 Fátima Méndez-López1,2
Fátima Méndez-López1,2 Bárbara Oliván-Blázquez1,2,3*
Bárbara Oliván-Blázquez1,2,3* Marta Domínguez-García1,2,4
Marta Domínguez-García1,2,4 Cruz Bartolomé-Moreno1,2,4,5Isabel Rabanaque6
Cruz Bartolomé-Moreno1,2,4,5Isabel Rabanaque6 Rosa Magallón-Botaya1,2,7
Rosa Magallón-Botaya1,2,7- 1Aragonese Primary Care Research Group, Health Research Institute of Aragon (IISA), Zaragoza, Spain
- 2Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS) RD21/0016/0001, Zaragoza, Spain
- 3Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
- 4Aragonese Healthcare Service (SALUD), Zaragoza, Spain
- 5Department of Family and Community Care Teaching - Sector I, Aragonese Healthcare Service, Zaragoza, Spain
- 6Department of Geography and Territorial Planning, University of Zaragoza, Zaragoza, Spain
- 7Department of Medicine, Psychiatry and Dermatology, University of Zaragoza, Zaragoza, Spain
Background: Depression and anxious symptoms are prevalent in the general population, and their onset and persistence may be linked to biological and psychosocial factors, many of which are lifestyle-related. The way we manage our care, physical and emotional health and/or discomfort is highly influenced by our own abilities, skills and attitudes despite life’s circumstances. The main aim of this protocol to analyze the relationship between psychological constructs (self-efficacy, activation, health literacy, resilience, personality traits, sense of coherence, self-esteem), and the presence of affective-emotional problems (anxiety, depression) and addictions in primary health care.
Methods: This is a protocol of a prospective longitudinal cohort study including people of 35–74 years old of Aragon primary health care centers (Spain). Three evaluations will be conducted: baseline evaluation, and follow-up assessments five and ten years after recruitment. The primary outcomes will be severity of depression, severity of anxiety, and addictive behaviors. A detailed set of secondary outcomes will be assessed across all three assessments. This will include psychosocial or personal factors on health behavior, social support, lifestyle patterns, quality of life, the use of health and social resources, and chronic comorbid pathology.
Discussion: The analysis of the impact of psychological constructs and lifestyles on the mental health of people and communities will provide evidence that will make it possible to better address and prevent these prevalent problems and address their improvement from a more global and holistic perspective. The evaluation of psychological constructs should be incorporated into health services to improve people’s ability their self-care, the level of knowledge of managing their disease and their physical, mental and social health.
Clinical trial registration: https://www.isrctn.com/, identifier ISRCTN12820058.
1. Introduction
Affective disorders are a relevant and growing health problem, with a significant level of morbidity worldwide (1). In 2017, the World Health Organization reported that 4.4% of the world’s population suffered from depression and 3.6% from anxiety. These disorders are more prevalent in women than in men (depression: 5.1% vs. 3.6; anxiety 4.6% vs. 2.6%, respectively) (2). Currently, the COVID-19 pandemic has had a severe impact on the mental health and wellbeing of the world population, increasing cases of major depression by 27.6% and cases of anxiety disorders by 25.6% (3, 4). In Spanish primary health care (PHC), the most frequently registered mental health problems are anxiety disorder (6.7%), and depressive disorder (4.1%) (5). Addictive behaviors are another relevant mental health problem in PHC (6). 33.1% of the population aged 15–64 years consume tobacco daily, while daily alcohol consumption stands at 9.0% (7). Finally, 3.5% of the same population engages in compulsive use of the Internet and 2.8% consumes cannabis daily (7, 8).
According to the International Classification of Diseases 11th, depression, anxiety, and addictive behavior disorders are mental, behavioral, or neurodevelopmental disorders (9). These syndromes are characterized by a clinically significant alteration in the cognition, emotional regulation, or behavior of an individual (9). Moreover, they are the result of complex interactions between social, psychological, and biological factors and are generally associated with significant distress or impairment in personal, family, social, educational, occupational, or other important areas of functioning (10). It must be considered that any mental health problem is a serious health problem when it is of long duration, of at least moderate-severe intensity, and alters the conciliation and daily life (11, 12).
The way we manage our care, physical and emotional health and/or discomfort is highly influenced by our own abilities, skills and attitudes regardless of life circumstances (13, 14). Some of these factors are health literacy (15), patient activation (16), self-efficacy (17), resilience (18), sense of coherence (19), self-esteem (20), and personality characteristics (21). First, the level of health literacy is defined as the knowledge of the population, their motivation and individual abilities to understand and make decisions related to the promotion and management of their health (15). In recent evidence, health literacy interventions improve the emotional state of patients in primary care, with a moderately positive effect on reducing depression and anxiety symptoms (22). Second, self-efficacy is represented as a feeling of confidence in one’s abilities to deal with certain stressors in life (17). Increased self-efficacy beliefs have also been connected to improved emotion management and psychosocial functioning (23, 24). Moreover, low self-efficacy is related, for example, to depression, alcohol use and internet addiction (25–27). Third, resilience represents as a positive adaptation to adversity, such as misfortunes and adverse life events (18). Low resilience has been associated with high levels of depression, addictive behavior, anxiety, and mortality (28–30). Encouraging high resilience in subjects has been found to be an effective method to minimize addictive Internet usage (31, 32). Fourth, sense of coherence is defined as the personal attitudes to the values of vital experiences (19). Some data show a positive relationship between an improved sense of coherence and lower levels of depression, anxiety, and problematic use of the Internet (33, 34). Fifth, self-esteem is represented as a positive or negative feeling about oneself and is constructed through the evaluation of one’s own attributes (20). Adults with higher overall self-esteem are more likely to experience physical, mental, professional and social well-being. For example, low self-esteem is associated with behavioral addictions such as emotional problems, substance abuse, and problematic use of new technologies (35, 36). Finally, the personality traits that influence mental health and addiction include introversion, low conscientiousness, neuroticism, low agreeableness, and low openness (37). Those with much higher neuroticism scores and lower extraversion and conscientiousness scores had higher anxiety and depressive symptoms (38). Addiction to new technologies is associated with adults with personality traits such as neuroticism, openness, and low conscientiousness (39, 40).
Furthermore, the onset and persistence of affective disorders has been associated with specific lifestyle characteristics (e.g., poor-quality diet, sleep disturbances, and sedentary lifestyle) (41–43). Therefore, some healthy habits (e.g., good nutrition, quality sleep, sufficient physical activity) are associated with lower levels of depression and anxiety (44, 45). In particular, improving physical activity has a moderate to large effect on improving depressive symptoms (46). Additionally, depression severity and current depression diagnosis are associated with unhealthy dietary intake and poorer food quality (47). Moreover, sleep disturbances increase the risk of suicidal behavior in depressed patients (48). Furthermore, addictive behaviors (e.g., tobacco use, harmful use of alcohol, substance abuse, and compulsive use of the Information and Communications Technologies (ICT) can coincide with, contribute to, or result from mental disorders such as depression or anxiety (49–51). Current evidence suggests the high probability of exacerbation of anxious or depressive disorders when they coexist with chronic comorbidities (52). Several studies have found that people with chronic diseases have a higher risk of developing mental disorders such as depression or anxiety (52–54). Simultaneously, people diagnosed with a mental health disorder are more likely to have chronic physical conditions than a person without a mental health diagnosis (52, 55). Moreover, a prospective cohort study of community individuals with a follow-up after 11 years indicated that the increase in depressive symptoms over time was associated with higher mortality rates (56).
Mental health disorders generate a great economic burden in the use of health system services and represent a significant proportion of health-seeking contacts in primary care (57, 58). In Spain, around 70–85% of the population opts for public primary health care over private insurance (59). Specifically, 60% of frequent users in primary health care suffer from some mental health problem, particularly depressive or anxiety disorders (60). Only 10% of patients with mental health problems seen in primary care are referred to mental health units (61). A World Health Organization report highlights the fundamental role of PHC personnel in the detection, diagnosis, and treatment of people with mental disorders (62, 63). The importance of the PHC lies in being the gateway to the health care system, its accessibility and its interaction with people with mental health problems and their families (61). Most people with mental health problems access primary care, and their disorders are more likely to be identified and treated appropriately and with less risk of stigma (62). In addition, the integration of mental health into primary care promotes comprehensive, coordinated, and person-cantered care for the many people with co-morbid physical and mental health problems (62).
Promoting the participation of the population in coping with diseases and their self-care and self-management of health is a key element in the health of the population in general and especially of the population with affective disorders (64). It is necessary to investigate further how people’s psychological constructs, beliefs and self-care capacity, as well as their lifestyles, can affect the well-being or discomfort of people and contribute to a healthier life from the perspective of mental health. Furthermore, it is important to assess longitudinal changes in these factors and affective disorders given their association with increased comorbidity and mortality (56). The analysis of the impact of psychological constructs and lifestyles on the mental health of individuals and communities will provide evidence that will make it possible to better address and prevent these prevalent problems as well as foster their improvement from a more global and holistic perspective.
Our main objective in this study is to analyze the relationship between psychological constructs (self-efficacy, activation, health literacy, resilience, personality traits, sense of coherence, self-esteem), affective-emotional problems (anxiety, depression) and addiction in primary health care. Therefore, our main hypothesis is that subjects with lower levels of the psychological constructs (self-efficacy, activation, health literacy, resilience, sense of coherence, self-esteem) will have more severe depressive, anxious, and addictive behavior symptoms than those with higher values of the psychological constructs.
One of the secondary objectives of this study is to analyze whether these psychological constructs act as mediating or moderating factors in the relationship between the diagnosis of comorbidities or healthy lifestyles and depression, anxiety, and addictive disorders. Therefore, our secondary hypothesis is that the relationship between the diagnosis of comorbidities or healthy lifestyles and depression, anxiety, or addictive disorders will change according to the value of the different moderators, such as self-efficacy, activation, health literacy, resilience, personality traits, sense of coherence, and self-esteem.
