
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 19 May 2023
Sec. Sleep Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1174719
This article is part of the Research TopicReviews in: Sleep DisordersView all 13 articles
 Kunihiro Futenma1,2
Kunihiro Futenma1,2 Yoshikazu Takaesu1,2
Yoshikazu Takaesu1,2 Yoko Komada3
Yoko Komada3 Akiyoshi Shimura2,4
Akiyoshi Shimura2,4 Isa Okajima5
Isa Okajima5 Kentaro Matsui2,6,7
Kentaro Matsui2,6,7 Kosuke Tanioka2,8
Kosuke Tanioka2,8 Yuichi Inoue2,8*
Yuichi Inoue2,8*Delayed sleep–wake phase disorder (DSWPD) is a sleep disorder in which the habitual sleep–wake timing is delayed, resulting in difficulty in falling asleep and waking up at the desired time. Patients with DSWPD frequently experience fatigue, impaired concentration, sleep deprivation during weekdays, and problems of absenteeism, which may be further complicated by depressive symptoms. DSWPD is typically prevalent during adolescence and young adulthood. Although there are no studies comparing internationally, the prevalence of DSWPD is estimated to be approximately 3% with little racial differences between Caucasians and Asians. The presence of this disorder is associated with various physiological, genetic and psychological as well as behavioral factors. Furthermore, social factors are also involved in the mechanism of DSWPD. Recently, delayed sleep phase and prolonged sleep duration in the young generation have been reported during the period of COVID-19 pandemic-related behavioral restrictions. This phenomenon raises a concern about the risk of a mismatch between their sleep–wake phase and social life that may lead to the development of DSWPD after the removal of these restrictions. Although the typical feature of DSWPD is a delay in circadian rhythms, individuals with DSWPD without having misalignment of objectively measured circadian rhythm markers account for approximately 40% of the cases, wherein the psychological and behavioral characteristics of young people, such as truancy and academic or social troubles, are largely involved in the mechanism of this disorder. Recent studies have shown that DSWPD is frequently comorbid with psychiatric disorders, particularly mood and neurodevelopmental disorders, both of which have a bidirectional association with the pathophysiology of DSWPD. Additionally, patients with DSWPD have a strong tendency toward neuroticism and anxiety, which may result in the aggravation of insomnia symptoms. Therefore, future studies should address the effectiveness of cognitive-behavioral approaches in addition to chronobiological approaches in the treatment of DSWPD.
Circadian rhythm, which runs for approximately 24 h, is present in all animate beings and acts as a regulatory mechanism that promotes optimal adaptation to various biological activities, including not only sleep and wakefulness but also various biological activities such as feeding, reproduction, and social activities (1). Normally, when circadian rhythms are synchronized with the light–dark cycle of the external world, melatonin is secreted as light exposure diminishes during the night and sleep is initiated during the downward phase of the core body temperature (CBT). Among the circadian rhythm markers, dim light melatonin onset (DLMO) and CBT rhythms show a phase relationship with the 24-h cycle. The relationship between the circadian rhythm markers (i.e., DLMO or CBT rhythm) and sleep timing (i.e., sleep onset or offset) is called the “phase angle” of circadian entrainment. Both Earth’s rotation and social activity rhythms run on the 24-h cycle, but the endogenous circadian rhythm in humans may be typically a little longer than 24 h. The length of the intrinsic circadian period is called “tau.” Although the length of tau varies from individual to individual, the mean period of tau is reported to be 24.15 h (standard deviation 0.2 h) (2–4), with the length of tau of women being approximately 6 min shorter than that of men (5). Endogenous circadian rhythms are entrained to follow a 24-h cycle of the external world by various zeitgebers, which are the external factors that serve as cues for entrainment. Among these, light stimulation at a certain time of the day alters the firing rate of neurons in the brain’s suprachiasmatic nucleus (SCN; the command center of the circadian clock), activates the molecular signaling pathway, and alters the transcription of clock genes that determine the phase of the circadian cycle by regulating the rhythm of endogenous melatonin secretion (6). The effect of circadian phase resetting through melatonin and photic stimulation in the SCN follows the phase-response curve (PRC). In the PRC, if light is applied before the minimal point of CBT (CBTmin) appears, the melatonin secretion phase is likely to be delayed, whereas if light is applied after CBTmin, the phase is likely to advance (7). In a normal lifestyle, evening light delays the circadian clock by delaying the sleep onset timing, whereas morning light advances the circadian clock. Light exposure is the most important entrainment factor, but other zeitgebers, such as exercise, mealtime, and social activities also contribute to circadian rhythm entrainment. However, the entrainment ability of these factors is weaker than that of light (8, 9).
Many adolescents and young adults worldwide exhibit a delayed sleep pattern, which can be considered a disorder when it significantly affects important areas of an individual’s functioning. Delayed Sleep–Wake Phase Disorder (DSWPD) (10) is a circadian rhythm disorder in which the delay of sleep phase causes difficulty in falling asleep and waking up at a desired time, resulting in daytime dysfunction. This disorder is associated with multiple factors including specific biological traits, socio-psychological backgrounds, sleep hygiene problems, and comorbid psychiatric diseases. DSWPD is prevalent during adolescence and young adulthood. The establishment of treatment strategies against this disorder is therefore important because the incidence of DSWPD during these critical developmental stages can damage an individual’s future prospects. However, the pathological mechanism of DSWPD as well as many aspects such as the adequate classification, assessment, and treatment strategy of subgroups based on patients’ backgrounds, psychosocial characteristics, and physiological findings remain unclear. Furthermore, recent changes in the light environment surrounding adolescents have increased the likelihood of eveningness chronotype possibly leading to the development of DSWPD (11). A significant number of young people do not meet the diagnostic criteria of DSWPD but have delayed sleep phases (DSP) (12). Social jetlag (SJL) is a new concept that refers to the difference in sleep timing between weekdays and rest days has also been proposed as a concern regarding circadian rhythm related sleep hygiene in young people (13).
The development of DSWPD reflects the multifaceted interaction between social schedules, timing of exposure to light and dark, genetic factors, homeostatic pressure on sleep, and the circadian system. The extent to which a combination of any of these factors is impaired is difficult to identify in a clinical setting. Moreover, approximately 40% (14) of patients with DSWPD have normal timing of melatonin secretion profile (the most important marker of circadian rhythm) even though their sleep–wake schedule is clearly delayed. This subgroup of DSWPD without circadian misalignment is termed circadian-entrained DSWPD and occurs based on the psychological and behavioral backgrounds in addition to biological factors in the young generation (15). Recent studies have also shown that DSWPD is frequently comorbid with some psychiatric disorders, particularly neurodevelopmental and mood disorders, both of which have a bidirectional association with the pathophysiology of DSWPD. In 2015, the American Academy of Sleep Medicine (AASM) published revised guidelines for the treatment of circadian rhythm sleep–wake disorders (CRSWDs), including DSWPD. However, additional treatment methods for circadian-entrained DSWPD and DSWPD complicated by psychiatric disorders should be established.
In this review, we describe the physiological and psycho-behavioral backgrounds of circadian-entrained and non-entrained DSWPD in young people, as well as the relationship between psychiatric disorders and DSWPD. Furthermore, we discuss the current problems and future development of the treatment of this disorder based on the results of psychological and psychiatric assessments.
In 1981, Weitzman et al. (16) first proposed the concept of delayed sleep phase syndrome (DSPS) as a chronobiological disorder in a group of patients with chronic difficulty falling asleep and waking, distinguishing it from insomnia and hypersomnia. The concept of DSPS, along with sleep disorders in shift workers, jet lag, and other chronobiological disorders, was included in the first edition of the International Classification of Sleep Disorders (ICSD) (17) as a group of circadian rhythm sleep disorders (CRSD). In the second edition (ICSD-2) (18), DSPS was conceptualized from a syndrome to a single disorder and was referred to as CRSD, delayed sleep phase type (DSPT), or delayed sleep phase disorder (DSPD). However, it is now referred to as DSWPD in ICSD-3 (10). In ICSD-3, the category of CRSD was also renamed circadian rhythm sleep–wake disorder (CRSWD). The ICSD-3 criteria of CRSWD consist of the following three items. First, chronic or recurrent pattern of sleep–wake rhythm disruption primarily because of alteration in the endogenous circadian timing system or misalignment between the endogenous circadian rhythm and the sleep–wake schedule that is desired or required by an individual’s physical environment or social/work schedules. Second, circadian rhythm disruption that leads to insomnia symptoms, excessive sleepiness, or both. Third, sleep and wake disturbances that cause clinically significant distress or impairment in mental, physical, social, occupational, educational, or other important areas of functioning.
The ICSD-3 (10) classifies CRSWD into the following seven categories: (a) DSWPD, (b) advanced sleep–wake phase disorder (ASWPD), (c) irregular sleep–wake rhythm disorder (ISWRD), (d) non-24-h sleep–wake rhythm disorder (N24SWD), (e) shift work disorder (SWD), (f) jet lag disorder (JLD), and (g) circadian sleep–wake disorder not otherwise specified (NOS). DSWPD is the most common sleep–wake disorder, accounting for 83% of CRSWDs in clinical settings (19). In addition to the above three common criteria items for CRSWD, the diagnostic criteria for DSWPD in ICSD-3 requires the fulfillment of the following five criteria. First, a significant delay in the phase of the major sleep episode in relation to the desired or required sleep time and wake-up time, as evidenced by a chronic or recurrent complaint by the patient or caregiver of the inability to fall asleep and difficulty awakening at a desired or required clock time. Second, symptoms are present for at least 3 months. Third, patients exhibit improved sleep quality and duration for their age and maintain a delayed phase of the 24-h sleep–wake pattern when they are allowed to choose their ad libitum schedule. Fourth, sleep log and, whenever possible, actigraphy monitoring for at least 7 days (preferably 14 days) demonstrates a delay in the timing of the habitual sleep period. Fifth, sleep disturbance is neither satisfactorily explained by another current sleep disorder nor by any medical, neurological, or mental disorder; medication use; or substance use disorder.
The sleep duration of patients with DSWPD is mostly well maintained during their free days, although the sleep phases are apparently delayed. However, on weekdays, they experience difficulty falling asleep and waking up at socially desirable times, such as school or work timings, which interferes with their daily lives. Patients with DSWPD frequently experience daytime sleepiness, fatigue, headache, anorexia, and depression. DSWPD with a regressed rhythm of melatonin secretion, as well as other hormones such as cortisol, may also present with decreased blood pressure during the daytime. This is particularly observed in the morning hours and is often manifested as orthostatic dysregulation (20). Patients with DSWPD with severely delayed circadian rhythms may also exhibit serious sleep inertia when attempting to wake them up at socially desirable times.
Many studies have reported a certain relationship between DSWPD and psychological problems or decreased social functioning, although some negative observations have also been reported (21). Cross-sectional studies have shown higher depression and anxiety scores in patients with DSWPD (14, 22–25), as well as lower health-related quality of life (25) and more frequent self-harm and suicidal ideation (26). Individuals with DSWPD may be unable to adjust to school life or employment (12, 27) when their symptoms are severe. In contrast, the removal of the constraints of attendance at school or work, the most important social zeitgebers, may worsen the symptom severity of the disorder (28). DSWPD has been suggested to be associated with lower grades in students (23, 29) and frequent absenteeism, as well as lower productivity and presenteeism in the working generation (25, 30). Socially, patients with DSWPD tend not to enjoy leisure time and are unable to fulfill their household responsibilities (30). Substance use issues, such as smoking, alcohol, caffeine, and cannabis, may also arise (12, 21, 23, 31). The above associations observed in patients with DSWPD are sometimes observed in individuals with the evening chronotype (32), which suggests that DSWPD is possibly an extreme phenotype of the eveningness chronotype.
The diagnosis of DSWPD requires a thorough investigation of the medical, mental, or sleep disorders that may cause sleep–wake cycle alterations, insomnia, or excessive daytime sleepiness. Social maladjustment, family dysfunction, school avoidance, and comorbid mood disorders should also be investigated in adolescents and young adults.
A sleep diary (sleep log) monitored for at least 7 days (ideally longer) is mandatory as an indicator for the diagnosis of DSWPD in ICSD-3. Actigraphy, which uses a non-invasive wrist-worn accelerometer, can capture rest-activity rhythms from which the timing and regularity of sleep can be estimated. In the ICSD-3 diagnostic criteria, an actigraphic recording is not necessary for diagnosis (listed as “whenever possible”). However, because sleep diaries may cause misunderstanding and recall bias, supportive actigraphic recording is desirable for objectively measuring an individual’s sleep–wake schedule. In ICSD-3, actigraphic recording is set as a mandatory item only for the diagnosis of N24SWD. Nevertheless, we believe that actigraphic recordings along with a sleep diary for a minimum evaluation period of 14 days are necessary for the accurate diagnosis of DSWPD. Although the information provided by actigraphy is inherently limited with respect to the assessment of the underlying chronobiological complexity associated with CRSWDs (11), previous studies (as shown below) showed that actigraphy can reflect the status of the melatonin secretion profile of patients with DSWPD (33). Alternatively, low burden and relatively inexpensive consumer-grade wearable and mobile technologies are now attracting interest as devices for measuring the conventional biomarkers of sleep (34). However, further studies are necessary to validate whether these devices can serve as a useful assessment tool for an individual’s sleep–wake schedule.
The CBT and melatonin secretory rhythms, which are generated by the SCN in parallel with the circadian sleep propensity rhythm, are well-established indicators of circadian rhythms and often used in clinical studies of DSWPD (35, 36). However, they are difficult to measure in general clinical practice. Previously, CBT assessment was a highly invasive approach that used a rectal probe. In recent years, a simple non-invasive tool that can be attached to the surface of the chest or other body parts has been developed to assess CBT (37, 38). Melatonin secretion can be measured through serial salivary assays, serum assays, or the measurement of urinary 6-sulphatoxymelatonin. Among these, DLMO, which is measured in light less than 10 lx, enables the estimation of the circadian phase of melatonin secretion (35, 39). However, since CBT and melatonin secretion can be obscured by masking effects (e.g., light suppresses melatonin secretion and activity and sleep modifies the CBT rhythm), these measurements are highly recommended to be performed in highly controlled conditions to minimize contamination by the masking effects.
