 Claire Maechling
Claire Maechling Antoine Yrondi
Antoine Yrondi Amandine Cambon3
Amandine Cambon3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 12 June 2023
Sec. Schizophrenia
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1137644
This article is part of the Research TopicEarly Psychosis and Early Intervention: Clinical, Functional, and Cognitive OutcomesView all 14 articles
Purpose: The purpose of this systematic literature review is to assess the therapeutic efficacy of mobile health methods in the management of patients with first-episode psychosis (FEP).
Method: The participants are patients with FEP. The interventions are smartphone applications. The studies assess the preliminary efficacy of various types of application.
Results: One study found that monitoring symptoms minimized relapses, visits to A&E and hospital admissions, while one study showed a decrease in positive psychotic symptoms. One study found an improvement in anxiety symptoms and two studies noted an improvement in psychotic symptoms. One study demonstrated its efficacy in helping participants return to studying and employment and one study reported improved motivation.
Conclusion: The studies suggest that mobile applications have potential value in the management of young patients with FEP through the use of various assessment and intervention tools. This systematic review has several limitations due to the lack of randomized controlled studies available in the literature.
The central issues in emerging psychosis are accessing and maintaining effective care. One factor that justifies early intervention is the stage of life at which FEP occurs: late adolescence and early adulthood. This period coincides with a critical phase of development, in which life plans can be disrupted. The aim of early intervention in psychosis (EIP) is to provide recovery-oriented care for young patients with FEP (1).
The first goal of early intervention is to reduce the duration of untreated psychosis (DUP). Long DUP may have a significant social impact, accentuating social withdrawal and stigmatization (1). The other goals concern the prevention of relapse and of unfavorable long-term evolution. The aim is to prevent allowing functional disability and social exclusion to set in (1).
The two main components of EIP are an adapted form of case management and the initiation of treatment as soon as possible after FEP (2).
The deployment of EIP programmes has been an important development in recent decades. Current scientific evidence suggests that these programmes are associated with better outcomes than standard treatment in the early stages of psychosis. A recent meta-analysis including 10 randomized controlled trials on three continents (Europe, North America and Asia) demonstrates the superiority of EIP programmes in terms of treatment discontinuation rates, proportion of patients requiring hospitalization, occupational and educational progression, global functioning and severity of positive and negative symptoms (3).
Patient engagement in care is fragile for psychotic disorders, and FEP in particular. A Swiss study estimated that 50% of patients were lost to follow-up or disengaged after their first hospitalization in a standard psychiatric department (4). The greater the patient's engagement, the lower the risk of relapse. Early intervention programmes aim to involve patients in their care by fostering a therapeutic alliance. AS a result, they limit the traumatic nature of early psychotic experiences (1).
Nevertheless, a significant proportion of patients (20.5%−40%) still drop out of specialized follow-up within the first 2 years (5). Factors associated with disengagement from early intervention programmes are lack of family support, poor adherence to treatment, substance misuse, coming from an ethnic minority and having a criminal record (5, 6). To reduce the risk of disengagement, particular attention should be paid to these factors by offering targeted intervention. These factors at patient level may thus influence engagement, but the level of care provided may also be at the root of patient disengagement. The most common reason given by patients is that the care does not meet their needs (7).
Recovery is now one of main objective in the field of schizophrenia-related disorder (mainly FEP) (8). Recovery includes, amongst others, perceived social integration and empowerment (9). However, individuals with psychosis report experiences of loneliness and social withdrawal (10, 11). The Survey of High Impact Psychosis indicates that loneliness and social withdrawal rank second on the list of challenges to recovery (12–14). Moreover, the face-to-face relationship could be reduced for individuals with psychosis due to a diminution of pleasure (anhedonia) and a sense of threat (15). Schlosser et al. (16) highlighted that internet-based interventions focusing on social connection could decrease social withdrawal in this population. Moreover, young patients going through FEP fear being stigmatized, that clinicians do not acknowledge their experiences and are unable to respond appropriately to their needs (17). Technology can offer the possibility of accessing resources or coping strategies without the fear of the stigma associated with mental health. It can provide platforms for young people to share their experiences and feel supported, provide new ways of working with their careers, allow more accurate assessment of their symptoms and promote positive changes in their daily lives. In addition, mobile health could help patient to increase their own empowerment (18).
Studies in Canada show that most young people admitted for FEP have access to a smartphone (19). A study conducted in an EIP programme in Montreal shows that over 90% of young people diagnosed with FEP have access to a smartphone (20) and many are receptive to using this technology for their mental health care (21). People with FEP report that the use of mobile technologies could be an acceptable way to access mental health information and support, decrease the stigma associated with care and could provide a sense of control over their recovery (referred to internationally as “empowerment”) (22). Most of these young people are open to using technology to receive therapy (21), to get in touch with their peers with similar problems, and they particularly appreciate it when the sites are professionally moderated (23).
The restrictions resulting from the COVID-19 pandemic have heightened the demand for mental health care and imposed a reorganization of our care system by stepping up the use of digital technologies, notably telemedicine (24–26). A 17-country study reports increased use of digital health in mental health care settings, as well as support to facilitate its adoption during the pandemic (27).
Mobile health uses mobile devices such as smartphones to deliver health care. These devices are compact, wireless and universally available at an affordable cost. They provide connectivity, Internet access and multimedia resources at any time and almost anywhere.
The most common mHealth strategies take the form of applications. It is now quite easy to create new applications, find them on online platforms, download them and share them. Mental health applications can be used for Ecological Momentary Assessment (EMA) or Ecological Momentary Intervention (EMI).
EMA is an assessment system that collects data from participants, in their environment and at different times. It includes active data, which generally refers to symptom monitoring questionnaires to be filled in by the individual on their smartphone. It also includes passive data, obtained automatically through sensors on the smartphone or on a wearable device (bracelet or connected watch).
EMI has a similar structure, but the content includes reminders, feedback messages or instructions to adopt specific behaviors or those important for psychotherapy (28). This type of intervention aims to provide support in daily life by sending electronic notifications that encourage therapeutic behaviors at the time they are needed (8). These mobile application-based interventions provide on-demand access to specific therapeutic or psycho-educational tools. Heron and Smyth (29) define these interventions as treatments that are provided to people during their everyday lives (i.e., in real time) and in natural settings (i.e., in the real world). This tool also provides access to a social network. Promising pilot data has been reported for the Moderated Online Social Therapy (MOST) model, an online intervention platform that offers personalized therapy combined with social links and other features. This system combines therapeutic tools, psycho-educational content and a secured, moderated social network. It was developed in Australia by eOrygen, the digital arm of Orygen, The National Center of Excellence in Youth Mental Health, and is led by Professor Mario Alvarez-Jimenez, Chief of Orygen Digital. It is a moderated online social therapy platform that targets 15 to 25-year-olds to improve the social functioning of young people at risk of psychosis (30). The platform can be accessed on mobile phones, tablets and computers. MOST was piloted in Victoria and expanded rapidly in Australia during the COVID-19 pandemic. It consists of a network of peers and expert mental health clinicians. The young patients can also use the platform to interact with other patients.
These tools are used in various ways, ranging from symptom monitoring, medication compliance and promotion of self-management strategies through to access to psycho-education and social relationships.
The evidence to date suggests that smartphone applications could provide an accessible, flexible and inexpensive means of delivering effective self-management interventions for depression and anxiety symptoms (31, 32). A meta-analysis of 18 randomized controlled trials covering 22 mobile applications has shown that using applications for symptom relief significantly reduces patients' depressive symptoms compared with the control group, mainly for people with mild to moderate depression (31). A second meta-analysis of 66 randomized controlled trials found results in favor of intervention groups for depressive symptoms, generalized anxiety and social anxiety (33).
The current published literature on the use of applications in psychosis is more limited. Reviews have highlighted the growing potential of technologies for the treatment of psychosis (26, 34–36) and studies of smartphone applications have shown that they are acceptable and feasible for this population. One review reports the feasibility of using smartphones to improve care for people with schizophrenia, with high rates of engagement and satisfaction over a wide range of applications (34). The FOCUS smartphone intervention study (37) trialed in 2014 on a population of schizophrenic patients shows that the intervention significantly reduces psychotic symptoms.
