
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Psychiatry, 25 May 2023
Sec. Neurostimulation
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1146492
This article is part of the Research TopicWomen in Psychiatry 2023: NeurostimulationView all 4 articles
 Florence Vorspan1,2*‡
Florence Vorspan1,2*‡ Philippe Domenech3,4†‡
Philippe Domenech3,4†‡ David Grabli3,5Jérôme Yelnik3Marine Delavest2Charles Dauré1
David Grabli3,5Jérôme Yelnik3Marine Delavest2Charles Dauré1 Frank Bellivier1,2Antoine Pelissolo4,6
Frank Bellivier1,2Antoine Pelissolo4,6 Hayat Belaid7†
Hayat Belaid7† Christelle Baunez8Carine Karachi3,7
Christelle Baunez8Carine Karachi3,7 Luc Mallet3,4,9
Luc Mallet3,4,9Crack-cocaine dependence is a severe condition with a high mortality rate. This single case study report details the first deep brain stimulation (DBS) trial targeting the sub-thalamic nucleus (STN) for crack-cocaine dependence. The investigation aimed to assess the effects of STN-DBS on cocaine craving and cocaine use, as well as STN-DBS safety and tolerance in this indication. In this pilot study, we performed double blind cross-over trials, with “ON-DBS” vs. “SHAM-DBS” for 1-month periods. STN-DBS failed to reduce cocaine craving and use. An episode of DBS-induced hypomania occurred after several weeks of cocaine intake at stimulation parameters previously well tolerated. Future research on cocaine dependence should be conducted after a prolonged abstinence period and/or explore novel types of stimulation patterns.
Crack cocaine dependence increases mortality (1, 2) and has significant health and social consequences (3–5). France is facing an increase in specialized addiction treatment entry for cocaine use disorder (6) in general, and an increase in crack-cocaine related mortality specifically (7). Current treatments (8, 9) show limited efficacy on abstinence maintenance and harm reduction. To date, four reported clinical cases of cocaine or methamphetamine addiction have utilized deep brain stimulation (DBS) treatment, with 3 out 4 patients showing a reduction in cocaine use (10–12), reviewed in (13). These trial studies targeted the bilateral ventral striatum, with parameters between 150–165 Hz, 2–3.3 V and 150–240 μs, with 240 μs in two cases associated with the emergence of hypomania. Three of the four trials were open label (10, 12), whilst the one double blind trial failed to show any difference between the ON vs. SHAM period (11). Consequently, causal modeling trial efficacy is subject to influence by non-specific factors.
We previously advocated the subthalamic nucleus (STN) as a potential target for severe cocaine dependence (14). Preclinical studies indicate that the STN is an important hub for controlling cocaine intake. High frequency STN-DBS corrects the balance between sucrose and cocaine preference in a conditioned place paradigm (15) and reduces re-escalation of cocaine self-administration after prolonged, but not short, abstinence (16). Low frequency STN-DBS also reduces cocaine intake in cocaine-dependent rats who developed an aversive shock-resistant cocaine intake (17). In humans, STN-DBS combined with a decrease of dopaminergic medication has been proposed to improve both medication abuse and other behavioral addictions in Parkinson's disease (PD) patients (18). STN-DBS also improves obsessions and compulsions in obsessive-compulsive disorder (OCD) and PD patients (19–22). The core cocaine dependence symptom, craving, has strong parallels with obsessional symptoms in OCD (23). There is also a high prevalence of transient OCD-like symptoms in patients with cocaine use disorder in care settings, with an OCD-like symptom prevalence of 58% in one study (24), mostly consisting of checking, and repetitive/ritualized movements. Within the general population, cocaine use positively associates with OCD with an odd-ratio of 4 (25). Thus, our hypothesis is that STN-DBS suppresses craving during abstinence, as indicated by the Obsessive Compulsive Cocaine Score (OCCS) score (26), in people with cocaine addiction.