Self-administered chronotype questionnaires have also been commonly used to assess patients highly suspected of having DSWPD. Among these, the morningness-eveningness questionnaire (MEQ) (40) and Munich chronotype questionnaire (MCTQ) (41) have been accepted as reliable chronotype measures. The MEQ can evaluate an individual’s circadian preference, whereas the MCTQ is advantageous in that it can evaluate an individuals’ sleep-midpoint and SJL, both of which are important indicators of circadian rhythm (42). As described later, DSWPD is commonly observed inpsychiatric disorders, particularly bipolar disorder, suggesting the close relation of pathophysiology between bipolar disorder and CRSWDs (43, 44). The Biological Rhythms Interview of Assessment in Neuropsychiatry (BRIAN) was first developed to measure circadian rhythm dysfunction in patients with bipolar disorder (45). However, our recent studies have shown that BRIAN can be effectively used also for the screening and severity assessment of DSWPD without comorbid psychiatric disorders (25, 46).
Although nocturnal polysomnography is not necessary to establish the diagnosis of DSWPD, it should be performed when the existence of other sleep disorders that may be responsible for subjective insomnia and sleep inertia in the morning is suspected. When performed during conventional sleep laboratory hours, the polysomnographic findings of individuals with DSWPD tend to show prolonged latency for sleep onset and normal or relatively long total sleep time, which are consistent with their sleep logs or actigraphic findings (47, 48).
DSWPD has a prevalence of 0.17–1.51% in the general population (49, 50), which is reported lower than that of DSP (12). In comparison, a survey of 10,220 adolescents aged 16–18 years in Norway found a relatively higher rate of 3.3% (27), while a more recent Norwegian survey of 50,054 students aged 18–35 years also showed a prevalence of 3.3% (26). These results suggest that DSWPD is possibly more prevalent in the younger generation than in the older generations. Similarly, a recent large Japanese survey estimated that 4.3% of the youth (15–30 years) is at risk for DSWPD (25). The higher prevalence of DSWPD in adolescents and young adults may reflect a preference for a “night owl” lifestyle and biological change in this generation (3, 51).
As aforementioned, studies on the sex differences in the prevalence of DSWPD have been inconclusive. The results of previous epidemiological studies demonstrated a higher prevalence in males (12, 26), females (25, 27), or no sex differences (49, 50, 52). Although the effect of a delayed sleep–wake schedule on the development of depression may be greater in women because of their intrinsically earlier circadian rhythm (53), sex differences in the effect of the disorder on daytime functioning has not been clarified.
No international comparative studies on racial or regional differences in the prevalence of DSWPD have been conducted to date. However, in Germany, people living in the western region of the country have later chronotypes than those living in the eastern region (42). The relatively later sunrise in the western part of the country (although both regions share the same time zone) was speculated to contribute to this difference (54). Table 1 shows a list of the major epidemiological studies on DSWPD over the last decade.
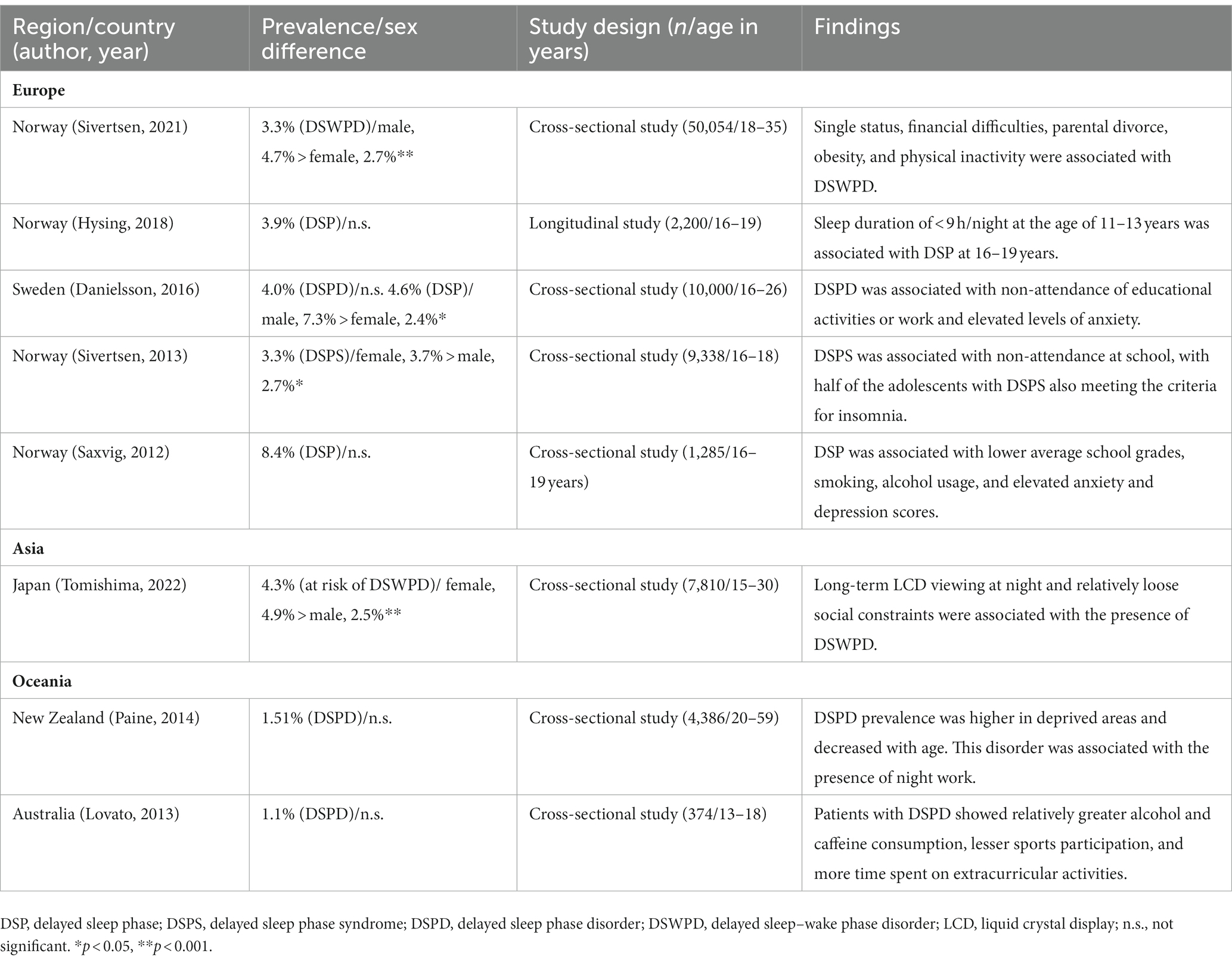
Table 1. Prevalence of DSWPD-related disorders by region/country as reported over the past decade.
Although the pathogenesis of DSWPD is heterogeneous and complicated by various factors, one of the most important features of typical DSWPD is the delayed circadian rhythm, which is assessed using DLMO or CBT measurements. Many studies have shown a circadian rhythm delay in DLMO in patients with DSWPD (55, 56).
As mentioned in the introduction, light stimulation is the most important zeitgeber; however, individual sensitivity to light varies 50-fold on a logarithmic scale (57). Studies have also shown that light exposure at the same timing and intensity may have different effects on the entrainment phase between individuals (58, 59). In DSWPD, photosensitivity seems to be weak (or the time width of the phase advance is narrow) during the phase advance portion of the circadian PRC to light stimuli (60). Additionally, photosensitivity at night is higher in patients with DSWPD than in normal sleepers, which may contribute to the delay in circadian rhythm (61).
Individual differences in the intrinsic circadian cycle are another cause of DSWPD. The length of tau varies among individuals, and individuals with longer tau are entrained at a later phase than those with shorter tau (62, 63). Furthermore, the circadian cycle of both melatonin secretion and CBT rhythms is longer in patients with DSWPD than in controls, with tau length being associated with the likelihood of developing DSWPD (63, 64). The PERIOD2 (PER2) gene encodes a core molecule in the circadian clock and plays an important role in the generation and maintenance of diurnal rhythms. Minor allele carriers of the PER2 variant have significantly longer circadian cycles than non-carriers, as demonstrated by CBT or plasma melatonin profile (65).
Problems with sleep inertia and sleep architecture may also be related to the pathophysiology of DSWPD. Previously, sleep architecture and sleep duration in patients with DSWPD were considered normal (66). However, several studies have reported prolonged sleep duration in patients with DSWPD (36, 67–69). Moreover, patients with DSWPD have a low amount of slow-wave sleep during the first half of sleep, corresponding to a delay in the timing of CBTmin (69). Patients with DSWPD also have a higher arousal threshold during REM sleep (47) and a prolonged interval between CBTmin and arousal (36, 67, 70). These factors may be related to the difficulty in waking up at a desirable time in the morning, possibly resulting in the decreased light exposure during the phase-advance portion of the PRC.
Chronotype change with age may also be involved in the development of DSWPD. In this regard, some researchers have suggested the role of age and sex differences in the development of DSWPD based on sex hormone changes (71, 72). Gonadal steroid receptors are expressed at most sites that receive direct inputs from the SCN. At each stage of the circadian system, brain nuclei bear estrogen receptors, androgen receptors, or both. From adolescence to young adulthood, the activational effects of sex hormones on the circadian timing system are associated with the phase delay of the circadian rhythm (71). Although the prevalence of DSWPD declines after middle age, a large survey of chronotypes in Brazil (n = 14,650) (73) showed that women were on an average more morning-oriented than men up to the age of 30 years. However, from age 30 to 45 years, the sex difference in the chronotype disappeared, and women tended to be more evening-oriented than men aged 45 years and older. The age-related plastic changes associated with sex differences in chronotypes remain largely unknown, however, changes in the sex hormone status may be partially related to the differences in the circadian phases among the respective generations.
Patients with DSWPD have been demonstrated to have a larger phase angle between sleep timing and circadian rhythm markers (67, 69, 74). Polymorphisms or mutations in clock genes may contribute to this expansion of the phase angle (75). Furthermore, DSWPD is frequently associated with difficulty in initiating sleep (27), which may be related to the expansion of the phase angle in DSWPD. Additionally, a sleep homeostatic problem leading to difficulty in increasing sleep pressure has been reported (74).
DSWPD and N24SWD often occur alternately in the same patient, suggesting pathological continuity between the two disorders. A large proportion of individuals with DSWPD as well as those with N24SWD exhibit longer periods of melatonin and temperature rhythms, with longer circadian tau appearing to be the common basis for these disorders (63). N24SWD can occur even in patients without visual impairment and could be an extreme form of DSWPD. On the other hand, DSWPD has also been suggested as the prodromal manifestation of N24SWD without visual impairment (76). In addition to longer intrinsic tau, other potential etiologies shared by DSWPD and N24SWD include altered light sensitivity (77) and homeostatic issues (difficulty in increasing sleep pressure) (63).
DSWPD appears to be strongly related to youth-specific behavioral factors. Our previous epidemiological study showed that behavioral patterns particular to youth, such as long-term liquid crystal display (LCD) viewing at night, were associated with the presence of DSWPD (25). Considering this, prolonged exposure to LCD screen-based devices, such as TVs, PCs, and smartphones, from evening to bedtime may be associated with the development or worsening of DSWPD. Similarly, the duration of monitor viewing time was also demonstrated to be adversely associated with sleep health, primarily via delayed bedtime and reduced sleep duration among school-aged youth (78). The scarcity of physical exercise habits (21, 25, 26) and the presence of night work (50) and extracurricular activities (21) were also associated with the risk of developing DSWPD. Another longitudinal study (52) showed that sleeping less than 9 h/night at the age of 11–13 years was associated with DSP at 16–19 years. In addition, one study reported smoking and drinking habits as factors associated with the presence of DSWPD (23).
DSWPD is a disorder that can develop on a psychosocial basis. In support of this, our recent study showed that being at risk for DSWPD had a greater association in students than in young adult workers of the same age group (25), suggesting that less social constraints could be associated with the presence of DSWPD in this generation. Several studies have also shown that absenteeism at school or work was associated with DSWPD (12, 27). Thus, the teenagers’ sleep–wake rhythm may be delayed because of their non-attendance at school, which was related to their maladjustment to school or relationship problems. Furthermore, DSWPD in students has been suggested to be associated with financial deprivation, parental divorce (26), and depression (31). However, many of these reports were cross-sectional studies, making the causal relationship unclear. Nevertheless, DSWPD and psychosocial issues may have a bidirectional relationship.
Many researchers have suggested that chronotypes and DSWPD occurrence are associated with specific personality traits. To date, the “Big Five” model, which proposes that personality can be grouped across five broad personality traits that include neuroticism (i.e., emotional instability and moodiness), extroversion (i.e., excitability and sociability), conscientiousness (i.e., thoughtfulness and goal-directed behaviors), agreeableness (i.e., altruism and kindness), and openness (i.e., imagination and insight), has been widely used as the personality trait model in studies on sleep hygiene and chronotypes (79). A meta-analysis of the studies published before the end of January 2009 found that conscientiousness was mostly related to morningness. Moreover, agreeableness was also related to morningness, albeit to a lesser degree (80). In contrast, studies conducted on college students after 2010 reported that high extroversion was associated with eveningness and high conscientiousness, openness, and low neuroticism was related to morningness tendency (81, 82). However, these were cross-sectional studies, and a longitudinal study showed that only low neuroticism predicted morningness 1 year later (83). Another study found that patients with DSWPD had higher neuroticism, lower extroversion, and lower conscientiousness than a healthy control group (84, 85). Taking these findings into consideration, levels of conscientiousness and neuroticism could be associated with the variation in the morningness-eveningness chronotype. Apart from these two personality traits, low extroversion could contribute to DSWPD development. Although few studies have directly examined the relationship between personality traits and sleep-related behavior, low conscientiousness and high neuroticism may become strong predictors of poor sleep hygiene (81) Taking these findings together, certain personality traits may contribute to the development and maintenance of sleep problems including DSWPD through indirect influences on behavioral aspects.
