 Megan Lipsett1*
Megan Lipsett1* Katie Wyant-Stein2Simone Mendes1
Katie Wyant-Stein2Simone Mendes1 Estelle Berger1
Estelle Berger1 Elliot T. Berkman1Mishka Terplan3
Elliot T. Berkman1Mishka Terplan3 Camille C. Cioffi1,4*
Camille C. Cioffi1,4*- 1Department of Psychology, Center for Translational Neuroscience, University of Oregon, Eugene, OR, United States
- 2Diamond Lab, Department of Psychology, University of Utah, Salt Lake City, UT, United States
- 3Friends Research Institute, Baltimore, MD, United States
- 4Prevention Science Institute, University of Oregon, Eugene, OR, United States
Substance use disorders are a common and treatable condition among pregnant and parenting people. Social, self, and structural stigma experienced by this group represent a barrier to harm reduction, treatment utilization, and quality of care. We examine features of research dissemination that may generate or uphold stigmatization at every level for pregnant and parenting individuals affected by substance use disorder and their children. We explore stigma reduction practices within the research community that can increase uptake of evidence-based treatment programs and prevent potential harm related to substance use in pregnant and parenting people. The strategies we propose include: (1) address researcher stereotypes, prejudice, and misconceptions about pregnant and parenting people with substance use disorder; (2) engage in interdisciplinary and transdisciplinary collaborations that engage with researchers who have lived experience in substance use; (3) use community-based approaches and engage community partners, (4) address stigmatizing language in science communication; (5) provide contextualizing information about the social and environmental factors that influence substance use among pregnant and parenting people; and (6) advocate for stigma-reducing policies in research articles and other scholarly products.
Introduction
More than 40 million Americans struggled with substance use disorders (SUD) in 2020 (1), many of whom are statistically likely to be pregnant or parenting (2, 3). It is difficult to estimate the national prevalence of SUD among pregnant and parenting people (e.g., due to the illegal nature of some substance use and lack of coordinated tracking across treatment facilities), but the prevalence of SUD among this group seems to be increasing (4). It has been estimated that 1 in 8 children live with a parent with a SUD (3).
The efficacy of evidence-based therapeutic interventions for SUD has now been established, with benefits across individuals, families, and society [(e.g., 5, 6)]. Yet, only 1 in 5 people with SUD report receiving the treatment they need. Stigma has been named as a barrier to receiving care (1). The National Institute on Drug Abuse (NIDA) has identified stigma reduction as a major priority, emphasizing that stigma inhibits the implementation and adoption of effective treatments and harm-reduction approaches [e.g., medications for opioid use disorder and other addictions, syringe service programs, and fentanyl testing strips to avoid unintentional fentanyl exposure; (7)]. Social, self, and structural stigma toward individuals who use substances, which is notably higher than stigma toward those with mental illness broadly (8), is an important driver of low uptake of and adherence to these programs. This may be especially true for pregnant and parenting people with SUD who may experience greater stigma based on their pregnancy and parenting status (9). Despite growing knowledge of the genetic and social determinants of SUD, stigma toward pregnant and parenting people who use substances remains a barrier to accessing care and a significant public health concern.
There is a need to promote stigma reduction which may also reduce substance-related harm to parents and their children. While stigma exists at many levels of society, this article explores opportunities for the research community to mitigate substance-related stigma toward pregnant and parenting people through research dissemination of scholarly and non-scholarly products. These research products include journal articles, conference presentations, and community-facing information on findings. How researchers articulate and contextualize their research findings [e.g., through the rhetoric of maternal unfitness; (10)] can have consequences for intervention uptake, public perception, policy, and the way practitioners perceive, communicate, and treat pregnant and parenting people with SUD. Researchers can examine the existence of stigma within their work as part of a larger effort to alleviate the adverse effects of both stigma itself and the impacts of stigma on accessing health services.
We present strategies within a unifying framework to reduce stigmatization of pregnant and parenting individuals who use substances in the dissemination of research findings. The strategies we propose include: (1) address researcher stereotypes, prejudice, and misconceptions about pregnant and parenting people with SUD; (2) engage in interdisciplinary and transdisciplinary collaborations that engage with researchers who have lived experience in substance use; (3) use community-based approaches and engage community partners, (4) address stigmatizing language in science communication; (5) provide contextualizing information about the social and environmental factors that influence substance use among pregnant and parenting people; and (6) advocate for stigma-reducing policies in research articles and other scholarly products.
Impacts of social, self, and structural stigma surrounding substance use disorder on pregnant and parenting people
Despite the prevalence of pregnant and parenting people with SUD, only about 9% of those with SUD receive any kind of treatment (11). While these treatment rates are driven by multiple structural factors (e.g., limited availability of treatment centers, inability to access or afford care, and limited screening for SUD in medical visits), fear of shame and stigmatization in seeking care remains a key determinant of treatment engagement (12–14). Indeed, stigma has been proposed as a key barrier to treatment utilization for those with SUD (1)–and SUD is the most globally stigmatized health condition according to the World Health Organization (15). Researchers first need to understand the impact of stigma on this population.
Stigma is embedded at multiple layers of social interaction. Pregnant and parenting people who use substances may experience compounding social, structural, and self- stigmatization. Social stereotypes manifest behaviorally (e.g., by social distancing or discrimination) and, ultimately, hinder care delivery and undermine treatment access (16). Stigma at every level increases distress, social isolation, and diminished access to resources (17). Stigma also influences the progression from substance use to the development of a SUD, undermines SUD treatment efforts, and drives health inequities across the life course (18). Stigmatization of opioid use, for instance, has hindered the national response to the opioid crisis in the United States by reducing public support for beneficial programs, such as the uptake of effective harm reduction strategies and evidence-based treatment [e.g., medication for opioid use disorder; (16)].
Social stigma arises from stereotypes about people who use substances in general, including harmful narratives that people who use substances are dangerous or purposefully choose not to abide by moral societal standards. When health professionals endorse stereotype perceptions (e.g., assigning poor motivation to patients) and display diminished empathy, this impacts patient empowerment, quality of care, and the type of treatment that parents with SUD receive (8, 19). Disregarding patient autonomy and engaging in nonbeneficent care policies occurs disproportionately among care providers when treating people who use substances (16). The suboptimal medical care that results from stigma also occurs with respect to children of parents who use substances, including when medical conditions are assumed to be connected to substance exposure rather than their root cause (19–23). Ultimately, stigma impacts appropriate healthcare provision via barriers to health-seeking behavior, engagement in structures of care, and treatment adherence (24). Further, there are racial disparities in access to treatment for SUD (25), emphasizing that pregnant and parenting people who use substances and who have a minoritized racial identity are at risk of racial discrimination and greater stigmatization. Degree of social stigma can vary based on substance used. This form of social stigma is more often related to racialized narratives than to pharmacological impacts of the substances themselves (26). Indeed, more severe substance-specific social stereotypes have been weaponized to attack the parental fitness of minoritized groups (27). Conversely, substances commonly used by White, middle class individuals (e.g., alcohol and cannabis) tend to have less severe societal stigma (28). As such, it is important to consider racialized narratives that underly individual ideologies about the impacts of use.
Stereotypes about pregnant and parenting people with SUD, specifically, are often related to the potential of (1) prenatal substance use to cause fetal harm and (2) parental substance use to cause harm to the child. When examining these potential risks, social narratives commonly link substance use with “maternal unfitness” and focus on parental deficits, particularly when parents are compared to hegemonic ideals of parenthood (29). While it is critical to prevent and address potential harms associated with substance use during pregnancy, the scientific evidence of actual meaningful consequences of exposure does not support the extent to which SUD has been linked to the unfitness of the birthing person to parent (10, 30). Instead, the narrative of parental unfitness undermines the importance of the parent -baby bond and often leads to depriving both mother and baby of the benefit of embeddedness in a supportive environment (30).
Focusing on parental deficits implies that parents who struggle with substance use are wholly unable to provide adequate nurturing to their children (31), despite the evidence of treatment and harm reduction approaches demonstrating that there are ways to use substances and still have strong parenting skills. For instance, our Center on Parenting and Opioids provides parenting resources to support parents to reduce substance use if that is their goal, reduce potential harm to self or child, and prepare for safe and successful parenting [e.g., obtaining additional supportive care when planning to use, not sleeping in the same bed with children, avoiding putting children around water, and keeping substances in medication boxes and away from children’s access; (32)]. This and other treatment and harm reduction approaches (e.g., programs like HomeSafe in New Jersey) prioritize meeting the primary needs of the whole family by providing wrap-around services rather than penalizing the parent for use of substances (33).
Pregnant and parenting people with SUD are also vulnerable to structural stigma, wherein social stigma becomes embedded in cultural norms, laws, and the policies and procedures of institutions, restricting their rights and opportunities (16, 34). For instance, drug use in pregnancy is codified as child abuse and results in parenting individuals with a record of child abuse. Structural stigma results in limited access to housing, work opportunities, and medical and behavioral treatment (35). The narrative of “maternal unfitness” has led to government interventions and punitive actions against pregnant people, such as arrest, detention, loss of parental custody, or “lock-in” programs, in which individuals are restricted to only obtaining substances from a single pharmacy (10, 36, 37). Though designed to protect fetal health, these responses fail to consider scientific evidence related to individual values and motivations, successful treatment of SUD, and structural factors that undermine treatment utilization for both SUD and obstetrical care (10). In fact, punitive responses can exacerbate the issue, including predicting increased likelihood of infant Neonatal Abstinence Syndrome [NAS; (38, 39)].
Punitive policies are centralized around criminalization, leading to high rates of prosecution and incarceration, family separation (40–42), and fewer resources to support those who are affected by substance use [e.g., restrictions on treatment, limited access to overdose prevention sites, and fewer social services generally; (43)]. Punitive approaches further increase the likelihood that pregnant people (21), will avoid accessing healthcare, ultimately widening health inequities (44–46). The impact of stigma on healthcare utilization may be further compounded for parents facing housing instability or houselessness, who often do not seek out supportive services for fear of being separated from their children.
