 Andrew A. McDonnell
Andrew A. McDonnell Marion C. O’Shea2
Marion C. O’Shea2 Stephanie J. Bews-Pugh
Stephanie J. Bews-Pugh- 1Birmingham City University, Birmingham, United Kingdom
- 2Studio 3 Clinical Services Limited, Alcester, United Kingdom
- 3Tizard Centre, University of Kent, Canterbury, United Kingdom
Background: Restrictive practices are used frequently by frontline staff in a variety of care contexts, including psychiatric hospitals, children’s services, and support services for older adults and individuals with intellectual and developmental disabilities. Physical restraint has been associated with emotional harm, physical injury to staff and consumers, and has even resulted in death of individuals in care environments. Various interventions have been implemented within care settings with the intention of reducing instances of restraint. One of the most common interventions is staff training that includes some physical intervention skills to support staff to manage crisis situations. Despite physical intervention training being used widely in care services, there is little evidence to support the effectiveness and application of physical interventions. This review will examine the literature regarding outcomes of staff training in physical interventions across care sectors.
Method: A systematic search was conducted following PRISMA guidelines using Cochrane Database, Medline EBSCO, Medline OVID, PsychINFO, and the Web of Science. Main search keywords were staff training, physical intervention, physical restraint. The MMAT was utilised to provide an analytical framework for the included studies.
Results and discussion: Seventeen articles have been included in this literature review. The included studies take place in a range of care settings and comprise a wide range of outcomes and designs. The training programmes examined vary widely in their duration, course content, teaching methods, and extent to which physical skills are taught. Studies were of relatively poor quality. Many descriptions of training programmes did not clearly operationalise the knowledge and skills taught to staff. As such, it is difficult to compare course content across the studies. Few papers described physical interventions in sufficient detail. This review demonstrates that, although staff training is a ‘first response’ to managing health and safety in care settings, there is very little evidence to suggest that staff training in physical intervention skills leads to meaningful outcomes.
Introduction
Rationale
The physical restraint, mechanical restraint, and seclusion of individuals in care environments is controversial. Restrictive practices are used frequently by frontline staff in a variety of care settings, including psychiatric hospitals, children’s services, and support services for older adults and individuals with learning disabilities and developmental disorders (1). Restrictive practices can be defined as those that limit freedom of movement, and include involuntary admission, enforced treatment, seclusion, and physical, chemical or mechanical restraint (2). There are ethical and legal issues around the use of restrictive practices that limit human rights, such as freedom of movement and freedom of choice (2). Organisational policies often state that restraints should be reduced and used as the ‘last resort’ (3), while training in physical interventions is frequently presented as a method of reducing the use of restrictive practices, staff training in physical interventions has had limited research emphasis over the years (1, 4).
Manual, mechanical and chemical restraint are in use across care sectors around the world. In a study that looked at acute psychiatric wards in a county in Norway over an eight-year period it was found that restraint was used on 1.7% of admitted patients per year (5). However, rates of restraint can vary quite dramatically. A study looked at nationwide rates of restraint in Pacific Rim countries in which the law requires these are reported and published. Rates of mechanical restraint varied between 0.03 restraint events per million population in New Zealand, 0.17 in Australia, 0.37 in the United States and 98.9 restraint in Japan, representing a variation greater than 3,000 fold (6). A critical review by Fitton and Jones (7) found rates of physical and mechanical restraint varied between 11–78% for periods over 1 year for people with intellectual disabilities living in services (7). In England, National Audit survey data of over 500 National Health Service (NHS) and independent services for people with intellectual disabilities, Sturmey (8) reported that 53% of service-users had been subjected to physical restraints and 10% to seclusion.
Use of restraint and other restrictive practices in schools for children with special educational needs is difficult to determine. A United Kingdom wide survey of families with a child with disabilities carried out by the Challenging Behaviour Foundation (CBF) found that 88% of families reported their child had experienced physical restraint, with 35% reporting that it happened regularly. Seventy-one per cent of the 204 respondents to the CBF survey reported their child had experienced seclusion, 21% of those said this was on a daily basis (9). Services for older adults have shown that incidences of manual and mechanical restraint are not always reported or recorded (10). Issues of definition likely have an impact on reporting. Some restrictive practices are viewed as necessary means to ‘maintain patients’ safety,’ these include the use of bedrails, or leaving a mobility aid out of reach to prevent a patient from ‘wandering.’ While such practices amount to physical restraints they often go unreported (11).
The use of restraint can lead to serious physical harm. In the United States, Weiss (12) reported on 142 deaths in 50 states showing shocking neglect and uncaring use of force, disproportionately impacting young people. Patterson et al. (13) have shown continuing evidence of deaths associated with restraint in the United Kingdom, as well as worldwide. Kersting et al. (14) conducted a systematic review looking at physical harms and death associated with restrictive practices, and found that death, followed by deep vein thrombosis, were the two most common reported physical harms. Emotional harm is also associated with restrictive practices. In a recent literature review, Chieze et al. (2) examined the use of seclusion and restraint in psychiatric services and estimated that incidence of post-traumatic stress disorder (PTSD) following being subjected to these practices is between 25 to 47%. In a systematic review of qualitative studies, Askew et al. (15) note that during seclusion service-users within psychiatric services report feeling vulnerable, neglected, abused, and disconnected, and conclude that seclusion is a risk to mental health. There is an increasing focus on the views of consumers by researchers, and it is becoming increasingly apparent that those on the receiving end of restrictive practices suffer physical and emotional injuries (16–18).
A number of interventions have been implemented in the effort to reduce the use of restrictive practices within care settings. Gaskin et al. (19) undertook a systematic review which included 14 single person case studies. Interventions included staff training, increasing service-users’ preferred activities, and increasing service-users’ choice and control. Restraint and seclusion showed average reductions of 75% in frequency and of 45% in duration, following intervention. Mindfulness training for staff, focusing on self-management and interactional style, has been reported as leading to decreases in use of restraints (20). Post incident review has been reported to decrease use of restraint in some cases, however in other cases it has been reported to increase use of restraint (21). Multi-component models that include a focus on senior leadership, feedback from frontline staff, target setting, outcomes monitoring, and staff training have been shown to reduce the use of restraint (22, 23).
Staff training in crisis management that includes teaching of physical interventions is a common approach in care services (24). Training aims to equip front line staff to safely manage aggressive behaviour, and typically includes both theoretical and practical components, covering topics such as understanding causes of behaviours, recognizing early warning signs, de-escalation techniques and instruction in physical interventions such as physical restraints (25–28). In the United Kingdom, Beech and Leather (29) reviewed the literature regarding workplace violence within healthcare settings and demonstrated that aggression management training is an established health and safety response in most organisations. Whilst training in physical interventions may well be a relatively commonplace response, the evidence for its effectiveness is limited. There have been claims made about a number of variables, including increased confidence (30–34), improved knowledge (30, 35), reduction in staff and patient injuries (36), and reduction in staff illness. While government guidelines and local policies imply that physical interventions are used as a last resort (2), staff training may not always lead to reductions in their use. There is some limited evidence that training in crisis management may even increase the use of physical interventions (37). The development, content, and impact of various training programmes are difficult to explore as many programmes have been modified and renamed over the years (38).
