 Vanessa Reimer
Vanessa Reimer Martina K. Kanning
Martina K. Kanning
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 12 May 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1111602
This article is part of the Research Topic Sport and Exercise: Challenges and Perspectives in Mental Health View all 11 articles
Physical exercise interventions improve quality of life in people with mental disorders and improve abstinence and cravings in substance use disorders patients in both the short term and long term. In people with mental illness, physical exercise interventions significantly reduce psychiatric symptoms of schizophrenia and symptoms of anxiety. For forensic psychiatry, there is little empirical evidence supporting mental health-enhancing effects of physical exercise interventions. Interventional studies in forensic psychiatry deal mainly with three problems: heterogeneity of the individuals, a small sample size, and a low compliance rate. Intensive longitudinal case studies could be a suitable approach to address these methodological challenges in forensic psychiatry. This study uses an intensive longitudinal design to determine whether forensic psychiatric patients are content to complete several data assessments per day over the course of several weeks. The feasibility of this approach is operationalized by the compliance rate. Additionally, single-case studies examine the effects of sports therapy (ST) on momentary affective states (energetic arousal, valence, and calmness). The results of these case studies reveal one aspect of feasibility and offer insights into the effects of forensic psychiatric ST on the affective states among patients with different conditions. The patients’ momentary affective states were recorded before (PRE), after (POST) and 1 h after (FoUp1h) ST by questionnaires. Ten individuals (Mage = 31.7, SD = 11.94; 60% male) participated in the study. A total of 130 questionnaires were completed. To perform the single-case studies, data of three patients were considered. Repeated-measures ANOVA was performed for the individual affective states to test for main effects of ST. Due to the results, ST has no significant effect on none of the three affect dimensions. However, effect sizes varied between small to medium (energetic arousal: η2 = 0.01, η2 = 0.07, η2 = 0.06; valence: η2 = 0.07; calmness: η2 = 0.02) in the three patients. Intensive longitudinal case studies are a possible approach to address heterogeneity and the low sample size. The low compliance rate in this study reveals that the study design needs to be optimized for future studies.
There is a considerable amount of evidence showing that physical exercise interventions improve quality of life in people with mental disorders and improve abstinence and cravings in substance use disorder patients in both the short term and long term (1). In people with mental illness, physical exercise interventions significantly reduce psychiatric symptoms of schizophrenia (2) and symptoms of anxiety (3). A systematic review and meta-analysis investigating physical activity interventions in people with mental illness showed small to large short-term effects of physical activity on symptoms of mental illness (4). However, for forensic psychiatry, there is little empirical evidence supporting the effects of physical exercise interventions. Conducting research studies to investigate the effects of sports therapy (ST) on forensic psychiatric patients is challenging due to various reasons (5). Typical barriers include a low sample size in ST sessions, as patients from different wards have to train in separate groups and cannot be put into one group (5). Additional challenges include low compliance rates and high heterogeneity within psychiatric diagnoses (5). Furthermore, there are sociopsychological deficits associated with the crime that are specific to forensic psychiatry (6). Forensic patients suffer from poor physical conditions and a high variability and fluctuation in momentary affective states, which could be an explanation for the low sample size and the low compliance rate (5). In forensic patients, there are only a few patients who (can) participate in a study due to symptomatology and heterogeneity, baseline restrictions, nonparticipation, etc. (5), thereby causing variations and fluctuations in behavior and well-being (5). On average, a ST group in forensic psychiatry consists of a small number of participants (5–10) that fluctuates in each unit (5). Regarding intervention studies, the average compliance rate in forensic psychiatric studies is 53% (7), which is lower than the rate (63%) in people with serious psychiatric disabilities (8). The high heterogeneity in psychiatric diagnoses is due to a combination of several factors causing a mental illness such as individual characteristics and experiences, social influences, when certain events took place, or how the person developed (9). Challenges such as motivation (10) and impulsivity (10, 11) are additional factors that contribute to a low compliance rate and generally a low number of participants (7). These hurdles initially make it difficult to conduct studies that can then provide information on forensic patients’ responses to specific ST interventions that are aimed at improving well-being, quality of life and psychological functioning.