Stigma may impede the advancement of evidence-based healthcare delivery policies (8) and policies oriented toward public health, which are designed to support individuals through expanded services for prevention and treatment (37). Public health-oriented policies, such as the expansion of Medicaid insurance to cover prescription opioid treatment or laws that ensure that those seeking help for overdose are protected from criminal charges, aim to address substance use without inhibiting healthcare access (37). Unlike punitive approaches, public health approaches are grounded in the understanding of SUD as a chronic, but treatable, condition. In fact, many people successfully manage SUD (47) and there are many examples of pregnant and parenting people with SUD that demonstrate hope, resilience, and restoration (16).
Self-stigma occurs when pregnant and parenting individuals internalize negative societal beliefs and sentiments (48). Internalized narratives become predictive as individuals with SUD anticipate stigmatizing and judgmental treatment when interacting with providers and healthcare systems; ultimately leading to poorer health outcomes (16, 49) and retention and follow-up care challenges (50). Impacts of self-stigma on psychological well-being, self-efficacy and resultant treatment outcomes for those with substance use disorders are well-documented (51–54). The downstream mental health consequences of self-stigma may itself be a determinant for continued substance use. For instance, Khantzian’s (55) Self-medication Hypothesis posits the misuse of substances as a self-regulation strategy to manage difficult life experiences, including stigma-related social anxiety and experiences of racial discrimination (38, 56, 57). Interventions that target experiences internalized stigma such as Acceptance and Commitment Therapy, are effective for reducing substance use and increasing treatment attendance (58, 59).
Overall, stigma harms pregnant and parenting individuals with SUD and their children by preventing access to necessary and vital services, contributing to internalized social devaluation, psychological distress, and underutilization of treatment (34, 48). These psychosocial and economic impacts further perpetuate challenges to parenting, impacting the families and children of parents with SUD. Critically, choices made within the research process such as language used to describe pregnant and parenting people who use substances and lack of inclusion of the role of stigma as a confounder to measured outcomes may perpetuate stigmatization and resulting discrimination. Examining opportunities to prevent the downstream impacts of research approaches that lead to stigma is an important step in creating supportive environments for pregnant and parenting people with SUD to ultimately improve health outcomes for this vulnerable population.
The role of research in shaping public perceptions, treatment utilization, and policy
Stigmatization that is created or upheld within research products may impact care experiences for pregnant and parenting individuals affected by SUD and their children by contributing to social, structural, and self-stigma. Stigma may arise in how research is conducted, shared, and interpreted. In many ways, effectively destigmatizing research starts even before the data are collected; it begins with working alongside and uplifting the voices of the individuals and communities under examination (60). Stigmatizing beliefs exist within research toward individuals who use substances generally, as described by Stull et al. (61), p. 2:
‘Those of us who have conducted human research have noticed that beliefs about addiction are incorporated into every aspect of it–the framing of questions, the screening criteria for studies, the experimental manipulations used in human laboratory sessions, and the outcome measures used in clinical trials or assessment studies. Most of those beliefs are based on data and are defensible, but often they do not allow for the degree of heterogeneity that we know, from experience, is characteristic of addiction.’
Ultimately, there is a need for a “toolbox” of various strategies and evidence-based interventions that address the multiple levels at which stigma arises [(e.g., 17, 62, 63)]. However, to provide timely guidance to researchers who are ready to share findings, the remainder of this paper will focus on strategies to reduce stigma toward pregnant and parenting people with SUD as it relates to the dissemination of research products.
Within dissemination, stigma may arise in how we portray our research, how it is shared, and how it is interpreted; impacting health and well-being experiences for pregnant and parenting individuals affected by substance use disorder. Stigma is a driving factor in the persistent barriers to the equitable and efficient translation of research into clinical practice, public health benefit, and policy change (64). There have been numerous calls for research to be increasingly patient-oriented (65, 66) and sensitive to the social impact of scientific research (67)–and for the creation of guidelines to support researchers in considering the way in which they frame SUD during publication (68). Stigmatizing pregnant and parenting individuals with SUD may prevent evidence-based practices in reaching implementation stages and later translation to community health policies and programs. To the extent that research products inform policy and institutional procedure, these products may inadvertently perpetuate structural stigma. Researchers may lend support to punitive approaches by failing to explore the potential for public health and harm reduction approaches to confer beneficial outcomes for pregnant and parenting people who use substances and their families.
Eliminating the use of stigmatizing narratives within the dissemination of research products is one step toward improving the ways society and care providers interact with pregnant and parenting people with SUD. The unconscious and insidious nature of stigma suggests the need for our active engagement to decrease substance-related stigma toward pregnant and parenting individuals in research dissemination. Using a framework to guide the research process increases impact (69). There are dozens of frameworks of research dissemination and implementation, with much of the guiding content focused on structural aspects of dissemination, such as research planning and measures selection (69). To our knowledge, there are no comprehensive frameworks to reduce stigma within research products related to SUD among pregnant and parenting individuals.
A framework of strategies to reduce stigma in the dissemination of research findings
We present the following strategies for guiding efforts to reduce stigma within research dissemination for pregnant and parenting people affected by SUD. We draw from related frameworks [e.g., The Health Stigma and Discrimination Framework; (26)], which articulate the process of stigmatization in the context of health broadly, to frame stigma-reduction strategies within research dissemination to reduce harm caused to pregnant and parenting individuals with SUD. We suggest how key components of these frameworks might be integrated into the dissemination of research products for those conducting research involving pregnant and parenting people with SUD. We provide a multi-level approach to consider the various levels that may perpetuate or address stigma (18). These strategies are organized by order of operations when approaching dissemination planning and procedures for research efforts (see Table 1).

Table 1. Strategies for reducing stigma toward pregnant and parenting people with SUD within research dissemination.
Actionable recommendations
Strategy #1: address researcher stereotypes, prejudice, and misconceptions about pregnant and parenting people with SUD
Despite positive intentions within the research community, normative judgments that exist at both conscious and unconscious levels are reflected in scientific endeavors and perpetuate stigma (70). Specifically, generalized assumptions that people with SUD are incapable of providing a supportive caregiving environment are reflected in academic language and are used to justify harmful and unwarranted child welfare reporting practices. Stigmatizing attitudes are known to be most prevalent among those without knowledge of or experience with a stigmatized condition [(e.g., 71)]. Without direct experience, for instance, researchers might not have had the opportunity to observe pregnant and parenting people who use substances acting as competent parents or recovering from SUD. Narratives that over-emphasize negative attributes and life circumstances can increase stigmatization (72). Effective stigma reduction strategies, such as providing education on stigma reduction or social contact interventions that focus on sharing experiences or stories of competent parenting or recovery among pregnant and parenting people with SUD, can be incorporated into research dissemination practices. For example, including a narrative account in tandem with quantitative research findings. Additionally, the enhanced stigmatization that is accompanied by the use of certain substances such as heroin (73) and methamphetamine (74) or the modality of use such as injection (75), necessitates the inclusion of parents with specific lived and living expertise to provide their accounts of parenting, particularly as it relates to the pain of removal, the hope of family cohesion, and the successful navigation of parenting when adequate social supports exist.
Evidence of the detrimental impacts of the negative attitudes upheld by health professionals [i.e., diminished communication and hindering the therapeutic alliance for clinical interventions; (76)] suggests that negative attitudes among researchers may have similar negative consequences. Researchers can examine personal biases toward pregnant and parenting people who use substances to mitigate potential harm resulting from research products. Beyond the potential to create negative experiences and outcomes of study participants, impact study adherence, and inhibit researcher awareness about relevant study events, diminished communication can negatively influence our theoretical approaches and interpretation of findings. Like ‘diagnostic overshadowing,’ wherein physical illness symptoms are misattributed to mental illness and result in underdiagnosis (77), our theoretical framings may incorrectly disregard important participant comorbidities or inaccurately assume they are a feature of substance use. The perceptions we hold about the controllability and culpability of having SUD, known as attributional beliefs, may impact the way we frame SUD in our research products. For instance, attributional beliefs may lead to reporting about SUD using a framework based on individualism and personal responsibility (e.g., narratives of “maternal unfitness”) rather than discussing upstream and social causes, which can change social perceptions and ultimately reduce motivation for social and interpersonal responsibility-taking behaviors (78). Meaningful interaction with individuals who have had the direct experience of substance use while pregnant and parenting may reduce biases by reducing anxiety related to those interactions, increasing knowledge about the lived experience of those individuals, and enhancing empathy [e.g., Pettigrew and Tropp’s contact hypothesis; (79)].
Models that recognize the physiological and psychosocial drivers of SUD (e.g., disease models and biopsychosocial models) may minimize the moralization of substance use and therefore reduce stigmatizing beliefs toward pregnant and parenting people who use substances. NIDA promotes the characterization of SUD as a “chronic relapsing brain disorder” that “powerfully compromises executive function circuits that mediate self-control and decision-making” as a method of stigma reduction toward those with SUDs (7). Compared to other models that have a focus on will power or personal characteristics as a driving element of SUD, recognizing the complex biopsychosocial drivers of SUD is both more accurate and more likely to prevent stigma. For example, the disease model asserts that a pregnant person who uses substances during pregnancy can be seen as someone suffering from a chronic disorder, rather than as someone who is choosing to actively harm their developing fetus. However, disease models may also be vulnerable to the process of moralization (80), and require reflection on how assertions of moral responsibility within our theoretical approaches may inform stigma. Biopsychosocial models consider psychological attributes, individual skills, and social and environmental context, which may increase understanding about the internal mechanisms of use within the individual. The integration of these models is important for providing holistic care for pregnant and parenting people with SUD. However, neither of these models fully address social and structural determinants of health, which are key drivers of parent substance use (81, 82).
To the extent that stigma occurs at the unconscious level, it is crucial to proactively support stigma reduction efforts by increasing awareness of social, self, and structural stigma. Specifically, we propose developing a clear understanding of stigma and its effects, becoming aware of and responsive to self-stigma among pregnant and parenting people with SUD [as recommended by Crandall and Holder; (83)], and using continuing education, self-evaluation tools, and professional training to reduce professional stigma. As awareness grows of the impact of stigma on individuals with SUD accessing care, the National Institutes of Health (NIH) has recently released various funding opportunities for research on trainings and tools designed to reduce stigma around SUD. Stigma is a fundamental cause of health inequities across the life course (18), and NIH continues to provide information and resources for stigma reduction in research [(e.g., 62)].
