 Omid Massah
Omid Massah Amir Masoud Arab2*
Amir Masoud Arab2* Ali Farhoudian
Ali Farhoudian Mehdi Noroozi
Mehdi Noroozi Fahimeh Hashemirad
Fahimeh Hashemirad- 1Substance Abuse and Dependence Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
- 2Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
- 3Department of Psychiatry, Tehran University of Medical Sciences, Tehran, Iran
- 4Department of Psychiatry, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
- 5Psychosis Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
Objectives: Opium smoking is commonly practiced via traditional and novel routes in Iran. Both smoking methods are practiced in a non-ergonomic position. According to previous studies and our hypothesis, it can be potentially harmful to the cervical spine. Thus, the present study aimed to investigate the relationship between opium smoking and neck range of motion and neck muscle strength.
Methods: In this cross-sectional and correlational study, the range of motion and strength of the neck muscles of 120 men with drug use disorder were measured by a CROM goniometer and a hand-held dynamometer. Other data gathering was performed using a demographic questionnaire, the Maudsley Addiction Profile, and the Persian version of Leeds Dependence Questionnaire. The obtained data were analyzed by Shapiro–Wilks test, Pearson’s correlation coefficient and stepwise linear regression.
Results: There was no significant correlation between the age of drug use onset and range of motion and muscle strength of the neck; however, the daily duration of opium smoking and the number of years of opium smoking were inversely and significantly correlated with the range of motion and muscle strength of the neck in some directions. Daily opium smoking time for decreasing in neck range of motion and total duration of opium smoking for reduction of neck muscles strength are stronger predictor variables.
Conclusion: Opium smoking by traditional routes causes non-ergonomic positions and has a moderate significant correlation with reduced range of motion and neck muscle strength, in Iran.
Highlights: – The harm of drug use disorder is not only AIDS and hepatitis, and harm reduction programs should go beyond the prevention of AIDS and hepatitis. According to more than 90% of smoking use of drug compared to other methods (oral and injectable, etc.) musculoskeletal disorders caused by the smoking use of drugs, have a greater cost burden in reducing the quality of life and the need for rehabilitation. – Drug abuse treatment and harm reduction programs should focus more seriously on replacing smoking use of drugs with oral medications assisted treatment. – Although in Iran and some countries in the region, a large number of people smoke opium for many years and sometimes all their lives, daily in a completely non-ergonomic position, but studying the deformation of the posture and musculoskeletal disorders related to the body position in them, is not a scientific concern and neither physical therapy researchers have paid attention to it nor addiction researchers. – Neck muscles strength and range of motion in opium addicts are correlated to the number of years of opium smoking and daily minutes of opium smoking, but not to its oral use. – There is no significant correlation between the onset age of continues and permanent opium smoking and substance dependence severity with neck range of motion and muscles strength. – People with drug use disorder (especially smoking users) as a large group of vulnerable people, should be the target population of musculoskeletal disorders researchers and addiction harm reduction researchers, and more experimental, comparative, cohort, etc. researches should be designed and implemented for them.
– The harm of drug use disorder is not only AIDS and hepatitis, and harm reduction programs should go beyond the prevention of AIDS and hepatitis. According to more than 90% of smoking use of drug compared to other methods (oral and injectable, etc.) musculoskeletal disorders caused by the smoking use of drugs, have a greater cost burden in reducing the quality of life and the need for rehabilitation.
– Drug abuse treatment and harm reduction programs should focus more seriously on replacing smoking use of drugs with oral medications assisted treatment.
– Although in Iran and some countries in the region, a large number of people smoke opium for many years and sometimes all their lives, daily in a completely non-ergonomic position, but studying the deformation of the posture and musculoskeletal disorders related to the body position in them, is not a scientific concern and neither physical therapy researchers have paid attention to it nor addiction researchers.
– Neck muscles strength and range of motion in opium addicts are correlated to the number of years of opium smoking and daily minutes of opium smoking, but not to its oral use.