To address these challenges in forensic psychiatric research, using single-case studies could be used as a methodological solution. Single-case studies offer a useful method for evaluating data from patients who experience the heterogeneity of psychiatric disorders (12, 13), as individual variability as well as valuable information about the individual treatment progress can be lost in a between-group design (14). Intensive longitudinal case studies offer the ability to examine participants over a longer period of time (e.g., several weeks) and several times a day in their natural context (15). Therefore, a low sample size is accounted for in such designs. These types of studies require a higher amount of effort for researchers and participants, and it is unclear whether or to what extent this is tolerated by forensic patients due to motivational problems and impulsivity (5–7) and if the low compliance rate can be addressed. Data collection at multiple measurement timepoints is used to generate a sufficient amount of data per patient. The terms “single case study” and “N-of-1” study are used synonymously (12, 16, 17). Throughout this article, the term single-case study is used. A clear distinction should be drawn to a case report (17). A case report is purely descriptive, whereas a single-case study demonstrates rigorous methods for the study design and data analysis using visual and statistical methods whenever possible (17). A single-case study design is a common study design in health care (17–19), e.g., in psychiatric disorders, such as schizophrenia (13, 20, 21). This design addresses intraindividual differences (16, 17, 22) and contributes to individualized medicine (12, 23). The authors of a study in forensic psychiatry show, within a randomized controlled trial, that the addition of a single-case experimental design enables a more intense investigation of specific patients (24). They report the advantage of the single-case study designs in the form of closer monitoring of each patient and receiving valuable information about each patient (25) that is more in-depth (24). These findings suggest that single-case studies in forensic psychiatry could be used to address heterogeneity.
In the field of forensic psychiatry, case study designs have been implemented in the form of neurofeedback training (25) or music therapy (20), but none have specifically examined the effect of ST. This study used an intensive longitudinal design to determine whether forensic psychiatric patients are content to complete several data assessments per day over the course of several weeks. The feasibility of this approach was operationalized by the compliance rate. Additionally, single-case studies were performed to examine the effects of ST on momentary affective states (energetic arousal, valence, calmness). To the best of our knowledge, this is the first study in forensic psychiatry to evaluate the feasibility of an intensive longitudinal case study design. Furthermore, the results of these case studies reflect one aspect of feasibility and offer insights into the effects of forensic psychiatric ST on the affective states among patients with different conditions.
Data were collected in 2021 at the Center for Psychiatry Reichenau. Approximately 100 patients are accommodated there and distributed across four forensic wards. People are referred to this center if their offense was specifically related to the use of intoxicating substances or mental illness (6). The total length of detention varies across individuals but ranges from a minimum of 2 years to multiple years (6). Participation in the study was voluntary and patients committed to submitting regular study data on days with ST (twice a week). The ST intervention represented the regularly occurring therapy and was firmly integrated at the Center for Psychiatry Reichenau. The repeated recording of the momentary affective states did not represent a psychological intervention. Prior to study inclusion, each subject signed an informed consent form. In total, 10 individuals participated in the study. The patients’ symptomatology included either paranoid schizophrenia, schizoaffective disorder (manic or mixed type), bipolar affective disorder (current episode manic without psychotic features), or mixed and other personality disorders or hyperkinetic conduct (Table 1). Participants received an organized bike tour as an incentive for participating in the study.
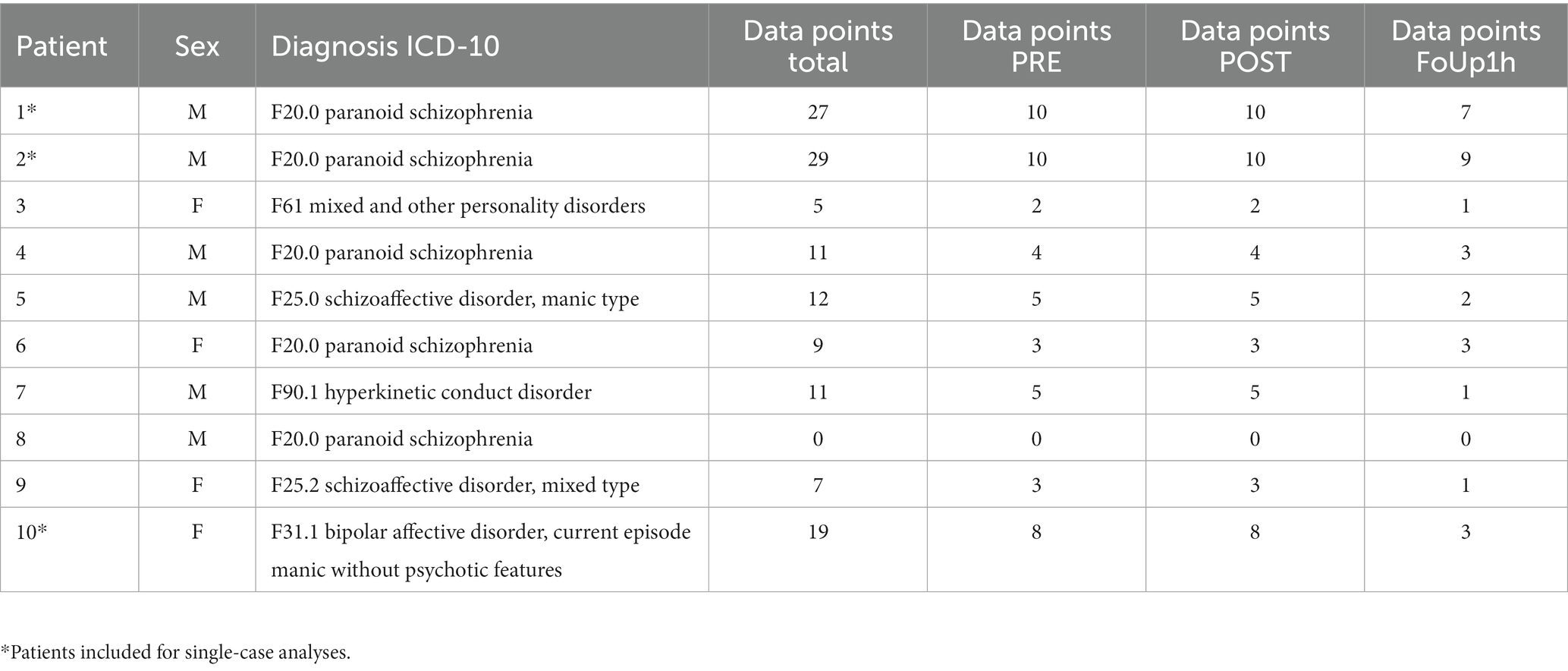
Table 1. Patient characteristics.
