
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 09 March 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1121313
 Anvar Sadath1,2*
Anvar Sadath1,2* M. Isabela Troya1,2
M. Isabela Troya1,2 Sarah Nicholson1,2Grace Cully1,2†Dorothy Leahy3Ana Paula Ramos Costa1,2
Sarah Nicholson1,2Grace Cully1,2†Dorothy Leahy3Ana Paula Ramos Costa1,2 Ruth Benson1,2
Ruth Benson1,2 Paul Corcoran1,2
Paul Corcoran1,2 Eve Griffin1,2
Eve Griffin1,2 Eunice Phillip1,2Eugene Cassidy4,5Anne Jeffers6Frances Shiely1,7Íñigo Alberdi-Páramo8Katerina Kavalidou2,9
Eunice Phillip1,2Eugene Cassidy4,5Anne Jeffers6Frances Shiely1,7Íñigo Alberdi-Páramo8Katerina Kavalidou2,9 Ella Arensman1,2,10
Ella Arensman1,2,10Background: Research has indicated an increased risk of self-harm repetition and suicide among individuals with frequent self-harm episodes. Co-occurring physical and mental illness further increases the risk of self-harm and suicide. However, the association between this co-occurrence and frequent self-harm episodes is not well understood. The objectives of the study were (a) to examine the sociodemographic and clinical profile of individuals with frequent self-harm (regardless of suicidal intent) episodes and, (b) the association between physical and mental illness comorbidity, self-harm repetition, highly lethal self-harm methods, and suicide intent.
Methods: The study included consecutive patients with five or more self-harm presentations to Emergency Departments across three general hospitals in the Republic of Ireland. The study included file reviews (n = 183) and semi-structured interviews (n = 36). Multivariate logistic regression models and independent samples t-tests were used to test the association between the sociodemographic and physical and mental disorders comorbidity on highly lethal self-harm methods and suicidal intent, respectively. Thematic analysis was applied to identify themes related to physical and mental illness comorbidity and frequent self-harm repetition.
Findings: The majority of individuals with frequent self-harm episodes were female (59.6%), single (56.1%), and unemployed (57.4%). The predominant current self-harm method was drug overdose (60%). Almost 90% of the participants had history of a mental or behavioral disorder, and 56.8% had recent physical illness. The most common psychiatric diagnoses were alcohol use disorders (51.1%), borderline personality disorder (44.0%), and major depressive disorder (37.8%). Male gender (OR = 2.89) and alcohol abuse (OR = 2.64) predicted the risk of a highly lethal self-harm method. Suicide intent was significantly higher among those with a diagnosis of major depressive disorder (t = 2.43; p = 0.020). Major qualitative themes were (a) the functional meaning of self-harm (b) self-harm comorbidity (c) family psychiatric history and (d) contacts with mental health services. Participants described experiencing an uncontrollable self-harm urge, and self-harm was referred to as a way to get relief from emotional pain or self-punishment to cope with anger and stressors.
Conclusion: Physical and mental illness comorbidity was high among individuals with frequent self-harm episodes. Male gender and alcohol abuse were associated with highly lethal self-harm methods. The mental and physical illness comorbidity of individuals with frequent self-harm episodes should be addressed via a biopsychosocial assessment and subsequent indicated treatment interventions.
Suicidal behavior is a leading cause of death and disability worldwide (1, 2). Although there are inconsistencies and varying definitions, suicidal behavior as a general term encompassing any suicidal thought or actions without taking additional steps to distinguish thoughts from plans, from non-fatal attempts, and from attempts that result in death (2). The term self-harm, used throughout this manuscript, refers to self-harm behavior regardless of suicidal intent. According to the Global Burden of Disease study 2019, self-harm was the main contributor to Years of Life Lost (YLL) from mental disorders in 31 European countries (1).
Self-harm is associated with multiple mental health conditions, including mood disorders (3–5), borderline personality disorder (BPD) (4, 6, 7), alcohol abuse, schizophrenia (5), adjustment disorder (3), eating disorders (7), and attention deficit hyper activity disorder (8). Emotional dysregulation, specifically a non-acceptance of emotional responses, lack of emotional awareness, difficulties in impulse control and engaging in goal-directed behavior, are all associated with self-harm (9). The act of self-harm has been described to be conducted with the intent to alleviate negative affect, and the negative affect and arousal are reduced by the performance of self-harm (10). Furthermore, studies that have examined self-harm severity/lethality in connection with mental disorders report that alcohol abuse (11, 12), BPD (13), and depression further increase the risk of more repeated highly lethal self-harm episodes (HLSMs) (14).
While the association between mental health conditions and self-harm is well established (15), the role of physical illness in self-harm or suicidal thoughts is less known. Previous research indicates that several chronic physical illnesses (5, 16, 17) including epilepsy, asthma, migraine, psoriasis, diabetes mellitus, eczema, and inflammatory polyarthritis are associated with an increased risk of self-harm (5). Suicide risk increases with the number of co-occurring physical illnesses (5). While a physical illness alone is not associated with self-harm or suicidal thoughts (15), the combination of physical and mental health conditions significantly increases the risk of both (15), with an elevated risk related to the onset of both physical and disorders occurring close in time to one another (18). Mental disorders, especially depression, often coexists among people with chronic physical illness (17, 19), and this is associated with heightened risk of self-harm. There is a wealth of studies in this area (20) albeit, specific to older people. The findings of a systematic review revealed that functional disability and numerous specific conditions (including malignant diseases, neurological disorders, pain, chronic obstructive pulmonary disease, liver disease, male genital disorders, and arthritis/arthrosis) were associated with self-harm among older persons (20).
Although mental and physical disorders are commonly reported among individuals who self-harm (5, 21), comorbidities specific to individuals with frequent self-harm episodes have rarely been studied. Yet, they are a high risk group due to the strong association between previous self-harm, future self-harm (22–26) and suicide (27, 28). The risk of self-harm repetition increases with each additional hospital self-harm presentation (23, 29), with the highest risk among those with a history of five or more presentations (30). Often referred to as major repeaters (30), these individuals represent a proportion of high suicide risk (31, 32). Individuals with frequent self-harm episodes comprise more than 10% of all self-harm presentations (29), frequently engage with health services (33) and have difficulties in controlling self-harm behavior, although the broader characteristics of this sub-group are under-researched (31, 32, 34). To our knowledge, only a few studies are available among this group (31, 35), and these studies included small samples of individuals with frequent self-harm episodes. These studies show that individuals with frequent self-harm episodes predominantly represent females and have a diagnosis of psychiatric illness (31, 35). Evidence is still lacking to conclusively provide a profile of these patients and associated comorbidities. Within this context, the main objectives of the present study were (a) to examine the sociodemographic and clinical profile of individuals with frequent self-harm episodes, (b) the association between physical and mental illness comorbidity and highly lethal self-harm methods (HLSMs), (c) the association between sociodemographic variables (age, gender, marital status, living and employment status) and HLSMs, (d) the association between suicide intent and psychiatric illnesses, and (e) to investigate the comorbidity factors contributing to self-harm repetition.
This study uses a mixed-methods convergent parallel design in which quantitative and qualitative data were collected and analyzed simultaneously (36). The study included retrospective file review and semi structured interviews (Figure 1).
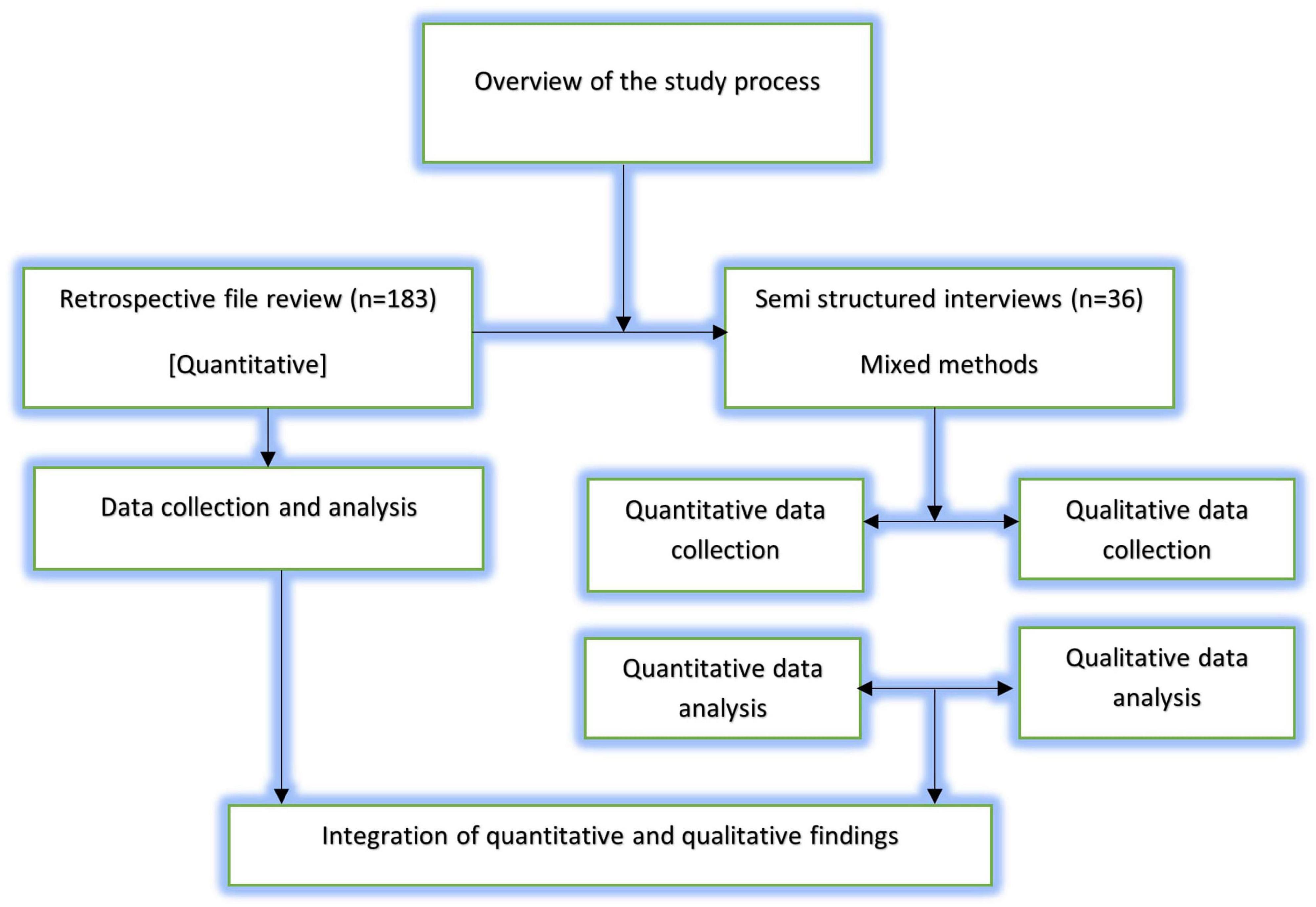
Figure 1. Overview of the study process.
