 Alireza Zangeneh1Nahid Khademi2Naser Farahmandmoghadam3*Arash Ziapour4Reyhane Naderlou5Somayyeh Shalchi Oghli6Raziyeh Teimouri7Komali Yenneti8Shahrzad Moghadam5
Alireza Zangeneh1Nahid Khademi2Naser Farahmandmoghadam3*Arash Ziapour4Reyhane Naderlou5Somayyeh Shalchi Oghli6Raziyeh Teimouri7Komali Yenneti8Shahrzad Moghadam5- 1Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran
- 2Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran
- 3Clinical Research Development Center, Imam Khomeini and Mohammad Kermanshahi Hospitals, Kermanshah University of Medical Sciences, Kermanshah, Iran
- 4Cardiovascular Research Center, Health Institute, Imam-Ali Hospital, Kermanshah University of Medical Sciences, Kermanshah, Iran
- 5Geography and Urban Planning, University of Zanjan, Zanjan, Iran
- 6Department of Health Education and Promotion, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
- 7UniSA Creative, University of South Australia, Adelaide, SA, Australia
- 8School of Architecture and the Built Environment, Faculty of Science and Engineering, University of Wolverhampton, Wolverhampton, United Kingdom
Background: A suicide attempt is a major societal problem because it imposes high costs on societies worldwide. This paper analyses the spatiotemporal clustering of suicide attempt in Kermanshah, Iran from 2006–14.
Methods: This study draws on 18,333 individuals (7,234 males and 11,097 females) who attempted suicide across the Kermanshah province. Data was collected from the records of individuals registered in hospitals across the Kermanshah province between 2006 and 2014. Mean Center, Standard Deviational Ellipse (SDE), Moran’s I and Kernel Density Estimation (KDE) in Arc/GIS10.6 software were used for the analysis of the spatial distribution of suicide attempt, while the chi-squared test in SPSS was used to examine the different demographic variables between groups within/outside spatial clusters of suicide.
Results: The results show that a total of 18,331 suicide attempts (39.46% male and 60.53% female) were reported between 2006 and 2014 in the Kermanshah province. The spatial pattern of suicide attempts was clustered in 16 clusters (6 high clusters and 10 low clusters) and statistically significant differences were found within and outside the hotspots of suicide attempts. Most hot spots were formed in and around cities. Younger people were at a greater risk. The rate of suicide attempts reduced in illiterate people and increased in people with university degrees. Unmarried people were associated with a higher risk of suicide attempt than was married status for both males and females.
Conclusion: The results of this study could help public health practitioners and policymakers in Iran prioritize resources and target efforts for suicide attempt prevention.
Introduction
Suicide attempts is a serious public health matter and is a leading cause of death across the world (1). Yearly, more than 703, 000 people attempt suicide. In 2019, suicide was the fourth leading cause of death in people aged 15–29, while more than 77% of suicides occurred in low- and middle-income countries (1, 2). Additionally, the number of suicide deaths among males in richer countries is three times that of females, while 1.5 males die by suicide per a woman in low- and middle-income countries (1).
In most countries, a suicide has many personal, family, and social impacts. For example, suicide attempts have strong emotional impact on not only the deceased’s friends and families, but also on the survivors themselves. It may include the medical costs and lost income for families, as well as the loss of employer’s productivity (3–5). In general, suicides impose huge social and economic costs to people, families, and society. In addition, suicide attempts have been a ripple effect that has had a major impact on our lives.
Suicide attempts are preventive. Many actions may be done to prevent suicide attempts at individual, community and national levels. Existing scholarship indicates that most people who attempt suicide have characteristics such as anxiety, aggression, and withdrawing from social interactions (6). Social withdrawal reflects individuals’ interactions and feelings of connectedness with the environment surrounding them which it has been linked to suicidal thoughts and/or behaviors (7). Major referrals to emergency departments in hospitals that are all voluntary, harmed themselves by different methods and motives (3, 8). However, suicidal behaviors are also influenced by different risk factors such as age, gender, ethnicity and socioeconomic conditions (9–12). For example, between 1991 and 2017 in the United States, black teenagers were the only population group with an increase in the rate of suicide attempts (12). Female teenagers have more non-fatal suicidal attempts than males (13), while teenagers from lower socio-economic backgrounds are at higher risk of suicide (14). In Canada, 10% of suicide related deaths occurred in the age group of 10 to 14 years, while 23% of deaths occurred in adolescents aged 15 to 19 (15). In New Zealand, the suicide attempts of children and adolescents from lower socioeconomic class are determined to be 31 times more likely than those of children and adolescents from higher socioeconomic status (16). In Asia, relationship issues, environmental problems and academic performance are common factors for suicide attempts in young people. In Singapore, most suicide attempts occur among teenagers and young people aged 15–24 (17). Self-harming behaviors like suicide amongst teenagers in Hong Kong (23.5%) were less compared with their peers in the United States (32%). The low rate of self-harm among young people in Hong Kong may be related to the differences between the Eastern and Western cultures, with strong family structures in Asian cultures (18). Suicide rate is also higher in Korea among the elderly and those over 65 years of age and is affected by economic conditions (19). Besides, marital status was related to various suicidal risk levels. All types of changes in marital status (widowed, divorced, married) are considered risk factors for suicidal attempts and suicidal behavior (20). The risk of suicide for divorced and widowed people depends on age: older people are at higher risk.
Research also shows high correlation between suicide attempts and residential environment and economic conditions (18, 21), but there is a little literature on the relation between suicides and community welfare. It is generally argued that the suicide rate is affected by the degree of urbanization, with the suicide the rate in rural areas being higher than that in urban areas (22, 23). In particular, the suicide rate among males in rural areas is higher than that of females (21, 24). However, the rate of suicide attempts in urban and rural areas has changed considerably in recent times (19), while most scholarship has been limited to just a few areas (23, 25). Existing literature also indicates a possibly very low relation between the specification of rural and urban areas and suicide rates at the national level (4, 26, 27).
Accident datasets reported in shape of tables or graphs are too involved to realize comprehensively (28). Indeed, it is essential to create an impressive spatial–temporal analyst methodology to explore the big accident datasets (29). Clustering is one of the most noteworthy unsupervised learning algorithms which has been widely used in determining hotspots (30). Wherein, events are grouped according to their strong similarity. There are four major types of clustering algorithms such as partitional, hierarchical, grid-based, and density-based clustering algorithms (31). Partitional algorithms contain k-means and k-medoids. This methodology requires predefined cluster numbers. Therefore, it is not used in many applicants. Hierarchical algorithms contain clustering using delegate and balanced iterative reducing and clustering using hierarchies, being effectual for summarizing and imagining data. Nevertheless, this methodology is difficult to scale up since each indecision needs to assess many events. Grid-based algorithms contain statistical information grid and clustering in quest. Partitioning and hierarchical algorithms are appropriate to recognize spherical-shaped clusters. Density-based algorithms contain Density-Based Spatial Clustering of Applications with Noise (DBSCAN), ordering points to recognize the clustering structure, and DBSCAN, being popular techniques for recognizing clusters of ideal shape. In density-based spatial clustering of applications with noise and ordering points to recognize the clustering structure, density is calculated by recounting the number of events in a surrounding area defined by a bandwidth. This is highly sensible to the bandwidth valuation applied. To deal with it, DBSCAN or KDE can be used, which is a non-parametric density estimator effective technique. The KDE methodology could efficiently reduce the effectiveness of noise by equally allocating noise into the input data (31, 32).
GIS algorithm, KDE could build a density scheme, which indicates the density of the points (33). DBSCAN, meanwhile, only recreates the form of the clusters and does not mention the density of the clusters. The density differentiation among clusters are not highlighted (34). Moreover, DBSCAN could not group well events with interchanged densities is the biggest drawback of this methodology (35). The great advantage of DBSCAN of applications is that it can identify clusters with arbitrary shapes (28). Moreover, differ from several clustering methodologies, KDE and DBSCAN do not require predefined cluster numbers (36).