There are two recent literature reviews on early psychosis: Mar Rus-Calafell and her team summarize the main results of studies between 2009 and 2019 on the use of digital technologies (virtual reality, smartphones and online interventions) to improve the treatment of early psychosis. Most of the studies included are only at the protocol stage and the participants are in an at-risk mental state for psychosis or have FEP (38). The systematic review by Erica Camacho and her team also includes participants in the prodromal and FEP phases. It includes 21 studies: seven papers on protocols, six on feasibility studies, five on validity studies and three on interventions (39). The published literature demonstrates the acceptability and feasibility of interventions. The results show that it is possible to use digital technologies to deliver psychological interventions in the early stages of psychosis, with participants expressing high levels of acceptability and willingness to use them to support their progress and recovery.
To our knowledge, assessment of the therapeutic efficacy of mobile health methods in the management of patients with FEP has not previously been summarized in a systematic review. We have therefore conducted a systematic review of the literature on the preliminary clinical outcomes of digital applications for the support or delivery of treatment for new-onset psychotic disorders. In this literature review, we focus only on patients with FEP and only on one type of technology, mobile smartphone applications that have been developed and validated for acceptability and feasibility. We have focused on studies that assess the preliminary efficacy of this type of tool. In addition, several studies published between 2019 and 2022 have been added. Most of these studies assess the value of adding mobile digital interventions alongside early intervention care or to extend its benefit.
Following the PICO model, the inclusion criteria were: (i) population representing young patients with first-episode psychosis, no more than 5 years after diagnosis; (ii) intervention using a mobile smartphone application; (iii) in comparison with usual care; (iv) paper written in English or French; (v) describing the effects of mobile health interventions in the management of young patients with FEP and (vi) studies assessing clinical outcomes that could be related to intervention objectives.
The exclusion criteria were: (i) any intervention using technology not provided by a smartphone; (ii) papers not published in English or French and literature reviews; (iii) papers describing experimental protocols with no current results or exploratory studies. Papers including patients in an at-risk mental state for psychosis were excluded, to make the patient sample as comparable and homogeneous as possible.
We have studied smartphone applications rather than other digital platforms because of their mobility and accessibility. We have included studies without a control group due to the fact that this literature is in its infancy.
A systematic search of the international literature was carried out using the Pubmed and Embase search engines. The search covered papers published between the creation of the database and 13 May 2022 using a search equation including the following Medical Subject Headings (MESH): (Psychosis OR Schizophrenia) AND (Early Medical intervention) AND (Digital Technology OR smartphone OR mobile applications OR social media OR internet). The references cited in the selected papers were reviewed to identify any additional relevant studies.
Two authors (CM and AC) screened the titles of the publications identified in the databases using the search strategy defined above to identify potentially eligible studies. Both authors, first independently and then jointly, screened the studies based on their abstracts. All online abstracts were reviewed and full-text papers were retrieved where relevant. In case of disagreement, a third author (AY) was called on to arbitrate. This search procedure followed PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (40) (Figure 1).
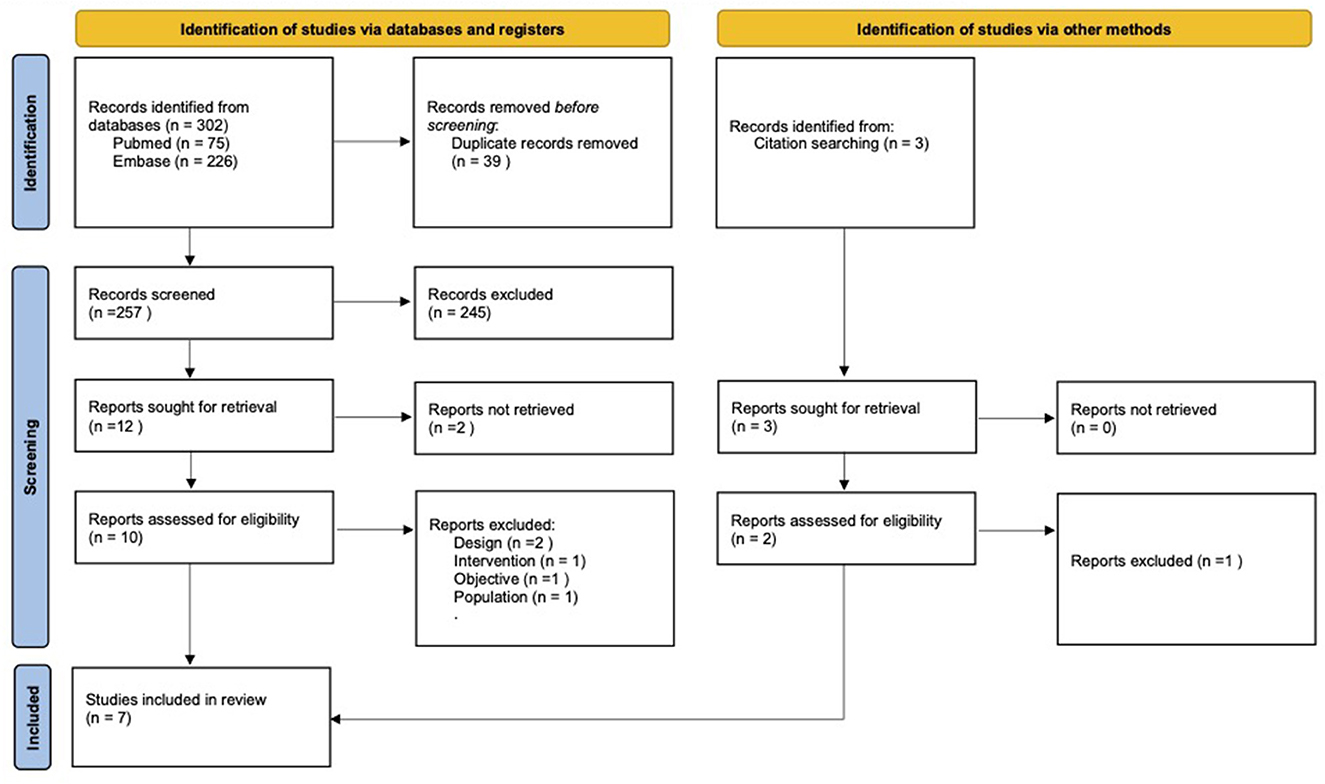
Figure 1. Flow chart of study selection according to PRISMA 2020 guidelines.
To our knowledge, no rigorously validated method of assessing the quality of studies in this field exists. We applied the method using the Jaddad scale (41) that includes: randomization, masking/double blind and a description of losses during follow-up. The variable of the existence or not of a “control group” was added as done by Bonet et al. in the 2017 review to conduct a reproducible analysis of the study quality (18).
The assessment is based on the presence or absence of the following criteria:
1. Randomized.
2. Double blind.
3. Losses.
4. Sufficiently randomized (studies that indicate the randomization technique used (computer-generated table of random numbers, throwing a coin, properly shuffled envelopes, etc.).
5. Sufficiently double blind.
6. Control group.
7. Total.
We considered studies to be of poor quality when they scored < 3 points, and they were considered to be of maximum quality at 5 and 6 points.
The flow chart (Figure 1) describes the study selection process and shows the initial selection of 302 papers and then the selection of 257 papers for in-depth assessment after eliminating duplicates. Two hundred forty-five further papers were excluded after review of their titles and abstracts. Full-text versions were retrieved for 12 papers, of which five were eligible for inclusion. Two further papers were added from the references cited in the papers studied. Hence, a total of seven studies have been included in this review.
The full details of each study are shown in Table 1 (and Supplementary Data S1). Results were available for four randomized controlled trials, one pragmatic clinical trial and two open trials. The average age of the sample was 24.4 years. Smartphone interventions lasted for an average of 25 weeks. Table 1 summarizes the papers included and their characteristics.
