , Polotskaia, A , and Joober, R . Relation between therapeutic response and side effects induced by methylphenidate as observed by parents and teachers of children with ADHD. BMC Psychiatry. (2011) 11:70. doi: 10.1186/1471-244X-11-70
133. Lilja, MM , Sandblom, E , Lichtenstein, P , Serlachius, E , Hellner, C , Bhagia, J, et al. The effect of autistic traits on response to and side-effects of pharmacological ADHD treatment in children with ADHD: results from a prospective clinical cohort. J Neurodev Disord. (2022) 14:17. doi: 10.1186/s11689-022-09424-2
134. Muit, JJ , Bothof, N , and Kan, CC . Pharmacotherapy of ADHD in adults with autism Spectrum disorder: effectiveness and side effects. J Atten Disord. (2020) 24:215–25. doi: 10.1177/1087054719866255
135. Rapport, MD , and Moffitt, C . Attention deficit/hyperactivity disorder and methylphenidate. A review of height/weight, cardiovascular, and somatic complaint side effects. Clin Psychol Rev. (2002) 22:1107–31. doi: 10.1016/S0272-7358(02)00129-0
136. Ritter, C , Hewitt, K , and McMorris, CA . Psychotropic polypharmacy among children and youth with autism: a systematic review. J Child Adolesc Psychopharmacol. (2021) 31:244–58. doi: 10.1089/cap.2020.0110
137. Spencer, D , Marshall, J , Post, B , Kulakodlu, M , Newschaffer, C , Dennen, T, et al. Psychotropic medication use and polypharmacy in children with autism spectrum disorders. Pediatrics. (2013) 132:833–40. doi: 10.1542/peds.2012-3774
138. Vohra, R , Madhavan, S , Sambamoorthi, U , StPeter, C , Poe, S , Dwibedi, N, et al. Prescription drug use and polypharmacy among Medicaid-enrolled adults with autism: a retrospective cross-sectional analysis. Drugs Real World Outcomes. (2016) 3:409–25. doi: 10.1007/s40801-016-0096-z
Keywords: endocannabinoid system, Pica, allotriophagy, Cannabis sativa , CBD, THC, patient-reported outcome survey, autism spectrum disorders
Citation: Montagner PSS, Medeiros W, da Silva LCR, Borges CN, Brasil-Neto J, de Deus Silva Barbosa V, Caixeta FV and Malcher-Lopes R (2023) Individually tailored dosage regimen of full-spectrum Cannabis extracts for autistic core and comorbid symptoms: a real-life report of multi-symptomatic benefits. Front. Psychiatry. 14:1210155. doi: 10.3389/fpsyt.2023.1210155
Edited by:
Debra Karhson, University of New Orleans, United StatesReviewed by:
Barış Ekici, Zatay Pediatric Neurology Clilnic, TürkiyeCopyright © 2023 Montagner, Medeiros, da Silva, Borges, Brasil-Neto, de Deus Silva Barbosa, Caixeta and Malcher-Lopes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renato Malcher-Lopes, bWFsY2hlcmxvcGVzQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.