Individuals with DSWPD commonly report difficulty initiating sleep, and 89% of adolescents with DSWPD experience “racing thoughts” in bed (86). Moreover, it has been suggested that individuals with DSWPD may exhibit cognitive pre-sleep arousal (e.g., worry and rehearsal today and planning tomorrow), dysfunctional beliefs about sleep (e.g., “I know that it will not work and then, I sort of just give up”), and safety behaviors (e.g., use of music, television, and computer games as a sleep aid), similar to patients with chronic insomnia (87). Furthermore, an overlap between DSWPD and insomnia has been reported, wherein more than half of the adolescents with DSWPD also met the criteria for insomnia (27). However, whether these cognitive-behavioral characteristics are specific to patients with DSWPD remains unclear.
DSWPD is frequently observed in neuropsychiatric disorders, such as major depressive (88); bipolar (89); obsessive–compulsive (90); neurodevelopmental disorders, including attention-deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) (91); and schizophrenia (92). Previous studies have suggested that the presence of DSWPD could result in an increased risk of the occurrence of neuropsychiatric disorders, worsened depressive symptoms, increased relapse risk of mood episodes, and deterioration in social and occupational functioning in the affected individuals. Therefore, accurate diagnosis of DSWPD, definitive biomarkers that can identify the association between DSWPD and psychiatric disorders, and the establishment of a treatment strategy for DSWPD in patients with neuropsychiatric diseases are required. Table 2 shows a list of the major studies investigating the relationship between DSWPD and neuropsychiatric disorders.
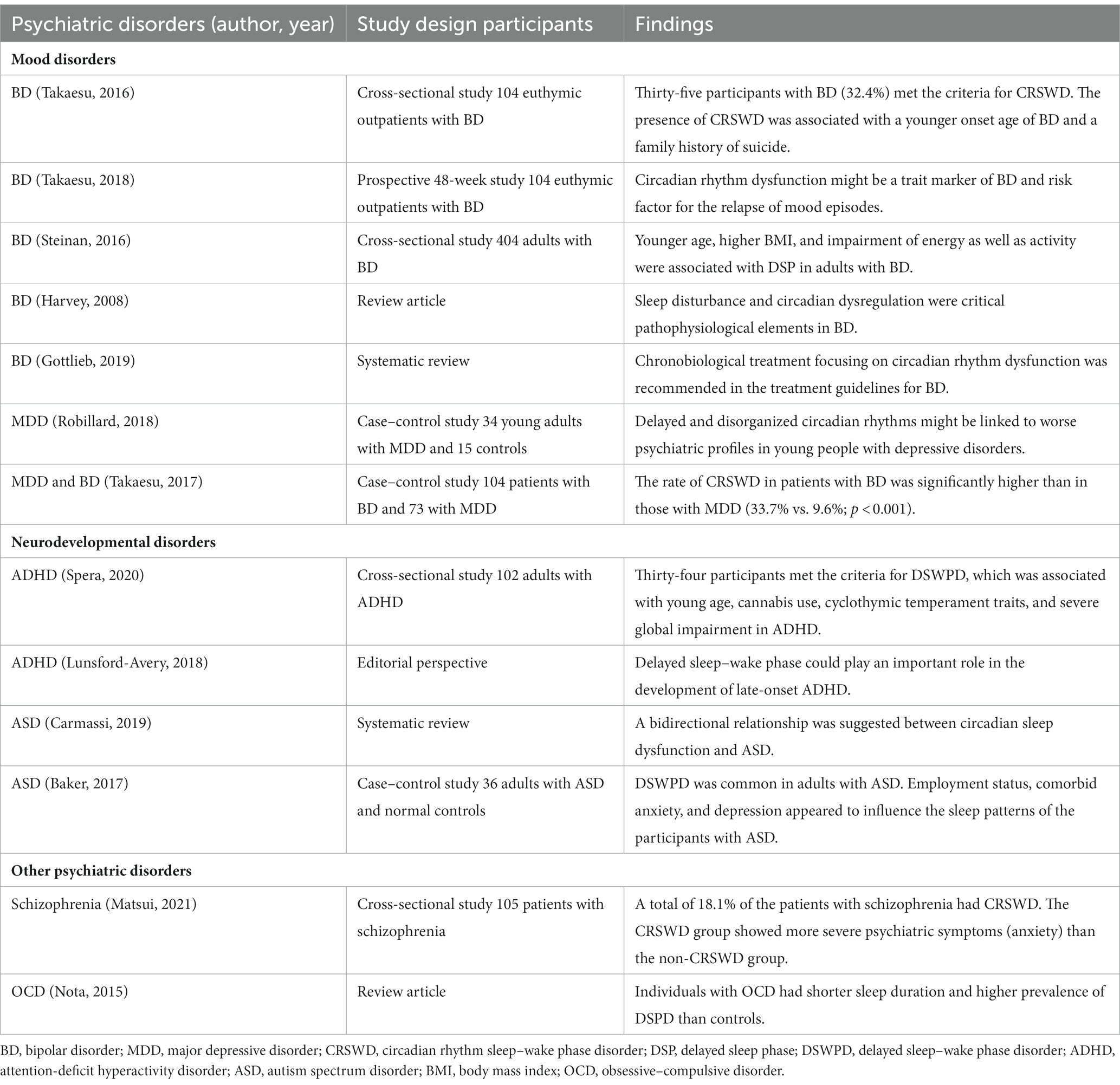
Table 2. Relationship between psychiatric disorders and circadian rhythm dysfunctions, particularly delayed sleep phase.
Many studies have reported a relationship between mood disorders and circadian rhythm dysfunction, including DSWPD. Although the causal relationship between depressive symptoms and delayed sleep–wake phase is unclear, depressive symptoms in individuals with DSWPD have been frequently reported. Abe et al. (22) reported that 46% of patients with DSWPD had moderate-to-severe depressive symptoms, as evaluated using the Zung Self-Rating Depression Scale. In contrast, DSWPD was reported in 9.6% of patients with major depressive disorder (93). Interestingly, another study suggested that DSWPD with delayed DLMO was associated with more severe depressive symptoms than DSWPD without delayed DLMO (14), which implies a pathophysiological relationship between depressive symptoms and circadian rhythm dysfunction.
Circadian rhythm dysfunction may be more prominent in bipolar disorder than in major depressive disorder (93, 94). Many studies have suggested a strong pathophysiological relationship between bipolar disorder and circadian rhythm dysfunction (95, 96), and this dysfunction has been suggested to act both as a trait marker of bipolar disorder and a risk factor for the relapse of mood episodes (43). Based on these results, chronobiological treatment focusing on circadian rhythm dysfunction in bipolar disorder has been recommended in the treatment guidelines for bipolar disorder (97). In particular, bright light therapy has been indicated for depressive symptoms, whereas dark therapy has been suggested for manic symptoms in patients with bipolar disorder (97).
Recent studies have suggested a significant relationship between circadian rhythm dysfunction and neurodevelopmental disorders, such as ADHD (98) and ASD (99). A study on ASD indicated that a higher proportion of adult patients with ASD met the criteria for CRSWD than adult controls. Moreover, DSWPD was found to be particularly common in individuals with ASD (100). Similarly, a cross-sectional study reported that 34 of 102 adult patients with ADHD met the criteria for DSWPD (91). Considering these findings, delayed sleep–wake phase has been hypothesized to play an important role in the development of ADHD symptoms in late adolescence and young adulthood (101), although no clear evidence supporting this hypothesis has been reported. Therefore, longitudinal studies evaluating the causal relationship between neurodevelopmental disorders and DSWPD are required to understand the pathophysiological relationship between these disorders.
DSWPD is diverse in not only its pathogenesis but also in its phenotypes. DSWPD phenotypes differ depending on a combination of various background factors. Delayed circadian rhythm is the most prominent feature of DSWPD; however, a recent study identified a group of patients with DSWPD having normal circadian entrainment (48, 102). As previously mentioned, 43% of DSWPD cases are circadian-entrained DSWPD (14). Circadian-entrained DSWPD often develops primarily based on problems of behavioral factors (103). “Conditioned insomnia” and “aversion to trying to sleep early” are considered as causes of delayed bedtime in circadian-entrained DSWPD (15). Patients with circadian-entrained DSWPD may be associated with negative experiences with going to bed early or have personality traits (e.g., perfectionism) that interfere with bedtime (e.g., staying up late to complete tasks) (104). In contrast, DSWPD with longer tau and an enlarged phase angle shows the most severe delay of sleep–wake phase, and this phenotype is suggested to have pathological continuity with N24SWD (36). The background factors and phenotypes of DSWPD are shown in Figure 1.
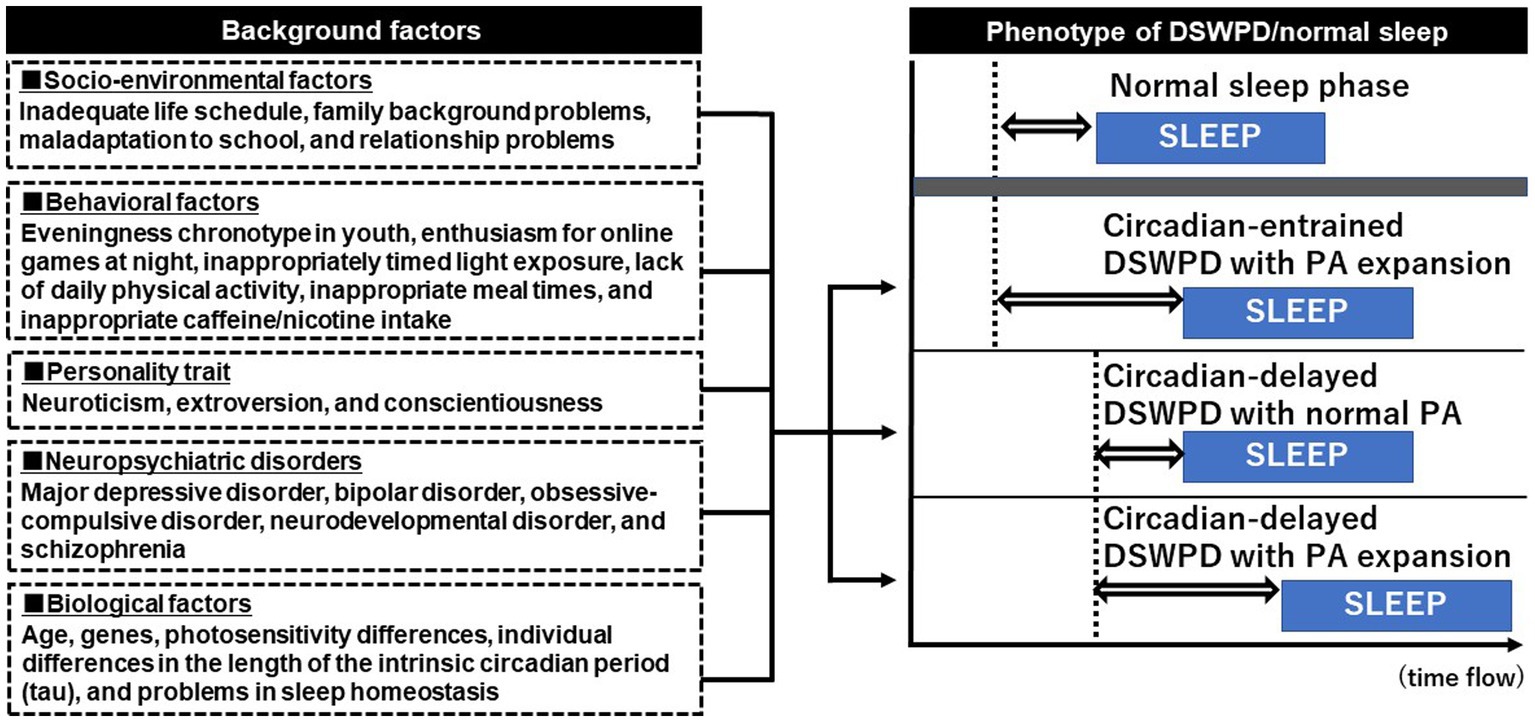
Figure 1. Phenotype of delayed sleep–wake phase disorder and its background factors. The dotted vertical line (---) indicates dim light melatonin onset (DLMO) and the blue box shows the sleep phase. The double-headed arrow (⇔) shows the phase angle (PA) between the DLMO and sleep period onset. The PA between the DLMO and sleep period onset is approximately 2 h in a normal sleeper. Delayed sleep–wake phase disorder (DSWPD) exhibits multiple phenotypes owing to the various combinations of background factors. Approximately 40% of DSWPD cases are reported as circadian-entrained DSWPD, in which the timing of DLMO is normal but the PA is enlarged because of night-oriented behavioral or psychological characteristics. Circadian-delayed DSWPD with PA expansion shows the most severely delayed sleep phase, and this phenotype may have pathological continuity with non-24-h sleep–wake rhythm disorder.
Compared to the natural light/dark cycle during outdoor camping, the nocturnal light exposure of modern lifestyles are associated with sleep phase delay (105). With this regard, a Finnish study found a decline in sleep duration and an increase in eveningness among the adult population even in the first decade (2007–2017) of the 21st century (106). The effect of light exposure on circadian rhythm differs depending on an individual’s age. Because the lenses in adolescents are relatively more transparent than those of older adults (107), melatonin secretion in adolescents is suppressed even with a relatively small amount of nighttime light exposure that would not affect adults (108). Therefore, nighttime light exposure may become an important risk factor for the development of the eveningness chronotype in this generation (109). Recent changes in the light environment surrounding adolescents have increased the risk of them developing the eveningness chronotype (110). In particular, one study found that the long-term use of smartphones in bed could be a significant risk factor for the eveningness chronotype because using it while lying down and observing the screen at very close range exposes one’s eyes to bright light that exceeds 100 lx (111).