All consecutive case files of individuals with frequent self-harm episodes from three general hospital Emergency Departments (ED) in the Republic of Ireland between March 2016 and July 2019 were reviewed.
Inclusion criteria: aged 18 and older, a history of five or more self-harm presentation to the ED, and alive on admission to the hospital following the self-harm episode. In each hospital, potential cases for review were first identified by hospital staff, i.e., Clinical Nurse Specialists or Crisis Nurses or Non-Consultant Hospital Doctors in the ED before the researchers were provided with access to the patients’ case files. The hospital staff were involved in screening self-harm cases according to the inclusion and exclusion criteria. The researchers conducted regular reviews of all self-harm cases to ensure that inclusion and exclusion criteria were being applied correctly and no cases were missed.
Data extraction was performed by the research team and included: medical history; psychiatric history; diagnosis; self-harm history; personal and family history; and sociodemographic information. Any relevant missing information in the files was coded accordingly by the research team.
Self-harm was defined as “an act with non-fatal outcome where an individual deliberately initiates a non-habitual behavior that without intervention from others will cause self-harm” (37). This included both acts with and without the intention to die. Frequent self-harm was defined as five or more previous self-harm presentations to hospital emergency departments, including the index presentation. Comorbidity was defined in the literature as “any distinct additional entity that has existed or may occur during the clinical course of a patient who has the index disease under study” (38). We operationally defined comorbidity as a co-occurring physical illness or mental disorder, or substance use disorder which existed with a self-harm episode among individuals with frequent self-harm episodes. We defined individuals with frequent self-harm episodes as those with a history of five or more self-harm presentations to the hospitals. We defined HLSMs in accordance with the criteria of Persett et al. (39), which includes hanging, strangulation, suffocation, cutting, submersion, firearm, jumping from a height or jumping in front of a moving object, fire and flames, and crashing of motor vehicles. Co-occurrence of any of these methods along with intentional drug overdose (IDO) was also recorded for this category. IDO in the absence of any other self-harm method was considered as non-HLSMs. Appendix 1 includes operationalization and dummy codes of the key independent (e.g., age, gender, marital status, BPD etc.) and dependent variable (HLSMs).
From the consecutive individuals with frequent self-harm episodes cases identified through file reviews, a subgroup participated in semi structured interview study. The interviews and file reviews were conducted by trained members of the research team comprising of postdoctoral researchers, a PhD scholar, and a research officer, under the supervision of the principal investigator. Following interest from the patients, researchers subsequently provided a brief introduction of the research with an invitation letter and study information leaflet via post or in person whilst at the hospital premises. When patients agreed and consented to participation, the patient’s preferred time and venue were considered when scheduling the interview.
A semi-structured interview schedule, containing both closed and open-ended questions, was used for the interviews. The interview schedule covered standard sociodemographic data, medical and psychiatric history and psychosocial variables representing risk and protective factors for self-harm. The interview schedule used for this study was flexible, enabling the exploration of further details as required.
Suicide intent during the index self-harm presentation was assessed using the Beck Suicide Intent Scale (SIS) (40). The SIS is a fifteen-item interviewer-administered questionnaire, designed to assess the severity of suicidal intent associated with self-harm episodes. Each item scores 0–2, giving a total score range of 0–30, whereby a high score indicates high levels of suicide intent. The questionnaire is divided into two sections: the first eight items comprise the “circumstances” section, concerned with the objective circumstances of the self-harm act. The remaining seven items form the “self-report” section and are based on the patient’s own reconstruction of their feelings and thoughts at the time of the self-harm act. The SIS fifteen-item Cronbach’s alpha score in the current sample was 0.84.
The study complies with the Irish Data Protection Act of 1988 (41), the Irish Data Protection Amendment Act of 2003 (41) and General Data Protection Regulation (GDPR) 2018 (42). Ethical approval was obtained before the implementation of the GDPR. Following the implementation of GDPR, information leaflets and consent forms were updated to comply with GDPR and subsequently approved by the ethics committees. All participants included in the interview study provided written informed consent.
The quantitative data collected through the file reviews and interviews were entered into Statistical Package for Social Sciences (SPSS) (version 26). Descriptive analyses were performed on data obtained from the file review and semi-structured interviews. Fisher’s exact test (FET) was used to compare the sociodemographic variables in both data sources. For all statistical tests, categorical variables were condensed into a binary response.
The association of sociodemographic variables, physical and mental disorders comorbidity and HLSMs was examined using FET and Odds Ratios with p-values and 95% confidence intervals provided. A multivariable logistic regression model was estimated introducing sociodemographic and physical and mental disorders comorbidity variables statistically significant in the FET. This variable selection procedure has the capability of retaining important confounding variables, resulting potentially in a richer model (43). The significant predictors from the first model (i.e., gender and alcohol use disorders) were further examined in an additional regression model for understanding the consistency of these predictors over two self-harm episodes. For the second model, “recent HLSMs” was treated as the dependent variable. All categorical variables were dummy coded (see Appendix 1). Further, we tested multicollinearity using linear regression and there was no evidence of this in the model (variance inflation factor ≤ 1.03).
An Independent t-test was used to test the association between physical and mental disorders comorbidity and suicide intent. The physical and mental disorders (depression, alcohol abuse, and chronic physical pain) were treated as grouping variables with two categories (yes/no) and SIS total score as a dependent variable. The SIS total score was normally distributed (Shapiro–Wilk test = p > 0.05).
For the file review study, missing data occurred due to incomplete assessments. The missing data frequencies for different study variables ranged from n = 0–58. Missing data were not accounted for in the descriptive analysis. The percentages were calculated after exclusion of cases with missing values for the variable in question. Missing data were not replaced for the regression models, and the cases with missing data were excluded from the analysis on variable-by-variable basis.
Following the transcription of the interviews, thematic analysis was performed to identify themes related to physical and mental disorders comorbidity and self-harm. We followed the five key steps for conducting thematic analysis developed by Braun and Clarke (44).
The verbatim transcription was performed whereby the audiotaped interviews were transcribed into text. A list of codes was developed based on the reading of the transcripts, and these codes were allocated to the data, which helped to classify and stratify the data in a logical way, resulting in a proposed set of themes. The author (AS) performed the initial coding and analysis, and the themes were finalized in agreement with two other authors (IT and SN) who were involved in transcribing the interviews.
We identified 191 individuals with frequent self-harm episodes, and eight individuals were excluded due to incomplete data, resulting in 183 files being included in the file review study.
From the consecutive cases identified through file reviews (n = 183), 79 (43%) were not approached for the semi-structured interviews. They were either deemed not suitable for interviews by hospital staff or consultant doctors due to acute symptoms (e.g., severe psychotic or mood symptoms), or were unconscious or in induced coma because of the severity of the self-harm act, history of violence and aggressive behavior, risk to researchers or their contact details were missing. The remaining patients (n = 104) were contacted by the research team via telephone or via face-to-face contact during their hospital visits to invite them to participate in the semi-structured interview study. However, 68 patients did not participate as they either refused (n = 22) or were never answered our phone or phone disconnected (n = 46). A total of 36 respondents participated in the semi-structured interview study, representing 20% of the file review sample (Figure 2).
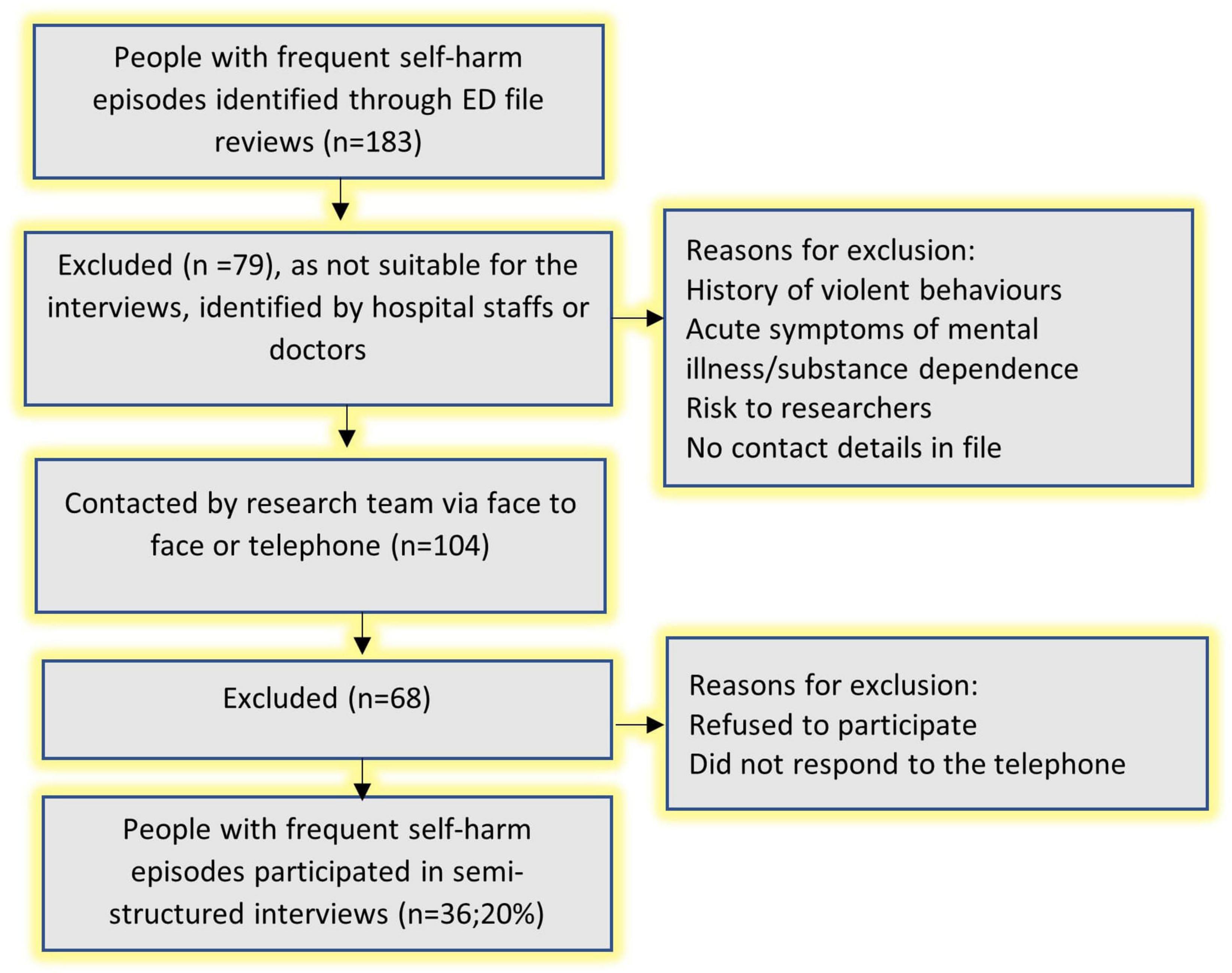
Figure 2. Recruitment of individuals with frequent self-harm episodes for semi-structured interviews.