Researchers can commit to participation in training opportunities designed to expose our normative judgments and to ensure that we have meaningful contact with the communities that are the focus of our research. For instance, the Mental Health First Aid training program, which focuses on mental health and substance use issues, has been shown to enhance knowledge and reduce stigmatizing perceptions (84). A growing number of training programs are available, such as those offered by Zero Block Society (85) and Prevention Technology Transfer Centers (86), as well as the perinatal harm reduction toolkit [(e.g., 87, 88)]. More such training programs are needed. The NIH offers training to reduce stigma toward people who use opioids for primary care clinicians through their HEAL Initiative (88), though we are not aware of training targeted for researchers. The Center for Parenting and Opioids (CPO) has offered several trainings for researchers, including one on community-based research focused on partnerships between researchers and harm reduction frontline workers in Vancouver, British Columbia (the recording is publicly available1).
Contact-based training and education programs are effective for addressing stigma (89), including among medical students and professionals (34). Engagement with people who have the lived experience of substance use while pregnant and/or parenting during stigma reduction trainings may enhance the effectiveness of stigma reduction training (90). Articles that highlight the lived experiences of pregnant and parenting people with SUD can be included in stigma reduction training, such as from the perinatal harm reduction coalition. At the time of this writing, the Journal of Substance Use and Addiction Treatment offers regular “lived experience” publications designed to “honor stories of addiction and recovery, mitigate stigma through a humanized portrayal of persons, families and caregivers affected by SUD, raise issues of social justice and inequity, explore the dynamics of patient-clinician relationships, and foster compassionate engagement with people with SUD” (91) and has published qualitative reports of the lived experience of pregnant and parenting people with SUD (92).
Strategy #2: engage in interdisciplinary and transdisciplinary collaborations
A variety of perspectives, frameworks, and lived experiences are needed to identify and address stigmatizing elements in research dissemination. From the perspective of expanding frameworks and approaches among researchers themselves, interdisciplinary and transdisciplinary approaches have the potential to shed light on the unrealized elements of our research that may otherwise introduce stigmatizing frameworks. The lack of careful examination of information being reviewed and communication issues across fields (93) demands an increase in ongoing collaboration with individuals from different fields of study. Transdisciplinary collaborations may enhance understanding about the role of stigma in treatment outcomes and address the complex, multifaceted social phenomenon of stigma within research products [(e.g., 94, 95)]. NIDA has funded several Transdisciplinary Prevention Research Centers (TPRCs) to “foster innovative translation of theories across disciplines” and “overcome the barriers inherent in integrating cross-disciplinary concepts, methods, and findings” (96).
Interdisciplinary and transdisciplinary collaborations may represent multiple benefits. For instance, they may enhance understanding of multiple streams of evidence and generate more practical and robust knowledge about the life course impacts of both fetal drug exposure and SUD-related stigma. Research collaborations also represent an opportunity for research teams to mutually inform one another’s approaches to stigma reduction. This would further promote clear and adaptable stigma reduction strategies that can be applied to many fields. Finally, collaborative approaches increase the likelihood of engaging with researchers with SUD in the context of pregnancy and parenting, who bring an informed perspective and awareness to the research process (61). While individual discretion related to self-disclosure of stigmatized identities among researchers with SUD should take precedence, doing so may further promote empowerment and reduce self-stigma (89), especially when safe spaces to do so exist.
Strategy #3: use community-based approaches and engage community partners
Research initiatives are too often out of touch with the communities they seek to study or serve (97). For instance, researchers may assume that parents who use substances have access to certain kinds of technology or fail to identify historical and cultural elements that inform their degree of engagement. We may not recognize misalignments between the values driving proposed studies and those of pregnant and parenting individuals with SUD (98), leading to oversights that may perpetuate stigma. Meta-analyzes and systematic reviews have demonstrated that community-based, patient-centered approaches can improve utilization and treatment outcomes for evidence-based substance use treatments (99, 100).
Community-based practices, such as engaging community advisory boards and digesting information from community surveys prior to introducing community health services, represent an ethical standard of inclusivity and have been found to reduce stigma and enhance care seeking (101). Community-based participatory research (CBPR) approaches can guide researchers in this process [e.g., having a prevention focus, being population-centered and collaborative, taking a multi-disciplinary approach, building on community strengths and resources, attending to social inequalities, taking an ecological perspective, and prioritizing mutual benefits for all partners; (102, 103)]. Researchers can increase community involvement by identifying relevant partner organizations (e.g., non-profits, community health centers, and peer organizations), planning research activities that meaningfully engage pregnant and parenting people with SUD in the research dissemination process (e.g., public presentation of study findings), ensuring that findings are communicated in understandable and usable ways (Patient-Centered Outcomes Research Institute; PCORI), and providing interventionists and practitioners structures for soliciting and communicating feedback passed along to them by participants and community partners about research products. Community partners should represent the specific population within the research, including subpopulations of pregnant and parenting people with SUD, who may differ in factors such as substances used or features of their SUD–as well as substance-specific stigmatization. For instance, not convening individuals with alcohol use disorder to provide insight into stigmatizing experiences among those with opioid use disorder who are injecting substances. This is even more relevant considering that those who use certain substances may themselves stigmatize those who use other substances. Pregnant and parenting people that use highly stigmatized substances are silenced by the systems they engage with. Researchers must understand how to create space, actively listen, and validate the experiences of these vulnerable groups. Including a member of the research team with experience facilitating groups, especially a researcher with lived experience, may improve the experiences of participants. Highly studied populations frequently emphasize the importance of researchers committing to real and meaningful benefit to study participants, including a plan for actively advocating for change based on research findings [(e.g., 60)]. Community-based practices encourage the creation of valuable materials (i.e., related to childcare, lactation spaces, or parenting practices) or novel resources for participants (e.g., affinity groups for those who have experienced loss or child removal).
The Patient-Centered Outcomes Research Institute2 provides grant funding and an online repository of engagement-related tools and resources including “stakeholder engagement plans,” to enhance effectiveness and likelihood of translation and dissemination of research. In addition to informing our research on the whole, involvement of pregnant and parenting people with SUD ensures relevancy of the research to this community and can help bring attention to potentially stigmatizing aspects of the research. Thong et al. (104) recommends researchers receive training on building rapport and engaging more deeply with prospective participants by involving participants’ families or significant others and taking time to discuss important elements of the research process. Others point to working with peer outreach workers and organizations to help build trust and participation (105, 106).
In addition to connecting directly with pregnant and parenting people who use substances, researchers can partner with Community-Based Organizations (CBOs) who engage with this group (107). CBOs are often familiar with community strengths, needs, and challenges. PCORI’s “Stakeholders’ Substance Use Research and Treatment Information Exchange” (SSURTIE) supports efforts to design and develop infrastructure to promote increased collaboration among researchers who focus on SUD and the community partners who are affected by the disorder or who provide treatment (108). Guidelines frequently emphasize the importance of developing trusting relationships with community partners and allowing their input to define the evidence collected, critically reflecting on and dismantling power structures, exploring potential adaptations relevant to the community being considered, and engaging in critical evaluation of how scientific frameworks and approaches may contribute to barriers by perpetuating stigma.
Strategy #4: address stigmatizing language in science communication
Stigma toward substance use and SUD has become embedded in language itself, in part due to political rhetoric aimed at reducing substance use (109, 110). For instance, the terms “addict” and “junkie” contribute to stigma among people with SUD (111). Calls have been made for scholars to “carefully and intentionally consider the language used to describe... drug use and disorders, the individuals affected by these conditions, and their related behaviors, comorbidities, treatment, and recovery” within research products (68), pp. 2. Indeed, language influences public perceptions regarding the cause and modifiability of substance use, as well as personal perceptions related to self-efficacy among those impacted (68). As language is a known driver of social and individual perceptions of SUD, examining our language choices within research products related to pregnant and parenting individuals may reduce stigma toward this population. Synthesizing these recommendations, we propose the following strategies: use language that (1) Respects the worth and dignity of all persons (“person-first language”), (2) Focuses on the medical nature of SUD and treatment, (3) Promotes the recovery process, and (4) Avoids perpetuating negative stereotypes and biases with slang and idioms (68).
“Person-first language” emphasizes the person over their condition when referring to individuals affected by SUD, for example, “people with OUD” instead of “opioid users.” The mere use of the term ‘substance abuser’ versus ‘having a substance use disorder,’ leads to beliefs that individuals with SUD engage in willful misconduct, pose a greater threat to society, and are more deserving of punishment (112). Nonetheless, person-first language remains uncommon in the research literature on substance use (113). The research community can adopt the use of person-first language (rather than disease-first terminology) by using terms such as ‘person with a SUD’, ‘person who uses drugs’, or ‘parent who misuses opioids’ instead of ‘substance abuser’ or ‘substance using’ (19, 112). The Drug Policy Alliance recommends the use of the terms “person with substance use disorder or SUD” and “person who uses/injects drugs (PWUD/PWID)” (114). Gender specific language is important in some contexts, such as when examining differential outcomes or tailored treatment approaches. Researchers can use gender inclusive language when reporting about gender non-specific research related to pregnant and parenting people, who can be of all genders. For instance, the use of gender inclusive terms such as “pregnancy,” “pregnant people,” “during pregnancy,” “birth,” and “birthing parent.” Researchers can also practice inclusivity through conducting research with pregnant and parenting people who are not cis-gendered. In general, there is little information about the parenting experiences of men with SUD (115, 116) and far less (if anything) about people who are not cis-gender (117).
Regarding children who have been exposed to opioids in utero and/or have become physiologically dependent on substances they were exposed to in utero, the National Perinatal Association recommends the phrase child with “prenatal substance exposure” or “physiological dependance,” rather than with the term “addict” or “addicted baby,” (118). They highlight the importance of underscoring that withdrawal is a temporary and treatable condition and that their drug exposure does is not fundamentally deterministic of their long-term outcomes overall (118). This value-neutral language focuses on the effects of the use of substances, rather than the consequences, when referring to the individual.
The Associated Press Stylebook (119) provides journalistic guidelines for language use within articles related to mental illness. NIH has developed a resource that outlines various considerations when reporting scientific findings and has published a Checklist for Communicating Science and Health Research to the Public (120), which includes a guideline for researchers to “convey information in a respectful tone that [does not] stigmatize or assign blame to individuals or groups [affected by the disorder]” (121). The Recovery Research Institute has created the “addictionary” for the purpose of creating a unified language to destigmatize addiction (122). Several institutes, including NIDA and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), have their own guidelines for person-first language. Community advisory board members can also be consulted about the terms they use when describing themselves, and the terms they prefer never to be used (123).