Objectives and research question
There has been an increasing emphasis in the literature on the reduction of restraint and other restrictive practices (39). In the United Kingdom, the Restraint Reduction Network (RNN) has been attempting to highlight the issues surrounding restrictive practices for people with intellectual disabilities, autism, and other related conditions. If we are to adopt an evidence-based approach to restraint reduction, this will require an understanding of organisational, cultural, and training issues. There have been a limited number of literature reviews that have focused on staff training in physical interventions and its impact (1, 4, 40). The literature is regarded as limited in nature with poorly designed studies (4, 24, 29). Given the importance of reducing restrictive practices, an understanding of the evidence-base for staff training in physical interventions is urgently required. In view of the prevalence of the use of restraint within care settings, its associated harm, and that staff training is an established health and safety response employed within care settings, physical interventions training is a suitable focus for evaluation by systematic review. This review will examine a selected published literature in order to establish the current evidence base for outcomes of staff training in physical interventions across care sectors.
Methods
Search methods for identification of studies
Using the Cochrane Database, Medline EBSCO, Medline OVID, PsychINFO, and the Web of Science a systematic literature search was conducted of empirical studies described in English speaking articles published up to January 2021, which examined the effectiveness of staff training in physical interventions within any healthcare service. The search equation was defined using the Boolean connectors “AND” and “OR” following the formulation “staff training” AND “physical intervention” OR (“physical restraint,” “aggression,” “violence” AND “learning disability,” “intellectual disability,” “developmental disability,” “mental handicap,” “elderly,” “education,” “psychiatry,” “mental health,” “disruptive behaviour”). To broaden our search, websites of 17 training organisations that deliver training services for people with a learning disability in the United Kingdom were examined for evidence of relevant research in staff training in physical interventions. Furthermore, we performed a manual search of the reference list of all studies selected for the review.
Inclusion and exclusion criteria
Articles were selected for inclusion in the review if they met the following criteria: (i) they were published in a peer reviewed journal; (ii) there was evidence that staff training had taken place and included training in physical interventions (iii) the study utilised a control or a comparison group.
Final studies included
Due to the heterogeneity of the studies, a formal quantitative synthesis (i.e., meta-analysis) was not possible. Instead, a systematic review was conducted using the Preferred Reporting for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (41). The initial search identified 204 papers. 190 papers remained after duplicates were removed. These papers were examined against the inclusion and exclusion criteria, resulting in 173 papers being excluded. 17 papers remained and are included in the literature review. A clear description of the process can be seen in the PRISMA flow diagram (Figure 1). Included studies were further checked for methodological quality by using the Mixed Methods Appraisal Tool (MMAT) and an overall quality score between 1 (indicating relatively poor quality) and 5 (indicating relatively high quality) was assigned to each study (42).
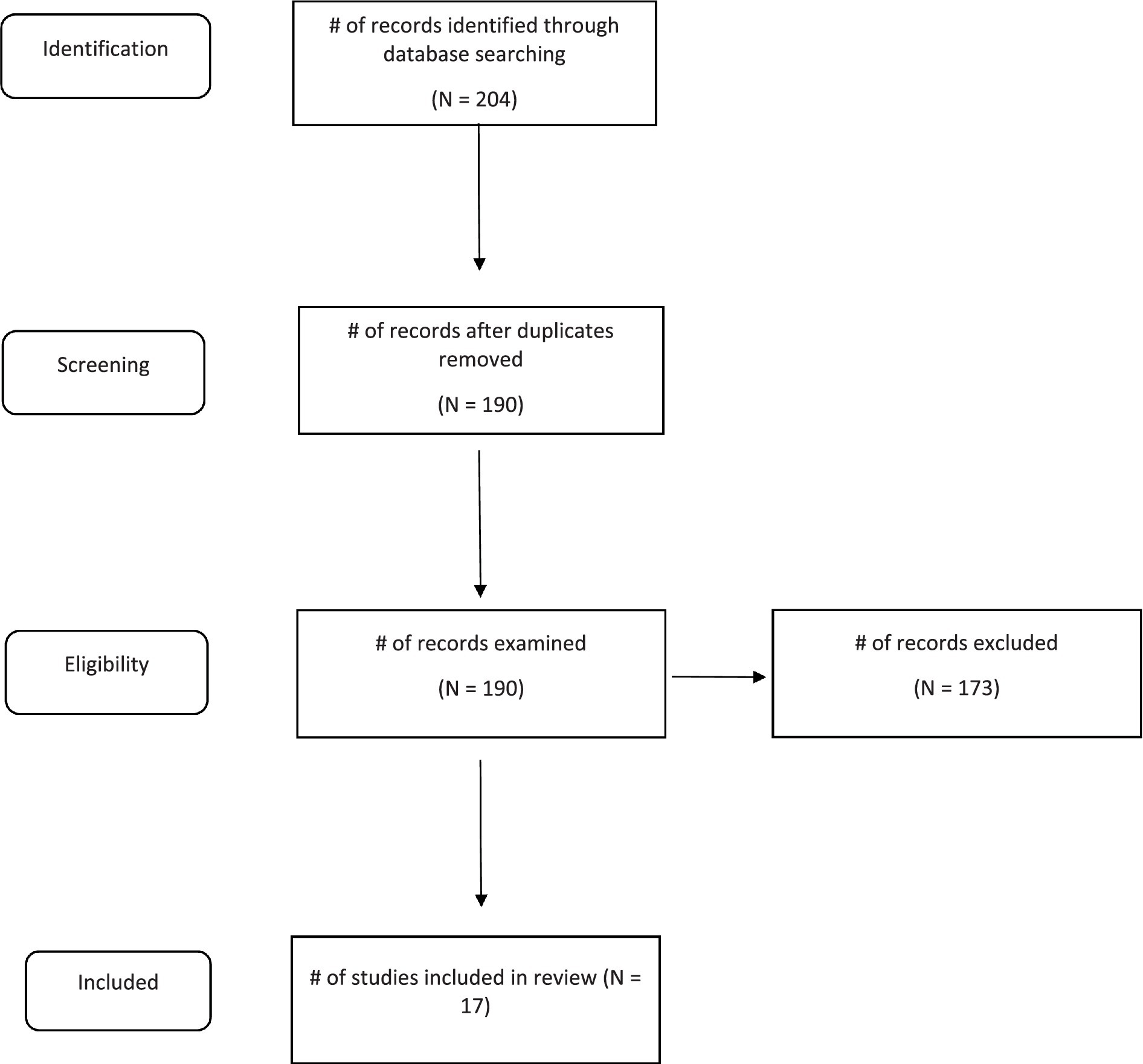
Figure 1. PRISMA flow diagram.
Results
Seventeen studies met inclusion criteria and are included in the literature review. Table 1 presents titles of training courses, setting, course content, physical interventions taught, and teaching methods described across the studies. A summary of study designs, measures utilised, and outcomes reported can be seen in Table 2.