The interviews ranged from 1 h and 10 min to 4 h and 18 min. Of the 36 participants interviewed, 31 agreed to (audio) record the interviews. For the other participants, we took notes on their responses. The data collection was completed between March 2016 and September 2019.
Table 1 shows the comparison of study participants in file review and interviews, and there was no significant difference between the two groups regarding sociodemographic characteristics.
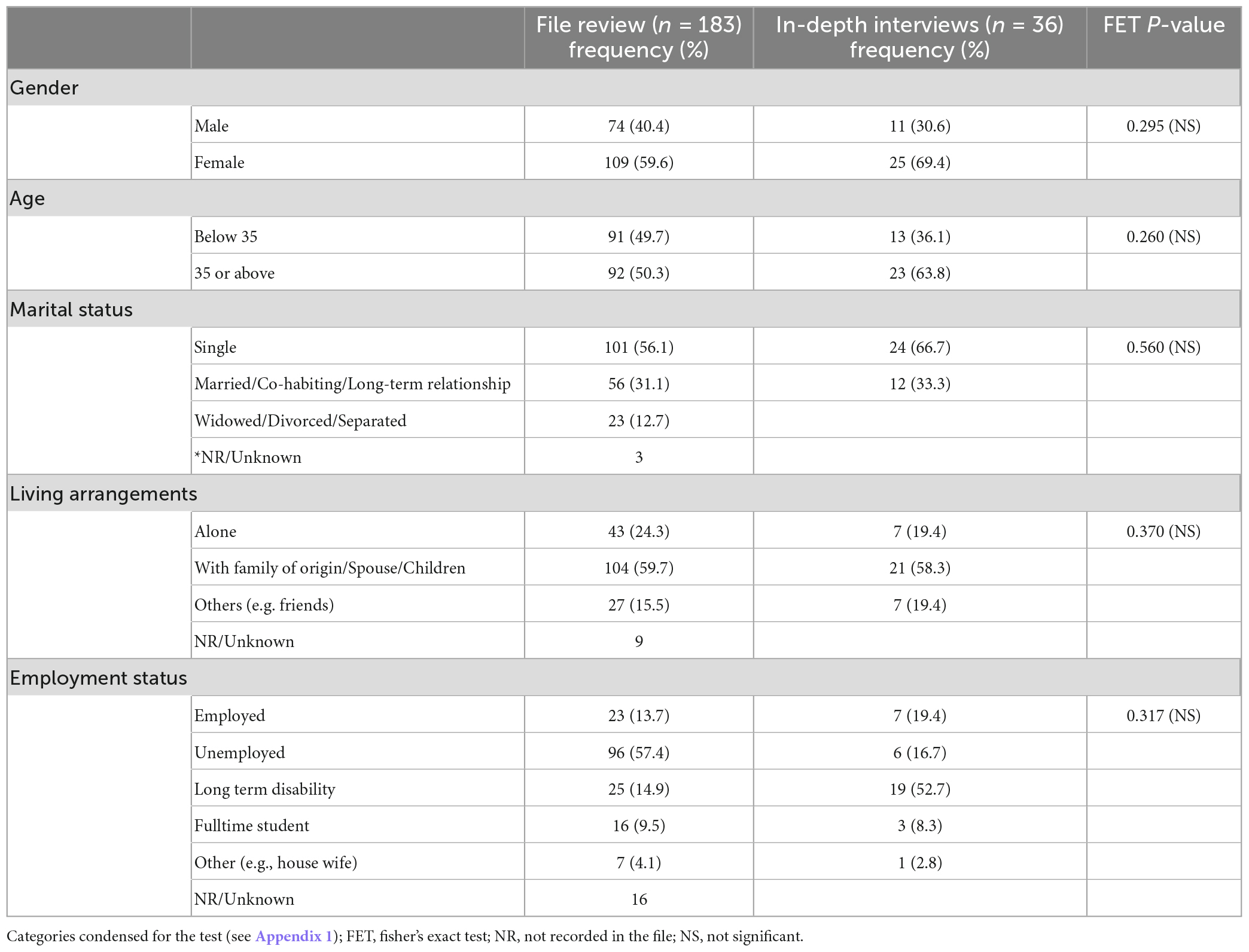
Table 1. Sociodemographic and self-harm characteristics of the study participants.
As shown in Table 2, the majority of participants had engaged in IDO in their current (61.3%) and recent (67.3%) self-harm episodes.
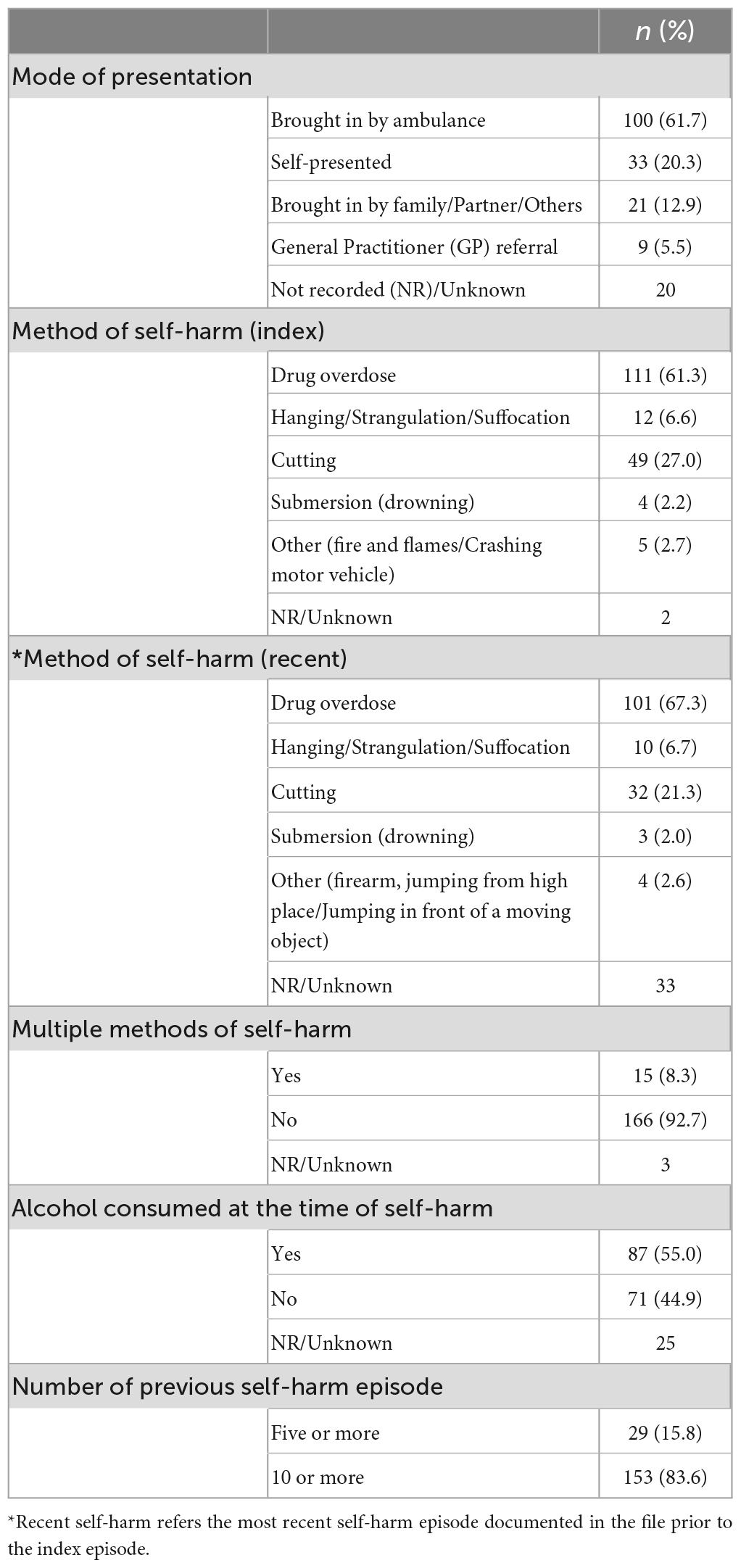
Table 2. Self-harm characteristics of the participants in file review study.
Table 3 displays physical and mental disorders comorbidity and treatment details of the study participants. As the table indicates, around 90% of the respondents were diagnosed with any mental or behavioral disorders and 56.8% had a physical illness in the recent past. Among the participants with a physical illness, almost all (96.7%) had a diagnosis of a mental/behavioral disorder.
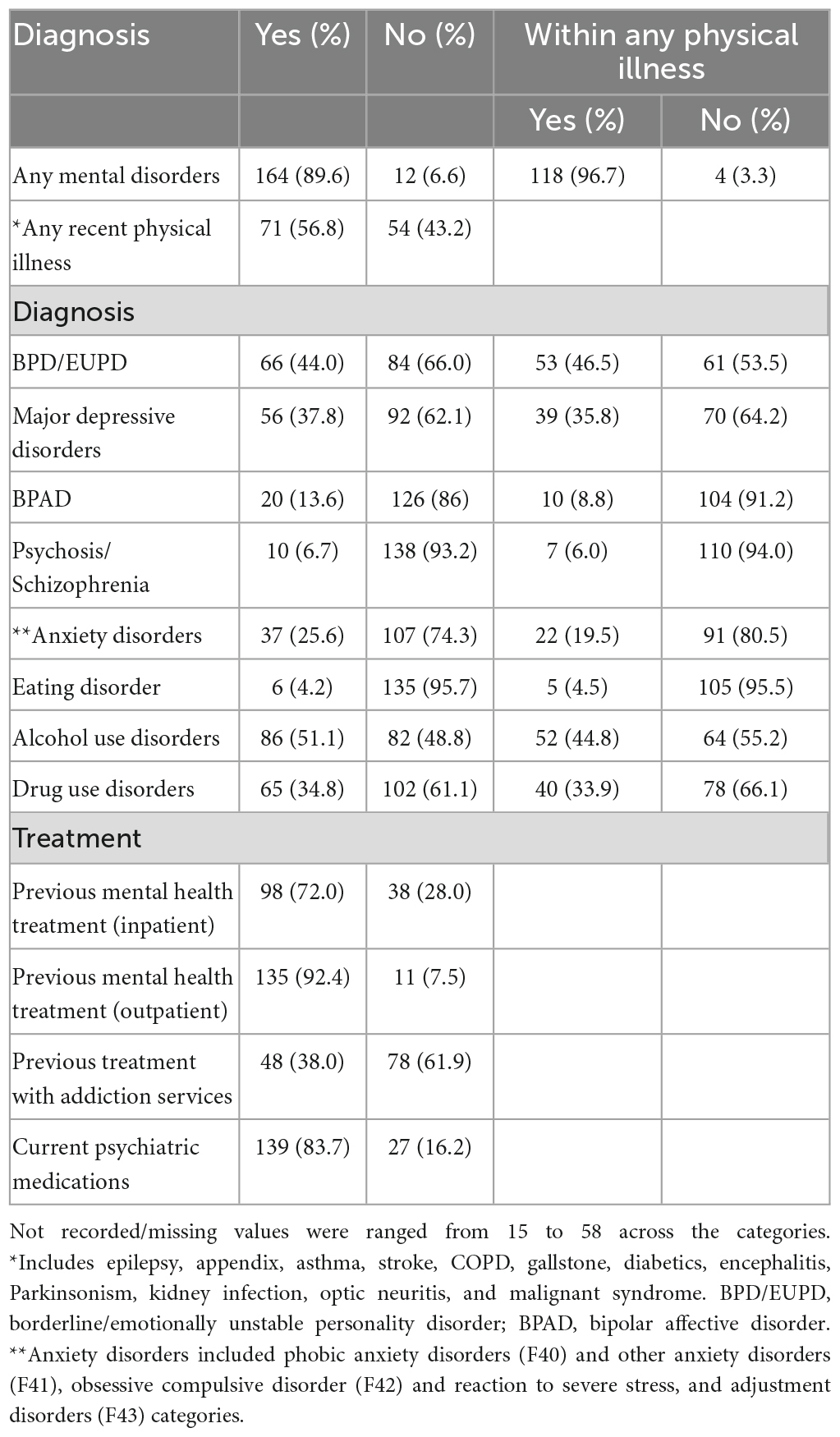
Table 3. Mental disorder, physical illness, and treatment details of the participants in file review study.