A recent cohort study has shown that the number of individuals who meet the diagnostic criteria of DSWPD and the number of people who only have DSP without any sleep complaints for at least 3 months is roughly equal among those who have a sleep–wake schedule delay (12). Undoubtedly, the pathological significance is higher for individuals with DSWPD; however, DSP in the young generation reportedly possesses identifiable psychological risk indicators (52). In the case of DSWPD, no sex difference exists in its prevalence, whereas elevated anxiety levels and the presence of absenteeism (absence from school or work) have been demonstrated (12). In contrast, DSP is more common in men and is associated with a lack of educational activity or work, the presence of shift work, the use of nicotine and alcohol, and less rumination score. Therefore, individuals with DSP could possibly include a substantial number of those in whom the sleep–wake phase is intentionally delayed by personal preference or lifestyle rather than by biological reasons. The ICSD-3 has subtyped DSWPD with poor motivation for treatment as motivated delayed sleep–wake phase disorder (MDSWPD), which is considered more common in adolescents and young adults with comorbid psychiatric disorders, such as developmental and anxiety disorders (10). Considering that MDSWPD is a state of poor internal motivation to regain a normal social life, many MDSWPD cases could be included in the DSP category. As described later, the chronobiological approach is the mainstay treatment for patients with DSWPD; however, behavioral approach would be a better choice for correcting DSP.
In the youth with eveningness chronotype, SJL is commonly observed along with DSP (13). SJL can be easily measured with the result of the aforementioned MCTQ (42). Individuals with larger SJL are more likely to report excessive daytime sleepiness (112, 113) and daytime dysfunction because of the internal desynchronization caused by circadian phase delay (13, 114), including low cognitive function (115), poor academic performance (116), depression (117), and substance use (118). In order to test the hypothesis that SJL can easily develop during adolescence and young adulthood (119), we previously conducted a cross-sectional survey in a large Japanese population. The result showed that the younger the age, the greater the SJL, with 61% of those in their 20s versus 53% of those in their 30s showing a SJL of >1 h (120). SJL is associated with the delay in circadian rhythms (13), and sometimes exacerbates the problem of falling asleep when resuming weekdays during the following week (121). However, whether SJL is a precursor of DSWPD remains unclear. Moreover, SJL is a relatively new concept and literature on its physiological characteristics and natural course is scarce. Therefore, further research from multiple perspectives is required to delineate the relationship between SJL and DSWPD.
From 2020 to 2022, the novel coronavirus disease (COVID-19) has spread globally. During this period, sleep disturbances were observed in up to two-fifths of the general population and up to three-fourths of the patients with COVID-19 globally (122, 123). Older age, presence of a partner, and residence in a high-income country were thought to reduce the risk of sleep disturbances during the pandemic, whereas younger age, female sex, financial problems, and coexisting stress, anxiety, and depression enhanced the risk of sleep disturbances (124). To prevent further spread of the infection, governments of many countries, particularly Western countries, imposed social restrictions on the general population. The resultant changes in lifestyle associated with home confinement, such as the lack of morning sunlight exposure, lack of physical exercise, and excessive use of blue light devices at night, contributed to the changes in sleep behaviors of the general population (125). Of note, the effect of sleep hygiene-related behavior during the pandemic was larger in the young population than in the middle-aged or elderly population (126). Consistent with the studies by Wright et al. (127) and Marelliet et al. (128), we recently reported a significant delay in sleep phase, prolongation of total sleep time, and decrease in SJL from before to during the pandemic in 2222 Japanese participants from a young population cohort of 15–30 years of age (129). However, the worsening of insomnia and depression, as well as deterioration in health-related quality of life that was observed in Western countries was unexpectedly not observed in our study population. This could possibly be because of the smaller infection intensity and milder social restrictions in Japan than in Western countries at the survey point. However, considering that chronic sleep phase delay may result in subjective sleep problems and psychological distress (130) and that Japanese outpatients with DSWPD tended to show symptom aggravation because of a decrease in social zeitgeber during the pandemic (28), prolonged sleep phase delay along with extended social restrictions possibly impairs psychological distress and health-related quality of life. Fortunately, social restrictions owing to the COVID-19 pandemic have already ended in most countries. Nevertheless, we should carefully monitor sleep behaviors and their impact on the daytime function of the youth during the post-social restriction period. This is because the social advancement of the sleep phase and shortened nocturnal sleep time after the resumption of their work or school life may cause a significant psychological dysfunction (131).
Gaming is one of the most popular leisure activities. The COVID-19 pandemic greatly expanded the market of video game industry because people spent more time playing games worldwide (132, 133). Healthy gaming benefits education and training (134), however, some minority gamers experience negative consequences from excessive gaming (135). Gaming disorder (GD) is a relatively new mental disorder that shows the persistence of gaming behavior (online as well as offline) with a loss of control for gaming despite harm to individuals, and conflicts stemming from gaming and functional impairment (136).
In particular, online games allow players to select opponents and cooperating partners from all over the world, making it much easier for players to continue playing and enjoying games than offline games. In 2013, “internet gaming disorder (IGD)” was included in the “diagnostic and statistical manual of mental disorders, fifth edition (DSM-5)” (137) published by the American Psychiatric Association. In 2019, with strong encouragement from Japan, the World Health Organization (WHO) decided to adopt “Gaming Disorder (GD)” in the “international classification of diseases 11th Revision (ICD-11)” (136), and its use started in 2022. Although the content of the criteria differed, the concordance between GD and IGD diagnoses was reported to be fairly high (138).
As expected from elevated enthusiasm and prolonged exposure to blue light emitted from game devices at night, patients with GD have been reported to be frequently complicated with DSWPD (139). Adolescent patients with DSWPD need to be carefully checked to identify if there is a GD in their background. Interestingly, DSWPD and GD may have the following commonalities. First, both GD and DSWPD tend to appear in younger generations, including adolescents (140, 141). Second, not only patients with DSWPD but also those with GD are often complicated by neurodevelopmental disorders. Several studies have indicated that patients with GD are frequently complicated by either ADHD (142) or ASD (143). In such cases, treatment approach focusing on neurodevelopmental disorders should be included.
The 2007 CRSWD treatment guidelines of the AASM recommended light therapy as the first-line treatment for DSWPD (66). As mentioned earlier, exposure to morning light after achieving CBTmin advances the phase of the circadian rhythm. Generally, light therapy for patients with DSWPD is administered for 30 min to 2 h at 2500–10,000 lx during the time for phase advancement (or at 1–3 h before spontaneous awakening) (66). Expectedly, higher light intensity and longer duration of light exposure lead to a greater phase-shifting effect; however, this effect is nonlinear in humans (144, 145). Human circadian rhythms are most sensitive to short-wavelength blue light (~480 nm) (146, 147). Short-wavelength blue light is a more potent melatonin suppressor than long-wavelength light (148), and its application in light therapy has the potential to reduce light intensity and exposure time (149). However, effectiveness may also be lost if the light exposure timing is extremely late and out of the phase-advancing zone.
The side effects of light therapy on the skin and retina should also be noted. Although commercial light therapy products do not emit ultraviolet light, patients with eye diseases or those using photosensitizing drugs should be monitored regularly by ophthalmologists and dermatologists for underlying conditions during the administration of light therapy (150–152). Mania induction as a side effect of light therapy should also be considered (153). Melatonin release appears to decrease during depression and increase during mania (96, 154). Careful monitoring of psychiatric symptoms is crucial to maintain the safety of light therapy in patients with DSWPD and bipolar disorder (155). The AASM guidelines updated in 2015 noted that little evidence exists for the efficacy of light therapy in adults and recommended that light therapy should be administered only for DSWPD in children and adolescents after spontaneous awakening in combination with behavioral approaches provided by caregivers or others (156). As for the case of circadian-entrained DSWPD, no studies have investigated the effectiveness of light therapy in this phenotype.
The DSWPD treatment guidelines of AASM, which were revised in 2015 (156), recommend the use of melatonin and melatonin receptor agonists for the treatment of DSWPD in children, adolescents, and adults. Exogenous melatonin and its agonists have hypnotic effects along with decrease in CBT via the MT1 receptor and circadian phase resetting effect via the MT2 receptor. As for the role of the MT2 receptor, the PRC of melatonin administration on circadian rhythm is approximately 180° out of phase with that of light. Similar to CBTmin serving as an “inflection point” for the phase-delay and -advance effects of light, DLMO serves as an approximate inflection point for the phase-delay and -advance effects of melatonin (157). In patients with DSWPD, melatonin (0.3 mg) administration for a 4-week period between 1.5 and 6.5 h prior to DLMO showed phase advance of the circadian rhythm, wherein the magnitude of phase advance was strongly correlated with the time of melatonin administration and earlier administration times were more effective (158). Another study also showed that the administration of melatonin (5 mg) for 4 weeks between 19:00 and 21:00 h reduced sleep onset latency in patients with DSWPD (159). Evidence for the efficacy of melatonin in DSWPD, including the result of a meta-analysis (160) is being accumulated. Melatonin administration has been shown to improve comorbid depression and advance the melatonin secretory rhythm in patients with DSWPD (161). A small dose of melatonin administered 6–7 h before natural sleep onset (158, 162) or 5 h before DLMO (157) has been reported to be effective for the treatment of DSWPD. However, a consensus regarding the optimal timing, dose, and duration of melatonin administration has not yet been achieved.
Concerning the side effects of melatonin, the use of <10 mg/day in adults has been reported to be safe (163, 164). However, side effects, such as headache, somnolence, hypotension, hypertension, gastrointestinal upset, and worsening of alopecia areata, have been reported with high-dose usage (165). Cases of side effects, such as increased depressive symptoms (166) and decreased glucose tolerance (167) have also been reported. In the case of children, several studies have not found any adverse events with melatonin treatment in pediatric patients with DSWPD complicated by neurodevelopmental disorders (168–170). However, concerns exist about the effects of melatonin treatment on growth hormones during this developmental stage (171, 172) and the resulting potential adverse effects on reproductive function (173). One study (Meldos Trial) has reported no adverse events with reproductive development of the children when using melatonin at 0.3–10 mg doses (mean dose 2.69 mg) (174). In 2018, follow-up study of this trial also reported that adverse events were scarce but the study showed a tendency towards delayed puberty in the former and current users of melatonin (175). Another longitudinal study of melatonin treatment in 44 children with neurodevelopmental disorders showed that pubertal timing was considered within normal limits except in five children with severe neurodevelopmental disability, most of whom experienced precocious puberty prior to the start of melatonin treatment (170). A recent review of this area concluded that no consensus could be reached yet, as only a few studies with small samples have investigated the pubertal timing of melatonin users (176).
Ramelteon is the first melatonin receptor agonist developed as a hypnotic in Japan. Ramelteon has a high affinity for the MT1 receptor, which is considered to be involved in human sleep, and the MT2 receptor, which seems to regulate circadian rhythms (177, 178). Therefore, similar to melatonin, ramelteon is expected to exhibit therapeutic effects in DSWPD (179). Administration of 1–4 mg of ramelteon at 30 min before bedtime produces a phase advance. However, no difference in the effect was found between a dose of 8 mg and a placebo (180), suggesting that a small drug dose would be preferable for the treatment of DSWPD (181, 182). However, clinical evidence regarding the optimal timing of ramelteon administration for the treatment of DSWPD remains scarce. In addition to ramelteon, other melatonin receptor agonists are available. Tasimelteon is a melatonin receptor agonist that was approved as an orphan drug by the US FDA in 2010 for treating N24SWD in blind individuals. This drug exhibits high affinity for MT1 and MT2 melatonergic receptors in humans, which is similar to the action of melatonin or ramelteon (183, 184). Agomelatine (185) acts as both a melatonin receptor agonist and serotonergic receptor antagonist and was approved by the European Union for the treatment of depression in 2009. Agomelatine may promote sleep at night through its melatonergic effect and help maintain alertness during the day via its 5-HT2C antagonistic effect (184). However, little evidence exists on agomelatonine’s ability to improve circadian rhythms when compared to other melatonergic drugs.
Among other DSWPD treatment methods, chronotherapy (60), in which sleep is intentionally delayed for 3 h each day to fix the sleep–wake rhythm to the desired time, has been formerly advocated. Although the literature on chronotherapy is scarce, few studies have reported cases that were effectively treated with chronotherapy. One case report showed that chronotherapy improved nighttime sleep and daytime psychiatric symptoms in children with attention deficit disorder complicated by DSWPD (186), while another case report found that the combination of chronotherapy and light therapy was effective in the treatment of DSWPD (187). However, chronotherapy is labor-intensive and carries the risk of developing N24SWD (188). Therefore, this therapy is not currently recommended in the AASM guidelines.
Aripiprazole is an antipsychotic drug that acts as a partial agonist of D2 receptors (189), but it appears to have no direct chronobiological action. However, a low dose of aripiprazole (3 mg or less) was reported to be effective in enabling patients with DSWPD to wake up in the morning (190). Although the detailed mechanism of its action is unknown, this drug appears to help in waking up at the desired time in the morning, which leads to a decrease in sleep time and consequent advancement of the sleep phase (191). Furthermore, aripiprazole is an effective adjunctive therapy for major depressive disorders (192). As previously mentioned, patients with DSWPD often have complications, such as depressive symptoms or prolonged sleep duration. Therefore, aripiprazole may be a new potential treatment option for DSWPD. Aripiprazole has fewer side effects than other antipsychotics and is increasingly prescribed to children, but drowsiness, extrapyramidal effects, metabolic effects, and weight gain should be noted (193). Although this drug is only used at low doses in DSWPD, it is an off-label prescription and requires careful monitoring of side effects in children and adolescents.
To date, the treatment of DSWPD has mainly focused on the chronobiological background. However, DSWPD is often recurrent and likely to follow a chronic course (19, 66), and either environmental or psychosocial factors may also contribute to the development and perpetuation of the disorder. Particularly in adolescent DSWPD, late work schedule, involvement in extracurricular activities, exposure to indoor lighting during evening hours (194), and/or delay in weekend wake-up time (195) may affect treatment responses (196). In these situations, a carefully individualized approach to change problematic situations is necessary. Furthermore, repeated exposure to frustration about sleep initiation can lead to psychological hyperarousal at night, which may contribute to the perpetuation of the disorder. Considering this process and that patients with DSWPD are likely to have elevated neuroticism (83), a cognitive-behavioral approach consisting of stimulus control, sleep hygiene education, cognitive restructuring, and mindfulness-based stress reduction to address sleep latency, in conjunction with the chronobiological approach, may become a treatment option for DSWPD. However, evidence for the effectiveness of combination treatment confirmed through randomized controlled trials on a large number of cases remains scarce. Of note, cognitive and behavioral approaches are also possible candidates for the treatment of circadian entrained-DSWPD. Given that, the likelihood of a favorable response to chronobiological treatment is quite low in patients with a lack of social zeitgebers, such as school attendance and employment or those without motivation for treatment; thus, less complex interventions should be considered for patients with these characteristics (156). In addition, ensuring diversity in social institutions so as to provide accommodation for the circadian preference of patients with DSWPD may be an important choice for some refractory cases (197).