Questionnaires to assess demographic details were completed before the first session of ST. Over a period of four weeks, affective state questionnaires were completed before ST (PRE), after ST (POST) and 1 h after ST (FoUp1h). For the FoUp1h assessment timepoint, the sport therapist searched and contacted every patient in the facility.
Demographics. Age and gender were self-reported and assessed with a paper and pencil questionnaire.
Momentary affective states. Self-report was used to assess patients’ momentary affective states. For this purpose, the short scale by Wilhelm and Schoebi (26) was used (see Appendix 1). This short scale is appropriate to minimize the effort for the patients. This instrument is validated and suitable for ambulatory assessment studies. The within-person reliability (energetic arousal: 0.77, valence: 0.70, calmness: 0.77) as well as the between-person reliability (energetic arousal: 0.90, valence: 0.92, calmness: 0.90) was acceptable (26). Three bipolar affect dimensions (energetic arousal, valence, calmness) were measured by six items that assess the intensity of each affect dimension: energetic arousal (tired vs. awake, without energy vs. full of energy), valence (unwell vs. well, discontent vs. content), and calmness (relaxed vs. tense, calm vs. agitated). Responses were given on a 6-point Likert response scale.
All 60-min ST sessions followed exactly the same structure and the units were comparable in procedure, duration, and intensity. Patients in this study participated in two different ST groups. The main intended effects of ST are to increase physical fitness, promote social skills in group sports, and contribute to a solid daily structure (6). First, there was a warm-up phase that focused on circulation activation and technique practice. In the main phase, patients performed different group sport activities together (e.g., volleyball, soccer, tennis, or table tennis). The intensity of the activity was structured in such a way that it was perceived as hard by the individuals (27). Furthermore, ST included technical elements (throwing and passing techniques, running routes, team formations, etc.). The ST session ended with a collective cool-down, which was followed by a reflection phase in which the group discussed what went well during the session and what could be improved. Data collection took place in June and July 2021 at the Center for Psychiatry Reichenau.
Intensive longitudinal single-case analyses were conducted to estimate whether forensic patients were content to complete several data assessments per day over the course of several weeks, with the feasibility being operationalized by the compliance rate (percentage of completed questionnaires). The longitudinal single-case analyses were also performed to address the methodological challenge of heterogeneity. In addition, differences between the three measurement timepoints (PRE, POST, FoUp1h) for each affect dimension (energetic arousal, valence, calmness) were examined. To analyze within-subject changes and to describe in more detail how ST affected momentary affective states, a one-way repeated-measures ANOVA was performed for the individual affective states. The ANOVA estimated if there were significant differences between the three measurement timepoints separately for each affect dimension. The weekly study sessions of ST as well as the factor time acted as independent variables, and the momentary affective states served as dependent variables.
Data were analyzed in RStudio with the corresponding describeBy() function from the psych package (28) (alpha level p < 0.05). For ANOVA, the aov() function of the afex package (29) was used. The effect sizes were calculated using the eta_squared() function from the effectsize package (30).
The requirements for ANOVA are the normal distribution of the data and variance homogeneity (31), which, as expected, was partially present in the dataset of this study. Nevertheless, repeated-measures ANOVA was conducted to give a certain trend recommendation.
A total of 130 questionnaires were completed (PRE: 50, POST: 50, FoUp1h: 30) by the 10 patients (Mage = 31.7, SD = 11.94; 60% male). Table 1 provides an overview of the data points provided by each patient (Table 1). The scores on the three affect dimensions were as follows (between-person distribution): energetic arousal, M = 4.6 (SD = 1.1; min = 1, max = 6); valence, M = 4.6 (SD = 1.47; min = 1, max = 6); and calmness, M = 4.9 (SD = 1.14; min = 1, max = 6).
