
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 16 June 2023
Sec. Psychopathology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1161097
 Bernd R. Förstner1*
Bernd R. Förstner1* Sarah Jane Böttger1
Sarah Jane Böttger1 Alexander Moldavski2
Alexander Moldavski2 Malek Bajbouj3
Malek Bajbouj3 Andrea Pfennig4
Andrea Pfennig4 André Manook5
André Manook5 Marcus Ising6Andre Pittig7,8Ingmar Heinig7
Marcus Ising6Andre Pittig7,8Ingmar Heinig7 Andreas Heinz9
Andreas Heinz9 Klaus Mathiak10,11
Klaus Mathiak10,11 Thomas G. Schulze12,13,14Frank Schneider10,15
Thomas G. Schulze12,13,14Frank Schneider10,15 Inge Kamp-Becker16Andreas Meyer-Lindenberg2
Inge Kamp-Becker16Andreas Meyer-Lindenberg2 Frank Padberg17
Frank Padberg17 Tobias Banaschewski18Michael Bauer4
Tobias Banaschewski18Michael Bauer4 Rainer Rupprecht5Hans-Ulrich Wittchen7,17
Rainer Rupprecht5Hans-Ulrich Wittchen7,17 Michael A. Rapp1
Michael A. Rapp1 Mira Tschorn1
Mira Tschorn1Background: Anxiety and depressive disorders share common features of mood dysfunctions. This has stimulated interest in transdiagnostic dimensional research as proposed by the Research Domain Criteria (RDoC) approach by the National Institute of Mental Health (NIMH) aiming to improve the understanding of underlying disease mechanisms. The purpose of this study was to investigate the processing of RDoC domains in relation to disease severity in order to identify latent disorder-specific as well as transdiagnostic indicators of disease severity in patients with anxiety and depressive disorders.
Methods: Within the German research network for mental disorders, 895 participants (n = 476 female, n = 602 anxiety disorder, n = 257 depressive disorder) were recruited for the Phenotypic, Diagnostic and Clinical Domain Assessment Network Germany (PD-CAN) and included in this cross-sectional study. We performed incremental regression models to investigate the association of four RDoC domains on disease severity in patients with affective disorders: Positive (PVS) and Negative Valance System (NVS), Cognitive Systems (CS) and Social Processes (SP).
Results: The results confirmed a transdiagnostic relationship for all four domains, as we found significant main effects on disease severity within domain-specific models (PVS: β = −0.35; NVS: β = 0.39; CS: β = −0.12; SP: β = −0.32). We also found three significant interaction effects with main diagnosis showing a disease-specific association.
Limitations: The cross-sectional study design prevents causal conclusions. Further limitations include possible outliers and heteroskedasticity in all regression models which we appropriately controlled for.
Conclusion: Our key results show that symptom burden in anxiety and depressive disorders is associated with latent RDoC indicators in transdiagnostic and disease-specific ways.
Major depressive (MDD), as well as anxiety disorders (AD) may be characterized by altered emotional processes expressed upwards from neural circuitry to clinically relevant variations of symptomatology. On symptom level, MDD and AD share common features of aberrations of mood and emotions. On the one hand, high negative affect is present in both types of disorders, with depressed mood/anhedonia as well as anxious mood associated with both MDD and AD. On the other hand, anxious hyperarousal and persistent fear, anxiety or avoidance of perceived threats are considered general characteristics of AD, whereas low positive affect is relatively specific to MDD and only to certain distress-related types of AD, such as social anxiety disorder (SAD) or generalized anxiety disorder (GAD) (1–3). Furthermore, symptoms of anhedonia, meaning the loss of pleasure or interest in previously rewarding activities, are strongly tied to MDD. There is also an association of cognitive dysfunction for both disorders, while this association is more heterogenous for AD due to its broad disease spectrum (4). Existing literature also shows heterogeneous associations with respect to social processes. For example, the construct of affiliation and attachment has been associated with MDD and SAD, whereas the construct of understanding of self and others has been associated with GAD (5).
Common features in symptomatology and common neurobiological mechanisms in depressive and anxiety disorders can be considered partly responsible for limitations in diagnostic specificity, which is necessary to develop precise treatments (precision medicine) that can improve the stagnant treatment of mental illness.
The Research Domain Criteria (RDoC) approach promoted by the National Institute of Mental Health (NIMH) aims to address these issues and guide research toward a better understanding of mental disorders and their underlying psychological, neural and biological mechanisms, ultimately leading to improved treatments. The RDoC approach views mental disorders as syndromes at multiple levels, also connected to disrupted or dysfunctional brain circuitry (6, 7). To gain a better understanding of the links between disease-specific symptomatology and the underlying neural mechanisms of emotional (dys) function, the latent RDoC domains Positive (PVS) and Negative Valance System (NVS), Cognitive Systems (CS) and Social Processes (SP) were established and proved to be valid research constructs (8–12).
The PVS domain includes mechanisms involved in responses to attractive stimuli, such as responding to reward, as well as learning and valuation of rewards as parts of the reward system. In contrast, the NVS domain comprises responses to aversive stimuli of acute, potential, and sustained threat, loss, or aggression due to frustration. The CS domain comprises of circuits generating attentional processes, perception, memory functioning, language processing and cognitive control. The SP domain contains concepts of affiliation and attachment, social communication, as well as perception and understanding of self and others (13). In our previous research, we identified four distinct domains (PVS, NVS, CS, SP) in a latent structure of four overlapping factors (12).
There is limited research on PVS functioning within the spectrum of anxiety disorders, with most studies focusing on patients with specific anxiety disorders such as SAD and GAD, (e.g., 14–16). These studies suggest that individuals with SAD and GAD tend to have reduced positive experiences and use experiential avoidance as a coping mechanism. However, PVS-related processing has been extensively studied in mood disorders. Symptoms of anhedonia in MDD have been associated with blunted reactivity to positively valanced and rewarding stimuli, (e.g., 17–20), as well as hypoactivation of brain circuits linked to those stimuli, (e.g., 21–23). In summary, existing literature on both types of disorders highlights disease-specific and therefore distinct profiles of reward processing.
Across units of behavioral, physiological, and neuronal data, there is ample evidence of similar NVS-related processing in MDD and AD: AD has been associated with a negativity bias toward negatively valanced stimuli, (e.g., 24–26), and altered activity in brain structures associated with responses to threat-related stimuli, (e.g., 27, 28); analogously, MDD has also been associated to a bias toward negatively valanced stimuli, (e.g., 21, 29, 30), and threat-related negative stimuli, (e.g., 31).
The occurrence of cognitive deficits regarding attention, memory and executive functioning in AD and MDD is well established (4, 32). However, the differentiation of disease-specific neural circuitry is challenging due to the lack of transdiagnostic and multimodal research (33) and because heterogeneous evidence exists for disorder-specific circuit alterations (3, 34).
While subconstructs of SP like attachment could be associated with social anxiety for example (35), the general impact of SP on AD is unclear due to the broad construct spectrum of SP in combination to the heterogenous disease patterns. Yet, the role of SP in specific types of AD such as SAD, has been more extensively investigated. This is because its symptomatology is closely linked to these processes, such as dysfunction in automatic association to social cues (36). As for MDD, impairment of social functioning is an evident sign and part of the structure of the disease. Kupferberg and colleagues (37) summarized that all SP subconstructs are impaired in patients with depression, hyper-sensitivity to social rejection, competition avoidance and increased altruistic punishment regarding the affiliation and attachment subconstruct, impaired emotion recognition, diminished cooperativeness regarding social communication and lastly reduced empathy or theory-of-mind deficits regarding social perception.