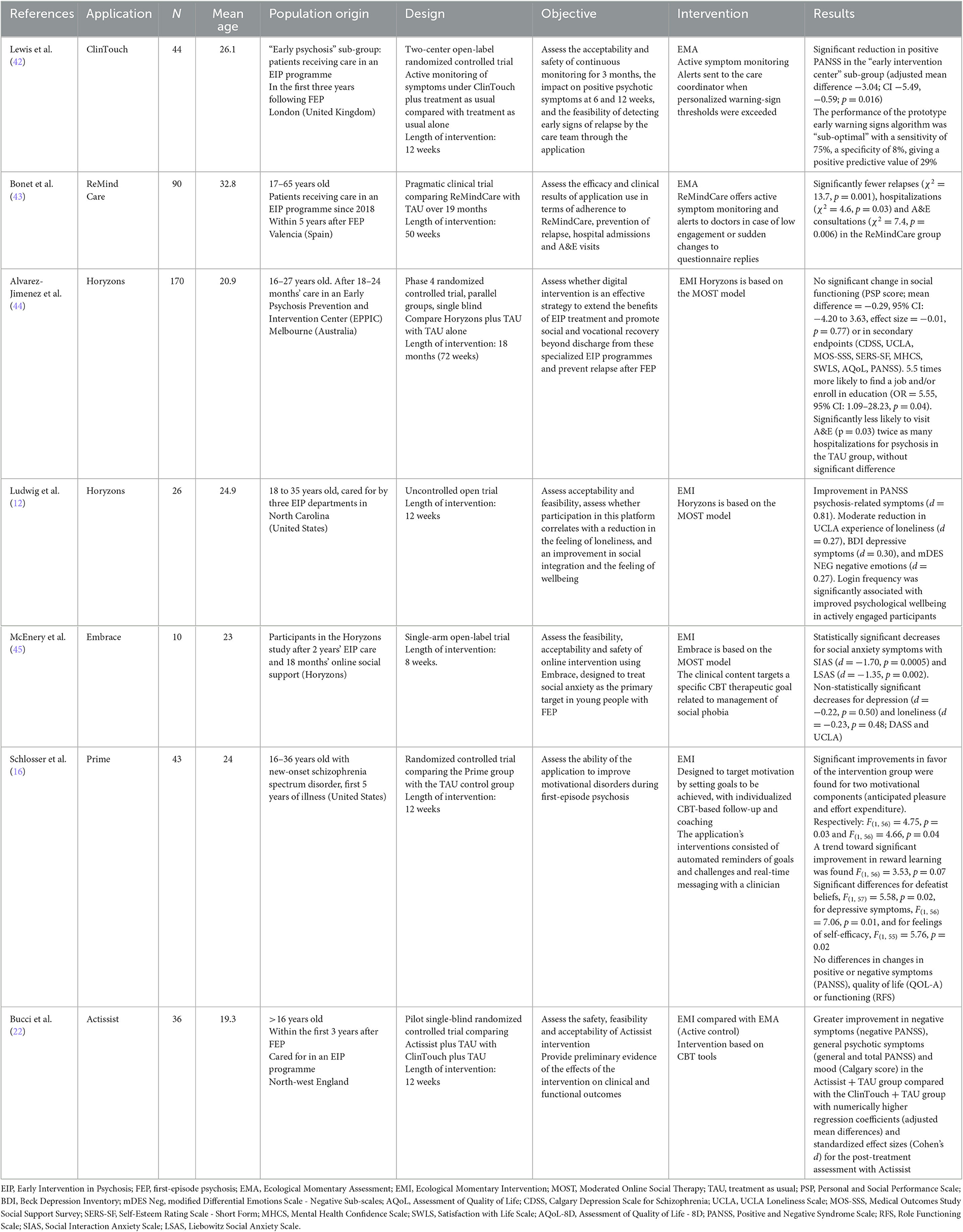
Table 1. Characteristics of seven studies on mobile health (mHealth) in the treatment of first-episode psychosis.
The seven studies assessed smartphone interventions focusing on symptoms monitoring, therapeutic intervention and/or social networks.
No study attained the highest score for methodology, as the lack of blind was their main limitation. In addition, four studies scored < 3 and were considered to be of poor quality (Table 2). Only four of the studies were randomized controlled trials (16, 42, 44, 46), one out of four was from a sub-group (47). The samples included in this study are small and the follow-up periods short. One study used a sample from a previous intervention.
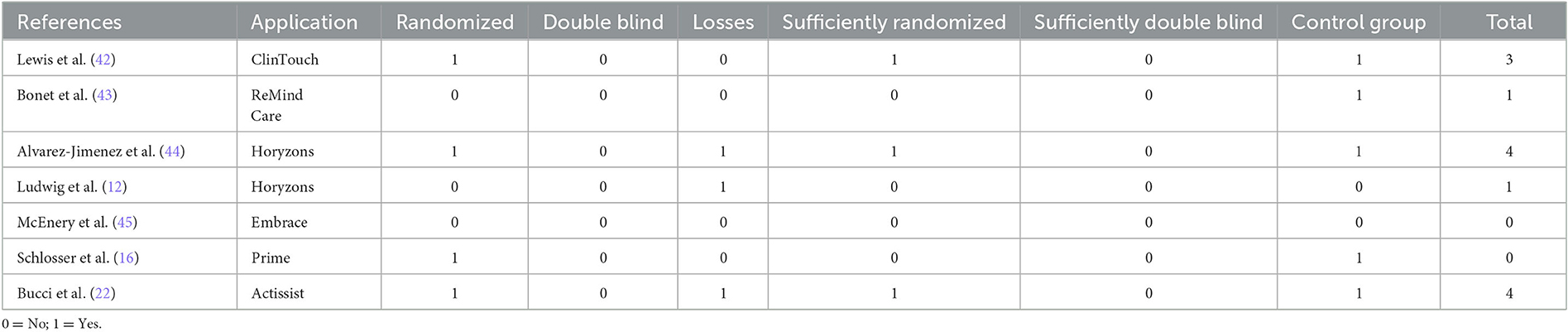
Table 2. The methodological quality of studies analyzed.
The symptom monitoring studied here consists of daily assessment of patients' state of health through short questionnaires covering positive psychotic symptoms, anxiety and mood. The mobile applications can monitor symptoms and may include a secure portal where the clinician receives clinical information. The clinician is thus aware of changes in symptoms and can adjust interventions accordingly, in addition to conventional clinical follow-up (48). Lewis et al. did not show any significant difference between the groups in the total positive PANSS after 6 and 12 weeks, and no difference in secondary endpoints. However, after a separate intention-to-treat analysis for each site, the study shows a significant reduction in positive PANSS after 12 weeks of ClinTouch monitoring in the Early Intervention sub-group (adjusted mean difference −3.04; CI −5.49, −0.59; p = 0.016). The results regarding the performance of the prototype early warning signs algorithm are “sub-optimal” for the accuracy of ClinTouch alerts compared with the warning signs as documented in the electronic patient record, with a sensitivity of 75%, a specificity of 8%, giving a positive predictive value of 29% (42). Bonet et al. (43), showed that after 19 months of using ReMindCare, only 20% of patients in the ReMindCare group suffered a relapse, while 58% of TAU patients had one or more relapses (χ2 = 13.7, p = 0.001). In addition, ReMindCare patients had fewer urgent care unit visits (χ2 = 7.4, p = 0.006) and fewer hospitalizations than TAU patients (χ2 = 4.6, p = 0.03). Of the 59 ReMindCare patients, 31% requested an urgent consultation, 20% relapsed while using the application and 8% developed a delusion involving the application and the research group. After 19 months of intervention, 63% of patients continued using the application, while 12% stopped using the application because they were discharged from the EIP department and 25% opted to stop using ReMindCare. Reasons for discontinuation: 33% of patients felt suspicious about the technology (among these patients, 4 had a relapse while using the application); 40% (6/15) perceived the application as boring and did not perceive any benefit; and 27% (4/15) of patients left treatment and did not continue in the programme. The 2018 Actissist (46) showed greater improvement in negative symptoms (negative PANSS), general psychotic symptoms (general and total PANSS) and mood (Calgary score) in the Actissist + TAU group compared with the ClinTouch + TAU group with numerically higher regression coefficients (adjusted mean differences) and standardized effect sizes (Cohen's d) for the post-treatment assessment with Actissist. The effects were not fully maintained at the 22-week follow-up, though there was no decline in any of the clinical outcomes measured. Focusing on Horyzons project, there was no significant difference in the hospitalization rate and no significant difference in psychotic symptoms. There were no significant changes in secondary endpoints (psychotic symptoms measured by PANSS, depressive symptoms measured by the Calgary Depression Scale for Schizophrenia CDSS, selfesteem measured by the Self-Esteem Rating Scale SERS-SF, selfefficacy measured by the Mental Health Confidence Scale MHCS). In addition, participants assigned to Horyzons were significantly less likely to visit A&E over the 18-month period (p = 0.03) compared with the TAU group. The TAU group had twice as many A&E visits as the Horyzons plus TAU group from baseline to 18 months, a statistically significant difference (39 vs. 19% respectively; OR=0.31, 95% CI: 0.11–0.86, p = 0.03, NNT = 5).The TAU participants had twice as many hospitalizations for psychosis as the Horyzons plus TAU group, without significant difference (27 vs. 13% respectively; OR = 0.36, 95% CI: 0.11–1.08, p = 0.07, NNT = 7). In Horyzons US (12), the results showed an improvement in psychosis-related symptoms (PANSS): large effect size from baseline to mid-treatment (Cohen's d = 0.81) and medium to large effect size from baseline to end of treatment (Cohen's d = 0.65). They also showed a moderate reduction in experiences of depressive symptoms and negative emotions after 6 weeks of using the platform. Self-reported experience of negative emotions (mDES NEG): small to medium effect size between baseline and end of treatment (Cohen's d = 0.27). Depressive symptoms (BDI): small to medium effect size between baseline and mid-treatment (Cohen's d = 0.30). McEnery et al. (47) using Embrace, showed a statistically significant reduction in social anxiety symptoms as measured by the Social Interaction Anxiety Scale [SIAS, (49)] between baseline and the end of the intervention (d = −1.70, p = 0.0005). This significant reduction is also confirmed using the Liebowitz Social Anxiety Scale (50), (d = −1.35, p = 0.002). Finally, non-statistically significant decreases were found for depression (d = −0.22, p = 0.50) the secondary endpoint. Participants reported that the application provides them with a sense of control over their social anxiety symptoms.