We present the first STN-DBS case for severe and treatment-resistant crack cocaine use disorder over a 2-year follow-up. The study (Clinicaltrials.gov Number NCT02892851) was approved by a local ethics committee. Inclusion criteria were diagnosis of DSM IV cocaine dependence; crack cocaine use (a smoked form of cocaine); previously classed as non-responder to a well conducted pharmacological treatment, with one long-term detoxification stay associated with after-care. Exclusion criteria were limited to surgery contra-indications or unstable psychiatric condition. Consequently, all stable psychiatric conditions and other substance use disorders were not subject to exclusion. The primary outcome was OCCS reduction (26), secondary outcomes were crack cocaine scale (CCQ) (27) immediate craving score reduction and self-declared and objective cocaine use reduction over the cross-over 1 months periods. One male patient in his 40 s with a 20-year history of severe smoked crack dependence participated in this trial. He was also opioid and benzodiazepine dependent, as well as satisfying criteria for DSM IV alcohol abuse. He was unemployed and homeless, with severed family ties for 11 years. The study participant had 2 previous in-patient cocaine cessation trials, followed by long-term residential care with a maximum abstinence period of 4 months, followed by relapses. He had also received 2 months of aripiprazole up to 15 mg/d (19) with no efficacy. Finally, he failed to attend cognitive behavioral therapy (CBT) relapse prevention group sessions. At inclusion, he was under prescribed oral buprenorphine 8 mg/day, cyamemazine 300 mg/d and oxazepam 150 mg/day.
During the hospitalization for pre-surgical check-ups and 2 days before the scheduled surgery date, the patient discharged himself and relapsed. Nine days later, he presented himself to the outpatient facility asking to be “re-enrolled” and gave a new written consent a few days later. The OCCS measurement of craving before surgery was 50/56.