Strategy #5: provide contextualizing information about the social and environmental factors that influence substance use among pregnant and parenting people
SUD, pregnancy, and parenting do not occur independently of social, environmental, and genetic factors, which have all been demonstrated as determinants of substance use initiation (124). Social and structural determinants of substance use, such as socioeconomic status, disparities in healthcare delivery, discrimination, racism, and social exclusion, have been well-documented (25, 125, 126). These structural factors, along with fear of related stigma, additionally drive treatment engagement (14). Without critically examining their frameworks and analytical approaches, researchers may unintentionally over-emphasize the role of parental substance use in public health issues, neglect to consider how the framing of study results will be perceived by society, or engage in “stigma by omission” (i.e., failing to acknowledge the important role of social and structural factors in SUD). Researchers can work to avoid the tendency to discount social contextual factors that influence child development and behavioral changes, which are more robust predictors of these outcomes than substance exposure alone (127). As misconceptions about the nature and strength of the relationship between exposure and developmental outcomes (see 10) may lead to researcher prejudice, addressing these misconceptions is needed. Despite extensive evidence of contextual and genetic influences on substance use, theoretical frameworks presented in scientific communications often do not acknowledge the role of factors outside individuals. This kind of de-contextualized communication may overemphasize the role of individual characteristics, such as lack of motivation or interest on the part of the individual, as the primary drivers of substance use and treatment non-initiation. For instance, many scientific frameworks for understanding substance use exclusively focus on internal psychological and behavioral mechanisms such as self-regulatory processes and habit extinction (128, 129). While individual-level factors are certainly related to substance use disorder trajectories, a failure to nest individual factors within the broader context may influence self-stigma related to personal ability to recover (130) and stigmatization within treatment systems of care (8). This lack of context may even translate to our statistical approaches. As noted by Terplan (131), p. 1729:
‘Categories such as race, gender, pregnancy, poverty, immigration status, sexual orientation, and medical comorbidities interact in an integrative (not additive or multiplicative) fashion. Logistic regression, even when augmented by sensitivity analyses, therefore executes a leveling effect on the data and, with each turn of the model, whittles away the richness, nuance, and suffering that is the human experience.’
In this way, guiding theories and patterns of data interpretation often “fail in scope to represent the many experiences of addiction” (61), p. 2.
Researchers can reduce stigma toward pregnant and parenting people who use substances by ensuring accurate representation of existing research and considering whether previous research has appropriately accounted for contextual factors. This includes exercising caution not to overstate findings. Researchers can vet research that is peer-reviewed and evidence-based, such as high-quality observational studies that adjust for potential confounding, randomized controlled trials, or meta-analysis. Adjusting for confounding (e.g., of socioeconomic and sociocultural variables) is especially important regarding reporting of biological effects on in-utero exposure to substances and when studying parenting behaviors, which are often sensationalized.
Contextual theoretical frameworks such as Bronfenbrenner’s Social Ecological Framework (132) or Engel’s Biopsychosocial Model (133) outline the multiply determined nature of SUD. Contextual frameworks incorporate key drivers in the development and onset of SUD, such as social isolation or social rejection [(see 116, 127) for examples]. By contextualizing substance use within research frameworks, researchers can frame the biological, social, and structural drivers of substance use. These frameworks may both address the determinants driving substance use more effectively and shift public perceptions regarding those who are affected by SUD. This can be done even if the study did not take a contextual approach during the design phase, through providing this context in the introductory and discussion sections of the paper.
Research related to the impact of substance use on pregnant and parenting people and their families often focuses heavily on the outcomes related to children [(e.g., 134)], rather than providing a balanced lens that also considers the parents’ wellbeing and the functioning of the family. This has led, for instance, to a research base that minimizes the harmful effects of the removal of children from their families. Family preservation approaches emphasize the responsibility of society to minimize the destructive potential impact of the child welfare system (135). Further, research products that overly focus on the child may inadvertently generate additional stigma toward children whose parents use substances. Indeed, people who experienced parental substance use report experiences of stigma and social exclusion (136). Research efforts aimed at supporting families in the context of substance use can consider how the parent might be best supported while they are with their child(ren).
Strategy #6: advocate for stigma-reducing policies in research articles and other scholarly products
Research plays a role in creating and amending policy. This occurs directly through channels by which research is communicated to policymakers and indirectly through influencing public interpretation of research theories and results (137). For instance, research informs evidence-based policies that have downstream impacts on treatment of parental SUD, including within the child welfare system (138). Indeed, research on the importance of parent–child relationships has encouraged policies that reunite children who have been removed from their home as a result of substance use, as opposed to previous policy that promoted children remaining with temporary caregivers (138). Careful evaluation of how we are portraying the implications of our findings may prevent unintended contribution to harmful policy.
Researchers can discuss our findings and their implications within the broader context of social policy in ways that minimize stigma. Grantmaking bodies are increasingly inviting researchers to submit “impact statements,” which are intended to demonstrate the potential benefit research might have in the world. Impact statements that (1) plainly discuss how findings relate to family policy and (2) clearly address how findings could be misinterpreted to promote stigmatizing family policy are critical for stigma reduction. Impact statements are an opportunity to clearly address what findings do and do not imply for public policy. For instance, researchers who evaluate the effects of substances on parenting practices can emphasize that their individual findings do not imply support for unethical child removal practices when applicable. Researchers can also make connections from their findings to policies that reduce harm for parents with SUD and their children (i.e., reunification practices and social support services).
Researchers can also proactively advocate for the development of frameworks and guidelines for stigma reduction when conducting research from influential regulatory and grantmaking bodies. Locally, researchers can work with their Institutional Review Boards (IRBs) to advocate for frameworks and guidelines for stigma reduction when conducting studies. IRBs can be encouraged to develop guidelines related to non-stigmatizing terminology and to support researchers to meaningfully consider practices to reduce stigma resulting from research participation for pregnant and parenting individuals who use substances. Nationally, laws related to stigma-reduction practices would afford dissemination guidelines a judicial basis and ensure that ethical review boards work to uphold these ethical standards (139). Researchers can also directly engage in dissemination efforts that connect our research to policies which impact pregnant and parenting individuals with SUD and their families. For instance, becoming aware of gaps in policy can provide insight into where more research is needed. The Research-to-Policy Collaboration (140) is one organization that connects researchers to relevant needs in policymaking. While research can directly inform policy, we can actively use our leverage as researchers to inform public opinion, including through op-ed papers. Publishing expert opinion in public news draws the attention of policy makers and promotes social pressure that can aid in the development or amendment of policy.
See Table 2 for a summary of proposed strategies and actionable recommendations.
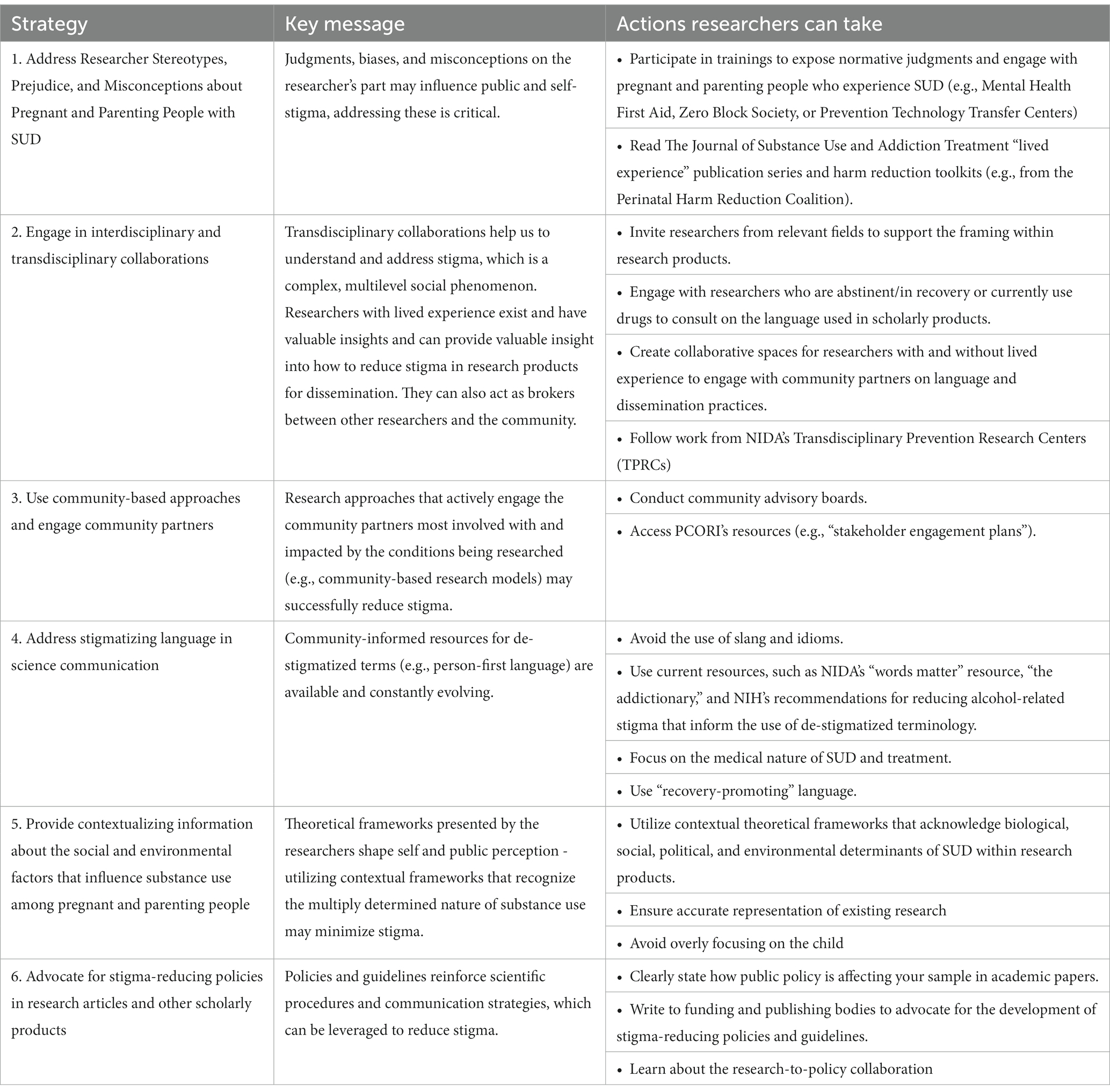
Table 2. Actionable steps to reduce stigma within research dissemination.