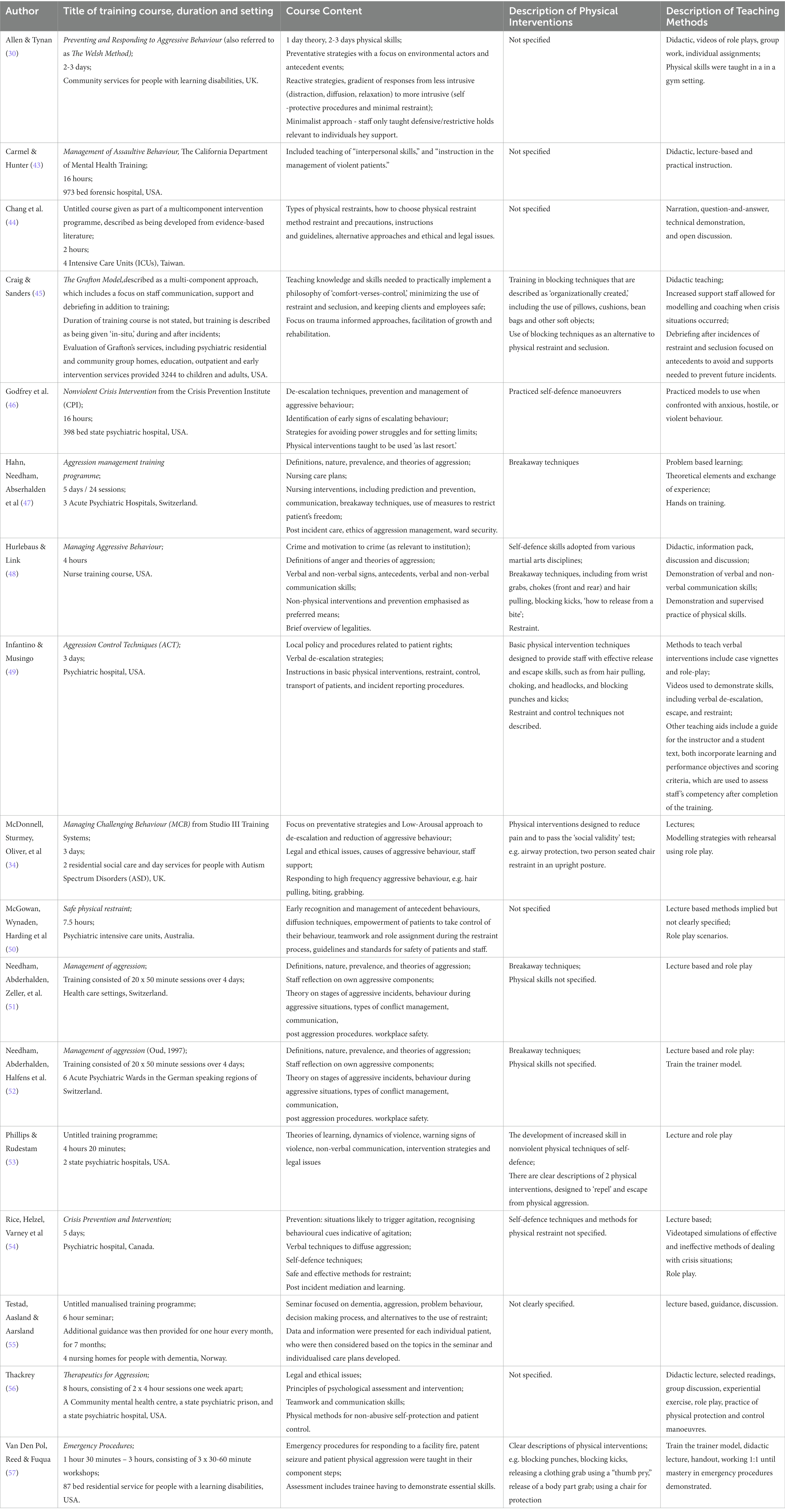
Table 1. Course content, physical interventions taught, and teaching methods described.

Table 2. Study design, measures utilised, and outcomes reported.
Descriptions of settings and client-groups
Studies took place in a variety of settings and with different population groups (see Table 1). Ten studies were carried out in adult psychiatric settings (43, 46, 47, 49–54, 56); three in adult learning disabilities settings (30, 45, 57); one in a service for older adults (55); and one in a service for adults with autism (34). Two studies took place in general hospitals (44, 48), one of which was an Intensive Care Unit (ICU) (44). Craig and Sanders (45) examined multiple services provided by one organisation for children and adults with intellectual and developmental disabilities and psychiatric needs. Studies were conducted in a variety of locations, including the United States (43, 45, 46, 48, 49, 56, 57); Switzerland (47, 51, 52); United Kingdom (30, 34); Canada (53, 54); Australia (50); Taiwan (44); and Norway (55). The number of participants in each study varied widely from thirteen (57) to 1,488 (43).
Training systems utilized
The majority of physical intervention training is provided under a brand name by commercial organisations (see Table 1). Two studies (46, 54), reported using a training course from the Crisis Prevention Institute (CPI). Three studies (47, 51, 52), reported using the Aggression Management Training Programme (Oud, 1997). One study reported using each of the following branded training: Studio III training (34); The Welsh Method (30); The Grafton Method (45) Aggression Control Techniques (ACT) (49); Management of Assaultive Behaviour (43); Safe Physical Restraint (50); Therapeutics for Aggression (56); and Emergency Procedures (57). Four studies did not describe a recognised training programme (44, 48, 53, 55).
The duration of the training courses ranged from less than 1 day to more than 5 days. Five studies reported training courses that were less than 1 day (44, 45, 48, 53, 57); three reported providing 1 day workshops (50, 55, 56); two reported 2 day courses, (43, 46); two reported 3 day courses (34, 49); one study specified two to 3 days training depending on need (30); and four reported five or more day courses (47, 51, 52, 54).
Teaching methods
A variety of teaching methods were described (see Table 1). Twelve studies reported using lecture or classroom-based formats (30, 34, 43, 44, 46–48, 51, 53–56). Four studies reported utilising groupwork or discussions, such as question and answer sessions (30, 44, 48, 56). Three studies reported use of audio-visual aids (30, 49, 54). Ten studies reported using role-play (30, 34, 49, 50–54, 56, 57). One study referred to ‘hands on training,’ but no further details were provided (47). One study reported using behavioural skills training (57). Two studies made reference to the use of additional teaching materials, such as manuals, incident books and theoretical information (48, 49). Two studies referred to physical demonstrations of physical restraint skills (44, 46). Two studies did not clearly outline teaching methods (45, 46).
Course content
Diffusion strategies were reported to have been taught on 14 training courses (30, 34, 43–46, 48–56). Four of these studies reported training in communication skills, including verbal and nonverbal, and psychological de-escalation techniques (45, 46, 48, 52). Another study discussed that training included a consideration of precautions when choosing a restraint method, consideration of alternative approaches, and ethical and legal issues (44). One study described training that included imparting knowledge and skills needed to practically implement a philosophy of comfort versus control (45).
In general, the included studies did not provide clear descriptions of physical interventions, with only three studies clearly describing the physical techniques taught (34, 53, 57). Nine studies did not provide a list of the specific physical interventions taught on training courses (43, 46, 47, 50, 51, 54–56), and five studies referred to other source materials to describe their physical interventions (30, 34, 45, 51, 52).
Four studies used the term ‘breakaway skills’ or ‘breakaway techniques’ to describe physical disengagement skills (46–48, 52); although two of these (47, 52) subsequently did not describe teaching skills or techniques which would usually be regarded as physical disengagement skills. Two training programmes referred to ‘self-defence manoeuvres’ (44, 46). Craig and Sanders (2018) described blocking techniques and alternative methods including the use of pillows, cushions, beanbags and other soft objects to deflect kicks, hits and slaps (45). A total of seven breakaway or ‘disengagement’ techniques were described in five studies in regards to: hair pulling (34, 48, 49); choking or strangulation (34, 48, 53); punching (49, 53, 57); wrist grabs (34, 48); biting, (34, 48); kicking (49); and headlocks (49).