The 2018 Prime group (16) did not highlight differences between the groups in changes in positive or negative symptoms (PANSS). In addition, there was a trend toward significant improvement in reward learning, F(1, 56) = 3.53, p = 0.07 and the results showed significant differences for defeatist beliefs, F(1, 57) = 5.58, p = 0.02, for depressive symptoms, F(1, 56) = 7.06, p = 0.01.
Three interventions can monitor symptoms (42, 43, 46). Except Horyzons that did not show any difference focusing on symptoms (44), the others interventions were associated with improvement of general (12, 46), positive (42, 46), negative symptoms (46), mood (12, 16, 46) and anxiety (47). One intervention was associated with a reduction of hospitalization (43) and A&E visits (43, 44).
Horyzons (44) incorporating a moderated social network aimed at recovery after FEP is, to date, the most advanced online psychosocial intervention programme for early psychosis. However, the results showed no difference in social functioning, the primary endpoint. There was no significant change in Personal and Social Performance Scale (PSP) scores at 18 months follow-up (mean difference = −0.29, 95% CI: −4.20 to 3.63, standardized effect size = −0.01, p = 0.77). The level of functioning remained stable for both groups between the start and 18-month follow-up. However, patients in the Horyzons intervention group were 5.5 times more likely to find a job and/or enroll in education compared with the TAU group (OR = 5.55, 95% CI: 1.09–28.23, p = 0.04).
According to a post-hoc analysis, participants in the top quartile of logins (i.e., logging in >77 times) show greater improvement in employment and education outcomes (OR = 59.71; 95% CI: 2.40–1484.37, p = 0.01) compared with those in the bottom quartile of logins (i.e., < 9 logins; OR = 1.40; 95% CI: 0.03–72.40, p = 0.87).
In US version (12), focusing on loneliness (UCLA), they highlighted small to medium effect size between baseline and mid-treatment (Cohen's d = 0.27). Login frequency is significantly associated with improved psychological wellbeing in actively engaged participants. Minimum use of the platform is defined as an average of at least one login per week (12 logins in total) and at least 10 uses of the application (e.g., comments, talking points, etc.). The rate of active participants (patients who met or exceeded this threshold) is 79%, while the rate of inactive participants (patients who did not meet the minimum usage) is 21%. The Embrace programme (45) was associated with a non-statistically significant decreases of loneliness (d = −0.23, p = 0.48) scores.
None study showed an impact on functioning or loneliness scale. However, Horyzons program was associated with a return to working life.
Most of the programs were associated with an engagement range from moderate to high. Six studies highlighted an engagement over 70% (16, 42–44, 46, 47). Moreover, Preliminary findings suggested active engagement in Horyzons was associated with enhanced social integration, improved psychological wellbeing, increased positive emotions, as well as decreased negative emotions and depressive symptoms (12). However, the methods for measuring engagement with the applications were different in each study, making comparisons difficult.
The results of this systematic review provide preliminary evidence for the efficacy of digital mobile applications in the treatment of young patients with FEP. Our review highlighted that mobile health can be used to monitor symptoms (42, 43, 46). Most of programs were associated with an improvement of symptoms (12, 16, 42, 43, 46, 47) and an acceptable engagement (16, 42–44, 46, 47). MHealth seemed have an impact on hospitalization (43) and A&E visits (43, 44) on the one hand and on the return to working life, on the other hand (44). In addition, none program was associated with functioning or social scale.
Regarding interventions based solely on EMA (symptom monitoring) methods, one study found that remote monitoring of symptoms minimized relapses, A&E visits and hospitalizations. The second indicated a reduction in positive psychotic symptoms.
Concerning EMI interventions, one study found an improvement in anxiety symptoms and two studies noted an improvement in psychotic symptoms. One EMI demonstrated its efficacy in helping participants return to studying and employment. One EMI study reported improved motivation. Two out of four studies found no significant changes in psychotic symptoms.
The studies have demonstrated the promising potential of applications in the recovery phase after FEP. They could facilitate self-management of the illness through symptom monitoring by providing instructions for self-management of symptoms in daily life. The addition of therapy modules increases access to evidence-based tools, improves the quality of treatment, facilitates goal achievement and encourages autonomy.
Nevertheless, there are several limitations. Chief among them are internal validity and power.
Moreover, these results should be interpreted with caution as two trials were not controlled, one trial was not randomized (PCT) and we included a sub-group from one trial in an intention-to-treat analysis.
Four studies scored < 3 and were considered to be of poor quality and the three others were considered as moderate quality. These methodological limitations reflect the fact that this field of research is in its infancy. A number of studies identified as relevant for this review were excluded as they did not present preliminary clinical outcome data. They highlight the feasibility and acceptability of a range of additional applications that use the EMA and EMI methods.
It should be noted that the methods for measuring engagement with the applications were different in each study, making comparisons difficult. In addition, engagement may have been encouraged (e.g., through a financial incentive) which may have increased the take-up rate.
Barriers to the implementation of digital technologies in mental health are highlighted (51–54), particularly in the care of new onset psychosis. A number of practical issues are described in relation to digital interventions in psychiatry, including the cost of installing and maintaining equipment and software (technical support, storage, data analysis and technology upgrades), the ability of healthcare IT infrastructures to adapt to new technologies and incorporate them into clinical practice. Cost-effectiveness data has not yet been reported. In addition, new technologies are not progressing at the same pace as clinical trials, which may affect the acceptability of digital interventions (52). A review of engagement with popular commercially available mental health applications found that only 4% of users who downloaded a mental health application reopened it after 15 days (55).
In a paper that reviews the challenges surrounding user engagement with smartphone mental health applications (56), the authors state that “low engagement,” in other words poor adherence to the intervention, represents a major barrier to widespread use of these technologies. In addition, there is no uniformity in the measurement of engagement across the studies. There are no standard measurements to compare engagement with applications in the various papers published and often engagement data is not reported.
Moreover, digital technology tools also raise important ethical issues regarding informed consent, confidentiality, data protection and patient privacy. These factors are all the more important when vulnerable populations and private health information are involved. This is problematic when digital health tools involve the collection of massive amounts of personal data. In a study of the views of patients with psychotic disorders on mobile health, Their first concern was privacy (followed by the reliability of the application) (57). Another study suggests that people with mental health problems are less comfortable with automatically sharing personal data (58). This suggests the importance of a patient-centered approach, and of working closely with future users from the start of any project. A 2016 review examined the specific features of 208 mental health applications and found that only 9% provided data security or privacy protection and 89% made no mention of it. Fifty-nine percent of the applications provided no information on the efficacy of the application (59).