Among the participants (total n = 36), the majority had chronic physical pain in the past year (72.2%), one-fourth of the participants had asthma (25%), more than one-fifth had orthopedic (19.4%), or metabolic problems (22.2%). More than half of the participants had a recent reduction in physical capabilities (55.6%) and 63.9% were on medication for a physical illness. The participants had history of various traumatic life events including, violent sexual assault (77.8%), directly witnessing a sudden death (22.2%), sudden death of a loved one (63.9%) severe bullying or torture (55.6%), and humiliation or loss of face (19.4%). Many participants had family history of self-harm/suicide (47.2%), mental illness (63.9%), substance abuse (69.4%), and violent behavior (55.6%).
Gender, employment status and alcohol use disorders were significantly associated with index HLSMs in FET, and these variables were subsequently entered into multivariate binary logistic regression model (see Table 4). The Omnibus tests of model coefficients was significant (χ2 = 17.63; df = 3; p = 0.001) while the Hosmer and Lemeshow test was not significant (p = 0.726), indicating that the model fitted the data well. Overall, the model explained 14.6% (Nagelkerke R2) of variance on the index HLSMs. Male gender (X2 = 8.45; P = 0.004; OR = 2.89) and alcohol use disorders (X2 = 7.32; P = 0.007; OR = 2.64) increased the likelihood of a HLSMs. Employment status was not significant (P > 0.05) when adjusted for confounders.
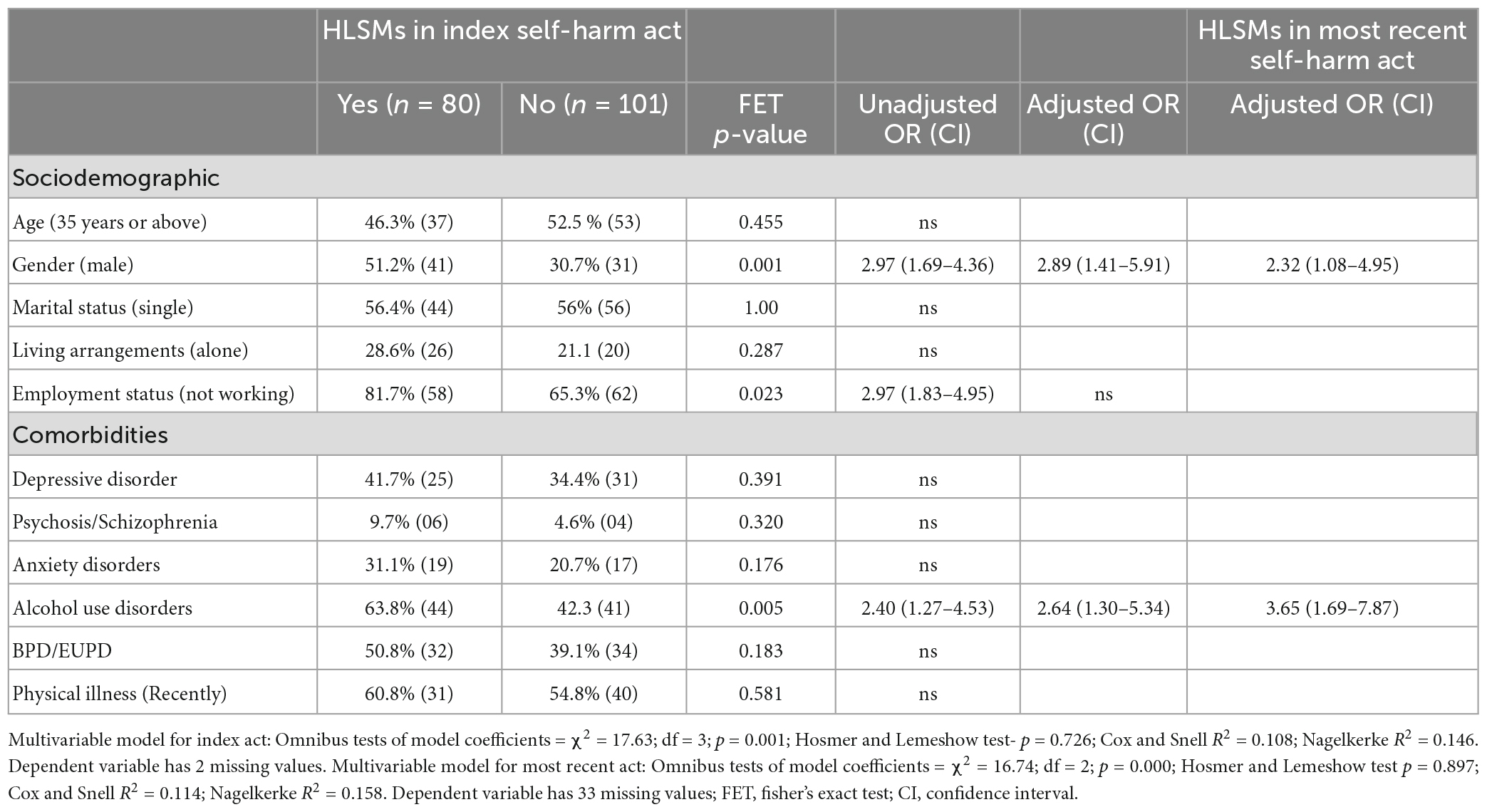
Table 4. Association of sociodemographic and comorbidity variables with the use of highly lethal self-harm methods in the index self-harm act and in the most recent self-harm act.
We further conducted a multivariate binary logistic regression model to validate the previously identified predictors (i.e., gender and alcohol use disorders) by treating the recent HLSMs as a dependent variable (see Table 4). The Omnibus tests of model coefficients was significant (χ2 = 16.74; df = 2; p = 0.000) while the Hosmer and Lemeshow test was not significant (p = 0.899), indicating that the model fit that data well. Overall, the model explained 15.8% (Nagelkerke R2) of variance on a recent HLSMs. Male gender (X2 = 4.73; P = 0.030; OR = 2.32) and alcohol use disorders (X2 = 10.89; P = 0.001; OR = 3.65) increased the likelihood of a recent HLSMs (see Table 4).
The mean score of the SIS was 17 (SD = 6.48), indicating mild to moderate suicide intent during the index self-harm. For the subdomains, “circumstances around the self-harm act,” the eight-item mean score was 6.74 (SD = 2.86), which indicated mild suicide intent while “thoughts and feelings at the time of self-harm act,” the seven-item mean score was 9.96 (SD = 4.41), indicating moderate suicide intent.
An independent sample t-test was conducted to compare suicide intent of those with a diagnosis of depressive disorder, personality disorder, alcohol use disorders, and chronic physical pain. There was a significant difference in suicide intent score between those with a diagnosis of depressive disorder (M = 19.15; SD = 4.08) and those without this diagnosis (M = 14.58; SD = 6.95); (t = 2.43; p = 0.020) (Table 5).
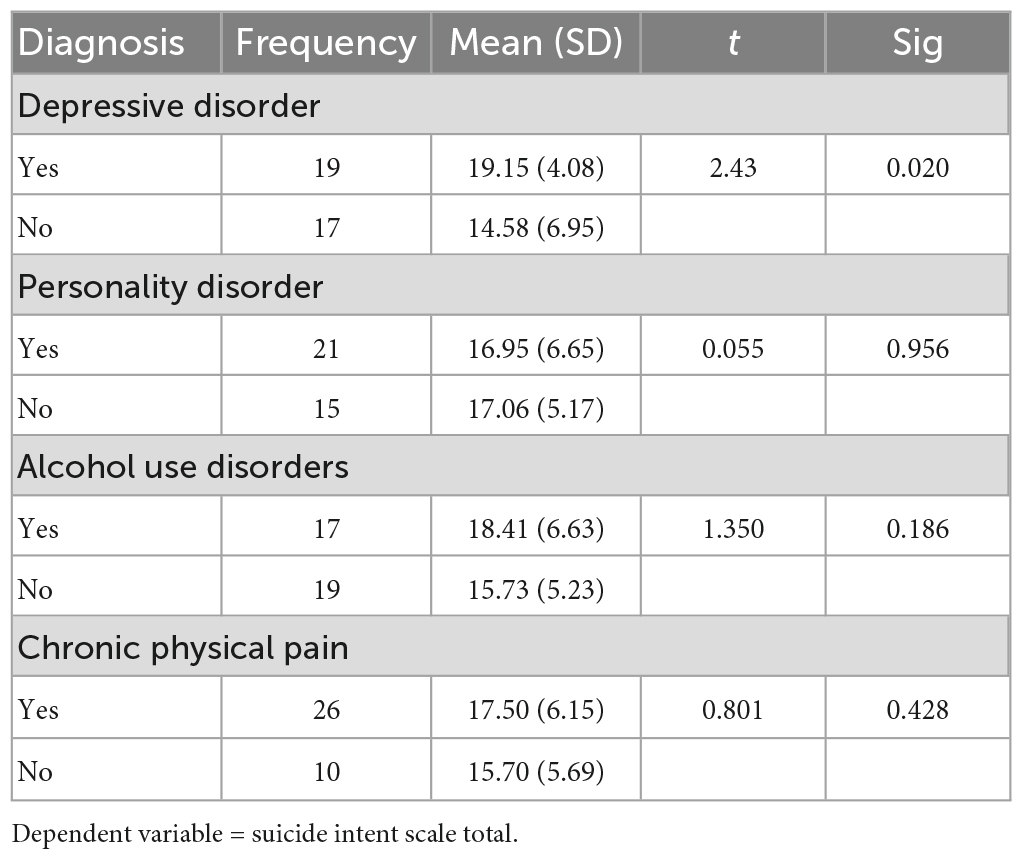
Table 5. Association of physical and mental illness comorbidity and suicide intent among individuals with frequent self-harm episodes participated in the interview study (n = 36).