In recent years, there has been growing interest in transdiagnostic research approaches [(e.g., 38)]. Recent studies aimed to provide evidence for transdiagnostic and disorder-specific psychopathological endophenotypes of NVS-related abnormal threat processing in AD and MDD (33, 39), an attentional bias to negative stimuli in AD and MDD (40–42), as well as PVS-related impaired reward functioning in MDD that is phenomenologically characterized by anhedonia (33, 41, 43). Regarding PVS on the domain level, low levels of positive emotions at a global level have been identified as risk factors for MDD, SAD, and GAD (44, 45).
Using the RDoC approach to investigate transdiagnostic markers of disease severity could help clarify whether mechanisms associated with PVS, NVS, CS and SP contribute to disease severity. Consequently, investigating how individual differences across RDoC domains (PVS, NVS, SP, CS) explain variance in disease severity, could enhance our understanding of possible mechanisms contributing to disease severity. Dimensional assessment of these four domains could help modify classical diagnostic categories and furthermore, it could inform the development of individualized precision treatment for psychiatric disorders (7, 42).
The main aim of this study was to investigate PVS, NVS, CS and SP processing in relation to disease severity implemented into a transdiagnostic and dimensional approach. We thereby aim to improve the understanding of underlying mechanisms of the AD and MDD disease spectrum and shed light on disease-specific as well as transdiagnostic indicators of disease severity. To the best of our knowledge, to date, no study has yet focused on testing RDoC domains as indicators of disease severity in psychiatric disorders. Therefore, our research focuses on both the relationship between the four RDoC domains and transdiagnostic disease severity, as well as the domains diagnosis-specific effects. We hypothesized that PVS, CS, SP would be negatively associated with disease severity, while NVS would be positively related with disease severity. Second, we predicted that PVS, CS and SP would have a disease-specific relationship with disease severity, while all four domains were expected to also show a general transdiagnostic relationship with disease severity.
This investigation is an observational cross-sectional study assessing four core domains of the RDoC matrix (PVS, NVS, CS, and SP) within the German research network for mental disorders [Forschungszentrum zu psychischen Erkrankungen; FZPE] (46) as outlined by Förstner et al. (12). Study centers throughout the FZPE network recruited participants for clinical and observational studies. A minimal RDoC test battery covering behavioral and self-report units of analysis was incorporated into the existing assessment process at baseline to evaluate the aforementioned RDoC domains. The process of data collection and processing has been previously described in further detail (12). A subsample of patients with a primary diagnosis of major depression (MDD; ICD-10: F32, F33, F34.1) or an anxiety disorder (AD; ICD-10: F40, F41) (N = 859) was selected for analysis (see Table 1 and Supplementary Tables S1, S2 for sample characteristics). Diagnoses were determined by expert clinicians in accordance with the 10th Revision of the International Classification of Diseases [ICD-10; World Health Organization (WHO) (47),] and/or the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorder [DSM-IV; (48)]. On average, patients with AD were younger than patients with MDD, had a higher number of comorbidities, and were more likely to be married. Regarding comorbidities 54.53% (n = 289) of patients with AD had comorbid MDD [diagnostic data from CIDI interview only (49)] and 23.08% (n = 12) of patients with MDD had comorbid AD. A greater proportion of patients with MDD were receiving psychotropic medication. There were no further significant differences between AD and MDD patients with respect to gender and sociodemographic variables, including education.
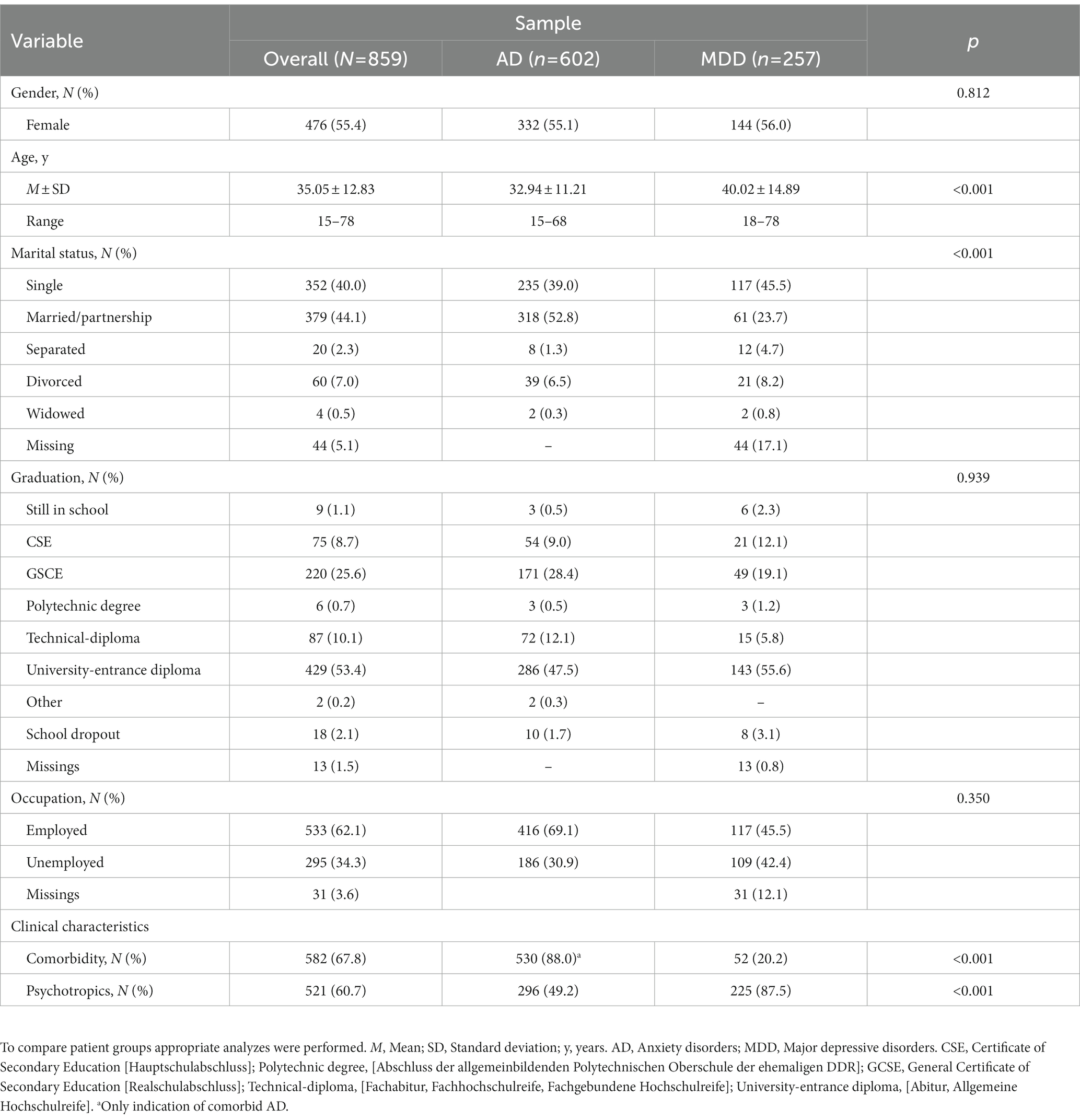
Table 1. Sample characteristics.