A case study: stigma-reduction efforts at the center on parenting and opioids
While implementing these practices is a long-term goal that is not without barriers, we aim to support researchers in taking steps toward minimizing substance-related stigma. The authors of this publication are colleagues at The Center on Parenting and Opioids (CPO), where we are implementing steps to align with the strategies outlined in this paper. The CPO is funded by NIDA and is jointly housed at the University of Oregon and Oregon Health & Science University. We hope our work at the CPO provides an example of taking meaningful steps toward bridging the gap between rigorous science and community impact. From professional workshops to a Knowledge Dissemination working group, the CPO’s initiatives seek to not only challenge researchers to engage reflexively with their research, but to also guide science communicators toward sharing research outcomes and policy recommendations in a way that reduces stigma and expands accessibility to information.
One such initiative is the composition of research briefs that synthesize key findings from current CPO-affiliated studies, with a focus on highlighting the practical utility of science. To actively work toward reducing the stigmatizing language that all too often surrounds research on substance use–particularly regarding pregnant and parenting people who use substances–the CPO has also generated a Destigmatizing Research Dissemination Checklist specifically intended for those writing and reviewing the research briefs. The Destigmatizing Research Dissemination Checklist includes items such as “building on community strengths” and “highlighting the utility of research,” with practical tips like (1) writing with a collective tone to avoid othering the communities we seek to positively impact and (2) using destigmatizing and person-first language. While attending to language and terminology is just one step toward reducing stigma in science (see Table 2), the CPO’s research briefs and Checklist represent an initiative designed to prioritize stigma reduction in research products. Our aim is for these institutional changes to impact social, self, and structural stigma.
Discussion
The goal of this set of strategies is to empower researchers to destigmatize their research products. We anticipate that by reducing stigma in research products, we will be able to reduce self-stigma, social stigma enacted by professionals who care for pregnant and parenting people with SUD, and structural stigma upheld by organizational, local, state, and federal policies. However, there are limitations to our proposed strategies. First, we understand that it takes time and energy to engage with community partners. While we believe their investment and direction is well worth the additional expenditures, we understand that community-engaged research is a new skill that many researchers do not currently practice or have access to training opportunities to learn. We also understand that the academic cycle does not currently well-incentivize community engagement, but incentivizes the quantity of scholarly products published in peer-reviewed journals and grants that bring institutional funding. Thus, destigmatizing research products also requires that the approaches outlined in our work are institutional priorities.
This paper explores opportunities to minimize stigma in the dissemination of research findings to relevant clinical, regulatory, and community audiences, with a specific focus on pregnant and parenting individuals with SUD. However, stigma reduction efforts are needed at all levels of the research process (e.g., planning, research conduct, and interpretation of findings). Examinations of stigma reduction practices across research phases is needed to produce research that accurately and substantively represents those individuals with SUD (141). Enacted stigma at every phase of research can create barriers to participation and preclude many people with SUD from feeling able or being able to participate in studies, ultimately limiting the generalizability of research findings. Additional work is needed to address participation barriers not discussed extensively here, including physical resource limitations [e.g., unstable housing, limited access to transportation, or lack of childcare; (111)], as well as related barriers, such as generalized mistrust of researchers, fear of legal repercussions, or duration and magnitude of the study (142).
The stigma reduction framework outlined here can be used to guide the examination of ways in which stigma has been perpetuated in prior research products. We also suggest that our proposed strategies may be modified to consider how to reduce stigmatization during other research processes.
We have argued that low participation in evidence-based substance misuse prevention and harm reduction programs among pregnant and parenting people who use substances is due in part to the role of stigma toward this group. We emphasize the detrimental impact of stigma at the level of the individual, society, and institution which includes undermining efforts to prevent and treat SUD and perpetuates health inequities. We examined the role of research in perpetuating stigma and its downstream effects and provided guidance based on available theory and evidence for practices to reduce stigma within our research products. These are: (1) address researcher stereotypes, prejudice, and misconceptions about pregnant and parenting people with SUD; (2) engage in interdisciplinary and transdisciplinary collaborations - emphasizing engagement with researchers with lived experience; (3) use community-based approaches and engage community partners, (4) address stigmatizing language in science communication; (5) provide context for research related to pregnant and parenting people with SUD; and (6) advocate for stigma-reducing policies in research articles and other scholarly products. By endeavoring to reduce stigma in our research dissemination practices, we may not only improve our theories, but also the degree to which our findings have real-world impact that minimize stigmatization and discrimination and ultimately transform health outcomes for families impacted by SUD.
Author contributions
ML, SM, KW-S, and CC contributed to conception of the paper. ML was the primary author of the manuscript. KW-S, SM, EB, and CC wrote sections of the manuscript. CC, ML, ETB, and MT provided edits and feedback to the draft. ML and CC revised the manuscript. All authors read and approved the submitted version.
Funding
This work was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number P50DA048756 (PIs Leve & Fisher). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. ML and ETB were supported by grants CA240452 and CA21122.
Acknowledgments
The authors would like to thank Chris Hannegan for their contribution to the formatting of references and in-text citations for this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Substance Abuse and Mental Health Services Administration . Key substance use and mental health indicators in the United States: results from the 2020 National Survey on drug use and health (HHS publication no. PEP21-07-01-003, NSDUH series H-56). Center for Behavioral Health Statistics and Quality Substance Abuse and Mental Health Services Administration. (2021) Available at: https://www.samhsa.gov/data/ (Accessed March 20, 2023).
2. Taplin, S, and Mattick, RP. The nature and extent of child protection involvement among heroin-using mothers in treatment: high rates of reports, removals at birth and children in care. Drug Alcohol Rev. (2015) 34:31–7. doi: 10.1111/dar.12165
3. Lipari, RN, and Van Horn, SL. Children living with parents who have a substance use disorder. The CBHSQ Report. Rockville, MD: Substance Abuse and Mental Health Services Administration. (2017) Available at: http://www.ncbi.nlm.nih.gov/books/NBK464590/ (Accessed March 20, 2023).
4. Center for Behavioral Health Statistics and Quality . Treatment episode data set admissions (TEDS-A). Substance Abuse and Mental Health Services Administration. (2018). Available at: https://www.datafiles.samhsa.gov/dataset/treatment-episode-data-set-admissions-2018-teds-2018-ds0001 (Accessed March 17, 2023).
5. Jhanjee, S . Evidence based psychosocial interventions in substance use. Indian J Psychol Med. (2014) 36:112–8. doi: 10.4103/0253-7176.130960
6. Magill, M, Ray, L, Kiluk, B, Hoadley, A, Bernstein, M, Tonigan, JS, et al. A meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: treatment efficacy by contrast condition. J Consult Clin Psychol. (2019) 87:1093–105. doi: 10.1037/ccp0000447
7. National Institute on Drug Abuse . National Institute on Drug Abuse 2016-2020 strategic plan. (2016). Available at: https://nida.nih.gov/sites/default/files/2016-2020nidastrategicplan.pdf
8. Van Boekel, LC, Brouwers, EPM, Van Weeghel, J, and Garretsen, HFL. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend. (2013) 131:23–35. doi: 10.1016/j.drugalcdep.2013.02.018
9. Hecksher, D, and Hesse, M. Women and substance use disorders. Mens Sana Monogr. (2009) 7:50–62. doi: 10.4103/0973-1229.42585
10. Terplan, M, Kennedy-Hendricks, A, and Chisolm, MS. Article commentary: prenatal substance use: exploring assumptions of maternal unfitness. Subst Abuse. (2015) 9:1–4. doi: 10.4137/SART.S23328
11. Martin, CE, Scialli, A, and Terplan, M. Unmet substance use disorder treatment need among reproductive age women. Drug Alcohol Depend. (2020) 206:107679–9. doi: 10.1016/j.drugalcdep.2019.107679
12. Benz, MB, Cabrera, KB, Kline, N, Bishop, LS, and Palm, RK. Fear of stigma mediates the relationship between internalized stigma and treatment-seeking among individuals with substance use problems. Subst Use Misuse. (2021) 56:808–18. doi: 10.1080/10826084.2021.1899224
13. Keyes, KM, Hatzenbuehler, ML, McLaughlin, KA, Link, B, Olfson, M, Grant, BF, et al. Stigma and treatment for alcohol disorders in the United States. Am J Epidemiol. (2010) 172:1364–72. doi: 10.1093/aje/kwq304
14. US Department of Health and Human Services . Facing addiction in America: the surgeon general’s report on alcohol, drugs, and health. he Surgeon General's Report. (2016) Available at: https://addiction.surgeongeneral.gov/ (Accessed November 30, 2022).
15. Room, R, Rehm, J, Paglia, A, and Üstün, TB. Cross-cultural views on stigma, valuation, parity, and societal values towards disability In: TB Üstün, S Chatterji, JE Bickenbach, RT TrotterII, R Room, and S Saxena, editors. Disability and culture: Universalism and diversity. Seattle, WA: Hogrefe & Huber Publishers (2001). 247–91.