Thematic analysis resulted in four themes associated with self-harm and physical and mental disorders.
Self-harm was described as an uncontrollable urge especially those with a diagnosis of BPD. The self-harm act was used to get relief from emotional pain. And while intention to die was low among individuals with frequent self-harm episodes with BPD, self-harm acts often resulted in hospitalization and moderately lethal injuries.
Actually, it’s a big word to say, “I want to die.” With me, it’s not really that I want to die. I just want problems and pain to stop…… It’s like, you know, trying to tell myself not to do it, knowing a part of me wanted to do it. And then just at that moment was like an explosion for me after everything that happened with my friends, and then my mom’s birthday and calling into work, and then my boyfriend left me… (Female, BPD).
Many others described self-harm as a means of self-punishment, in which anger toward another person was oriented to themselves as form of self-punishment.
I didn’t want to die, I felt I just needed to punish myself for what the council had done to me, I had no other way out, I couldn’t harm anyone else so I had to harm myself…. I brought satisfaction on myself for somebody else for what they had done (Female, BPD).
Self-harm urges often were precipitated by multiple psychosocial stressors. There was a sudden outbreak of multiple stressful life events prior to the self-harm act. As these demands were perceived excessive, participants felt helpless, and the self-harm act occurred as a way of coping.
In contrast, self-harm occurred in some cases, without report of any acute stressors.
I used to cut and burn just here and there every couple of months. I used to just get this urge and used to just kind of a comfort and I don’t even know why I used to do it. One day I was just sitting at home, having a great time with everyone and I just went into the bathroom and I was calm and relaxed, and I cut just for the sake of doing it like and cover them up and went out and sat down 5 min later got up and went out and did the same thing and just came out laughing a joker like nothing happened…… (Female, BPD).
Medication often helped to improve mood and reduce self-harm urge. However, when the self-harm urge became stronger, some patients stopped taking their medication and engaged in self-harm.
In March I stopped the medication because I knew that I didn’t want to have control anymore, I wanted to be destructive to myself, I wanted to harm myself, I wanted to do it, I felt I felt I wanted to (Female, BPD).
Many participants with BPD had a diagnosis of depressive episode or a recurrent depressive disorder. And also, they had a chronic physical health condition or physical pain. In addition, multiple substance misuse was also very common, and most participants had alcohol consumption prior to their self-harm episode.
I am an alcoholic, I use cannabis, cocaine, and prescribed medication as well. I started the drug use from the age of 15…. I was under the influence of both alcohol and cannabis at the time of self-harm…. I don’t remember how much I had (referring quantity of alcohol) (female, BPD and MDD).
I had been off cannabis for most of last year. When I was in Canada, and I kind of wanted to keep things chiller in Christmas and family time, so I started taking Cannabis again, in December. I did drink and smoke cannabis on the day (referring the day of the index self-harm) (Female, BPD).
Participants described the impact that alcohol use and misuse had on their self-harming behavior. In a few cases, participants used alcohol to get rid of traumatic flashbacks and to maintain sleep. Many described an increased likelihood of self-harming and more severe self-harm acts following alcohol use.
I lost my nephew, who hang himself on a tree. All images and memories of this like. I get nightmares and I couldn’t sleep. I’m just constantly waking up see my nephew hanging on a tree. I started go on drinking (alcohol) to get rid of this, which escalated the problem even more like. I felt so down myself, I didn’t know what to do…I just gave up my life basically. I did the same (hanging), but the rope snapped (Male, MDD).
Physical illness, especially chronic physical pain and a reduction in physical capabilities were described as issues impacting participants prior to the self-harm episodes. For some, the pain and reduction in physical capabilities were associated with a depressive episode. Some participants described unexplained somatic symptoms and these symptoms often coexisted with a diagnosis of MDD.
I feel like every day there’s something (pain), you know, whether it’s my stomach or my head. I have low energy and kind of just random pains…. If I took painkillers I just had that bit of energy, and that bit of energy to get stuff done, get up, and get into library, study, and be able to go to the gym things like that (Female, MDD).
For many participants, reduced physical capabilities and physical pain were described in relation to multiple physical health conditions.
My thyroid had completely given up… I was just getting more ill and had no energy, my body was just shutting down (Female, BPD).
I had a prolapsed disc which was operated on… I have back pain, it’s a kind of chronic condition so that’s going on more than 12 months… I go through phases when it gets really bad, I go on painkillers (Male, BPAD).
While experience of physical illness or physical pain was not described as having a direct link to self-harm episodes, these conditions often co-existed with a psychiatric illness such as depressive disorder or bipolar affective disorder or borderline personality disorder, and these together heightened the risk of self-harm. For instance, experience of unbearable physical pain and a pessimistic view that there is no solution to this problem (due to depression) often triggered to self-harm episodes.
In many cases, participants described the existence of multiple mental illnesses or behavioral disorders in their families. Specifically, a family history of substance use disorders, depression, or self-harm/suicide were most described.
My mom, dad, and my other brother are alcoholic. My mom had depression, my dad had depression and anger management issues. My other brother and my sister had attention deficit hyperactivity disorder (Female, MDD, and BPD).
Every one of my family see psychiatrists. They all take antidepressants or some type of sleeping tablet or something to keep them going (Female, BPD).
My uncle hang himself suffered mental illness, and my mom’s mother, she killed herself. My dad is an alcoholic (Female, BPD).
Family psychiatric history contributed to self-harm mainly in two ways. First, individuals with frequent self-harm episodes were vulnerable to self-harm due to the significant family history. Second, prescribed drugs were available in the home for the treatment, which increased the risk for intentional overdoses.
Since most individuals with frequent self-harm episodes had been suffering with significant mental health difficulties, they were required to continue treatment with healthcare services. For mental health issues, participants preferred contacting the specialized mental health services rather than their General Practitioner (GP). However, most participants reported substantial difficulties in accessing of help when they were in need. Most participants contacted mental health services when they experienced low mood or self-harm urges. When they experience delays in accessing support, it has led to worsening of mood symptoms and or increasing self-harm urges, which subsequently resulted in self-harm episodes.
Appointment is in 3 months. If you need an appointment sooner, it’s very hard. But it’s hard enough to get an appointment (Female, MDD).
I am waiting for an appointment with a psychologist for a long period… I am still waiting. They have told me this is (waiting period) is usual because only one psychologist is available (Male, BPD).
Nevertheless, some participants were able to get help from a private therapist or private psychiatrist.
There is such a long waiting list (hospitals), I’m happy that I found someone (psychotherapist) but if there is someone not so confident to look for help themselves, then they might not even be here anymore at this stage (Female, BPD).
The study’s findings are in line with the emerging academic and clinical discourse that individuals with frequent self-harm episodes are a self-harm subgroup with a distinct sociodemographic and clinical profile. The findings are consistent with two other studies in this area, indicating that individuals with frequent self-harm episodes are predominantly female, have a psychiatric diagnosis, (31, 35) are unemployed (31), have a diagnosis of BPD and/or substance abuse, and have a high personal and familial risk history (31, 35). We provide further information on this subgroup: the predominant self-harm method was IDO, they reported a history of recent physical illness and physical pain, a history of many traumatic life events including violent sexual assault, severe bullying, and torture, with an extensive family history of mental illness, self-harm and substance abuse, and they expressed mild to moderate suicide intent. Physical (5) and psychiatric co-existing disorders are known to be associated with self-harm (5, 23). However, the proportion of individuals with frequent self-harm episodes suffering from BPD, MDD, substance abuse, physical illness, physical pain, sexual assault was substantially high in our study. For instance, we have found high prevalence of chronic pain (72.2%) and/or major depressive disorders (37.8%) among individuals with frequent self-harm episodes as compared to the prevalence of 35.5% (chronic pain) (45) or depressive disorders (22.8%) (46) reported in primary care population (45) or in general community population (46). Moreover, many of these conditions coexisted each other and constituted to an extensive comorbidity profile (Figure 3).
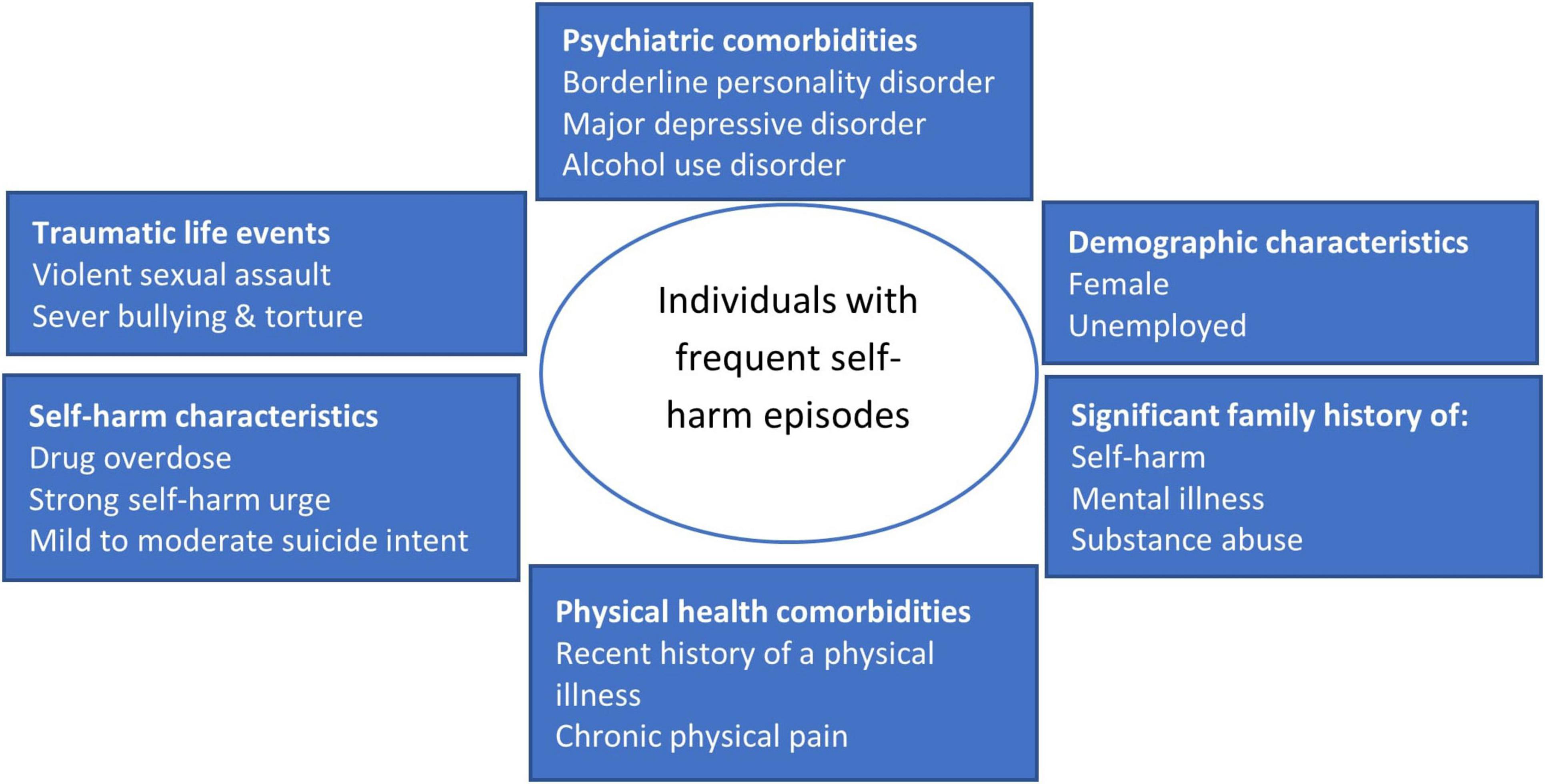
Figure 3. Key profile of individuals with frequent self-harm episodes.