Furthermore, suicide attempts also differ widely across geographical areas. Previous researches exploring differences in rural and urban suicide attempts rates observed higher rates of suicide attempts in rural regions, with rural–urban disparities increased (4, 37). Researches using spatial analysis techniques have been able to identify geographical area with high suicide attempts rates relative to other areas, also highlight region characteristics associated with elevated suicide attempts rates within specific geographic areas (4). A suicide attempts cluster might be defined as a higher number of suicides attempts occurring within a defined space and/or time than would otherwise be expected for a specific area (4). Other study revealed the spatial patterning of suicide attempts in Taiwan and found that the factors most strongly associated with region suicide attempts rates were median household income, population density, and single parent households (38). Another study in Quebec revealed that clusters of heightened suicide attempts risk were most likely to be showed in distant rural regions and in neighborhoods with higher proportions of immigrations and individuals living alone (39).
Notwithstanding, despite the burgeoning literature on suicide attempts across the world there is little scholarship that looks at both sex and age as potential factors affecting suicide rates (19) and cross-cultural perspectives of suicidal behavior, intentional self-harm, and non-suicidal self-injury of young people in a systematic way, especially in the developing world (40). Most of the literature on suicidal behaviors has been focused on Western and Asian developed countries (4, 15, 41, 42). Similarly, studies from Iran shows that the increase in suicide rate in the country is due to unfavorable economic conditions, such as unemployment, poverty and diseases (43–45). Although religion plays a vital role in mollifying suicidal attempts, it may dictate privacy and exacerbate the stigma of mental health and suicide among Arab societies (46).
As previous studies declaration, doing more research on suicide as an important social issue is required in developing countries (4). This research examined spatial patterns of suicide attempts over 8 years in an Iranian province. In this context, this study focuses on exploring the spatiotemporal clustering of suicide attempt in Kermanshah, Iran for the period of 2006–2014. Understanding the spatial distribution of suicide attempts can play an important role in predicting family and community socioeconomic situation and individual characteristics (4), and help in proper planning for prevention of suicide attempts (4). Following this introduction, the rest of the paper follows the structure: section 2 briefly describes the case study and outlines the research methodology adopted in this study. Section 3 presents the results and findings of this research. Finally, the paper ends with some discussion and conclusions.
Materials and methods
Study area
The Kermanshah with an area of 24,998 square kilometers located in a Zagros Mountain range west of Iran at latitude 34°19′N, longitude 47°7′E. According to the Census of Population and Housing in 2016, the population of Kermanshah was 1,952,434. This province consists of 14 townships, 30 districts, 29 cities, 85 hamlets, and 3,163 villages, and has 69.66% urban, and 30.15% rural population (47). Kermanshah has been facing several socioeconomic challenges including increased unemployment, poverty, cancer, and suicide, and inequality accessibility to healthcare centres among urban and rural areas (47, 48).
Study population
This study was conducted on 18,333 individuals (7,234 males and 11,097 females) attempted suicide in Kermanshah province, Iran. Data was collected from the records of individuals registered in hospitals across the Kermanshah province between 2006 and 2014. Furthermore, information about people who attempted suicide was collected through forms provided to by the Ministry of Health and completed by health personnel. The documents with information about the patient’s history were checked by medical records experts and sent to the Vice Chancellor of Kermanshah University of Medical Sciences. Information was also collected and archived confidentially. This study was approved by the ethics committee and institutional review board of the Medical Association of the Kermanshah University of Medical Science.
The patients’ records were systematically reviewed. The location data of all people who had attempted a suicide multiple times was recorded only once. Demographic data, including gender, age, marital status, and level of education (illiterate, primary education, the secondary education includes 7-9th grade, and high school includes 10-12th grade, University), was gathered and related to suicide attempts.
Methods
Spatial statistics refer to the use of statistical methodologies to analyze and describe the distributor of events, with a special emphasis on spatial data (49). Presently, there being considerable advancements in both technological and theoretic aspects of GIS science, which have greatly helped spatial statistics. Nevertheless, with the increasing use of spatial statistics in various fields, it plays an essential role in the interaction between methods, computational capabilities, and the distinct characterizations of each discipline (50). This study was pursued the procedures outlined in Figure 1.
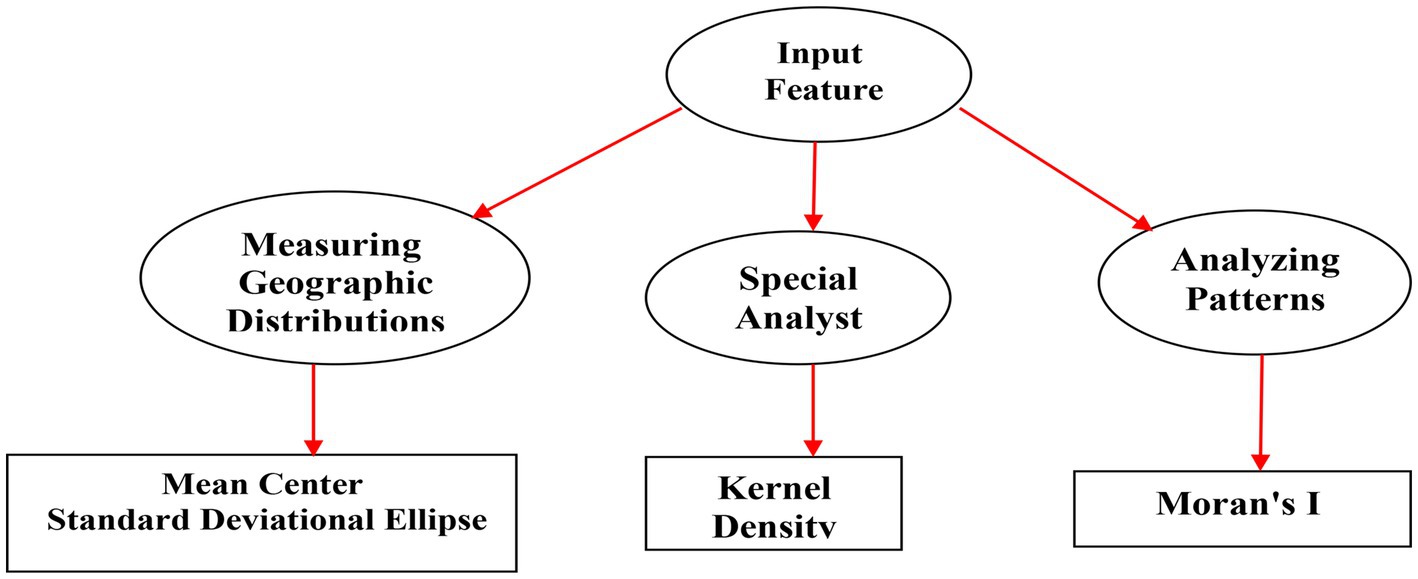
Figure 1. Schematic diagram of the workflow of the paper.
Participants’ data were collected from all hospital centers under the supervision of Kermanshah University of Medical Sciences and digitized using GIS with the collected information we run an Arc/Catalog environment. The tests used in GIS included: Mean Center, SDE, Moran’s I and KDE to identify spatial clusters Figure 1.
Mean Center was used for tracking changes in the distribution or for comparing the distributions of different types of suicide attempts. SDE was used to determine whether the distribution of suicide attempt has changed over time. The Moran’s I tool measures spatial autocorrelation of based on both feature locations and feature values simultaneously. Given a set of features and an associated attribute, it evaluates whether the pattern expressed is clustered, dispersed, or random. The tool calculates the Moran’s I Index value and both a z-score and value of p to evaluate the significance of that index. p-values are numerical approximations of the area under the curve for a known distribution, limited by the test statistic. The KDE tool calculated the density of suicide attempt in a neighborhood around those features.
In addition, the T-independent test was used to examine the different demographic variables between groups within and Outside Spatial Clusters of Suicide. The findings were examined at confidence level of 95% (p ≥ 0.05). Also, all data were analysed by the SPSS software package.
In this study, a suicide cluster is specified as an unusually high number of suicidal attempts occurring closer together in time and/or space than would be expected by odds (51). The Chi-square test was used to examine the correlations between the independent variables and dependent variable. The chi-square goodness of fit test was used to test whether there were statistical differences among different groups. The chi-squared test was used to examine the different demographic variables between groups within and outside spatial clusters of suicide attempts. The findings were examined at confidence level of 95% (p ≥ 0.05).
Results
The results show that there were 18, 331 suicide attempts, of which 39.46% were male and 60.53% were female, during the study period (2006–2014) in Kermanshah province. In terms of education level, most people who attempted suicide received secondary (29.08%) and high school (19.03%) education. The rate of suicide attempts in the illiterate decreased, while it increased in those with higher education (Table 1). Furthermore, 16,763 cases (91.48) were fatal. 39.46% of decedents were male and 60.53 were female (Table 2).