Moreover, a final secondary objective is to create a cohort for an analysis of the relationship between these psychological constructs and lifestyles and the incidence rate of diagnoses of depression and/or anxiety to be revisited after 5–10 years. Consequently, our last secondary hypothesis is that people with lower levels of the psychological constructs and less healthy lifestyle habits will be more likely to experience increased incidence of diagnoses of depression and anxiety or worsening symptoms in the following 5 to 10 years than will those with higher values of the psychological constructs of healthy lifestyles.
2. Materials and methods
2.1. Study design
This study is a protocol of a prospective longitudinal cohort study. This study will be the first baseline measurement for creating a cohort with expected follow-up at 5–10 years. According to current evidence from prospective studies in the community population (56), and the advantages of a cohort study, follow-up at 5–10 years will make it possible to determine incidence, natural history, clinical course, and assess mortality (65). This protocol was registered with ISRCTN Registry before commencement (ISRCTN12820058). For the creation of this protocol, we followed the standard protocol items: recommendations for interventional trials (SPIRIT) guidance (Supplementary Material 1), and the study will be performed and reported according to the guidance for strengthening the reporting of observational studies in epidemiology (STROBE).
2.2. Contextual framework
The study will be carried out within the framework of primary health care in the Spanish region of Aragon. Aragon is an Autonomous Community located in the northeast of Spain. It is the fourth Spanish Autonomous Community by territory but ranks 11 out of 17 in terms of population. It has a population of 1.3 million inhabitants: 60% live in urban areas (675,301 inhabitants live in the city of Zaragoza) and semi-urban areas and 40% of the remaining population lives in towns with fewer than 5,000 inhabitants. Aragon has an aging population, with 23.5% of people over 64 years of age. The average socioeconomic level of Aragon is medium, and the unemployment rate is lower than the national average. Public health provides assistance for nearly the entire population [around 70–85% of the population opts for public primary health care over private (59)]. Aragon public primary health care is structured into 8 health sectors organized into 123 Basic Healthcare Areas (BHA), which include 118 health centers and 870 local clinics (66, 67). Spanish primary health care is made up of a multidisciplinary team of general practitioners, nurses, psychologists, social workers, physiotherapists and occupational therapists.
2.3. Inclusion and exclusion criteria
The inclusion criteria are (A) participants of 35–74 years old; (B) ability to speak and write in Spanish; (C) ability to understand the study and provide consent to participate in the study voluntarily. According to national clinical data from Primary Care, the most frequent stage of onset of depression and anxiety is the decade between 30 and 40 years of age. At this age, these disorders are more prevalent in women than in men (depression: 4.2% vs. 2.0%; anxiety: 10% vs. 5.7%, respectively) (5). In addition, in this age range, these affective disorders have a notable impact on people who are usually at the age of full work, economic and family activity (68). The prevalence of these pathologies increases with age, decreasing slightly from the age of 75, and the trend of higher prevalence in women than in men continues to increase with age (depression: 12.2% vs. 4.8%; anxiety: 11.3% vs. 5.0%, respectively) (5).
The exclusion criteria are (A) suffering from a terminal illness; (B) being institutionalized at the time of the appointment; (C) difficulty participating due to cognitive dysfunction, dementia, or any serious disease that may seriously interfere with the patient’s participation in the study; (D) persons who plan to move out of Spain within five years after the initiation of the study.
2.4. Sample size and sampling
The sample size was computed using the formula for caclulating the population estimates of the most prevalent affective disorders in primary care (anxiety and depression) (69). To calculate the sample size, we will use the data obtained in the study by Santomauro et al. (57). We used the prevalence of the most frequent affective disorders and addictions in primary care (anxiety, depression) as the main variable: 3.1% for major depression and 4.8% for anxiety disorders. Accepting an alpha value of 0.05 and a margin of error of 3% of units, the total sample size required was 290 with the expectation of a possible 30% withdrawal rate.
For selecting potential participants, stratified selection will be made by age, sex and population distribution in urban and rural areas with respect to the National Institute of Statistics data from the census of Aragon 2021 (Figure 1 and Table 1). This stratification will be carried out with the intention of establishing the greatest variability within the sample and reaching a maximum level of representativeness for the population (Table 2). To achieve this, different primary care health centers in the autonomous community, 1–2 rural centers and 1–2 urban centers, will be selected. The rural centers sampled will be in towns with a population of under 2,000 inhabitants.
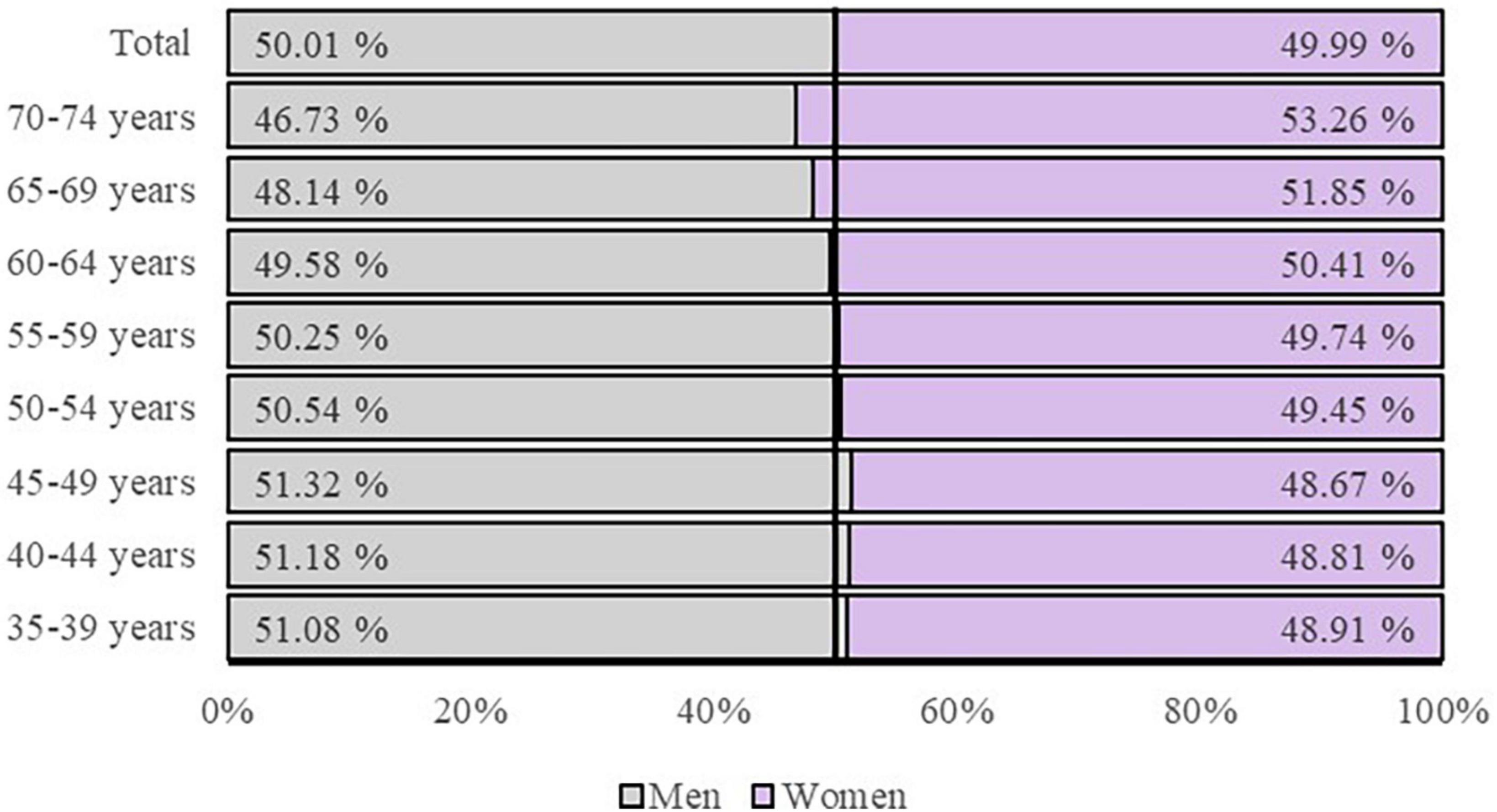
Figure 1. Total population distribution of Aragon by age and sex respect to National Institute of Statistics data from the census of Aragon 2021.
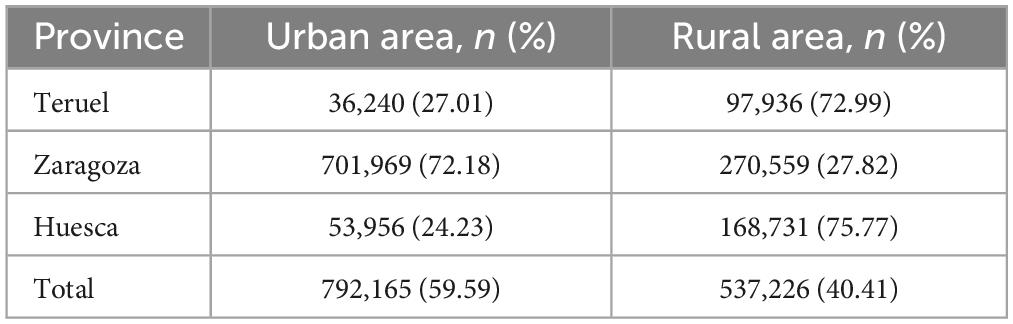
Table 1. Total population distribution in urban and rural areas of Aragon respect to National Institute of Statistics data from the census of Aragon 2021.