The IDO as a predominant self-harm method among individuals with frequent self-harm episodes could be explained in the context of psychiatric illness and treatment. For instance, most of the individuals with frequent self-harm episodes or their family members were on treatment for a psychiatric illness, or physical pain, thus increasing the risk by stock piling prescribed medication. It is likely that accessibility and availability of the drugs, combined with strong self-harm urges increase the risk of IDOs. This is in line with previous research indicating that the prescription of psychotropic drugs is associated with the use of these drugs in IDOs, particularly minor tranquillizers (47).
Although most individuals with frequent self-harm episodes had engaged in IDO, we examined the characteristics of the subgroup representing those with HLSMs. Male gender and alcohol use disorders consistently predicted HLSMs, while other sociodemographic or physical and mental disorders variables were not significant. The association between gender and self-harm methods has been documented previously, with male gender increasing the risk of having a violent (39, 48, 49) or severe self-harm episodes (50, 51). Violent methods were further associated with risk of suicide (52). Studies also reported an association between substance abuse and violent (53) or lethal self-harm (54). Inconsistent with other studies, (55, 56), a coexisting psychosis was not associated with HLSMs in the current study. However, notably, the prevalence of psychosis was relatively lower in the study samples. A diagnosis of MDD was not associated with HLSMs, while this was associated with suicide intent. The association between MDD and suicide intent is well established (57–59). Although a higher proportion of individuals with frequent self-harm episodes had physical illness, this was not associated with HLSMs. The association between a physical illness and HLSMs is under researched. Nevertheless, some available research has demonstrated the association of physical illness with self-harm repetition (5), although this was also inconsistent (60). Physical pain was reported by most of the study participants, but this was not associated with suicide intent. A few other studies had reported the association between pain intensity and suicide ideation (61) and pain-related condition and suicide (62). However, the association between physical illness or physical pain and self-harm is under-researched (23), and requires more research to provide reliable conclusions.
The qualitative findings reveal critical themes including functional meaning of self-harm, self-harm comorbidity, family psychiatric history, and contacts with mental health services. Most of the participants who engaged in repeated self-harm had low intention to die and the self-harm often resulted from an uncontrollable self-harm urge, as reported in previous research (63). Previous researchers have even developed instruments to measure the cognitive and emotional aspects of this craving (64) and repeated self-harm behaviors have been conceptualized as an addiction (32, 34). Only one study examined self-harm craving among individuals with frequent self-harm episodes, and reported characteristics similar to addictive behaviors including tolerance, loss of control, and continuation of self-harm behaviors despite significant negative consequences (34). The findings of the current study support the notion that individuals with frequent self-harm episodes engage in addictive behaviors relating to self-harm, mostly coexisting with BPD. An uncontrollable self-harm urge or some addictive behaviors are mostly suited to explain the repeated self-harm behavior in BPD but is insufficient to explain the repeated episodes of other individuals with frequent self-harm episodes who presented without this diagnosis. It is unlikely that a single conceptualization like self-harm urges, or addiction would be adequate to explain these complex behaviors. Thus, it is postulated that this subgroup has an extensive profile of self-harm comorbidity evidenced by the qualitative and quantitative findings. Among individuals with frequent self-harm episodes with a physical illness, almost all had a diagnosis of a mental/behavioral disorder, a finding supported by previous research demonstrating that a number of chronic diseases are associated with suicidal thoughts and suicide attempts (15, 65). Congruent to the current findings, high personal and family risk history including sexual abuse was also reported among individuals with frequent self-harm episodes (35, 66). We also identified mental health system related barriers for accessing help, which indeed has potential impact on self-harm and wellbeing. Many system related issues including lack of mental health professionals and delays in availing of appointments with public mental health services had been identified previously, with a recommendation for effective system planning (67).
This study has many strengths, including the focus on individuals with frequent self-harm episodes who have the highest risk of prospective repeated self-harm. Hence, examining their unique profile and associated comorbidities is important for effective assessment and management of self-harm. Among this subgroup, this is the first mixed-method study involving a large sample size. Participants in the semi-structured interview group can be considered a strong representation of individuals with frequent self-harm episodes while there were no significant differences between the two groups on key sociodemographic characteristics. The file review and interview data complemented each other to address the study objectives. For example, physical pain, suicide intent, traumatic life events and family history of mental disorders were not documented well in the file review, while the semi structured interview data had provided more comprehensive information. Similarly, the file review data addressed the potential predictors of HLSMs, while the qualitative data reflected participants’ own experiences of having physical and mental health comorbidities related to self-harm. A further strength of this study is that the potential predictors identified were consistent over multiple self-harm episodes within one individual. Therefore, these variables may be considered to be more strongly associated with HLSMs. Highly lethal methods of a recent self-harm episode are known to be related to a high risk of subsequent suicide (68), which underlines the significance of these findings for suicide prevention.
Nevertheless, the study findings must be interpreted with the following considerations. First, we concurrently used file review data and semi-structured interview data to examine the study objectives. Although this approach has potential to complement each other, the file review data is retrospective in nature, hence, the limitations applicable to retrospective findings are applicable to the current findings. Second, many variables in the file review had unrecorded values, which were not included for the analysis, while this would have impacted on our prevalence estimates. This under recording points out the need for improving biopsychosocial assessment and documentation for this self-harm subgroup. Third, the diagnosis of a physical or mental disorder was based on the casefiles of the patients, made by a registered physician or psychiatrist. While the diagnosis was relied on the individual clinician’s judgment, we did not use any standard instruments to verify the diagnosis with the subgroup participated in the interview study. Fourth, certain groups of patients could not be considered for the study (e.g., patients with acute psychotic or mood symptoms or those who were unconscious or in induced coma because of the severity of the self-harm act). While their condition implied inability to take part in the interview study and or provide informed consent, valuable lived experience was missed from this group. Fifth, the operationalization of highly lethal or violent self-harm methods varied, and this could include (39) or exclude (69) self-cutting. We considered self-cutting as HLSM as there are large scale longitudinal studies which demonstrate that self-cutting increases the risk of suicide, compared to those with self-poisoning (26, 70). Although a HLSM can increase the risk for suicide, the method alone can’t be completely attributed to suicide or even lethality or severity. A serious suicide attempt is a combination of medical lethality, potential lethality of the method used, and severity of the objective circumstances of the suicide intent (71).
Biopsychosocial assessment should be carried out to all individuals with frequent self-harm episodes as a part of routine clinical services in EDs. Due to incompleteness of biopsychosocial assessments in 30% of participants, it is recommended to improve training and supervision to ensure completeness of core elements of the biopsychosocial assessment, which is line with recommendations of the National Clinical Programme for Self-harm and Suicide related Ideation in Ireland (72), Royal College of Psychiatrists (73) and NICE guideline (74). Screening of possible comorbidities should be introduced on the clinical practices, specifically, screening for substance use disorder, borderline personality disorder and major depressive disorders. Physical illnesses especially chronic physical pain also should be assessed and managed. While the association between physical and mental health comorbidities and self-harm repetition is evident, future studies should examine the specific association between these comorbidities and completed suicide.
In addition, future studies should also identify the effective components of psychotherapeutic interventions (e.g., biopsychosocial risk assessment/safety planning/cognitive behavior therapy) for individuals with frequent self-harm episodes and or training and capacity building programmes for key healthcare professionals for addressing the increased self-harm and suicide risk among this self-harm subgroup.
This is one of few studies examining mental and physical health comorbidities among a high-risk self-harm group. The findings demonstrate that almost all individuals with frequent self-harm episodes had a diagnosis of mental disorders, and two thirds had a diagnosis of physical pain, indicating a high level of physical and mental disorders comorbidity. This study underlines the need to consider individuals with frequent self-harm episodes as a self-harm subgroup with a unique clinical and comorbidity profile, with the requirement for these patients to receive a biopsychosocial assessment after each episode of self-harm.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Clinical Research Ethics Committee of the Cork University Teaching Hospitals [reference number EMC 4(2) 12/04/16] and the HSE Mid-Western Regional Hospital Research Ethics Committee (reference number REC 018/6). The patients/participants provided their written informed consent to participate in this study.
AS, MT, SN, GC, DL, AR, PC, and EA: conceptualization. AS, MT, SN, GC, DL, AR, EA, and ÍA-P: methodology. AS, MT, SN, GC, DL, AR, and EA: investigation. AS and EA: writing—original draft. MT, SN, GC, DL, AR, RB, PC, EG, EP, EC, AJ, FS, ÍA-P, KK, and EA: writing—review and editing. EA: funding acquisition and supervision. EA, EC, and AJ: resources. All authors contributed to the article and approved the submitted version.
This work was supported by the Irish Health Research Board (Grant Number: IRRL-2015-1586). The funding source had no involvement in the study design, collection, analysis and interpretation of data, writing of the report, or decision to submit the article for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Castelpietra G, Knudsen A, Agardh E, Armocida B, Beghi M, Iburg K, et al. The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990-2019: findings from the Global Burden of Disease Study 2019. Lancet Reg Health Eur. (2022) 16:100341. doi: 10.1016/j.lanepe.2022.100341
2. Klonsky E, May A, Saffer B. Suicide, suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. (2016) 12:307–30. doi: 10.1146/annurev-clinpsy-021815-093204
3. Ghimire S, Devkota S, Budhathoki R, Sapkota N, Thakur A. Psychiatric comorbidities in patients with deliberate self-harm in a tertiary care center. J Nepal Med Assoc. (2014) 52:697–701.