– There is no significant correlation between the onset age of continues and permanent opium smoking and substance dependence severity with neck range of motion and muscles strength.
– People with drug use disorder (especially smoking users) as a large group of vulnerable people, should be the target population of musculoskeletal disorders researchers and addiction harm reduction researchers, and more experimental, comparative, cohort, etc. researches should be designed and implemented for them.
Introduction
The physical posture of individuals is generated by their movement habits. Moreover, it is formed on a morphological and functional basis and is a manifestation of the individual’s physical and mental conditions (1). Therefore, it is an indicator of one’s kinetic status, as well as muscle balance and neuromuscular coordination. The human body condition is influenced by changes throughout life. In fact, posture visibly echoes musculoskeletal activity (2, 3). Modern urban life is associated with rapid changes in the environment, lifestyle, physical activity restrictions, and improper nutrition (4). Despite numerous preventive and protective measures, many health problems are caused by the contemporary world’s lifestyle (5).
As long as corrective action is not taken to improve posture, its adverse effects on the body will continue and postural pressure will be imposed on the person. Accordingly, the odds of musculoskeletal disorders related to work or non-ergonomic position remains high (3). Performing repetitive tasks in incorrect posture and non-neutral position leads to postural strain, fatigue, and pain (6). In such positions, the muscles bear further load and are exposed to damage along with the surrounding connective tissues. If continued and repetitive, these positions can lead to irreversible changes in the form of shortening or stretching of muscle fibers and soft tissues (advancing from the elasticity stage to the plasticity phase) (7, 8). Therefore, being in certain recurrent positions over days and hours leads to alternations in the musculoskeletal system. In addition, such cases have been proven in various operations and sports activities (9, 10). Considering the high prevalence of musculoskeletal disorders in today’s societies (11), investigating the prevalence of these conditions and the factors affecting them in diverse age groups, genders, occupations, etc., is an essential area of research in rehabilitation. The smoking of opium is common in traditional (using a device called Vafour) and novel (using a type of hookah called in Iran “Gholgholei” or using spoke and pin called in Iran “Sikh-o-sang”) methods in Iran. Furthermore, as both methods are a non-ergonomic position, individuals with opium use disorder who consume via smoking route are more prone to some musculoskeletal disorders. This issue can be attributed to long-term exposure to non-ergonomic positions during consumption, as well as the lack of movement, malnutrition, and unhygienic conditions, heavy smoking, and so on (12–14). Opium smoking is not common in other regions. In European and American countries, heroin and marijuana are mainly smoked, and their smoking time is very short, compared to opium; therefore, this issue has not been a research priority in Europe and America. Opium smoking is very common in the Middle East and especially in Iran (15). In addition, its use has increased after the onset of Coronavirus Disease 2019 (COVID-19) pandemic (due to the false belief that opium use can prevent the spread of COVID-19) (16). Iran has the highest prevalence rate of opium smoking in proportion to the population globally (17), Thus, this study aimed to investigate the relationship between the Range of Motion (ROM) of the neck and its muscle strength and opium smoking and the severity of opium use disorder.
Methods
This cross-sectional and correlation study was conducted in 2021 in Tehran City, Iran. By snowball sampling method, we selected 120 men from four main branches according to the inclusion and exclusion criteria of the study among the referrals to four outpatient and residential substance abuse treatment centers.
The inclusion criteria were as follows: a diagnosis of substance use disorder according to the International Classification of Diseases-11th Revision (ICD-11) criteria (18), ability to stand, age between 25 and 50 years, Body Mass Index (BMI) below 27.5 kg/m2 (there are lower probabilities of musculoskeletal disorders in these age and BMI ranges). Also, the exclusion criteria were a history of neuromuscular or skeletal disease, a history of surgery in spine and shoulder girdle areas, a history of championship or practicing sports regularly, any impairments in balance control caused by a specific disease, any obvious postural deformities and anatomical disorders, and using smartphones and tablets for more than 30 min a day (19).