Statistical analysis
Twelve studies reported reliability data for at least their main dependent measures (30, 34, 43, 44, 47, 50–54, 56, 57). Five studies did not report reliability data for their main dependent measures (45, 46, 48, 49, 55). One study reported reliability data for staff knowledge measures (30). One study used a patient restraint written test with high inter-rater reliability, but reported no test–retest reliability measures (54). One study reported validity and reliability for a questionnaire on knowledge about physical restraint (44). Five studies used measures of staff confidence with acceptable reliability (30, 34, 47, 50, 56), while two studies did not report on reliability for this measure (48, 51).
Seven studies solely used parametric statistics (34, 43, 46, 48, 53, 54, 56), six studies used nonparametric statistics only (30, 47, 49, 50, 52, 55), and one study used a combination of parametric and non-parametric statistical analyses (51). Two studies reported descriptive statistics (45, 57). One study was unspecified ‘General Estimation Equation’ (44).
Statistical significance was reported in 15 studies (30, 34, 43, 44, 46–56). Two studies reported descriptive statistics only (45), (57): Craig and Sanders (45) was a relatively large-scale study, whereas Van den Pol et al. (57) was a small study reporting on a training intervention for 13 participants.
Methodological quality of the studies
Due to the small number of selected articles and their variability in design quality, sample sizes and statistical analysis, it was decided not to compare these studies in terms of statistical power and rank order them in terms of quality. The MMAT (39) facilitated a degree of statistical analysis to provide further qualitative interpretation. Table 3 reports the characteristics of studies as assessed by the MMAT. Thirteen of the 17 studies included control groups to evaluate the efficacy of the training programmes (30, 44, 47–57). Two of these utilised a randomised control trial (51, 55). The remaining four studies included comparison groups for evaluation of the training programmes used (34, 43, 45, 46). The study conducted by Craig and Saunders (45) met the inclusion criteria for comparison groups as one of the settings they sampled was acquired during the course of the study, which provided a natural opportunity for comparison.
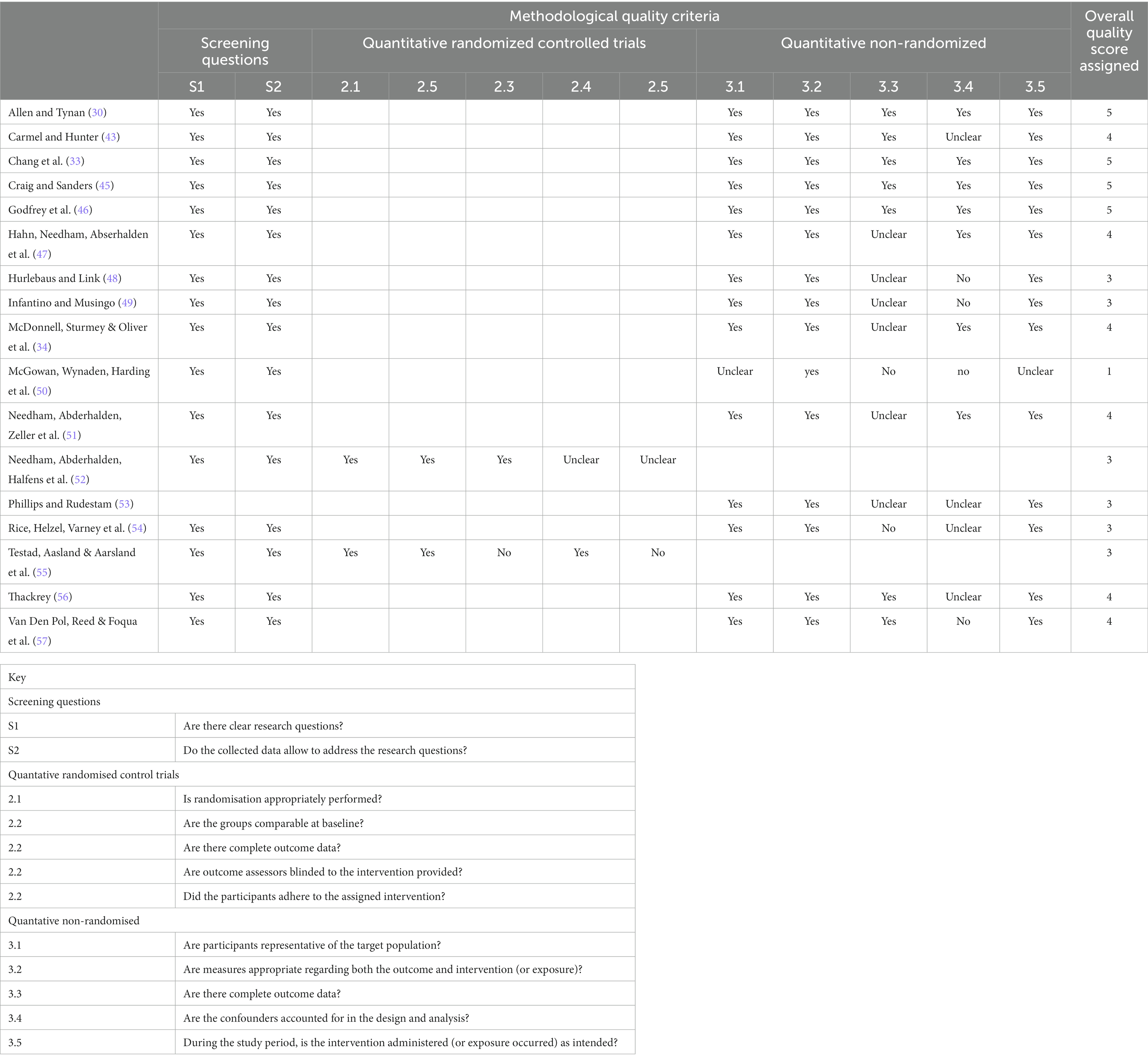
Table 3. Methodological qualities of studies as assessed by the mixed method appraisal tool (MMAT).
Reported outcomes
Twelve outcome measures were reported across the 17 studies chosen: staff knowledge, staff confidence, staff attitudes and behaviours, use of physical restraint, use of mechanical restraint, use of seclusion, use of PRN medication, staff/service user injury, staff assault rate, staff sickness, physical skill acquisition, and service user outcomes.
Staff knowledge was reported to have improved in one study (30), using questionnaire measures. One study reported no significant increase in a knowledge-based measure post training (48). One study reported that in-service education for physical restraints enhanced relevant knowledge and techniques (44). Five studies reported improvement in staff confidence (30, 34, 50, 51, 56). Two studies reported no improvements post-training in confidence (47, 48). Two studies reported no significant effect upon staff attitudes (44, 51), or behaviours post training (44).
Three studies reported reductions in the use of physical restraint post training (30, 45, 55). One study reported significant reductions in the number of mechanical restraints, but no statistically significant reduction in the use of ‘manual holds’ (46). Two studies reported a statistically significant reduction in the use of seclusion (45, 46); one reported a reduction in seclusion across the whole service (45), and the other study reported a reduction in seclusion in one site of the service (46). One study reported a significant increase in the administration of PRN medication as the use of mechanical restraint decreased (46). No studies reported staff injuries during training courses. One study reported reductions in staff injuries post training (43). Another study reported reductions in both staff and service user injuries (46). Two studies reported reductions in rates of assault on trained staff versus untrained staff after training (49, 53), and one study reported increases in assault rates post training (54). One study reported a reduction in sickness rates relating to aggression post training (54). Four studies reported acquisition of physical interventions skills on training courses as an outcome (44, 53, 54, 57). For example, Van den Pol et al. (53) reported data using unannounced assessments of physical skills competency in the workplace.