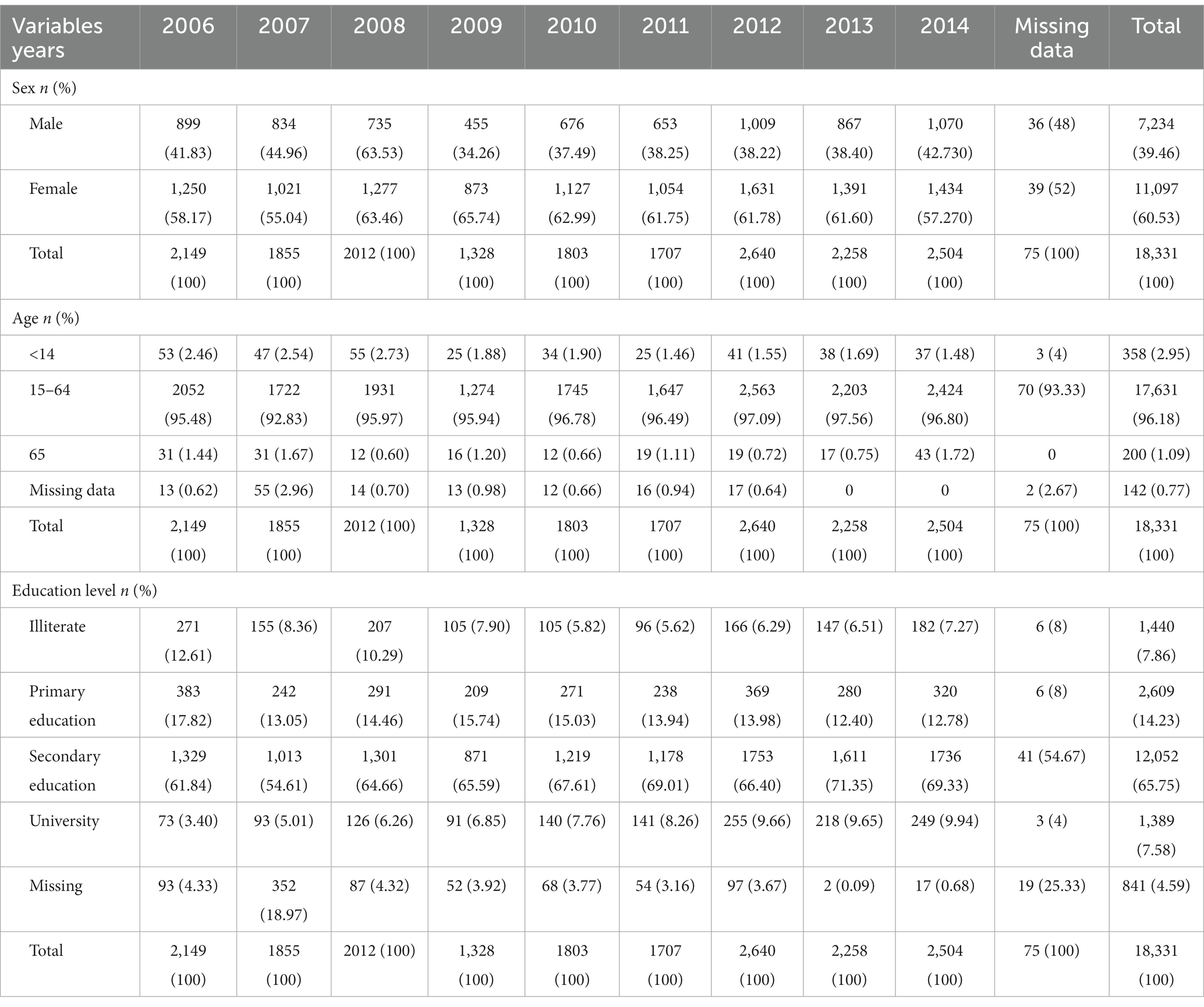
Table 1. Demographic characteristics of suicide attempt in the Kermanshah province during the period of 2006–2014.
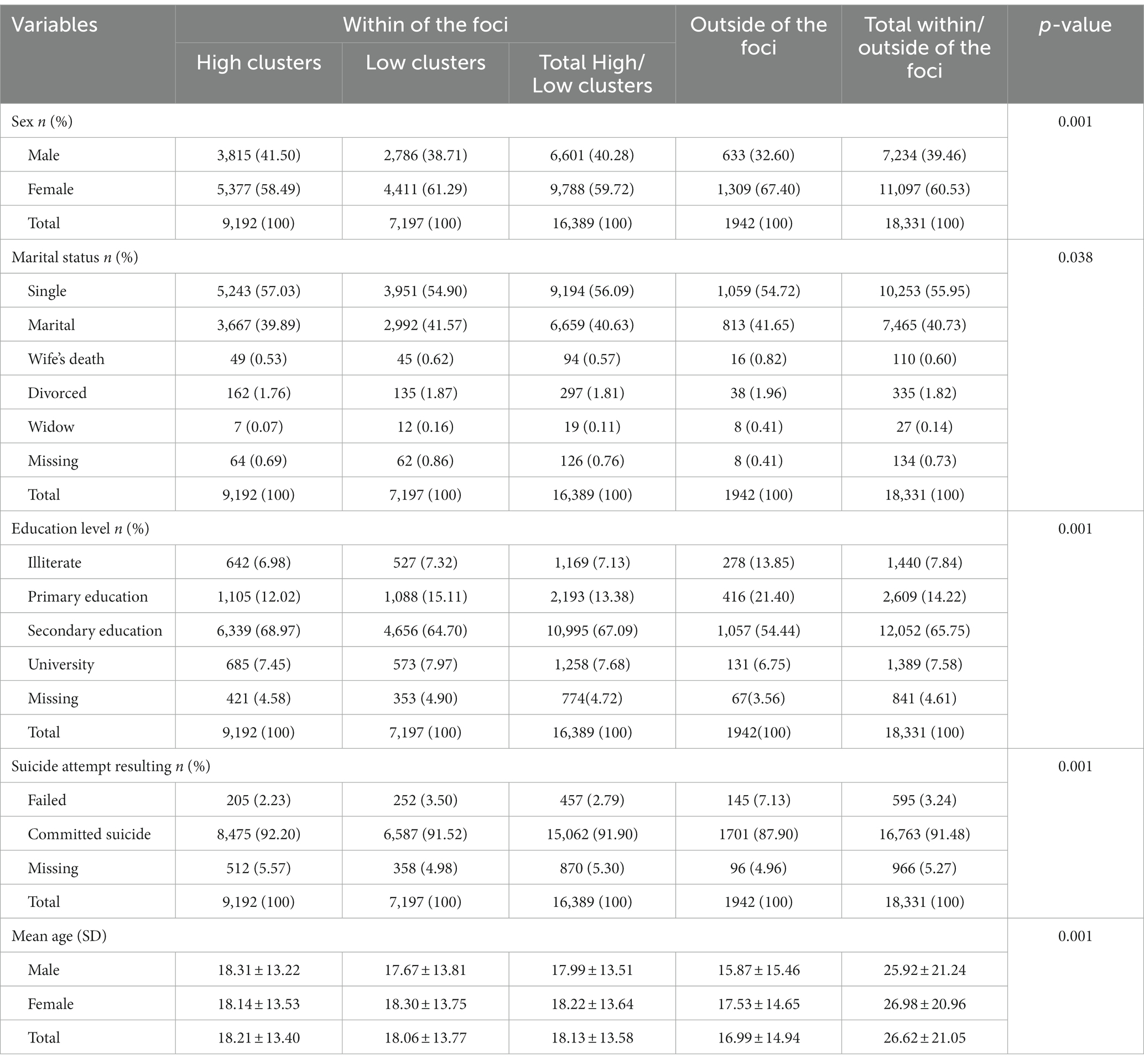
Table 2. Characteristics groups in within and outside of the foci of suicide attempt, Kermanshah Province, 2006–2014.