Data collection was performed using demographic questionnaire, Maudsley Addiction Profile (MAP) (20) and Persian version of Leeds Dependence Questionnaire (LDQ) (21). The maximal isometric strength of flexor, extensor, and lateral flexor muscles of the neck (MVIC) was measured by a hand-held dynamometer (Model: Micro Manual Muscle Tester; North Coast Medical Inc.). Before starting the measurement, the device was calibrated using standard weights. The dynamometer was programmed for 7 s, and after placing the device on the head, the person increased the contraction force of the muscle within 2 s to reach the maximum contraction force, and then kept it in the same position for 5 s. All tests were performed once (due to the odds of encountering fatigue in repetitions and associations distorted results) and the data obtained from the strength measurement tests were normalized to the BMI of the study subjects. The neck ROM was calculated using a cervical inclinometer (Model: Baseline CROM-3 goniometer), while the subject was sitting on a chair and the chest was tied to the chair support with a tight band.
To confirm the reliability of the measurement method, 10 subjects participated in an extra four testing sessions of neck muscle strength and ROM test in 2 weeks.
Statistical analysis was done by SPSS software version 23 through Shapiro–Wilk test, correlation coefficient tests (ANOVA and Pearson) and stepwise linear regression.
The study has been approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences with the code of IR.USWR.REC.1398.120. This article is extracted from doctoral thesis of the first author.
Results
The mean ± SD age of the study participants was 39.30 ± 5.05 years and their mean BMI score was 24.29 ± 2.12 kg/m2. 53 people were workers, 58 people were employees, and the rest were unemployed. Also, 37 people had primary education, 68 people had high school education, seven people had university education, and the rest were illiterate. The substance use profile of the study participants is available in Table 1.
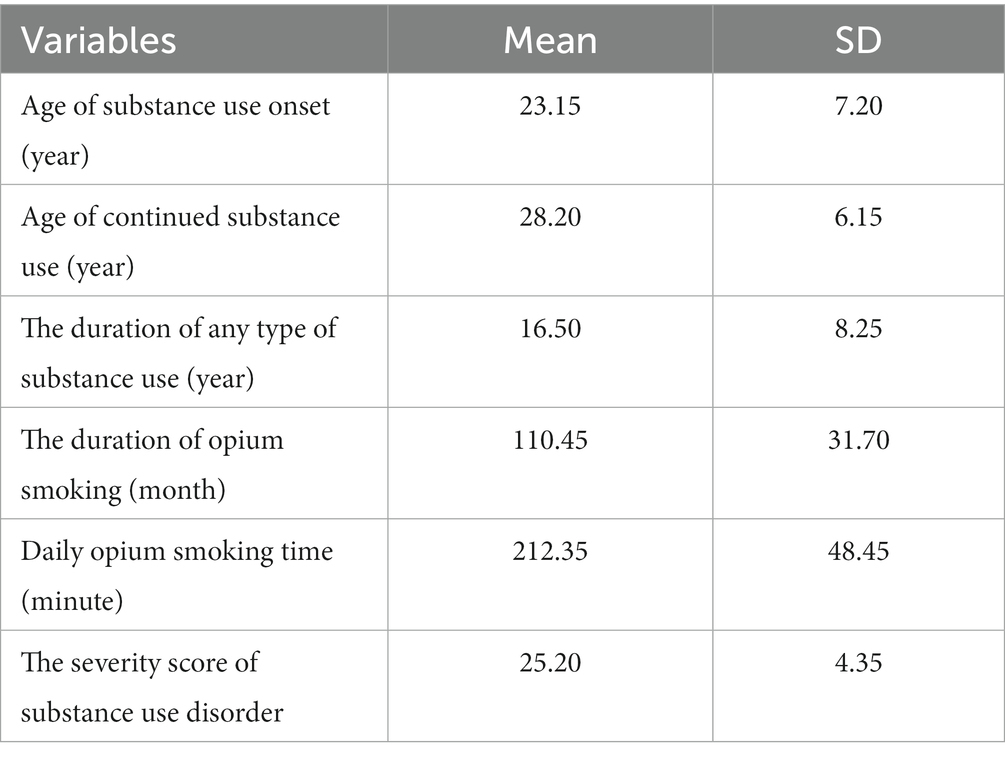
Table 1. Substance use profile of participants.