The four RDoC domains PVS, NVS, CS and SP were represented as individual patient factor scores from the four-factor CFA that had been conducted previously. Standardized factor scores were estimated using a linear regression method as reported by Förstner et al. (12). For ease of interpretation, factor scores were recoded positively, so that higher scores indicate higher expressions of the assessed domain. Therefore, higher scores in PVS indicate greater hedonic affect, and higher NVS scores indicate higher levels of anxious affect and somatization. Higher CS scores indicate better executive control, attention and working memory and higher SP scores indicate increased social skills, less interpersonal hostility and sensitivity, less paranoid ideas and less social anhedonia. For further details regarding the factor score composition, see Supplementary Table S3 (12). Table 2 provides sample details on the domain scores and the outcome variable disease severity, which is described below.
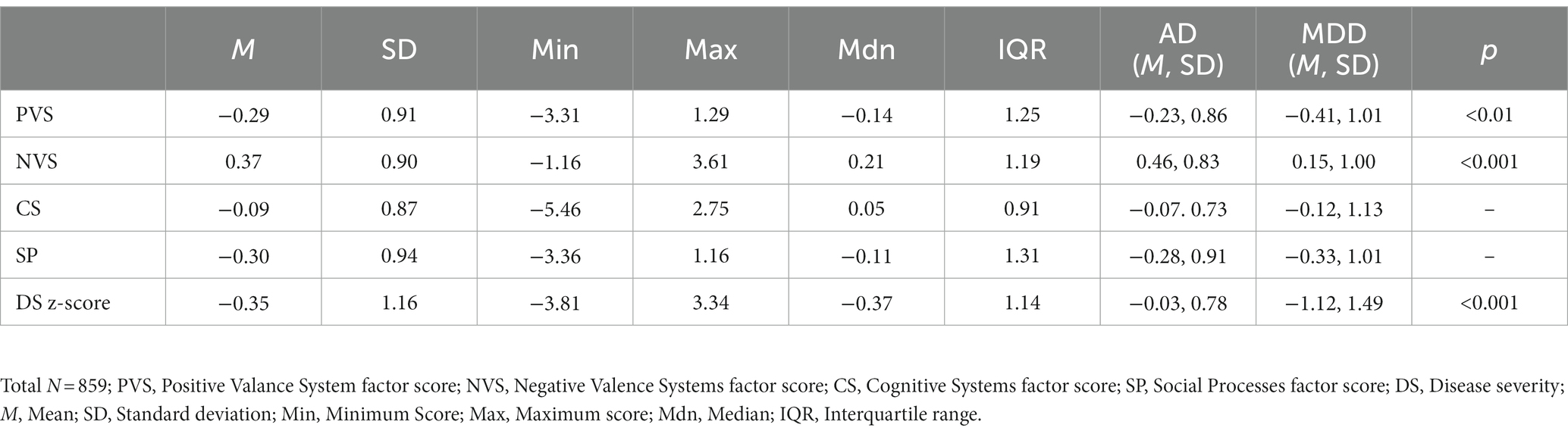
Table 2. Characteristics of domain-factor scores and disease severity.
Disease severity was assessed using disease-specific symptom-based self-report scales (4.7%), observer ratings (85.4%) or expert-based global rating scales (9.9%). To serve as a transdiagnostic outcome variable, all disease-specific severity values were z-standardized considering normative data from adult clinical samples. These samples had to meet the following criteria (1): provide a baseline distribution for the specific disease severity score, (2) contain as closely as possible represent the reference population (e.g., patients with MDD), and (3) contain a minimum of 500 participants and be representative if possible. Supplementary Table S4 provides detailed information on the normative data that was used for z-transformation.
Several simple and multiple Linear Models (LM) were used (models 0–6) in this analysis with step-by-step insertion of type of diagnosis (dichotomous variable) as fixed-effect, followed by PVS, NVS, CS and SP factor scores as continuous independent covariates, and followed by PVS by diagnosis, NVS by diagnosis, CS by diagnosis and SP by diagnosis (factor-covariate) interactions, and disease severity z-score as the dependent outcome. To address the overlapping structure identified in the previous CFA (12), we controlled for multicollinearity in the models m1 and m2. Since multicollinearity was present in both models, we decided to perform further analyzes on domain-specific models (m3-6) by including diagnosis as fixed effect, the specific domain as an independent covariate, and their respective interaction (f.e., m3: disease severity ~ diagnosis + PVS + PVS by diagnosis).
The Shapiro-Wilks test, which was used to check for normal distribution of variables, indicated that all 5 variables were significantly different from a normal distribution (p < 0.001). Since our sample size largely exceeded the central limit theorem cut-off (N > 30), these deviations can be considered acceptable. To identify possible outliers, grouped boxplots were used for independent variables. Furthermore, Cook’s Distance (50) was used to identify influential data points in the analyzed regression models [Di > 0.85 (51)]. No data were removed as no data point exceeded the cut-off in any model. Levene’s test showed that equal variances between groups (AD vs. MDD) could be assumed for SP but not for disease severity (p < 0.001), PVS (p < 0.05), NVS (p < 0.01) and CS (p < 0.001). Breush Pagan tests were used to check for homoscedasticity. When heteroscedasticity was present, a suitable heteroskedasticity-consistent (HC) covariance estimation method (f.e., 52) was used in addition. All analyzes were performed using R version 4.2.2 with RStudio 2022.07.2 Build 576.
We performed incremental linear regression models (LM) in four steps starting with a simple LM containing only main diagnosis and disease severity [m0: R2 = 0.19; F(1,857) = 198.70, p < 0.001]. Main diagnosis significantly predicted disease severity (β = −0.43; p < 0.001) with higher scores of disease severity in the AD group compared to the MDD group. In the next step (m1), we added all four RDoC domain factor scores as independent covariates to the m0 equation [R2 = 0.41; F(5,853) = 116.80, p < 0.001]. M1 revealed significant main effects for main diagnosis (β = −0.42; p < 0.001), PVS (β = −0.37; p < 0.001), NVS (β = 0.30; p < 0.001) and SP (β = 0.18; p < 0.05). The previous effect of diagnosis remained significant and additionally PVS was negatively associated to disease severity, while NVS and SP were positively associated with disease severity. We found no significant main effect of CS on disease severity. To control for multicollinearity, we calculated variance inflation factors (VIF) for m1. PVS (VIF = 10.04) and SP (VIF = 10.74) exceeded the cut-off (VIF > 10) indicating a high correlation of those predictors. Compared to m0, m1 showed a significantly better fit [F(4,853) = 78.38, p < 0.001] and larger R2. In a third step (m2), we added the four interactions of the domains with main diagnosis to m1 [R2 = 0.42; F(9,849) = 67.01, p < 0.001] to assess additional diagnosis-specific effects. Here we found significant main effects for main diagnosis (β = −0.45; p < 0.001), PVS (β = −0.30; p < 0.01) and NVS (β = 0.31; p < 0.001) while SP was only significant in the robust model (β = 0.18; p = 0.07; HC robust: p < 0.01). Other interactions included were not found to be significant. Even though R2 only increased by 0.01, model m2 had a significantly better fit [F(4,849) = 3.231, p = 0.05] than model m1. To check for multicollinearity in model m2, we calculated the variance inflation factors (GVIFs) for each predictor. This involved combining the main effect of the predictor with any interactions it has with other predictors in the model. The VIFs for PVS (VIF = 136.68), NVS (VIF = 15.09), and SP (VIF = 193.77) largely exceeded the cut-off. Consequently, we analyzed domain-specific models (m3-6) with main diagnosis, separate domain covariates and their associated interaction as predictors. Table 3 includes the results of models 3–6, which indicate significant domain-by-disease severity interactions for all domains. Figure 1 shows the interaction plots of the fitted values from these separate models for the four domains.