STN-DBS surgery was performed 3 months later. Bilateral electrodes (Medtronic, Minneapolis, 3389 connected to an Activa PC generator) were implanted under general anesthesia. Parameter testing revealed stimulation-induced diplopia on both ventral contacts (0 and 8; >3 V, 60 μs, 130 Hz, all impedances < 2,000 Ω), as well as mild hypomania after 3 h of unipolar stimulation on contact 9 (2.5 V) and dyskinesia/akathisia after 4 h of unipolar stimulation on contact 1 (2.5 V), but not on contact 0 or 2 [see electrode locations (28) in Figure 1].
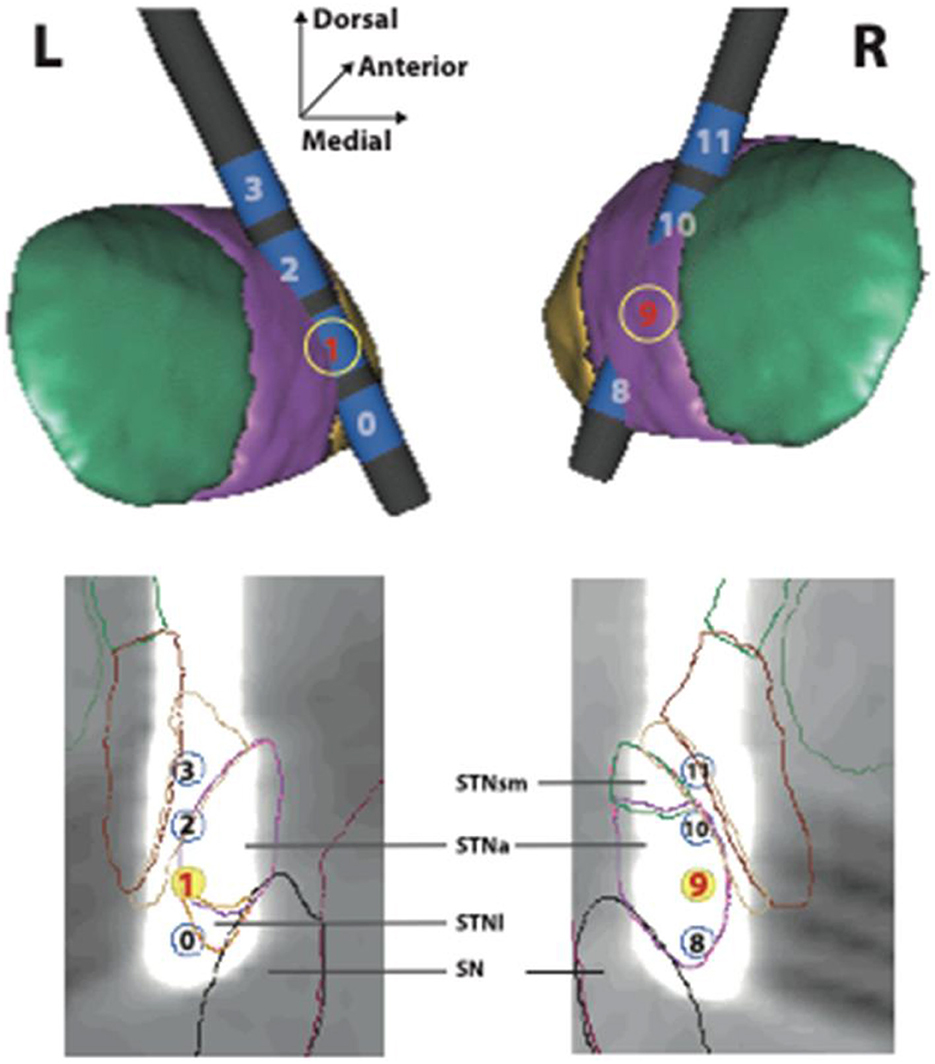
Figure 1. Location of stimulating electrodes in the STN region. Localization of stimulating electrodes. (Upper frame) The left (L) and right (R) subthalamic nuclei are seen from a posterior view on 3D reconstructions from a computerized atlas (24). The sensori-motor (green), associative (purple) and limbic (yellow) subdivisions are shown. The individual electrode contacts (in blue) are numbered (0–3 and 8–11). (Lower frame) The artifact produced by each electrode in the MRI acquisition is shown in a plane of section parallel to its long axis. The exact localization of each contact is indicated in relation to the sensori-motor, associative, limbic subdivisions of the subthalamic nucleus in this plane (STNsm, STNa, STNl). The substantia nigra is also shown (SN).
The double-blind cross-over trial (1 month SHAM, then 1 month ON-DBS) started 1-month post-surgery. During the ON-DBS period, a bilateral unipolar stimulation on contact 1 and 9 at 2 V (60 μs, 130 Hz) was utilized, which was well tolerated. Treatment efficacy on craving could not be assessed due to absence of craving at the baseline (OCCS baseline: 0/56) (see Table 1) and remained low most of the time during this first double-blind cross-over.
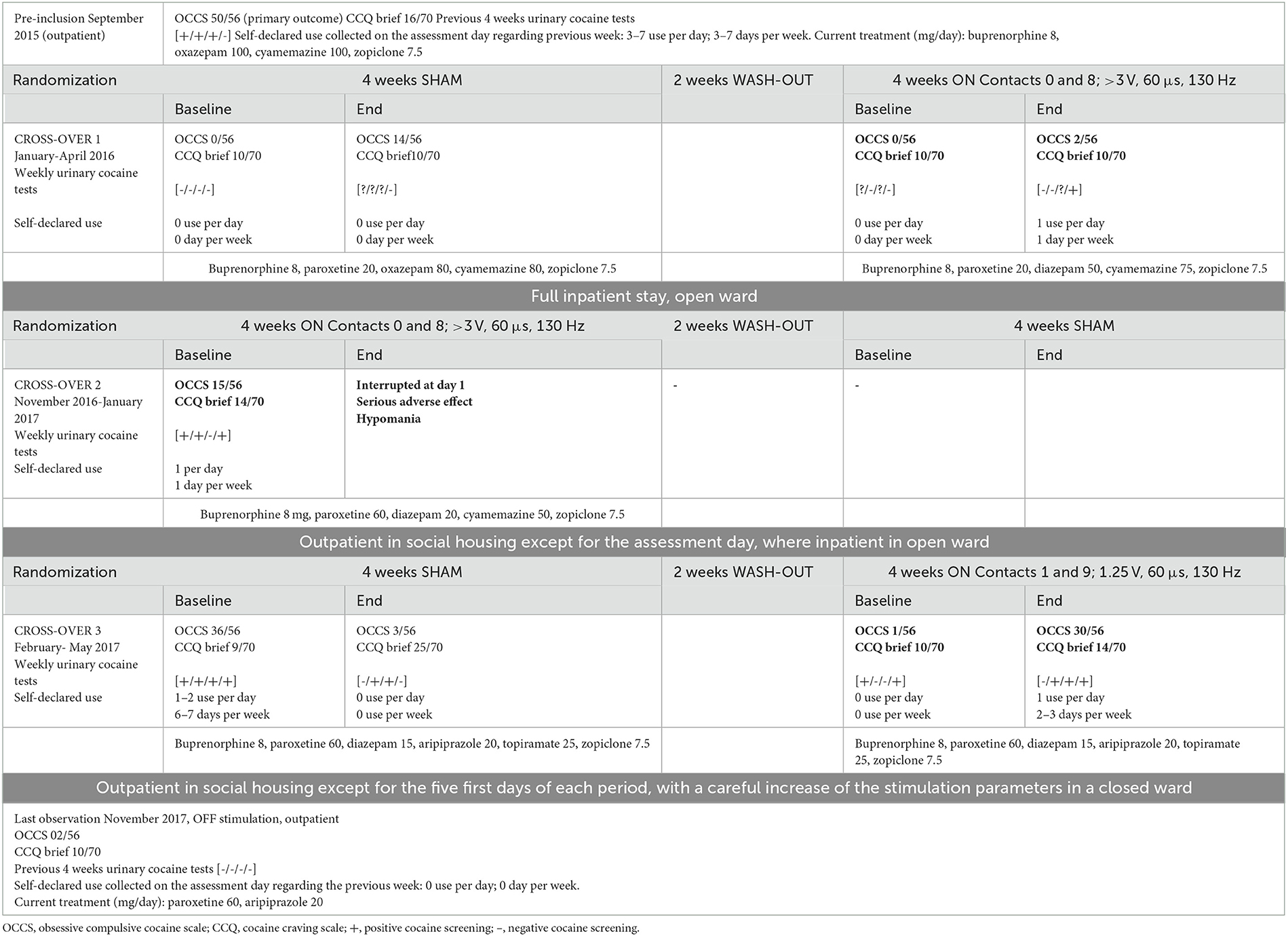
Table 1. Primary and secondary outcomes of STN-DBS in this clinical case.