16. Tsai, AC, Kiang, MV, Barnett, ML, Beletsky, L, Keyes, KM, McGinty, EE, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med. (2019) 16:e1002969. doi: 10.1371/journal.pmed.1002969
17. Earnshaw, VA . Stigma and substance use disorders: a clinical, research, and advocacy agenda. Am Psychol. (2020) 75:1300–11. doi: 10.1037/amp0000744
18. Hatzenbuehler, ML, Phelan, JC, and Link, BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health. (2013) 103:813–21. doi: 10.2105/AJPH.2012.301069
19. Kelly, JF, and Westerhoff, CM. Does it matter how we refer to individuals with substance-related conditions? A randomized study of two commonly used terms. Int J Drug Policy. (2010) 21:202–7. doi: 10.1016/j.drugpo.2009.10.010
20. Howard, H . Reducing stigma: lessons from opioid-dependent women. J Soc Work Pract Addict. (2015) 15:418–38. doi: 10.1080/1533256X.2015.1091003
21. Stone, R . Pregnant women and substance use: fear, stigma, and barriers to care. Health Justice. (2015) 3:2. doi: 10.1186/s40352-015-0015-5
22. Weber, A, Miskle, B, Lynch, A, Arndt, S, and Acion, L. Substance use in pregnancy: identifying stigma and improving care. Subst Abus Rehabil. (2021) 12:105–21. doi: 10.2147/SAR.S319180
23. Wouldes, TA, and Lester, BM. Stimulants: how big is the problem and what are the effects of prenatal exposure? Semin Fetal Neonatal Med. (2019) 24:155–60. doi: 10.1016/j.siny.2019.01.011
24. Stangl, AL, Earnshaw, VA, Logie, CH, van Brakel, W, Simbayi, LC, Barré, I, et al. The health stigma and discrimination framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. (2019) 17:31. doi: 10.1186/s12916-019-1271-3
25. Center for Behavioral Health Statistics and Quality. Racial/ethnic differences in substance use, substance use disorders, and substance use treatment utilization among people aged 12 or older (2015-2019). Substance Abuse and Mental Health Services Administration. (2021). Available at: https://www.samhsa.gov/data/report/racialethnic-differences-substance-use (Accessed March 17, 2023).
26. Manderson, D . Symbolism and racism in drug history and policy. Drug Alcohol Rev. (1999) 18:179–86. doi: 10.1080/09595239996617
27. Lyons, P, and Rittner, B. The construction of the crack babies phenomenon as a social problem. Am J Orthopsychiatry. (1998) 68:313–20. doi: 10.1037/h0080340
28. Schlussel, D . “The mellow pot-smoker”: White individualism in marijuana legalization campaigns. Calif Law Rev. (2017) 105:885–927. doi: 10.15779/Z38PZ51K8D
29. Nichols, TR, Welborn, A, Gringle, MR, and Lee, A. Social stigma and perinatal substance use services: recognizing the power of the good mother ideal. Contemp Drug Probl. (2021) 48:19–37. doi: 10.1177/0091450920969200
30. Terplan, M, and Wright, T. The effects of cocaine and amphetamine use during pregnancy on the newborn: myth versus reality. J Addict Dis. (2010) 30:1–5. doi: 10.1080/10550887.2011.532048
31. Schiff, DM, Stoltman, JJK, Nielsen, TC, Myers, S, Nolan, M, Terplan, M, et al. Assessing stigma towards substance use in pregnancy: a randomized study testing the impact of stigmatizing language and type of opioid use on attitudes toward mothers with opioid use disorder. J Addict Med. (2022) 16:77–83. doi: 10.1097/ADM.0000000000000832
32. Center on Parenting and Opioids . Substance use and recovery in pregnancy and early parenting. (2022). Available at: https://cpo.uoregon.edu/substance-use-and-recovery-pregnancy-and-early-parenting (Accessed November 27, 2022).
33. Pfefferle, SG, Karon, SS, and Wyant, B. Choice matters: housing models that may promote recovery for individuals and families facing opioid use disorder. The Assistant Secretary for Planning and Evaluation. (2019). Available at: https://aspe.hhs.gov/reports/choice-matters-housing-models-may-promote-recovery-individuals-families-facing-opioid-use-disorder-0 (Accessed March 20, 2023).
34. Livingston, JD, Milne, T, Fang, ML, and Amari, E. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction. (2012) 107:39–50. doi: 10.1111/j.1360-0443.2011.03601.x
35. Crapanzano, KA, Hammarlund, R, Ahmad, B, Hunsinger, N, and Kullar, R. The association between perceived stigma and substance use disorder treatment outcomes: a review. Subst Abus Rehabil. (2019) 10:1–12. doi: 10.2147/SAR.S183252
36. Flavin, J, and Paltrow, LM. Punishing pregnant drug-using women: defying law, medicine, and common sense. J Addict Dis. (2010) 29:231–44. doi: 10.1080/10550881003684830
37. Kennedy-Hendricks, A, Barry, CL, Gollust, SE, Ensminger, ME, Chisolm, MS, and McGinty, EE. Social stigma toward persons with prescription opioid use disorder: associations with public support for punitive and public health-oriented policies. Psychiatr Serv. (2017) 68:462–9. doi: 10.1176/appi.ps.201600056
38. Faherty, LJ, Kranz, AM, Russell-Fritch, J, Patrick, SW, Cantor, J, and Stein, BD. Association of punitive and reporting state policies related to substance use in pregnancy with rates of neonatal abstinence syndrome. JAMA Netw Open. (2019) 2:–e1914078. doi: 10.1001/jamanetworkopen.2019.14078
39. Faherty, LJ, Heins, S, Kranz, AM, Patrick, SW, and Stein, BD. Association between punitive policies and neonatal abstinence syndrome among Medicaid-insured infants in complex policy environments. Addiction. (2022) 117:162–71. doi: 10.1111/add.15602
40. Amnesty International . Criminalizing pregnancy: Policing pregnant women who use drugs in the USA. Amnesty International Ltd. (2017). Available at: https://www.amnesty.org/en/wp-content/uploads/2021/05/AMR5162032017ENGLISH.pdf (Accessed March 20, 2023).
41. Times Editorial Board . The mothers society condemns. New York Times. (2018). Available at: https://www.nytimes.com/interactive/2018/12/28/opinion/abortion-law-poverty.html, https://www.nytimes.com/interactive/2018/12/28/opinion/abortion-law-poverty.html (Accessed November 30, 2021).
42. Miranda, L, Dixon, V, and Reyes, C. How states handle drug use during pregnancy. Publica. (2015). Available at: http://projects.propublica.org/graphics/maternity-drug-policies-by-state (Accessed February 1, 2019).
43. Sharfstein, JM, and Olsen, Y. The role of evidence in the US response to the opioid crisis. Epidemiol Rev. (2020) 42:167–70. doi: 10.1093/epirev/mxaa004
44. Poland, ML, Dombrowski, MP, Ager, JW, and Sokol, RJ. Punishing pregnant drug users: enhancing the flight from care. Drug Alcohol Depend. (1993) 31:199–203. doi: 10.1016/0376-8716(93)90001-7
45. Patrick, SW, Schiff, DM, Quigley, J, Gonzalez, PK, and Walker, LR. A public health response to opioid use in pregnancy. Pediatrics. (2017) 139:e20164070. doi: 10.1542/peds.2016-4070
46. Atkins, DN, and Durrance, CP. State policies that treat prenatal substance use as child abuse or neglect fail to achieve their intended goals. Health Aff (Millwood). (2020) 39:756–63. doi: 10.1377/hlthaff.2019.00785
47. Kelly, JF, Bergman, B, Hoeppner, BB, Vilsaint, C, and White, WL. Prevalence and pathways of recovery from drug and alcohol problems in the United States population: implications for practice, research, and policy. Drug Alcohol Depend. (2017) 181:162–9. doi: 10.1016/j.drugalcdep.2017.09.028
48. Corrigan, PW, and Rao, D. On the self-stigma of mental illness: stages, disclosure, and strategies for change. Can J Psychiatr. (2012) 57:464–9. doi: 10.1177/070674371205700804
49. Smith, LR, Earnshaw, VA, Copenhaver, MM, and Cunningham, CO. Substance use stigma: reliability and validity of a theory-based scale for substance-using populations. Drug Alcohol Depend. (2016) 162:34–43. doi: 10.1016/j.drugalcdep.2016.02.019
50. Syvertsen, JL, Toneff, H, Howard, H, Spadola, C, Madden, D, and Clapp, J. Conceptualizing stigma in contexts of pregnancy and opioid misuse: a qualitative study with women and healthcare providers in Ohio. Drug Alcohol Depend. (2021) 222:108677. doi: 10.1016/j.drugalcdep.2021.108677
51. Da Silveira, PS, Casela, ALM, Monteiro, ÉP, Ferreira, GCL, de Freitas, JVT, Machado, NM, et al. Psychosocial understanding of self-stigma among people who seek treatment for drug addiction. Stigma Health. (2018) 3:42–52. doi: 10.1037/sah0000069
52. Hammarlund, R, Crapanzano, KA, Luce, L, Mulligan, L, and Ward, KM. Review of the effects of self-stigma and perceived social stigma on the treatment-seeking decisions of individuals with drug- and alcohol-use disorders. Subst Abus Rehabil. (2018) 9:115–36. doi: 10.2147/SAR.S183256
53. Luoma, JB, Kohlenberg, BS, Hayes, SC, Bunting, K, and Rye, AK. Reducing self-stigma in substance abuse through acceptance and commitment therapy: model, manual development, and pilot outcomes. Addict Res Theory. (2008) 16:149–65. doi: 10.1080/16066350701850295
54. Melchior, H, Hüsing, P, Grundmann, J, Lotzin, A, Hiller, P, Pan, Y, et al. Substance abuse-related self-stigma in women with substance use disorder and comorbid posttraumatic stress disorder. Eur Addict Res. (2019) 25:20–9. doi: 10.1159/000496113
55. Khantzian, EJ . The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv Rev Psychiatry. (1997) 4:231–44.
56. Gerrard, M, Stock, ML, Roberts, ME, Gibbons, FX, O’Hara, RE, Weng, C-Y, et al. Coping with racial discrimination: the role of substance use. Psychol Addict Behav. (2012) 26:550–60. doi: 10.1037/a0027711
57. Hart, CL, and Hart, MZ. Opioid crisis: another mechanism used to perpetuate American racism. Cultur Divers Ethnic Minor Psychol. (2019) 25:6–11. doi: 10.1037/cdp0000260
58. Osaji, J, Ojimba, C, and Ahmed, S. The use of acceptance and commitment therapy in substance use disorders: a review of literature. J Clin Med Res. (2020) 12:629–33. doi: 10.14740/jocmr4311
59. Luoma, JB, Chwyl, C, and Kaplan, J. Substance use and shame: a systematic and meta-analytic review. Clin Psychol Rev. (2019) 70:1–12. doi: 10.1016/j.cpr.2019.03.002
60. Neufeld, SD, Chapman, J, Crier, N, Marsh, S, McLeod, J, and Deane, LA. Research 101: a process for developing local guidelines for ethical research in heavily researched communities. Harm Reduct J. (2019) 16:41–1. doi: 10.1186/s12954-019-0315-5
61. Stull, SW, Smith, KE, Vest, NA, Effinger, DP, and Epstein, DH. Potential value of the insights and lived experiences of addiction researchers with addiction. J Addict Med. (2022) 16:135–7. doi: 10.1097/ADM.0000000000000867
62. The Danya Institute . Anti-stigma toolkit. Danya Inst. (2012). Available at: https://attcnetwork.org/sites/default/files/2019-04/Anti-Stigma%20Toolkit.pdf (Accessed November 30, 2022).