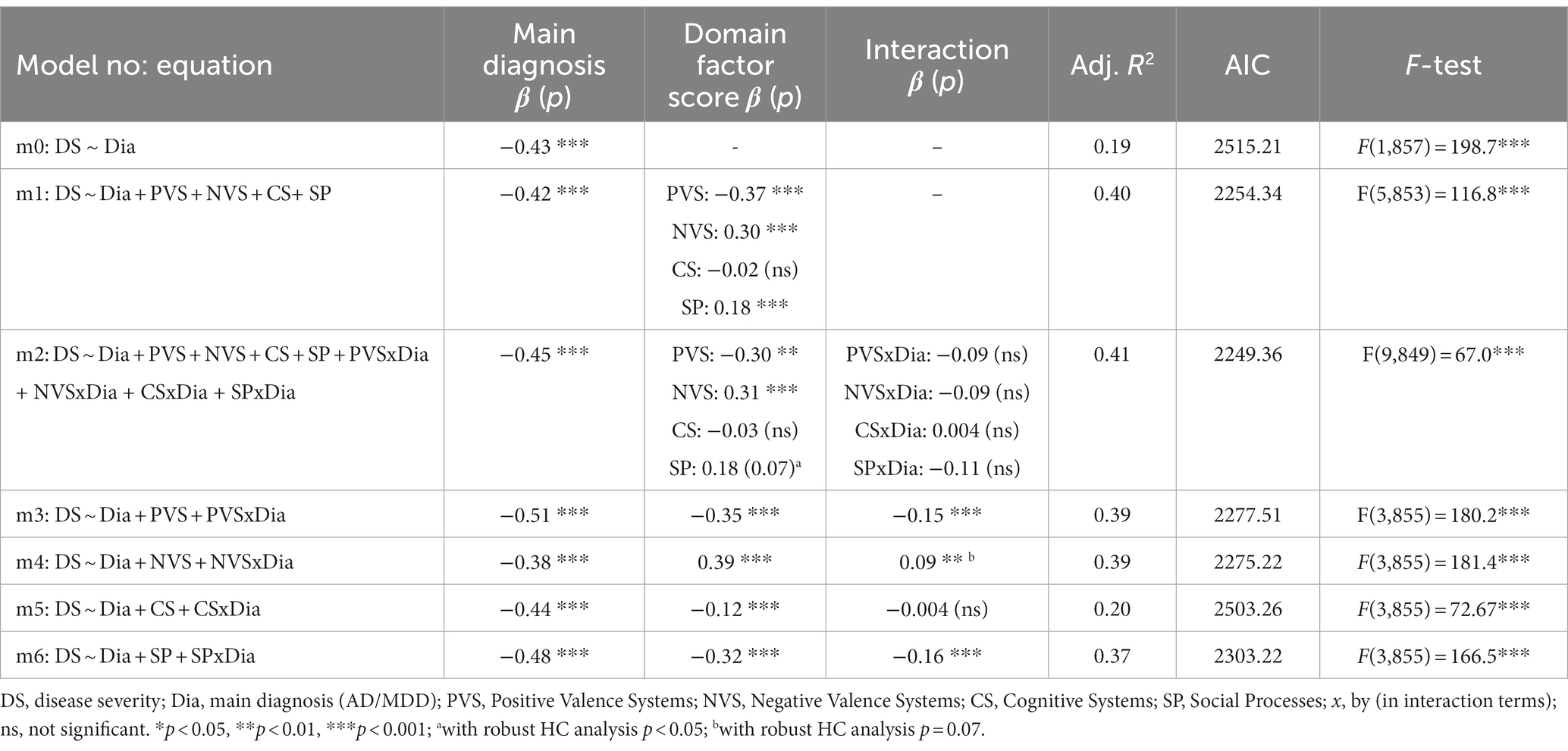
Table 3. Results of models 0–6.
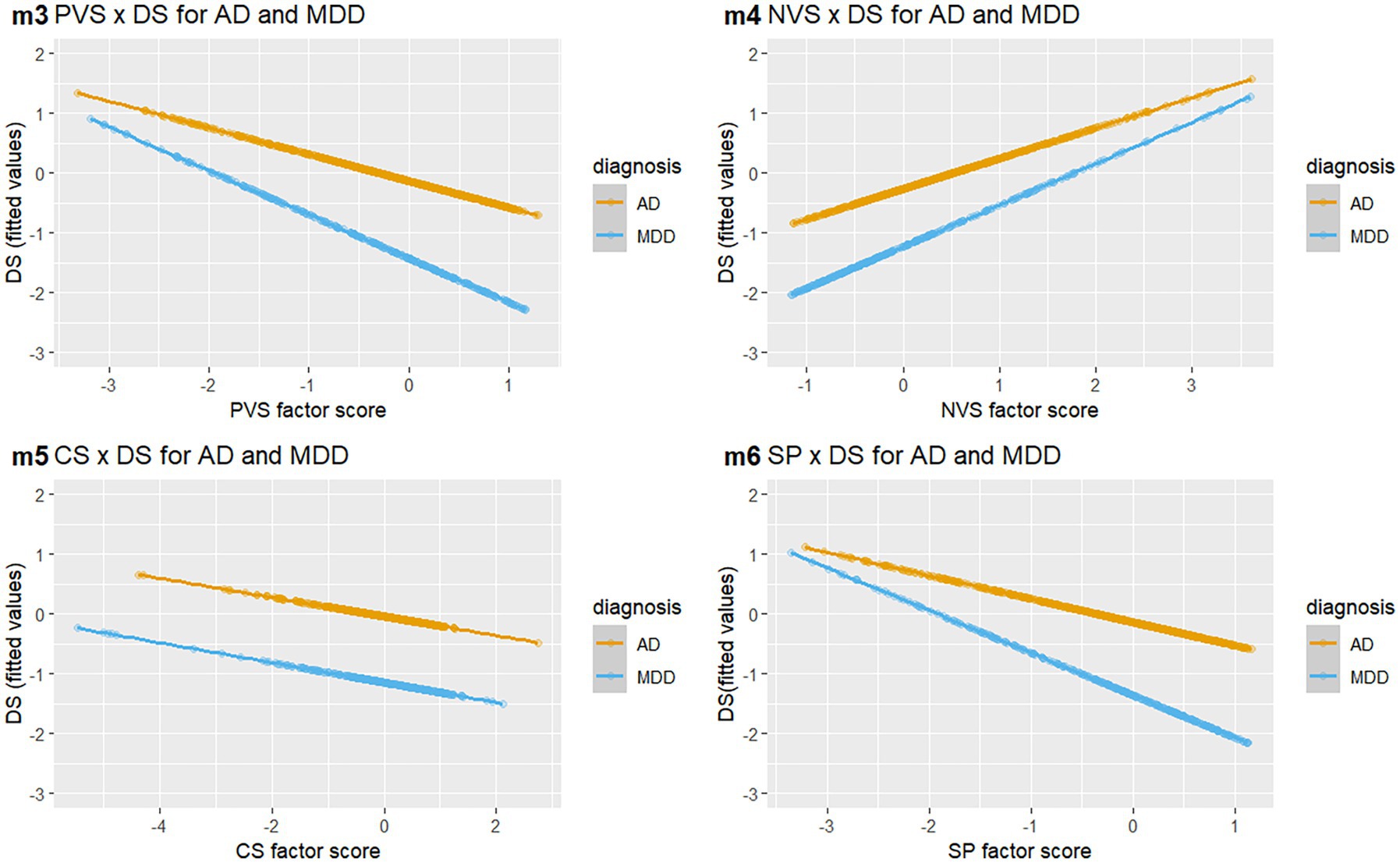
Figure 1. Relationship of RDoC domains with disease severity in AD and MDD. Grouped scatter graph of domain associations (PVS, NVS, CS, and SP) with fitted DS scores. Each dot corresponds to an individual score on both variables, the color represents the patient groups (orange: AD; blue: MDD). RDoC, Research Domain Criteria; AD, Anxiety disorders; MDD, Major depressive disorders; DS, disease severity; PVS, Positive Valence Systems; NVS, Negative Valence Systems; CS, Cognitive Systems; SP, Social Processes.