Because weekly urinary screening was only partially collected, a second crossover was decided and randomized (1 month ON-DBS, then 1 month SHAM). During this second cross-over attempt, the patient lived in a social housing facility and actively smoked crack (declared use 100 mg/day, 3 positive urinary tests in a month), so that he entered the ON-DBS phase with only two weekly urine cocaine free tests. After 12 h ON-DBS, following the same parameter setting protocol as previous, the patient exhibited an unexpected hypomanic episode, became unruly, and left before being brought by the police to the emergency department. When the DBS was turned off the following day, the hypomanic state quickly faded.
Finally, in accordance with the independent safety committee recommendations, and in agreement with the patient who believed that this state was an unprecedent feeling of wellbeing that could be useful to maintain crack abstinence, a third cross-over was initiated (1 month SHAM, then 1 month DBS-ON) with a progressive increase of DBS intensity over 5 days up to a reduced target intensity (contact 1 and 9; 1.25 V, 60 μs, 130 Hz) and performed in a closed ward (see Table 1). No hypomanic state occurred. The patient was discharged with the DBS ON.
During this second cross-over, craving scores fluctuated irrespective of DBS status, with OCCS from baseline to the end of the sham stimulation fluctuating from 36/56 to 3/56, whilst OCCS from baseline to the end of the DBS-ON fluctuating from 1/56 to 30/56. Urinary cocaine tests confirmed an absence of correlation between crack use and STN-DBS status. Indeed, 3 out of 4 weekly urinary cocaine tests were positive at baseline, SHAM-DBS and ON-DBS periods. We could not enroll the patient in the scheduled open-label ON-DBS follow-up because he decided to move back to his family home, located overseas, where DBS could not be safely monitored. Thus, DBS was turned OFF when he finally reached abstinence and moved to his native hometown. His return to his native hometown was a long-standing plan that had been continually thwarted by a lack of funds due to long-term crack cocaine use.