63. Chaudoir, SR, Wang, K, and Pachankis, JE. What reduces sexual minority stress? A review of the intervention “toolkit”. J Soc Issues. (2017) 73:586–617. doi: 10.1111/josi.12233
64. Estabrooks, PA, and Glasgow, RE. Translating effective clinic-based physical activity interventions into practice. Am J Prev Med. (2006) 31:S45–56. doi: 10.1016/j.amepre.2006.06.019
65. Johnson, LB, and Smalley, JB. Engaging the patient: patient-centered research In: KL Hall, AL Vogel, and RT Croyle, editors. Strategies for team science success: Handbook of evidence-based principles for cross-disciplinary science and practical lessons learned from health researchers. Cham: Springer International Publishing (2019). 135–47.
66. Frank, L, Basch, E, and Selby, JV. The PCORI perspective on patient-centered outcomes research. JAMA. (2014) 312:1513–4. doi: 10.1001/jama.2014.11100
67. Bornmann, L . Measuring the societal impact of research: research is less and less assessed on scientific impact alone--we should aim to quantify the increasingly important contributions of science to society. EMBO Rep. (2012) 13:673–6. doi: 10.1038/embor.2012.99
68. Broyles, LM, Binswanger, IA, Jenkins, JA, Finnell, DS, Faseru, B, Cavaiola, A, et al. Confronting inadvertent stigma and pejorative language in addiction scholarship: a recognition and response. Subst Abuse. (2014) 35:217–21. doi: 10.1080/08897077.2014.930372
69. Tabak, RG, Khoong, EC, Chambers, DA, and Brownson, RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med. (2012) 43:337–50. doi: 10.1016/j.amepre.2012.05.024
70. Corrigan, PW, and Watson, AC. Understanding the impact of stigma on people with mental illness. World Psychiatry. (2002) 1:16–20.
71. Corrigan, PW, Green, A, Lundin, R, Kubiak, MA, and Penn, DL. Familiarity with and social distance from people who have serious mental illness. Psychiatr Serv. (2001) 52:953–8. doi: 10.1176/appi.ps.52.7.953
72. National Academies of Sciences . Engineering, and medicine, division of behavioral and social sciences and education, Board on behavioral, cognitive, and sensory sciences, committee on the science of changing behavioral health social norms In: ME Evans, JL Geller, GL Kreps, MW Kreuter, BG Link, and BM Melnyk, et al. editors. Ending discrimination against people with mental and substance use disorders: The evidence for stigma change. Washington, DC: National Academies Press (2016). 171.
73. Goodyear, K, Ahluwalia, J, and Chavanne, D. The impact of race, gender, and heroin use on opioid addiction stigma. J Subst Abus Treat. (2022) 143:108872. doi: 10.1016/j.jsat.2022.108872
74. Semple, SJ, Grant, I, and Patterson, TL. Utilization of drug treatment programs by methamphetamine users: the role of social stigma. Am J Addict. (2005) 14:367–80. doi: 10.1080/10550490591006924
75. Muncan, B, Walters, SM, Ezell, J, and Ompad, DC. “They look at us like junkies”: influences of drug use stigma on the healthcare engagement of people who inject drugs in New York City. Harm Reduct J. (2020) 17:53. doi: 10.1186/s12954-020-00399-8
76. Thornicroft, G, Rose, D, and Kassam, A. Discrimination in health care against people with mental illness. Int Rev Psychiatry. (2007) 19:113–22. doi: 10.1080/09540260701278937
77. Palmer, RS, Murphy, MK, Piselli, A, and Ball, SA. Substance user treatment dropout from client and clinician perspectives: a pilot study. Subst Use Misuse. (2009) 44:1021–38. doi: 10.1080/10826080802495237
78. Sun, Y, Krakow, M, John, KK, Liu, M, and Weaver, J. Framing obesity: how news frames shape attributions and behavioral responses. J Health Commun. (2016) 21:139–47. doi: 10.1080/10810730.2015.1039676
79. Pettigrew, TF, and Tropp, LR. How does intergroup contact reduce prejudice? Meta-analytic tests of three mediators. Eur J Soc Psychol. (2008) 38:922–34. doi: 10.1002/ejsp.504
80. Frank, LE, and Nagel, SK. Addiction and moralization: the role of the underlying model of addiction. Neuroethics. (2017) 10:129–39. doi: 10.1007/s12152-017-9307-x
81. Volkow, DN . Social determinants of health can’t be extricated from addiction science. National Institute on Drug Abuse. (2023). Available at: https://nida.nih.gov/about-nida/noras-blog/2023/04/social-determinants-health-cant-be-extricated-addiction-science (Accessed May 5, 2023).
82. Sukhera, J, Knaak, S, Ungar, T, and Rehman, M. Dismantling structural stigma related to mental health and substance use: an educational framework. Acad Med. (2022) 97:175–81. doi: 10.1097/ACM.0000000000004451
83. Crandall, LA, and Holder, SM. Research, writing, editorial reviewing, and publishing as social justice issues: the effects of stigma. J Appl Rehabil Couns. (2020) 51:295–303. doi: 10.1891/JARC-D-20-00025
84. Peralta, L, Jackson, A, Franchino, K, Green, N, Park, S, Chen, L, et al. Helping frontline workers respond to mental health issues. NEJM Catal Innov Care Deliv. (2021) 2021:623. doi: 10.1056/CAT.20.0623
85. Zero Block Society . Harm reduction workers guild. Zero Block Society. (2023). Available at: https://thezeroblock.org/guild/ (Accessed March 20, 2023).
86. Prevention Technology Transfer Center Network . Training and events calendar. Prevention Technology Transfer Center Network. (2023). Available at: https://pttcnetwork.org/centers/global-pttc/training-and-events-calendar (Accessed March 23, 2023).
87. Academy of Perinatal Harm Reduction . Pregnancy and substance use: a harm reduction toolkit. National Harm Reduction Coalition. (2020). Available at: https://harmreduction.org/wp-content/uploads/2020/10/09.17.20_Pregnancy-and-Substance-Use-2.pdf (Accessed November 1, 2022).
88. U.S. Department of Health and Human Services . Helping to end addiction long-term. National Institutes of Health. (2019) Available at: https://heal.nih.gov (Accessed December 20, 2022).
89. Corrigan, PW, Kosyluk, KA, and Rüsch, N. Reducing self-stigma by coming out proud. Am J Public Health. (2013) 103:794–800. doi: 10.2105/AJPH.2012.301037
90. Kohrt, BA, Jordans, MJD, Turner, EL, Rai, S, Gurung, D, Dhakal, M, et al. Collaboration with people with lived experience of mental illness to reduce stigma and improve primary care services: a pilot cluster randomized clinical trial. JAMA Netw Open. (2021) 4:e2131475. doi: 10.1001/jamanetworkopen.2021.31475
91. Journal of Substance Abuse Treatment . Journal of substance use and addiction treatment. JSAT call for papers: lived experience. Journal of Substance Abuse Treatment. (2023). Available at: https://www.sciencedirect.com/journal/journal-of-substance-use-and-addiction-treatment/about/call-for-papers (Accessed March 30, 2023).
92. Adams, ZM, Ginapp, CM, Price, CR, Qin, Y, Madden, LM, Yonkers, K, et al. “A good mother”: impact of motherhood identity on women’s substance use and engagement in treatment across the lifespan. J Subst Abus Treat. (2021) 130:108474–4. doi: 10.1016/j.jsat.2021.108474
93. Phillips, KW, Liljenquist, KA, and Neale, MA. Is the pain worth the gain? The advantages and liabilities of agreeing with socially distinct newcomers. Personal Soc Psychol Bull. (2009) 35:336–50. doi: 10.1177/0146167208328062
94. McGinty, E, Pescosolido, B, Kennedy-Hendricks, A, and Barry, CL. Communication strategies to counter stigma and improve mental illness and substance use disorder policy. Psychiatr Serv. (2018) 69:136–46. doi: 10.1176/appi.ps.201700076
95. Ashford, RD, Brown, AM, and Curtis, B. Systemic barriers in substance use disorder treatment: a prospective qualitative study of professionals in the field. Drug Alcohol Depend. (2018) 189:62–9. doi: 10.1016/j.drugalcdep.2018.04.033
96. National Institute on Drug Abuse . Director’s report to the National Advisory Council on drug abuse. (2003). Available at: https://archives.drugabuse.gov/sites/default/files/directors_report_2-03.pdf (Accessed September 9, 2022).
97. Bruce, ML, Smith, W, Miranda, J, Hoagwood, K, and Wells, KB. Community-based interventions. Ment Health Serv Res. (2002) 4:205–14. doi: 10.1023/A:1020912531637
98. Collins, SE, Clifasefi, SL, Stanton, J, Straits, KJE, Gil-Kashiwabara, E, Espinosa, PR, et al. Community-based participatory research (CBPR): towards equitable involvement of community in psychology research. Am Psychol. (2018) 73:884–98. doi: 10.1037/amp0000167
99. Guerrero, EG . Enhancing access and retention in substance abuse treatment: the role of Medicaid payment acceptance and cultural competence. Drug Alcohol Depend. (2013) 132:555–61. doi: 10.1016/j.drugalcdep.2013.04.005
100. Davis, EL, Kelly, PJ, Deane, FP, Baker, AL, Buckingham, M, Degan, T, et al. The relationship between patient-centered care and outcomes in specialist drug and alcohol treatment: a systematic literature review. Subst Abuse. (2020) 41:216–31. doi: 10.1080/08897077.2019.1671940
101. Kearns, M, Muldoon, OT, Msetfi, RM, and Surgenor, PWG. The impact of community-based mental health service provision on stigma and attitudes towards professional help-seeking. J Ment Health Abingdon Engl. (2019) 28:289–95. doi: 10.1080/09638237.2018.1521928
102. Strand, K, Marullo, S, Cutforth, N, Stoecker, R, and Donohue, P. Community-based research and higher education: principles and practices. San Francisco, CA: Jossey-Bass (2003).