From a psychiatric perspective, we reviewed the sleep behavior of adolescents and young adults, the psycho-behavioral characteristics of DSWPD in this young generation, and the association of DSWPD with psychiatric disorders. The pathogenesis of DSWPD is heterogeneous, with many mechanisms yet to be elucidated. The phenotype of DSWPD (including the presence or absence of circadian entrainment and phase angle expansion) varies depending on the interrelationship among various factors, including biological, social, and environmental factors, psycho-behavioral characteristics, and psychiatric disorders. DSWPD is a recurrent disorder, and its treatment is labor-intensive and time-consuming. Conventional DSWPD treatment has focused on biological factors; however, individually optimized treatment that considers not only the chronobiological factors but also psychological factors as well as the lifestyle and environment of young people should be developed.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This research was funded by a grant from the Japan Society for the Promotion of Science (KAKENHI) (grant number: JP21K13703).
We would like to thank Yoko Tomori, Assistant Professor at the University of the Ryukyus, for reducing the burden of clinical work to complete this manuscript.
KF reported personal fees from Eisai., Ltd. and MSD outside the submitted work. YT reported lecture fees from Takeda Pharmaceutical, Sumitomo Pharma, Otsuka Pharmaceutical, Meiji Seika Pharma, Kyowa Pharmaceutical, Eisai, MSD, and Yoshitomi Pharmaceutical outside the submitted work. KM reported personal fees from Eisai, Meiji Seika Pharma, MSD, Otsuka Pharmaceutical, Takeda Pharmaceutical, and Yoshitomi Pharmaceutical outside the submitted work. AS reported personal fees from Eisai and Sumitomo Pharma outside the submitted work. IO reported grants from NEC Solution Innovators Co., Ltd. and Infocom Co.; personal fees from Otsuka Pharmaceutical MSD, and Eisai.; and consultation fees from NEC Solution Innovators Co., Ltd. and Suntory Wellness Ltd. outside the submitted work. YK reported lecture fees from Eisai outside the submitted work. YI reported personal fees from Eisai, Otsuka Pharmaceutical, Takeda Pharmaceutical, Astellas Pharma Inc., and MED K.K. and grants from Philips Japan Co., Ltd., Koike Medical Co., Ltd., and Teijin Pharma Ltd. outside the submitted work.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Moore, RY. The fourth C.U. Ariens Kappers lecture. The organization of the human circadian timing system. Prog Brain Res. (1992) 93:99–115.
2. Czeisler, CA, Duffy, JF, Shanahan, TL, Brown, EN, Mitchell, JF, Rimmer, DW, et al. Stability, precision, and near-24-hour period of the human circadian pacemaker. Science. (1999) 284:2177–81. doi: 10.1126/science.284.5423.2177
3. Carskadon, MA, Labyak, SE, Acebo, C, and Seifer, R. Intrinsic circadian period of adolescent humans measured in conditions of forced desynchrony. Neurosci Lett. (1999) 260:129–32. doi: 10.1016/S0304-3940(98)00971-9
4. Meyer, N, Harvey, AG, Lockley, SW, and Dijk, DJ. Circadian rhythms and disorders of the timing of sleep. Lancet. (2022) 400:1061–78. doi: 10.1016/S0140-6736(22)00877-7
5. Duffy, JF, Cain, SW, Chang, AM, Phillips, AJ, Munch, MY, Gronfier, C, et al. Sex difference in the near-24-hour intrinsic period of the human circadian timing system. Proc Natl Acad Sci U S A. (2011) 108:15602–8. doi: 10.1073/pnas.1010666108
6. Hastings, MH, Maywood, ES, and Brancaccio, M. Generation of circadian rhythms in the suprachiasmatic nucleus. Nat Rev Neurosci. (2018) 19:453–69. doi: 10.1038/s41583-018-0026-z
7. St Hilaire, MA, Gooley, JJ, Khalsa, SB, Kronauer, RE, Czeisler, CA, and Lockley, SW. Human phase response curve to a 1 h pulse of bright white light. J Physiol. (2012) 590:3035–45. doi: 10.1113/jphysiol.2012.227892
8. Mistlberger, RE, and Skene, DJ. Nonphotic entrainment in humans? J Biol Rhythm. (2005) 20:339–52. doi: 10.1177/0748730405277982
9. Tamura, N, Sasai-Sakuma, T, Morita, Y, Okawa, M, Inoue, S, and Inoue, Y. Prevalence and associated factors of circadian rhythm sleep-wake disorders and insomnia among visually impaired Japanese individuals. BMC Public Health. (2021) 21:31. doi: 10.1186/s12889-020-09993-8
10. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine (2014).
11. Smith, MT, McCrae, CS, Cheung, J, Martin, JL, Harrod, CG, Heald, JL, et al. Use of Actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: an American Academy of sleep medicine systematic review, Meta-analysis, and GRADE assessment. J Clin Sleep Med. (2018) 14:1209–30. doi: 10.5664/jcsm.7228
12. Danielsson, K, Markstrom, A, Broman, JE, von Knorring, L, and Jansson-Frojmark, M. Delayed sleep phase disorder in a Swedish cohort of adolescents and young adults: prevalence and associated factors. Chronobiol Int. (2016) 33:1331–9. doi: 10.1080/07420528.2016.1217002
13. Wittmann, M, Dinich, J, Merrow, M, and Roenneberg, T. Social jetlag: misalignment of biological and social time. Chronobiol Int. (2006) 23:497–509. doi: 10.1080/07420520500545979
14. Murray, JM, Sletten, TL, Magee, M, Gordon, C, Lovato, N, Bartlett, DJ, et al. Prevalence of circadian misalignment and its association with depressive symptoms in delayed sleep phase disorder. Sleep. (2017) 40:zsw002. doi: 10.1093/sleep/zsw002
15. Kroese, FM, De Ridder, DT, Evers, C, and Adriaanse, MA. Bedtime procrastination: introducing a new area of procrastination. Front Psychol. (2014) 5:611. doi: 10.3389/fpsyg.2014.00611
16. Weitzman, ED, Czeisler, CA, Coleman, RM, Spielman, AJ, Zimmerman, JC, Dement, W, et al. Delayed sleep phase syndrome. A chronobiological disorder with sleep-onset insomnia. Arch Gen Psychiatry. (1981) 38:737–46. doi: 10.1001/archpsyc.1981.01780320017001
17. Thorpy, MJ. Diagnostic Classification Steering Committee: International Classification of Sleep Disorders: Diagnostic and Coding Manual. Rochester, NY: American Sleep Disorders Association (1990).
18. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 2nd ed. Daren, IL: American Academy of Sleep Medicine (2005).
19. Dagan, Y, and Eisenstein, M. Circadian rhythm sleep disorders: toward a more precise definition and diagnosis. Chronobiol Int. (1999) 16:213–22. doi: 10.3109/07420529909019087
20. Tsuchiya, A, Kitajima, T, Tomita, S, Esaki, Y, Hirose, M, and Iwata, N. High prevalence of orthostatic dysregulation among circadian rhythm disorder patients. J Clin Sleep Med. (2016) 12:1471–6. doi: 10.5664/jcsm.6268
21. Lovato, N, Gradisar, M, Short, M, Dohnt, H, and Micic, G. Delayed sleep phase disorder in an Australian school-based sample of adolescents. J Clin Sleep Med. (2013) 09:939–44. doi: 10.5664/jcsm.2998
22. Abe, T, Inoue, Y, Komada, Y, Nakamura, M, Asaoka, S, Kanno, M, et al. Relation between morningness-eveningness score and depressive symptoms among patients with delayed sleep phase syndrome. Sleep Med. (2011) 12:680–4. doi: 10.1016/j.sleep.2010.12.017
23. Saxvig, IW, Pallesen, S, Wilhelmsen-Langeland, A, Molde, H, and Bjorvatn, B. Prevalence and correlates of delayed sleep phase in high school students. Sleep Med. (2012) 13:193–9. doi: 10.1016/j.sleep.2011.10.024
24. Sivertsen, B, Harvey, AG, Pallesen, S, and Hysing, M. Mental health problems in adolescents with delayed sleep phase: results from a large population-based study in Norway. J Sleep Res. (2015) 24:11–8. doi: 10.1111/jsr.12254
25. Tomishima, S, Komada, Y, Tanioka, K, Okajima, I, and Inoue, Y. Prevalence and factors associated with the risk of delayed sleep-wake phase disorder in Japanese youth. Front Psych. (2022) 13:878042. doi: 10.3389/fpsyt.2022.878042
26. Sivertsen, B, Harvey, AG, Gradisar, M, Pallesen, S, and Hysing, M. Delayed sleep-wake phase disorder in young adults: prevalence and correlates from a national survey of Norwegian university students. Sleep Med. (2021) 77:184–91. doi: 10.1016/j.sleep.2020.09.028
27. Sivertsen, B, Pallesen, S, Stormark, KM, Boe, T, Lundervold, AJ, and Hysing, M. Delayed sleep phase syndrome in adolescents: prevalence and correlates in a large population based study. BMC Public Health. (2013) 13:1163. doi: 10.1186/1471-2458-13-1163
28. Otsuki, R, Matsui, K, Yoshiike, T, Nagao, K, Utsumi, T, Tsuru, A, et al. Decrease in social Zeitgebers is associated with worsened delayed sleep-wake phase disorder: findings during the pandemic in Japan. Front Psych. (2022) 13:898600. doi: 10.3389/fpsyt.2022.898600
29. Thorpy, MJ, Korman, E, Spielman, AJ, and Glovinsky, PB. Delayed sleep phase syndrome in adolescents. J Adolesc Health Care. (1988) 9:22–7. doi: 10.1016/0197-0070(88)90014-9
30. Rajaratnam, SMW, Licamele, L, and Birznieks, G. Delayed sleep phase disorder risk is associated with absenteeism and impaired functioning. Sleep Health. (2015) 1:121–7. doi: 10.1016/j.sleh.2015.03.001
31. Glozier, N, O'Dea, B, McGorry, PD, Pantelis, C, Amminger, GP, Hermens, DF, et al. Delayed sleep onset in depressed young people. BMC Psychiatry. (2014) 14:33. doi: 10.1186/1471-244X-14-33
32. Zou, H, Zhou, H, Yan, R, Yao, Z, and Lu, Q. Chronotype, circadian rhythm, and psychiatric disorders: recent evidence and potential mechanisms. Front Neurosci. (2022) 16:811771. doi: 10.3389/fnins.2022.811771
33. Cole, RJ, Smith, JS, Alcala, YC, Elliott, JA, and Kripke, DF. Bright-light mask treatment of delayed sleep phase syndrome. J Biol Rhythm. (2002) 17:89–101. doi: 10.1177/074873002129002366
34. Ong, JL, Tandi, J, Patanaik, A, Lo, JC, and Chee, MWL. Large-scale data from wearables reveal regional disparities in sleep patterns that persist across age and sex. Sci Rep. (2019) 9:3415. doi: 10.1038/s41598-019-40156-x
35. Pandi-Perumal, SR, Smits, M, Spence, W, Srinivasan, V, Cardinali, DP, Lowe, AD, et al. Dim light melatonin onset (DLMO): a tool for the analysis of circadian phase in human sleep and chronobiological disorders. Prog Neuro-Psychopharmacol Biol Psychiatry. (2007) 31:1–11. doi: 10.1016/j.pnpbp.2006.06.020
36. Uchiyama, M, Okawa, M, Shibui, K, Kim, K, Tagaya, H, Kudo, Y, et al. Altered phase relation between sleep timing and core body temperature rhythm in delayed sleep phase syndrome and non-24-hour sleep-wake syndrome in humans. Neurosci Lett. (2000) 294:101–4. doi: 10.1016/S0304-3940(00)01551-2
37. Matsunaga, D, Tanaka, Y, Seyama, M, and Nagashima, K. Non-invasive and wearable thermometer for continuous monitoring of core body temperature under various convective conditions. Annu Int Conf IEEE Eng Med Biol Soc. (2020) 2020:4377–80. doi: 10.1109/EMBC44109.2020.9176403
38. Dolson, CM, Harlow, ER, Phelan, DM, Gabbett, TJ, Gaal, B, McMellen, C, et al. Wearable sensor technology to predict Core body temperature: a systematic review. Sensors. (2022) 22:7639. doi: 10.3390/s22197639
39. Arendt, J. Melatonin: characteristics, concerns, and prospects. J Biol Rhythm. (2005) 20:291–303. doi: 10.1177/0748730405277492