During this trial, the patient was monitored and intensively treated for his substance use disorder over 24 months consisting of 19 months of inpatient treatment, intensive outpatient treatments, including a dedicated social worker, social housing for 5 months, individual CBT, and pharmacological treatment optimization. He maintained alcohol abstinence for 19 months and showed low-risk alcohol use 5 months afterward. After his return to his native town, 6 months after the end of the cross-over and without STN-DBS, the patient was still abstinent from cocaine (and other stimulants), and maintained an abstinence from buprenorphine and other opioids, as well as benzodiazepines and cyamemazine. The patient viewed the treatment trial as a success. However, the trial failed to demonstrate a significant reduction in both craving and cocaine use under STN-DBS set with standard parameters during the double-blind phase of the protocol. This is parsimonious with the only previous DBS double-blind cross-over trial for cocaine dependence that targeted the Nucleus Accumbens, which also found a long term improvement in the absence of any chronological correlation with the DBS-ON phase (11). Importantly, our trial showed a severe adverse event due to STN-DBS that occurred at parameters previously well tolerated. Hypomania has already been observed in two patients under ventral striatum DBS for methamphetamine dependence (10), and is even presented by the authors as a desirable effect to counteract withdrawal-associated depressive symptoms presented by patients suffering from severe methamphetamine dependence. However, this effect was observed at much high stimulation parameters, namely 150 Hz, 210 μs, and 2.5 V in one patient and 165 Hz, 240 μs, and 3.3 V in the other, and occurred from the initiation of stimulation.
Here the patient experimented hypomania at 130 Hz, 60 μs, and 3 V that he had previously tolerated 6 months earlier. The two main differences between the two challenges were that for the second challenge, the patient had used crack recently and that the tapering of several sedative treatments was ongoing when DBS was reapplied. This highlights a possible interaction between the re-start of the STN-DBS and concomitant cocaine intake, which merits further investigation.
Other stimulation parameters also require further investigation. Recent animal studies suggest that low, but not high, frequency STN-DBS can be effective in reducing cocaine intake in a model of compulsive cocaine intake (14). More detailed exploration of the mechanisms associated with DBS treatment response, as suggested by recent data for several other DBS-treated conditions (22), may better refine the ability of STN-DBS to modify the brain network (ventral striatum, dorsolateral prefrontal cortex and orbitofrontal cortex) associated with cue-induced cocaine craving (23). This can be achieved during laboratory sessions, thereby guiding personalized, tailored, progressive parameter settings. Future trials should include a prolonged abstinence period before starting STN-DBS and include progressive voltage increase, over several weeks, in a carefully monitored environment.
We failed to demonstrate a significant decrease in cocaine craving in the DBS-ON, vs. DBS-SHAM, double-blind controlled trial of STN-DBS in one patient with refractory crack cocaine dependence. Over the 2-year treatment period, the patient reduced his crack use and finally reached abstinence. However, this was not correlated with DBS-ON periods. STN-DBS for crack–cocaine dependence may be associated with serious impacts on affective state and should be performed only with caution in crack cocaine therapeutic research trials. Our data will prove of benefit to future treatment interventions, including as to a study design that involves a prolonged abstinence period before initiating STN-DBS, a personalized cue-induced cocaine craving brain network monitoring to choose the best target and a progressive voltage increase over several weeks in a carefully monitored environment.
The datasets presented in this article are not readily available because the generated data belong to the Clinical Research Direction (DRCI) from the Assistance Publique – Hôpitaux de Paris (APHP) and may be accessible upon reasonable request under the restriction of French laws. Requests to access the datasets should be directed to bHVjLm1hbGxldEBpbnNlcm0uZnI=.
The studies involving human participants were reviewed and approved by the Committee for the Protection of People Ile-de-France VI. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
FV and PD wrote the first draft of the manuscript. LM and FV designed the study. FV, PD, CK, HB, DG, and LM collected the data. All authors have actively participated in the manuscript revision and approved the final version.
This work was supported by Ministère de la Santé (France), PHRC-Régional 2011, AOR11036 to LM.