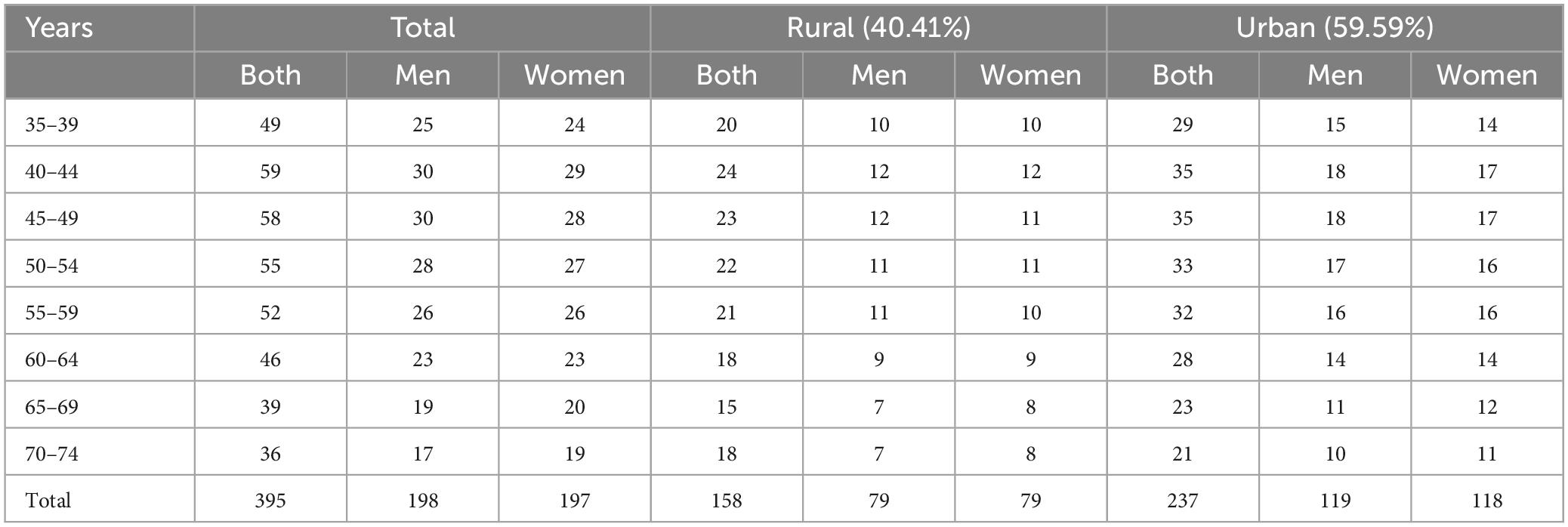
Table 2. Stratified selection of Aragon population by sex, age, and population distribution.
2.5. Data collection
The research team will perform an information session about the study at the selected health centers. In these sessions, the research team will explain the project to be carried out and its methodology to all primary care professionals (family doctors, nurses, psychologists, social workers, physiotherapists) who work in the selected health centers. With these informative sessions for PHC professionals and a good line of contact established with the research team, the aim is to ensure and improve the recruitment rate since PHC professionals maintain good and trustworthy contact with the population. They will also be provided with the telephone number of the research unit for the initial appointment if any patient that these professionals receive in their daily work is interested in participating in the study.
The research team will send an information letter to the participants obtained from the stratified sampling. This letter will include information on the study procedure and contact details of the research unit, so participants who are interested can contact the research team. All members of the multidisciplinary research group come from primary health care and public health.
In addition, broadcasting will be carried out through general media, posters, and press releases, which will raise awareness and obtain greater data at the beginning of the study. Patients who will be interested in the study will arrange a meeting with the research team at their health center to explain the study in more detail, verify that they meet the inclusion and stratification criteria and sign the informed consent if they wish (Supplementary Material 2). All researchers will be trained to conduct research in a systematic and unified method for data collection. A research assistant will collect the data, and another will enter and encode the data into a database. All subjects’ data will be anonymized and will only be used for the purposes of the study. To maintain anonymity, researchers who manage the data of the database or who perform the evaluation of the results and the analysis of the data will not know or have access to data that would allow them to identify the patient directly. At each appointment, the different questionnaires will be administered, a physical examination will be performed that will include anthropometric measurements, and a second appointment will be made with the participant to perform a blood draw at their health center that same week. The research team will include a monitoring and management committee. It will review the quality of the data included in the database and will discuss any conclusions resulting from data of doubtful origin. Additionally, this committee will monitor recruitment rates, dropout rates, and any concerns related to the study. The reasons for dropping out, having made the appointment, or even the reasons for definitive non-participation will also be recorded. Participants and health professionals will be informed about these results. Figure 2 details the registration and evaluation schedule for this study, with dates included.
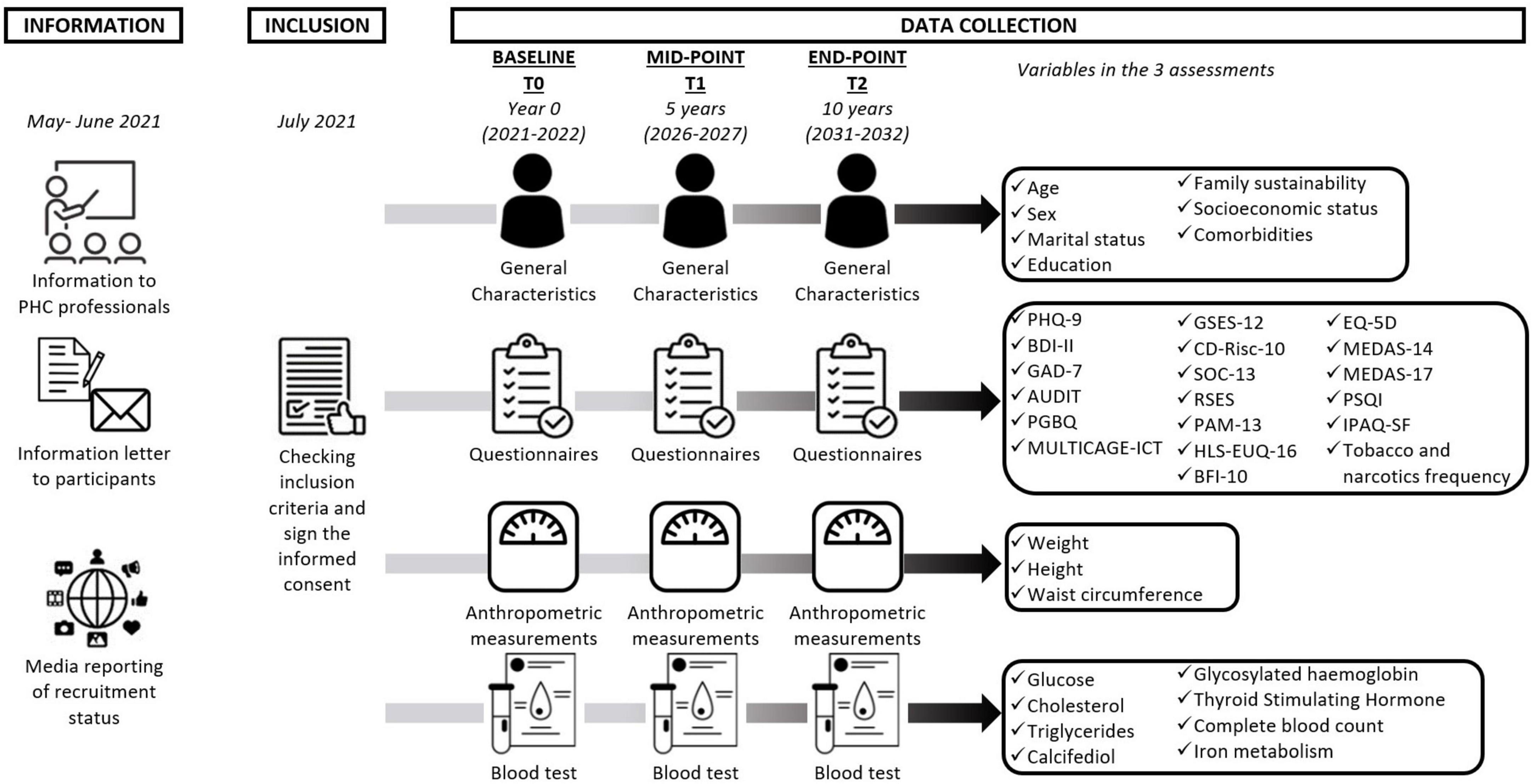
Figure 2. Chronological data collection. PHQ-9, Patient Health Questionnaire; BDI-II, Beck Depression Inventory; GAD-7, Generalized Anxiety Disorder; AUDIT, Alcohol Use Disorders Identification Test; PGBQ, Pathological Gambling Brief Questionnaire; MULTICAGE-ICT, MULTICAGE-Information and Communications Technologies; GSES-12, General Self Efficacy Scale; CD-Risc-10, Connor–Davidson Resilience Scale; SOC-13, Sense of Coherence Scale; RSES, Rosenberg Self-Esteem Scale; PAM-13, Patient Activation Questionnaire; HLS-EUQ-16, Health Literacy Survey European Questionnaire; BFI-10, Big Five Inventory; EQ-5D, European Quality of Life-5 Dimensions Questionnaire; MEDAS, Mediterranean Diet Adherence Screener; PSQI, Pittsburgh Sleep Quality Index; IPAQ-SF, International Physical Activity Questionnaire-Short Form.
2.6. Measures
An evaluation will be carried out at baseline with further assessments five and ten years following the end of the baseline assessment. In this study, we will use valid instruments whose psychometric properties have been tested on the Spanish population to collect data; the validity and reliability of the questionnaires are reported in Table 3.
