

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 27 June 2023
Sec. Psychopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1189768
This article is part of the Research TopicReviews in Psychiatry 2022: PsychopharmacologyView all 6 articles
 Yarmila Elena Valencia Carlo1†
Yarmila Elena Valencia Carlo1† Ricardo Arturo Saracco-Alvarez2*†Verónica Angela Valencia Carlo3Daniela Vázquez Vega1
Ricardo Arturo Saracco-Alvarez2*†Verónica Angela Valencia Carlo3Daniela Vázquez Vega1 Guillermina Natera Rey4
Guillermina Natera Rey4 Raul Ivan Escamilla Orozco5
Raul Ivan Escamilla Orozco5Introduction: Our objective was to conduct a systematic review and meta-analysis of adverse effects on sleep in patients with schizophrenia receiving antipsychotic treatment.
Methods: A systematic search was performed in PubMed, Cochrane Central, Embase, Toxline, Ebsco, Virtual Health Library, Web of Science, SpringerLink, and in Database of abstracts of Reviews of Effects of Randomized Clinical Trials to identify eligible studies published from January 1990 to October 2021. The methodological quality of the studies was evaluated using the CONSORT list, and the Cochrane bias tool. Network meta-analysis was performed using the Bayesian random-effects model, with multivariate meta-regression to assess the association of interest.
Results: 87 randomized clinical trials were identified that met the inclusion criteria, and 70 articles were included in the network meta-analysis. Regarding the methodological quality of the studies, 47 had a low or moderate bias risk. The most common adverse effects on sleep reported in the studies were insomnia, somnolence, and sedation. The results of the network meta-analysis showed that ziprasidone was associated with an increased risk of insomnia (OR, 1.56; 95% credible interval CrI, 1.18–2.06). Several of the included antipsychotics were associated with a significantly increased risk of somnolence; haloperidol (OR, 1.90; 95% CrI, 1.12–3.22), lurasidone (OR, 2.25; 95% CrI, 1.28–3.97) and ziprasidone (OR, 1.79; 95% CrI, 1.06–3.02) had the narrowest confidence intervals. In addition, perphenazine (OR, 5.33; 95% CrI, 1.92–14.83), haloperidol (OR, 2.61; 95% CrI, 1.14–5.99), and risperidone (OR, 2.41; 95% CrI, 1.21–4.80) were associated with an increased risk of sedation compared with placebo, and other antipsychotics did not differ. According to the SUCRAs for insomnia, chlorpromazine was ranked as the lowest risk of insomnia (57%), followed by clozapine (20%), while flupentixol (26 %) and perospirone (22.5%) were associated with a lower risk of somnolence. On the other hand, amisulpride (89.9%) was the safest option to reduce the risk of sedation.
Discussion: Insomnia, sedation, and somnolence were the most frequent adverse effects on sleep among the different antipsychotics administered. The evidence shows that chlorpromazine, clozapine, flupentixol, perospirone, and amisulpride had favorable safety profiles. In contrast, ziprasidone, perphenazine, haloperidol, and risperidone were the least safe for sleep.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42017078052, identifier: PROSPERO 2017 CRD42017078052.
Schizophrenia is a psychiatric disorder that affects ~1% of the world population and is characterized by positive or psychotic symptoms (e.g., hallucinations, delusions, and disorganized thoughts and/or disorganized speech), negative symptoms (e.g., decreased motivation, decreased emotional expressiveness, autism and social withdrawal), and cognitive deficits (e.g., impaired executive functions, memory, and processing speed) (1).
Patients with schizophrenia frequently report sleep problems. There are numerous factors contributing to the comorbidity, including medication intake (2). Although AP medications have prominent effect of sleep, however, have also demonstrated beneficial by increasing sleep efficiency and total sleep time, and reducing sleep onset latency (SOL) (3, 4).
Antipsychotics (AP) are essential component of schizophrenia treatment. These drugs are classified into first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs), according to their molecular mechanism of action. As with other medications, AP despite their proven therapeutic utility, can also generate multiple adverse drug reactions (ADRs), ranging from metabolic to motor effects (5). Many of these consequences affect the patients' lifestyle, contribute to the rate of abandonment of treatment, and influence the prognosis of the disease (6). Some studies focusing on antipsychotic medication have demonstrated that adverse effects have a negative impact on patient adherence to treatment, both in institutional and outpatient setting. Thus, it is in the best interest of the patient and of the clinical staff to reduce adverse effects and prevent their recurrence (7, 8).
The results of some studies showed that increasing antipsychotic dosages were linked to better sleep, although antipsychotic medications only accounted for a relatively small amount of the variance in sleep (8). Furthermore, sleep complaints were pervasive in 70% of this medicated clinical sample. These findings suggest that the use of the sedative properties of antipsychotic medication has limited efficacy as a treatment option for sleep dysfunctions, and is not an appropriate substitute for sleep interventions (9, 10). The degree of discomfort caused by each type of side effect is variable in patient reports; (11) certain ones report indicate that most patients find extrapyramidal effects, sexual dysfunction, and weight gain to be the most intolerable, as opposed to sedation and other vegetative effects. The presence of these effects is associated with poor treatment adherence (12), and some of these effects may be therapeutic for people with schizophrenia, such as sedation in those with insomnia or perhaps the inversion of sleep architecture seen in some patients, since the pharmacological effects of medications used to treat schizophrenia can affect sleep-wake function. In general, FGAs are linked to increased REM sleep latency and SGAs to increased slow-wave sleep reduction (13, 14).
Another possible AP adverse effect is somnolence. It can be defined as a propensity to fall asleep and while in this state, conscious effort may need to be made to stay awake; in contrast to fatigue which is more related to physical exhaustion (15). All antipsychotics have been observed to cause sedation, but the severity and frequency varies widely between agents (16). Although it is a common adverse effect and a common reason for medication non-adherence, the evidence for sedation has not been widely examined in systematic reviews. Sedation, instead, is a term denoting the use of pharmacological agents to calm acutely agitated patients, both in a psychiatric care service as well as in general acute care setting (17). Somnolence and sedation are related to the delivered dose and are the most bothersome problems for patients, compared to insomnia, which is also common with AP medications, and may be the cause of poor adherence to treatment, if persistent, may interfere with the individual's social and vocational functioning (18). A systematic review with meta-analysis by Andrade et al. (19) found no significant differences in daytime sleepiness between placebo and antipychotics associated with modafinil or armodafinil using a random effects model (mean difference = 0.78; 95% CI = 3.33–1.76).
Antipsychotic medication has an effect on various neurotransmitter receptors such as acetylcholine, dopamine, histamine, norepinephrine, and serotonin. For example, serotonin receptor antagonism promotes sedation and may increase slow-wave sleep, whereas 5-HT1A receptors agonism may cause sleep disturbances and suppress REM sleep. Blockage of histamine receptors promotes sedative and sleep-enhancing effects, can reduce REM sleep intensity, and increase REM latency (20). Antagonism of dopamine receptors can result in restless leg syndrome, which may interfere with sleep (21). Aside from antidopaminergic activity, many other receptors bind to almost all dopamine receptor antagonists or APs, including cholinergic receptors (22). There is an inverse relationship between the potency of the antipsychotic and blockade of these receptors, so those with less D2 affinity are the ones that most frequently generate somnolence. For its management, it is recommended to administer the entire dose or most of it at night. If somnolence is incapacitating, it is recommended to reduce the dose of the DRA or change it to another with less drowsiness effect (23, 24).
According to polysomnographic studies, administration of some AP such as clozapine, paliperidone and olanzapine to patients with schizophrenia frequently results in a significant reduction of sleep latency (SL) and increase in total sleep time and sleep efficiency. In addition, olanzapine and paliperidone augmented slow wave sleep (SWS) and REM sleep. In contrast, quetiapine administration further disrupted sleep measured by reduction of SWS and REM sleep, also for the increase of SL, wake time after onset (WASO) and REM sleep latency (25, 26).
The variability in the AP effects on sleep structure appears to be related to the individual receptor binding profiles of the drugs for the mentioned neurotransmitters (26). Indeed, clinicians acknowledge the prevalence and importance of sleep problems in patients, but in current practice formal assessment is rare and evidence is limited. However, there is clear interest in treating this side effect, as three quarters of patients with psychosis who have insomnia would like to improve their sleep (27).
Reviewing the studies published in the last 20 years, we tried to answer the following question: what are the adverse effects of typical and atypical antipsychotics on the sleep of patients diagnosed with schizophrenia? The aim of this research, therefor, was to perform a systematic review and meta-analysis of adverse effects on sleep in patients with schizophrenia receiving antipsychotic treatment.
The research protocol was registered on the PROSPERO platform (CRD42017078052), developed by the University of York (http://www.crd.york.ac.uk/prospero/). A search was made for studies published between 1990 and October 2021, using the following electronic databases: Pubmed, Embase, Cochrane library, Ebsco, Toxline, Springerlink, Web of Science, Database of abstracts of Reviews of Effects and the Virtual Health Library; Abstracts.
The search strategy was carried out with the following terms: (schizophrenia AND antipsychotic agents AND sleep disorders OR sleep disturbances OR sleep effects OR sleep wake up disorders) and (Schizophrenia AND antipsychotic effects AND Sleep), and in Spanish (Esquizofrenia AND Agentes Antipsicóticos AND Trastornos del Sueño OR problemas de sueño OR efectos en el sueño OR trastornos del sueño vigilia), and (Esquizofrenia AND efectos de antipsicóticos AND sueño).
The inclusion criteria of our systematic review were: (a) randomized and controlled clinical trials in which antipsychotic treatment is provided, in monotherapy or together with an adjuvant medication, (b) written in English or Spanish, (c) studies in which to people ≥18 years, diagnosed with schizophrenia, regardless of subtype or severity of symptoms, (d) trials that reported adverse effects on sleep related to the use or withdrawal of any antipsychotic. As exclusion criteria we have (a) observational studies, case reports, systematic reviews or meta-analysis, (b) investigations with incomplete or unclear methodology, (c) those that do not analyze the relationship between antipsychotics and adverse effects in sleep, and (d) inclusion of participants with other psychiatric disorders, medical or neurological conditions.
Initially, titles and abstracts were initially reviewed, in a second step, the extensive content of the potentially eligible articles was evaluated, in pairs and independently. In the event of discrepancies regarding the inclusion of a study in the review, another of the authors served as the third evaluator to reach consensus. Using the bibliographical references of these articles, we searched twenty-four additional studies to verify if they met inclusion criteria. For that, a flow chart (PRISMA) of the number of articles selected in each phase, of those eliminated and the reason for exclusion was developed. Figure 1 shows the details of all the studies included in the systematic review.