In addition, in 2017, more than 10,000 mental health-related applications were commercially available (60), yet despite the proliferation of health applications, few can be considered to be of good quality. There is currently limited evidence on the value and robustness of the theoretical foundations provided by the applications (61). Research in 2019 found that only 3% of commercially available mental health applications had an evidence base to support their claims of efficacy (61, 62). In addition, access to these interventions is still restricted for non-English speaking populations.
There is no regulation or consensus on health applications and few guidelines or standards on which to base application research and quality assessment. The disparity in the quality of mobile applications has stimulated the development of assessment tools. The American Psychiatric Association (APA) has developed a model to help clinicians improve informed decision-making about mental health applications: the “APA App Advisor” (63). It assesses the accessibility, confidentiality, safety, clinical basis, ease of use and data integration of the tool in terms of a therapeutic goal.
The Mobile Application Rating Scale (MARS) is another tool that aims to provide a standardized assessment of mental health applications for clinicians (64). The “uMARS” version has been developed for users. In 2019, the World Health Organization (WHO) published a guide to pilot and assess digital solutions and help harmonize practices, with summary tables of the different methodological approaches according to the clinical assessment goals of these applications.
Nevertheless, it remains difficult for users and clinicians to identify the quality and usefulness of the applications available.
In future, passive data and personalized interventions could improve the use of mHealth. The term “active data” refers to data generated through the active involvement of a patient, such as self-questionnaires, while “passive data” refers to data generated without the patient's involvement (GPS, accelerometer, voice calls and SMS) (65). The many sensors built into smartphones offer a wealth of data, such as GPS to monitor spatial location, an accelerometer to record movement and overall motor activity, call and messaging histories to document social activity, voice and sound recordings to estimate mood, a camera for facial expression. The sensors may be on the smartphone or on a wearable device (a connected watch or bracelet). Often referred to as “digital phenotyping,” passive monitoring provides a means of understanding mental health experiences in context.
Qualitative data from studies on the ClinTouch application report that some patients find the self-questionnaires repetitive (66). This may lead to disengagement in the longer term. Researchers are currently investigating whether passive monitoring of psychotic relapse indicators using sensor technologies embedded in smartphones may be more acceptable to users and more responsive to change than active self-assessment. The Crosscheck system (67) is currently being developed and tested by Dr Ben-Zeev's team, to detect changes in speech properties, physical activity and location to generate personalized alert patterns. An early prototype of the system appears to be acceptable to participants with psychosis, although the research team notes that self-selection is likely: those who are concerned about such monitoring will choose not to participate in the tests. If successful, Crosscheck could be used to signal a potential relapse and trigger an early intervention response in the same way as ClinTouch (52). The Crosscheck application combines the use of active EMA data with passive data such as physical activity (accelerometer), geospatial activity (GPS), speech frequency and duration (microphone) and phone use (telecommunication, application use, screen unlocking) to predict relapse in people with psychosis. The results of the study reveal that the digital indicators of relapse are not the same for each person with psychosis.
In the study by Cella et al. (68), the investigators combine active and passive digital technology using a wrist-worn device (the Empatica E4) and the ClinTouch application. The study assessed whether there was a link between psychotic symptoms and a physiological response. The results showed increased electrodermal activity during hallucinations or delusions, but no association between symptoms and heart rate variability. This study suggests that it may be possible to identify a reliable biosignature indicating worsening symptoms and a risk of relapse.
Other research supports the feasibility of digital phenotyping in psychotic disorders, such as the study of the Beiwe application (69). This study suggests that 2 weeks before relapse, people with schizophrenia show significant changes in mobility indicators derived from GPS data, sociability indicators derived from text messages and call data, and symptom exacerbation indicators derived from self-assessment surveys within the application. This indicates that it may be possible to capture digital indicators of relapse. The rate of behavioral abnormalities detected in the 2 weeks prior to relapse is 71% higher than the rate of abnormalities in other periods.
As Torous points out (51), this could help to understand the heterogeneity of clinical presentation and offer a more personalized understanding of psychotic illness. Smartphones and other portable devices can now capture real-time environmental data on behavioral indicators. This data offers potential insights into how symptoms can lead to clinical presentations such as social withdrawal and anhedonia via changes in call/text reciprocity, or avolition and lethargy via changes in GPS-tracked movements (70). This wealth of readily available information offers a new perspective to better characterize the lived experience of people with FEP and to explore new subtypes and clusters of psychoses based on new data.
Digital technologies could also be used to predict illness trajectory: smartphones and related mobile devices offer a means of capturing daily fluctuations in the multitude of indicators needed to better understand, model and predict the trajectory of the illness. It remains to be seen whether this means of data capture is acceptable to users and whether it risks increasing the symptoms of paranoia in people with psychotic disorders.
This objective measure of digital phenotyping occurs in the context of patients' lived experience, reflecting how they function in their environment. The smartphone may be an opportunity to measure real-world functioning and potentially offer real-time interventions (71). In just-in-time adaptive intervention (JITAI), active and passive data is collected to help develop personalized, real-time intervention strategies. For example, the smartphone can deduce low mood in the context of social isolation and suggest a relevant intervention, while if it deduces low mood in the context of poor sleep, it can recommend an alternative intervention. While still in its infancy, the use of JITAI to deliver mental health interventions would be an interesting area for future research (72).
A major opportunity offered by digital technology is to improve engagement, especially among young people. Gamification is promising in this respect (73), e.g., by adapting the techniques of digital gaming, offering rewards and challenges to complete activities. The most commonly observed gamification features in mental health are: progress tracking; points; rewards; introduction of themes or stories; personalization; configuration (74). The addition of gaming features could support engagement, increasing motivation, creating a sense of empowerment and inducing positive emotional responses in users, such as a sense of pride.
The use of mobile applications for smartphones represents an interesting prospect for improving the engagement of FEP patients receiving care (75). A meta-analysis (76) assessing the opinions of 1,172 psychotic patients on mHealth services reports that 60.2% of users are in favor of using mobile phones to track and monitor their mental health and 51.1% to facilitate contact with health professionals. The study shows that this population is interested in this type of tool to facilitate the link between patient and healthcare department.
In a study assessing interest in new technologies among psychotic patients, the service of most interest to patients was the “contact alarm to clinicians in case of emergency” (77). Patients demand more personalized, more interactive and closer clinical attention. However, as noted in the studies, when it comes to the clinical implications associated with these interventions, it is very important to design these systems from the clinician's perspective. In a study exploring the attitude of mental healthcare staff in England to digital health interventions, staff expressed concern about their moral, legal and professional obligations in relation to assessing information about risks such as suicidal ideas and behavior. They preferred patients to report symptoms themselves during consultations. Not only did staff feel that this would give patients control over the information they share, but also that their level of responsibility would be minimized. This somewhat contradicts the current focus of smartphone applications for symptom monitoring in this population, which, although they can be used by patients to share with their care team, tend to provide symptom reports to a central server that staff can use to identify early signs of relapse. Issues surrounding the legal and moral responsibilities of staff when viewing automatic symptom reports and their level of comfort in implementing such approaches in practice must be considered (78).
These various limitations need to be considered when jointly building new technologies with the people affected by FEP to ensure that the technologies are appropriate and that they will be used. Among the possible solutions identified to increase young people's interest in quality applications, the inclusion of users in the development process is essential, involving them in development of the objectives, the planned functions and the design of the application.
One prospect that shows promise concerns case management follow-up with a mobile application used jointly by patients and case managers. The Heal Your Mind application (79), currently under development, offers case management based on CBT techniques and symptom monitoring for young people with FEP. Surveys have shown that most participants use at least five of the six modules, find the application easy to use and express satisfaction with the tool. The feature that is most frequently used, most highly appreciated and perceived as most useful is communication with the case manager.