The results of inter-rater and intra-rater reliability tests suggested that the measurement methods were reliable. For inter-rater reliability, the Intraclass Correlation Coefficients (ICCs) ranged from 0.6 (CI: 0.18–0.86) for measuring the range of left lateral flexion to 0.88 (CI: 0.64–0.95) for forward flexion; regarding muscle strength, ICCs ranged from 0.64 (CI: 0.22–0.91) for extension to 0.92 (CI: 0.66–0.97) for forward flexion. For intra-rater reliability, the ICCs ranged from 0.68 (CI: 0.20–0.90) for right lateral flexion to 0.94 (CI: 0.86–0.98) for extension; and in muscle strength ICCs, they ranged from 0.68 (CI: 0.20–0.89) for left lateral flexion to 0.9 (CI: 0.65–0.93) for extension.
There was no significant relationship between the onset age of permanent opium smoking and the ROM of the neck. However, a significant correlation was recorded between the opium smoking duration (months/lifetime) and daily opium smoking time (minutes/day), and the ROM of the neck in most directions (Table 2).

Table 2. Correlation coefficients of neck range of motion with the age of starting permanent opium smoking, drug dependence severity, daily opium smoking duration, and life opium smoking duration.
Furthermore, as per Table 3, the maximum contraction strength of the neck muscles were significantly and inversely correlated with the opium smoking duration (months/lifetime) and daily opium smoking duration (minutes/day).

Table 3. Correlation coefficients of neck muscles strength with the age of starting permanent opium smoking, drug dependence severity, daily opium smoking duration and life opium smoking duration.
In order to determine the most effective independent variable in decreasing the range of motion and muscles strength of neck, stepwise regression analysis was used. For this purpose, the average of the total range of motion of the neck in all six directions was calculated for each participant and considered as a unique index of the range of motion of the neck. Also, average muscle strength in four directions was used as an index of neck muscle strength in regression analysis. As shown in Table 4, opium smoking duration (month) is the first predictive variable for the possibility of decreased neck muscles strength and daily opium smoking time (minute) for decrease in neck range of motion. According to the results of the regression analysis, daily opium smoking time predicts the reduction of neck range of motion. According to these results, it predicts 10% of decreasing the range of motion of neck and the sum of the two predictive variables (daily opium smoking time and opium smoking duration) predicts 16%. 13% of the decrease in the strength of the neck muscles can be predicted by the duration of opium smoking and 17% by the sum of the opium smoking duration and daily opium smoking time.