We found significant main effects for diagnosis and the respective domain in all four models (m3-m6). Specifically, PVS was significantly associated with disease severity in both AD and MDD, but the effect was stronger in MDD. A similar picture emerged for NVS and SP. With regard to the CS domain, we found a significant negative association with disease severity as a main effect in m5. A higher score on the CS factor was associated with lower disease severity.
Considering the heteroskedasticity of the models, we performed additional robust model analyzes for all models (m0-m6). The results showed no changes in the reported results, except for the following two models: In m2 the main effect of SP at trend level became significant (t = 2.53, p = 0.012) and in m4 the interaction of main diagnosis and NVS changed from a significant effect to an effect at trend level (t = 1,81, p = 0.071). Furthermore, results did not differ when controlling for age differences and present comorbidities in our analyzed models. In the CS single domain model (m5) age additionally significantly predicted disease severity (p < 0.01).
The main aim of our study was to examine the relationship between four core RDoC domains and disease severity among AD and MDD. As far as we know, this is the first study investigating these four transdiagnostic indicators on a domain level and their associations with disease severity in a transdiagnostic sample. Our first aim was to explore the relationship of PVS, NVS, CS, SP and disease severity across diagnostic categories. The results confirmed our hypotheses on this transdiagnostic relationship for all four domains, as we found significant main effects for PVS, NVS, CS and SP on disease severity within domain-specific models. For three domains, except CS, this main effect could also be found in the overall model as well. While NVS was positively associated with disease severity in our sample, PVS, CS and SP had a negative association with disease severity. Since we were able to show that some of these effects only occur within domain-specific analysis with similar R2 values, it stands to reason to assume that for AD and MDD, especially the effects of PVS and NVS play a superior role in this relationship to disease severity within patients with AD and MDD. However, this does not necessarily imply that anxiety predicts AD and anhedonia predicts depression; specifically, both PVS and NVS predicted diseases severity across disorders, and more so in patients suffering from MDD. Thus, we could show a transdiagnostic predictive value of both domains, which corresponds to our second main aim.
For this second aim, we investigated a disorder-specific interaction between these four domains and disease severity. Our results yielded three significant interaction effects within domain-specific models. Overall, we found a stronger association of PVS, NVS and SP with disease severity in MDD in comparison to AD, despite lower disease severity in patients with MDD compared to patients with AD. Therefore, future research should aim to replicate our findings in a longitudinal design to confirm this association.
In regards to the single RDoC domains starting with PVS, we found that low PVS manifestations, representing low hedonic affect and low habituation, were associated with high symptom burden, which is consistent with previous findings of diminished PVS processing in MDD, (e.g., 19, 21), and SAD and GAD, (e.g., 14, 45, 53). The finding that disease severity scores were affected by low PVS manifestations most strongly in patients with MDD is also consistent with previous research that suggests PVS-related processing as a marker for MDD, (e.g., 40, 42, 54).
Our results regarding NVS are also in line with previous research in AD, (e.g., 25–27), and MDD, (e.g., 21, 30, 31). This previous research supports our findings of a link between high symptom burden in patients with AD and MDD with high NVS manifestations, representing high levels of anxiety and behavioral inhibition. As NVS-related processing is a common dysfunction in AD and MDD, (e.g., 39, 42, 55), our results are further evidence for altered NVS functioning as a transdiagnostic marker for the spectrum of depressive and anxiety disorders.
As mentioned earlier, research on the association of a latent construct CS domain with disease severity is limited. Our results are in line with previous findings on a negative association of cognitive functioning and disease severity in MDD and AD (32, 56, 57). Our findings did not reveal a disease-specific interaction for CS, represented by executive functioning, attention, and working memory, but we did find a main effect of the disorder, indicating a decreased cognitive function in patients with MDD. The lack of a significant interaction, in the presence of known disease-specific evidence for cognitive deficits in episodic memory in patients with MDD and attentional bias in patients with AD, may be due to combining variables of several different cognitive processes into one latent variable, thereby losing crucial variance. This should be closely examined in future research.
Our findings for the SP domain are consistent with previous research that has identified dysfunction in affiliation and attachment in patients with MDD, as well as dysfunction in perception and understanding of self in patients with AD, particularly GAD (5). Additionally, there is evidence of global social functioning deficits in both AD and MDD (37, 58). Previous research on the SP domain that aligned with RDoC has primarily focused on youth or adolescent samples (11, 59). Our study extends previous research on this particular domain to adult populations by identifying disease-specific and transdiagnostic associations of social processes and symptom burden within an adult sample.
As noted, the data of this present study was provided by pooling anonymized data from all FZPE consortia. Incomplete information on comorbidities and some main diagnoses resulted in the limited availability of subgroup data sets. Specifically, the comorbidity overlap in our sample may have diluted symptom specific effects on disease severity. It should be noted, however, that despite this possible limitation, we found different associations of the domains with the diagnosis-specific symptom burden. Especially for NVS, which has been associated with anxiety, our results present differential associations despite the high comorbidity of AD with MDD in the subsample. Future studies are needed to investigate PVS, NVS, CS and SP dys−/function in specific types of AD and MDD, as well as to consider comorbidities within AD and MDD. As this is a cross-sectional study, the interpretation of our results is limited. Given that the relationship of PVS, NVS, CS and SP functioning with disease severity in AD and MDD unfolds over time, no causal conclusions can be inferred. However, we reliably showed that RDoC domains are associated with disease severity across disorders.
We would also like to point out that the majority of our disease severity ratings was based on self-report. Since the RDoC domains maybe more sensitive to self-reported disease severity future research on differential effects on self-reported versus expert-based ratings of disease severity could be additionally informative. While we used LM models as a statistical method of analysis, this approach may have limited our understanding of the domain-specific relations to the disease severity burden, because we were unable to account for random effects which could have affected the results. More sophisticated models like generalized linear mixed models (GLMM) should be considered for further investigations.
Since domain factor scores were constructed using many BSI-Items and considering the presence of well documented correlations between BSI-53 (SCL-90) and other severity measures f.e., BDI-II (60) this could be considered as another limitation impacting our results. We would like to argue, that even though there is a surplus of BSI-53 items involved in the factor structure, we still measured the latent RDoC domains and not only different types of symptom burden. Model fit of the four-factor model was significantly better in comparison to a one factor model (measuring general psychopathology) and a model with independent factors (12). Additionally, if our results were solely driven by symptom burden, we would expect that the association of NVS to disease-specific AD severity would be stronger than for MDD, which is not the case.
Given the presence of possible outliers, heteroskedasticity, and multicollinearity during our analyzes, which we addressed adequately, it is important to interpret our results within the context of these specific conditions. Especially in light of multicollinearity and the change in significance with robust testing in two of the models, the associational structure between PVS, NVS and SP has to be further investigated.