4. Nitkowski D, Petermann F. [Non-suicidal self-injury and comorbid mental disorders: a review]. Fortschr Neurol Psychiatr. (2011) 79:9–20. doi: 10.1055/s-0029-1245772
5. Singhal A, Ross J, Seminog O, Hawton K, Goldacre M. Risk of self-harm and suicide in people with specific psychiatric and physical disorders: comparisons between disorders using English national record linkage. J R Soc Med. (2014) 107:194–204. doi: 10.1177/0141076814522033
6. Turner B, Dixon-Gordon K, Austin S, Rodriguez M, Zachary Rosenthal M, Chapman A. Non-suicidal self-injury with and without borderline personality disorder: differences in self-injury and diagnostic comorbidity. Psychiatry Res. (2015) 230:28–35. doi: 10.1016/j.psychres.2015.07.058
7. Cipriano A, Cella S, Cotrufo P. Nonsuicidal self-injury: a systematic review. Front Psychol. (2017) 8:1946. doi: 10.3389/fpsyg.2017.01946
8. Balázs J, Győri D, Horváth L, Mészáros G, Szentiványi D. Attention-deficit hyperactivity disorder and nonsuicidal self-injury in a clinical sample of adolescents: the role of comorbidities and gender. BMC Psychiatry. (2018) 18:34. doi: 10.1186/s12888-018-1620-3
9. Wolff J, Thompson E, Thomas S, Nesi J, Bettis A, Ransford B, et al. Emotion dysregulation and non-suicidal self-injury: a systematic review and meta-analysis. Eur Psychiatry. (2019) 59:25–36. doi: 10.1016/j.eurpsy.2019.03.004
10. Klonsky E. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. (2007) 27:226–39. doi: 10.1016/j.cpr.2006.08.002
11. Oh S, Lee K, Kim S, Park K, Kim Y, Kim H. Factors associated with choice of high lethality methods in suicide attempters: a cross-sectional study. Int J Ment Health Syst. (2014) 8:43. doi: 10.1186/1752-4458-8-43
12. Xiao Y, Zhao N, Yu M, Zhao M, Zhong J, Gong W, et al. Factors associated with severe deliberate self-harm among Chinese internal migrants. PLoS One. (2013) 8:e80667. doi: 10.1371/journal.pone.0080667
13. Tyrer P, Reed G, Crawford M. Classification, assessment, prevalence, and effect of personality disorder. Lancet. (2015) 385:717–26. doi: 10.1016/S0140-673661995-4
14. Ramleth R, Groholt B, Diep L, Walby F, Mehlum L. The impact of borderline personality disorder and sub-threshold borderline personality disorder on the course of self-reported and clinician-rated depression in self-harming adolescents. Borderline Personal Disord Emot Dysregul. (2017) 4:22. doi: 10.1186/s40479-017-0073-5
15. Kavalidouᵃ K, Smith D, Der G, O’Connor R. The role of physical and mental multimorbidity in suicidal thoughts and behaviours in a Scottish population cohort study. BMC Psychiatry. (2019) 19:38. doi: 10.1186/s12888-019-2032-8
16. Jia C, Wang L, Xu A, Dai A, Qin P. Physical illness and suicide risk in rural residents of contemporary China: a psychological autopsy case-control study. Crisis. (2014) 35:330–7. doi: 10.1027/0227-5910/a000271
17. Webb R, Kontopantelis E, Doran T, Qin P, Creed F, Kapur N. Risk of self-harm in physically ill patients in UK primary care. J Psychosom Res. (2012) 73:92–7. doi: 10.1016/j.jpsychores.2012.05.010
18. Qin P, Hawton K, Mortensen P, Webb R. Combined effects of physical illness and comorbid psychiatric disorder on risk of suicide in a national population study. Br J Psychiatry. (2014) 204:430–5. doi: 10.1192/bjp.bp.113.128785
19. Pompili M, Venturini P, Campi S, Seretti M, Montebovi F, Lamis D, et al. Do stroke patients have an increased risk of developing suicidal ideation or dying by suicide? An overview of the current literature. CNS Neurosci Ther. (2012) 18:711–21. doi: 10.1111/j.1755-5949.2012.00364.x
20. Fässberg M, Cheung G, Canetto S, Erlangsen A, Lapierre S, Lindner R, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults. Aging Ment Health. (2016) 20:166–94. doi: 10.1080/13607863.2015.1083945
21. Cully G, Leahy D, Shiely F, Arensman E. Patients’ experiences of engagement with healthcare services following a high-risk self-harm presentation to a hospital emergency department: a mixed methods study. Arch Suicide Res. (2022) 26:91–111. doi: 10.1080/13811118.2020.1779153
22. Duarte T, Paulino S, Almeida C, Gomes H, Santos N, Gouveia-Pereira M. Self-harm as a predisposition for suicide attempts: a study of adolescents’ deliberate self-harm, suicidal ideation, and suicide attempts. Psychiatry Res. (2020) 287:112553. doi: 10.1016/j.psychres.2019.112553
23. Larkin C, Di Blasi Z, Arensman E. Risk factors for repetition of self-harm: a systematic review of prospective hospital-based studies. PLoS One. (2014) 9:e84282. doi: 10.1371/journal.pone.0084282
24. Olfson M, Wall M, Wang S, Crystal S, Gerhard T, Blanco C. Suicide following deliberate self-harm. Am J Psychiatry. (2017) 174:765–74. doi: 10.1176/appi.ajp.2017.16111288
25. Griffin E, Kavalidou K, Bonner B, O’Hagan D, Corcoran P. Risk of repetition and subsequent self-harm following presentation to hospital with suicidal ideation: a longitudinal registry study. EClinicalMedicine. (2020) 23:100378. doi: 10.1016/j.eclinm.2020.100378
26. Bennardi M, McMahon E, Corcoran P, Griffin E, Arensman E. Risk of repeated self-harm and associated factors in children, adolescents and young adults. BMC Psychiatry. (2016) 16:421. doi: 10.1186/s12888-016-1120-2
27. Hawton K, Zahl D, Weatherall R. Suicide following deliberate self-harm: long-term follow-up of patients who presented to a general hospital. Br J Psychiatry. (2003) 182:537–42. doi: 10.1192/bjp.182.6.537
28. Zahl D, Hawton K. Repetition of deliberate self-harm and subsequent suicide risk: long-term follow-up study of 11,583 patients. Br J Psychiatry. (2004) 185:70–5. doi: 10.1192/bjp.185.1.70
29. Perry I, Corcoran P, Fitzgerald A, Keeley H, Reulbach U, Arensman E. The incidence and repetition of hospital-treated deliberate self harm: findings from the world’s first national registry. PLoS One. (2012) 7:e31663. doi: 10.1371/journal.pone.0031663
30. Kreitman N, Casey P. Repetition of parasuicide: an epidemiological and clinical study. Br J Psychiatry. (1988) 153:792–800.
31. Irigoyen-Otiñano M, Puigdevall-Ruestes M, Prades-Salvador N, Salort-Seguí S, Gayubo L, de Leon J, et al. Further evidence for major repeaters as a subgroup of suicide attempters. Rev Psiquiatr Salud Ment. (2018) 11:60–1. doi: 10.1016/j.rpsm.2017.04.004
32. Blasco-Fontecilla H. The addictive hypothesis of suicidal behavior. Med Hypotheses. (2012) 78:350. doi: 10.1016/j.mehy.2011.11.005
33. Sinclair J, Gray A, Rivero-Arias O, Saunders K, Hawton K. Healthcare and social services resource use and costs of self-harm patients. Soc Psychiatry Psychiatr Epidemiol. (2011) 46:263–71. doi: 10.1007/s00127-010-0183-5
34. Blasco-Fontecilla H, Artieda-Urrutia P, Berenguer-Elias N, Garcia-Vega J, Fernandez-Rodriguez M, Rodriguez-Lomas C, et al. Are major repeater patients addicted to suicidal behavior? Adicciones. (2014) 26:321–33.
35. Blasco-Fontecilla H, Jaussent I, Olié E, Béziat S, Guillaume S, Artieda-Urrutia P, et al. A cross-sectional study of major repeaters: a distinct phenotype of suicidal behavior. Prim Care Companion CNS Disord. (2014) 16:10.4088/PCC.14m01633. doi: 10.4088/PCC.14m01633
36. Creswell J. Qualitative Inquiry and Research Design: Choosing Among Five Traditions. New York, NY: Sage Publications (1998).
37. Schmidtke A, Bille-Brahe U, DeLeo D, Kerkhof A, Bjerke T, Crepet P, et al. Attempted suicide in Europe: rates, trends and sociodemographic characteristics of suicide attempters during the period 1989-1992. Results of the WHO/EURO Multicentre Study on Parasuicide. Acta Psychiatr Scand. (1996) 93:327–38. doi: 10.1111/j.1600-0447.1996.tb10656.x
38. Feinstein A. The pre-therapeutic classification of co-morbidity in chronic disease. J Chronic Dis. (1970) 23:455–68. doi: 10.1016/0021-968190054-8
39. Persett P, Grimholt T, Ekeberg O, Jacobsen D, Myhren H. Patients admitted to hospital after suicide attempt with violent methods compared to patients with deliberate self-poisoning -a study of background variables, somatic and psychiatric health and suicidal behavior. BMC Psychiatry. (2018) 18:21. doi: 10.1186/s12888-018-1602-5
40. Beck A, Schuyler D, Herman I. Development of suicidal intent scales. In: Beck AT, Resnik HL, Lettieri DJ, editors. The Prediction of Suicide. Philadelphia, PA: Charles Press Publishers (1974).
41. electronic Irish Statute Book [eISB]. Data Protection Act, 1988. (2020). Available online at: http://www.irishstatutebook.ie/eli/1988/act/25/enacted/en/html (accessed December 7, 2020).
42. Citizens information. Overview of the General Data Protection Regulation (GDPR). (2020). Available online at: https://www.citizensinformation.ie/en/government_in_ireland/data_protection/overview_of_general_data_protection_regulation.html# (accessed December 7, 2020).