40. Horne, JA, and Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. (1976) 4:97–110.
41. Kantermann, T, Sung, H, and Burgess, HJ. Comparing the morningness-eveningness questionnaire and Munich ChronoType questionnaire to the dim light melatonin onset. J Biol Rhythm. (2015) 30:449–53. doi: 10.1177/0748730415597520
42. Roenneberg, T, Kumar, CJ, and Merrow, M. The human circadian clock entrains to sun time. Curr Biol. (2007) 17:R44–5. doi: 10.1016/j.cub.2006.12.011
43. Takaesu, Y, Inoue, Y, Ono, K, Murakoshi, A, Futenma, K, Komada, Y, et al. Circadian rhythm sleep-wake disorders predict shorter time to relapse of mood episodes in euthymic patients with bipolar disorder: a prospective 48-week study. J Clin Psychiatry. (2018) 79:17m11565. doi: 10.4088/JCP.17m11565
44. Moon, JH, Cho, CH, Son, GH, Geum, D, Chung, S, Kim, H, et al. Advanced circadian phase in mania and delayed circadian phase in mixed mania and depression returned to Normal after treatment of bipolar disorder. EBioMedicine. (2016) 11:285–95. doi: 10.1016/j.ebiom.2016.08.019
45. Giglio, LM, Magalhaes, PV, Andreazza, AC, Walz, JC, Jakobson, L, Rucci, P, et al. Development and use of a biological rhythm interview. J Affect Disord. (2009) 118:161–5. doi: 10.1016/j.jad.2009.01.018
46. Kanda, Y, Takaesu, Y, Kobayashi, M, Komada, Y, Futenma, K, Okajima, I, et al. Reliability and validity of the Japanese version of the biological rhythms interview of assessment in neuropsychiatry-self report for delayed sleep-wake phase disorder. Sleep Med. (2021) 81:288–93. doi: 10.1016/j.sleep.2021.02.009
47. Solheim, B, Langsrud, K, Kallestad, H, Engstrom, M, Bjorvatn, B, and Sand, T. Sleep structure and awakening threshold in delayed sleep-wake phase disorder patients compared to healthy sleepers. Sleep Med. (2018) 46:61–8. doi: 10.1016/j.sleep.2018.03.001
48. Reis, C, and Paiva, T. Delayed sleep-wake phase disorder in a clinical population: gender and sub-population diferences. Sleep Sci. (2019) 12:203–13. doi: 10.5935/1984-0063.20190086
49. Schrader, H, Bovim, G, and Sand, T. The prevalence of delayed and advanced sleep phase syndromes. J Sleep Res. (1993) 2:51–5. doi: 10.1111/j.1365-2869.1993.tb00061.x
50. Paine, SJ, Fink, J, Gander, PH, and Warman, GR. Identifying advanced and delayed sleep phase disorders in the general population: a national survey of New Zealand adults. Chronobiol Int. (2014) 31:627–36. doi: 10.3109/07420528.2014.885036
51. Adolescent Sleep Working Group; Committee on Adolescence; Council on School HealthAu, R, Carskadon, M, and Millman, R. School start times for adolescents. Pediatrics. (2014) 134:642–9. doi: 10.1542/peds.2014-1697
52. Hysing, M, Harvey, AG, Stormark, KM, Pallesen, S, and Sivertsen, B. Precursors of delayed sleep phase in adolescence: a population-based longitudinal study. Sleep. (2018) 41:zsy163. doi: 10.1093/sleep/zsy163
53. Morita, Y, Sasai-Sakuma, T, Asaoka, S, and Inoue, Y. The impact of a delayed sleep-wake schedule on depression is greater in women – a web-based cross-sectional study in Japanese young adults. Chronobiol Int. (2015) 32:952–8. doi: 10.3109/07420528.2015.1055756
54. Foster, RG, and Roenneberg, T. Human responses to the geophysical daily, annual and lunar cycles. Curr Biol. (2008) 18:R784–94. doi: 10.1016/j.cub.2008.07.003
55. Saxvig, IW, Wilhelmsen-Langeland, A, Pallesen, S, Vedaa, O, Nordhus, IH, Sorensen, E, et al. Objective measures of sleep and dim light melatonin onset in adolescents and young adults with delayed sleep phase disorder compared to healthy controls. J Sleep Res. (2013) 22:365–72. doi: 10.1111/jsr.12030
56. Micic, G, Lovato, N, Gradisar, M, Burgess, HJ, Ferguson, SA, Kennaway, DJ, et al. Nocturnal melatonin profiles in patients with delayed sleep-wake phase disorder and control sleepers. J Biol Rhythm. (2015) 30:437–48. doi: 10.1177/0748730415591753
57. Phillips, AJK, Vidafar, P, Burns, AC, McGlashan, EM, Anderson, C, Rajaratnam, SMW, et al. High sensitivity and interindividual variability in the response of the human circadian system to evening light. Proc Natl Acad Sci U S A. (2019) 116:12019–24. doi: 10.1073/pnas.1901824116
58. Wright, KP Jr, Gronfier, C, Duffy, JF, and Czeisler, CA. Intrinsic period and light intensity determine the phase relationship between melatonin and sleep in humans. J Biol Rhythm. (2005) 20:168–77. doi: 10.1177/0748730404274265
59. Chellappa, SL. Individual differences in light sensitivity affect sleep and circadian rhythms. Sleep. (2021) 44:zsaa214. doi: 10.1093/sleep/zsaa214
60. Czeisler, CA, Richardson, GS, Coleman, RM, Zimmerman, JC, Moore-Ede, MC, Dement, WC, et al. Chronotherapy: resetting the circadian clocks of patients with delayed sleep phase insomnia. Sleep. (1981) 4:1–21. doi: 10.1093/sleep/4.1.1
61. Aoki, H, Ozeki, Y, and Yamada, N. Hypersensitivity of melatonin suppression in response to light in patients with delayed sleep phase syndrome. Chronobiol Int. (2001) 18:263–71. doi: 10.1081/CBI-100103190
62. Gronfier, C, Wright, KP Jr, Kronauer, RE, and Czeisler, CA. Entrainment of the human circadian pacemaker to longer-than-24-h days. Proc Natl Acad Sci U S A. (2007) 104:9081–6. doi: 10.1073/pnas.0702835104
63. Micic, G, Lovato, N, Gradisar, M, Burgess, HJ, Ferguson, SA, and Lack, L. Circadian melatonin and temperature Taus in delayed sleep-wake phase disorder and Non-24-hour sleep-wake rhythm disorder patients: an Ultradian constant routine study. J Biol Rhythm. (2016) 31:387–405. doi: 10.1177/0748730416650069
64. Micic, G, de Bruyn, A, Lovato, N, Wright, H, Gradisar, M, Ferguson, S, et al. The endogenous circadian temperature period length (tau) in delayed sleep phase disorder compared to good sleepers. J Sleep Res. (2013) 22:617–24. doi: 10.1111/jsr.12072
65. Chang, AM, Duffy, JF, Buxton, OM, Lane, JM, Aeschbach, D, Anderson, C, et al. Chronotype genetic variant in PER2 is associated with intrinsic circadian period in humans. Sci Rep. (2019) 9:5350. doi: 10.1038/s41598-019-41712-1
66. Sack, RL, Auckley, D, Auger, RR, Carskadon, MA, Wright, KP Jr, Vitiello, MV, et al. Circadian rhythm sleep disorders: part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. An American Academy of sleep medicine review. Sleep. (2007) 30:1484–501. doi: 10.1093/sleep/30.11.1484
67. Ozaki, S, Uchiyama, M, Shirakawa, S, and Okawa, M. Prolonged interval from body temperature nadir to sleep offset in patients with delayed sleep phase syndrome. Sleep. (1996) 19:36–40.
68. Shibui, K, Uchiyama, M, and Okawa, M. Melatonin rhythms in delayed sleep phase syndrome. J Biol Rhythm. (1999) 14:72–6. doi: 10.1177/074873099129000371
69. Watanabe, T, Kajimura, N, Kato, M, Sekimoto, M, Nakajima, T, Hori, T, et al. Sleep and circadian rhythm disturbances in patients with delayed sleep phase syndrome. Sleep. (2003) 26:657–61. doi: 10.1093/sleep/26.6.657
70. Okawa, M, and Uchiyama, M. Circadian rhythm sleep disorders: characteristics and entrainment pathology in delayed sleep phase and non-24-h sleep-wake syndrome. Sleep Med Rev. (2007) 11:485–96. doi: 10.1016/j.smrv.2007.08.001
71. Bailey, M, and Silver, R. Sex differences in circadian timing systems: implications for disease. Front Neuroendocrinol. (2014) 35:111–39. doi: 10.1016/j.yfrne.2013.11.003
72. Yan, L, and Silver, R. Neuroendocrine underpinnings of sex differences in circadian timing systems. J Steroid Biochem Mol Biol. (2016) 160:118–26. doi: 10.1016/j.jsbmb.2015.10.007
73. Duarte, LL, Menna-Barreto, L, Miguel, MA, Louzada, F, Araujo, J, Alam, M, et al. Chronotype ontogeny related to gender. Braz J Med Biol Res. (2014) 47:316–20. doi: 10.1590/1414-431X20143001
74. Uchiyama, M, Okawa, M, Shibui, K, Liu, X, Hayakawa, T, Kamei, Y, et al. Poor compensatory function for sleep loss as a pathogenic factor in patients with delayed sleep phase syndrome. Sleep. (2000) 23:553–8.
75. Ashbrook, LH, Krystal, AD, Fu, YH, and Ptacek, LJ. Genetics of the human circadian clock and sleep homeostat. Neuropsychopharmacology. (2020) 45:45–54. doi: 10.1038/s41386-019-0476-7
76. Uchiyama, M, and Lockley, SW. Non-24-hour sleep-wake rhythm disorder in sighted and blind patients. Sleep Med Clin. (2015) 10:495–516. doi: 10.1016/j.jsmc.2015.07.006
77. Abbott, SM, Choi, J, Wilson, J, and Zee, PC. Melanopsin-dependent phototransduction is impaired in delayed sleep-wake phase disorder and sighted non-24-hour sleep-wake rhythm disorder. Sleep. (2021) 44:zsaa184. doi: 10.1093/sleep/zsaa184
78. Hale, L, and Guan, S. Screen time and sleep among school-aged children and adolescents: a systematic literature review. Sleep Med Rev. (2015) 21:50–8. doi: 10.1016/j.smrv.2014.07.007
79. Goldberg, LR. An alternative "description of personality": the big-five factor structure. J Pers Soc Psychol. (1990) 59:1216–29. doi: 10.1037/0022-3514.59.6.1216
80. Tsaousis, I. Circadian preferences and personality traits: a meta-analysis. Eur J Personal. (2010) 24:356–73. doi: 10.1002/per.754
81. Duggan, KA, Friedman, HS, McDevitt, EA, and Mednick, SC. Personality and healthy sleep: the importance of conscientiousness and neuroticism. PLoS One. (2014) 9:e90628. doi: 10.1371/journal.pone.0090628
82. Milic, J, Milic Vranjes, I, Krajina, I, Heffer, M, and Skrlec, I. Circadian typology and personality dimensions of Croatian students of health-related university majors. Int J Environ Res Public Health. (2020) 17:4794. doi: 10.3390/ijerph17134794
83. Stolarski, M, Gorgol, J, and Matthews, G. The search for causality of personality-chronotype associations: insights from a one-year longitudinal study of adolescents. Chronobiol Int. (2021) 38:489–500. doi: 10.1080/07420528.2020.1867157
84. Shirayama, M, Shirayama, Y, Iida, H, Kato, M, Kajimura, N, Watanabe, T, et al. The psychological aspects of patients with delayed sleep phase syndrome (DSPS). Sleep Med. (2003) 4:427–33. doi: 10.1016/S1389-9457(03)00101-1
85. Wilhelmsen-Langeland, A, Saxvig, IW, Pallesen, S, Nordhus, IH, Vedaa, O, Sorensen, E, et al. The personality profile of young adults with delayed sleep phase disorder. Behav Sleep Med. (2014) 12:481–92. doi: 10.1080/15402002.2013.829063
86. Gradisar, M, Dohnt, H, Gardner, G, Paine, S, Starkey, K, Menne, A, et al. A randomized controlled trial of cognitive-behavior therapy plus bright light therapy for adolescent delayed sleep phase disorder. Sleep. (2011) 34:1671–80. doi: 10.5665/sleep.1432
87. Richardson, CE, Gradisar, M, and Barbero, SC. Are cognitive "insomnia" processes involved in the development and maintenance of delayed sleep wake phase disorder? Sleep Med Rev. (2016) 26:1–8. doi: 10.1016/j.smrv.2015.05.001
88. Robillard, R, Carpenter, JS, Rogers, NL, Fares, S, Grierson, AB, Hermens, DF, et al. Circadian rhythms and psychiatric profiles in young adults with unipolar depressive disorders. Transl Psychiatry. (2018) 8:213. doi: 10.1038/s41398-018-0255-y
89. Takaesu, Y, Inoue, Y, Murakoshi, A, Komada, Y, Otsuka, A, Futenma, K, et al. Prevalence of circadian rhythm sleep-wake disorders and associated factors in euthymic patients with bipolar disorder. PLoS One. (2016) 11:e0159578. doi: 10.1371/journal.pone.0159578
90. Nota, JA, Sharkey, KM, and Coles, ME. Sleep, arousal, and circadian rhythms in adults with obsessive-compulsive disorder: a meta-analysis. Neurosci Biobehav Rev. (2015) 51:100–7. doi: 10.1016/j.neubiorev.2015.01.002
91. Spera, V, Maiello, M, Pallucchini, A, Novi, M, Elefante, C, De Dominicis, F, et al. Adult attention-deficit hyperactivity disorder and clinical correlates of delayed sleep phase disorder. Psychiatry Res. (2020) 291:113162. doi: 10.1016/j.psychres.2020.113162
92. Matsui, K, Inada, K, Kuriyama, K, Yoshiike, T, Nagao, K, Oshibuchi, H, et al. Prevalence of circadian rhythm sleep-wake disorder in outpatients with schizophrenia and its association with psychopathological characteristics and psychosocial functioning. J Clin Med. (2021) 10:1513. doi: 10.3390/jcm10071513
93. Takaesu, Y, Inoue, Y, Ono, K, Murakoshi, A, Futenma, K, Komada, Y, et al. Circadian rhythm sleep-wake disorders as predictors for bipolar disorder in patients with remitted mood disorders. J Affect Disord. (2017) 220:57–61. doi: 10.1016/j.jad.2017.05.041
94. Steinan, MK, Morken, G, Lagerberg, TV, Melle, I, Andreassen, OA, Vaaler, AE, et al. Delayed sleep phase: an important circadian subtype of sleep disturbance in bipolar disorders. J Affect Disord. (2016) 191:156–63. doi: 10.1016/j.jad.2015.11.025