Although it is still at an early stage, there is some indication from our results that a specific RDoC-based treatment may be more effective for patients with MDD. Further investigation is needed to confirm this hypothesis. Nevertheless, there is already some evidence in this direction with an RDoC-based treatment called ENGAGE, which targets f.e., reward processing (PVS) and has shown promising results in improving outcomes for patients with MDD (61). Therefore, further development and implementation of RDoC-based disease-specific treatments could lead to more tailored and effective interventions for all mental disorders. Overall, our findings suggest that a more nuanced transnosological understanding of mental disorders’ underlying mechanisms and dimensions is needed to inform the development of more effective treatment.
In Conclusion, our key results demonstrate a strong association between symptom burden in patients with AD and MDD and latent RDoC indicators (PVS, NVS, CS, and SP) in a transdiagnostic way. There is also evidence for a disease-specific association between PVS, NVS and SP, which requires future research to further understand the association of PVS, NVS and SP with disease severity, hopefully informing specific treatment options in the future (62).
The datasets presented in this article are not readily available because they are not available publicly based on local and national data protection regulations. All original data are on record and accessible to inspection. Requests to access the datasets should be directed to bWljaGFlbC5yYXBwQHVuaS1wb3RzZGFtLmRl.
The studies involving human participants were reviewed and approved by Potsdam Research Ethics Committee, University of Potsdam. The patients/participants provided their written informed consent to participate in this study.
BF, SB, and MT managed the literature searches and analyzes. BF, MT, SB, and MR undertook the statistical analysis. BF wrote the first draft of the manuscript. All authors designed the study, wrote the protocol, and contributed to the article and approved the submitted version.
This work was supported by the Phenotypic, Diagnostic and Clinical Domain Assessment Network Germany (PD-CAN) research consortium (FKZ 01EE1406I) and the following research consortia AERIAL (01EE1406), APIC (01EE1405), ASD-Net (01EE1409), ESPRIT (01EE1407), GCBS (01EE1403), ESCAlife (01EE1408), BipoLife (01EE1404), OptiMD (01EE1401), and PROTECT-AD (01EE1402) funded by the German Federal Ministry of Education and Research (BMBF; http://www.Bmbf.de). Open Access-Publication funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Project number 491466077.
The authors would like to thank the following individuals for their help regarding the PROTECT-AD consortium: Jule Dehler, Dorte Westphal, Katrin Hummel, Jürgen Hoyer (Dresden), Verena Pflug, Dirk Adolph, Cornelia Mohr, Jan Cwik (Bochum), Maike Hollandt, Anne Pietzner, Jörg Neubert (Greifswald), Carsten Konrad, Yunbo Yang, Isabelle Ridderbusch, Adrian Wroblewski, Hanna Christiansen, Anne Maenz, Sophia Tennie, Jean Thierschmidt (Marburg), Marcel Romanos, Kathrin Zierhut, Kristina Dickhöver, Markus Winkler, Maria Stefanescu, Christiane Ziegler (Würzburg), Nathalia Weber, Sebastian Schauenberg, Sophia Wriedt, Carina Heitmann (Münster) Caroline im Brahm, Annika Evers (Cologne), Isabel Alt, Sophie Bischoff, Jennifer Mumm, Jens Plag, and Anne Schreiner (Berlin). Xina Grählert and Marko Käppler of the Coordinating Center for Clinical Trials (KKS) data center (Dresden) provided support with the electronic data assessment and data banking. Eva Stolzenburg, Stanislav Bologov, and Karina Bley provided administrative support. A complete list of project publications can be found at www.fzpe.de They would also like thank Johannes Weigl for excellent study recruitment and clinical ratings as well as Karin Völlner for her very good study nurse support. Within the Phenotypic, Diagnostic and Clinical Domain Assessment Network Germany (PD-CAN), the authors like to thank: Gerit Brenner-Fließer for data quality checks, Carole Klein, Olena Mostova, Laura Szalek for their help in manuscript preparation.
FP is a member of the European Scientific Advisory Board of Brainsway Inc., Jerusalem, Israel, and the International Scientific Advisory Board of Sooma, Helsinki, Finland. He has received speaker’s honoraria from Mag&More GmbH, the neuroCare Group, Munich, Germany, and Brainsway Inc. His lab has received support with equipment from neuroConn GmbH, Ilmenau, Germany, Mag&More GmbH and Brainsway Inc. TB served in an advisory or consultancy role for eye level, Infectopharm, Lundbeck, Medice, Neurim Pharmaceuticals, Oberberg GmbH, Roche, and Takeda. He received conference support or speaker’s fee by Janssen, Medice and Takeda. He received royalities from Hogrefe, Kohlhammer, CIP Medien, Oxford University Press; the present work is unrelated to these relationships.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1161097/full#supplementary-material
AD, Anxiety Disorders; MDD, (Major) Depressive Disorder; SAD, Social Anxiety Disorder; GAD, Generalized Anxiety Disorder; PD-CAN, Phenotypic, Diagnostic and Clinical Domain Assessment Network Germany; FZPE, German research network for mental disorders [Forschungszentrum zu psychischen Erkrankungen]; PVS, Positive Valence Systems; NVS, Negative Valence Systems; CS, Cognitive Systems; SP, Social Processes.
1. Clark, LA , and Watson, D . Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications. J Abnorm Psychol. (1991) 100:316–36. doi: 10.1037/0021-843X.100.3.316
2. Brown, TA , Chorpita, BF , and Barlow, DH . Structural relationships among dimensions of the DSM-IV anxiety and mood disorders and dimensions of negative affect, positive affect, and autonomic arousal. J Abnorm Psychol. (1998) 107:179–92. doi: 10.1037//0021-843X.107.2.179
3. Wei, M , and Roodenrys, S . A scoping review on the extent and nature of anxiety-related research within the research domain criteria (RDoC) framework: limited coverage using non-disorder-specific search terms. New Ideas Psychol. (2021) 63:100901. doi: 10.1016/j.newideapsych.2021.100901
4. Rock, PL , Roiser, JP , Riedel, WJ , and Blackwell, AD . Cognitive impairment in depression: a systematic review and meta-analysis. Psychol Med. (2014) 44:2029–40. doi: 10.1017/S0033291713002535
5. Praus, P , Bilek, E , Holz, NE , and Braun, U . Die Domäne “soziale Prozesse” im System der Research Domain Criteria: aktueller Stand und Perspektive. Nervenarzt. (2021) 92:925–32. doi: 10.1007/s00115-021-01161-6
6. Insel, TR , Cuthbert, B , Garvey, M , Heinssen, R , Pine, DS , Quinn, K, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry. (2010) 167:748–51. doi: 10.1176/appi.ajp.2010.09091379
7. Cuthbert, BN . The role of RDoC in future classification of mental disorders. Dialogues Clin Neurosci. (2020) 22:81–5. doi: 10.31887/DCNS.2020.22.1/bcuthbert
8. Paulus, MP , Stein, MB , Craske, MG , Bookheimer, S , Taylor, CT , Simmons, AN, et al. Latent variable analysis of positive and negative valence processing focused on symptom and behavioral units of analysis in mood and anxiety disorders. J Affect Disord. (2017) 216:17–29. doi: 10.1016/j.jad.2016.12.046
9. Lee, M , Aggen, SH , Carney, DM , Hahn, S , Moroney, E , Machlin, L, et al. Latent structure of negative valence measures in childhood. Depress Anxiety. (2017) 34:742–51. doi: 10.1002/da.22656
10. Schretlen, DJ , Peña, J , Aretouli, E , Orue, I , Cascella, NG , Pearlson, GD, et al. Confirmatory factor analysis reveals a latent cognitive structure common to bipolar disorder, schizophrenia, and normal controls. Bipolar Disord. (2013) 15:422–33. doi: 10.1111/bdi.12075
11. Uljarević, M , Frazier, TW , Phillips, JM , Jo, B , Littlefield, S , and Hardan, AY . Quantifying research domain criteria social communication subconstructs using the social communication questionnaire in youth. J Clin Child Adolesc Psychol. (2020) 50:609–18. doi: 10.1080/15374416.2019.1669156
12. Förstner, BR , Tschorn, M , Reinoso-Schiller, N , Maričić, LM , Röcher, E , Kalman, JL, et al. Mapping research domain criteria using a transdiagnostic mini-RDoC assessment in mental disorders: a confirmatory factor analysis. Eur Arch Psychiatry Clin Neurosci. (2022) 273:527–39. doi: 10.1007/s00406-022-01440-6
13. NIMH . Definitions of the RDoC domains and constructs (2023). Available at: https://www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/definitions-of-the-rdoc-domains-and-constructs.shtml. (Accessed Jan 13, 2023).