43. Bursac Z, Gauss C, Williams D, Hosmer D. Purposeful selection of variables in logistic regression. Source Code Biol Med. (2008) 3:17. doi: 10.1186/1751-0473-3-17
44. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
45. Raftery M, Sarma K, Murphy A, De la Harpe D, Normand C, McGuire B. Chronic pain in the Republic of Ireland–community prevalence, psychosocial profile and predictors of pain-related disability: results from the Prevalence, Impact and Cost of Chronic Pain (PRIME) study, part 1. Pain. (2011) 152:1096–103. doi: 10.1016/j.pain.2011.01.019
46. Hyland P, Shevlin M, McBride O, Murphy J, Karatzias T, Bentall R, et al. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr Scand. (2020) 142:249–56. doi: 10.1111/acps.13219
47. Wysowski D. Surveillance of prescription drug-related mortality using death certificate data. Drug Saf. (2007) 30:533–40. doi: 10.2165/00002018-200730060-00007
48. Giner L, Jaussent I, Olié E, Béziat S, Guillaume S, Baca-Garcia E, et al. Violent and serious suicide attempters: one step closer to suicide? J Clin Psychiatry. (2014) 75:e191–7. doi: 10.4088/JCP.13m08524
49. Nordentoft M, Branner J. Gender differences in suicidal intent and choice of method among suicide attempters. Crisis. (2008) 29:209–12. doi: 10.1027/0227-5910.29.4.209
50. Chao Q, Yang X, Luo C. Boy crisis? Sex differences in self-injurious behaviors and the effects of gender role conflicts among college students in China. Am J Mens Health. (2016) 10:N1–10. doi: 10.1177/1557988315579096
51. Tsirigotis K, Gruszczynski W, Tsirigotis M. Gender differentiation in methods of suicide attempts. Med Sci Monit. (2011) 17:H65–70. doi: 10.12659/msm.881887
52. Beckman K, Mittendorfer-Rutz E, Waern M, Larsson H, Runeson B, Dahlin M. Method of self-harm in adolescents and young adults and risk of subsequent suicide. J Child Psychol Psychiatry. (2018) 59:948–56. doi: 10.1111/jcpp.12883
53. Dumais A, Lesage A, Lalovic A, Séguin M, Tousignant M, Chawky N, et al. Is violent method of suicide a behavioral marker of lifetime aggression? Am J Psychiatry. (2005) 162:1375–8. doi: 10.1176/appi.ajp.162.7.1375
54. Li Y. Deliberate self-harm and relationship to alcohol use at an emergency department in eastern Taiwan. Kaohsiung J Med Sci. (2007) 23:247–53. doi: 10.1016/S1607-551X70405-X
55. Nielssen O, Glozier N, Babidge N, Reutens S, Andrews D, Gerard A, et al. Suicide attempts by jumping and psychotic illness. Aust N Z J Psychiatry. (2010) 44:568–73. doi: 10.3109/00048671003606086
56. Nielssen O, Large M. Untreated psychotic illness in the survivors of violent suicide attempts. Early Interv Psychiatry. (2009) 3:116–22. doi: 10.1111/j.1751-7893.2009.00117.x
57. Astruc B, Torres S, Jollant F, Jean-Baptiste S, Castelnau D, Malafosse A, et al. A history of major depressive disorder influences intent to die in violent suicide attempters. J Clin Psychiatry. (2004) 65:690–5. doi: 10.4088/jcp.v65n0515
58. Pompili M, Innamorati M, Raja M, Falcone I, Ducci G, Angeletti G, et al. Suicide risk in depression and bipolar disorder: do impulsiveness-aggressiveness and pharmacotherapy predict suicidal intent? Neuropsychiatr Dis Treat. (2008) 4:247–55. doi: 10.2147/ndt.s2192
59. Liu B, Wang X, Jia C. Suicide attempters with high and low suicide intent: different populations in rural China. Psychiatry Res. (2017) 251:176–81. doi: 10.1016/j.psychres.2017.01.096
60. Brown H, Wilton A, Ray J, Dennis C, Guttmann A, Vigod S. Chronic physical conditions and risk for perinatal mental illness: a population-based retrospective cohort study. PLoS Med. (2019) 16:e1002864. doi: 10.1371/journal.pmed.1002864
61. Smith M, Perlis M, Haythornthwaite J. Suicidal ideation in outpatients with chronic musculoskeletal pain: an exploratory study of the role of sleep onset insomnia and pain intensity. Clin J Pain. (2004) 20:111–8. doi: 10.1097/00002508-200403000-00008
62. O’Neill S, Graham B, Ennis E. Prescribed pain and mental health medication prior to suicide: a population based case control study. J Affect Disord. (2019) 246:195–200. doi: 10.1016/j.jad.2018.12.018
63. Klonsky E, Glenn C. Assessing the functions of non-suicidal self-injury: psychometric properties of the Inventory of Statements About Self-injury (ISAS). J Psychopathol Behav Assess. (2009) 31:215–9. doi: 10.1007/s10862-008-9107-z
64. Washburn J, Juzwin K, Styer D, Aldridge D. Measuring the urge to self-injure: preliminary data from a clinical sample. Psychiatry Res. (2010) 178:540–4. doi: 10.1016/j.psychres.2010.05.018
65. Wei M, Mukamal K. Multimorbidity and mental health-related quality of life and risk of completed suicide. J Am Geriatr Soc. (2019) 67:511–9. doi: 10.1111/jgs.15678
66. Troya M, Cully G, Leahy D, Cassidy E, Sadath A, Nicholson S, et al. Investigating the relationship between childhood sexual abuse, self-harm repetition and suicidal intent: mixed-methods study. BJPsych Open. (2021) 7:e125. doi: 10.1192/bjo.2021.962
67. Dunne E. The Views of Adult Users of the Public Sector Mental Health Services: Report of a Survey for the Mental Health Commission Item Type Report. (2006). Available online at: http://hdl.handle.net/10147/43828Findthisandsimilarworksat- http://www.lenus.ie/hse (accessed August 19, 2022).
68. Carter G. Method of most recent self-harm episode is related to risk of subsequent suicide. Evid Based Ment Health. (2012) 15:68. doi: 10.1136/ebmental-2012-100693
69. Olfson M, Wall M, Wang S, Crystal S, Bridge J, Liu S, et al. Suicide after deliberate self-harm in adolescents and young adults. Pediatrics. (2018) 141:e20173517. doi: 10.1542/peds.2017-3517
70. Carroll R, Thomas K, Bramley K, Williams S, Griffin L, Potokar J, et al. Self-cutting and risk of subsequent suicide. J Affect Disord. (2016) 192:8–10. doi: 10.1016/j.jad.2015.12.007
71. Levi-Belz Y, Beautrais A. Serious suicide attempts. Crisis. (2016) 37:299–309. doi: 10.1027/0227-5910/a000386
72. Health Service Executive. National Clinical Programme for the Assessment and Management of Patients Presenting to Emergency Departments Following Self-Harm. (2018). Available online at: https://www.hse.ie/eng/about/who/cspd/ncps/self-harm-suicide-related-ideation/ (accessed June 25, 2022).
73. Royal College of Psychiatrists. Assessment Following Self-Harm in Adults. Counc Rep CR 122. London: Royal College of Psychiatrists (2004).
74. National Collaborating Centre for Mental Health. Self-Harm: The Short-Term Physical and Psychological Management and Secondary Prevention of Self-Harm in Primary and Secondary Care. Leicester: British Psychological Society (2004).
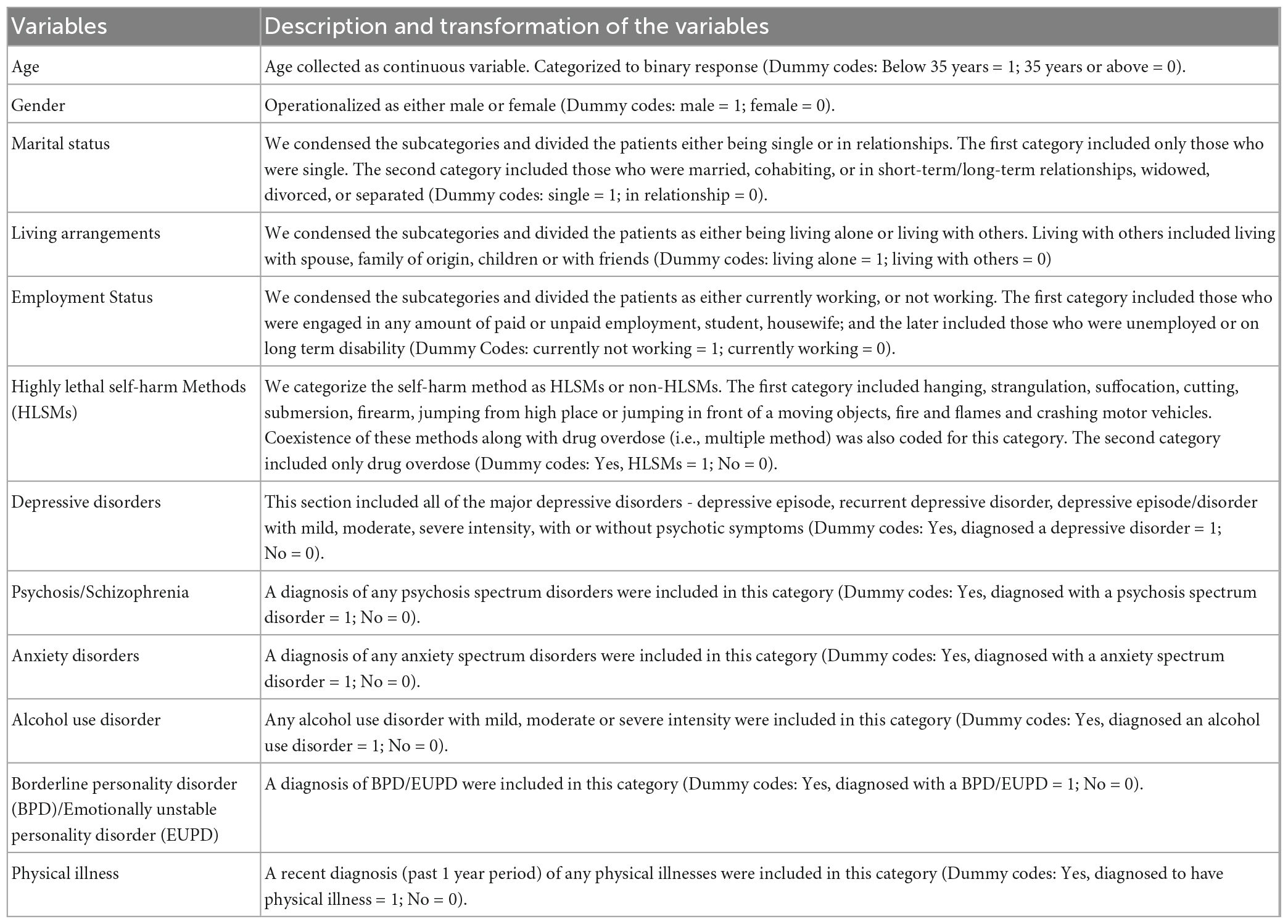
Appendix 1. Operationalization and dummy codes of the study variables.
Keywords: frequent self-harm, self-harm repetition, suicide intent, comorbidity, mental illness, physical illness, highly lethal self-harm
Citation: Sadath A, Troya MI, Nicholson S, Cully G, Leahy D, Ramos Costa AP, Benson R, Corcoran P, Griffin E, Phillip E, Cassidy E, Jeffers A, Shiely F, Alberdi-Páramo Í, Kavalidou K and Arensman E (2023) Physical and mental illness comorbidity among individuals with frequent self-harm episodes: A mixed-methods study. Front. Psychiatry 14:1121313. doi: 10.3389/fpsyt.2023.1121313
Received: 11 December 2022; Accepted: 13 February 2023;
Published: 09 March 2023.
Edited by:
Fredrik A. Walby, University of Oslo, NorwayReviewed by:
Elfrida Hartveit Kvarstein, Oslo University Hospital, NorwayCopyright © 2023 Sadath, Troya, Nicholson, Cully, Leahy, Ramos Costa, Benson, Corcoran, Griffin, Phillip, Cassidy, Jeffers, Shiely, Alberdi-Páramo, Kavalidou and Arensman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anvar Sadath, YW52YXIuc2FkYXRodmFra2F5aWxAdWNjLmll
†ORCID: Grace Cully, orcid.org/0000-0002-9236-1545
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.