103. Blumenthal, DS, RJ, DC, Braithwaite, R, and Smith, S. Community-based participatory health research: issues, methods, and translation to practice. 2nd ed. New York: Springer (2013). 296 p.
104. Thong, ISK, Ulph, F, Barrowclough, C, and Gregg, L. Facilitators and barriers to participating in a randomized controlled trial of a psychological therapy for substance use. J Nerv Ment Dis. (2019) 207:487–96. doi: 10.1097/NMD.0000000000001000
105. Brown, G, Crawford, S, Perry, G-E, Byrne, J, Dunne, J, Reeders, D, et al. Achieving meaningful participation of people who use drugs and their peer organizations in a strategic research partnership. Harm Reduct J. (2019) 16:37–7. doi: 10.1186/s12954-019-0306-6
106. Hoffman, KA, Baker, R, Kunkel, LE, Waddell, EN, Lum, PJ, McCarty, D, et al. Barriers and facilitators to recruitment and enrollment of HIV-infected individuals with opioid use disorder in a clinical trial. BMC Health Serv Res. (2019) 19:862–2. doi: 10.1186/s12913-019-4721-x
107. Atkins, MS, Rusch, D, Mehta, TG, and Lakind, D. Future directions for dissemination and implementation science: aligning ecological theory and public health to close the research to practice gap. J Clin Child Adolesc Psychol. (2016) 45:215–26. doi: 10.1080/15374416.2015.1050724
108. Patient-Centered Outcomes Research Institute . Stakeholders’ substance use research and treatment information exchange (SSURTIE). Patient-Centered Outcomes Research Institute. (2015). Available at: https://www.pcori.org/research-results/2014/stakeholders-substance-use-research-and-treatment-information-exchange-ssurtie (Accessed June 22, 2022).
109. Zwick, J, Appleseth, H, and Arndt, S. Stigma: how it affects the substance use disorder patient. Subst Abuse Treat Prev Policy. (2020) 15:50. doi: 10.1186/s13011-020-00288-0
110. Loper, A, Woo, B, and Metz, A. Equity is fundamental to implementation science. Stanf Soc Innov Rev. (2021) 19:A3–5. doi: 10.48558/QNGV-KG05
111. National Institute on Drug Abuse . Words matter: preferred language for talking about addiction. National Institute on Drug Abuse. (2021). Available at: https://nida.nih.gov/research-topics/addiction-science/words-matter-preferred-language-talking-about-addiction (Accessed March 24, 2023).
112. Kelly, JF, Dow, SJ, and Westerhoff, C. Does our choice of substance-related terms influence perceptions of treatment need? An empirical investigation with two commonly used terms. J Drug Issues. (2010) 40:805–18. doi: 10.1177/002204261004000403
113. Sharp, P, Slattery, J, Johnson, A, Torgerson, T, Ottwell, R, Vassar, M, et al. The use of person-first language in scientific literature focused on drug-seeking behavior: a cross-sectional analysis. J Osteopath Med. (2021) 121:827–33. doi: 10.1515/jom-2021-0149
114. Drug Policy Alliance . Stigma and people who use drugs. Drug Policy Alliance. (2014). Available at: https://drugpolicy.org/sites/default/files/DPA_Fact_Sheet_Stigma_and_People_Who_Use_Drugs.pdf (Accessed September 30, 2022).
115. McMahon, TJ, and Rounsaville, BJ. Substance abuse and fathering: adding poppa to the research agenda: substance abuse and fathering. Addiction. (2002) 97:1109–15. doi: 10.1046/j.1360-0443.2002.00159.x
116. Cioffi, CC, and DeGarmo, DS. Improving parenting practices among fathers who misuse opioids: fathering through change intervention. Front Psychol. (2021) 12:683008–8. doi: 10.3389/fpsyg.2021.683008
117. Connolly, D. Non-binary people who use drugs are an underserved group at high risk of harm. BMJ Sexual and Reproductive Health blog. (2021). Available at: https://blogs.bmj.com/bmjsrh/2021/07/19/non-binary-people-who-use-drugs-are-an-underserved-group-at-high-risk-of-harm/ (Accessed May 5, 2023).
118. National Perinatal Association . Perinatal substance use. National Perinatal Association. Available at: https://www.nationalperinatal.org/substance-use (Accessed September 9, 2022).
119. Press, Associated . The associated Press stylebook 2022-2024. Basic Books. (2021). Available at: https://www.basicbooks.com/titles/the-associated-press/the-associated-press-stylebook/9781541601659/ (Accessed March 20, 2023).
120. National Institutes of Health . A checklist for communicating science and health research to the public. National Institutes of Health. (2018). Available at: https://www.nih.gov/about-nih/what-we-do/science-health-public-trust/checklist-communicating-science-health-research-public (Accessed October 15, 2022).
121. US Department of Health and Human Services . Stigma and discrimination research toolkit. National Institute of Mental Health. (2022). Available at: https://www.nimh.nih.gov/about/organization/dar/stigma-and-discrimination-research-toolkit (Accessed December 20, 2022).
122. Recovery Research Institute . Addictionary®. Recovery Research Institute. (2022). Available at: https://www.recoveryanswers.org/addiction-ary/ (Accessed December 20, 2022).
123. Pivovarova, E, and Stein, MD. In their own words: language preferences of individuals who use heroin. Addiction. (2019) 114:1785–90. doi: 10.1111/add.14699
124. Volkow, ND, Koob, GF, and McLellan, AT. Neurobiologic advances from the brain disease model of addiction. N Engl J Med. (2016) 374:363–71. doi: 10.1056/NEJMra1511480
125. Galea, S, and Vlahov, D. Social determinants and the health of drug users: socioeconomic status, homelessness, and incarceration. Public Health Rep. (2002) 117 Suppl 1:S135–45.
126. Beard, SJ, Hastings, PD, Ferrer, E, Robins, RW, and Guyer, AE. Neural response to social exclusion moderates the link between adolescent anxiety symptoms and substance use. Biol Psychiatry Cogn Neurosci Neuroimaging. (2022) 7:180–91. doi: 10.1016/j.bpsc.2021.06.006
127. Cioffi, CC, Leve, LD, and Seeley, JR. Accelerating the pace of science: improving parenting practices in parents with opioid use disorder. Parenting. (2019) 19:244–66. doi: 10.1080/15295192.2019.1615801
128. Leshner, AI . Addiction is a brain disease, and it matters. Science. (1997) 278:45–7. doi: 10.1126/science.278.5335.45
129. Volkow, N, and Li, T-K. The neuroscience of addiction. Nat Neurosci. (2005) 8:1429–30. doi: 10.1038/nn1105-1429
130. Corrigan, PW, Bink, AB, Schmidt, A, Jones, N, and Rüsch, N. What is the impact of self-stigma? Loss of self-respect and the “why try” effect. J Ment Health Abingdon Engl. (2016) 25:10–5. doi: 10.3109/09638237.2015.1021902
131. Terplan, M . Can perinatal quality collaboratives address racial (in)justice? Am J Public Health. (2020) 110:1728–9. doi: 10.2105/AJPH.2020.305982
132. Bronfenbrenner, U . The ecology of human development. Cambridge, MA: Harvard University Press (1979).
133. Engel, GL . The clinical application of the biopsychosocial model. J Med Philos. (1981) 6:101–24. doi: 10.1093/jmp/6.2.101
134. Morton, C, and Wells, M. Behavioral and substance use outcomes for older youth living with a parental opioid misuse: a literature review to inform child welfare practice and policy. J Public Child Welf. (2017) 11:546–67. doi: 10.1080/15548732.2017.1355866
135. Roberts, DE . Shattered bonds: the color of child welfare. Faculty Scholarship at Penn Carey Law, p. 356. (2001). Available at: https://scholarship.law.upenn.edu/faculty_scholarship/2777.
136. Meulewaeter, F, De Schauwer, E, De Pauw, SSW, and Vanderplasschen, W. “I grew up amidst alcohol and drugs:” a qualitative study on the lived experiences of parental substance use among adults who developed substance use disorders themselves. Front Psych. (2022) 13:768802–2. doi: 10.3389/fpsyt.2022.768802
138. Child Welfare Information Gateway . Substance use disorders and cross-system collaboration. Child Welfare Information Gateway. (2022). Available at: https://www.childwelfare.gov/topics/systemwide/bhw/collaboration/sud/ (Accessed June 22, 2022).
139. Snoek, A, and Horstkötter, D. Ethical issues in research on substance-dependent parents: the risk of implicit normative judgements by researchers. Bioethics. (2018) 32:620–7. doi: 10.1111/bioe.12514
140. Research to Policy Collaboration . Research to policy collaboration. Research to Policy Collaboration. (2022). Available at: https://research2policy.org/ (Accessed September 9, 2022).
141. Subbaraman, MS, Laudet, AB, Ritter, LA, Stunz, A, and Kaskutas, LA. Multi-source recruitment strategies for advancing addiction recovery research beyond treated samples. J Community Psychol. (2015) 43:560–75. doi: 10.1002/jcop.21702
Keywords: stigma, substance use disorder, dissemination, perinatal, harm reduction, parenting, treatment accessibility, health equity
Citation: Lipsett M, Wyant-Stein K, Mendes S, Berger E, Berkman ET, Terplan M and Cioffi CC (2023) Addressing stigma within the dissemination of research products to improve quality of care for pregnant and parenting people affected by substance use disorder. Front. Psychiatry. 14:1199661. doi: 10.3389/fpsyt.2023.1199661
Edited by:
Yukiko Washio, RTI International, United StatesReviewed by:
Dennis Hand, Thomas Jefferson University, United StatesRachel Gunn, Brown University, United States
Copyright © 2023 Lipsett, Wyant-Stein, Mendes, Berger, Berkman, Terplan and Cioffi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Megan Lipsett, bWxpcHNldHRAdW9yZWdvbi5lZHU=; Camille C. Cioffi, Y2Npb2ZmaUB1b3JlZ29uLmVkdQ==