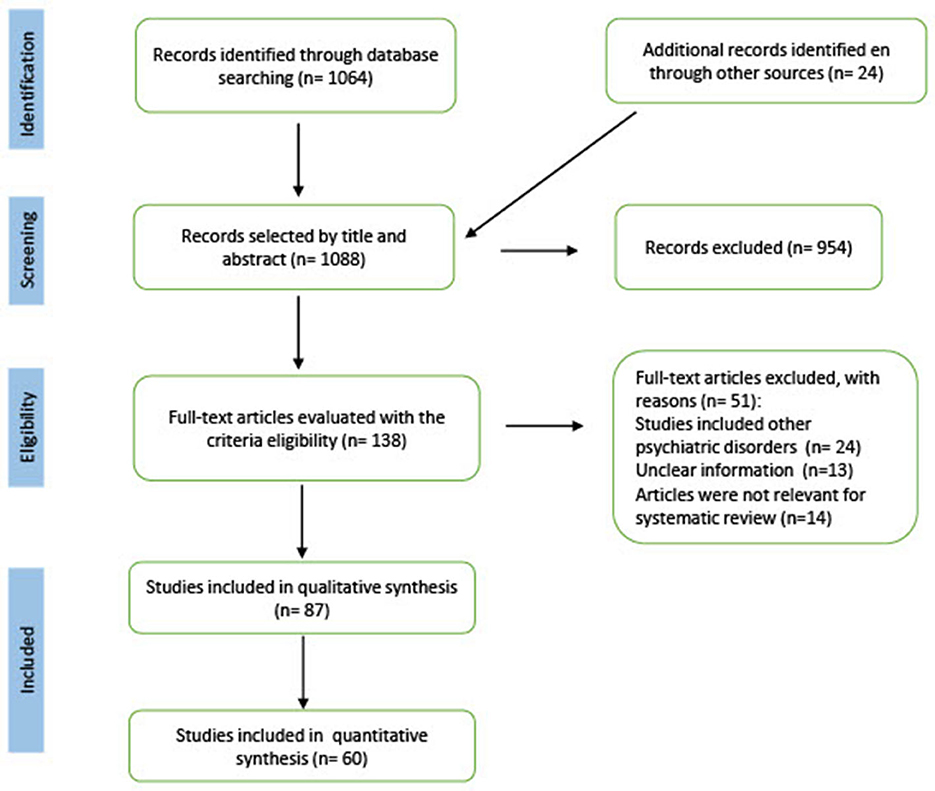
Figure 1. PRISMA flow diagram of study selection. A PRISMA flowchart showing the number of articles selected in each phase, the number of articles excluded, and the details of all studies included and excluded from the systematic review.
To carry out the qualitative synthesis of the results, the following data were extracted in a table of variables: authors, year of publication, country of origin, prescribed antipsychotics, sample size, comparison groups, frequency of adverse effects on sleep, loss to follow-up, funding, conflict of interest and protocol registration number (see Data extraction in the Supplementary material).
We evaluated the quality of the publications through the checklist of the CONSORT statement (28). For each item, three types of response were recorded: “yes”, “does not include” and “not applicable”, following the recommendations on how to evaluate the CONSORT items of the article published by Moher et al. (29). Some items on the checklist have multiple components, so if at least half of them were met, we scored that item “yes.” If less than half of the components were fulfilled or a key component was missing or the information was unclear, the item was scored as “does not include”, then the scores of all the items were added to obtain an overall score and this was expressed in percentage.
Three quality assessment categories were used that were applied in other published research: (1) the study meets more than 80% of the criteria, (2) the study meets between 50 and 80% of the criteria, and (3) the study meets <50% of the criteria identified in the CONSORT checklist (30). To assess the individual risk of bias for each clinical trial, we applied the Cochrane collaboration risk of bias tool. This tool poses six levels of bias: selection, performance, detection, attrition, reporting, and other biases. The response options of the level of bias were classified as: (1) high risk of bias, in this case the bias seriously weakens the confidence in the results, (2) unclear risk, the bias causes some doubt about the results and (3) low risk, refers to the fact that the bias is unlikely to significantly alter the results (28, 30).
The network meta-analysis (NMA) generates evidence from direct and indirect comparisons within a network of trials and enables inference about every possible comparison between a pair of interventions in this network, even when some comparisons have never been directly evaluated in a trial (31).
The NMA resulted in a complex network, in which direct comparisons for each antipsychotic are observed when comparing them individually against placebo. The use of placebo in RCT is widely considered the gold standard for testing the efficacy of new treatments, beyond the psychological results of a simple belief in the curative capacity of the drug, the researchers compare the results of the experimental treatment with those obtained with the placebo (32, 33). It is also useful when the treatment used is of questionable efficacy or has a high frequency of adverse reactions and the risks may significantly outweigh the benefits (34).
To present the evidence graphically, we used network plots of antipsychotic interventions, which provide a visual representation of the evidence base and a description of its characteristics. A network plot consists of nodes representing the interventions being compared, and edges representing the available direct comparisons between pairs of interventions (35). Each treatment node or comparison edge can be weighted according to the number of trials and the average control group risk for placebo vs. active treatment comparisons (36). We estimated summary odds ratios (ORs) for dichotomous outcomes with a 95% credible interval.
We estimated summary odds ratios (ORs) for dichotomous outcomes with a 95% credible interval.
Consistency was evaluated by examining the agreement between direct and indirect treatment effects in all closed loops and assuming loop-specific heterogeneity using the loop-specific approach. To evaluate the presence of inconsistency for any treatment contrast in the network, the node-splitting analysis method was applied.
In addition to OR estimation, treatment ranking was ascertained using the surface under the cumulative ranking curve (SUCRA), which represents the percentage of effectiveness or safety for each treatment compared with a hypothetical treatment that would be ranked first without uncertainty (37). We also plot rankograms, which are graphs that show the probability that each treatment has of reaching a certain ranking. On the X-axis they show the possible ranking and on the Y-axis the probability that each treatment has of reaching it (38).
A Bayesian network meta-analysis based on the random effects model was performed using the STATA 16.1 program. In this analysis the treatment arms with the maximum dose of each antipsychotic and placebo were included. Effect sizes and 95% credible intervals were calculated for the selected articles. The ranking of the different treatments was based on the calculation of the areas under the cumulative rank probability curve or surface under the cumulative ranking curve (SUCRA) (39), which is expressed as a percentage and is interpreted as the probability that all other treatments are inferior or the probability (Pr) of being the best treatment (38).
Of the 1,088 studies initially identified in the search, we excluded 954 studies after reviewing the title, abstract and keywords, as they did not meet the inclusion criteria. During the manual search we found eight eligible studies, of which two were included in the systematic review.
Our review found that 87 clinical trials (40–126) met the established inclusion criteria, 3,813 participants (13.82%) had adverse effects on sleep out of a total of 27,595 people who received treatment with any antipsychotic medication (Table 1). Insomnia (85.54%), somnolence (43.37%) and sedation (16.87%) were the most common adverse events (see Table 2). Other unspecified sleep problems were reported in the articles, but to a lesser extent (3.45%).
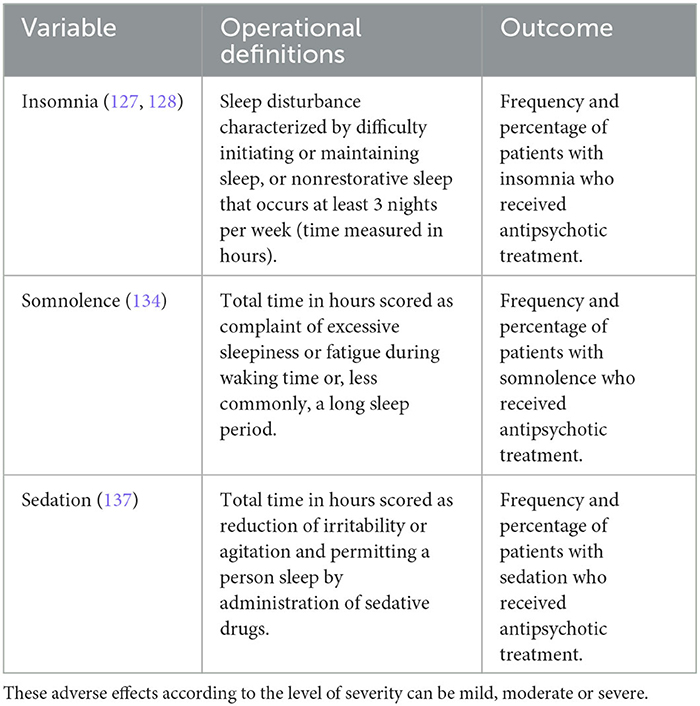
Table 2. Operational definitions of insomnia, somnolence, and sedation.
The AP given in randomized clinical trials (RCT) were the following: amisulpride, aripiprazole, aripiprazole LAI (every 28 days), asenapine, blonanserin, brexpiprazole, cariprazine, chlorpromazine, clozapine, fluphenazine, flupentixol, haloperidol, iloperidone, lurasidone, olanzapine, olanzapine LAI (monthly), paliperidone, paliperidone LAI (monthly), perphenazine, perospirone, quetiapine, risperidone, risperidone LAI (every 15 days), sertindole, ziprasidone, zotepine, and placebo.
It is important to note that in most of the studies included in the review, antipsychotics were administered orally (n = 72, 82.76%), or they were administered intramuscularly, the safety and efficacy of antipsychotics were compared, an antipsychotic tablet vs. the injectable presentation (n = 15, 17.24%). Of the total number of RCTs included in the systematic review, 61 were included in the quantitative analysis phase of the network meta-analysis according to the criterion of having at least two treatment arms comparing different antipsychotics or comparing an antipsychotic with another placebo (see Figure 2).