There was limited outcome data presented that described the impacts of training in physical interventions on service-users. One study noted that training did not lead to a reduction in service-users’ challenging behaviour (34). One study reported reductions in service-user injuries post training (46). Only one study reported on qualitative outcomes for service-users (45), reporting that service-user goal mastery increased by 133%.
Discussion
The purpose of this literature review was to examine the outcomes of staff training in physical interventions across care sectors. A systematic search of the literature was conducted following PRISMA guidelines utilising main keywords “staff training,” “physical intervention,” and “physical restraint;” 190 studies were identified in the search, but only 17 met inclusion criteria relating to publication in a peer reviewed journal and utilising a comparison group. The 17 studies included in this literature review took place in a variety of sectors that comprised of services of adults and children, including psychiatric settings, intellectual and developmental disability settings, and general hospital settings. There are several methodological criticisms of the studies presented. The findings from this literature review offer an insight into the broader structural and empirical issues in evidence-based training practices within the care sectors identified above.
The studies that were included and examined in further detail for the purpose of this literature review were of relatively poor quality. Many of the studies that were reviewed did not give appropriate detail as to how the studies were conducted or to how the training programmes were administered, which calls into question their replicability. There was also a large amount of variability between studies with regard to robustness of study design, use of validated measures, methods of statistical analysis, and the outcomes being evaluated.
Many of the included studies described use of a quasi-experimental design, the sample sizes varied from small case designs, such as that employed by Van Den Pol et al. (57), to larger audits of service data, as described by Craig and Saunders (45). Several experimental evaluations of courses had strengths. Rice et al. (54) used multiple dependent variables, reported reliability data, and used a control group and one-year follow up. There are two studies (52, 55) in this literature review that described themselves as adopting a randomised control trial (RCT). Needham et al. (52) discuss a ‘cluster RCT’ in which 3 psychiatric wards are randomly assigned to the intervention condition and compared to 3 wards that act as a wait list control. Testad et al. (55) use a similar design, in which 2 residential/nursing homes are randomly allocated to receive training, and compared to 2 homes where training is not implemented. While random allocation of ward/home to intervention or treatment condition has been implemented, in practice the designs utilised in these studies do not differ significantly from the quasi-experimental designs described in the other included studies.
Many of the studies did not clearly operationalise the knowledge and skills taught to staff in the training courses being evaluated. As such, it is difficult to compare course content across the studies. Brand names of training courses (e.g., CPI, ACT, NVCI) were often used in the articles with no clear description of these courses. Without accurate descriptions of training courses it is difficult to ascertain whether accurate replication has been achieved, and it is not clear that training programmes referred to by brand names across multiple papers are delivered in a similar manner. Few papers operationally described physical disengagement (breakaway) skills and restraint procedures in sufficient detail. Only three of the papers provide task analyses of restraint procedures (34, 36, 57) that would allow a reader to have a clearer understanding of the methods that were taught to staff. Comparing different training programmes across different settings is also a problematic issue due to the large number of variables that may impact on the delivery of training. These include the relationship with the trainer/coach, the setting of delivery, and the experience of the trainers (38).
The quality of the course content also varied across the studies in the review. Some training courses were delivered over the period of several days, while other training courses were delivered in half a day or less. Where detailed descriptions of training courses were included some studies did demonstrate strengths of course content and teaching methods. Van den Pol et al. (53) used task analyses and videotaped models of the intervention procedures used (57). In this study, behavioural skills training was used to train staff to implement restraint procedures and to train other staff, and use of unannounced observations in the workplace to observe implementation was described (57). Philips and Rudestam’s (53) describe the use of role play and rehearsal, and use of observer ratings of staff behaviour and fear. Two studies provided ongoing training and supervision for the trainees to support staff in managing crises (45, 46), with one study discussing how debriefing was utilised during these coaching periods to identify antecedents. Another study provided follow up, but the staff who had been trained were no longer employed when follow up occurred (57).
Training aims range widely between the studies and include increasing staff skill, knowledge, and confidence, reducing staff fear, reducing the use of physical interventions utilised by staff, increasing the use of other forms of interventions, reducing assault rates, reducing service user and staff injuries and associated costs, and reducing staff sick days. Each of these aims implies the use of different measures, and it is not surprising that outcomes measures in these studies vary dramatically with most utilising multiple measures. Although the MMAT questions described in Table 3 demonstrate that overall the measures were appropriately utilised statistically to determine outcomes based on the interventions, there are some difficulties with measurement. There are a number of outcome measures that should be refined and standardised. Nomothetic measures, such as rates of use of restraint, seclusion or other physical intervention, staff or service user injury or staff sick days, are influenced by definitional issues that affect how incidents are reported and recorded (11). Measures of psychological constructs, such as staff confidence, staff attitudes, or staff perception of aggressive behaviour, vary between studies as to whether they have established reliability and validity, or have been developed specifically for the purposes of the study. There is also variation in regard to reporting of reliability and validity data. This reflects that there is a need of multiple outcome measures that have good construct validity in the area of behaviour management within care settings (24, 38).
Outcome measures that focus on the impact of physical interventions on consumers of services were absent for the majority of these studies. Three studies reported on impacts on service-users (34, 45, 46), with only one of these focusing on qualitative outcomes for service-users (45). In a longitudinal service evaluation of a restraint reduction programme, Craig and Sanders (45) found that over a period of 12 years consumers’ ‘goal mastery’ increased by 133%. In recent years, there has been an increasing emphasis placed on the voices of service-users to encourage a more person-centred approach to crisis management (58, 59). Hawsawi et al. (60) reviewed literature on nurses’ and consumers’ shared experiences of seclusion and restraint. The inclusion of consumer views as a meaningful outcome would represent a significant improvement in the quality of studies that focus on staff training in physical interventions.
Another outcome variable is the impact of training in real-world settings. Staff training is influenced by a wide range of variables. Understanding the generalisation to and impact in real-world settings is critical to meaningful outcomes. The impact of training may have unforeseen consequences. A training course which results in increased acquisition of physical intervention skills and reduction in client incidents may still not be judged adequate if it also results in increases in staff and service user injuries, staff turnover, and associated costs. Similarly, a course that does not impact client incidents may still have benefits, such as reduced staff injuries associated with increased use of appropriate safe forms of restraint.
Staff training outcomes are not just determined by the delivery of a programme in a classroom setting. There are a wide range of organisational variables which will influence outcomes. At the organisational level, various models have been shown to reduce the use of physical restraints, for example multicomponent models such as ‘Six Core Strategies’ (61). Multicomponent group interventions include a range of activities such as senior leadership focus, target setting, monitoring, and reviewing outcomes data at all levels, feedback to frontline teams, in addition to staff training (22, 61). Two studies included in this review evaluate training as part of a multi-component model (44, 45). Craig and Sanders (45) report a 97% decrease in use of restraint and a 100% decrease in use of seclusion over a 12-year period of organisational change within psychiatric services, while Chang et al. (44) report an increase in staff knowledge and correct use of techniques in an ICU setting. Other studies have also found that group level interventions led to moderate to large reductions in the use of restraints (8, 61–63). Duxbury et al. (63) reported restraint reductions of 22% on mental health wards, with some wards showing a 60% reduction.