Patients 3 and 4 dropped out of the study after 10 and 14 days, respectively. Patient 8 did not participate in a single intervention measurement timepoint and consequently could not provide any conclusions about the effectiveness of ST. Due to the amount of missing data (≥40%), patients 5, 6, 7, and 9 were also excluded from the descriptive presentation of the results, as their incomplete data could not provide any conclusions about the effectiveness of ST. Therefore, a statistical presentation of the results of patient 1 (PRE: N = 10, POST: N = 10, FoUp1h: N = 7), patient 2 (PRE: N = 10, POST: N = 10, FoUp1h: N = 9), and patient 10 (PRE: N = 8, POST: N = 8, FoUp1h: N = 3) was included for analyses (compliance rate: >63%). The effect size is an important finding to report, as a p value only indicates the presence of an effect, but does not indicate the size of the effect (32). Effect sizes, unlike significance tests, are not dependent on sample size, but a significance test does (32). When describing the effect sizes, the following values are considered: η2 = 0.01 (small effect), η2 = 0.06 (medium effect), and η2 = 0.14 (large effect) (33).
In patient 1 (Figure 1), our analyses showed a difference between the three measurement timepoints for energetic arousal, with the median score increasing from 4.5 (PRE) to 5.0 (POST) l. The valence scores increased from 2.5 (PRE) to 3.75 (POST), and the calmness scores increased from 5.5 (PRE) to 5.75 (POST). This indicates that patient 1 felt more energized, more comfortable, and less restless immediately after ST. The median energetic arousal score was stable at FoUp1h (5.0), while the median scores on valence (3.5) and calmness (5.5) decreased at follow-up.

Figure 1. The indicated values (1–6) of the dimensions energetic arousal, valence and calmness for measurement timepoint 1 (PRE), measurement timepoint 2 (POST) and measurement timepoint 3 (FoUp1h) for patient 1. The boxplots display the median and the 2nd and 3rd quartile.
Small effect sizes were observed for energetic arousal (η2 = 0.01) and calmness (η2 = 0.02), while no effect was observed for valence (η2 = 0.0041).
In patient 2 (Figure 2), our analyses showed differences in affective dimensions between the three measurement timepoints, with the median energetic arousal score increasing from 5.0 (PRE) to 5.5 (POST), the median valence score increasing from 5.75 (PRE) to 6.0 (POST), and the median calmness score increasing from 5.5 (PRE) to 6.0 (POST). This indicates that patient 2 felt more energized, more comfortable, and less restless immediately after ST. The scores at FoUp1h were stable for valence (6.0) and in calmness (6.0), while the median energetic arousal score decreased at follow-up (5.0).
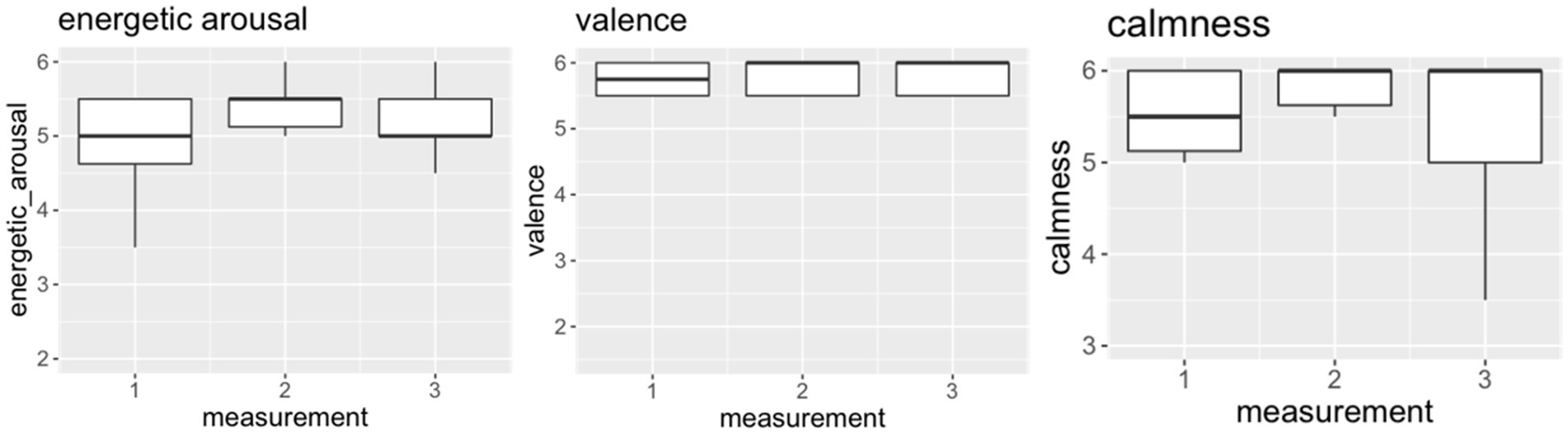
Figure 2. The indicated values (1–6) of the dimensions energetic arousal, valence and calmness for measurement timepoint 1 (PRE), measurement timepoint 2 (POST) and measurement timepoint 3 (FoUp1h) for patient 2. The boxplots display the median and the 2nd and 3rd quartile.