The French Plan-e-Psy project, led by Dr Frederic Haesebaert, aims to work with people affected by FEP and their families to jointly build a monitoring application in the context of case management. The protocol describes improvement in patient functioning as the primary endpoint (80). It aims to allow both the case manager and the patient to plan and monitor the achievement of individualized care goals. The assumption is that the use of such an application will improve the functioning of patients receiving care for FEP. This randomized, multi-center clinical trial will include 168 participants aged 18–30 with first-episode psychosis. The results are expected in January 2024.
Schizophrenia is one of the most severe psychiatric illnesses. It is frequent and still too often incapacitating. Clinical research in recent years has shown that early intervention leads to a more favorable evolution of this illness. Mobile health could also have a role to play in changing and enhancing the quality of care for psychosis. It could provide new opportunities to increase access to existing mental health resources, improve the quality of treatment and enhance the provision of mental health care. The future of mobile technology in mental health care is indeed gaining momentum in the literature. Preliminary data on efficacy is emerging in the literature.
Mobile health could help make users more autonomous and take greater responsibility for their own care, through monitoring and assessing symptoms and facilitating self-management strategies. This autonomy does not imply the replacement of health professionals, but would instead optimize their contribution by providing assistance in caring for patients. It could promote patient involvement in healthcare in general by encouraging them to be actors in their own care, enhancing their empowerment.
The use of technology for therapeutic purposes has the potential to increase access to standard treatments and to allow greater patient choice and control. It can offer the choice of a wide range of therapeutic interventions, personalized resources, psycho-education and various types of specialized therapy tools. These interventional applications can be personalized to address individual issues in real time and promote functional recovery. They could also facilitate peer support and social integration by providing secure social networking platforms.
Applications could be clinically incorporated into existing healthcare environments to provide patients with FEP with new tools and ways to engage in care by facilitating connections to clinical care. Smartphone-based symptom monitoring could be incorporated into electronic patient record systems and regular clinical monitoring to generate clinically usable information and predictions for preventive and personalized care. New models of healthcare could take advantage of these technologies while preserving the therapeutic relationship and including patients in the tool development process.
The literature highlights many of the challenges facing this new field of research, including ethical issues, cost, and the capacity of healthcare infrastructure, along with doubts about the quality of applications on the market. The rapid pace of technological development is at odds with the long scientific process required to develop a quality application. Clinical evidence for the efficacy of applications is currently limited. The lack of quality validation is one of the main problems. The rapid expansion of the mobile health sector makes it difficult for users to choose and for professionals to recommend the right application. On the other hand, these technological advances can make applications more attractive and improve results. To facilitate this, future research can explore barriers and potential solutions, focusing particularly on feedback from users and healthcare providers.
Mobile applications are emerging as interesting tools for better engagement in care, enhanced self-management of symptoms and better coordination of resources. This systematic review has several limitations due to the lack of randomized controlled studies. Overall, the studies to date suggest promising preliminary efficacy data on the use of mobile applications in early psychosis. Given the importance placed on early intervention in psychosis, the implementation of technologies for therapeutic purposes in young adult populations in the early stages of psychosis seems essential. While engagement is a challenge in traditional clinical practice, technological progress can enhance the engagement of young people in particular.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
CM and AC conceived the study and screened the titles of the publications identified in the databases using the search strategy defined above to identify potentially eligible studies. Both authors, first independently and then jointly, screened the studies based on their abstracts. All online abstracts were reviewed and full-text papers were retrieved where relevant. In case of disagreement, a AY was called on to arbitrate. CM wrote the initial draft and all tabular material. AC and AY supervised the study and critically revised the manuscript. All authors read and agreed to the published version of the manuscript.
AY received speaker's honoraria from AstraZeneca, Janssen, Lundbeck, Otsuka, Servier, and carried out clinical studies in relation to the development of medicine Janssen and Lundbeck medicine unrelated to this work.
The remaining authors declare the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1137644/full#supplementary-material
1. Lecardeur L. Troubles Psychotiques : Protocoles d'intervention Précoce: Le Guide du Clinicien. Amsterdam: Elsevier Health Sciences (2019), p. 224.
2. Malla A, Roy M-A, Abdel-Baki A, Conus P, McGorry P. Intervention précoce pour les premiers épisodes psychotiques d'hier à demain : comment relever les défis liés à son déploiement pour en maximiser les bénéfices? Santé Ment Au Qué. (2021) 46:391–415. doi: 10.7202/1088190ar
3. Correll CU, Galling B, Pawar A, Krivko A, Bonetto C, Ruggeri M, et al. Comparison of early intervention services vs treatment as usual for early-phase psychosis. JAMA Psychiatry. (2018) 75:555–65. doi: 10.1001/jamapsychiatry.2018.0623
4. Bonsack C, Pfister T, Conus P. Insertion dans les soins après une première hospitalisation dans un secteur pour psychose. L'Encéphale. (2006) 32:679–85. doi: 10.1016/S0013-7006(06)76219-4
5. Doyle R, Turner N, Fanning F, Brennan D, Renwick L, Lawlor E, et al. First-episode psychosis and disengagement from treatment: a systematic review. Psychiatr Serv. (2014) 65:603–11. doi: 10.1176/appi.ps.201200570
6. Mascayano F, van der Ven E, Martinez-Ales G, Henao AR, Zambrano J, Jones N, et al. Disengagement from early intervention services for psychosis: a systematic review. Psychiatr Serv. (2021) 72:49–60. doi: 10.1176/appi.ps.201900375
7. Smith TE, Easter A, Pollock M, Pope LG, Wisdom JP. Disengagement from care: perspectives of individuals with serious mental illness and of service providers. Psychiatr Serv. (2013) 64:770–5. doi: 10.1176/appi.ps.201200394
8. Roe D, Mashiach-Eizenberg M, Lysaker PH. The relation between objective and subjective domains of recovery among persons with schizophrenia-related disorders. Schizophr Res. (2011) 131:133–8. doi: 10.1016/j.schres.2011.05.023
9. Lloyd C, King R, Moore L. Subjective and objective indicators of recovery in severe mental illness: a cross-sectional study. Int J Soc Psychiatry. (2010) 56:220–9. doi: 10.1177/0020764009105703
10. Badcock JC, Shah S, Mackinnon A, Stain HJ, Galletly C, Jablensky A, et al. Loneliness in psychotic disorders and its association with cognitive function and symptom profile. Schizophr Res. (2015) 169:268–73. doi: 10.1016/j.schres.2015.10.027
11. Stain HJ, Galletly CA, Clark S, Wilson J, Killen EA, Anthes L, et al. Understanding the social costs of psychosis: the experience of adults affected by psychosis identified within the second Australian National Survey of Psychosis. Aust N Z J Psychiatry. (2012) 46:879–89. doi: 10.1177/0004867412449060