Figure 2. The network of comparisons of the antipsychotics included in this study for somnolence, sedation, and insomnia. (A) Somnolence. (B) Sedation. (C) Insomnia. The width of the lines is proportional to the number of trials comparing each treatment pair and the size of each node is proportional to the number of randomized participants. The nodes represent the included interventions, and their size is proportional to the sample size. The thickness of the edges connecting the nodes reflects the number of trials included in the given comparison. The thickness of the edges connecting the nodes reflects the number of trials included in the given comparison. AMI, amisulpride; ASE, asenapine; ARI, aripiprazole; ARI LAI, aripiprazole long-acting injection; BLO, blonanserin; BRE, brexpiprazole; CAR, cariprazine; CLO, clozapine; CPZ, chlorpromazine; FLU, fluphenazine; FPX, flupentixol; HAL, haloperidol; ILO, iloperidone; LUR, lurasidone; OLA, olanzapine; OLA LAI, olanzapine long-acting injection; PAL, paliperidone; PAL LAI, paliperidone long-acting injectable; PBO, placebo; PER, perospirone; PERPH, perphenazine; QUE, quetiapine; RIS, risperidone; RIS LAI, risperidone long-acting injection; SER, sertindole; ZIP, ziprasidone; ZOT, zotepine.
Clinical observations, subjective reports or validated questionnaires were used to report adverse sleep effects in the clinical trials. There was a low percentage of studies in which the method of reporting these negative effects was unclear (n = 3, 3.45 %).
In the clinical trials included in the review, all evaluating the safety of one or more antipsychotics vs. another antipsychotic or placebo, the studies varied in reporting the most important methodological characteristics, including: random sequence generation, concealment of allocation, blinding of interventions, appropriate blinding, intention to treat, and description of loss to follow up. When evaluating the level of bias risk, it was observed that the unclear risk predominates, at the point of incomplete data of the results the bis risk is low, it is worth mentioning that in other types of bias risk is high. CONSORT evaluations of methodological quality are summarized in Table 3.
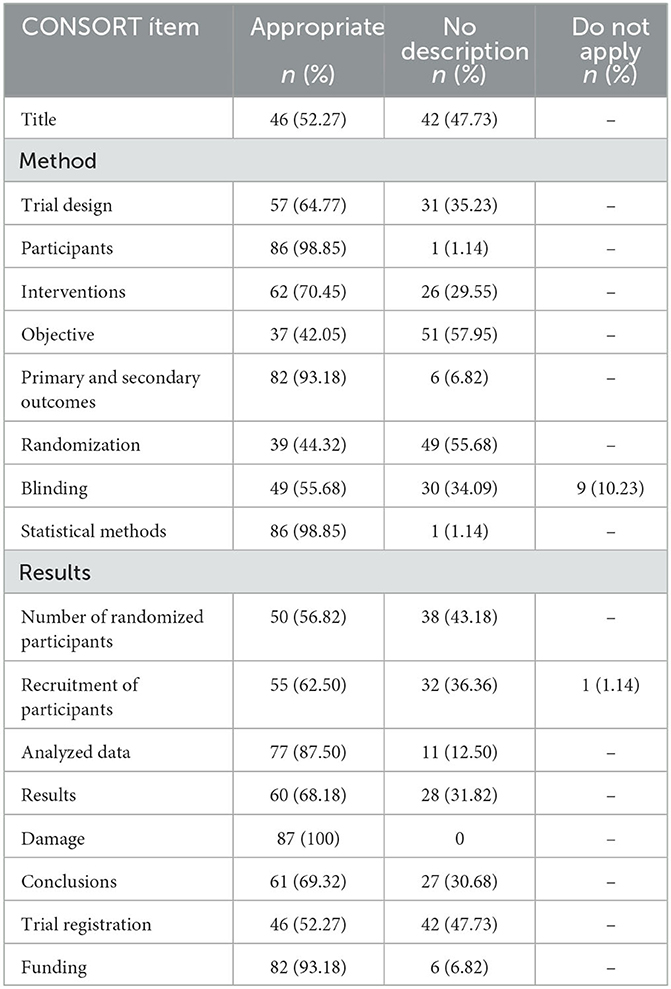
Table 3. Percentage distribution of scoring for each quality item in CONSORT checklist for articles included.
Bias risk assessment was done in the following order: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other biases.
When reviewing the bias risk in the 87 articles (40–126), it was found there was low or moderate risk in most clinical trials, 36 studies (41.38%) reported adequate random sequence generation and in 39 studies (44.83%) the bias risk was unclear. Concerning participants and health personnel blinding, 37 trials (42.53%) had a low bias risk and 38 were unclear (43.68%). In 15 studies (17.24%) it was reported that the allocation concealment was carried out by a person independent of the research team and in 45 (51.72%) it was not clear. In the section on blinding of outcome assessors, 20 studies (22.98%) had a low bias risk and in 54 (62.07%) the risk was unclear. Intention-to-treat analysis was applied in 58 studies (66.67%), in the rest of the studies it is not mentioned, or it is unclear how the analysis of missing data was done. Regarding the selective reporting of results, 95.39% (n = 83) of the articles had a low or unclear level of bias (see Risk table of bias, of the Supplementary material).
A total of 25 CONSORT items were evaluated in duplicate for each article, according to the response options: yes, no and not applicable. After calculating the frequencies and percentages of all the items, we found that 47 articles (53.41%) met the quality criteria in more than 50% and 41 (46.59%) met <50% of the checklist criteria of CONSORT, according to these results, the methodological quality in more than half of the articles was acceptable.
We compared the safety on sleep of 22 orally administered AP and four injectable AP used for schizophrenia treatment, the established reference category being placebo. We reviewed 70 randomized clinical trials published between 1990 and 2021; 61 trials reported insomnia as an adverse effect (87.14%), 41 studies reported somnolence (58.57%), and 15 (21.42%) reported sedation related to antipsychotic use. Figure 2 shows the network of comparisons of the antipsychotics included in this study for insomnia, somnolence, and sedation. The size of the nodes indicates that placebo is the most common comparator across trials, we weight all edges connecting placebo to an active treatment according to the number of trials.
Network consistency was examined using the loop-specific approach. Inconsistency factors were not found to be significant, although this cannot be taken as evidence of the absence of inconsistency. This is due to low power in some of the loops, especially in the presence of large heterogeneity in pairwise comparisons. On the other hand, when performing the analysis of global inconsistency in the network, there was no inconsistency in the case of insomnia (x2 = 36.85, df = 39, p = 0.57), somnolence (x2 = 34.10, df = 22, p = 0.05) and sedation (x2 = 7.46, df = 9, p = 0.59).
In the SUCRA analysis of studies reporting insomnia, chlorpromazine clearly ranked as the safest antipsychotic and the least likely to cause difficulty sleeping (Pr = 57%, SUCRA = 0.9), followed by clozapine (Pr = 20%, SUCRA = 0.8) and iloperidone (Pr = 16.9%, SUCRA = 0.8). The multivariate meta-regression analysis performed to examine the main nodes of the network taking placebo as the reference category, found that ziprasidone increases the risk of insomnia, OR= 1.56 (95% CrI: 1.18–2.06) while this risk is reduced with the use of olanzapine OR= 0.67 (95% CrI: 0.52–0.85), see Table 4.
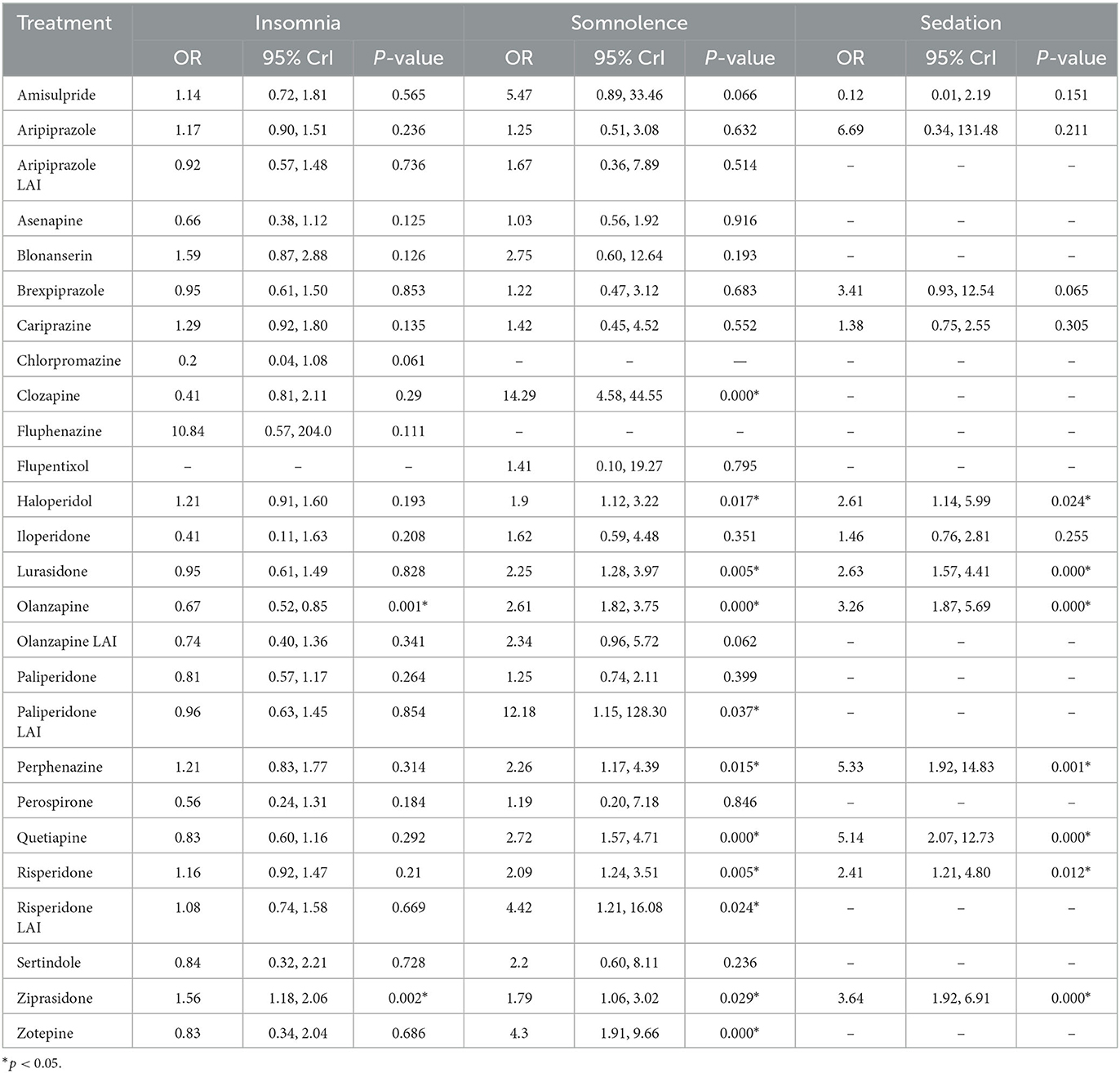
Table 4. Antipsychotic multivariate meta-regression results and adverse effects on sleep.