14. Kashdan, TB . Social anxiety spectrum and diminished positive experiences: theoretical synthesis and meta-analysis. Clin Psychol Rev. (2007) 27:348–65. doi: 10.1016/j.cpr.2006.12.003
15. Kashdan, TB , Farmer, AS , Adams, LM , Ferssizidis, P , McKnight, PE , and Nezlek, JB . Distinguishing healthy adults from people with social anxiety disorder: evidence for the value of experiential avoidance and positive emotions in everyday social interactions. J Abnorm Psychol. (2013) 122:645–55. doi: 10.1037/a0032733
16. Taylor, CT , Bomyea, J , and Amir, N . Attentional bias away from positive social information mediates the link between social anxiety and anxiety vulnerability to a social stressor. J Anxiety Disord. (2010) 24:403–8. doi: 10.1016/j.janxdis.2010.02.004
17. Baskin-Sommers, AR , and Foti, D . Abnormal reward functioning across substance use disorders and major depressive disorder: considering reward as a transdiagnostic mechanism. Int J Psychophysiol. (2015) 98:227–39. doi: 10.1016/j.ijpsycho.2015.01.011
18. Barch, DM , Pagliaccio, D , and Luking, K . Mechanisms underlying motivational deficits in psychopathology: similarities and differences in depression and schizophrenia. Curr Top Behav Neurosci. (2016) 27:411–49. doi: 10.1007/7854_2015_376
19. Dillon, DG , Rosso, IM , Pechtel, P , Killgore, WD , Rauch, SL , and Pizzagalli, DA . Peril and pleasure: an rdoc-inspired examination of threat responses and reward processing in anxiety and depression. Depress Anxiety. (2014) 31:233–49. doi: 10.1002/da.22202
20. Hägele, C , Schlagenhauf, F , Rapp, M , Sterzer, P , Beck, A , Bermpohl, F, et al. Dimensional psychiatry: reward dysfunction and depressive mood across psychiatric disorders. Psychopharmacology. (2015) 232:331–41. doi: 10.1007/s00213-014-3662-7
21. Groenewold, NA , Opmeer, EM , de Jonge, P , Aleman, A , and Costafreda, SG . Emotional valence modulates brain functional abnormalities in depression: evidence from a meta-analysis of fMRI studies. Neurosci Biobehav Rev. (2013) 37:152–63. doi: 10.1016/j.neubiorev.2012.11.015
22. Nusslock, R , and Alloy, LB . Reward processing and mood-related symptoms: an RDoC and translational neuroscience perspective. J Affect Disord. (2017) 216:3–16. doi: 10.1016/j.jad.2017.02.001
23. Treadway, MT , and Zald, DH . Reconsidering anhedonia in depression: lessons from translational neuroscience. Neurosci Biobehav Rev. (2011) 35:537–55. doi: 10.1016/j.neubiorev.2010.06.006
24. Klumpp, H , Post, D , Angstadt, M , Fitzgerald, DA , and Phan, KL . Anterior cingulate cortex and insula response during indirect and direct processing of emotional faces in generalized social anxiety disorder. Biol Mood Anxiety Disord. (2013) 3:7. doi: 10.1186/2045-5380-3-7
25. Shin, LM , and Liberzon, I . The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology. (2010) 35:169–91. doi: 10.1038/npp.2009.83
26. Bar-Haim, Y , Lamy, D , Pergamin, L , Bakermans-Kranenburg, MJ , and Van IJzendoorn, MH . Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull. (2007) 133:1–24. doi: 10.1037/0033-2909.133.1.1
27. Etkin, A , and Wager, TD . Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry. (2007) 164:1476–88. doi: 10.1176/appi.ajp.2007.07030504
28. Killgore, WD , Britton, JC , Schwab, ZJ , Price, LM , Weiner, MR , Gold, AL, et al. Cortico-limbic responses to masked affective faces across ptsd, panic disorder, and specific phobia. Depress Anxiety. (2014) 31:150–9. doi: 10.1002/da.22156
29. Stuhrmann, A , Suslow, T , and Dannlowski, U . Facial emotion processing in major depression: a systematic review of neuroimaging findings. Biol Mood Anxiety Disord. (2011) 1:10. doi: 10.1186/2045-5380-1-10
30. Hamilton, EA , Furman, DJ , Lemus, MG , Johnson, RF , and Gotlib, IH . Functional neuroimaging of major depressive disorder: a meta-analysis and new integration of base line activation and neural response data. Am J Psychiatry. (2012) 169:693–703. doi: 10.1176/appi.ajp.2012.11071105
31. Jaworska, N , Yang, X-R , Knott, V , and Mac, QG . A review of fMRI studies during visual emotive processing in major depressive disorder. World J Biol Psychiatry. (2015) 16:448–71. doi: 10.3109/15622975.2014.885659
32. Ferreri, F , Lapp, LK , and Peretti, C-S . Current research on cognitive aspects of anxiety disorders. Curr Opin Psychiatry. (2011) 24:49–54. doi: 10.1097/YCO.0b013e32833f5585
33. Williams, LM . Defining biotypes for depression and anxiety based on large-scale circuit dysfunction: a theoretical review of the evidence and future directions for clinical translation. Depress Anxiety. (2017) 34:9–24. doi: 10.1002/da.22556
34. Sindermann, L , Redlich, R , Opel, N , Böhnlein, J , Dannlowski, U , and Leehr, EJ . Systematic transdiagnostic review of magnetic-resonance imaging results: depression, anxiety disorders and their co-occurrence. J Psychiatr Res. (2021) 142:226–39. doi: 10.1016/j.jpsychires.2021.07.022
35. Fang, A , Hoge, EA , Heinrichs, M , and Hofmann, SG . Attachment style moderates the effects of oxytocin on social behaviors and cognitions during social rejection: applying an RDoC framework to social anxiety. Clin Psychol Sci. (2014) 2:740–7. doi: 10.1177/2167702614527948
36. Glashouwer, KA , Vroling, MS , de Jong, PJ , Lange, W-G , and de Keijser, J . Low implicit self-esteem and dysfunctional automatic associations in social anxiety disorder. J Behav Ther Exp Psychiatry. (2013) 44:262–70. doi: 10.1016/j.jbtep.2012.11.005
37. Kupferberg, A , Bicks, L , and Hasler, G . Social functioning in major depressive disorder. Neurosci Biobehav Rev. (2016) 69:313–32. doi: 10.1016/j.neubiorev.2016.07.002
38. Fusar-Poli, P , Solmi, M , Brondino, N , Davies, C , Chae, C , Politi, P, et al. Transdiagnostic psychiatry: a systematic review. World Psychiatry. (2019) 18:192–207. doi: 10.1002/wps.20631
39. MacNamara, A , Klumpp, H , Kennedy, AE , Langenecker, SA , and Phan, KL . Transdiagnostic neural correlates of affective face processing in anxiety and depression. Depress Anxiety. (2017) 34:621–31. doi: 10.1002/da.22631