12. Ludwig KA, Browne JW, Nagendra A, Gleeson JF, D'Alfonso S, Penn DL, et al. Horyzons USA: a moderated online social intervention for first episode psychosis. Early Interv Psychiatry. (2021) 15:335–43. doi: 10.1111/eip.12947
13. Lim MH, Gleeson JFM, Alvarez-Jimenez M, Penn DL. Loneliness in psychosis: a systematic review. Soc Psychiatry Psychiatr Epidemiol. (2018) 53:221–38. doi: 10.1007/s00127-018-1482-5
14. Morgan VA, Waterreus A, Carr V, Castle D, Cohen M, Harvey C, et al. Responding to challenges for people with psychotic illness: updated evidence from the Survey of High Impact Psychosis. Aust N Z J Psychiatry. (2017) 51:124–40. doi: 10.1177/0004867416679738
15. Schneider M, Reininghaus U, van Nierop M, Janssens M, Myin-Germeys I, GROUP Investigators. Does the Social Functioning Scale reflect real-life social functioning? An experience sampling study in patients with a non-affective psychotic disorder and healthy control individuals. Psychol Med. (2017) 47:2777–86. doi: 10.1017/S0033291717001295
16. Schlosser DA, Campellone TR, Truong B, Etter K, Vergani S, Komaiko K, et al. Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophr Bull. (2018) 44:1010–20. doi: 10.1093/schbul/sby078
17. Gronholm PC, Thornicroft G, Laurens KR, Evans-Lacko S. Mental health-related stigma and pathways to care for people at risk of psychotic disorders or experiencing first-episode psychosis: a systematic review. Psychol Med. (2017) 47:1867–79. doi: 10.1017/S0033291717000344
18. Bonet L, Izquierdo C, Escartí MJ, Sancho JV, Arce D, Blanquer I, et al. Use of mobile technologies in patients with psychosis: a systematic review. Rev Psiquiatr Salud Ment. (2017) 10:168–78. doi: 10.1016/j.rpsmen.2017.05.010
19. Lal S, Dell'Elce J, Malla AK. Technology access and use among young adults with a first episode of psychosis. Psychiatr Serv. (2015) 66:764–5. doi: 10.1176/appi.ps.201400580
20. Abdel-Baki A, Lal S, D-Charron O, Stip E, Kara N. Understanding access and use of technology among youth with first-episode psychosis to inform the development of technology-enabled therapeutic interventions. Early Interv Psychiatry. (2017) 11:72–6. doi: 10.1111/eip.12250
21. Lal S, Dell'Elce J, Tucci N, Fuhrer R, Tamblyn R, Malla A. Preferences of young adults with first-episode psychosis for receiving specialized mental health services using technology: a survey study. JMIR Ment Health. (2015) 2:e18. doi: 10.2196/mental.4400
22. Bucci S, Morris R, Berry K, Berry N, Haddock G, Barrowclough C, et al. Early psychosis service user views on digital technology: qualitative analysis. JMIR Ment Health. (2018) 5:e10091. doi: 10.2196/10091
23. Lal S, Nguyen V, Theriault J. Seeking mental health information and support online: experiences and perspectives of young people receiving treatment for first-episode psychosis. Early Interv Psychiatry. (2018) 12:324–30. doi: 10.1111/eip.12317
24. Kola L. Global mental health and COVID-19. Lancet Psychiatry. (2020) 7:655–7. doi: 10.1016/S2215-0366(20)30235-2
25. Torous J, Keshavan M. COVID-19, mobile health and serious mental illness. Schizophr Res. (2020) 218:36–7. doi: 10.1016/j.schres.2020.04.013
26. Torous J, Bucci S, Bell IH, Kessing LV, Faurholt-Jepsen M, Whelan P, et al. The growing field of digital psychiatry: current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry. (2021) 20:318–35. doi: 10.1002/wps.20883
27. Kinoshita S, Cortright K, Crawford A, Mizuno Y, Yoshida K, Hilty D, et al. Changes in telepsychiatry regulations during the COVID-19 pandemic: 17 countries and regions' approaches to an evolving healthcare landscape. Psychol Med. (2022) 52:2606–13. doi: 10.1017/S0033291720004584
28. Baños RM, Herrero R, Vara MD. What is the Current and future status of digital mental health interventions? Span J Psychol. (2022) 25:e5. doi: 10.1017/SJP.2022.2
29. Heron KE, Smyth JM. Ecological momentary interventions: Incorporating mobile technology into psychosocial and health behaviour treatments. Br J Health Psychol. (2010) 15:1–39. doi: 10.1348/135910709X466063
30. Rice S, Gleeson J, Leicester S, Bendall S, D'Alfonso S, Gilbertson T, et al. Implementation of the Enhanced Moderated Online Social Therapy (MOST+) model within a national youth E-mental health service (eheadspace): protocol for a single group pilot study for help-seeking young people. JMIR Res Protoc. (2018) 7:e48. doi: 10.2196/resprot.8813
31. Firth J, Torous J, Nicholas J, Carney R, Pratap A, Rosenbaum S, et al. The efficacy of smartphone-based mental health interventions for depressive symptoms: a meta-analysis of randomized controlled trials. World Psychiatry. (2017) 16:287–98. doi: 10.1002/wps.20472
32. Firth J, Torous J, Nicholas J, Carney R, Rosenbaum S, Sarris J. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. (2017) 218:15–22. doi: 10.1016/j.jad.2017.04.046
33. Linardon J, Cuijpers P, Carlbring P, Messer M, Fuller-Tyszkiewicz M. The efficacy of app-supported smartphone interventions for mental health problems: a meta-analysis of randomized controlled trials. World Psychiatry. (2019) 18:325–36. doi: 10.1002/wps.20673
34. Firth J, Torous J. Smartphone apps for schizophrenia: a systematic review. JMIR MHealth UHealth. (2015) 3:e102. doi: 10.2196/mhealth.4930
35. Bell IH, Lim MH, Rossell SL, Thomas N. Ecological momentary assessment and intervention in the treatment of psychotic disorders: a systematic review. Psychiatr Serv. (2017) 68:1172–81. doi: 10.1176/appi.ps.201600523
36. Craig TK, Rus-Calafell M, Ward T, Leff JP, Huckvale M, Howarth E, et al. therapy for auditory verbal hallucinations in people with psychosis: a single-blind, randomised controlled trial. Lancet Psychiatry. (2018) 5:31–40. doi: 10.1016/S2215-0366(17)30427-3
37. Ben-Zeev D, Brenner CJ, Begale M, Duffecy J, Mohr DC, Mueser KT. Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull. (2014) 40:1244–53. doi: 10.1093/schbul/sbu033
38. Rus-Calafell M, Schneider S. Are we there yet?!—a literature review of recent digital technology advances for the treatment of early psychosis. mHealth. (2020) 6:3. doi: 10.21037/mhealth.2019.09.14
39. Camacho E, Levin L, Torous J. Smartphone apps to support coordinated specialty care for prodromal and early course schizophrenia disorders: systematic review. J Med Internet Res. (2019) 21:e16393. doi: 10.2196/16393
40. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
41. Halpern S, Douglas MJ. Jadad scale for reporting randomized controlled trials. In:Halpern SH, Douglas MJ, , eds. Evidence-based Obstetric Anesthesia. Oxford, UK: Blackwell Publishing Ltd (2007), 237–8.
42. Lewis S, Ainsworth J, Sanders C, Stockton-Powdrell C, Machin M, Whelan P, et al. Smartphone-enhanced symptom management in psychosis: open, randomized controlled trial. J Med Internet Res. (2020) 22:e17019. doi: 10.2196/17019
43. Bonet L, Torous J, Arce D, Blanquer I, Sanjuan J. ReMindCare app for early psychosis: pragmatic real world intervention and usability study. JMIR MHealth UHealth. (2020) 8:e22997. doi: 10.2196/22997
44. Alvarez-Jimenez M, Koval P, Schmaal L, Bendall S, O'Sullivan S, Cagliarini D, et al. The Horyzons project: a randomized controlled trial of a novel online social therapy to maintain treatment effects from specialist first-episode psychosis services. World Psychiatry. (2021) 20:233–43. doi: 10.1002/wps.20858
45. McEnery C, Lim MH, Knowles A, Rice S, Gleeson J, Howell S, et al. Development of a moderated online intervention to treat social anxiety in first-episode psychosis. Front Psychiatry. (2019) 10:581. doi: 10.3389/fpsyt.2019.00581
46. Bucci S, Barrowclough C, Ainsworth J, Machin M, Morris R, Berry K, et al. Actissist: proof-of-concept trial of a theory-driven digital intervention for psychosis. Schizophr Bull. (2018) 44:1070–80. doi: 10.1093/schbul/sby032
47. McEnery C, Lim MH, Knowles A, Rice S, Gleeson J, Howell S, et al. Social anxiety in young people with first-episode psychosis: pilot study of the EMBRACE moderated online social intervention. Early Interv Psychiatry. (2021) 15:76–86. doi: 10.1111/eip.12912