In the case of sedation, amisulpride was the safest antipsychotic (Pr = 89.9%, SUCRA = 1.0). The results of the multivariate meta -regression indicated that haloperidol increased the risk of sedation OR = 2.61 (95% CrI: 1.14–5.99), the same occurred with lurasidone OR = 2.63 (95% CrI: 1.57–4.41), olanzapine OR = 3.25 (95% CrI: 1.87–5.69), perphenazine OR = 5.33 (95% CrI: 1.92–14.83), quetiapine OR = 5.14 (95% CrI: 2.07–12.72), risperidone OR = 2.41 (95% CrI: 1.21–4.80) and ziprasidone OR = 3.64 (95% CrI: 1.92–6.91), while with the rest of the antipsychotics there were no statistically significant associations.
Regarding somnolence, fluphenazine (Pr = 26%, SUCRA = 0.6) and perospirone (Pr = 22.5%, SUCRA = 0.7) were the safest medications; in the multivariate meta-regression we found that clozapine OR = 14.29 (95% CrI: 4.58–44.55), haloperidol OR = 1.90 (95% CrI: 1.12–3.22), lurasidone OR = 2.25 (95% CrI: 1.28–3.97), olanzapine OR = 2.61 (95% CrI: 1.82–3.75), paliperidone LAI OR = 12.18 (95% CrI: 1.15–128.30), perphenazine OR = 2.26 (95% CrI: 1.17 – 4.39), quetiapine OR = 2.72 (95% CrI: 1.57–4.71), risperidone OR = 2.09 (95% CrI: 1.24–3.51), risperidone LAI OR= 4.42 (95% CrI: 1.21–16.08), ziprasidone OR = 1.79 (95% CrI: 1.06–3.02) and zotepine OR = 4.30 (95% CrI: 1.91–9.66) increased the risk of somnolence. Finally, in the geometry of the network it is observed that the size of the nodes corresponds to the number of RCTs that studied the adverse effects of antipsychotics on sleep, the directly comparable antipsychotics are linked with a line, and the thickness of each line corresponds to the inverse variance of the number of direct comparisons [see The ranking of antipsychotics (SUCRA) table, in the Supplementary material].
The original objective of this research was to carry out a systematic review and meta-analysis of the adverse effects on sleep in patients over 18 with schizophrenia receiving antipsychotic treatment. The most frequently reported sleep effects in randomized clinical trials were insomnia, somnolence, and sedation. This is consistent with studies describing DRA effects on sleep. Waite et al. (127) reported in a systematic review that 50% of patients with psychosis presented insomnia. This sleep problem improved considerably and modest changes in psychotic symptoms were observed when receiving some psychological intervention. In another study, Thompson et al. (128) conducted a review evaluating the benefits and adverse effects of atypical antipsychotics, finding that there was no clinical difference in insomnia administering quetiapine or placebo. However, they included only 13 studies, so the evidence quality was low.
When evaluating the quality of the studies reviewed using the CONSORT checklist, we found that more than half of the articles (53.41%) showed acceptable methodological quality. In most of the included studies (n = 87) bias risk was classified as low and unclear. For example, in random sequence generation, the sum of the percentage of low and unclear risk reached 86.21%, in allocation concealment it reached 68.97%, in blinding of participants and personnel it showed 86.21%, in the blinding of result evaluators, it was 85.06%, in the incomplete data it reached 87.36%, in the selective reporting of results it reached 95.40% and in other biases it was 62.07%.
We also found that FGAs and SGAs have adverse effects on sleep and are less safe than no antipsychotic for the treatment of symptoms in schizophrenia. The effect sizes are clinically meaningful and comparable to previous findings. In contrast to our results, in a head-to-head comparison study of 37 antipsychotics, zuclopenthixol was found to rank first in association with sedation and somnolence among drugs reported to FAERS (129), and are consistent with the large-scale network meta-analysis in which zuclopenthixol stood out among 32 antipsychotics and their found that older antipsychotics were associated with prolactin elevation and more extrapiramidal side effects, whereas newer antipsychotics were associated with more sedation and weight gain (12). In addition, Kishi et al. (130) examined the safety of antipsychotic use in schizophrenia using only randomized trials conducted in Japan. They found that asenapine, lurasidone, olanzapine, perospirone, quetiapine, and mosapramine were associated with a higher incidence of somnolence. Clozapine was associated with a lower incidence of insomnia compared with placebo.
The safety ranking of different AP, based on the SUCRA calculation regarding insomnia, indicated that probability of presenting insomnia as an adverse effect, chlorpromazine and clozapine were the safest AP. Participants receiving amisulpride were less likely to experience sedation, while those receiving flupentizole and perospirone reported less sleepiness. In contrast, the AP most likely to affect sleep were ziprasidone and fluphenazine (insomnia), perphenazine and quetiapine (sedation), and clozapine and zotepine (somnolence).
Our results show that olanzapine reduced insomnia risk by 22% when compared to placebo. This AP has been shown to have a positive effect on sleep efficiency, slow wave sleep and REM sleep (131, 132). Ziprasidone increased the risk of insomnia by 1.58 times (p < 0.01). There is evidence that the three most frequent adverse events associated with the use of ziprasidone are: insomnia (21–42%), somnolence (14–26%), and anxiety (19–21%) (133).
On the other hand, we found that haloperidol, lurasidone, olanzapine, perphenazine, quetiapine, risperidone, zotepine, and ziprasidone caused sedation and somnolence as adverse sleep effects. Those that caused greater sedation were perphenazine (OR= 5.33), quetiapine (OR= 5.14) and ziprasidone (OR= 3.64). Among the AP that caused more sedation were clozapine (OR = 14.42), zotepine (OR = 4.30), and quetiapine (OR = 2.77). All these values were statistically significant (p < 0.01).
Our results are similar to other previous studies. Fang et al. (134) carried out a systematic review in which they considered the Absolute Risk Increase and the NNH to classify AP by the level of somnolence. Clozapine had a high level of somnolence; olanzapine, perphenazine, quetiapine, risperidone, and ziprasidone had a moderate level of somnolence, while those that produced low somnolence were aripiprazole, haloperidol, lurasidone, asenapine, paliperidone, and cariprazine.
Ziprasidone is generally better tolerated on sleep compared to more sedating AP, because it has a shorter duration of action (2–4 h) (135).
Adverse effects on sleep related to antipsychotic drugs use generally have a negative impact on functionality and social interaction, preventing patients with schizophrenia from benefiting from psychiatric rehabilitation and other treatments. For example, sedation and somnolence would negatively increase negative feelings and attitudes toward taking AP, making it difficult for patients to reintegrate into society (136–138). In contrast, AP with mild or no adverse effects on sleep would improve treatment compliance and long-term efficacy (130).
Regarding the limitations, it is important to mention that some articles could not be retrieved in full, despite performing the search in different bibliographic databases, for this reason they were not included in the analysis. Search terms were limited to thesaurus Mesh and DeCS, it cannot be assumed that all the articles and areas in the health field that address the safety of AP have been covered. The available evidence was limited for some comparisons, especially for the older antipsychotics and those of recent appearance. We missed some RCT that were published before 1990, however in 1994, might have conditioned some differences between oldest and newer studies. For example, the change from DSM-III-TR to DSM-IV (139).
All articles were written in English, and despite the search of journal databases in Spanish, no article was found that met our inclusion criteria. Overall, we identified a wide variety of doses and treatment durations in the intervention groups, many different groups of comparators, and variations in the diagnostic criteria and clinical characteristics of patients with schizophrenia, which increased the heterogeneity between trials. Despite the abundance of safety variables that we planned to assess, the available information in each clinical trial was usually reported using different methods, making meta-analyses challenging. Nevertheless, it is possible to draw conclusions from direct and indirect comparisons.
On the other hand, articles that studied AP adverse effects in patients with other psychotic disorders (e.g., schizoaffective disorder, schizophreniform disorder, brief psychotic disorder, and delusional disorder) were not included. In addition, there is the heterogeneity shown by the articles found by age range, the duration of the studies, the size of the participant samples, as well as the results reported.
In terms of clinical practice, our review provides information on the adverse effects of antipsychotics on sleep. This may improve the decision-making process when prescribing AP treatment for each patient, taking into account the safety profile and which of these AP exacerbate or ameliorate sleep problems. Regarding the implications for research, we show that the available evidence on sleep effects of most AP is still insufficient, and further studies are needed in this population. We suggest better reporting of methodological features in primary studies (e.g., description of allocation concealment procedure, blinding of outcome assessors, RCT registration).
In order to better elucidate the safety of AP on sleep, new studies on larger populations are needed. Furthermore, there was a degree of uncertainty in identifying which sleep-related adverse effects were linked to antipsychotic drugs, as this was generally determined by the staff members' understanding, study investigators or by spontaneous reports of patients, especially in articles that were published between 1990 and 2000, because the conceptual definitions or methodological quality of ADRs is not well-described. In this way, health care decision makers can consider the safest therapeutic option at a lower cost, which could be an alternative to be implemented in adults with schizophrenia.
The antipsychotics with the least adverse effects on sleep were olanzapine, chlorpromazine, and clozapine for insomnia; flupentixol and perospirone for somnolence; amisulpride had a lower risk of sedation.
In contrast, those with a less secure profile were ziprasidone, blonanserin, and fluphenazine (insomnia); clozapine, zotepine, and paliperidone LAI (somnolence); perphenazine and quetiapine (sedation).
These results are mainly referable to oral AP; in the case of injectable AP, it is necessary to expand the scientific evidence, route of administration should be considered in the analysis. We also suggest carrying out a systematic review on injectables AP effects on sleep.