Medium effect sizes were observed for energetic arousal (η2 = 0.07) and valence (η2 = 0.07), but no effect was observed for calmness (η2 = 0.000572).
In patient 10 (Figure 3), our analyses showed a difference in calmness between the three measurement timepoints, with the median score increasing from 5.5 (PRE) to 5.75 (POST) and the decreasing to 5.5 again at FoUp1h. For energetic arousal and valence, the median score did not change between the PRE to POST timepoints (5.5 and 5.75, respectively). Furthermore, the median scores for energetic arousal (5.5) and valence (6.0) increased at FoUp1h.
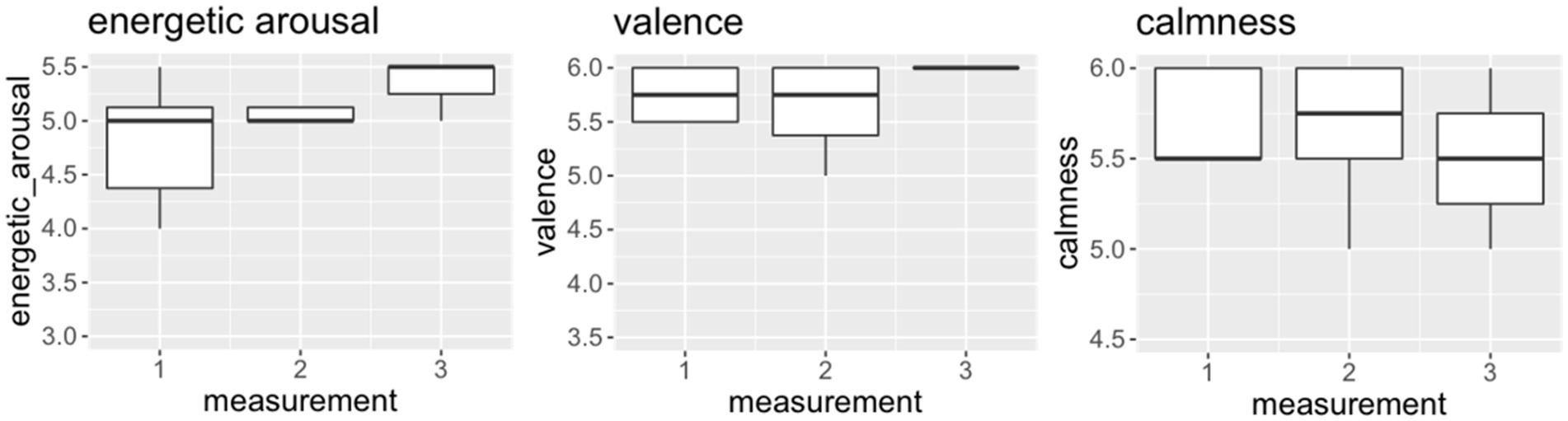
Figure 3. The indicated values (1–6) of the dimensions energetic arousal, valence and calmness for measurement timepoint 1 (PRE), measurement timepoint 2 (POST) and measurement timepoint 3 (FoUp1h) for patient 10. The boxplots display the median and the 2nd and 3rd quartile.
A medium effect size was observed for energetic arousal (η2 = 0.06), but no effects were observed for valence (η2 = 0.00133) and calmness (η2 = 0.00217).
In our study, we evaluated the feasibility of an intensive longitudinal case study design in forensic psychiatry to determine whether forensic patients are content to complete several data assessments per day over the course of several weeks, with feasibility operationalized by the compliance rate. Herein, single-case studies were performed to examine the effects of ST on momentary affective states (energetic arousal, valence, and calmness); the completion of these assessments reflect one aspect of feasibility. The findings reveal effects of ST in forensic psychiatric patients with different conditions.
On the one hand, our results provide insight into the feasibility of an intensive longitudinal design with respect to the compliance rate. Intensive longitudinal case studies, however, also bring new challenges, such as a high effort for the patients and thus a declining compliance rate. The compliance rate of >63% was only based on three patients. Concerning the challenge due to the compliance rate, our findings showed that out of 10 participants, three subjects dropped out before the end of the study. Four additional participants did not provide sufficient data for analysis. Ultimately, three patients provided data that were suitable for analysis. Thus, the compliance rate was ≤37% in seven out of 10 patients. Our data show that single-case studies are able to express heterogeneity more precisely. Regarding the low compliance rate in our study or other studies with special populations such as forensic psychiatric subjects (7), the very different daily routines of the participants made it difficult to determine the appropriate measurement timepoints at which all participants could be reached for the FoUp1h measurement timepoint. Of the three intervention measurement timepoints, the FoUp1h was extremely difficult to implement (see Table 1) since the patients had to be actively sought. Reaching the participants for this intervention measurement timepoint was extremely difficult, while reaching the subjects for the PRE and POST measurement timepoints was easier.