95. Harvey, AG. Sleep and circadian rhythms in bipolar disorder: seeking synchrony, harmony, and regulation. Am J Psychiatry. (2008) 165:820–9. doi: 10.1176/appi.ajp.2008.08010098
96. Takaesu, Y. Circadian rhythm in bipolar disorder: a review of the literature. Psychiatry Clin Neurosci. (2018) 72:673–82. doi: 10.1111/pcn.12688
97. Gottlieb, JF, Benedetti, F, Geoffroy, PA, Henriksen, TEG, Lam, RW, Murray, G, et al. The chronotherapeutic treatment of bipolar disorders: a systematic review and practice recommendations from the ISBD task force on chronotherapy and chronobiology. Bipolar Disord. (2019) 21:741–73. doi: 10.1111/bdi.12847
98. Korman, M, Palm, D, Uzoni, A, Faltraco, F, Tucha, O, Thome, J, et al. ADHD 24/7: circadian clock genes, chronotherapy and sleep/wake cycle insufficiencies in ADHD. World J Biol Psychiatry. (2020) 21:156–71. doi: 10.1080/15622975.2018.1523565
99. Carmassi, C, Palagini, L, Caruso, D, Masci, I, Nobili, L, Vita, A, et al. Systematic review of sleep disturbances and circadian sleep desynchronization in autism Spectrum disorder: toward an integrative model of a self-reinforcing loop. Front Psych. (2019) 10:366. doi: 10.3389/fpsyt.2019.00366
100. Baker, EK, and Richdale, AL. Examining the behavioural sleep-wake rhythm in adults with autism spectrum disorder and no comorbid intellectual disability. J Autism Dev Disord. (2017) 47:1207–22. doi: 10.1007/s10803-017-3042-3
101. Lunsford-Avery, JR, and Kollins, SH. Editorial perspective: delayed circadian rhythm phase: a cause of late-onset attention-deficit/hyperactivity disorder among adolescents? J Child Psychol Psychiatry. (2018) 59:1248–51. doi: 10.1111/jcpp.12956
102. Micic, G, Lovato, N, Gradisar, M, and Lack, LC. Personality differences in patients with delayed sleep-wake phase disorder and non-24-h sleep-wake rhythm disorder relative to healthy sleepers. Sleep Med. (2017) 30:128–35. doi: 10.1016/j.sleep.2016.04.002
103. Micic, G, Lovato, N, Ferguson, SA, Burgess, HJ, and Lack, L. Circadian tau differences and rhythm associations in delayed sleep-wake phase disorder and sighted non-24-hour sleep-wake rhythm disorder. Sleep. (2021) 44:zsaa132. doi: 10.1093/sleep/zsaa132
104. Lin, RM, Xie, SS, Yan, YW, Chen, YH, and Yan, WJ. Perfectionism and adolescent sleep quality: the mediating role of repetitive negative thinking. J Health Psychol. (2019) 24:1626–36. doi: 10.1177/1359105317693914
105. Wright, KP Jr, McHill, AW, Birks, BR, Griffin, BR, Rusterholz, T, and Chinoy, ED. Entrainment of the human circadian clock to the natural light-dark cycle. Curr Biol. (2013) 23:1554–8. doi: 10.1016/j.cub.2013.06.039
106. Merikanto, I, and Partonen, T. Increase in eveningness and insufficient sleep among adults in population-based cross-sections from 2007 to 2017. Sleep Med. (2020) 75:368–79. doi: 10.1016/j.sleep.2020.07.046
107. Pokorny, J, Smith, VC, and Lutze, M. Aging of the human lens. Appl Opt. (1987) 26:1437–40. doi: 10.1364/AO.26.001437
108. Higuchi, S, Nagafuchi, Y, Lee, S-i, and Harada, T. Influence of light at night on melatonin suppression in children. J Clin Endocrinol Metabol. (2014) 99:3298–303. doi: 10.1210/jc.2014-1629
109. Shimura, A, Sakai, H, Takaesu, Y, Nomura, R, Komada, Y, and Inoue, T. Comprehensive assessment of the impact of life habits on sleep disturbance, chronotype, and daytime sleepiness among high-school students. Sleep Med. (2018) 44:12–8. doi: 10.1016/j.sleep.2017.10.011
110. Lunn, RM, Blask, DE, Coogan, AN, Figueiro, MG, Gorman, MR, Hall, JE, et al. Health consequences of electric lighting practices in the modern world: a report on the National Toxicology Program's workshop on shift work at night, artificial light at night, and circadian disruption. Sci Total Environ. (2017) 607-608:1073–84. doi: 10.1016/j.scitotenv.2017.07.056
111. Yoshimura, M, Kitazawa, M, Maeda, Y, Mimura, M, Tsubota, K, and Kishimoto, T. Smartphone viewing distance and sleep: an experimental study utilizing motion capture technology. Nat Sci Sleep. (2017) 9:59–65. doi: 10.2147/NSS.S123319
112. Komada, Y, Breugelmans, R, Drake, CL, Nakajima, S, Tamura, N, Tanaka, H, et al. Social jetlag affects subjective daytime sleepiness in school-aged children and adolescents: a study using the Japanese version of the pediatric daytime sleepiness scale (PDSS-J). Chronobiol Int. (2016) 33:1311–9. doi: 10.1080/07420528.2016.1213739
113. Sasawaki, Y, Inokawa, H, Obata, Y, Nagao, S, and Yagita, K. Association of social jetlag and eating patterns with sleep quality and daytime sleepiness in Japanese high school students. J Sleep Res. (2022) 32:e13661. doi: 10.1111/jsr.13661
114. Okajima, I, Komada, Y, Ito, W, and Inoue, Y. Sleep debt and social jetlag associated with sleepiness, mood, and work performance among Workers in Japan. Int J Environ Res Public Health. (2021) 18:2908. doi: 10.3390/ijerph18062908
115. Panev, AS, Tserne, TA, Polugrudov, AS, Bakutova, LA, Petrova, NB, Tatarinova, OV, et al. Association of chronotype and social jetlag with human non-verbal intelligence. Chronobiol Int. (2017) 34:977–80. doi: 10.1080/07420528.2017.1324473
116. Smarr, BL, and Schirmer, AE. 3.4 million real-world learning management system logins reveal the majority of students experience social jet lag correlated with decreased performance. Sci Rep. (2018) 8:4793. doi: 10.1038/s41598-018-23044-8
117. Mathew, GM, Li, X, Hale, L, and Chang, AM. Sleep duration and social jetlag are independently associated with anxious symptoms in adolescents. Chronobiol Int. (2019) 36:461–9. doi: 10.1080/07420528.2018.1509079
118. Gau, SS, Shang, CY, Merikangas, KR, Chiu, YN, Soong, WT, and Cheng, AT. Association between morningness-eveningness and behavioral/emotional problems among adolescents. J Biol Rhythm. (2007) 22:268–74. doi: 10.1177/0748730406298447
119. Wright, KP, Lowry, CA, and Lebourgeois, MK. Circadian and wakefulness-sleep modulation of cognition in humans. Front Mol Neurosci. (2012) 5:50. doi: 10.3389/fnmol.2012.00050
120. Komada, Y, Okajima, I, Kitamura, S, and Inoue, Y. A survey on social jetlag in Japan: a nationwide, cross-sectional internet survey. Sleep Biol Rhythms. (2019) 17:417–22. doi: 10.1007/s41105-019-00229-w
121. Taylor, A, Wright, HR, and Lack, LC. Sleeping-in on the weekend delays circadian phase and increases sleepiness the following week. Sleep Biol Rhythms. (2008) 6:172–9. doi: 10.1111/j.1479-8425.2008.00356.x
122. Morin, CM, Bjorvatn, B, Chung, F, Holzinger, B, Partinen, M, Penzel, T, et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: an international collaborative study. Sleep Med. (2021) 87:38–45. doi: 10.1016/j.sleep.2021.07.035
123. Morin, CM, and Carrier, J. The acute effects of the COVID-19 pandemic on insomnia and psychological symptoms. Sleep Med. (2021) 77:346–7. doi: 10.1016/j.sleep.2020.06.005
124. Jahrami, H, BaHammam, AS, Bragazzi, NL, Saif, Z, Faris, M, and Vitiello, MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. (2021) 17:299–313. doi: 10.5664/jcsm.8930
125. Bonmati-Carrion, MA, Arguelles-Prieto, R, Martinez-Madrid, MJ, Reiter, R, Hardeland, R, Rol, MA, et al. Protecting the melatonin rhythm through circadian healthy light exposure. Int J Mol Sci. (2014) 15:23448–500. doi: 10.3390/ijms151223448
126. Korman, M, Tkachev, V, Reis, C, Komada, Y, Kitamura, S, Gubin, D, et al. COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci Rep. (2020) 10:22225. doi: 10.1038/s41598-020-79299-7
127. Wright, KP Jr, Linton, SK, Withrow, D, Casiraghi, L, Lanza, SM, Iglesia, H, et al. Sleep in university students prior to and during COVID-19 stay-at-home orders. Curr Biol. (2020) 30:R797–8. doi: 10.1016/j.cub.2020.06.022
128. Marelli, S, Castelnuovo, A, Somma, A, Castronovo, V, Mombelli, S, Bottoni, D, et al. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J Neurol. (2021) 268:8–15. doi: 10.1007/s00415-020-10056-6
129. Tanioka, K, Kayaba, M, Tomishima, S, Komada, Y, and Inoue, Y. Changes in sleep behavior, sleep problems, and psychological distress/health-related quality of life of young Japanese individuals before and during the COVID-19 pandemic. Chronobiol Int. (2022) 39:781–91. doi: 10.1080/07420528.2022.2034839
130. Gradisar, M, and Crowley, SJ. Delayed sleep phase disorder in youth. Curr Opin Psychiatry. (2013) 26:580–5. doi: 10.1097/YCO.0b013e328365a1d4
131. Asaoka, S, Komada, Y, Aritake, S, Morita, Y, Fukuda, K, and Inoue, Y. Effect of delayed sleep phase during university life on the daytime functioning in work life after graduation. Sleep Med. (2014) 15:1155–8. doi: 10.1016/j.sleep.2014.05.017
132. Matti Vuorre, DZ, Petrovskaya, E, Ballou, N, and Przybylski, AK. A large-scale study of changes to the quantity, quality, and distribution of video game play during a global health pandemic. Technol Mind Behav. (2021) 2:0048. doi: 10.1037/tmb0000048
133. King, DL, Achab, S, Higuchi, S, Bowden-Jones, H, Muller, KW, Billieux, J, et al. Gaming disorder and the COVID-19 pandemic: treatment demand and service delivery challenges. J Behav Addict. (2022) 11:243–8. doi: 10.1556/2006.2022.00011
134. Rochelle Cade, JG. Gamers and video game culture: an introduction for counselors. Fam J. (2017) 25:70–5. doi: 10.1177/1066480716679809
135. Stevens, MW, Dorstyn, D, Delfabbro, PH, and King, DL. Global prevalence of gaming disorder: a systematic review and meta-analysis. Aust N Z J Psychiatry. (2021) 55:553–68. doi: 10.1177/0004867420962851
136. World Health Organization (WHO). International Classification of Diseases 11th Revision (ICD-11); (2019). Available at: https://icd.who.int/en.
137. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publishing, Inc (2013).
138. Higuchi, S, Nakayama, H, Matsuzaki, T, Mihara, S, and Kitayuguchi, T. Application of the eleventh revision of the international classification of diseases gaming disorder criteria to treatment-seeking patients: comparison with the fifth edition of the diagnostic and statistical manual of mental disorders internet gaming disorder criteria. J Behav Addict. (2021) 10:149–58. doi: 10.1556/2006.2020.00099
139. Ko, CH, Lin, HC, Lin, PC, and Yen, JY. Validity, functional impairment and complications related to internet gaming disorder in the DSM-5 and gaming disorder in the ICD-11. Aust N Z J Psychiatry. (2020) 54:707–18. doi: 10.1177/0004867419881499
140. King, DL, Delfabbro, PH, Zwaans, T, and Kaptsis, D. Clinical features and axis I comorbidity of Australian adolescent pathological internet and video game users. Aust N Z J Psychiatry. (2013) 47:1058–67. doi: 10.1177/0004867413491159
141. Muller, KW, Janikian, M, Dreier, M, Wolfling, K, Beutel, ME, Tzavara, C, et al. Regular gaming behavior and internet gaming disorder in European adolescents: results from a cross-national representative survey of prevalence, predictors, and psychopathological correlates. Eur Child Adolesc Psychiatry. (2015) 24:565–74. doi: 10.1007/s00787-014-0611-2
142. Salerno, L, Becheri, L, and Pallanti, S. ADHD-gaming disorder comorbidity in children and adolescents: a narrative review. Children (Basel). (2022) 9:1528. doi: 10.3390/children9101528
143. Tateno, M, Matsuzaki, T, Takano, A, and Higuchi, S. Increasing important roles of child and adolescent psychiatrists in the treatment of gaming disorder: current status in Japan. Front Psych. (2022) 13:995665. doi: 10.3389/fpsyt.2022.995665
144. Zeitzer, JM, Dijk, DJ, Kronauer, R, Brown, E, and Czeisler, C. Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol. (2000) 526:695–702. doi: 10.1111/j.1469-7793.2000.00695.x
145. Chang, AM, Santhi, N, St Hilaire, M, Gronfier, C, Bradstreet, DS, Duffy, JF, et al. Human responses to bright light of different durations. J Physiol. (2012) 590:3103–12. doi: 10.1113/jphysiol.2011.226555
146. Thapan, K, Arendt, J, and Skene, DJ. An action spectrum for melatonin suppression: evidence for a novel non-rod, non-cone photoreceptor system in humans. J Physiol. (2001) 535:261–7. doi: 10.1111/j.1469-7793.2001.t01-1-00261.x
147. Brainard, GC, Hanifin, JP, Greeson, JM, Byrne, B, Glickman, G, Gerner, E, et al. Action spectrum for melatonin regulation in humans: evidence for a novel circadian photoreceptor. J Neurosci. (2001) 21:6405–12. doi: 10.1523/JNEUROSCI.21-16-06405.2001
148. Figueiro, MG, Wood, B, Plitnick, B, and Rea, MS. The impact of light from computer monitors on melatonin levels in college students. Neuro Endocrinol Lett. (2011) 32:158–63.