Adverse effects on sleep may not always be desirable, but they are often difficult to avoid in psychiatric patients. Some of the most AP have unique benefits that may justify their use. Dosing according to the clinical response may improve tolerability, adverse effects do not get in the way.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
YV contributed to the conception and design of the study, organized the database, and performed the statistical analysis. RS-A contributed to the conception and design of the study, organized the database, and wrote the first draft of the manuscript. VV, DV, and GN contributed to the conception and design of the study. RE wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
We would like to thank the Universidad Nacional Autónoma de México and Consejo Nacional de Ciencia y Tecnología (Conacyt), with number of CVU 481771 for the support received. We would also like to thank all the individuals who participated in this study and the following individuals for their assistance with data collection and management, in special Ricardo Orozco Zavala.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1189768/full#supplementary-material
1. Marder SR, Cannon TD. Schizophrenia. N Engl J Med. (2019) 381:1753–61. doi: 10.1056/NEJMra1808803
2. Cohrs S. Sleep disturbances in patients with schizophrenia: Impact and effect of antipsychotics. CNS Drugs. (2008) 22:939–62. doi: 10.2165/00023210-200822110-00004
3. Monti J, Monti D. Sleep disturbance in schizophrenia. Int Rev Psychiatry. (2005) 17:247–53. doi: 10.1080/09540260500104516
4. Winokur A, Kamath J. The effect of typical and atypical antipsychotic drugs on sleep of schizophrenic patients. In: En: Serotonin and Sleep: Molecular, Functional and Clinical Aspects. Basel: Birkhäuser Basel (2008). p. 587–610.
5. Teasdale S, Mörkl S, Müller-Stierlin AS. Nutritional psychiatry in the treatment of psychotic disorders: current hypotheses and research challenges. Brain Behav Immun Health. (2020) 5:100070. doi: 10.1016/j.bbih.2020.100070
6. Longden E, Sampson M, Read J. Childhood adversity and psychosis: generalised or specific effects? Epidemiol Psychiatr Sci. (2016) 25:349–59. doi: 10.1017/S204579601500044X
7. Haddad P, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat Outcome Meas. (2014) 5:43–62. doi: 10.2147/PROM.S42735
8. Lambert M, Conus P, Eide P, Mass R, Karow A, Moritz S, et al. Impact of present and past antipsychotic side effects on attitude toward typical antipsychotic treatment and adherence. Eur Psychiatry. (2004) 19:415–22. doi: 10.1016/j.eurpsy.2004.06.031
9. Wang F, Zhang P, Cao N, Hu J, Sorrentino R. Exploring the associations between drug side-effects and therapeutic indications. J Biomed Inform. (2014) 51:15–23. doi: 10.1016/j.jbi.2014.03.014
10. Pillinger T, McCutcheon RA, Vano L, Mizuno Y, Arumuham A, Hindley G, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with Schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. (2020) 7:64–77. doi: 10.1016/S2215-0366(19)30416-X
11. Citrome L. Activating and sedating adverse effects of second-generation antipsychotics in the treatment of schizophrenia and major depressive disorder: absolute risk increase and number needed to harm. J Clin Psychopharmacol. (2017) 37:138–47. doi: 10.1097/JCP.0000000000000665
12. Huhn M, Nikolakopoulou A, Schneider-Thoma J, Krause M, Samara M, Peter N, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. (2019) 394:939–51. doi: 10.1016/S0140-6736(19)31135-3
13. Doghramji K, Jangro, W. Adverse effects of psychotropic medications on sleep. Sleep Med Clin. (2016) 11:503–14. doi: 10.1016/j.jsmc.2016.08.001
14. Krystal A, Goforth H, Roth T. Effects of antipsychotic medications on sleep in schizophrenia. Int Clin Psychopharmacol. (2008) 23:150–60. doi: 10.1097/YIC.0b013e3282f39703
15. Shen J, Barbera J, Shapiro CM. Distinguishing sleepiness and fatigue: Focus on definition and measurement. Sleep Med Rev. (2006) 10:63–76. doi: 10.1016/j.smrv.2005.05.004
16. Leucht S, Cipriani A, Spineli L, Mavridis D, Örey D, Richter F, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments metaanalysis. Lancet. (2013) 382:951–62. doi: 10.1016/S0140-6736(13)60733-3
17. Zareifopoulos N, Panayiotakopoulos G. Treatment options for acute agitation in psychiatric patients: Theoretical and empirical evidence. Cureus. (2019) 11:e6152. doi: 10.7759/cureus.6152
18. Cramer JA, Rosenheck R. Compliance with medication regimens for mental and physical disorders. Psychiatr Serv. (1998) 49:196–201. doi: 10.1176/ps.49.2.196
19. Andrade C, Kisely S, Monteiro I, Rao S. Antipsychotic augmentation with modafinil or armodafinil for negative symptoms of schizophrenia: systematic review and meta-analysis of randomized controlled trials. J Psychiatr Res. (2015) 60:14–21. doi: 10.1016/j.jpsychires.2014.09.013
20. Connor JR. Pathophysiology of restless legs syndrome: evidence for iron involvement. Curr Neurol Neurosci Rep. (2008) 8:162–6. doi: 10.1007/s11910-008-0026-x
21. Bollu PC, Yelam A, Thakkar MM. Sleep medicine: restless legs syndrome. Mol Med. (2018) 115:380–7.
22. Shah C, Sharma T, Kablinger A. Controversies in the use of second-generation antipsychotics as sleep agent. Pharmacol Res. (2014) 79:1–8. doi: 10.1016/j.phrs.2013.10.005
23. Stroup TS, Gray N. Management of common adverse effects of antipsychotic medications. World Psychiatry. (2018) 17:341–56. doi: 10.1002/wps.20567
24. Kaar SJ, Natesan S, McCutcheon R, Howes OD. Antipsychotics: Mechanisms underlying clinical response and side-effects and novel treatment approaches based on pathophysiology. Neuropharmacology. (2020) 172:107704. doi: 10.1016/j.neuropharm.2019.107704
25. Monti JM, Torterolo P, Pandi Perumal SR. The effects of second-generation antipsychotic drugs on sleep variables in healthy subjects and patients with schizophrenia. Sleep Med Rev. (2017) 33:51–7. doi: 10.1016/j.smrv.2016.05.002
26. Lin CY, Chiang CH, Tseng MM, Tam KW, Loh EW. Effects of quetiapine on sleep: a systematic review and meta-analysis of clinical trials. Eur Neuropsychopharmacol. (2023) 67:22–36. doi: 10.1016/j.euroneuro.2022.11.008
27. Stummer L, Markovic M, Maroney ME. Pharmacologic treatment options for insomnia in patients with schizophrenia. Medicines. (2018) 5:88. doi: 10.3390/medicines5030088
28. Cui Q, Tian J, Song X, Yang K. Does the CONSORT checklist for abstracts improve the quality of reports of randomized controlled trials on clinical pathways? Quality of RCTs on clinical pathway. J Eval Clin Pract. (2014) 20:827–33. doi: 10.1111/jep.12200
29. Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c869. doi: 10.1136/bmj.c869
30. Higgins JPT, Green, S, editors,. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration (2011). Available online at: https://www.cochranelibrary.com/es/central/doi/10.1002/central/CN-00871375/full (accessed February, 2023).
31. Higgins JPT, Welton NJ. Network meta-analysis: a norm for comparative effectiveness? Lancet. (2015) 386:628–30. doi: 10.1016/S0140-6736(15)61478-7
32. Gupta U, Verma M. Placebo in clinical trials. Perspect Clin Res. (2013) 4:49–52. doi: 10.4103/2229-3485.106383
33. European Medicines Agency (EMA),. Scientific Guidelines for Human Medicinal Products-Clinical Efficacy Safety Guidelines. (2020). Available online at: https://www.ema.europa.eu/en/human-regulatory/research-development/scientific-guidelines/clinical-efficacy-safety-guidelines (accessed February, 2023).
34. Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Intern Emerg Med. (2017) 12:103–11. doi: 10.1007/s11739-016-1583-7
35. Catalá F., Alonso A., Hutton B. Global collaborative networks on meta-analyses of randomized trials published in high impact factor medical journals: a social network analysis. BMC Med. (2014) 12:15. doi: 10.1186/1741-7015-12-15
36. Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS ONE. (2013) 8:e76654. doi: 10.1371/journal.pone.0076654
37. Veroniki AA, Straus SE, Rücker G, Tricco AC. Is providing uncertainty intervals in treatment ranking helpful in a network meta-analysis? J Clin Epidemiol. (2018) 100:122–9. doi: 10.1016/j.jclinepi.2018.02.009
38. Salanti G, Ades AE, Ioannidis JPA. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. (2011) 64:163–71. doi: 10.1016/j.jclinepi.2010.03.016
39. Bai F, Li GG, Liu Q, Niu X, Li R, Ma H. Short-term efficacy and safety of IL-17, IL-12/23, and IL-23 inhibitors brodalumab, secukinumab, ixekizumab, ustekinumab, guselkumab, tildrakizumab, and risankizumab for the treatment of moderate to severe plaque psoriasis: a systematic review and network meta-analysis of randomized controlled trials. J Immunol Res. (2019) 2019:1–25. doi: 10.1155/2019/2546161
40. Abdolahian E, Mohareri F, Bordbar MRF. Haloperidol versus risperidone: a comparison of beneficial effect on cognitive function of patients with chronic schizophrenia. Iran J Psychiatry Behav Sci. (2008) 2:14–20.