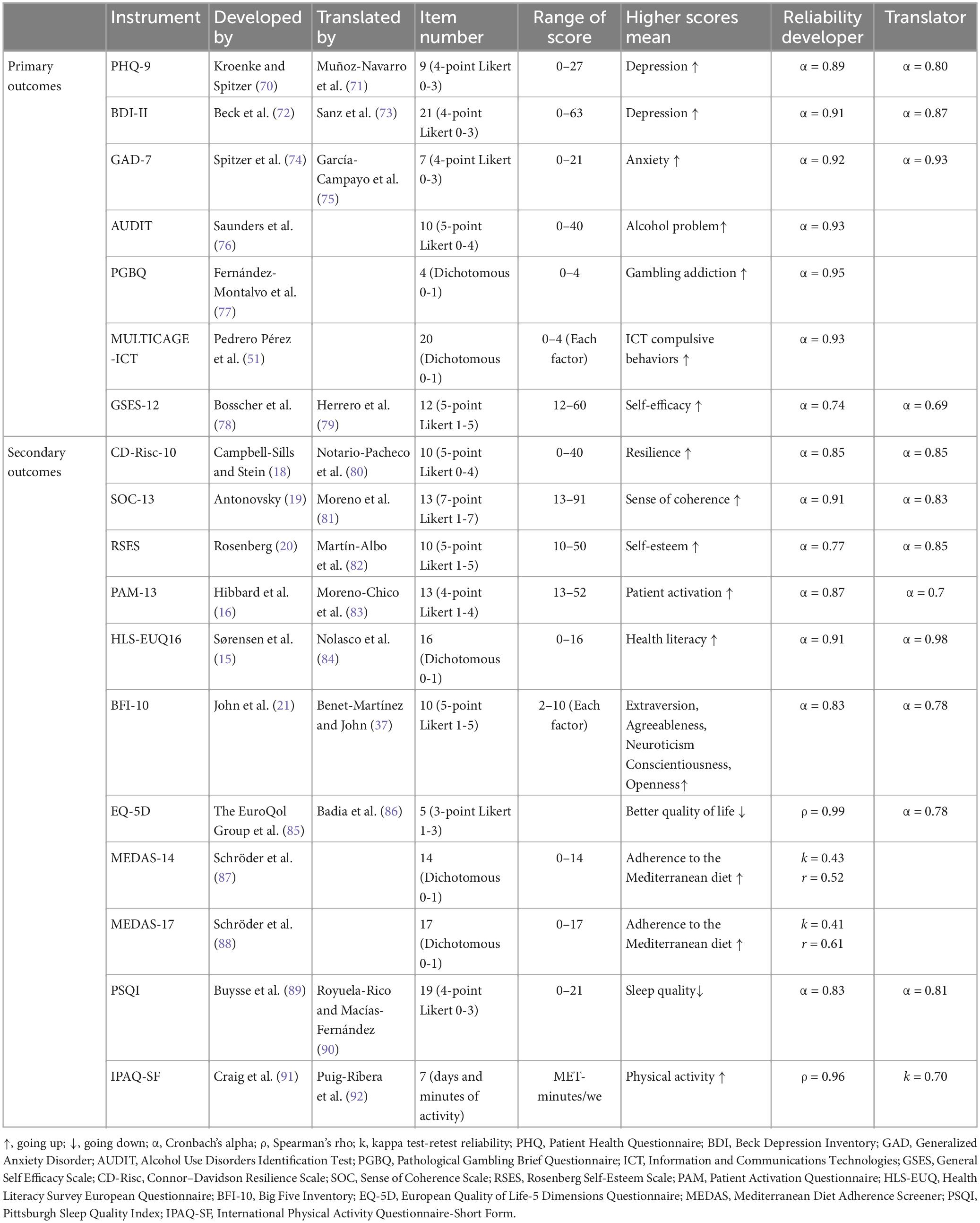
Table 3. Instruments used in the study.
2.6.1. Primary outcomes
The main variables will be severity of depression, severity of anxiety, and addictive behaviors.
2.6.1.1. Depression
Depression will be assessed by Patient Health Questionnaire-9 and Beck Depression Inventory. The Patient Health Questionnaire-9 (PHQ-9, Spanish version) will be used to measure the degree of depression in the past 2 weeks (70). The severity levels include no depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19) and severe depression (20–27). The validated Spanish version has a Cronbach’s alpha value (α) of 0.80 (71). The Beck Depression Inventory-Second Edition (BDI-II, Spanish version) will be used to measure the severity of depression (72). The severity levels include minimal depression/no depression (0–13), mild depression (14–19), moderate depression (20–28), and severe depression (29–63). In its Spanish version, the Cronbach’s alpha coefficient is 0.87 (73).
2.6.1.2. Anxiety
The Generalized Anxiety Disorder-7 (GAD-7, Spanish version) will be used to measure anxiety level. Each item describes one of the typical symptoms of generalized anxiety disorders experienced over the last 2 weeks (74). The severity levels in the original study include no anxiety (0–4), mild anxiety (5–9), moderate anxiety (10–14) and severe anxiety (15–21). The validated Spanish version has a Cronbach’s alpha value (α) of 0.93 (75).
2.6.1.3. Alcohol consumption
The Alcohol Use Disorders Identification Test Form (AUDIT, Spanish version) will be used to screen for excessive alcohol consumption. It will act as a support in the evaluation and identification of excessive alcohol consumption as a cause of disease, dependence and consequences of harmful consumption (76). Alcohol consumption dependence levels include no dependence (0–7), low dependence (8–15), moderate dependence (16–19) and high dependence (20–40). The validated Spanish version has a Cronbach’s alpha value (a) of 0.93 (75).
2.6.1.4. Pathological gambling
The Pathological Gambling Brief Questionnaire (PGBQ) will be used to assess the psychometric behavior with respect to gambling addictions in the general population (77). A score ≥ 2 indicates possible gambling addiction problems, with a maximum score of 4. In its Spanish version, the Cronbach’s alpha coefficient is 0.95 (77).
2.6.1.5. Pathological use of information and communication technologies
The MULTICAGE-ICT Questionnaire will be used to Assess problems related to the use of the Internet, mobile phones, video games, instant messaging, and social networks (51). Composed of 20 total items distributed in 5 scales (internet; mobile phone; video games; instant messaging; social networks). In each scale, item 1, the estimation of excess in temporary dedication; item 2, the estimation of significant others; item 3, the difficulty of not performing the behavior; item 4, the difficulties in voluntarily interrupting the behavior. Higher scores indicate higher use/abuse of Information and Communications Technologies (ICT). The validated Spanish version has a Cronbach’s alpha value (α) of 0.93 (51).
2.6.2. Secondary outcomes
2.6.2.1. Sociodemographic and clinical data
Sociodemographic information, including age, sex, marital status, education, socioeconomic status, and family sustainability, will also be obtained through an ad hoc questionnaire prepared by the research team. Health-related characteristics will include physical and psychological comorbidities. These data will be collected from the electronic medical record and will be included in the database following the definitions of diseases according to the International Classification of Primary Care (3rd edition). In addition, the physical examination will obtain anthropometric measurements (weight, height, and waist circumference). The analytical determination will complement the diagnosis of comorbidities with chronic diseases. In all patients, the concentrations of glucose (mg/dL), cholesterol, triglycerides, glycosylated hemoglobin (%), Thyroid-Stimulating Hormone (μIU/mL), complete blood count, iron metabolism, and calcifediol will be obtained.
2.6.2.2. Self-efficacy
The General Self Efficacy Scale (GSES-12, Spanish version) will be used to evaluate perceived global self-efficacy as feeling confident in one’s abilities to adequately handle certain stressors in life (78). The final score on the questionnaire is the sum of the responses obtained on each item (range 12–60) and higher scores indicate higher levels of self-efficacy. The validated Spanish version has a Cronbach’s alpha value (α) of 0.69 (79).
2.6.2.3. Resilience
The Connor–Davidson Resilience Scale (CD-Risc-10, Spanish version) will be used to evaluate resilience as the positive adaptation to circumstances of significant adversity such as misfortunes and tragic situations in life (18). The final score on the questionnaire is the sum of the responses obtained on each item (range 0–40), and higher scores indicate higher levels of resilience. The validated Spanish version has a Cronbach’s alpha value (α) of 0.85 (80).
2.6.2.4. Sense of coherence
The Sense of Coherence Scale (SOC-13, Spanish version) will be used to measure sense of coherence in terms of the personal disposition toward the values of vital experiences. It also measures understandability, manageability and meaning (19). Higher scores (after flipping the flipped items) (range 13–91) indicate a greater sense of coherence. The validated Spanish version has a Cronbach’s alpha value (α) of 0.83 (81).
2.6.2.5. Self-esteem
The Rosenberg Self-Esteem Scale (RSES, Spanish version) will be used to assess self-esteem during the past 2 weeks (20). Self-esteem is defined as feelings toward oneself, which can be positive or negative, and is determined based on an evaluation of one’s own characteristics. Scores below 25 points are considered to reflect significant low self-esteem issues. The validated Spanish version has a Cronbach’s alpha value (α) of 0.85 (82).
2.6.2.6. Patient activation
The Patient Activation Questionnaire (PAM-13, Spanish version) will be used to measure activation as the capacity and ability to manage one’s personal condition of his/her health and how competent he/she feels in taking on this role (16). The final score on the questionnaire is the sum of the responses obtained on each item (range 13–52) and higher scores indicate a higher level of patients’ activation in addressing their own health. We decided not to include the category “not applicable” to avoid misinterpretations. In its Spanish version, the Cronbach’s alpha coefficient is 0.7 (83).
2.6.2.7. Health literacy
The Health Literacy Survey European Questionnaire (HLS-EU-Q16, Spanish version) will be used to measure the level of health literacy as knowledge of the population, motivation, and individual abilities to understand and make decisions related to the promotion and management of participants’ own health (15). The score of each subject will be obtained from the sum of the scores of the 16 items, transforming each one into a dichotomous response: very difficult and difficult = 0; easy and very easy = 1. The health literacy levels include an inadequate or problematic level (0–12) and a sufficient level (13–16). In its Spanish version, the Cronbach’s alpha coefficient is 0.98 (84).