On the other hand, our single-case analyses reveal that the results are heterogeneous. Except for energetic arousal, the effects are heterogeneous overall. The rate of missing data was high in our study. We did not have a sufficient amount of data per patient for a proper single-case analysis. Power analyses revealed that the study was underpowered in all three patients (patient 1: 0.39; patient 2: 0.36; patient 10: 0.26). For a sufficiently powered study (0.80), at least 73 data per analysis would have been needed (34). The many missing data can be explained by the fact that a lack of motivation quickly spread. After 2 weeks of the study, the patients had to be extremely motivated to continue filling out the questionnaires. The fourth and last week of the study had the most missing data, which is why the study was terminated after 4 weeks. Ultimately, only the people who participated at enough measurement timepoints could be included. Additionally, the FoUp1h measurement timepoint was a huge barrier because there were only very few patients left at that time. Our low sample size of 10 participants represents the normal sample size in forensic psychiatric ST. Concerning the effects of ST on affective states, none of the three affect dimensions changed significantly between the three measurement timepoints. There were low to medium differences between the three measurement timepoints on energetic arousal, although these differences were nonsignificant. It must be noted that two of the three patients started with high values, and thus, no large increases could be expected. Our findings are partly in line with previous results: an intervention study showed positive associations between a sport and exercise therapy program (3 months with a 90-min session twice a week) and affective states in a single-case study with one person diagnosed with posttraumatic stress disorder (35). As the duration of the program increased, positive affective states were perceived more often (35). A meta-analysis examining within-person changes in affective responses to physical activity in people with depression shows that acute bouts of physical activity moderately improve affective states (36). The discrepancy between these findings and the findings of our study is due to the fact that forensic psychiatric studies present challenges that differ from the challenges associated with studies among patients with mental illness without a forensic connection. Forensic psychiatry has stricter rules, and thus, there is less freedom in the design and implementation of studies in ST.
Further research in this area is needed. This intervention provides initial approaches with the special population of forensic psychiatric patients.
It should be noted that repeated-measures ANOVA was conducted with normality and variance homogeneity partially being present since other statistical methods would not have produced more significant results either. Moreover, it was used for data that all came from the same individual. There is a possibility that this could have limited the variability between measurements and led to inaccurate results.
In addition, it must be noted that a sufficiently powered study (0.80) was not achievable due to the small amount of data.
The high baseline values on the affective dimensions for two patients might represent ceiling effects.
Forensic psychiatric patients are heterogeneous, and the individual effects of interventions on their affective states are also heterogeneous. Therefore, the results obtained herein can hardly be generalized. Even patients with the same diagnosis can present a different symptoms and medication regimes; therefore, it is extremely challenging to compare or equate one forensic patient to another.
This study suggests that an intensive longitudinal case study design in forensic psychiatry is feasible and that ST has small to medium short-term effects on affective states in individual patients who show a compliance rate of >63%. Compared to a between-subject design, we only used data of patients with an appropriate compliance rate for the evaluation.
However, the study design needs intensive revision to increase the compliance rate for particular study samples such as forensic patients. For example, a longer study duration and a survey of PRE and POST measurement timepoints alone could ensure a better compliance rate. Future studies should consider that data collection timepoints must be firmly integrated into the patients’ schedule (especially for the FoUp1h measurement). In collaboration with the facility, an individualized plan should be developed for each patient so that they are able to complete each questionnaire at every measurement timepoint.
Especially for longer-term data collection, participants of the study could be provided with a study smartphone (digital data collection). They could be reminded about the digital questionnaire via a signal tone, thereby enabling data collection even on days without ST to evaluate whether and to what extent patients feel better on days with ST.
Furthermore, participation in a study is only meaningful for patients who regularly participate in ST. In our study, it was shown that patients who regularly participated in ST also completed this study with a compliance rate of >63%. Patients who did not participate regularly in ST were more likely to drop out of the study or not to participate conscientiously. If only patients who regularly participate in ST are included in a study, less missing data can be expected. Data collection on at least 2 days of ST per week (à 3 measurement timepoints) over a period of at least 12 weeks is reasonable and realistic.
Another option is to stagger the reward (a small reward after each week and a large reward at the end of the study).
Further studies, e.g., multicenter studies, need to find out how and to whom the results can be generalized (patients with same diagnosis, same sex, similar age, similar medication, etc.).
Due to the abovementioned challenges (heterogeneity, low sample size, low and compliance rate) in conducting studies in ST in forensic psychiatry, intensive longitudinal case studies are a possible approach to address heterogeneity and the low sample size. To counteract the high effort of data delivery for the patients and the associated low compliance rate, a change of the study design (e.g., digital data collection) and a fixed establishment of the measurement timepoints in the patients’ schedule could improve the power of intensive longitudinal case studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
VR and MK contributed to the conception and design of the study and wrote sections of the manuscript. VR organized the database, performed the statistical analysis, and wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Centre for Psychiatry Reichenau for financing the third-party project funding and library of the University of Konstanz for paying the fees for open access.