Staff training evaluations need to include an emphasis on the organisational impact of training (63). Single component models that focus on interventions other than staff training have also had some success in reducing the use of physical restraints, such as ‘SafeWards’ (64). Bowers et al. (62) reported on a cluster randomised control group trial with an average reduction of 15% of ‘conflict’ events and 26.4% reduction in ‘containment’ events following an experimental intervention focused upon staff interactions within mental health services. Lickiewicz et al. (65) implemented elements of the SafeWards programme in Poland, and reported that the number of patients restrained during the course of the study decreased by 34%.
Future research that focuses on training in physical interventions needs to address the following areas. First, training courses should be explicit in their aims and provide sufficient content to inform researchers. Second, the integrity of the independent variable needs to be acknowledged and clearly defined. Third, evaluations should use experimental designs that include adequate control groups and follow-up measures in situ. Fourth, studies need to use measures that are, where possible, empirically reliable and valid. Fifth, there needs to be a stronger emphasis on the implementation, generalisation, maintenance of skills after training in the workplace, and specifically how they are monitored in an organisational context. Sixth, the views of consumers as well as staff need to be strongly considered as outcome measures in future studies.
The use of randomised controlled designs is considered to be a ‘gold standard,’ however, there are significant barriers to adopting such a methodology in this field. Even if a standardised measurement protocol could be agreed, evaluating established training programmes is different from evaluating a new treatment or intervention. That only 17 out of a 190 studies identified met inclusion criteria relating to scientific rigor (and only three in last 10 years) indicates a lack of a robust evidence base for staff training in physical interventions. In practice, these training programmes are already in use without an established evidence base. In the European Union, in 2011 about 23 million persons were employed in health and social care, which made up 10.4% of the total workforce (66). Conservatively speaking, if only 1% of this workforce received either standard or refresher training annually, that would mean a minimum of 230,000 people a year receive training in physical interventions of some form. A figure of 5% (which may not be unreasonable) would produce 1 million people.
Evidence-based practice is considered to be the cornerstone of the scientist practitioner model. Consideration needs to be given to balancing the evidence-based practice for staff training in physical interventions by supplementing it with the construct of practice-based evidence (67). Practice-based evidence incorporates the complexities of real-world clinical practice by documenting and measuring outcomes as they occur (68). If we are to develop methodologies moving forward that reduce the use of physical interventions, this will require an approach where best practice in restraint reduction and elimination is evaluated through practice-based designs such as service audits and individualised case designs. This equally applies to studies which examine staff training that includes physical interventions.
Understanding practice in real world settings (as opposed to teaching/classroom settings) is central to understanding the use, application and ultimately the reduction of restrictive practices. Deveau and Leitch (21) suggested that ‘practice leadership’ and the prevailing culture within staff teams is likely to impact upon restraint and physical intervention use. There is also an opportunity to expand the methodology to include longitudinal approaches and qualitative methodologies that assist in understanding processes surrounding the use of physical interventions. There would still be a need for well-designed empirical studies that evaluate the impact of staff training in physical interventions: these should be viewed as necessary, but not sufficient to, reduce the use of such practices.
In conclusion, this review has highlighted the crude and limited nature of the research literature that focuses on staff training in physical interventions across care settings. If we are to provide clearer evidence for meaningful outcomes, then there is a need for clear and robustly designed studies. At present, the vast majority of training in physical interventions that takes place around the world could be described by researchers as in effect ‘unlicensed products.’
Author contributions
AM was the main author and supervisor of the project. MO’S, SB-P, HM, and RD contributed to the analysis and production of the final script. All authors contributed to the article and approved the submitted version.
Conflict of interest
The lead researcher, AM, is also a director of Studio 3 Training Systems Ltd. Authors MO’S, SB-P and HM were employed by company Studio 3 Training Systems Ltd.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.The authors declare that this study received funding from Studio 3 Training Systems Ltd. The funder had the following involvement in the study: The lead researcher, Professor Andrew McDonnell, is a director of Studio 3 Training Systems Ltd. Authors Marion O’Shea, Stephanie Bews-Pugh and Hannah McAuliffe were employees of Studio 3 Training Systems Ltd at the time of their contribution to the literature review. The remaining author, Roy Deveaux, does not have a commercial or financial relationship with the funders.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. McDonnell, A . The effectiveness of staff training in physical interventions In: D Allen , editor. Ethical approaches to physical interventions. 2nd ed. Avon: BILD publications (2009).
2. Chieze, M, Hurst, S, Kaiser, S, and Sentissi, O. Effects of seclusion and restraint in adult psychiatry: a systematic review. Front Psych. (2019) 10:491. doi: 10.3389/fpsyt.2019.00491
3. Deveau, R, and McDonnell, A. As the last resort: reducing the use of restrictive physical interventions using organisational approaches. Br J Learn Disabil. (2009) 37:172–7. doi: 10.1111/j.1468-3156.2008.00536.x
4. Allen, D . Recent research on physical aggression in persons with intellectual disability: an overview. J Intellect Dev Dis. (2000) 25:41–57. doi: 10.1080/132697800112776
5. Reitan, SK, Helvik, AS, and Iversen, V. Use of mechanical and pharmacological restraint over an eight-year period and its relation to clinical factors. Nord J Psychiatry. (2018) 72:24–30. doi: 10.1080/08039488.2017.1373854
6. Newton-Howes, G, Savage, MK, Arnold, R, Hasegawa, T, Staggs, V, and Kisely, S. The use of mechanical restraint in Pacific rim countries: an international epidemiological study. Epidemiol Psychiatr Sci. (2020) 29:e190. doi: 10.1017/S2045796020001031
7. Fitton, L, and Jones, DR. Restraint of adults with intellectual disabilities: a critical review of the prevalence and characteristics associated with its use. J Intellect Disabil. (2020) 24:268–83. doi: 10.1177/1744629518778695
8. Sturmey, P . Restraint, seclusion and PRN medication in English services for people with learning disabilities administered by the National Health Service: an analysis of the 2007 National Audit Survey. J Appl Res Intellect Disabil. (2009) 22:140–4. doi: 10.1111/j.1468-3148.2008.00481.x
9. Hollins, L . Reducing restrictive intervention of children and young people. Int J Posit Behav Support. (2019) 9:54–6. Available at: https://www.ingentaconnect.com/content/bild/ijpbs/2019/00000009/00000002;jsessionid=283v6wgkaamjc.x-ic-live-03 (Accessed May 21, 2023).
10. Strumpf, NE, and Evans, LK. Physical restraint of the hospitalized elderly: perceptions of patients and nurses. Nurs Res. (1988) 37:132–7. doi: 10.1097/00006199-198805000-00002
11. Gunawardena, R, and Smithard, DG. The attitudes towards the use of restraint and restrictive intervention amongst healthcare staff on acute medical and frailty wards-a brief literature review. Geriatr. (2019) 4:50. doi: 10.3390/geriatrics4030050
12. Weis, E. Deadly restraint: a Hartford courant investigative report. (1998). Available at: https://www.charlydmiller.com/LIB05/1998hartforddata.html (Accessed June 19, 2023).