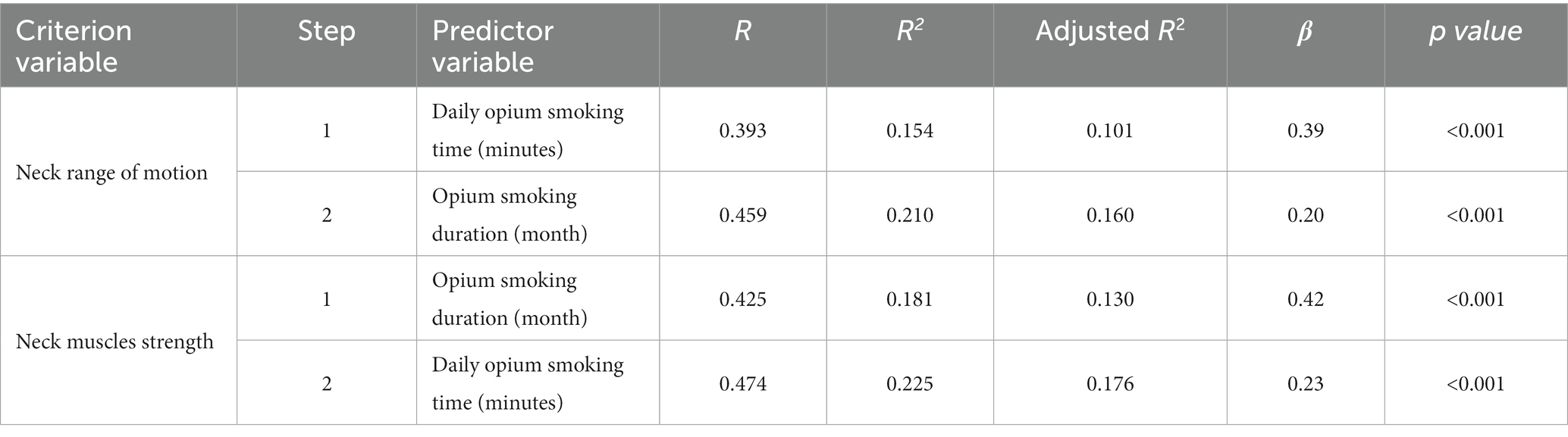
Table 4. Stepwise regression analysis for neck range of motion and neck muscles strength (criterion variable) based on predictor variables.
Discussion
Perhaps in recent decades, the most serious complication and the riskiest consequence of substance use disorder is the transmission of Human Immunodeficiency Virus (HIV) and hepatitis viruses to substance users, through injection drug use. However, it is certainly not the most frequent issue, especially if we consider the harms associated with substance use disorder regionally and the most common route of substance use in that region (17). For example, in Iran, on the one hand, the use of injectable drugs was greatly reduced by starting an opioid maintenance treatment program with agonist medications (22, 23). On the other hand, the use of smoking drugs, especially opium smoking, is traditionally and historically very common (15). Moreover, its prevalence increased due to the COVID-19 pandemic (16). Therefore, the harm of substance use disorder is no longer limited to HIV and Hepatitis contradiction. Thus, depending on the specific geographical region, the scope of harm reduction programs should be expanded. Musculoskeletal-related adverse effects of substance smoking, i.e., caused by long-term placement in non-ergonomic positions, are prevalent disorders. Subsequently, if not taken into account in prevention and harm reduction programs, such conditions can exorbitant rehabilitation costs.
Many people, depending on their habit or work needs, foster an inappropriate body position, which causes postural pains in the long term. Each individual, depending on the type of practiced physical or sports activities, is prone to certain types of mild postural abnormalities or deviations, i.e., suitable for that activity at that given time (24, 25). However, over years of repetition, these postural deviations may lead to a wide range of disorders (26). This is why disabled people who use a computer head controller have reduced neck ROM and neck muscles strength in some directions, which correlates with their head movement habits (27). Obviously, the unusual neck movements and non-ergonomic positions performed during opium smoking are related and consistent with the opium smoking duration (minutes per day) and the years of overall course of opium smoking. In this study, there was an inverse and significant correlation between the ROM and muscles strength of the neck in most directions with the increase in the duration of opium smoking. To some extent, these findings are in line with those of Ghamkhar’s study. In their study, although the performance of the neck muscles did not reveal a relationship with forward head posture and even neck pain and disability (in patients with chronic neck pain), the reduction in endurance and strength of the neck muscles was associated with some postural deformities (28). These findings are also in line with the results of studies conducted on dentists. Because dentists also work in the same harmful position for several hours a day, and the reduction of function and mobility of the neck and the strength of the neck muscles and decreasing in neck range of motion has been proven in many studies (29–31).