Figure 2 and Table 1 illustrate that during the study period (2006–14), the suicide attempt rate in females (60.53%) was higher than that in males (39.46%). During the waves, we find that the suicide attempt rate among females and males increased, especially females. Particularly, the suicide attempts in 2012 were higher than in other years. The rate of suicide attempts in males decreased in 2006, 2007, 2008, and 2009, and increased after 2010, while the rate of suicide attempt in females increased during 2006, 2008, 2010, 2012, and 2014. Also, we observed that the suicide attempts increased dramatically in aged 15–64 years. In addition, suicide attempts increased sharply in secondary education from 2006 to 2014.
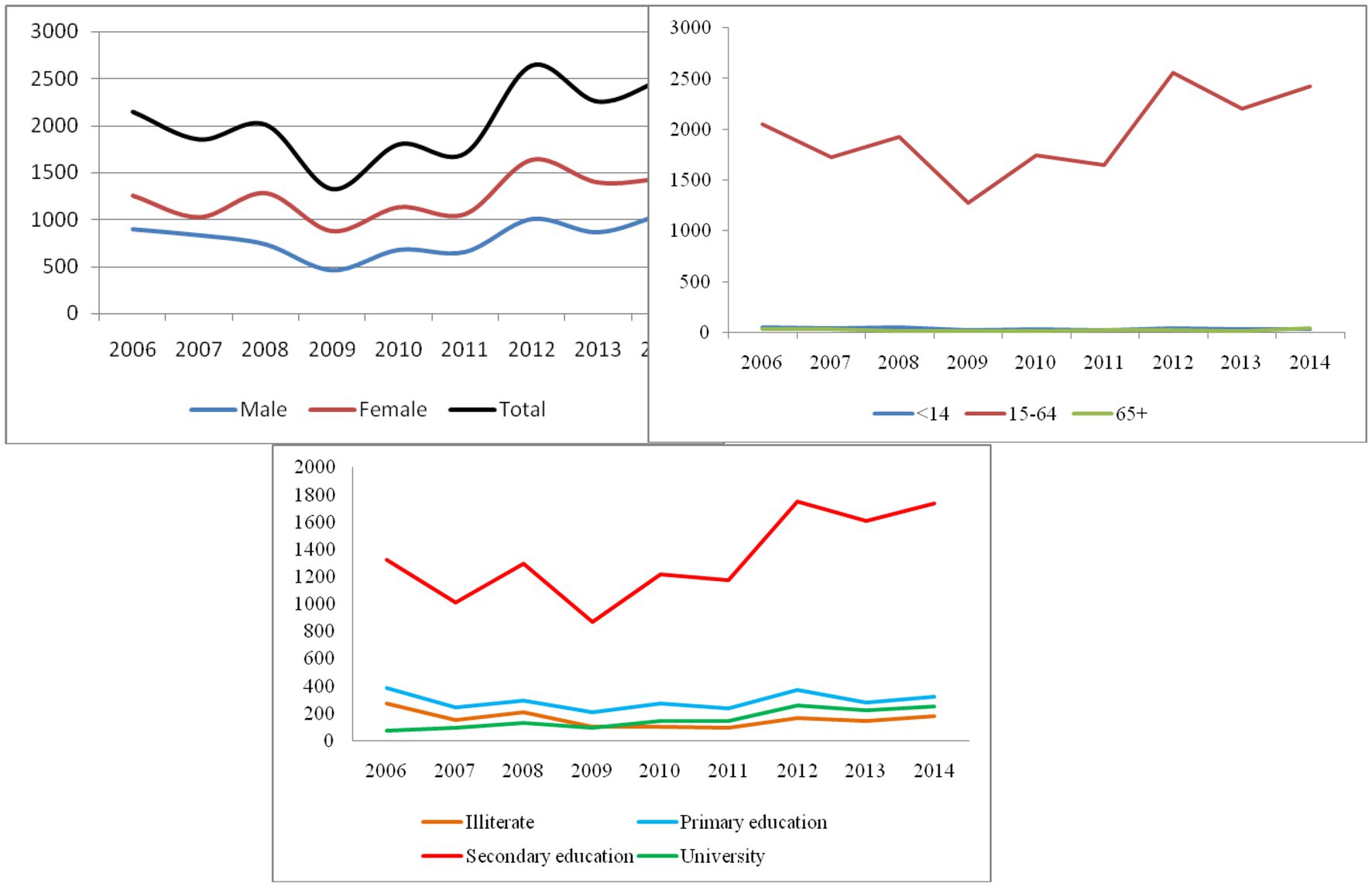
Figure 2. Trend suicide attempt based on gender, age groups, and education levels in Kermanshah province in years 2014–2006.
The results of the Moran’s I test show that the spatial pattern of suicide attempts in Kermanshah province took a cluster form during 2006–2014. In 2006, the Moran’s I was (Index = 0.09, z = 3.55, p = p < 0.001), but in 2014 the Moran’s I increased (Index = 0.18, z = 5.78, p = p < 0.001), indicating a greater increase in suicide attempt rates in suicide foci Figure 3. This result also indicates a high level of spatial dependence for suicides in Kermanshah province.
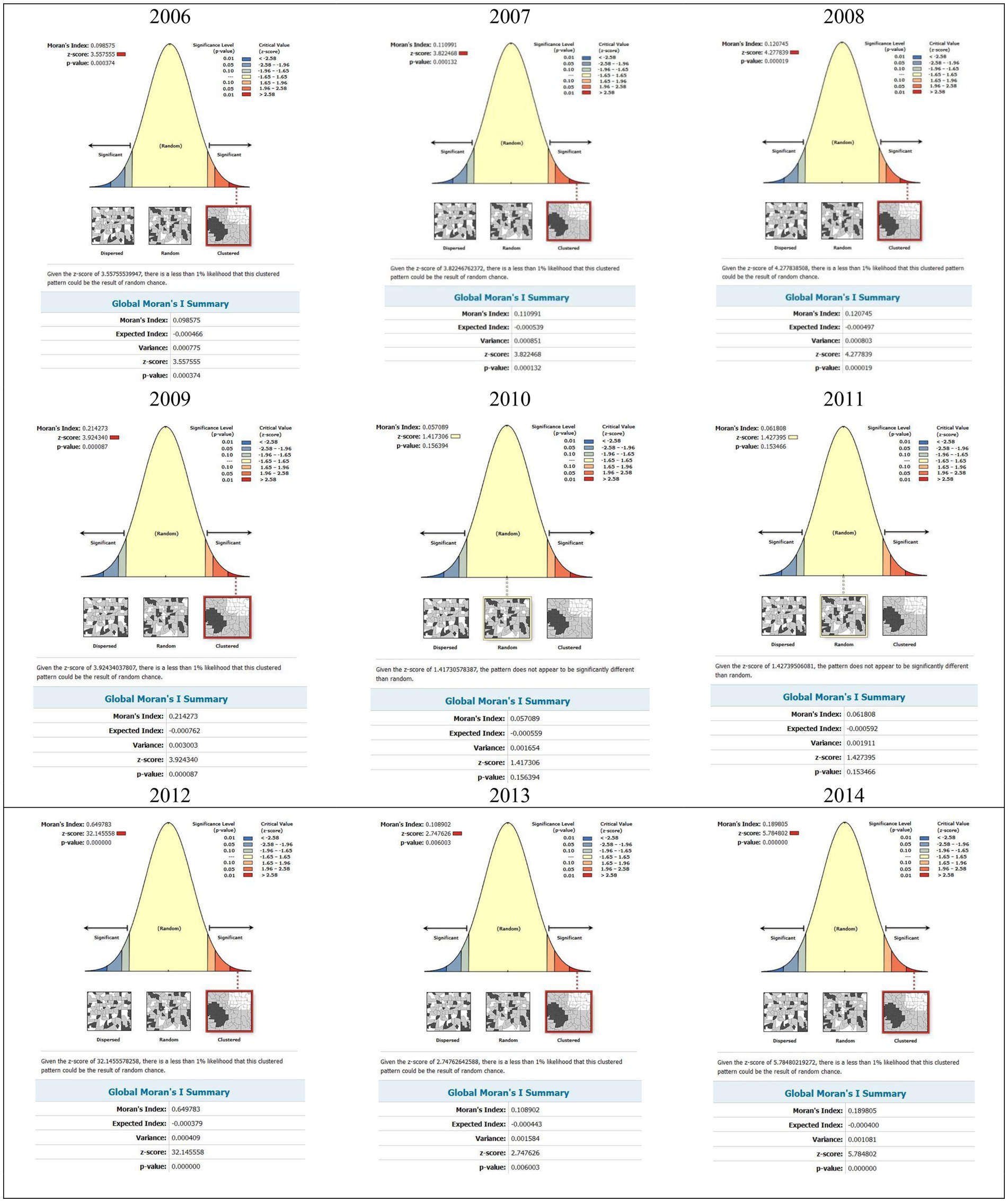
Figure 3. The Global Moran’s I statistic for suicides attempt in the Kermanshah Province, 2006–2014.