41. Álvarez E, Olivares JM, Bousoño M, Gómez JC. A randomized, 1-year follow-up study of olanzapine and risperidone in the treatment of negative symptoms in outpatients with schizophrenia. J Clin Psychopharmacol. (2006) 26:238–49. doi: 10.1097/01.jcp.0000222513.63767.de
42. Arato M, O'Connor R, Meltzer HY, ZEUS Study Group. A 1-year, double-blind, placebo-controlled trial of ziprasidone 40, 80 and 160 mg/day in chronic schizophrenia: the Ziprasidone Extended Use in Schizophrenia (ZEUS) study. Int Clin Psychopharmacol. (2002) 17:207–15. doi: 10.1097/00004850-200209000-00001
43. Azorin JM, Strub N, Loft H. A double-blind, controlled study of sertindole versus risperidone in the treatment of moderate-to-severe schizophrenia. Int Clin Psychopharmacol. (2006) 21:49–56. doi: 10.1097/01.yic.0000177020.26311.a7
44. Beasley CM Jr, Tollefson G, Tran P, Satterlee W, Sanger T, Hamilton S, et al. Olanzapine versus placebo and haloperidol: acute phase results of the North American double-blind olanzapine trial. Neuropsychopharmacology. (1996) 14:111–23. doi: 10.1016/0893-133X(95)00069-P
45. Berwaerts J, Liu Y, Gopal S, Nuamah I, Xu H, Savitz A, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA psychiatry. (2015) 72:830–9. doi: 10.1001/jamapsychiatry.2015.0241
46. Bitter I, Dossenbach MR, Brook S, Feldman PD, Metcalfe S, Gagiano CA, et al. Olanzapine versus clozapine in treatment-resistant or treatment-intolerant schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. (2004) 28:173–80. doi: 10.1016/j.pnpbp.2003.09.033
47. Breier A, Berg PH, Thakore JH, Naber D, Gattaz WF, Cavazzoni P, et al. Olanzapine versus ziprasidone: results of a 28-week double-blind study in patients with schizophrenia. Am J Psychiatry. (2005) 162:1879–87. doi: 10.1176/appi.ajp.162.10.1879
48. Bhowmick S, Hazra A, Ghosh M. Amisulpride versus olanzapine in the treatment of schizophrenia in Indian patients: randomized controlled trial. Aust New Zeal J Psychiatry. (2010) 44:237–42. doi: 10.3109/00048670903487134
49. Chue P, Eerdekens M, Augustyns I, Lachaux B, Molčan P, Eriksson L, et al. Comparative efficacy and safety of long-acting risperidone and risperidone oral tablets. Eur Neuropsychopharmacol. (2005) 15:111–7. doi: 10.1016/j.euroneuro.2004.07.003
50. Colonna L, Saleem P, Dondey-Nouvel L, Rein W. Long-term safety and efficacy of amisulpride in subchronic or chronic schizophrenia. Amisulpride Study Group. Int Clin Psychopharmacol. (2000) 15:13–22. doi: 10.1097/00004850-200015010-00002
51. Cooper SJ, Butler A, Tweed J, Welch C, Raniwalla J. Zotepine in the prevention of recurrence: a randomised, double-blind, placebo-controlled study for chronic schizophrenia. Psychopharmacology. (2000) 150:237–43. doi: 10.1007/s002130000452
52. Conley RR, Tamminga CA, Bartko JJ, Richardson C, Peszke M, Lingle J, et al. Olanzapine compared with chlorpromazine in treatment-resistant schizophrenia. Am J Psychiatry. (1998) 155:914–20. doi: 10.1176/ajp.155.7.914
53. Correll CU, Skuban A, Ouyang J, Hobart M, Pfister S, McQuade RD, et al. Efficacy and safety of brexpiprazole for the treatment of acute schizophrenia: a 6-week randomized, double-blind, placebo-controlled trial. Am J Psychiatry. (2015) 172:870–80. doi: 10.1176/appi.ajp.2015.14101275
54. Cutler AJ, Marcus RN, Hardy SA, O'Donnell A, Carson WH, McQuade RD. The efficacy and safety of lower doses of aripiprazole for the treatment of patients with acute exacerbation of schizophrenia. CNS Spectr. (2006) 11:691–702. doi: 10.1017/S1092852900014784
55. Cutler AJ, Kalali AH, Weiden PJ, Hamilton J, Wolfgang CD. Four-week, double-blind, placebo-and ziprasidone-controlled trial of iloperidone in patients with acute exacerbations of schizophrenia. J Clin Psychopharmacol. (2008) 28:S20–8. doi: 10.1097/JCP.0b013e318169d4ce
56. Davidson M, Emsley R, Kramer M, Ford L, Pan G, Lim P, et al. Efficacy, safety and early response of paliperidone extended-release tablets (paliperidone ER): results of a 6-week, randomized, placebo-controlled study. Schizophr Res. (2007) 93:117–30. doi: 10.1016/j.schres.2007.03.003
57. Detke HC, Weiden PJ, Llorca PM, Choukour M, Watson SB, Brunner E, et al. Comparison of olanzapine long-acting injection and oral olanzapine: a 2-year, randomized, open-label study in outpatients with schizophrenia. J Clin Psychopharmacol. (2014) 34:426–34. doi: 10.1097/JCP.0000000000000140
58. Dossenbach MR, Folnegovic-Smalc V, Hotujac L, Uglesic B, Tollefson GD, Grundy SL, et al. Double-blind, randomized comparison of olanzapine versus fluphenazine in the long-term treatment of schizophrenia. Progr Neuropsychopharmacol Biol Psychiatry. (2004) 28:311–8. doi: 10.1016/j.pnpbp.2003.10.010
59. Downing AM, Kinon BJ, Millen BA, Zhang L, Liu L, Morozova MA, et al. A double-blind, placebo-controlled comparator study of LY2140023 monohydrate in patients with schizophrenia. BMC Psychiatry. (2014) 14:1–12. doi: 10.1186/s12888-014-0351-3
60. Durgam S, Starace A, Li D, Migliore R, Ruth A, Németh G, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. (2014) 152:450–7. doi: 10.1016/j.schres.2013.11.041
61. Durgam S, Cutler AJ, Lu K, Migliore R, Ruth A, Laszlovszky I, et al. Cariprazine in acute exacerbation of schizophrenia: a fixed-dose, phase 3, randomized, double-blind, placebo- and active-controlled trial. J Clin Psychiatry. (2015) 76:e1574–82. doi: 10.4088/JCP.15m09997
62. Durgam S, Litman RE, Papadakis K, Li D, Németh G, Laszlovszky I. Cariprazine in the treatment of schizophrenia: a proof-of-concept trial. Int Clin Psychopharmacol. (2016) 31:61–8. doi: 10.1097/YIC.0000000000000110
63. Durgam S, Earley W, Li R, Li D, Lu K, Laszlovszky I, et al. Long-term cariprazine treatment for the prevention of relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled trial. Schizophr Res. (2016) 176:264–71. doi: 10.1016/j.schres.2016.06.030
64. Emsley RA, Raniwalla J, Bailey PJ, Jones AM. A comparison of the effects of quetiapine (‘seroquel') and haloperidol in schizophrenic patients with a history of and a demonstrated, partial response to conventional antipsychotic treatment. PRIZE Study Group. Int Clin Psychopharmacol. (2000) 15:121–31. doi: 10.1097/00004850-200015030-00001
65. Fleischhacker WW, Gopal S, Lane R, Gassmann-Mayer C, Lim P, Hough D, et al. A randomized trial of paliperidone palmitate and risperidone long-acting injectable in schizophrenia. Int J Neuropsychopharmacol. (2012) 15:107–18. doi: 10.1017/S1461145711001076
66. Fleischhacker WW, Sanchez R, Perry PP, Jin N, Peters-Strickland T, Johnson BR, et al. Aripiprazole once-monthly for treatment of schizophrenia: double-blind, randomised, non-inferiority study. Br J Psychiatry. (2014) 205:135–44. doi: 10.1192/bjp.bp.113.134213
67. Garcia E, Robert M, Peris F, Nakamura H, Sato N, Terazawa Y. The efficacy and safety of blonanserin compared with haloperidol in acute-phase schizophrenia: a randomized, double-blind, placebo-controlled, multicentre study. CNS Drugs. (2009) 23:615–25. doi: 10.2165/00023210-200923070-00006
68. Gattaz WF, Diehl A, Geuppert MS, Hubrich P, Schmitt A, Linde I, et al. Olanzapine versus flupenthixol in the treatment of inpatients with schizophrenia: a randomized double-blind trial. Pharmacopsychiatry. (2004) 37:279–85. doi: 10.1055/s-2004-832684
69. Golden G, Honigfeld G. Bioequivalence of clozapine orally disintegrating 100-mg tablets compared with clozapine solid oral 100-mg tablets after multiple doses in patients with schizophrenia. Clin Drug Investig. (2008) 28:231–9. doi: 10.2165/00044011-200828040-00004
70. Hirsch SR, Kissling W, Bäuml J, Power A, O'Connor R. A 28-week comparison of ziprasidone and haloperidol in outpatients with stable schizophrenia. J Clin Psychiatry. (2002) 63:516–23. doi: 10.4088/JCP.v63n0609
71. Hough D, Lindenmayer JP, Gopal S, Melkote R, Lim P, Herben V, et al. Safety and tolerability of deltoid and gluteal injections of paliperidone palmitate in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. (2009) 33:1022–31. doi: 10.1016/j.pnpbp.2009.05.014
72. Huang M, Yu L, Pan F, Lu S, Hu S, Hu J, et al. A randomized, 13-week study assessing the efficacy and metabolic effects of paliperidone palmitate injection and olanzapine in first-episode schizophrenia patients. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 81:122–30. doi: 10.1016/j.pnpbp.2017.10.021
73. Hwang TJ, Lin SK, Lin HN. Efficacy and safety of zotepine for the treatment of Taiwanese schizophrenic patients: a double-blind comparison with haloperidol. J Formos Med Assoc. (2001) 100:811–6.