The authors are very grateful to the social workers who were involved in patient care and follow-up: M. Thierry Jouet, Ms. Elodie Denizanne, as well as to the whole team of the social housing facility managed by Association Charonne directed by Dr. Catherine Pequart.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Degenhardt L, Singleton J, Calabria B, McLaren J, Kerr T, Mehta S, et al. Mortality among cocaine users: a systematic review of cohort studies. Drug Alcohol Depend. (2011) 113:88–95. doi: 10.1016/j.drugalcdep.2010.07.026
2. Degenhardt L, Whiteford HA, Ferrari AJ, Baxter AJ, Charlson FJ, Hall WD, et al. Global burden of disease attributable to illicit drug use and dependence: findings from the Global Burden of Disease Study 2010. Lancet. (2013) 382:1564–74. doi: 10.1016/S0140-6736(13)61530-5
3. Cornish JW, O'Brien CP. Crack cocaine abuse: an epidemic with many public health consequences. Annu Rev Public Health. (1996) 17:259–73. doi: 10.1146/annurev.pu.17.050196.001355
4. Goulian A, Jauffret-Roustide M, Dambélé S, Singh R, Fullilove RE. A cultural and political difference: comparing the racial and social framing of population crack cocaine use between the United States and France. Harm Reduct J. (2022) 19:44. doi: 10.1186/s12954-022-00625-5
5. Toledo L, Góngora A, Bastos FIPM. On the sidelines of society: crack use, deviation, criminalization and social exclusion - a narrative review. Cien Saude Colet. (2017) 22:31–42. doi: 10.1590/1413-81232017221.02852016
6. Antoine J, Berndt N, Astudillo M, Cairns D, Jahr S, Jones A, et al. Cocaine treatment demands in 10 western European countries: observed trends between 2011 and 2018. Addiction. (2021) 116:1131–43. doi: 10.1111/add.15237
7. Eiden C, Vincent M, Serrand C, Serre A, Richard N, Picot M, et al. Health consequences of cocaine use in France: data from the French Addictovigilance Network. Fundam Clin Pharmacol. (2020) 35:455–65. doi: 10.1111/fcp.12603
8. Schwartz EKC, Wolkowicz NR, De Aquino JP, MacLean RR, Sofuoglu M. Cocaine use disorder (CUD): current clinical perspectives. Subst Abuse Rehabil. (2022) 13:25–46. doi: 10.2147/SAR.S337338
9. Brandt L, Chao T, Comer SD, Levin FR. Pharmacotherapeutic strategies for treating cocaine use disorder-what do we have to offer? Addiction. (2021) 116:694–710. doi: 10.1111/add.15242
10. Ge S, Chen Y, Li N, Qu L, Li Y, Jing J, et al. Deep brain stimulation of nucleus accumbens for methamphetamine addiction: two case reports. World Neurosurg. (2019) 122:512–7. doi: 10.1016/j.wneu.2018.11.056
11. Gonçalves-Ferreira A, do Couto FS, Rainha Campos A, Lucas Neto LP, Gonçalves-Ferreira D, Teixeira J. Deep brain stimulation for refractory cocaine dependence. Biol Psychiatry. (2016) 79:e87–9. doi: 10.1016/j.biopsych.2015.06.023
12. Zhang C, Wei H, Zhang Y, Du J, Liu W, Zhan S, et al. Increased dopamine transporter levels following nucleus accumbens deep brain stimulation in methamphetamine use disorder: a case report. Brain Stimulation. (2019) 12:1055–7. doi: 10.1016/j.brs.2019.02.023
13. Chang R, Peng J, Chen Y, Liao H, Zhao S, Zou J, et al. Deep brain stimulation in drug addiction treatment: research progress and perspective. Front Psychiatry. (2022) 13:858638. doi: 10.3389/fpsyt.2022.858638
14. Vorspan F, Mallet L, Corvol JC, Pelissolo A, Lépine JP. Treating addictions with deep brain stimulation is premature but well-controlled clinical trials should be performed. Addiction. (2011) 106:1535–6. doi: 10.1111/j.1360-0443.2011.03450.x
15. Rouaud T, Lardeux S, Panayotis N, Paleressompoulle D, Cador M, Baunez C. Reducing the desire for cocaine with subthalamic nucleus deep brain stimulation. Proc Natl Acad Sci USA. (2010) 107:1196–200. doi: 10.1073/pnas.0908189107
16. Pelloux Y, Degoulet M, Tiran-Cappello A, Cohen C, Lardeux S, George O, et al. Subthalamic nucleus high frequency stimulation prevents and reverses escalated cocaine use. Mol Psychiatry. (2018) 23:2266–76. doi: 10.1038/s41380-018-0080-y