40. Goldstein, BL , and Klein, DN . A review of selected candidate endophenotypes for depression. Clin Psychol Rev. (2014) 34:417–27. doi: 10.1016/j.cpr.2014.06.003
41. Hasler, G , Drevets, WC , Manji, HK , and Charney, DS . Discovering endophenotypes for major depression. Neuropsychopharmacology. (2004) 29:1765–81. doi: 10.1038/sj.npp.1300506
42. Williams, LM . Precision psychiatry: a neural circuit taxonomy for depression and anxiety. Lancet Psychiatry. (2016) 3:472–80. doi: 10.1016/S2215-0366(15)00579-9
43. Webb, CA , Dillon, DG , Pechtel, P , Goer, FK , Murray, L , Huys, QJ, et al. Neural correlates of three promising Endophenotypes of depression: evidence from the EMBARC study. Neuropsychopharmacology. (2016) 41:454–63. doi: 10.1038/npp.2015.165
44. Khazanov, GK , and Ruscio, AM . Is low positive emotionality a specific risk factor for depression? A meta-analysis of longitudinal studies. Psychol Bull. (2016) 142:991–1015. doi: 10.1037/bul0000059
45. Kendall, AD , Zinbarg, RE , Mineka, S , Bobova, L , Prenoveau, JM , Revelle, W, et al. Prospective associations of low positive emotionality with firstnusslock onsets of depressive and anxiety disorders: results from a 10-wave latent trait-state modeling study. J Abnorm Psychol. (2015) 124:933–43. doi: 10.1037/abn0000105
46. Bauer, M , Banaschewski, T , Heinz, A , Kamp-Becker, I , Meyer-Lindenberg, A , Padberg, F, et al. Das deutsche forschungsnetz zu psychischen erkrankungen. Nervenarzt. (2016) 87:989–1010. doi: 10.1007/s00115-016-0169-y
47. World Health Organization . International statistical classification of diseases and related health problems. Geneva, Switzerland: World Health Organization (2015).
48. American Psychiatric Association . Diagnostic and statistical manual of mental disorders: DSM-IV-TR. Washington, DC: American Psychiatric Association (2000).
49. Robins, LN , Wing, J , Wittchen, HU , Helzer, JE , Babor, TF , Burke, J, et al. The composite international diagnostic interview. An epidemiologic instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Arch Gen Psychiatry. (1988) 45:1069–77. doi: 10.1001/archpsyc.1988.01800360017003
50. Cook, RD . Detection of influential observation in linear regression. Technometrics. (1977) 19:15. doi: 10.2307/1268249
51. McDonald, BA . Teaching Note on Cook’s Distance - A Guideline (2002). Retrieved from Massey University at Albany website: https://www.massey.ac.nz/massey/fms/Colleges/College%20of%20Sciences/IIMS/RLIMS/Volume03/A_Teaching_Note_on_Cooks_Distance-A_Guideline.pdf (Accessed January 13, 2023).
52. Zeileis, A . Econometric computing with HC and HAC covariance matrix estimators. J. Stat. Soft. (2004) 11. doi: 10.18637/jss.v011.i10
53. Richey, JA , Brewer, JA , Sullivan-Toole, H , Strege, MV , Kim-Spoon, J , White, SW, et al. Sensitivity shift theory: a developmental model of positive affect and motivational deficits in social anxiety disorder. Clin Psychol Rev. (2019) 72:101756. doi: 10.1016/j.cpr.2019.101756
54. Heinz, A , Schmidt, LG , and Reischies, FM . Anhedonia in schizophrenic, depressed, or alcohol-dependent patients–neurobiological correlates. Pharmacopsychiatry. (1994) 27:7–10. doi: 10.1055/s-2007-1014317
55. Feldker, K , Heitmann, CY , Neumeister, P , Tupak, SV , Schrammen, E , Moeck, R, et al. Transdiagnostic brain responses to disorder-related threat across four psychiatric disorders. Psychol Med. (2017) 47:730–43. doi: 10.1017/S0033291716002634
56. Lee, RS , Hermens, DF , Porter, MA , and Redoblado-Hodge, MA . A meta-analysis of cognitive deficits in first-episode major depressive disorder. J Affect Disord. (2012) 140:113–24. doi: 10.1016/j.jad.2011.10.023
57. Castaneda, AE , Tuulio-Henriksson, A , Marttunen, M , Suvisaari, J , and Lönnqvist, J . A review on cognitive impairments in depressive and anxiety disorders with a focus on young adults. J Affect Disord. (2008) 106:1–27. doi: 10.1016/j.jad.2007.06.006
58. Saris, IM , Aghajani, M , van der Werff, SJ , van der Wee, NJ , and Penninx, BWJH . Social functioning in patients with depressive and anxiety disorders. Acta Psychiatr Scand. (2017) 136:352–61. doi: 10.1111/acps.12774
59. King, LS , Salo, VC , Kujawa, A , and Humphreys, KL . Advancing the RDoC initiative through the assessment of caregiver social processes. Dev Psychopathol. (2021) 33:1648–64. doi: 10.1017/S095457942100064X
60. Steer, RA , Ball, R , Ranieri, WF , and Beck, AT . Further evidence for the construct validity of the Beck depression inventory-II with psychiatric outpatients. Psychol Rep. (1997) 80:443–6. doi: 10.2466/pr0.1997.80.2.443
61. Alexopoulos, GS , Raue, PJ , Gunning, F , Kiosses, DN , Kanellopoulos, D , Pollari, C, et al. "Engage" therapy: behavioral activation and improvement of late-life major depression. Am J Geriatr Psychiatry. (2016) 24:320–6. doi: 10.1016/j.jagp.2015.11.006
Keywords: Research Domain Criteria, depression, anxiety disoders, disease severity, transdiagnostic, RDoC
Citation: Förstner BR, Böttger SJ, Moldavski A, Bajbouj M, Pfennig A, Manook A, Ising M, Pittig A, Heinig I, Heinz A, Mathiak K, Schulze TG, Schneider F, Kamp-Becker I, Meyer-Lindenberg A, Padberg F, Banaschewski T, Bauer M, Rupprecht R, Wittchen H-U, Rapp MA and Tschorn M (2023) The associations of Positive and Negative Valence Systems, Cognitive Systems and Social Processes on disease severity in anxiety and depressive disorders. Front. Psychiatry 14:1161097. doi: 10.3389/fpsyt.2023.1161097
Edited by:
Roberto Viviani, University of Innsbruck, AustriaReviewed by:
Birgit Abler, University of Ulm, GermanyCopyright © 2023 Förstner, Böttger, Moldavski, Bajbouj, Pfennig, Manook, Ising, Pittig, Heinig, Heinz, Mathiak, Schulze, Schneider, Kamp-Becker, Meyer-Lindenberg, Padberg, Banaschewski, Bauer, Rupprecht, Wittchen, Rapp and Tschorn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bernd R. Förstner, YmVybmQuZm9lcnN0bmVyQHVuaS1wb3RzZGFtLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.