2.6.2.8. Personality characteristics
The Big Five Inventory-10 (BFI-10, Spanish version) will be used to examine personality characteristics (21). The questionnaire measures the 5 factors of personality from the five factors model (each factor entails two items). Extraversion (Extraverts engage actively with others to earn friendship, admiration, power, status, excitement, and romance; Introverts conserve their energy and do not work as hard to earn these social rewards). Agreeableness (High scores have a great deal of empathy and tend to get pleasure out of serving and taking care of others; Low scorers are often described as hostile, competitive, and antagonistic). Conscientiousness (High scorers are organized and determined; Low scorers are impulsive and easily side-tracked). Neuroticism (High scorers are more likely to react to a situation with fear, anger, sadness, and the like. Low scorers are more likely to brush off their misfortune and move on). Openness (High scorers tend to be creative, adventurous, and intellectual; Low scorers tend to be practical, conventional, and focused on concrete information). The validated Spanish version has a Cronbach’s alpha value (α) of 0.78 (37).
2.6.2.9. Health-related quality of life
The European Quality of Life-5 Dimensions Questionnaire (EQ-5D, Spanish version) will be used to measure health-related quality of life. It will be used to calculate the quality-adjusted life year (QALY) during the monitoring period by adjusting the length of time affected by the health result in relation to the utility value (85). It contains five health dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression), and each of these has three levels (no problems, slight or moderate problems, and severe problems). Moreover, this questionnaire incorporates a Visual Analog Scale (VAS) which can be used as a quantitative measure of health outcome reflecting the patient’s own judgment. Patients mark the point on the vertical line that best reflects their assessment of their current global health status. In its Spanish version, the Cronbach’s alpha coefficient is 0.78 (86).
2.6.2.10. Diet adherence
The Mediterranean Diet Adherence Screener (MEDAS) was developed within the Mediterranean diet (PREDIMED) study group. We will also evaluate the adherence to the Mediterranean diet, assessed with the MEDAS (14 items) (87) and MEDAS plus (17 items) (88) questionnaires. Both questionnaires share many of their items, including food and consumption habits: the use of olive oil as the main source of cooking fat, preference for white meat over red meat, servings of vegetables, portions of fruit, red meat or sausages, servings of animal fat, sugar-sweetened beverages, red wine, legumes, fish, commercial pastries and dressing foods with a traditional sauce made of tomatoes, garlic, onion or leeks sautéed in olive oil. However, the stricter values of some items and the inclusion of some additional items in the 17-point version is an attempt to better reflect the possible caloric restriction that should be applied to the Mediterranean diet pattern when the goal is to lose weight. The MEDAS-14 levels include low adherence (0–8) and good adherence (9–14) (87). The MEDAS-17 levels include low adherence (0–7), medium adherence (8–10) and high adherence (11–17) (88). The construct validity of MEDAS was determined by analyzing the correlations of the MEDAS score with dietary intake reported on the food frequency questionnaire (FFQ) with a moderate correlation and moderate mean agreement for both versions (r = 0.52 and k = 0.43 for the 14-item version and r = 0.61 and k = 0.41 for the 17-item version) (87, 88).
2.6.2.11. Sleep quality
Pittsburgh Sleep Quality Index (PSQI, Spanish version) will be used to measure quality and patterns of sleep over the past month (89). It differentiates between “poor” and “good” sleep by measuring seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication and daytime dysfunction. It consists of 19 self-applied questions and five questions that request the evaluation of the patient’s bedmate or roommate (these are not scored). The sleep quality levels include good sleep quality (0–5) and poor sleep quality (6–21). The validated Spanish version has a Cronbach’s alpha value (α) of 0.81 (90).
2.6.2.12. Physical activity
International Physical Activity Questionnaire-Short Form (IPAQ-SF, Spanish version) will be used to measure levels of habitual physical activity over the last 7 days (91). It has seven items and records the activity of four intensity levels: vigorous-intensity activity, moderate-intensity activity, walking and sitting. A total physical activity result MET (minutes/week) can be calculated as the following: total physical activity is the sum of the total results (walking + moderate + vigorous) MET. The Physical Activity levels include low (0-600 MET), moderate (601-3000 MET), high (more than 3000 MET). The validated Spanish version has a kappa value (k) of 0.70 (92).
2.6.2.13. Consumption of tobacco and narcotic substances
Examination of the frequency of consumption of substances such as tobacco and narcotics will be carried out through an ad hoc questionnaire prepared by the research team measured with the 4-question scale adapted from the WHO MONICA study (91, 92). It will assess the current consumption or time since the last consumption, starting age, type of substance consumed and the specific amount of each substance.
2.7. Data analysis
Baseline analysis of the results: Descriptive analysis of all variables (percentage and confidence interval for qualitative variables; means and standard deviation for parametric quantitative variables or median and interquartile range for non-parametric quantitative variables) and univariate analysis (we will use the T-Student for parametric quantitative variable, Mann-Whitney U for non-parametric quantitative variables, and the Chi-Square test for qualitative variables) to evaluate the differences between the patients who have some of the most prevalent affective-emotional problems in primary care (anxiety, depression) compared with those who do not. Statistical analyses will be chosen based on the size of the sample (parametric or non-parametric tests). To compare the two groups, missing data will be assessed and the need to use an intention-to-treat (ITT) analysis and a multiple imputation (MI) technique to handle missing data will be assessed.
To answer the main objective, we will use a multiple linear regression model. To do this, each main variable, the PHQ-9 score, BDI-II, GAD-7, PGBQ, AUDIT, and MULTICAGE-ICT, will be used as a continuous variable. Multiple linear regression will be performed using a stepwise method to obtain a better fit result to the statistical analysis. This stepwise regression simply will repeat the multiple regression, each time removing the least correlated variable. Only the significant variables obtained in the bivariate analysis will be entered into the regression model.
Finally, mediation/moderation analyses will be carried out to analyze whether psychological constructs participate as a mediator or as a moderator in the association of lifestyles (exposure) and anxiety, depression and/or addictions (outcome). The PROCESS analytical tool developed by Hayes will be used to assess mediation/moderation. These analyses were based on multiple linear regression path analysis (93). Bootstrap resampling (10.000 samples) will be used to estimate 95% confidence intervals. Given that heteroscedasticity is common in cross-sectional data, all analyses will include a correction for heteroscedasticity (HC0) (94). The Johnson-Neyman technique will be used to compute the range of significance and simple slopes for the interaction analyses (93). We will report unstandardized regression coefficients; all analyses will be two-tailed and used conventional significance thresholds (α = 0.05). Data collection and statistical analysis will be performed using Excel software, SPSS software (version 25.0) (95) and the statistical software environment R (version 3.6.2) (96).
3. Discussion
Affective disorders are a serious and expanding public health issue, with a high morbidity rate worldwide (57, 58). According to the Global Burden of Disease Study (GBD), depression is the third cause in women and the fifth in men of years lived with disability (97). 60% of frequent users in primary health care suffer from a depressive or anxiety disorder (60). However, only 9% of all primary care patients with depression and anxiety receive adequate treatment and only 6% achieve remission, making affective disorders a significant management issue in primary care (98). Addictive behaviors are another relevant mental health problem in PHC (6). The harmful use of alcohol and tobacco or other substances has serious repercussions on public health and is considered one of the main risk factors for poor health worldwide (99). Not only the consumption of addictive substances is relevant. In recent years, there has been a growing convergence between gaming and betting on various platforms, aided significantly by the internet (100).
The onset and persistence of affective disorders have been associated with psychological constructs (self-efficacy, activation, health literacy, resilience, personality traits, sense of coherence, self-esteem) and lifestyles (poor-quality diet, sleep disturbances, and sedentary lifestyle, as well as alcohol consumption, tobacco, and other addictions) (43). These psychological constructs are framed around the theory of salutogenesis (14). The salutogenic approach seeks to improve participants’ mental health and well-being by enhancing their knowledge, confidence, and ability to employ personal health-related elements (101).
There is evidence from longitudinal studies that evaluate personal factors in the adult population and their relationship with the development of depressive and anxious symptoms. In several cohort studies in older patients, advancing age, alcohol use, sleep problems, severe pain, and multiple disease burden are shown to be risk factors for predicting the development of depression and anxiety in participants who did not have these mental health problems at baseline. Protective factors were income, social support, higher self-efficacy, resilience, and well-being at baseline (102, 103). In another general population study with the same age as our study population, it was shown that individuals who showed higher self-esteem and cognitive ability were negatively associated with a latent initial level of depression (104). These studies support the potential feasibility of this study. The analysis of different psychological constructs in a general population can provide us with an interesting perspective on their relationship to the development and persistence of affective problems about which there is not much research.
Primary health care is the ideal setting for a psychosocial conflict and mental illness prevention approach for three reasons (105). First, PHC is perhaps the social instrument with which the greatest number of citizens are exposed during the year and in the life of each one of them. Second, numerous studies have shown that patients with chronic psychosis or psychosocial conflict often refer to different PHC settings multiple times. Third, at a pragmatic and health level, emotional disorders that are not detected early by primary care providers have a worse prognosis (105). Based on current evidence, a randomized clinical trial conducted in primary care evaluated whether a complex intervention to promote the Mediterranean diet, physical activity, and/or smoking cessation is effective in preventing depression at 12 months follow-up of a population aged 457–75 years. As a result, the intervention provided a non-significant reduction in the incidence of major depression, compared with usual care (106). Our study will provide the opportunity to evaluate and explore what individual conditions influence the evolution of the disease or the development of new diagnoses of affective-emotional disorders so prevalent in the community, such as depression and anxiety. The findings of our study will allow the development of individualized and preventive interventions to provide timely help to adults in groups at risk of developing one of these mental disorders or to reduce symptoms in those who have already been diagnosed.