Posture deformities, i.e., mostly acquired and caused by non-ergonomic positions, are related to the ROM of the neck (32, 33). As per the study of Quek et al., there was a significant correlation between thoracic hyperkyphosis and forward head posture, and the ROM of the neck (34); these results are in line with those obtained in this study. A large body of literature has reported a relationship between repetitive work positions and the use of upper body and upper limbs when operating with work tools, and the occurrence of musculoskeletal disorders of the neck (35). Opium smoking tools also force the user to hold this position for several hours a day. As a result, after years, the risk of such conditions, as reduced ROM of the neck and declined strength of the neck muscles is not far from expected. In a similar way and with the same mechanism, welders and many workers in other industries suffer from reduced neck range of motion (36, 37). Decreasing in neck muscles strength due to non-ergonomic positions of opium smoking is similar to what happens in industries workers (38).
Furthermore, previous studies indicated a correlation between psychosocial characteristics and mental health confounders as well as the incidence of musculoskeletal disorders; the results of this study are in line with these prior investigations. This is because substance use disorder is among the main psychosocial health disorders in today’s societies (39, 40).
Limitations and suggestions
The main limitation of this study was the lack of previous similar studies and the literature review was not very helpful. I hope this study will draw the attention of researchers and policymakers to the allocation of funds and efforts for this issue, and will make them document more convincing results with more extensive studies and with more accurate scientific and experimental methods. Another limitation of this study was that the samples were only male. Although we did not intend to do so from the beginning, we had to use only men.
Conclusion
The traditional and novel methods of opium smoking, which are used in the Persian Gulf countries, the Middle East, Central Asia, and even the countries of East Asia, and require sitting in non-ergonomic positions for long hours, have a significant correlation with neck problems and it seems to be effective in reducing muscle strength and range of motion of neck.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences with the code of IR.USWR.REC.1398.120. This article is extracted from doctoral thesis of the OM in PhD by Research of Addiction Studies. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Data gathering and data analysis were done by OM. OM, AA, AF, MN, and FH contributed to design, drafting, and writing and editing of the article. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. van Balen, LC, Dijkstra, LJ, and Hadders-Algra, M. Development of postural adjustments during reaching in typically developing infants from 4 to 18 months. Exp Brain Res. (2012) 220:109–19. doi: 10.1007/s00221-012-3121-9
2. Skelton, DA . Effects of physical activity on postural stability. Age Ageing. (2001) 30:33–9. doi: 10.1093/ageing/30.suppl_4.33
3. Karwowski, W, and Zhang, W. The discipline of human factors and ergonomics In: G. Salvendy and W. Karwowski, editors. Handbook Of Human Factors and Ergonomics (2021). 1–37.
4. Seefeldt, V, Malina, RM, and Clark, MA. Factors affecting levels of physical activity in adults. Sports Med. (2002) 32:143–68. doi: 10.2165/00007256-200232030-00001
5. de Assis, SJC, Sanchis, GJB, de Souza, CG, and Roncalli, AG. Influence of physical activity and postural habits in schoolchildren with scoliosis. Archiv Public Health. (2021) 79:63. doi: 10.1186/s13690-021-00584-6
6. Haslegrave, CM . What do we mean by a ‘working posture’? Ergonomics. (1994) 37:781–99. doi: 10.1080/00140139408963688
7. Kumar, S . Selected theories of musculoskeletal injury causation In: S Kumar , editor. Biomechanics in Ergonomics. UK, London: Taylor & Francis (1999). 3–24.