13. Paterson, B, Bradley, P, Stark, C, Saddler, D, Leadbetter, D, and Allen, D. Deaths associated with restraint use in health and social care in the UK. The results of a preliminary survey. J Psychiatr Ment Health Nurs. (2003) 10:3–15. doi: 10.1046/j.1365-2850.2003.00523.x
14. Kersting, XAK, Hirsch, S, and Steinert, T. Physical harm and death in the context of coercive measures in psychiatric patients: a systematic review. Front Psych. (2019) 10:400. doi: 10.3389/fpsyt.2019.00400
15. Askew, L, Fisher, P, and Beazley, P. What are adult psychiatric inpatients’ experience of seclusion: a systematic review of qualitative studies. J Psychiatr Ment Health Nurs. (2019) 26:274–85. doi: 10.1111/jpm.12537
16. Fish, R, and Hatton, C. Gendered experiences of physical restraint on locked wards for women. Disabil Soc. (2017) 32:790–809. doi: 10.1080/09687599.2017.1329711
17. Sequeira, H, and Halstead, S. Control and restraint in the UK: service user perspectives. Br J Forensic Pract. (2002) 4:9–18. doi: 10.1108/14636646200200003
18. Sequeira, H, and Halstead, S. Is it meant to hurt, is it? Management of violence in women with developmental disabilities. Violence Against Wom. (2001) 7:462–76. doi: 10.1177/10778010122182550
19. Gaskin, CJ, McVilly, KR, and McGillivray, JA. Initiatives to reduce the use of seclusion and restraints on people with developmental disabilities: a systematic review and quantitative synthesis. Res Dev Disabil. (2013) 34:3946–61. doi: 10.1016/j.ridd.2013.08.010
20. Singh, NN, Lancioni, GE, Karazsia, BT, and Myers, RE. Caregiver training in mindfulness-based positive behavior supports (MBPBS): effects on caregivers and adults with intellectual and developmental disabilities. Front Psychol. (2016) 7:98. doi: 10.3389/fpsyg.2016.00098
21. Deveau, R, and Leitch, S. Implementation of policy regarding restrictive practices in England. Tizard Learn Disabil Rev. (2020) 25:1–8. doi: 10.1108/TLDR-05-2018-0016
22. Allen, D, Neil, K, Horwood, S, Gray, D, and Mines, S. The impact of a whole-organisation approach to positive behavioural support on the use of physical interventions. Int J Posit Behav Support. (2012) 2:26–30. Available at: https://www.ingentaconnect.com/content/bild/ijpbs/2012/00000002/00000002;jsessionid=283v6wgkaamjc.x-ic-live-03 (Accessed May 21, 2023).
23. Huckshorn, KA, LeBel, J, and Jacobs, HE. An organizational approach to reducing and preventing restraint and seclusion use with people with acquired brain injury. NeuroRehabilitation. (2014) 34:671–80. doi: 10.3233/NRE-141073
24. McDonnell, AA . Managing aggressive behaviour in care settings: understanding and applying low arousal approaches. Chichester: Wiley-Blackwell (2010).
25. Health and Safety Executive (HSE), United Kingdom . Violence at work: a guide for employers. (2013). Available at: https://www.hse.gov.uk/pubns/indg69.pdf (Accessed May 21, 2023).
26. WorkSafe Victoria, Australia . Physical and mechanical restraint in health services. (2017). Available at: https://www.worksafe.vic.gov.au/__data/assets/pdf_file/0006/246033/Physical-and-mechanical-restraint-in-health-services-guidance-note.pdf (Accessed May 21, 2023).
27. Ontario Ministry of Health and Long-Term Care, Canada . Physical interventions for managing behavioural and psychological symptoms of dementia (BPSD). (2018). Available at: https://www.ontario.ca/page/physical-interventions-managing-behavioural-and-psychological-symptoms-dementia-bpsd (Accessed May 21, 2023).
28. Ministry of Health and Welfare, Republic of Korea . Guidelines for the prevention and management of violence in health care facilities. (2019). Available at: http://www.mohw.go.kr/react/jb/sjb0406vw.jsp?PAR_MENU_ID=03&MENU_ID=032501&CONT_SEQ=347086 (Accessed May 21, 2023).
29. Beech, B, and Leather, P. Workplace violence in the health care sector: a review of staff training and integration of training evaluation models. Aggress Violent Behav. (2006) 11:27–43. doi: 10.1016/j.avb.2005.05.004
30. Allen, D, and Tynan, H. Responding to aggressive behavior: impact of training on staff members’ knowledge and confidence. Ment Retard. (2000) 38:97–104. doi: 10.1352/0047-6765(2000)038<0097:RTABIO>2.0.CO;2
31. Cahill, D . The effect of ACT-SMART on nurses’ perceived level of confidence toward managing the aggressive and violent patient. Adv Emerg Nurs J. (2008) 30:252–68. doi: 10.1097/01.tme.0000334378.90270.be
32. Davies, B, Griffiths, J, Liddiard, K, Lowe, K, and Stead, L. Changes in staff confidence and attributions for challenging behaviour after training in positive behavioural support within a forensic medium secure service. J Forensic Psychiatry Psychol. (2015) 27:886–906. doi: 10.1080/14789949.2015.1072574
33. Killick, S, and Allen, D. Training staff in an adolescent inpatient psychiatric unit in positive approaches to managing aggressive and harmful behaviour: does it improve confidence and knowledge? Child Care Pract. (2005) 11:323–39. doi: 10.1080/13575270500151870
34. McDonnell, A, Sturmey, P, Oliver, C, Cunningham, J, Hayes, S, Galvin, M, et al. The effects of staff training on staff confidence and challenging behavior in services for people with autism spectrum disorders. Res Autism Spectr Disord. (2008) 2:311–9. doi: 10.1016/j.rasd.2007.08.001
35. Visser, SM, McCabe, MP, Hudgson, C, Buchanan, G, Davison, TE, and George, K. Managing behavioural symptoms of dementia: effectiveness of staff education and peer support. Aging Ment Heal. (2008) 12:47–55. doi: 10.1080/13607860701366012
36. Sanders, K . The effects of an action plan, staff training, management support and monitoring on restraint use and costs of work-related injuries. J Appl Res Intellect Disabil. (2009) 22:216–20. doi: 10.1111/j.1468-3148.2008.00491.x
37. Baker, PA, and Bissmire, D. A pilot study of the use of physical intervention in the crisis Management of People with intellectual disabilities who present challenging behaviour. J Appl Res Intellect Disabil. (2000) 13:38–45. doi: 10.1046/j.1468-3148.2000.00004.x
38. McDonnell, A . Freedom from restraint and seclusion: the studio 3 approach. Petersborough: Studio 3 Publications (2022).