We would like to thank Annette Stübinger, who performed a great amount of data collection. We would also like to thank the Centre for Psychiatry Reichenau for financing the third-party project funding and the library of the University of Konstanz for paying the fees for open access.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1111602/full#supplementary-material
1. Giménez-Meseguer, J, Tortosa-Martínez, J, and Cortell-Tormo, JM. The benefits of physical exercise on mental disorders and quality of life in substance use disorders patients. Systematic review and Meta-analysis. Int J Environ Res Public Health. (2020) 17:3680. doi: 10.3390/ijerph17103680
2. Firth, J, Cotter, J, Elliott, R, French, P, and Yung, AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. (2015) 45:1343–61. doi: 10.1017/S0033291714003110
3. Gordon, BR, McDowell, CP, Lyons, M, and Herring, MP. The effects of resistance exercise training anxiety: a Meta-analysis and Meta-regression analysis of randomized controlled trials. Sports Med. (2017) 47:2521–32. doi: 10.1007/s40279-017-0769-0
4. Rosenbaum, S, Tiedemann, A, Sherrington, C, Curtis, J, and Ward, PB. Physical activityinterventions for people with mental illness: a systematic review and meta-analysis. J Clin Psychiatry. (2014) 75:964–74. doi: 10.4088/JCP.13r08765
5. Ross, T, Reder, S, Querengässer, J, Mess, F, and Schmid, O. Sporttherapie in der forensischen Psychiatrie und Psychotherapie—eine Standortbestimmung. [sports therapy in the forensic psychiatry and psychotherapy—an assessment of the situation]. Forensische Psychiatrie und Psychotherapie. (2016) 23:37–65.
6. Schmid, O, Abele, L, Wichmann, P, Kluttig, T, Hoffmann, K, and Mess, F. Sporttherapeutische Ansätze in der forensischen Psychiatrie. Forensische Psychiatrie und Psychotherapie. (2016) 23:315–35.
7. Wynaden, D, Barr, L, Omari, O, and Fulton, A. Evaluation of service users’ experiences of participating in an exercise programme at the Western Australian state forensic mental health services. Int J Ment Health Nurs. (2012) 21:229–35. doi: 10.1111/j.1447-0349.2011.00787.x
8. Skrinar, GS, Huxley, NA, Hutchinson, DS, Menninger, E, and Glew, P. The role of a fitness intervention on people with serious psychiatric disabilities. Psychiatr Rehabil J. (2005) 29:122–7. doi: 10.2975/29.2005
9. Cicchetti, D, and Rogosch, FA. Equifinality and multifinality in developmental psychopathology. Dev Psychopathol. (1996) 8:597–600. doi: 10.1017/S0954579400007318
10. Stellmacher, M, and Häbler, A. Sportmotivation unter Zwang—Besonderheiten der Motivation zum Sporttreiben im Maßregelvollzug In: A Schneider, A Köhler, and J Schumann, editors. Sport im Spannungsfeld zwischen Medien und Psychologie. Wiesbaden: Springer VS (2016). 201–14.
11. Billen, E, Garofalo, C, and Bogaerts, S. Trajectories of self-control in a forensic psychiatric sample. Stability and Association with Psychopathology, Criminal History, and Recidivism. Crim Justice Behav. (2019) 46:1255–75. doi: 10.1177/0093854819856051
12. Lillie, EO, Patay, B, Diamant, J, Issell, B, Topol, EJ, and Schork, NJ. The n-of-1 clinical trial: the ultimate strategy for individualizing medicine? Pers Med. (2011) 8:161–73. doi: 10.2217/pme.11.7
13. Marwick, KFM, Stevenson, AJ, Davies, C, and Lawrie, SM. Application of n-of-1 treatment trials in schizophrenia: a systematic review. Br J Psychiatry. (2018) 213:398–403. doi: 10.1192/bjp.2018.71
14. Rizvi, S, and Nock, M. Single-case experimental designs for the evaluation of treatments for self-injurious and suicidal behaviors. Suicide Life Threat Behav. (2008) 38:498–510. doi: 10.1521/suli.2008.38.5.498
15. Venetz, M, and Zurbriggen, C. Intensive Longitudinal Methods – ihre Eignung für die sonderpädagogische Forschung und exemplarische Anwendungsmöglichkeiten. Empirische Sonderpädagogik. (2015) 7:194–205.