3.1. Strengths and limitations
The strengths of this study include the design and the wide range of outcome measures. Another strength is that it involves recruiting a general adult population from a Spanish region whose sociodemographic characteristics (age, sex, population distribution) are very similar to those of the rest of the European population and other regions of the world (107). These characteristics will allow a greater representativeness of the results and a better extrapolation of the results to other regions. Public health covers practically the entire population (around 70–85% of the population opts for public primary health care over private) (59). Due to this, a recruitment of the population from PHC will allow us to improve the scope of the representativeness of the sample.
Our study will provide a wealth of information on the interaction between depression, anxiety, addictive behaviors, personal health behavioral factors, and lifestyles. In addition, no longitudinal studies carried out in our population have been identified that analyze in depth all these psychological constructs together while considering their impact on health. Therefore, this study will allow us to provide new evidence on the relationship between psychological constructs and lifestyles in the onset and development of depression and anxiety.
This study includes self-report and hetero-administered questionnaires, as well as a physical and laboratory examination. Among the limitations of the study will be the difficulty of the questionnaires used. This difficulty will be minimized by prior training and quality control of the data collection process to ensure that accurate results comparable to other studies are obtained.
The most important difficulties of the study would be a possible low participation rate and the possible withdrawal of participants due to refusal to complete the follow-up (65). However, possible reasons for dropout and other problems will be recorded. One strategy to achieve a high initial participation rate is to send an informative letter with information about the study; in this way, when the potential participant is contacted, they already know the objective and their confidence in the study is greater. Another of the strategies used for a higher participation rate is the contact of primary care professionals with potential study participants. It has been shown that the general population feels more comfortable when talking to their PHC professionals given their closeness and habitual treatment (108). Due to the possibility of follow-up and continuity of care and attention to the population, PHC is the ideal means to carry out this type of prospective study. The privileged relationships and patient care-oriented knowledge that PHC professionals can establish with patients represents an important tool that could contribute to reducing the global burden of chronic diseases (109). The promotion of the participation of the population in coping with diseases and their self-care and self-management of health is a key element in addressing the health of the general population and especially in the part of the population with mental disorders.
The evaluation of psychological constructs should be incorporated into health services to improve people’s ability to improve their self-care, as well as their level of knowledge of managing their disease and their physical, mental and social health. Mental health is a social and health challenge.
Ethics statement
This study was approved by the Clinical Research Ethics Committee of Aragon N° PI20/302. This study was developed in accordance with the Declaration of Helsinki. Since the project involves the collection and processing of personal data, including personal information; the collection, treatment, communication, and transfer of personal data of all participating subjects must comply with the provisions of the General Data Protection Regulation (EU) (GDPR 2016/679) and the applicable national legislation, Organic Law 3/2018, of December 5, on the Protection of Personal Data. Informed consent was obtained from all participants. All subjects allowed their data to be anonymized and used only for the purposes and publication of the results of this study.
Author contributions
RM-B and BO-B conceived the quantitative part of the study. FM-L and RM-B led the drafting of this manuscript. RM-B obtained the ethical approval from each institution and contributed to design the training program on the questionnaires and measurements. CB-M, MD-G, and IR advised and contributed to the study design. FM-L, CB-M, and BO-B developed the statistical analysis plan. All authors reviewed the manuscript content and approved the final version for submission addressed.
Funding
This study has been funded by Health Institute Carlos III (ISCIII) through the project grant number PI19/01076 (Feder Funds Another way to make Europe) and through internal funds from the Aragonese Primary Care Research Group (B21_23R) of the Health Research Institute of Aragon (IIS Aragon), Zaragoza, Spain. The funder had no role in the study design, data collection, analysis, decision to publish or preparation of the manuscript. The funding organisation will audit trial conduct once a year.
Acknowledgments
We thank the Aragonese Primary Care Research Group (GAIAP, B21_20R) that is part of the Department of Innovation, Research and University at the Government of Aragón (Spain) and the Institute for Health Research Aragón (IIS Aragón); the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS, RD21/0016/0005) that is part of the Results-Oriented Cooperative Research Networks in Health (RICORS) (Carlos III Health Institute); and Feder Funds “Another way to make Europe”. This research has been developed during a short-research term of National School of Public Health (ENSAP), Havana, Cuba supported by Health Research Institute of Aragon (IISA), “Intramural call for research promotion IIS Aragón. Action to Support the Figure of the Predoctoral Researcher”.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1121389/full#supplementary-material
References
1. Institute for Health Metrics and Evaluation. Global Health Data Exchange. (2019). Available online at: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed August 1, 2022).
2. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. (2017). Available online at: https://apps.who.int/iris/handle/10665/254610 (accessed July 1, 2022).
3. WHO Headquarters. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief, 2 March 2022. Geneva: WHO (2022).
4. Nicolini H. Depression and anxiety during COVID-19 pandemic. Cirugia y Cirujanos. (2020) 88(5):542–7. doi: 10.24875/CIRUE.M22000167
5. Subdirección General de Información Sanitaria. Subdirección General de Información Sanitaria. Salud Mental en datos: Prevalencia de los Problemas de salud y Consumo de Psicofármacos y Fármacos Relacionados a Partir de Registros Clínicos de Atención Primaria. BDCAP Series 2. Madrid: Ministerio de Sanidad, Centro de Publicaciones (2021). Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/home.htm (accessed April 15, 2023).
6. Sayre M, Lapham G, Lee A, Oliver M, Bobb J, Caldeiro R, et al. Routine assessment of symptoms of substance use disorders in primary care: prevalence and severity of reported symptoms. J Gen Intern Med. (2020) 35(4):1111–9. doi: 10.1007/s11606-020-05650-3
7. Spanish Observatory of Drugs and Addictions. Survey on Alcohol and Drugs in Spain (EDADES), 1995-2022. Madrid: Spanish Ministry of Health (2022).
8. Spanish Observatory of Drugs and Addictions.Report on Behavioral Disorders 2022: Gambling with Money, use of Video Games and Compulsive use of the Internet in Surveys on Drugs and Other Addictions in Spain EDADES and ESTUDES. Madrid: Spanish Ministry of Health (2022).
9. ICD. International Classification of Diseases 11th revision. Mental, Behavioural or Neurodevelopmental Disorders. (2022). Available online at: http://id.who.int/icd/entity/334423054 (accessed August 25, 2022).
11. Acero González A, Cano-Prous A, Canga A. Experiences of the family living with severe mental illness: a qualitative study in Navarre. An Sist Sanit Navar. (2016) 39(2):203–12. doi: 10.23938/ASSN.0273
12. WHO. World Health Organization Mental Health: Strengthening Our Response. (2022). Available Online at: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed August 1, 2022).
13. Gaxiola-Romero J, Manriquez-Betanzos J, Yánez-Peñúñuri y LY. Evolution of Constructs in Psychology. Examples and Conceptual Contributions. First. Gaxiola Romero J editor. Hermosillo: Qartuppi (2021).
14. Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. (1996) 11(1):11–8. doi: 10.1093/heapro/11.1.11
15. Sørensen K, Van den Broucke S, Pelikan J, Fullam J, Doyle G, Slonska Z, et al. Measuring health literacy in populations: illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health. (2013) 13(1):948. doi: 10.1186/1471-2458-13-948
16. Hibbard J, Mahoney E, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. (2005) 40:1918–30. doi: 10.1111/j.1475-6773.2005.00438.x
17. Sherer M, Maddux J, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers R. The self-efficacy scale: construction and validation. Psychol Rep. (1982) 51(2):663–71. doi: 10.2466/pr0.1982.51.2.663
18. Campbell-Sills L, Stein M. Psychometric analysis and refinement of the connor-davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. (2007) 20(6):1019–28. doi: 10.1002/jts.20271
19. Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. (1993) 36(6):725–33. doi: 10.1016/0277-9536(93)90033-Z