8. Niu, S . Ergonomics and occupational safety and health: an ILO perspective. Appl Ergon. (2010) 41:744–53. doi: 10.1016/j.apergo.2010.03.004
9. Gallagher, S . Physical limitations and musculoskeletal complaints associated with work in unusual or restricted postures: a literature review. J Saf Res. (2005) 36:51–61. doi: 10.1016/j.jsr.2004.12.001
10. Grabara, M . Comparison of posture among adolescent male volleyball players and non-athletes. Biol Sport. (2015) 32:79–85. doi: 10.5604/20831862.1127286
11. Woolf, AD, and Akesson, K. Understanding the burden of musculoskeletal conditions. The burden is huge and not reflected in national health priorities. BMJ. (2001) 322:1079–80. doi: 10.1136/bmj.322.7294.1079
12. Muller, AE, Skurtveit, S, and Clausen, T. Many correlates of poor quality of life among substance users entering treatment are not addiction-specific. Health Qual Life Outcomes. (2016) 14:39. doi: 10.1186/s12955-016-0439-1
13. Mahboub, N, Rizk, R, Karavetian, M, and de Vries, N. Nutritional status and eating habits of people who use drugs and/or are undergoing treatment for recovery: a narrative review. Nutr Rev. (2020) 79:627–35. doi: 10.1093/nutrit/nuaa095
14. Al-Bashaireh, AM, Haddad, LG, Weaver, M, Kelly, DL, Chengguo, X, and Yoon, S. The effect of tobacco smoking on musculoskeletal health: a systematic review. J Environ Public Health. (2018) 2018:1–106. doi: 10.1155/2018/4184190
15. Zarghami, M . Iranian common attitude toward opium consumption. Iran J Psychiatry Behav Sci. (2015) 9:e2074. doi: 10.17795/ijpbs2074
16. Mahdavi, A, and Aliramezany, M. Addiction and Covid-19 disease: risks and misconceptions. Addict Health. (2021) 13:66–7. doi: 10.22122/ahj.v13i1.279
17. UNODC (2022). World Drug Report 2022. Vienna, Austria: (United Nations publication, 2022). Available at: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2022.html
18. Poznyak, V, Reed, GM, and Medina-Mora, ME. Aligning the ICD-11 classification of disorders due to substance use with global service needs. Epidemiol Psychiatr Sci. (2018) 27:212–8. doi: 10.1017/S2045796017000622
19. Neupane, S, Ali, U, and Mathew, A. Text neck syndrome-systematic review. Imp J Interdiscip Res. (2017) 3:141–8.
20. Marsden, J, Gossop, M, Stewart, D, Best, D, Farrell, M, Lehmann, P, et al. The Maudsley addiction profile (MAP): a brief instrument for assessing treatment outcome. Addiction. (1998) 93:1857–67. doi: 10.1046/j.1360-0443.1998.9312185711.x
21. Massah, O, Rafiey, H, Shariatirad, S, Radfar, SR, Ahounbar, E, and Farhoudian, A. The validity and reliability of the Persian version of the Leeds dependence questionnaire. Iran Rehabil J. (2019) 17:91–6. doi: 10.32598/irj.17.2.91
22. Alam-mehrjerdi, Z, Abdollahi, M, Higgs, P, and Dolan, K. Drug use treatment and harm reduction programs in Iran: a unique model of health in the most populated Persian gulf country. Asian J Psychiatr. (2015) 16:78–83. doi: 10.1016/j.ajp.2015.06.002
23. Razzaghi, E, Nassirimanesh, B, Afshar, P, Ohiri, K, Claeson, M, and Power, R. HIV/AIDS harm reduction in Iran. Lancet. (2006) 368:434–5. doi: 10.1016/S0140-6736(06)69132-0