17. Degoulet M, Tiran-Cappello A, Combrisson E, Baunez C, Pelloux Y. Subthalamic low-frequency oscillations predict vulnerability to cocaine addiction. Proc Natl Acad Sci USA. (2021) 118:e2024121118. doi: 10.1073/pnas.2024121118
18. Lhommée E, Klinger H, Thobois S, Schmitt E, Ardouin C, Bichon A, et al. Subthalamic stimulation in Parkinson's disease: restoring the balance of motivated behaviours. Brain. (2012) 135:1463–77. doi: 10.1093/brain/aws078
19. Mallet L, Polosan M, Jaafari N, Baup N, Welter ML, Fontaine D, et al. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. N Engl J Med. (2008) 359:2121–34. doi: 10.1056/NEJMoa0708514
20. Mallet L, Du Montcel ST, Clair AH, Arbus C, Bardinet E, Baup N, et al. Long-term effects of subthalamic stimulation in obsessive-compulsive disorder: follow-up of a randomized controlled trial. Brain Stimul. (2019) 12:1080–2. doi: 10.1016/j.brs.2019.04.004
21. Polosan M, Chabardes S, Bougerol T, Ardouin C, Pollak P, Benabid AL, et al. Long-term improvement in obsessions and compulsions with subthalamic stimulation. Neurology. (2016) 87:1843–4. doi: 10.1212/WNL.0000000000003248
22. Tyagi H, Apergis-Schoute AM, Akram H, Foltynie T, Limousin P, Drummond LM, et al. A randomized trial directly comparing ventral capsule and anteromedial subthalamic nucleus stimulation in obsessive-compulsive disorder: clinical and imaging evidence for dissociable effects. Focus. (2022) 20:160–9. doi: 10.1176/appi.focus.20105
23. Skinner MD, Aubin HJ. Craving's place in addiction theory: contributions of the major models. Neurosci Biobehav Rev. (2010) 34:606–23. doi: 10.1016/j.neubiorev.2009.11.024
24. Vorspan F, Brousse G, Bloch V, Bellais L, Romo L, Guillem E, et al. Cocaine-induced psychotic symptoms in French cocaine addicts. Psychiatry Res. (2012) 200:1074–6. doi: 10.1016/j.psychres.2012.04.008
25. Crum RM, Anthony JC. Cocaine use and other suspected risk factors for obsessive-compulsive disorder: a prospective study with data from the Epidemiologic Catchment Area surveys. Drug Alcohol Depend. (1993) 31:281–95. doi: 10.1016/0376-8716(93)90010-N
26. Vorspan F, Bellais L, Romo L, Bloch V, Neira R, Lépine JP. The Obsessive-Compulsive Cocaine Scale (OCCS): a pilot study of a new questionnaire for assessing cocaine craving. Am J Addict. (2012) 21:313–9. doi: 10.1111/j.1521-0391.2012.00248.x
27. Sussner BD, Smelson DA, Rodrigues S, Kline A, Losonczy M, Ziedonis D. The validity and reliability of a brief measure of cocaine craving. Drug Alcohol Depend. (2006) 83:233–7. doi: 10.1016/j.drugalcdep.2005.11.022
28. Bardinet E, Bhattacharjee M, Dormont D, Pidoux B, Malandain G, Schüpbach M, et al. A three-dimensional histological atlas of the human basal ganglia. II. Atlas deformation strategy and evaluation in deep brain stimulation for Parkinson disease: Clinical article. JNS. (2009) 110:208–19. doi: 10.3171/2008.3.17469
Keywords: cocaine dependence, deep brain stimulation, subthalamic nucleus, crack-cocaine, controlled clinical trial
Citation: Vorspan F, Domenech P, Grabli D, Yelnik J, Delavest M, Dauré C, Bellivier F, Pelissolo A, Belaid H, Baunez C, Karachi C and Mallet L (2023) A single case report of STN-DBS for severe crack-cocaine dependence: double-blind ON vs. SHAM randomized controlled assessment. Front. Psychiatry 14:1146492. doi: 10.3389/fpsyt.2023.1146492
Received: 17 January 2023; Accepted: 25 April 2023;
Published: 25 May 2023.
Edited by:
Albino J. Oliveira-Maia, Champalimaud Foundation, PortugalReviewed by:
J. Luis Lujan, Mayo Clinic, United StatesCopyright © 2023 Vorspan, Domenech, Grabli, Yelnik, Delavest, Dauré, Bellivier, Pelissolo, Belaid, Baunez, Karachi and Mallet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florence Vorspan, ZmxvcmVuY2Uudm9yc3BhbkBscmIuYXBocC5mcg==
†Present addresses: Philippe Domenech, Université de Paris Cité, Institut de Neuromodulation, Groupe Hospitalo-Universitaire Paris, Psychiatrie et Neurosciences, Paris, Île-de-France, France
Hayat Belaid, Service de neurochirurgie, Hôpital Fondation Adolphe de Rothschild, Paris, Île-de-France, France
‡These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.