Figure 4 and Table 2 present the demographic characteristics of those who attempted suicide within and outside the foci. Accordingly, high clusters and low clusters were identified in Kermanshah province. There were 6 cases of high clusters and 10 cases of low clusters. The results show that suicide attempt in females were (inside foci = 59.72% and out of foci = 67.40%) and in males were (within foci = 40.28% and outside foci = 32.60%).
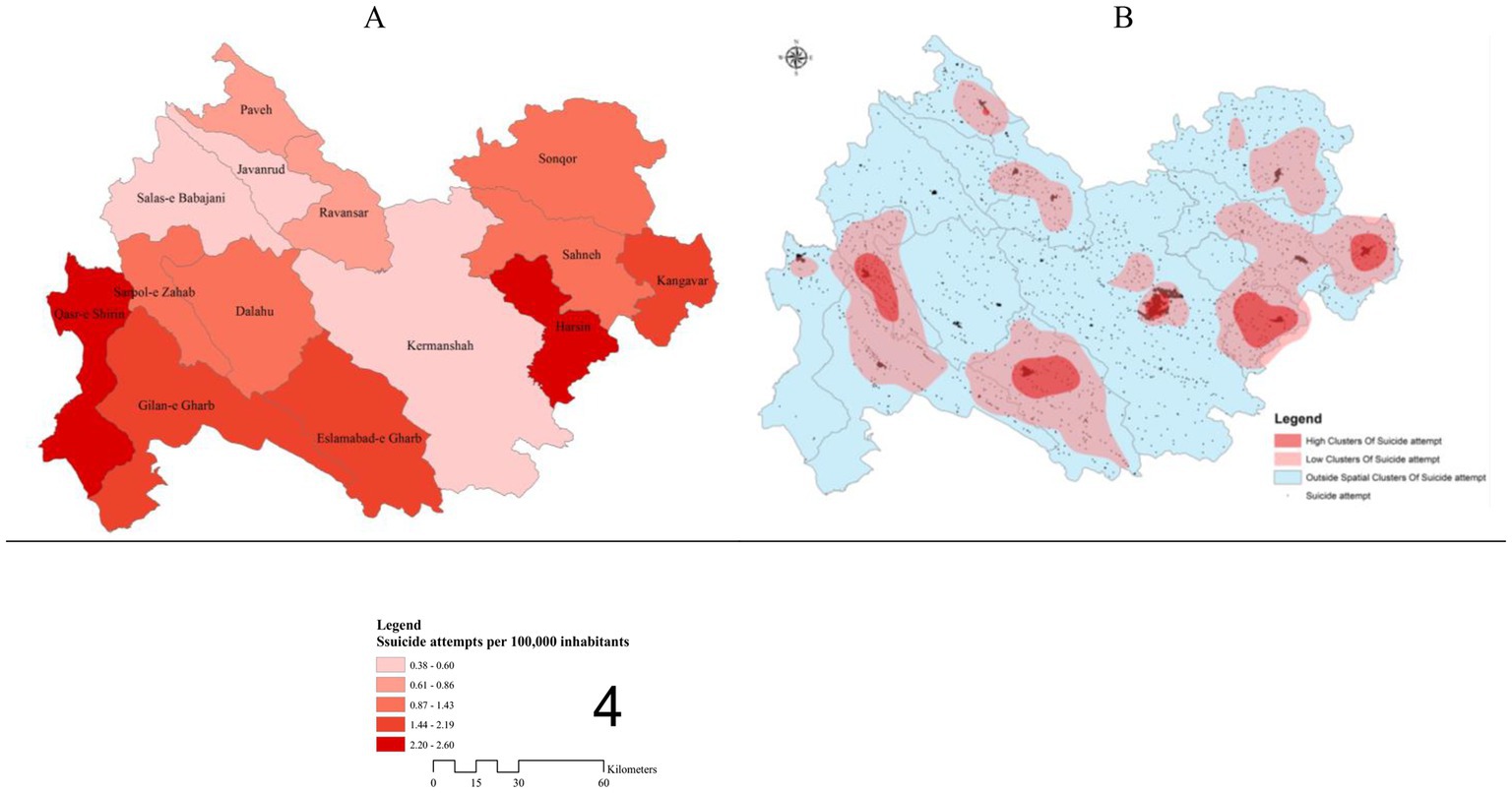
Figure 4. (A) Spatial analysis of resident suicide attempts per 100,000 inhabitants. (B) Hot spots using KDE in the Kermanshah province, 2006–2014.
A chi-square test of independence was performed to examine the relation between males and females (X2 (2, N = 18,331) =0.06, p < 0.001), between single, marital status, wife’s death, divorced, and widow (X2 (2, N = 18,331) =0.02, p < 0.048), between educational status (X2 (2, N = 18,331) =0.08, p < 0.001), and between mean age (X2 (2, N = 18,331) =0.11, p < 0.001) in within foci and out of foci, and the relation between all the variables was significant, respectively. In addition, the mean age in the foci (M = 18.13, SD = 13.58) was higher than that of outside the foci (M = 16.99, SD = 14.94).
The results reveal that during the study period (2006–2014), the mean center for suicide attempts appeared in Kermanshah city. Moreover, the standard deviation of suicide attempts in Kermanshah province shifted from Southwest-Northeast to West–East direction, covering the townships in the Western and Eastern parts of the province; these areas have the highest concentration in the province Figure 5.
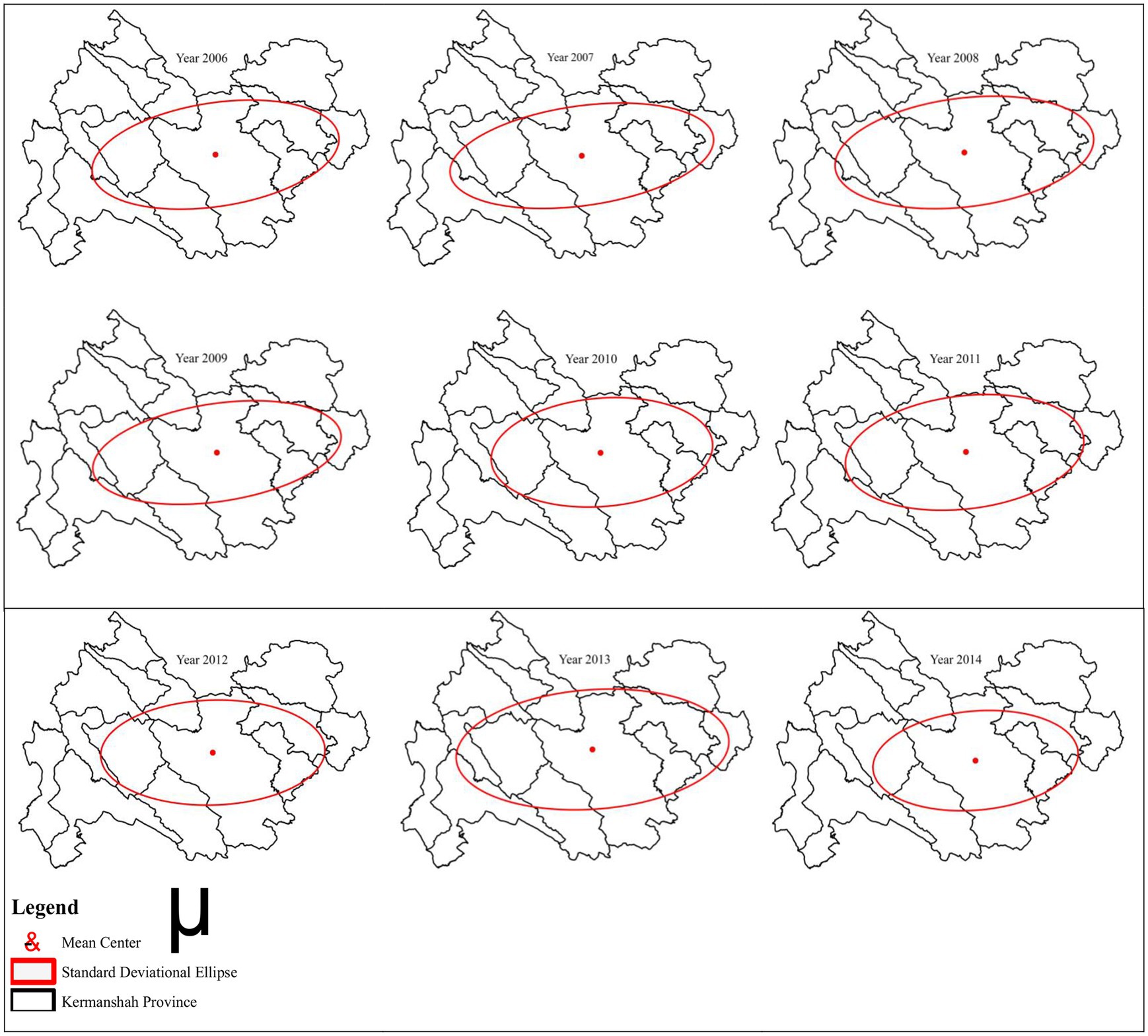
Figure 5. Mean center and SDE suicide attempt in the Kermanshah province during 2006–2014.