74. Ishigooka J, Nakamura J, Fujii Y, Iwata N, Kishimoto T, Iyo M, et al. Efficacy and safety of aripiprazole once-monthly in Asian patients with schizophrenia: a multicenter, randomized, double-blind, non-inferiority study versus oral aripiprazole. Schizophr Res. (2015) 161:421–8. doi: 10.1016/j.schres.2014.12.013
75. Kahn RS, Schulz SC, Palazov VD, Reyes EB, Brecher M, Svensson O, et al. Efficacy and tolerability of once-daily extended release quetiapine fumarate in acute schizophrenia: a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. (2007) 68:832–42. doi: 10.4088/JCP.v68n0603
76. Kane JM, Eerdekens M, Lindenmayer JP, Keith SJ, Lesem M, Karcher K. Long-acting injectable risperidone: efficacy and safety of the first long-acting atypical antipsychotic. Am J Psychiatry. (2003) 160:1125–32. doi: 10.1176/appi.ajp.160.6.1125
77. Kane JM, Canas F, Kramer M, Ford L, Gassmann-Mayer C, Lim P, et al. Treatment of schizophrenia with paliperidone extended-release tablets: a 6-week placebo-controlled trial. Schizophr Res. (2007) 90:147–61. doi: 10.1016/j.schres.2006.09.012
78. Kane JM, Detke HC, Naber D, Sethuraman G, Lin DY, Bergstrom RF, et al. Olanzapine long-acting injection: a 24-week, randomized, double-blind trial of maintenance treatment in patients with schizophrenia. Am J Psychiatry. (2010) 167:181–9. doi: 10.1176/appi.ajp.2009.07081221
79. Kane JM, Mackle M, Snow-Adami L, Zhao J, Szegedi A, Panagides J, et al. randomized placebo-controlled trial of asenapine for the prevention of relapse of schizophrenia after long-term treatment. J Clin Psychiatry. (2011) 72:349–55. doi: 10.4088/JCP.10m06306
80. Kane JM, Sanchez R, Perry PP, Jin N, Johnson BR, Forbes RA, et al. Aripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. (2012) 73:617–24. doi: 10.4088/JCP.11m07530
81. Kane JM, Skuban A, Ouyang J, Hobart M, Pfister S, McQuade RD, et al. A multicenter, randomized, double-blind, controlled phase 3 trial of fixed-dose brexpiprazole for the treatment of adults with acute schizophrenia. Schizophr Res. (2015) 164:127–35. doi: 10.1016/j.schres.2015.01.038
82. Kasper S, Lerman MN, McQuade RD, Saha A, Carson WH, Ali M, et al. Efficacy and safety of aripiprazole vs. haloperidol for long-term maintenance treatment following acute relapse of schizophrenia. Int J Neuropsychopharmacol. (2003) 6:325–37. doi: 10.1017/S1461145703003651
83. Kramer M, Simpson G, Maciulis V, Kushner S, Vijapurkar U, Lim P, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. (2007) 27:6–14. doi: 10.1097/JCP.0b013e31802dda4a
84. Kerwin R, Millet B, Herman E, Banki CM, Lublin H, Pans M, et al. A multicentre, randomized, naturalistic, open-label study between aripiprazole and standard of care in the management of community-treated schizophrenic patients Schizophrenia Trial of Aripiprazole: (STAR) study. Eur Psychiatry. (2007) 22:433–43. doi: 10.1016/j.eurpsy.2007.03.002
85. Lal S, Thavundayil JX, Vasavan Nair NP, Annable L, Ng MK, Ng YK, et al. Levomepromazine versus chlorpromazine in treatment-resistant schizophrenia: a double-blind randomized trial. J Psychiatry Neurosci. (2006) 31:271–9.
86. Landbloom R, Mackle M, Wu X, Kelly L, Snow-Adami L, McIntyre RS, et al. Asenapine for the treatment of adults with an acute exacerbation of schizophrenia: results from a randomized, double-blind, fixed-dose, placebo-controlled trial with olanzapine as an active control. CNS Spectr. (2017) 22:333–41. doi: 10.1017/S1092852916000377
87. Lecrubier Y, Quintin P, Bouhassira M, Perrin E, Lancrenon S. The treatment of negative symptoms and deficit states of chronic schizophrenia: olanzapine compared to amisulpride and placebo in a 6-month double-blind controlled clinical trial. Acta Psychiatr Scand. (2006) 114:319–27. doi: 10.1111/j.1600-0447.2006.00887.x
88. Li H, Rui Q, Ning X, Xu H, Gu N. A comparative study of paliperidone palmitate and risperidone long-acting injectable therapy in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. (2011) 35:1002–8. doi: 10.1016/j.pnpbp.2011.02.001
89. Li Y, Li H, Liu Y, Yan X, Yue Y, Qian M. Comparison of quetiapine and risperidone in Chinese Han patients with schizophrenia: results of a single-blind, randomized study. Curr Med Res Opin. (2012) 28:1725–32. doi: 10.1185/03007995.2012.728524
90. Li H, Yao C, Shi J, Yang F, Qi S, Wang L, et al. Comparative study of the efficacy and safety between blonanserin and risperidone for the treatment of schizophrenia in Chinese patients: a double-blind, parallel-group multicenter randomized trial. J Psychiatr Res. (2015) 69:102–9. doi: 10.1016/j.jpsychires.2015.07.015
91. Lin CH, Wang FC, Lin SC, Huang YH, Chen CC, Lane HY. Antipsychotic combination using low-dose antipsychotics is as efficacious and safe as, but cheaper, than optimal-dose monotherapy in the treatment of schizophrenia: a randomized, double-blind study. Int Clin Psychopharmacol. (2013) 28:267–74. doi: 10.1097/YIC.0b013e3283633a83
92. Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. (2005) 353:1209–23. doi: 10.1056/NEJMoa051688
93. Loebel AD, Cucchiaro JB, Sarma K, Xu L, Hsu C, Kalali AH, et al. Efficacy and safety of lurasidone 80 mg/day and 160 mg/day in the treatment of schizophrenia: a randomized, double-blind, placebo- and active-controlled trial. Schizophr Res. (2013) 145:101–9. doi: 10.1016/j.schres.2013.01.009
94. Loebel AD, Siu CO, Cucchiaro JB, Pikalov AA, Harvey PD. Daytime sleepiness associated with lurasidone and quetiapine XR: results from a randomized double-blind, placebo-controlled trial in patients with schizophrenia. CNS Spectr. (2014) 19:197–205. doi: 10.1017/S1092852913000904
95. Luthringer R, Staner L, Noel N, Muzet M, Gassmann-Mayer C, Talluri K, et al. A double-blind, placebo-controlled, randomized study evaluating the effect of paliperidone extended-release tablets on sleep architecture in patients with schizophrenia. Int Clin Psychopharmacol. (2007) 22:299–308. doi: 10.1097/YIC.0b013e3281c55f4f
96. Marder SR, Kramer M, Ford L, Eerdekens E, Lim P, Eerdekens M, et al. Efficacy and safety of paliperidone extended-release tablets: results of a 6-week, randomized, placebo-controlled study. Biol Psychiatry. (2007) 62:1363–70. doi: 10.1016/j.biopsych.2007.01.017
97. Meltzer HY, Cucchiaro JB, Silva R, Ogasa M, Phillips D, Xu J, et al. Lurasidone in the treatment of schizophrenia: a randomized, double-blind, placebo- and olanzapine-controlled study. Am J Psychiatry. (2011) 168:957–67. doi: 10.1176/appi.ajp.2011.10060907
98. Meltzer HY, Risinger R, Nasrallah HA, Du Y, Zummo J, Corey L, et al. A randomized, double-blind, placebo-controlled trial of aripiprazole lauroxil in acute exacerbation of schizophrenia. J Clin Psychiatry. (2015) 76:1085–90. doi: 10.4088/JCP.14m09741
99. Naber D, Hansen K, Forray C, Baker RA, Sapin C, Beillat M, et al. Qualify: a randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophr Res. (2015) 168:498–504. doi: 10.1016/j.schres.2015.07.007
100. Nakamura M, Ogasa M, Guarino J, Phillips D, Severs J, Cucchiaro JB, et al. Lurasidone in the treatment of acute schizophrenia: a double-blind, placebo-controlled trial. J Clin Psychiatry. (2009) 70:829–36. doi: 10.4088/JCP.08m04905
101. Nakamura T, Kubota T, Iwakaji A, Imada M, Kapás M, Morio Y. Clinical pharmacology study of cariprazine (MP-214) in patients with schizophrenia (12-week treatment). Drug Des Devel Ther. (2016) 10:327–38. doi: 10.2147/DDDT.S95100
102. Nasser AF, Henderson DC, Fava M, Fudala PJ, Twumasi-Ankrah P, Kouassi A, et al. Efficacy, safety, and tolerability of RBP-7000 once-monthly risperidone for the treatment of acute schizophrenia: an 8-week, randomized, double-blind, placebo-controlled, multicenter phase 3 study. J Clin Psychopharmacol. (2016) 36:130–40. doi: 10.1097/JCP.0000000000000479
103. Németh G, Laszlovszky I, Czobor P, Szalai E, Szatmári B, Harsányi J, et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet. (2017) 389:1103–13. doi: 10.1016/S0140-6736(17)30060-0
104. Ogasa M, Kimura T, Nakamura M, Guarino J. Lurasidone in the treatment of schizophrenia: a 6-week, placebo-controlled study. Psychopharmacology. (2013) 225:519–30. doi: 10.1007/s00213-012-2838-2
105. Olié JP, Spina E, Murray S, Yang R. Ziprasidone and Amisulpride effectively treat negative symptoms of schizophrenia: results of a 12-week, double-blind study. Int Clin Psychopharmacol. (2006) 21:143–51. doi: 10.1097/01.yic.0000182121.59296.70
106. Pandina G, Lane R, Gopal S, Gassmann-Mayer C, Hough D, Remmerie B, et al. A double-blind study of paliperidone palmitate and risperidone long-acting injectable in adults with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. (2011) 35:218–26. doi: 10.1016/j.pnpbp.2010.11.008
107. Pigott TA, Carson WH, Saha AR, Torbeyns AF, Stock EG, Ingenito GG. Aripiprazole for the prevention of relapse in stabilized patients with chronic schizophrenia: a placebo-controlled 26-week study. J Clin Psychiatry. (2003) 64:1048–56. doi: 10.4088/JCP.v64n0910
108. Potkin SG, Cohen M, Panagides J. Efficacy and tolerability of asenapine in acute schizophrenia: a placebo- and risperidone-controlled trial. J Clin Psychiatry. (2007) 68:1492–500. doi: 10.4088/JCP.v68n1004
109. Potkin SG, Kimura T, Guarino J. A 6-week, double-blind, placebo- and haloperidol-controlled, phase II study of lurasidone in patients with acute schizophrenia. Ther Adv Psychopharmacol. (2015) 5:322–31. doi: 10.1177/2045125315606027
110. Purdon SE, Malla A, Labelle A, Lit W. Neuropsychological change in patients with schizophrenia after treatment with quetiapine or haloperidol. J Psychiatry Neurosci. (2001) 26:137–49.