149. Lockley, SW, Brainard, GC, and Czeisler, CA. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab. (2003) 88:4502–5. doi: 10.1210/jc.2003-030570
150. Terman, M, and Terman, JS. Light therapy for seasonal and nonseasonal depression: efficacy, protocol, safety, and side effects. CNS Spectr. (2005) 10:647–63. doi: 10.1017/S1092852900019611
151. Gallin, PF, Terman, M, Reme, CE, Rafferty, B, Terman, JS, and Burde, RM. Ophthalmologic examination of patients with seasonal affective disorder, before and after bright light therapy. Am J Ophthalmol. (1995) 119:202–10. doi: 10.1016/S0002-9394(14)73874-7
152. Reme, CE, Rol, P, Grothmann, K, Kaase, H, and Terman, M. Bright light therapy in focus: lamp emission spectra and ocular safety. Technol Health Care. (1996) 4:403–13. doi: 10.3233/THC-1996-4405
153. Tuunainen, A, Kripke, DF, and Endo, T. Light therapy for non-seasonal depression. Cochrane Database Syst Rev. (2004) 2004:CD004050. doi: 10.1002/14651858.CD004050.pub2
155. Dauphinais, DR, Rosenthal, JZ, Terman, M, DiFebo, HM, Tuggle, C, and Rosenthal, NE. Controlled trial of safety and efficacy of bright light therapy vs. negative air ions in patients with bipolar depression. Psychiatry Res. (2012) 196:57–61. doi: 10.1016/j.psychres.2012.01.015
156. Auger, RR, Burgess, HJ, Emens, JS, Deriy, LV, Thomas, SM, and Sharkey, KM. Clinical practice guideline for the treatment of intrinsic circadian rhythm sleep-wake disorders: advanced sleep-wake phase disorder (ASWPD), delayed sleep-wake phase disorder (DSWPD), Non-24-hour sleep-wake rhythm disorder (N24SWD), and irregular sleep-wake rhythm disorder (ISWRD). An update for 2015: an American Academy of sleep medicine clinical practice guideline. J Clin Sleep Med. (2015) 11:1199–236. doi: 10.5664/jcsm.5100
157. Lewy, AJ, Ahmed, S, Jackson, JM, and Sack, RL. Melatonin shifts human circadian rhythms according to a phase-response curve. Chronobiol Int. (1992) 9:380–92. doi: 10.3109/07420529209064550
158. Mundey, K, Benloucif, S, Harsanyi, K, Dubocovich, ML, and Zee, PC. Phase-dependent treatment of delayed sleep phase syndrome with melatonin. Sleep. (2005) 28:1271–8. doi: 10.1093/sleep/28.10.1271
159. Kayumov, L, Brown, G, Jindal, R, Buttoo, K, and Shapiro, CM. A randomized, double-blind, placebo-controlled crossover study of the effect of exogenous melatonin on delayed sleep phase syndrome. Psychosom Med. (2001) 63:40–8. doi: 10.1097/00006842-200101000-00005
160. van Geijlswijk, IM, Korzilius, HP, and Smits, MG. The use of exogenous melatonin in delayed sleep phase disorder: a meta-analysis. Sleep. (2010) 33:1605–14. doi: 10.1093/sleep/33.12.1605
161. Rahman, SA, Kayumov, L, and Shapiro, CM. Antidepressant action of melatonin in the treatment of delayed sleep phase syndrome. Sleep Med. (2010) 11:131–6. doi: 10.1016/j.sleep.2009.07.013
162. Kamei, Y, Hayakawa, T, Urata, J, Uchiyama, M, Shibui, K, Kim, K, et al. Melatonin treatment for circadian rhythm sleep disorders. Psychiatry Clin Neurosci. (2000) 54:381–2. doi: 10.1046/j.1440-1819.2000.00724.x
163. Seabra, ML, Bignotto, M, Pinto, LR Jr, and Tufik, S. Randomized, double-blind clinical trial, controlled with placebo, of the toxicology of chronic melatonin treatment. J Pineal Res. (2000) 29:193–200. doi: 10.1034/j.1600-0633.2002.290401.x
164. Buscemi, N, Vandermeer, B, Hooton, N, Pandya, R, Tjosvold, L, Hartling, L, et al. The efficacy and safety of exogenous melatonin for primary sleep disorders. A meta-analysis. J Gen Intern Med. (2005) 20:1151–8. doi: 10.1111/j.1525-1497.2005.0243.x
165. Institute of Medicine (US) and National Research Council (US) Committee on the Framework for Evaluating the Safety of Dietary Supplements. Dietary Supplements: A Framework for Evaluating Safety. Washington (DC): National Academies Press (US) (2005).
166. Werneke, U, Turner, T, and Priebe, S. Complementary medicines in psychiatry: review of effectiveness and safety. Br J Psychiatry. (2006) 188:109–21. doi: 10.1192/bjp.188.2.109
167. Rubio-Sastre, P, Scheer, FA, Gomez-Abellan, P, Madrid, JA, and Garaulet, M. Acute melatonin administration in humans impairs glucose tolerance in both the morning and evening. Sleep. (2014) 37:1715–9. doi: 10.5665/sleep.4088
168. Hoebert, M, van der Heijden, KB, van Geijlswijk, IM, and Smits, MG. Long-term follow-up of melatonin treatment in children with ADHD and chronic sleep onset insomnia. J Pineal Res. (2009) 47:1–7. doi: 10.1111/j.1600-079X.2009.00681.x
169. Wasdell, MB, Jan, JE, Bomben, MM, Freeman, RD, Rietveld, WJ, Tai, J, et al. A randomized, placebo-controlled trial of controlled release melatonin treatment of delayed sleep phase syndrome and impaired sleep maintenance in children with neurodevelopmental disabilities. J Pineal Res. (2008) 44:57–64. doi: 10.1111/j.1600-079X.2007.00528.x
170. Carr, R, Wasdell, MB, Hamilton, D, Weiss, MD, Freeman, RD, Tai, J, et al. Long-term effectiveness outcome of melatonin therapy in children with treatment-resistant circadian rhythm sleep disorders. J Pineal Res. (2007) 43:351–9. doi: 10.1111/j.1600-079X.2007.00485.x
171. Valcavi, R, Zini, M, Maestroni, GJ, Conti, A, and Portioli, I. Melatonin stimulates growth hormone secretion through pathways other than the growth hormone-releasing hormone. Clin Endocrinol. (1993) 39:193–9. doi: 10.1111/j.1365-2265.1993.tb01773.x
172. Chowdhury, VS, Yamamoto, K, Saeki, I, Hasunuma, I, Shimura, T, and Tsutsui, K. Melatonin stimulates the release of growth hormone and prolactin by a possible induction of the expression of frog growth hormone-releasing peptide and its related peptide-2 in the amphibian hypothalamus. Endocrinology. (2008) 149:962–70. doi: 10.1210/en.2007-1427
173. Luboshitzky, R, Shen-Orr, Z, Nave, R, Lavi, S, and Lavie, P. Melatonin administration alters semen quality in healthy men. J Androl. (2002) 23:572–8.
174. van Geijlswijk, IM, Mol, RH, Egberts, TC, and Smits, MG. Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacology. (2011) 216:111–20. doi: 10.1007/s00213-011-2202-y
175. Zwart, TC, Smits, MG, Egberts, TCG, Rademaker, CMA, and van Geijlswijk, IM. Long-term melatonin therapy for adolescents and young adults with chronic sleep onset insomnia and late melatonin onset: evaluation of sleep quality, Chronotype, and lifestyle factors compared to age-related randomly selected population cohorts. Healthcare (Basel). (2018) 6:23. doi: 10.3390/healthcare6010023
176. Boafo, A, Greenham, S, Alenezi, S, Robillard, R, Pajer, K, Tavakoli, P, et al. Could long-term administration of melatonin to prepubertal children affect timing of puberty? A clinician's perspective. Nat Sci Sleep. (2019) 11:1–10. doi: 10.2147/NSS.S181365
177. Kato, K, Hirai, K, Nishiyama, K, Uchikawa, O, Fukatsu, K, Ohkawa, S, et al. Neurochemical properties of ramelteon (TAK-375), a selective MT1/MT2 receptor agonist. Neuropharmacology. (2005) 48:301–10. doi: 10.1016/j.neuropharm.2004.09.007
178. Dubocovich, ML. Melatonin receptors: role on sleep and circadian rhythm regulation. Sleep Med. (2007) 8:34–42. doi: 10.1016/j.sleep.2007.10.007
179. Williams, WP 3rd, McLin, DE 3rd, Dressman, MA, and Neubauer, DN. Comparative review of approved melatonin agonists for the treatment of circadian rhythm sleep-wake disorders. Pharmacotherapy. (2016) 36:1028–41. doi: 10.1002/phar.1822
180. Richardson, GS, Zee, PC, Wang-Weigand, S, Rodriguez, L, and Peng, X. Circadian phase-shifting effects of repeated ramelteon administration in healthy adults. J Clin Sleep Med. (2008) 04:456–61. doi: 10.5664/jcsm.27282
181. Takeshima, M, Shimizu, T, Ishikawa, H, and Kanbayashi, T. Ramelteon for delayed sleep-wake phase disorder: a case report. Clin Psychopharmacol Neurosci. (2020) 18:167–9. doi: 10.9758/cpn.2020.18.1.167
182. Shimura, A, Kanno, T, and Inoue, T. Ultra-low-dose early night ramelteon administration for the treatment of delayed sleep-wake phase disorder: case reports with a pharmacological review. J Clin Sleep Med. (2022) 18:2861–5. doi: 10.5664/jcsm.10188
183. Rajaratnam, SM, Polymeropoulos, MH, Fisher, DM, Roth, T, Scott, C, Birznieks, G, et al. Melatonin agonist tasimelteon (VEC-162) for transient insomnia after sleep-time shift: two randomised controlled multicentre trials. Lancet. (2009) 373:482–91. doi: 10.1016/S0140-6736(08)61812-7
184. Kim, HK, and Yang, KI. Melatonin and melatonergic drugs in sleep disorders. Transl Clin Pharmacol. (2022) 30:163–71. doi: 10.12793/tcp.2022.30.e21
185. Millan, MJ, Gobert, A, Lejeune, F, Dekeyne, A, Newman-Tancredi, A, Pasteau, V, et al. The novel melatonin agonist agomelatine (S20098) is an antagonist at 5-hydroxytryptamine2C receptors, blockade of which enhances the activity of frontocortical dopaminergic and adrenergic pathways. J Pharmacol Exp Ther. (2003) 306:954–64. doi: 10.1124/jpet.103.051797
186. Dahl, RE, Pelham, WE, and Wierson, M. The role of sleep disturbances in attention deficit disorder symptoms: a case study. J Pediatr Psychol. (1991) 16:229–39. doi: 10.1093/jpepsy/16.2.229
187. Weyerbrock, A, Timmer, J, Hohagen, F, Berger, M, and Bauer, J. Effects of light and chronotherapy on human circadian rhythms in delayed sleep phase syndrome: cytokines, cortisol, growth hormone, and the sleep-wake cycle. Biol Psychiatry. (1996) 40:794–7. doi: 10.1016/0006-3223(95)00661-3
188. Oren, DA, and Wehr, TA. Hypernyctohemeral syndrome after chronotherapy for delayed sleep phase syndrome. N Engl J Med. (1992) 327:1762. doi: 10.1056/NEJM199212103272417
189. Shapiro, DA, Renock, S, Arrington, E, Chiodo, LA, Liu, LX, Sibley, DR, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. (2003) 28:1400–11. doi: 10.1038/sj.npp.1300203
190. Takaki, M, and Ujike, H. Aripiprazole is effective for treatment of delayed sleep phase syndrome. Clin Neuropharmacol. (2014) 37:123–4. doi: 10.1097/WNF.0000000000000035
191. Omori, Y, Kanbayashi, T, Sagawa, Y, Imanishi, A, Tsutsui, K, Takahashi, Y, et al. Low dose of aripiprazole advanced sleep rhythm and reduced nocturnal sleep time in the patients with delayed sleep phase syndrome: an open-labeled clinical observation. Neuropsychiatr Dis Treat. (2018) 14:1281–6. doi: 10.2147/NDT.S158865
192. Marcus, RN, McQuade, RD, Carson, WH, Hennicken, D, Fava, M, Simon, JS, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a second multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. (2008) 28:156–65. doi: 10.1097/JCP.0b013e31816774f9
193. Coustals, N, Menard, ML, and Cohen, D. Aripiprazole in children and adolescents. J Child Adolesc Psychopharmacol. (2021) 31:4–32. doi: 10.1089/cap.2020.0014
194. Peixoto, CA, da Silva, AG, Carskadon, MA, and Louzada, FM. Adolescents living in homes without electric lighting have earlier sleep times. Behav Sleep Med. (2009) 7:73–80. doi: 10.1080/15402000902762311
195. Burgess, HJ, and Eastman, CI. A late wake time phase delays the human dim light melatonin rhythm. Neurosci Lett. (2006) 395:191–5. doi: 10.1016/j.neulet.2005.10.082
196. Auger, RR, Burgess, HJ, Dierkhising, RA, Sharma, RG, and Slocumb, NL. Light exposure among adolescents with delayed sleep phase disorder: a prospective cohort study. Chronobiol Int. (2011) 28:911–20. doi: 10.3109/07420528.2011.619906
Keywords: delayed sleep–wake phase disorder, DSWPD, circadian rhythm sleep–wake disorder, adolescent and young adult, circadian-entrained DSWPD
Citation: Futenma K, Takaesu Y, Komada Y, Shimura A, Okajima I, Matsui K, Tanioka K and Inoue Y (2023) Delayed sleep–wake phase disorder and its related sleep behaviors in the young generation. Front. Psychiatry 14:1174719. doi: 10.3389/fpsyt.2023.1174719
Edited by:
Athanasia Pataka, Aristotle University of Thessaloniki, GreeceReviewed by:
Kamalesh K. Gulia, Sree Chitra Tirunal Institute for Medical Sciences and Technology (SCTIMST), IndiaCopyright © 2023 Futenma, Takaesu, Komada, Shimura, Okajima, Matsui, Tanioka and Inoue. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuichi Inoue, aW5vdWVAc29tbm9sb2d5LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.