16. Kwasnicka, D, Inauen, J, Nieuwenboom, W, Nurmi, J, Schneider, A, Short, CE, et al. Challenges and solutions for N-of-1 design studies in health psychology. Health Psychol Rev. (2019) 13:163–78. doi: 10.1080/17437199.2018.1564627
17. McDonald, S, and Nikles, J. N-of-1 trials in healthcare. Healthcare. (2021) 9:330. doi: 10.3390/healthcare9030330
18. Trompetter, HR, Johnston, DW, Johnston, M, Vollenbroek-Hutten, MM, and Schreurs, KMG. Are processes in Acceptance & Commitment Therapy (ACT) related to chronic pain outcomes within individuals over time? An exploratory study using n-of-1 designs. J Pers Oriented Res. (2019) 5:123–36. doi: 10.17505/jpor.2019.11
19. Cha, YH, Gleghorn, D, and Doudican, BC. Double-blind randomized N-of-1 trial of transcranial alternating current stimulation for mal de débarquement syndrome. PLoS One. (2022) 17:e0263558. doi: 10.1371/journal.pone.0263558
20. Pioch, A, Spreen, M, and Bokers, H. Music therapy for negative symptoms in patients with schizophrenia: five systemic N-of-1 trials in a high-security psychiatric hospital. Tijdschr Psychiatr. (2021) 63:412–8.
21. Mehta, UM, Ravishankar, V, and Thirthalli, J. Eszopiclone for persistent negative symptoms in schizophrenia—an unintended N-of-1 study. Schizophr Res. (2018) 193:438–40. doi: 10.1016/j.schres.2017.06.035
22. Goyal, P, Safford, M, Hilmer, SN, Steinman, MA, Matlock, D, Maurer, MS, et al. N-of-1 trials to facilitate evidence-based Deprescribing: rationale and case study. Br J Clin Pharmacol. (2022) 88:4460–73. doi: 10.1111/bcp.15442
23. Wolters, TLC, Van Vlijmen, J, and Zoals, N. 1 is er geen één [N-of-1 trials: the one and only]. Nedschr Geneeskd. (2022) 165:D6149.
24. Fielenbach, S, Donkers, FC, Spreen, M, and Bogaerts, S. Neurofeedback as a treatment for impulsivity in a forensic psychiatric population with substance use disorder: study protocol of a randomized controlled trial combined with an N-of-1 clinical trial. JMIR Res Protoc. (2017) 6:e13. doi: 10.2196/resprot.6907
25. Fielenbach, S, Donkers, FCL, Spreen, M, Smit, A, and Bogaerts, S. Theta/SMR neurofeedback training works well for some forensic psychiatric patients, but not for others: a sham-controlled clinical case series. Int J Offender Ther Comp Criminol. (2019) 63:2422–39. doi: 10.1177/0306624X19849562
26. Wilhelm, P, and Schoebi, D. Assessing mood in daily life. Eur J Psychol Assess. (2007) 23:258–67. doi: 10.1027/1015-5759.23.4.258
28. Revelle, W. Procedures for psychological, psychometric, and personality research. (2023). Available at: https://cran.r-project.org/web/packages/psych/psych.pdf (Accessed 11 April 2023)
29. Singmann, H, Bolker, B, Westfall, J, Aust, F, and Ben-Shachar, MS. Analysis of Factorial Experiments. (2023). Available at: https://cran.r-project.org/web/packages/afex/afex.pdf (Accessed 11 April 2023).
30. Ben-Shachar, MS, Makowski, D, Lüdecke, D, Patil, I, Wiernik, BM, and Thériault, R. Indices of Effect Size. (2023). Available at: https://cran.r-project.org/web/packages/effectsize/effectsize.pdf (Accessed 11 April 2023).
31. Kim, YJ, and Cribbie, RA. ANOVA and the variance homogeneity assumption: exploring a better gatekeeper. Br J Math Stat Psychol. (2018) 71:1–12. doi: 10.1111/bmsp.12103
32. Sullivan, GM, and Feinn, R. Using effect size-or why the P value is not enough. J Grad Med Educ. (2012) 4:279–82. doi: 10.4300/JGME-D-12-00156.1
33. Cohen, J. Statistical power analysis for the behavioral sciences. 2nd ed. NJ Hillsdale Routledge: L. Erlbaum Associates (1988).
34. Faul, F, Erdfelder, E, Lang, AG, and Buchner, A. G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
35. Ley, C, Rato Barrio, M, and Koch, A. "in the sport I am Here": therapeutic processes and health effects of sport and exercise on PTSD. Qual Health Res. (2018) 28:491–507. doi: 10.1177/1049732317744533
Keywords: intensive longitudinal case studies, sports therapy, forensic psychiatry, affective states, energetic arousal, valence, calmness
Citation: Reimer V and Kanning MK (2023) Does sports therapy affect momentary affective states? Feasibility of intensive longitudinal case studies in forensic psychiatry. Front. Psychiatry. 14:1111602. doi: 10.3389/fpsyt.2023.1111602
Edited by:
Thomas Wenzel, University of Vienna, AustriaReviewed by:
Ana Grilo, Escola Superior de Tecnologia da Saúde de Lisboa (ESTeSL), PortugalCopyright © 2023 Reimer and Kanning. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vanessa Reimer, dmFuZXNzYS5yZWltZXJAdW5pLWtvbnN0YW56LmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.