24. Ackland, TR, Elliott, B, and Bloomfield, J. Applied Anatomy and Biomechanics in Sport Human Kinetics (2009).
25. Lynch, SS, Thigpen, CA, Mihalik, JP, Prentice, WE, and Padua, D. The effects of an exercise intervention on forward head and rounded shoulder postures in elite swimmers. Br J Sports Med. (2010) 44:376–81. doi: 10.1136/bjsm.2009.066837
26. Sahrmann, S . Movement System Impairment Syndromes of the Extremities, Cervical and Thoracic Spines—E-Book. USA: Elsevier Health Sciences (2010). Available at: https://books.google.com/books?id=hAZT-VFiTUoC
27. LoPresti, E, Brienza, DM, Angelo, J, Gilbertson, L, and Sakai, J. “Neck range of motion and use of computer head controls.” in Proceedings of the fourth international ACM conference on assistive technologies. (2000) Association for Computing Machinery, Arlington, Virginia, USA. p. 121–128
28. Ghamkhar, L, and Kahlaee, AH. Is forward head posture relevant to cervical muscles performance and neck pain? A case–control study. Braz J Phys Ther. (2019) 23:346–54. doi: 10.1016/j.bjpt.2018.08.007
29. Valachi, B, and Valachi, K. Mechanisms leading to musculoskeletal disorders in dentistry. J Am Dent Assoc. (2003) 134:1344–50. doi: 10.14219/jada.archive.2003.0048
30. Morse, T, Bruneau, H, and Dussetschleger, J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work. (2010) 35:419–29. doi: 10.3233/WOR-2010-0979
31. Zhou, Y, Zhou, W, Aisaiti, A, Wang, B, Zhang, J, Svensson, P, et al. Dentists have a high occupational risk of neck disorders with impact on somatosensory function and neck mobility. J Occup Health. (2021) 63:e12269. doi: 10.1002/1348-9585.12269
32. Shin, S-J, and Yoo, W-G. Changes in cervical range of motion, flexion-relaxation ratio and pain with visual display terminal work. Work. (2014) 47:261–5. doi: 10.3233/WOR-121580
33. Kim, DH, Kim, CJ, and Son, SM. Neck pain in adults with forward head posture: effects of Craniovertebral angle and cervical range of motion. Osong Public Health Res Perspect. (2018) 9:309–13. doi: 10.24171/j.phrp.2018.9.6.04
34. Quek, J, Pua, Y-H, Clark, RA, and Bryant, AL. Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. Man Ther. (2013) 18:65–71. doi: 10.1016/j.math.2012.07.005
35. Putri, BA . The correlation between age, years of service, and working postures and the complaints of musculoskeletal disorders. Indones J Occup Safe Health. (2019) 8:187–96. doi: 10.20473/ijosh.v8i2.2019.187-196
36. Shahriyari, M, Afshari, D, and Latifi, SM. Physical workload and musculoskeletal disorders in back, shoulders and neck among welders. Int J Occup Saf Ergon. (2020) 26:639–45. doi: 10.1080/10803548.2018.1442401
37. Pascarelli, EF, and Hsu, Y-P. Understanding work-related upper extremity disorders: clinical findings in 485 computer users, musicians, and others. J Occup Rehabil. (2001) 11:1–21. doi: 10.1023/A:1016647923501
38. Chowdhury, SK, Zhou, Y, Wan, B, Reddy, C, and Zhang, X. Neck strength and endurance and associated personal and work-related factors. Hum Factors. (2022) 64:1013–26. doi: 10.1177/0018720820983635
39. Balogh, I, Arvidsson, I, Björk, J, Hansson, G-Å, Ohlsson, K, Skerfving, S, et al. Work-related neck and upper limb disorders – quantitative exposure–response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet Disord. (2019) 20:139. doi: 10.1186/s12891-019-2491-6
Keywords: opium smoking, drug use disorder, neck range of motion, neck muscles strength, Iran
Citation: Massah O, Arab AM, Farhoudian A, Noroozi M and Hashemirad F (2023) The correlation between strength and range of motion of the neck muscles and opium smoking in Iran. Front. Psychiatry. 14:1200091. doi: 10.3389/fpsyt.2023.1200091
Edited by:
Lucy J. Troup, University of the West of Scotland, United KingdomReviewed by:
Ellie Ahounbar, The University of Melbourne, AustraliaSchwann Shariatirad, Tehran University of Medical Sciences, Iran
Copyright © 2023 Massah, Arab, Farhoudian, Noroozi and Hashemirad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Omid Massah, b21pZDcybWFzc2FoQGdtYWlsLmNvbQ==; Amir Masoud Arab, YXJhYmxvb19tYXNvdWRAaG90bWFpbC5jb20=