20. Rosenberg M. Society and the Adolescent Self-Image. Princeton NJ: Princeton University Press (1965).
21. John O, Donahue E, Kentle R. The Big Five Inventory–Versions 4a and 54. Berkeley: University of California (1991). doi: 10.1037/t07550-000
22. Magallón-Botaya R, Méndez-López F, Oliván-Blázquez B. Carlos Silva-Aycaguer L, Lerma-Irureta D, Bartolomé-Moreno C. effectiveness of health literacy interventions on anxious and depressive symptomatology in primary health care: a systematic review and meta-analysis. Front Public Health. (2023) 9:1007238. doi: 10.3389/fpubh.2023.1007238
23. Milanovic M, Ayukawa E, Usyatynsky A, Holshausen K, Bowie C. Self efficacy in depression. J Nervous Mental Dis. (2018) 206(5):350–5. doi: 10.1097/NMD.0000000000000804
24. Schönfeld P, Preusser F, Margraf J. Costs and benefits of self-efficacy: differences of the stress response and clinical implications. Neurosci Biobehav Rev. (2017) 75:40–52. doi: 10.1016/j.neubiorev.2017.01.031
25. Mei S, Yau Y, Chai J, Guo J, Potenza M. Problematic Internet use, well-being, self-esteem and self-control: data from a high-school survey in China. Addict Behav. (2016) 61:74–9. doi: 10.1016/j.addbeh.2016.05.009
26. Yang S. Effects of self-efficacy and self-control on internet addiction in middle school students: a social cognitive theory-driven focus on the mediating influence of social support. Child Health Nursing Res. (2020) 26(3):357–65. doi: 10.4094/chnr.2020.26.3.357
27. Blank M, Connor J, Gray A, Tustin K. Alcohol use, mental well-being, self-esteem and general self-efficacy among final-year university students. Soc Psychiatry Psychiatr Epidemiol. (2016) 51(3):431–41. doi: 10.1007/s00127-016-1183-x
28. Smith J, Hollinger-Smith L. Savoring, resilience, and psychological well-being in older adults. Aging Ment Health. (2015) 19(3):192–200. doi: 10.1080/13607863.2014.986647
29. To Q, Vandelanotte C, Cope K, Khalesi S, Williams S, Alley S, et al. The association of resilience with depression, anxiety, stress and physical activity during the COVID-19 pandemic. BMC Public Health. (2022) 22:491. doi: 10.1186/s12889-022-12911-9
30. Aydin N, Celikay Soyler H. The relationship between alcohol use–smoking and psychological resilience in the COVID-19 pandemic. Turkish J Addict. (2022) 9:126–36. doi: 10.5152/ADDICTA.2022.22038
31. Zhou P, Zhang C, Liu J, Wang Z. The relationship between resilience and internet addiction: a multiple mediation model through peer relationship and depression. Cyberpsychol Behav Soc Netw. (2017) 20(10):634–9. doi: 10.1089/cyber.2017.0319
32. Yilmaz R, Karaoglan Yilmaz F. Problematic internet use in adults: the role of happiness, psychological resilience, dispositional hope, and self-control and self-management. J Rational Emot Cogn Behav Therapy. (2022) 10:1–19. doi: 10.1007/s10942-022-00482-y
33. Giglio R, Rodriguez-Blazquez C, de Pedro-Cuesta J, Forjaz M. Sense of coherence and health of community-dwelling older adults in Spain. Int Psychogeriatr. (2015) 27(4):621–8. doi: 10.1017/S1041610214002440
34. Skonieczna J, Fronczak A, Kielan A, Brytek-Matera A, Olejniczak D. The impact of the sense of coherence on the problematic internet use among secondary school students. J Health Educ Res Dev. (2018) 6:4. doi: 10.4172/2380-5439.1000290
35. Orth U, Robins R, Widaman K. Life-span development of self-esteem and its effects on important life outcomes. J Pers Soc Psychol. (2012) 102(6):1271–88. doi: 10.1037/a0025558
36. Seabra L, Loureiro M, Pereira H, Monteiro S, Afonso R, Esgalhado G. Relationship between internet addiction and self-esteem: cross-cultural study in portugal and Brazil. Interact Comput. (2017) 29(5):767–78. doi: 10.1093/iwc/iwx011
37. Benet-Martínez V, John O. Los Cinco grandes across cultures and ethnic groups: multitrait-multimethod analyses of the big five in Spanish and english. J Pers Soc Psychol. (1998) 75(3):729–50. doi: 10.1037/0022-3514.75.3.729
38. Jourdy R, Petot J. Relationships between personality traits and depression in the light of the “Big five” and their different facets. L’Évolution Psychiatrique. (2017) 82(4):e27–37. doi: 10.1016/j.evopsy.2017.08.002
39. Rachubińska K, Cybulska A, Szkup M, Grochans E. Analysis of the relationship between personality traits and internet addiction. Eur Rev Med Pharmacol Sci. (2021) 25(6):2591–9.
40. Marciano L, Camerini A, Schulz P. Neuroticism and internet addiction: what is next? a systematic conceptual review. Pers Individ Dif. (2022) 185:111260. doi: 10.1016/j.paid.2021.111260
41. Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutrition Phys Activity. (2016) 13(1):108. doi: 10.1186/s12966-016-0432-4
42. El Ansari W, Adetunji H, Oskrochi R. Food and mental health: relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent Eur J Public Health. (2014) 22(2):90–7. doi: 10.21101/cejph.a3941
43. Aguilar-Latorre A, Serrano-Ripoll M, Oliván-Blázquez B, Gervilla E, Navarro C. Associations between severity of depression, lifestyle patterns, and personal factors related to health behavior: secondary data analysis from a randomized controlled trial. Front Psychol. (2022) 18:856139. doi: 10.3389/fpsyg.2022.856139
44. Velten J, Lavallee K, Scholten S, Meyer A, Zhang X, Schneider S, et al. Lifestyle choices and mental health: a representative population survey. BMC Psychol. (2014) 2(1):58. doi: 10.1186/s40359-014-0055-y
45. Saneei P, Esmaillzadeh A, Hassanzadeh Keshteli A, Reza Roohafza H, Afshar H, Feizi A, et al. Combined healthy lifestyle is inversely associated with psychological disorders among adults. Matsuoka YJ, editor. PLoS One. (2016) 11:e0146888. doi: 10.1371/journal.pone.0146888
46. Kvam S, Kleppe C, Nordhus I, Hovland A. Exercise as a treatment for depression: a meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
47. Oliván-Blázquez B, Aguilar-Latorre A, Motrico E, Gómez-Gómez I, Zabaleta-del-Olmo E, Couso-Viana S, et al. The relationship between adherence to the mediterranean diet, intake of specific foods and depression in an adult population (45–75 Years) in primary health care. a cross-sectional descriptive study. Nutrients. (2021) 13(8):2724. doi: 10.3390/nu13082724
48. Wang X, Cheng S, Xu H. Systematic review and meta-analysis of the relationship between sleep disorders and suicidal behaviour in patients with depression. BMC Psychiatry. (2019) 19(1):303. doi: 10.1186/s12888-019-2302-5
49. Kuria M, Ndetei D, Obot I, Khasakhala L, Bagaka B, Mbugua M, et al. The Association between alcohol dependence and depression before and after treatment for alcohol dependence. ISRN Psychiatry. (2012) 2012:482802. doi: 10.5402/2012/482802
50. Luger T, Suls J, Vander Weg M. How robust is the association between smoking and depression in adults? a meta-analysis using linear mixed-effects models. Addict Behav. (2014) 39(10):1418–29. doi: 10.1016/j.addbeh.2014.05.011
51. Pedrero Pérez E, Ruiz Sánchez de León J, Rojo Mota G, Llanero Luque M, Pedrero Aguilar J, Morales Alonso S, et al. Information and communication technologies (ICT): abuse of the Internet, video games, mobile phones, instant messaging and social networks through MULTICAGE-ITC. Adicciones. (2017) 30(1):19. doi: 10.20882/adicciones.806
52. National Institute Mental of Heath. Chronic Illness and Mental Health: How to Recognize and Treat Depression. (2017). Bethesda, MA: National Institute Mental of Heath.
53. Read J, Sharpe L, Modini M, Dear B. Multimorbidity and depression: a systematic review and meta-analysis. J Affect Disord. (2017) 221:36–46. doi: 10.1016/j.jad.2017.06.009
54. Vancampfort D, Koyanagi A, Hallgren M, Probst M, Stubbs B. The relationship between chronic physical conditions, multimorbidity and anxiety in the general population: a global perspective across 42 countries. Gen Hosp Psychiatry. (2017) 45:1–6. doi: 10.1016/j.genhosppsych.2016.11.002
55. Scott K, Lim C, Al-Hamzawi A, Alonso J, Bruffaerts R, Caldas-de-Almeida J, et al. Association of mental disorders with subsequent chronic physical conditions. JAMA Psychiatry. (2016) 73(2):150–8. doi: 10.1001/jamapsychiatry.2015.2688
56. Zhang J, Kahana B, Kahana E, Hu B, Pozuelo L. Joint modeling of longitudinal changes in depressive symptoms and mortality in a sample of community-dwelling elderly people. Psychosom Med. (2009) 71(7):704–14. doi: 10.1097/PSY.0b013e3181ac9bce
57. Santomauro D, Mantilla Herrera A, Shadid J, Zheng P, Ashbaugh C, Pigott D, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. (2021) 398(10312):1700–12. doi: 10.1016/S0140-6736(21)02143-7
58. Parés-Badell O, Barbaglia G, Jerinic P, Gustavsson A, Salvador-Carulla L, Alonso J. Cost of disorders of the brain in Spain. Foffani G, editor. PLoS One. (2014) 9(8):e105471. doi: 10.1371/journal.pone.0105471
59. Salud y Sanidad | Transparencia Aragón. Available Online at: https://transparencia.aragon.es/content/salud-y-sanidad (accessed April 11, 2023).
60. Butler D, Fons D, Fisher T, Sanders J, Bodenhamer S, Owen J, et al. A review of the benefits and limitations of a primary care-embedded psychiatric consultation service in a medically underserved setting. Int. J. Psychiatry Med. (2018) 53(5–6):415–26. doi: 10.1177/0091217418791456
61. Galvez-Llompart A, Valor Gisbert M, Perez-Almarcha M, Ballester-Gracia I, Canete-Nicolas C, Reig-Cebria M, et al. Impacto en la asistencia en salud mental tras la colaboración entre atención primaria y salud mental. Medicina de Familia Semergen. (2021) 47(6):385–93. doi: 10.1016/j.semerg.2021.04.006
62. World Health Organization. Mental Health in Primary Care: Illusion or Inclusion?. Geneva: World Health Organization (2018).
63. World Health Organization. Comprehensive Mental Health Action Plan 2013–203. Geneva: World Health Organization (2021).
64. World Health Organization. Global Status Report on Noncommunicable Diseases 2014. Geneva: World Health Organization (2014).
65. Salazar FP, Manterola C, Quiroz SG, García MN, Otzen HT, Mora VM, et al. Estudios de cohortes. 1a parte. Descripción, metodología y aplicaciones. Rev Cir. (2019) 71:482–493. doi: 10.35687/s2452-45492019005431
66. Government of Aragon. Aragón Sanitary Map (2022). Available online at: https://www.aragon.es/-/mapa-sanitario (accessed August 31, 2022).
67. Government of Aragon. Aragonese Institute of Statistics (IAEST). (2022). Available Online at: https://www.aragon.es/-/demografia-y-poblacion (accessed August 31, 2022).