Discussion
Despite previous studies, this study can provide new insights into suicide in Iran. Due to the time of this study, study was not conducted in Iran. Our findings regarding the spatial trend of suicide attempt over a period of time (2006–2014) in the Kermanshah province showed that the center of suicide attempt was located in the Kermanshah city, and the SDE of suicide attempt has shifted from southwest-northeast to west–east with more focus on the Kermanshah city. This situation may have been affected by the increasing migration from other parts of the province to the Kermanshah city. In this regard, the results of studies have shown that poverty, unemployment, inadequate health, and environmental conditions, and also living in high-risk neighborhoods are among the problems faced by migrants (52). These are probably among the factors causing suicide in the Kermanshah province. On the other hand, the results of our study showed that the spatial distribution of suicide attempts in the Kermanshah province was in the clustered form Figure 2. These results were similar to the results of the studies of Fontanella et al. in Ohio, USA (4) as well as Torok et al. studies in Australia. The results of other studies indicate socioeconomic deprivation, low household income, low education, lack of social support have considered as effective factors for suicide cluster formation (53). Likely, the Kermanshah province has faced similar conditions. Therefore, it is suggested to investigate these issues in future studies.
Younger people were at greater risks than older people. Similar results were found in Australia (54). The suicide risk factors among older people are related to employment, depression, bereavement, feelings of social disconnectedness, social exclusion, cognitive impairment and inhibition, illnesses, psychological and physical pain, disability, and neurocognitive and psychological disorders (55, 56). The high suicide attempt rate of young people in Kermanshah may be related to a range of risk factors, such as psychological and economic crisis (unemployment), addiction to drugs as a result of poverty, inappropriate social and economic situation, behaviors, lifestyle, environmental exposure, lack of supervision and community control, weak community structures, and other inherited characteristics (54, 57, 58). A lower average age indicates that more planning is needed to protect and improve young people’s health, especially from a mental health perspective (42, 58). Future research should further investigate the reasons for the lower average age of suicide attempts in the Kermanshah province.
There was a meaningful difference between male and female suicide attempts (p < 0.05). Generally, within and outside the foci, females committed suicide more than males. The disparities in sex can be attributed to unequal socio-economic and cultural conditions in Iranian society. Females commit suicide because of inequality in social relationships, traditional societal attitudes toward females, patriarchal culture, forced marriage, polygamy, domestic violence, divorce, and restraints of females in the family (59, 60). In this regard, the result of studies in Kermanshah showed that the suicide rate in this province has been increasing which probably due to unfavorable economic conditions (36, 37, 41–43), as this province has been facing serious problems such as unemployment, poverty and diseases (38, 44–46).
A strong relation between education level and suicide attempts exists both within and outside the foci. Suicidal attempts among people with higher education within the foci were more than that outside the foci. Importantly, the rate of suicide attempts reduced in illiterate people and increased in people with university degrees. Lack of suitable jobs and unemployment may be some of the risk factors for suicide attempts among highly educated individuals (61). More specifically, high unemployment rates negatively affect the morale of educated people and increase suicide attempts (62). This finding is in contrast with existing research, which indicates that the rate of suicide attempt is connected to lower education (63). Low education is closely correlated with suicide attempts and suicidal ideation around the world (64, 65). People with lower education may be at greater risk of a suicide attempt due to insufficient coping skills (58).
The findings of this study show that marriage is associated with a higher risk of suicide attempts. Previous studies on the relation between marriage and suicide attempts have varied results–some argue that marriage and having a family reduces the probability of suicide attempts (59, 66), while others find that suicide attempts are more common in married people (67). In Denmark, at least one indecent of depression occurred in 1,606 male and 1,168 females suicide cases, most of whom were employed and married (68). Studies also argue that compared with unmarried people, married female s and males have a lower suicide risk, while the suicide rate is significantly higher among separated and divorced people than that of never married. These varying results could be due to different cultural patterns in different societies.
Limitations
This study has several limitations. First, missing data on residential addresses resulted in incomplete geo-coding; however, less than 4% of suicide cases were missing data on residential addresses. Second, the findings might not reflect current high-risk areas as data was from 2006–2014. Third, the socioeconomic factors such as poverty, unemployment, social support and the welfare system were not examined and warrant further research. We recommend that future studies consider them. Ultimately, however, we believe that our measure of spatiotemporal clustering of suicide attempt is an important step toward a richer understanding of suicide attempt in Iran. Due to no research was conducted in Iran to study the spatial distribution of suicide. Our study could be the based studies in future.
Conclusion
The results of this study show that the spatial pattern of suicide attempts in the Kermanshah were clustered and most hot spots of suicide were formed in and around cities. Clusters of high suicide attempt risk span the rural–urban continuum in Kermanshah province. Younger people compared to older people were at a greater risk. In addition, the rate of suicide attempts decreases in illiterate people and increases in people with university degrees. Being unmarried was associated with a greater risk, while marriage and having a family reduces the probability of a suicide attempt. The findings could help public health practitioners and policymakers prioritise resources and target efforts for suicide attempt prevention, particularly in Iran.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the ethics committee and institutional review board of the Medical Association of the Kermanshah University of Medical Science. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AZa, NK, NF, AZi, RN, SO, RT, KY, and SM were responsible for the study. AZa, NK, and AZi conceptualization and led the paper’s writing. AZa and KY conducted the Literature review and assisted in writing the paper. AZa and NF performed the analysis, assisted in interpreting the data, and writing the paper. RN, SO, SM, and RT assisted with the interpretation of the results and drafting programmatic Implications. AZa and AZi were responsible for the data collection and coordination of the study. AZa co-led the conceptualization, supervised all aspects of writing the paper, and provided extensive comments on the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The project received financial support from the Deputy Head of the Research & Technology Department of the Kermanshah University of Medical Sciences. The article processing cost is covered by the Kermanshah University of Medical Sciences, Kermanshah, Iran.
Acknowledgments
Support and assistance of our respected colleagues in the Kermanshah University of Medical Sciences, Iran, as well as the financial support of the Deputy Head of the Research & Technology Department of the Kermanshah University of Medical Sciences are acknowledged and greatly appreciated.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. Suicide; key facts (2018). Available at: https://www.who.int/en/news-room/fact-sheets/detail/suicide.