111. Riedel M, Spellmann I, Strassnig M, Douhet A, Dehning S, Opgen-Rhein M, et al. Effects of risperidone and quetiapine on cognition in patients with schizophrenia and predominantly negative symptoms. Eur Arch Psychiatry Clin Neurosci. (2007) 257:360–70. doi: 10.1007/s00406-007-0739-x
112. Riedel M, Schmitz M, Østergaard PK, Ferrannini L, Franco MA, Alfano V, et al. Comparison of the effects of quetiapine extended-release and quetiapine immediate-release on cognitive performance, sedation and patient satisfaction in patients with schizophrenia: a randomised, double-blind, crossover study (eXtRa). Schizophr Res. (2015) 162:162–8. doi: 10.1016/j.schres.2014.12.027
113. Savitz AJ, Xu H, Gopal S, Nuamah I, Ravenstijn P, Janik A, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. (2016) 19:pyw018. doi: 10.1093/ijnp/pyw018
114. Sacchetti E, Galluzzo A, Valsecchi P, Romeo F, Gorini B, Warrington L. Ziprasidone vs clozapine in schizophrenia patients refractory to multiple antipsychotic treatments: the MOZART study. Schizophr Res. (2009) 113:112–21. doi: 10.1016/j.schres.2009.05.002
115. Shen JH, Zhao Y, Rosenzweig-Lipson S, Popp D, Williams JB, Giller E, et al. A 6-week randomized, double-blind, placebo-controlled, comparator referenced trial of vabicaserin in acute schizophrenia. J Psychiatr Res. (2014) 53:14–22. doi: 10.1016/j.jpsychires.2014.02.012
116. Sirota P, Pannet I, Koren A, Tchernichovsky E. Quetiapine versus olanzapine for the treatment of negative symptoms in patients with schizophrenia. Hum Psychopharmacol. (2006) 21:227–34. doi: 10.1002/hup.763
117. Small JG, Hirsch SR, Arvanitis LA, Miller BG, Link CG. Quetiapine in patients with schizophrenia. A high- and low-dose double-blind comparison with placebo Seroquel Study Group. Arch Gen Psychiatry. (1997) 54:549–57. doi: 10.1001/archpsyc.1997.01830180067009
118. Smith MA, McCoy R, Hamer-Maansson J, Brecher M. Rapid dose escalation with quetiapine: a pilot study. J Clin Psychopharmacol. (2005) 25:331–5. doi: 10.1097/01.jcp.0000168486.14516.7c
119. Stroup TS, Lieberman JA, McEvoy JP, Swartz MS, Davis SM, Rosenheck RA, et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry. (2006) 163:611–22. doi: 10.1176/ajp.2006.163.4.611
120. Stroup TS, Lieberman JA, McEvoy JP, Swartz MS, Davis SM, Capuano GA, et al.. Effectiveness of olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia after discontinuing perphenazine: a CATIE study. Am J Psychiatry. (2007) 164:415–27. doi: 10.1176/ajp.2007.164.3.415
121. Takekita Y, Kato M, Wakeno M, Sakai S, Suwa A, Nishida K, et al. A 12-week randomized, open-label study of perospirone versus aripiprazole in the treatment of Japanese schizophrenia patients. Progr Neuropsychopharmacol Biol Psychiatry. (2013) 40:110–4. doi: 10.1016/j.pnpbp.2012.09.010
122. Takeuchi H, Fervaha G, Lee J, Agid O, Remington G. Effectiveness of different dosing regimens of risperidone and olanzapine in schizophrenia. Eur Neuropsychopharmacol. (2015) 25:295–302. doi: 10.1016/j.euroneuro.2014.12.008
123. Tandon R, Cucchiaro JB, Phillips D, Hernandez D, Mao Y, Pikalov AA, et al. A double-blind, placebo-controlled, randomized withdrawal study of lurasidone for the maintenance of efficacy in patients with schizophrenia. J Psychopharmacol. (2016) 30:69–77. doi: 10.1177/0269881115620460
124. Tzimos A, Samokhvalov V, Kramer M, Ford L, Gassmann-Mayer C, Lim P, et al. Safety and tolerability of oral paliperidone extended-release tablets in elderly patients with schizophrenia: a double-blind, placebo-controlled study with six-month open-label extension. Am J Geriatr Psychiatry. (2008) 16:31–43. doi: 10.1097/JGP.0b013e31815a3e7a
125. Weiden PJ, Manning R, Wolfgang CD, Ryan JM, Mancione L, Han G, et al. A randomized trial of iloperidone for prevention of relapse in schizophrenia: the REPRIEVE study. CNS Drugs. (2016) 30:735–47. doi: 10.1007/s40263-016-0345-4
126. Zhong KX, Sweitzer DE, Hamer RM, Lieberman JA. Comparison of quetiapine and risperidone in the treatment of schizophrenia: a randomized, double-blind, flexible-dose, 8-week study. J f Clin Psychiatry. (2006) 67:1093–103. doi: 10.4088/JCP.v67n0712
127. Waite F, Sheaves B, Ishama L, Reeve S, Freeman D. Sleep and schizophrenia: from epiphenomenon to treatable causal target. Schizoph Res. (2020) 221:44–56. doi: 10.1016/j.schres.2019.11.014
128. Thompson W, Quay TAW, Rojas-Fernandez C, Farrell B, Bjerre LM. Atypical antipsychotics for insomnia: a systematic review. Sleep Med. (2016) 22:13–7. doi: 10.1016/j.sleep.2016.04.003
129. Eugene AR, Eugene B, Masiak M, Masiak JS. Head-to-head comparison of sedation and somnolence among 37 antipsychotics in schizophrenia, bipolar disorder, major depression, autism spectrum disorders, delirium, and repurposed in COVID-19, infectious diseases, and oncology from the FAERS 2004-2020. Front Pharmacol. (2021) 12:621691. doi: 10.3389/fphar.2021.621691
130. Kishi T, Ikuta T, Matsunaga S, Matsuda Y, Oya K, Iwata N. Comparative efficacy and safety of antipsychotics in the treatment of schizophrenia: a network meta-analysis in a Japanese population. Neuropsychiatr Dis Treat. (2017) 13:1281–302. doi: 10.2147/NDT.S134340
131. Kluge M, Schacht A, Himmerich H, Rummel-Kluge C, Wehmeier PM, Dalal M, et al. Olanzapine and clozapine differently affect sleep in patients with schizophrenia: results from a double-blind, polysomnographic study and review of the literature. Schizophr Res. (2014) 152:255–60. doi: 10.1016/j.schres.2013.11.009
132. Weiden PJ, Daniel DG, Simpson G, Romano SJ. Improvement in indices of health status in outpatients with schizophrenia switched to ziprasidone. J Clin Psychopharmacol. (2003) 23:595–600. doi: 10.1097/01.jcp.0000095347.32154.08
133. Kassew T, Demilew D, Birhanu A, Wonde M, Liyew B, Shumet S. Attitude towards antipsychotic medications in patients diagnosed with schizophrenia: a cross-sectional study at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia. Schizophr Res Treat. (2019) 2019:5094017. doi: 10.1155/2019/5094017
134. Fang F, Sun H, Wang Z, Ren M, Calabrese JR, Gao K. Antipsychotic drug-induced somnolence: incidence, mechanisms, and management. CNS Drugs. (2016) 30:845–67. doi: 10.1007/s40263-016-0352-5
135. Orsolini L, Tomasetti C, Valchera A, Vecchiotti R, Matarazzo I, Vellante F, et al. An update of safety of clinically used atypical antipsychotics. Expert Opin Drug Saf. (2016) 15:1329–47. doi: 10.1080/14740338.2016.1201475
136. Read J, Williams J. Positive and negative effects of antipsychotic medication: an international online survey of 832 recipients. Curr Drug Saf. (2019) 14:173–81. doi: 10.2174/1574886314666190301152734
137. Miller DD. Atypical antipsychotics: sleep, sedation, and efficacy. J Clin Psychiatry. (2004) 6:3–7.
138. Chohan PS, Mittal R, Javed A. Antipsychotic medication and QT prolongation. Pak J Med Sci Q. (2015) 31:1269–71. doi: 10.12669/pjms.315.8998
139. Tsuang MT, Stone WS, Faraone SV. Toward reformulating the diagnosis of schizophrenia. Am J Psychiatry. (2000) 157:1041–50. doi: 10.1176/appi.ajp.157.7.1041
PROSPERO, International prospective register of systematic reviews; REM, Rapid eyes movement; AP, Antipsychotics; DRA, Dopamine receptor antagonists; FGAs, First Generation Antipsychotics; SGAs, Second Generation Antipsychotics; ADRs, Adverse Drug reactions; LAI, Long-action injectable; CONSORT, Consolidated Standards of Reporting Trials; NMA, Network meta-analysis; RCT, Randomized Clinical Trials; CrI, Credible Interval; CONACyT, Consejo Nacional de Ciencia y Tecnología; NNH, Number Needed to Harm; SUCRA, Surface under the cumulative ranking curve; MeSH, Medical subject headings terms; DeCS, Descriptores en Ciencias de la Salud; Pr, Probability; IR, Immediate release; XR, extended release; ER, extended release; BID, Twice a day; LD, Low dose; MD, Median dose; HD, High dose; mg/d, Milligrams per day; mg Eq, Milligram per equivalent; AMI, Amisulpride; ASE, Asenapine; ARI, Aripiprazole; ARI LAI, Aripiprazole Long-acting injection; BLO, Blonanserin; BRE, Brexpiprazole; CAR, Cariprazine; CLO, Clozapine; CPZ, Chlorpromazine; FLU, Fluphenazine; FPX, Flupentixol; HAL, Haloperidol; ILO, Iloperidone; LUR, Lurasidone; OLA, Olanzapine; OLA LAI, Olanzapine Long-acting injection; PAL, Paliperidone; PAL LAI, Paliperidone Long-acting injectable; PBO, Placebo; PER, Perospirone; PERPH, Perphenazine; QUE, Quetiapine; RIS, Risperidone; RIS LAI, Risperidone Long-acting injection; SER, Sertindole; ZIP, Ziprasidone; ZOT, Zotepine.
Keywords: antipsychotics, schizophrenia, insomnia, somnolence, sedation
Citation: Valencia Carlo YE, Saracco-Alvarez RA, Valencia Carlo VA, Vázquez Vega D, Natera Rey G and Escamilla Orozco RI (2023) Adverse effects of antipsychotics on sleep in patients with schizophrenia. Systematic review and meta-analysis. Front. Psychiatry 14:1189768. doi: 10.3389/fpsyt.2023.1189768
Received: 20 March 2023; Accepted: 31 May 2023;
Published: 27 June 2023.
Edited by:
Mirko Manchia, University of Cagliari, ItalyReviewed by:
Vassilis Martiadis, Asl Napoli 1 Centro, ItalyCopyright © 2023 Valencia Carlo, Saracco-Alvarez, Valencia Carlo, Vázquez Vega, Natera Rey and Escamilla Orozco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardo Arturo Saracco-Alvarez, ZHJfc2FyYWNjb0B5YWhvby5jb20ubXg=; c2FyYWNjb0BpbXAuZWR1Lm14
†ORCID: Yarmila Elena Valencia Carlo orcid.org/0000-0001-8640-7212
Ricardo Arturo Saracco-Alvarez orcid.org/0000-0002-0004-1318
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.