68. World Health Organization. Depressive Disorde. (2023). Available Online at: https://www.who.int/news-room/fact-sheets/detail/depression (accessed April 10, 2023).
70. Kroenke K, Spitzer R. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. (2002) 32(9):509–15. doi: 10.3928/0048-5713-20020901-06
71. Muñoz-Navarro R, Cano-Vindel A, Medrano L, Schmitz F, Ruiz-Rodríguez P, Abellán-Maeso C, et al. Utility of the PHQ-9 to identify major depressive disorder in adult patients in Spanish primary care centres. BMC Psychiatry. (2017) 17(1):291. doi: 10.1186/s12888-017-1450-8
72. Beck A, Steer R, Ball R, Ranieri W. Comparison of beck depression inventories-IA and-II in psychiatric outpatients. J Pers Assess. (1996) 67(3):588–97. doi: 10.1207/s15327752jpa6703_13
73. Sanz J, Perdigón A, Vázquez C. The spanish adaptation of Beck’s depression inventory-II (BDI-II): 2. psychometric properties in the general population. Clin Salud. (2003) 14(3):249–80.
74. Spitzer R, Kroenke K, Williams J, Löwe BA. Brief measure for assessing generalized anxiety disorder. Arch Intern Med. (2006) 166(10):1092. doi: 10.1001/archinte.166.10.1092
75. Garcia-Campayo J, Zamorano E, Ruiz M, Pardo A, Perez-Paramo M, Lopez-Gomez V, et al. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual Life Outcomes. (2010) 8(1):8. doi: 10.1186/1477-7525-8-8
76. Saunders J, Aasland O, Babor T. De la Fuente J, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. (1993) 88(6):791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x
77. Fernández-Montalvo J, Echeburúa-Odriozola E, Báez-Gallo C. The brief pathological gambling questionnaire (BPGQ): a new screening instrument. Análisis y modificación de conducta. (1995) 21(76):211–23.
78. Bosscher R, Smit J, Kempen G. General competency expectations in the elderly: an examination of the psychometric characteristics of the general competency scale (ALCOS). Nederlands Tijdschrift voor de Psychologie. (1997) 52:239–48.
79. Herrero R, Espinoza M, Molinari G, Etchemendy E, Garcia-Palacios A, Botella C, et al. Psychometric properties of the general self efficacy-12 scale in Spanish: general and clinical population samples. Compr Psychiatry. (2014) 55(7):1738–43. doi: 10.1016/j.comppsych.2014.05.015
80. Notario-Pacheco B, Solera-Martínez M, Serrano-Parra M, Bartolomé-Gutiérrez R, García-Campayo J, Martínez-Vizcaíno V. Reliability and validity of the Spanish version of the 10-item connor-davidson resilience scale (10-item CD-RISC) in young adults. Health Qual Life Outcomes. (2011) 9(1):63. doi: 10.1186/1477-7525-9-63
81. Moreno B, Alonso M, Álvaréz E. Sense of coherence, resistant, personality, self-esteem and health. J Health Psychol. (1997) 9(2):115–37.
82. Martín-Albo J, Núñez J, Navarro J, Grijalvo F. The Rosenberg self-esteem scale: translation and validation in university students. Spanish J Psychol. (2007) 10(2):458–67. doi: 10.1017/S1138741600006727
83. Moreno-Chico C, González-de Paz L, Monforte-Royo C, Arrighi E, Navarro-Rubio M. Gallart Fernández-Puebla a. adaptation to European Spanish and psychometric properties of the patient activation measure 13 in patients with chronic diseases. Fam Pract. (2017) 34(5):627–34. doi: 10.1093/fampra/cmx022
84. Nolasco A, Barona C, Tamayo-Fonseca N, Irles M, Más R, Tuells J, et al. Health literacy: psychometric behaviour of the HLS-EU-Q16 questionnaire. Gac Sanit. (2020) 34:399–402. doi: 10.1016/j.gaceta.2018.08.006
85. The EuroQol Group. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy. (1990):199–208. doi: 10.1016/0168-8510(90)90421-9
86. Badia X, Roset M, Montserrat S, Herdman M, Segura A. The Spanish version of EuroQol: a description and its applications. European quality of life scale. Med Clin. (1999) 112:79–85.
87. Schröder H, Fitó M, Estruch R, Martínez-González M, Corella D, Salas-Salvadó J, et al. A short screener is valid for assessing mediterranean diet adherence among older Spanish men and women. J Nutr. (2011) 141(6):1140–5. doi: 10.3945/jn.110.135566
88. Schröder H, Zomeño M, Martínez-González M, Salas-Salvadó J, Corella D, Vioque J, et al. Validity of the energy-restricted mediterranean diet adherence screener. Clin Nutr. (2021) 40(8):4971–9. doi: 10.1016/j.clnu.2021.06.030
89. Buysse D, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28(2):193–213. doi: 10.1016/0165-1781(89)90047-4
90. Royuela-Rico A, Macías-Fernández J. Clinimetric properties of the spanish version of the pittsburgh questionnaire. Vigilia-Sueño. (1997) 9(2):81–94.
91. Craig C, Marshall A, Sjöström M, Bauman A, Booth M, Ainsworth B, et al. International physical activity questionnaire: 12-Country reliability and validity. Med Sci Sports Exerc. (2003) 35(8):1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
92. Puig-Ribera A, Martín-Cantera C, Puigdomenech E, Real J, Romaguera M, Magdalena-Belio J, et al. Screening physical activity in family practice: validity of the Spanish version of a brief physical activity questionnaire. Reddy H, editor. PLoS One. (2015) 10:e0136870. doi: 10.1371/journal.pone.0136870
93. Hayes A. Introduction to Mediation, Moderation, and Conditional Process Analysis. a Regression-Based Approach. 3rd ed. New York, NY: Guildford Press (2022).
94. Hayes A, Cai L. Using heteroskedasticity-consistent standard error estimators in OLS regression: an introduction and software implementation. Behav Res Methods. (2007) 39(4):709–22. doi: 10.3758/BF03192961
96. R Core Team. R: a Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2019).
97. James S, Abate D, Abate K, Abay S, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of disease study 2017. Lancet. (2018) 392(10159):1789–858.
98. Pence B, O’Donnell J, Gaynes B. The depression treatment cascade in primary care: a public health perspective. Curr Psychiatry Rep. (2012) 14(4):328–35. doi: 10.1007/s11920-012-0274-y
99. World Health Organization. Global Strategy to Reduce the Harmful use of Alcohol. Geneva: World Health Organization (2010).
100. World Health Organization.Addictive Behaviour. (2023). Available Online at: https://www.who.int/health-topics/addictive-behaviour#tab=tab_1 (accessed April 24, 2023).
101. Mittelmark M, Sagy S, Eriksson M, Bauer G, Pelikan J, Lindström B, et al. The Handbook of Salutogenesis. Cham: Springer International Publishing (2017). doi: 10.1007/978-3-319-04600-6
102. Wicke F, Dinh T, Riedel-Heller S, Weyerer S, König H, Gensichen J, et al. Predictors of change in depressive symptoms in older and multimorbid patients: a longitudinal analysis of the multicare cohort. Aging Ment Health. (2022) 26(4):818–27. doi: 10.1080/13607863.2021.1902470
103. Martins E, Salamene L, Lucchetti A, Lucchetti G. The role of positive behaviors, attitudes and virtues in the mental health of community-dwelling older adults: a 1-year follow-up study. J Psychosom Res. (2022) 154:110721. doi: 10.1016/j.jpsychores.2022.110721
104. Lee J. Trajectories of depression between 30s and 50s: latent growth modeling. Issues Ment Health Nurs. (2020) 41(7):624–36. doi: 10.1080/01612840.2019.1688438
105. Buitrago Ramírez F, Ciurana Misol R, Chocrón Bentata L, Carmen Fernández Alonso M, García Campayo J, Montón Franco C, et al. Prevención de los trastornos de la salud mental en atención primaria. actualización PAPPS 2018. Aten Primaria. (2018) 50:83–108. doi: 10.1016/S0212-6567(18)30364-0
106. Gómez-Gómez I, Motrico E, Moreno-Peral P, Casajuana-Closas M, López-Jiménez T, Zabaleta-del-Olmo E, et al. A multiple health behaviour change intervention to prevent depression: a randomized controlled trial. Gen Hosp Psychiatry. (2023) 82:86–94. doi: 10.1016/j.genhosppsych.2023.02.004
107. Eurostat. Demography of Europe — Statistics visualised —. 2021 ed. Luxembourg: Eurostat (2021).
108. Siniscalchi K, Broome M, Fish J, Ventimiglia J, Thompson J, Roy P, et al. Depression screening and measurement-based care in primary care. J Prim Care Community Health. (2020) 11:215013272093126. doi: 10.1177/2150132720931261
Keywords: behavior and behavior mechanism, anxiety, depression, mental health, primary health care
Citation: Méndez-López F, Oliván-Blázquez B, Domínguez-García M, Bartolomé-Moreno C, Rabanaque I and Magallón-Botaya R (2023) Protocol for an observational cohort study on psychological, addictive, lifestyle behavior and highly prevalent affective disorders in primary health care adults. Front. Psychiatry 14:1121389. doi: 10.3389/fpsyt.2023.1121389
Received: 11 December 2022; Accepted: 23 May 2023;
Published: 09 June 2023.
Edited by:
Jesus Gonzalez-Lama, Maimonides Biomedical Research Institute of Cordoba (IMIBIC), SpainReviewed by:
Rebecca Erschens, University of Tübingen, GermanyJoanna Blahopoulou, University of the Balearic Islands, Spain
Copyright © 2023 Méndez-López, Oliván-Blázquez, Domínguez-García, Bartolomé-Moreno, Rabanaque and Magallón-Botaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bárbara Oliván-Blázquez, Ym9saXZhbkB1bml6YXIuZXM=