2. Shahnaz, A, Bagley, C, Simkhada, P, and Kadri, S. Suicidal behaviour in Bangladesh: a scoping literature review and a proposed public health prevention model. Open J Soc Sci. (2017) 05:254–82. doi: 10.4236/jss.2017.57016
3. Swahn, MH, Palmier, JB, Kasirye, R, and Yao, H. Correlates of suicide ideation and attempt among youth living in the slums of Kampala. Int J Environ Res Public Health. (2012) 9:596–609. doi: 10.3390/ijerph9020596
4. Fontanella, CA, Saman, DM, Campo, JV, Hiance-Steelesmith, DL, Bridge, JA, Sweeney, HA, et al. Mapping suicide mortality in Ohio: a spatial epidemiological analysis of suicide clusters and area level correlates. Prev Med. (2018) 106:177–84. doi: 10.1016/j.ypmed.2017.10.033
5. Phillips, J, Padfield, N, and Gelsthorpe, L. Suicide and community justice. Health Justice. (2018) 6:1–12. doi: 10.1186/s40352-018-0072-7
6. Hagen, J, Hjelmeland, H, Espeland, K, and Knizek, BL. Better care, fewer suicides? Tidsskrift for den Nor Laegeforen. (2018) 138:1–13. doi: 10.4045/tidsskr.17.1039
7. Park, JY, Rogers, ML, Bloch-Elkouby, S, Richards, JA, Lee, S, Galynker, I, et al. Factor structure and validation of the revised suicide crisis inventory in a Korean population. Psychiatry Investig. (2023) 20:162–73. doi: 10.30773/pi.2022.0208
8. Rozanov, VA, and Mid'ko, AA. Personality patterns of suicide attempters: gender differences in Ukraine. Spanish J Psycholol. (2011) 14:693–700. doi: 10.5209/rev_SJOP.2011.v14.n2.17
9. Xiao, Y, and Lindsey, MA. Adolescent social networks matter for suicidal trajectories: disparities across race/ethnicity, sex, sexual identity, and socioeconomic status. Psychol Med. (2022) 52:3677–88. doi: 10.1017/S0033291721000465
10. Baiden, P, Xiao, Y, Asiedua-Baiden, G, LaBrenz, CA, Boateng, GO, Graaf, G, et al. Sex differences in the association between sexual violence victimization and suicidal behaviors among adolescents. J Affect Disord Rep. (2020) 1:100011. doi: 10.1016/j.jadr.2020.100011
11. Xiao, Y, Romanelli, M, and Lindsey, MA. A latent class analysis of health lifestyles and suicidal behaviors among US adolescents. J Affect Disord. (2019) 255:116–26. doi: 10.1016/j.jad.2019.05.031
12. Lindsey, MA, Sheftall, AH, Xiao, Y, and Joe, S. Trends of suicidal behaviors among high school students in the United States: 1991–2017. Pediatrics. (2019) 144:22–30. doi: 10.1542/peds.2019-1187
13. Cha, CB, Franz, PJM, Guzmán, E, Glenn, CR, Kleiman, EM, and Nock, MK. Annual research review: suicide among youth–epidemiology, (potential) etiology, and treatment. J Child Psychol Psychiatry. (2018) 59:460–82. doi: 10.1111/jcpp.12831
14. Farrell, CT, Moledina, Z, and Katta, M. Suicidal thoughts in low-income adolescents: a longitudinal analysis. Int J Public Health. (2019) 64:285–92. doi: 10.1007/s00038-019-01201-8
15. Skinner, R, and McFaull, S. Suicide among children and adolescents in Canada: trends and sex differences, 1980–2008. CMAJ. (2012) 184:1029–34. doi: 10.1503/cmaj.111867
16. Beautrais, AL, Joyce, PR, and Mulder, RT. Youth suicide attempts: a social and demographic profile. Aust N Z J Psychiatry. (1998) 32:349–57. doi: 10.3109/00048679809065527
17. Choo, CC, Chew, PK, and Ho, RC. Suicide precipitants differ across the lifespan but are not significant in predicting medically severe attempts. Int J Environ Res Public Health. (2018) 15:691. doi: 10.3390/ijerph15040691
18. Law, B, and Shek, D. Self-harm and suicide attempts among young Chinese adolescents in Hong Kong: prevalence, correlates, and changes. J Pediatr Adolesc Gynecol. (2013) 26:S26–32. doi: 10.1016/j.jpag.2013.03.012
19. Cheong, K-S, Choi, M-H, Cho, B-M, Yoon, T-H, Kim, C-H, Kim, Y-M, et al. Suicide rate differences by sex, age, and urbanicity, and related regional factors in Korea. J Prev Med Public Health. (2012) 45:70–7. doi: 10.3961/jpmph.2012.45.2.70
20. Roškar, S, Podlesek, A, Kuzmanić, M, Demšar, LO, Zaletel, M, and Marušič, A. Suicide risk and its relationship to change in marital status. Crisis. (2011) 32:24–30. doi: 10.1027/0227-5910/a000054
21. Hendin, H, World Health Organization WH. Suicide and suicide prevention in Asia: World Health Organization; (2008).
22. Park, Y-J, Kim, M-h, Kown, S-M, and Shin, Y-j. The association between public social expenditure and suicides: evidence from OECD countries. J Prev Med Public Health. (2009) 42:123–9. doi: 10.3961/jpmph.2009.42.2.123
23. Ryu, J-K. Regional differentials in elderly suicide rate: the focusing on effects of family instability, 1995-2005. Korea J Popul Stud. (2008) 31:21–44.
24. Park, J-Y, Chae, Y-M, Jung, S-H, and Moon, K-T. Effect of sociodemographic factors, cancer, psychiatric disorder on suicide: gender and age-specific patterns. J Prev Med Public Health. (2008) 41:51–60. doi: 10.3961/jpmph.2008.41.1.51
25. Razvodovsky, Y, and Stickley, A. Suicide in urban and rural regions of Belarus, 1990–2005. Public Health. (2009) 123:27–31. doi: 10.1016/j.puhe.2008.10.003
26. Torok, M, Konings, P, Batterham, PJ, and Christensen, H. Spatial clustering of fatal, and non-fatal, suicide in new South Wales, Australia: implications for evidence-based prevention. BMC Psychiatry. (2017) 17:339. doi: 10.1186/s12888-017-1504-y
27. Loureiro, A, Almendra, R, Costa, C, and Santana, P. Mortality from suicide in the municipalities of mainland Portugal: Spatio-temporal evolution between 1980 and 2015. Acta Med Port. (2018) 31:38–44. doi: 10.20344/amp.9423
28. Shi, Z, and Pun-Cheng, LS. Spatiotemporal data clustering: a survey of methods. ISPRS Int J Geo-Inf. (2019) 8:112. doi: 10.3390/ijgi8030112
29. Shekhar, S, Evans, MR, Kang, JM, and Mohan, P. Identifying patterns in spatial information: a survey of methods. Wiley Interdiscip Rev: Data Min Knowl Discov. (2011) 1:193–214. doi: 10.1002/widm.25
30. Kamber, HJM In: J Pei, editor. Data mining: Concepts and techniques: concepts and techniques. 3rd ed. Amsterdam, Netherlands: Elsevier (2011)
31. Han, J, Kamber, M, and Pei, J. Data mining concepts and techniques, Morgan Kaufmann Publishers, San Francisco, CA. (2001):335–391.
32. Le, KG, Liu, P, and Lin, L-T. Determining the road traffic accident hotspots using GIS-based temporal-spatial statistical analytic techniques in Hanoi, Vietnam. Geo-spatial Inform Sci. (2020) 23:153–64. doi: 10.1080/10095020.2019.1683437
33. Mohaymany, AS, Shahri, M, and Mirbagheri, B. GIS-based method for detecting high-crash-risk road segments using network kernel density estimation. Geo-spatial Inform Sci. (2013) 16:113–9. doi: 10.1080/10095020.2013.766396
34. Hegyi, P, Borsos, A, and Koren, C. Searching possible accident black spot locations with accident analysis and GIS software based on GPS coordinates. Pollack Period. (2017) 12:129–40. doi: 10.1556/606.2017.12.3.12