39. Luciano, M, Sampogna, G, Del Vecchio, V, Pingani, L, Palumbo, C, De Rosa, C, et al. Use of coercive measures in mental health practice and its impact on outcome: a critical review. Expert Rev Neurother. (2014) 14:131–41. doi: 10.1586/14737175.2014.874286
40. Stubbs, B . The manual handling of the aggressive patient: a review of the risk of injury to nurses: practice development. J Psychiatr Ment Health Nurs. (2009) 16:395–400. doi: 10.1111/j.1365-2850.2008.01354.x
41. Moher, D, Liberati, A, Tetzlaff, J, Altman, DG, The PRISMA Group, Antes, G, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
42. Hong, QN, Fàbregues, S, Bartlett, G, Boardman, F, Cargo, M, Dagenais, P, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. (2018) 34:285–91. doi: 10.3233/EFI-180221
43. Carmel, H, and Hunter, M. Compliance with training in managing assaultive behavior and injuries from inpatient violence. Hosp Community Psychiatry. (1990) 41:558–60. doi: 10.1176/ps.41.5.558
44. Chang, YY, Yu, HH, Loh, EW, and Chang, LY. The efficacy of an in-service education program designed to enhance the effectiveness of physical restraints. J Nurs Res. (2016) 24:79–86. doi: 10.1097/jnr.0000000000000092
45. Craig, JH, and Sanders, KL. Evaluation of a program model for minimizing restraint and seclusion. Adv Neurodev Disord. (2018) 22:216–20. doi: 10.1007/s41252-018-0076-2
46. Godfrey, JL, McGill, AC, Jones, NT, Oxley, SL, and Carr, RM. Anatomy of a transformation: a systematic effort to reduce mechanical restraints at a state psychiatric hospital. Psychiatr Serv. (2014) 65:1277–80. doi: 10.1176/appi.ps.201300247
47. Hahn, S, Needham, I, Abderhalden, C, Duxbury, JAD, and Halfens, RJG. The effect of a training course on mental health nurses’ attitudes on the reasons of patient aggression and its management. J Psychiatr Ment Health Nurs. (2006) 13:197–204. doi: 10.1111/j.1365-2850.2006.00941.x
48. Hurlebaus, A, and Link, S. The effects of an aggressive behavior management program on nurses’ levels of knowledge, confidence and safety. J Nurs Staff Dev. (1997) 13:260–5.
49. Infantino, JA, and Musingo, SY. Assaults and injuries among staff with and without training in aggression control techniques. Hosp Community Psychiatry. (1985) 36:1312–4. doi: 10.1176/ps.36.12.1312
50. McGowan, S, Wynaden, D, Harding, N, Yassine, A, and Parker, J. Staff confidence in dealing with aggressive patients: a benchmarking exercise. Aust N Z J Ment Health Nurs. (1999) 8:104–8. doi: 10.1046/j.1440-0979.1999.00140.x
51. Needham, I, Abderhalden, C, Zeller, A, Dassen, T, Haug, HJ, Fischer, JE, et al. The effect of a training course on nursing students’ attitudes toward, perceptions of, and confidence in managing patient aggression. J Nurs Educ. (2005) 44:415–20. doi: 10.3928/01484834-20050901-06
52. Needham, I, Abderhalden, C, Halfens, RJG, Dassen, T, Haug, HJ, and Fischer, JE. The effect of a training course in aggression management on mental health nurses’ perceptions of aggression: a cluster randomised controlled trial. Int J Nurs Stud. (2005) 42:649–55. doi: 10.1016/j.ijnurstu.2004.10.003
53. Phillips, D, and Rudestam, KE. Effect of nonviolent self-defense training on male psychiatric staff members’ aggression and fear. Psychiatr Serv. (1995) 46:164–8. doi: 10.1176/ps.46.2.164
54. Rice, ME, Helzel, MF, Varney, GW, and Quinsey, VL. Crisis prevention and intervention training for psychiatric hospital staff. Am J Community Psychol. (1985) 13:289–394. doi: 10.1007/BF00914934
55. Testad, I, Aasland, AM, and Aarsland, D. The effect of staff training on the use of restraint in dementia: a single-blind randomised controlled trial. Int J Geriatr Psychiatry. (2005) 20:587–90. doi: 10.1002/gps.1329
56. Thackrey, M . Clinician confidence in coping with patient aggression: assessment and enhancement. Prof Psychol Res Pract. (1987) 18:57–60. doi: 10.1037/0735-7028.18.1.57
57. Van Den Pol, RA, Reid, DH, and Fuqua, RW. Peer training of safety-related skills to institutional staff: benefits for trainers and trainees. J Appl Behav Anal. (1983) 16:139–56. doi: 10.1901/jaba.1983.16-139
58. Fish, R, and Culshaw, E. The last resort? Staff and client perspectives on physical intervention. J Intellect Disabil. (2005) 9:93–107. doi: 10.1177/1744629505049726
59. Brophy, LM, Roper, CE, Hamilton, BE, Tellez, JJ, and McSherry, BM. Consumers and Carer perspectives on poor practice and the use of seclusion and restraint in mental health settings: results from Australian focus groups. Int J Ment Health Syst. (2016) 10:1–10. doi: 10.1186/s13033-016-0038-x
60. Hawsawi, T, Power, T, Zugai, J, and Jackson, D. Nurses’ and consumers’ shared experiences of seclusion and restraint: a qualitative literature review. Int J Ment Health Nurs. (2020) 29:831–45. doi: 10.1111/inm.12716
61. LeBel, JL, Duxbury, JA, Putkonen, A, Sprague, T, Rae, C, and Sharpe, J. Multinational experiences in reducing and preventing the use of restraint and seclusion. J Psychosoc Nurs Ment Health Serv. (2014) 52:22–9. doi: 10.3928/02793695-20140915-01
62. Bowers, L, James, K, Quirk, A, Simpson, A, Stewart, D, and Hodsoll, J. Reducing conflict and containment rates on acute psychiatric wards: the Safewards cluster randomised controlled trial. Int J Nurs Stud. (2015) 52:1412–22. doi: 10.1016/j.ijnurstu.2015.05.001
63. Duxbury, J, Baker, J, Downe, S, Jones, F, Greenwood, P, Thygesen, H, et al. Minimising the use of physical restraint in acute mental health services: the outcome of a restraint reduction programme (‘REsTRAIN YOURSELF’). Int J Nurs Stud. (2019) 95:40–8. doi: 10.1016/j.ijnurstu.2019.03.016
64. Bowers, L . Safewards: a new model of conflict and containment on psychiatric wards. J Psychiatr Ment Health Nurs. (2014) 21:499–508. doi: 10.1111/jpm.12129
65. Lickiewicz, J, Adamczyk, N, Hughes, PP, Jagielski, P, Stawarz, B, and Makara-Studzińska, M. Reducing aggression in psychiatric wards using Safewards - a polish study. Perspect Psychiatr Care. (2021) 57:50–5. doi: 10.1111/ppc.12523
66. Schultz, E . Employment in health and long-term care sector in European countries. Zdrowie Publiczne i Zarządzanie. (2013) 11:107–24. doi: 10.4467/20842627OZ.14.011.1621
67. Horn, SD, and Gassaway, J. Practice based evidence incorporating clinical heterogeneity and patient-reported outcomes for comparative effectiveness research. Med Care. (2010) 48:17–32. doi: 10.1097/MLR.0b013e3181d57473
Keywords: staff training, physical interventions, restraint, seclusion, seclusion and restraint reduction
Citation: McDonnell AA, O’Shea MC, Bews-Pugh SJ, McAulliffe H and Deveau R (2023) Staff training in physical interventions: a literature review. Front. Psychiatry. 14:1129039. doi: 10.3389/fpsyt.2023.1129039
Edited by:
Tilman Steinert, ZfP Südwürttemberg, GermanyReviewed by:
Mary Lavelle, Queen's University Belfast, United KingdomErik Søndenaa, Norwegian University of Science and Technology, Norway
Copyright © 2023 McDonnell, O’Shea, Bews-Pugh, McAulliffe and Deveau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrew A. McDonnell, YW5keW1Ac3R1ZGlvMy5vcmc=