48. Thibaudeau E, Raucher-Chéné D, Lecardeur L, Cellard C, Lepage M, Lecomte T. Les interventions psychosociales destinées aux personnes composant avec un premier épisode psychotique : une revue narrative et critique. Santé Ment Au Qué. (2021) 46:217–47. doi: 10.7202/1088184ar
49. Mattick RP, Clarke JC. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav Res Ther. (1998) 36:455–70. doi: 10.1016/S0005-7967(97)10031-6
50. Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry. (1987) 22:141–73. doi: 10.1159/000414022
51. Torous J, Woodyatt J, Keshavan M, Tully LM. A new hope for early psychosis care: the evolving landscape of digital care tools. Br J Psychiatry J Ment Sci. (2019) 214:269–72. doi: 10.1192/bjp.2019.8
52. O'Hanlon P, Aref-Adib G, Fonseca A, Lloyd-Evans B, Osborn D, Johnson S. Tomorrow's world: current developments in the therapeutic use of technology for psychosis. BJPsych Adv. (2016) 22:301–10. doi: 10.1192/apt.bp.115.014654
53. Bell I, Pot-Kolder RMCA, Wood SJ, Nelson B, Acevedo N, Stainton A, et al. Digital technology for addressing cognitive impairment in recent-onset psychosis: a perspective. Schizophr Res Cogn. (2022) 28:100247. doi: 10.1016/j.scog.2022.100247
54. Ouellet-Morin I, Robitaille M-P, Juster R-P. Applications mobiles pour soutenir la santé mentale des jeunes : opportunités et défis. Santé Ment Au Qué. (2021) 46:17–34. doi: 10.7202/1081508ar
55. Baumel A, Muench F, Edan S, Kane JM. Objective user engagement with mental health apps: systematic search and panel-based usage analysis. J Med Internet Res. (2019) 21:e14567. doi: 10.2196/14567
56. Torous J, Nicholas J, Larsen ME, Firth J, Christensen H. Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evid Based Ment Health. (2018) 21:116–9. doi: 10.1136/eb-2018-102891
57. Torous J, Wisniewski H, Liu G, Keshavan M. Mental health mobile phone app usage, concerns, and benefits among psychiatric outpatients: comparative survey study. JMIR Ment Health. (2018) 5:e11715. doi: 10.2196/11715
58. Matteo DD, Fine A, Fotinos K, Rose J, Katzman M. Patient willingness to consent to mobile phone data collection for mental health apps: structured questionnaire. JMIR Ment Health. (2018) 5:e9539. doi: 10.2196/mental.9539
59. Radovic A, Vona PL, Santostefano AM, Ciaravino S, Miller E, Stein BD. Smartphone applications for mental health. Cyberpsychol Behav Soc Netw. (2016) 19:465–70. doi: 10.1089/cyber.2015.0619
60. Torous J, Roberts LW. Needed innovation in digital health and smartphone applications for mental health: transparency and trust. JAMA Psychiatry. (2017) 74:437–8. doi: 10.1001/jamapsychiatry.2017.0262
61. Huckvale K, Nicholas J, Torous J, Larsen ME. Smartphone apps for the treatment of mental health conditions: status and considerations. Curr Opin Psychol. (2020) 36:65–70. doi: 10.1016/j.copsyc.2020.04.008
62. Marshall JM, Dunstan DA, Bartik W. The digital psychiatrist: in search of evidence-based apps for anxiety and depression. Front Psychiatry. (2019) 10:831. doi: 10.3389/fpsyt.2019.00831
63. Torous JB, Chan SR, Gipson SY-MT, Kim JW, Nguyen T-Q, Luo J, et al. Hierarchical framework for evaluation and informed decision making regarding smartphone apps for clinical care. Psychiatr Serv. (2018) 69:498–500. doi: 10.1176/appi.ps.201700423
64. Terhorst Y, Philippi P, Sander LB, Schultchen D, Paganini S, Bardus M, et al. Validation of the mobile application rating scale (MARS). PLoS ONE. (2020) 15:e0241480. doi: 10.1371/journal.pone.0241480
65. Torous J, Staples P, Onnela J-P. Realizing the potential of mobile mental health: new methods for new data in psychiatry. Curr Psychiatry Rep. (2015) 17:602. doi: 10.1007/s11920-015-0602-0
66. Palmier-Claus JE, Rogers A, Ainsworth J, Machin M, Barrowclough C, Laverty L, et al. Integrating mobile-phone based assessment for psychosis into people's everyday lives and clinical care: a qualitative study. BMC Psychiatry. (2013) 13:34. doi: 10.1186/1471-244X-13-34
67. Ben-Zeev D, Brian R, Wang R, Wang W, Campbell AT, Aung MSH, et al. CrossCheck: integrating self-report, behavioral sensing, and smartphone use to identify digital indicators of psychotic relapse. Psychiatr Rehabil J. (2017) 40:266–75. doi: 10.1037/prj0000243
68. Cella M, He Z, Killikelly C, Okruszek Ł, Lewis S, Wykes T. Blending active and passive digital technology methods to improve symptom monitoring in early psychosis. Early Interv Psychiatry. (2019) 13:1271–5. doi: 10.1111/eip.12796
69. Barnett I, Torous J, Staples P, Sandoval L, Keshavan M, Onnela J-P. Relapse prediction in schizophrenia through digital phenotyping: a pilot study. Neuropsychopharmacology. (2018) 43:1660–6. doi: 10.1038/s41386-018-0030-z
70. Torous J, Staples P, Barnett I, Sandoval LR, Keshavan M, Onnela J-P. Characterizing the clinical relevance of digital phenotyping data quality with applications to a cohort with schizophrenia. NPJ Digit Med. (2018) 1:15. doi: 10.1038/s41746-018-0022-8
71. Insel TR. Digital phenotyping: a global tool for psychiatry. World Psychiatry. (2018) 17:276–7. doi: 10.1002/wps.20550
72. Nahum-Shani I, Smith SN, Spring BJ, Collins LM, Witkiewitz K, Tewari A, et al. Just-in-time adaptive interventions (JITAIs) in mobile health: key components and design principles for ongoing health behavior support. Ann Behav Med Publ Soc Behav Med. (2018) 52:446–62. doi: 10.1007/s12160-016-9830-8
73. Cugelman B. Gamification: what it is and why it matters to digital health behavior change developers. JMIR Serious Games. (2013) 1:e3. doi: 10.2196/games.3139
74. Cheng VWS, Davenport T, Johnson D, Vella K, Hickie IB. Gamification in apps and technologies for improving mental health and well-being: systematic review. JMIR Ment Health. (2019) 6:e13717. doi: 10.2196/13717
75. Lal S, Malla A. Service engagement in first-episode psychosis: current issues and future directions. Can J Psychiatry Rev Can Psychiatr. (2015) 60:341–5. doi: 10.1177/070674371506000802
76. Firth J, Cotter J, Torous J, Bucci S, Firth JA, Yung AR. Mobile phone ownership and endorsement of “mHealth” among people with psychosis: a meta-analysis of cross-sectional studies. Schizophr Bull. (2016) 42:448–55. doi: 10.1093/schbul/sbv132
77. Bonet L, Llácer B, Hernandez-Viadel M, Arce D, Blanquer I, Cañete C, et al. Differences in the use and opinions about new eHealth technologies among patients with psychosis: structured questionnaire. JMIR Ment Health. (2018) 5:e9950. doi: 10.2196/preprints.9950
78. Berry N, Bucci S, Lobban F. Use of the internet and mobile phones for self-management of severe mental health problems: qualitative study of staff views. JMIR Ment Health. (2017) 4:e8311. doi: 10.2196/mental.8311
79. Kim S-W, Lee G-Y, Yu H-Y, Jung E-I, Lee J-Y, Kim S-Y, et al. Development and feasibility of smartphone application for cognitive-behavioural case management of individuals with early psychosis. Early Interv Psychiatry. (2018) 12:1087–93. doi: 10.1111/eip.12418
80. Haesebaert F, El Oussoul S, Pavard A, Fabre D, Cellard C, Magaud L, et al. PLAN-e-PSY, a mobile application to improve case management and patient's functioning in first episode psychosis: protocol for an open-label, multicentre, superiority, randomised controlled trial. BMJ Open. (2021) 11:e050433. doi: 10.1136/bmjopen-2021-050433
Keywords: early psychosis, first-episode psychosis, early intervention, mobile health, mobile applications, digital intervention, smartphone
Citation: Maechling C, Yrondi A and Cambon A (2023) Mobile health in the specific management of first-episode psychosis: a systematic literature review. Front. Psychiatry 14:1137644. doi: 10.3389/fpsyt.2023.1137644
Received: 04 January 2023; Accepted: 23 May 2023;
Published: 12 June 2023.
Edited by:
Wing Chung Chang, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Ana Carolina Guidorizzi Zanetti, University of São Paulo, BrazilCopyright © 2023 Maechling, Yrondi and Cambon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antoine Yrondi, YW50b2luZXlyb25kaUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.