35. Bhattacharjee, P, and Mitra, P. A survey of density based clustering algorithms. Front Comput Sci. (2021) 15:1–27.
36. Zhou, A, Zhou, S, Cao, J, Fan, Y, and Hu, Y. Approaches for scaling DBSCAN algorithm to large spatial databases. J Computer Sci Technol. (2000) 15:509–26. doi: 10.1007/BF02948834
37. Fontanella, CA, Hiance-Steelesmith, DL, Phillips, GS, Bridge, JA, Lester, N, Sweeney, HA, et al. Widening rural-urban disparities in youth suicides, United States, 1996-20. JAMA Pediatr. (2015) 169:466–73. doi: 10.1001/jamapediatrics.2014.3561
38. Chang, S-S, Sterne, JA, Wheeler, BW, Lu, T-H, Lin, J-J, and Gunnell, D. Geography of suicide in Taiwan: spatial patterning and socioeconomic correlates. Health Place. (2011) 17:641–50. doi: 10.1016/j.healthplace.2011.01.003
39. Ngui, AN, Apparicio, P, Moltchanova, E, and Vasiliadis, H-M. Spatial analysis of suicide mortality in Québec: spatial clustering and area factor correlates. Psychiatry Res. (2014) 220:20–30. doi: 10.1016/j.psychres.2014.07.033
40. Lim, K-S, Wong, CH, McIntyre, RS, Wang, J, Zhang, Z, Tran, BX, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. (2019) 16:4581. doi: 10.3390/ijerph16224581
41. Phillips, JA, and Hempstead, K. Differences in US suicide rates by educational attainment, 2000–2014. Am J Prev Med. (2017) 53:E123–e130. doi: 10.1016/j.amepre.2017.04.010
42. Batty, GD, Jung, KJ, Lee, S, Back, JH, and Jee, SH. Systemic inflammation and suicide risk: cohort study of 419 527 Korean men and women. J Epidemiol Community Health. (2018) 72:572–4. doi: 10.1136/jech-2017-210086
43. Shojaei, A, and Hashemi Nazari, SS. Suicide mortality trends in four provinces of Iran with the highest mortality, from 2006-2016. J Res Health Sci. (2017) 17:e00382
44. Reshadat, S, Tohidi, M, Ghasemi, M, Zangeneh, A, Saeidi, S, Teimouri, R, et al. Interrelationship between underprivileged neighborhoods and health promotion lifestyles: insights from Kermanshah, Iran. J Public Health. (2019) 28:693–702. doi: 10.1007/s10389-019-01086-0
45. Khademi, N, Reshadat, S, Zangeneh, A, Saeidi, S, Ghasemi, S, Rajabi-Gilan, N, et al. A comparative study of the spatial distribution of HIV prevalence in the metropolis of Kermanshah, Iran, in 1996− 2014 using geographical information systems. HIV Med. (2017) 18:220–4. doi: 10.1111/hiv.12416
46. El Halabi, S, El Hayek, R, Kahil, K, Nofal, M, and El Hayek, S. Characteristics of attempted suicide in the Middle East and North Africa region: the mediating role of Arab culture and religion. Mediterr J Emerg Med Acute Care. (2020) 1:1–11.
47. Zangeneh, A, Yenneti, K, Teimouri, R, Saeidi, S, Najafi, F, Shakiba, E, et al. The spatiality of COVID-19 in Kermanshah Metropolis, Iran. Urban Sci. (2022) 6:30. doi: 10.3390/urbansci6020030
48. Reshadat, S, Zangeneh, A, Saeidi, S, Teimouri, R, and Yigitcanlar, T. Measures of spatial accessibility to health centers: investigating urban and rural disparities in Kermanshah. Iran J Public Health. (2019) 27:519–29. doi: 10.1007/s10389-018-0966-9
49. Getis, A, and Ord, JK. The analysis of spatial association by use of distance statistics. Geogr Anal. (1992) 24:189–206. doi: 10.1111/j.1538-4632.1992.tb00261.x
50. Güneyli, H, and Ahmed, SMS. Detecting abnormal seismic activity areas of Anatolian plate and deformation directions using Python geospatial libraries. Heliyon. (2023) 9:e14394. doi: 10.1016/j.heliyon.2023.e14394
51. Too, L, Pirkis, J, Milner, A, and Spittal, M. Clusters of suicides and suicide attempts: detection, proximity and correlates. Epidemiol Psychiatr Sci. (2017) 26:491–500. doi: 10.1017/S2045796016000391
52. Rahimi, H, Kalantari, A, Rafiee, N, and Khosravi, S. Social trends affecting the future of Iran's health system: a qualitative study using focus group discussion. Int J Prev Med. (2019) 10:115. doi: 10.4103/ijpvm.IJPVM_322_18
53. Lin, C-Y, Hsu, C-Y, Gunnell, D, Chen, Y-Y, and Chang, S-S. Spatial patterning, correlates, and inequality in suicide across 432 neighborhoods in Taipei City,Taiwan. Soc Sci Med. (2019) 222:20–34. doi: 10.1016/j.socscimed.2018.12.011
54. Bastiampillai, T, Looi, JC, Kisely, SR, and Allison, S. Commentary on Jorm and Kitchener 2020: rising Australian youth suicide rates despite headspace and better access. Aust N Z J Psychiatry. (2021) 55:628–30. doi: 10.1177/00048674211009614
55. Beghi, M, Butera, E, Cerri, CG, Cornaggia, CM, Febbo, F, Mollica, A, et al. Suicidal behaviour in older age: a systematic review of risk factors associated to suicide attempts and completed suicides. Neurosci Biobehav Rev. (2021) 127:193–211. doi: 10.1016/j.neubiorev.2021.04.011
56. Conejero, I, Olié, E, Courtet, P, and Calati, R. Suicide in older adults: current perspectives. Clin Interv Aging. (2018) 13:691–9. doi: 10.2147/CIA.S130670
57. Kõlves, K. Child suicide, family environment, and economic crisis. Queensland, Australia: Hogrefe Publishing (2010).
58. Bazrafshan, MR, Sharif, F, Molazem, Z, and Mani, A. Cultural concepts and themes of suicidal attempt among Iranian adolescents. Int J High Risk Behav Addict. (2015) 4:e22589. doi: 10.5812/ijhrba.22589
59. Azizpour, Y, Sayehmiri, K, Asadollahi, K, Kaikhavani, S, and Bagheri, M. Epidemiological study of suicide by physical methods between 1993 and 2013 in Ilam province, Iran. BMC Psychiatry. (2017) 17:304. doi: 10.1186/s12888-017-1461-5
60. Ziapour, A, Chirico, F, Nucera, G, Soltanipour, S, Moradgholi, A, Lebni, JY, et al. Suicide attempts, suicide and their association with socio-demographic variables in Iran: A retrospective, registry-based, cohort study (2016–2021). Disaster Emerg Med J. : IEEE (2023) 8:27–32.
61. Mohammadinia, N, Rezaei, M, Sameizadehtoosi, T, and Darban, F. Assessing suicidal ideation frequency in medical students. Q J Nurs Manag. (2012) 1:83–91.
62. Bakhtar, M, and Rezaeian, M. The prevalence of suicide thoughts and attempted suicide plus their risk factors among Iranian students: a systematic review study. J Rafsanjan Univ Med Sci. (2017) 15:1061–76.
63. Wiebenga, JX, Eikelenboom, M, Heering, HD, van Oppen, P, and Penninx, BW. Suicide ideation versus suicide attempt: examining overlapping and differential determinants in a large cohort of patients with depression and/or anxiety. Aust N Z J Psychiatry. (2021) 55:167–79. doi: 10.1177/0004867420951256
64. Nock, MK, Borges, G, Bromet, EJ, Alonso, J, Angermeyer, M, Beautrais, A, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. (2008) 192:98–105. doi: 10.1192/bjp.bp.107.040113
65. May, AM, and Klonsky, ED. What distinguishes suicide attempters from suicide ideators? A meta-analysis of potential factors. Clin Psycholo: Sci Pract. (2016) 23:5.
66. Hill, J, and Viner-Brown, S. Suicide deaths among Rhode Island adults aged 25 years and older: an epidemiologic and spatial analysis. R I Med J. (2017) 100:37.
67. Afghah, S, Aghahasani, M, Noori-Khajavi, M, and Tavakoli, E. Survey of suicide attempts in sari. Iran J Psychiatry. (2014) 9:89–95.
Keywords: suicide attempts, spatial pattern of suicide, spatial analysis, geographic information system, Kermanshah, Iran
Citation: Zangeneh A, Khademi N, Farahmandmoghadam N, Ziapour A, Naderlou R, Oghli SS, Teimouri R, Yenneti K and Moghadam S (2023) Spatiotemporal clustering of suicide attempt in Kermanshah, West-Iran. Front. Psychiatry. 14:1174071. doi: 10.3389/fpsyt.2023.1174071
Edited by:
Xenia Gonda, Semmelweis University, Budapest, HungaryReviewed by:
Fatemeh Mohamadkhah, Babol University of Medical Sciences, IranFakhreddin Chaboksavar, Babol University of Medical Sciences, Iran
Roya Malekzadeh, Mazandaran University of Medical Sciences, Iran
Copyright © 2023 Zangeneh, Khademi, Farahmandmoghadam, Ziapour, Naderlou, Oghli, Teimouri, Yenneti and Moghadam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Naser Farahmandmoghadam, naser8620@yahoo.com