 Javad Alaghband-rad1
Javad Alaghband-rad1 Arman Hajikarim-Hamedani
Arman Hajikarim-Hamedani Mahtab Motamed
Mahtab Motamed
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 16 March 2023
Sec. Autism
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1108110
Introduction: Autism spectrum disorder (ASD) is characterized by persistent deficits in social communication and social interaction across multiple contexts. Social camouflaging was first shown to be a characteristic of autistic persons, who actively try to disguise and compensate for their autism features in social contexts in an effort to socially blend in better. Recently, an increasing, though still insufficient, number of studies has been conducted on the concept of camouflage; however, different aspect of it, from psychopathology and etiology to its complications and consequences, are not clearly defined. We aimed to systematically review the existing literature on camouflage in autistic adults to describe the correlates of camouflage, motivations for exhibiting camouflage behavior, and the potential impacts of camouflage on the mental health of autistic individuals.
Methods: We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist guidelines to conduct a systematic review. The databases of PubMed and Scopus, and PsycInfo were searched for eligible studies. Studies were published between January 1st, 1980, to April 1st, 2022.
Results: We included 16 articles, of which four studies were qualitative and 11 were quantitative. One study used a mix method. The assessment tools used for camouflage, the correlates of camouflage including autism severity, gender, age, cognitive profile and neuroanatomical correlates, reasons for camouflage and the impacts of camouflaging behavior on mental health are discussed in this review.
Discussion: In synthesizing the literature, we conclude that camouflage seems to be more common among females who report more autistic symptoms themselves. There may also be some differences between men and women in reasons of exhibiting it and its neuroanatomical correlates. Further research is needed as to why this phenomenon is more prevalent in females with implications for gender related cognitive and neuroanatomical differences. Effects of camouflage on mental health and daily life measures of individuals such as employment, university graduation, relationship, financial status, and quality of life should be studied with more details in future studies.
Autism spectrum disorder (ASD) is characterized by persistent deficits in social communication and social interaction across multiple contexts, including deficits in social reciprocity, non-verbal communicative behaviors used for social interaction, and skills in developing, maintaining, and comprehending relationships (1). This disorder is highly hereditary, with an estimated 80 to 90% heritability (2). ASD has a frequency of 16.8 per 1,000 individuals (3). Most research on ASD has focused on children; however, studies on different aspects of autism in adulthood have increased in the past two decades (4).
Besides all the commonalities, autistic individuals are a group of heterogenous individuals presenting with a variety of symptoms. This variation in symptoms might be due to differences in gender, intellectual abilities, or adaptive abilities gained throughout developmental and social life.
In addition to variability in terms of clinical presentations, many autistic individuals show a range of behaviors and strategies that help them mask some of their symptoms and mimic behaviors of neurotypical individuals in order to fit in the community. Social camouflaging was first shown to be a characteristic of autistic persons, who actively try to disguise and compensate for their autism features in social contexts in an effort to blend in socially better (5–7). Camouflaging consists of complicated copying behaviors and/or masking certain personality features with an adaptive role that aids changes to different situational demands (5, 8, 9). Camouflage is more prevalent on social occasions, although it is not limited to them (6).
Recently, an increasing, though still insufficient, number of studies have been conducted on the concept of camouflage; however, different aspects of it, from psychopathology and etiology to its complications and consequences, are not clearly defined. A growing body of evidence shows that it is a reasonably prevalent characteristic among high-functioning females with ASD. Females with ASD are more competent than males to mask their symptoms from adult observers. Being in close proximity to peer groups helped females access chances for social contact, but a deeper study indicates that girls with ASD were less likely to have the skills required to utilize those opportunities to connect with peers effectively (10).
There have been observed gender differences in the prevalence of ASD diagnosis in females (11–13). Males are diagnosed with ASD three to four times more often than females (3). Females are diagnosed with autism at a later age than boys, reducing their possibilities of obtaining care (14). In comparison to males, females with an ASD diagnosis often have more severe symptoms and comorbidities (such as intellectual disability [ID] or epilepsy) (13, 15).
Multiple biological and cognitive factors seem to explain the disparities between men and girls in terms of ASD diagnosis (5), such as: (a) cognitive development disparities exist since females seem to have superior visual abilities and higher IQ scores (8); (b) the fact that females are preserved by intrinsic systems, such as sex-steroid hormones (16); (c) variations in empathizing and systemizing, whereby females seem to be more sympathetic due to social compensating abilities, and/or (d) the camouflage of ASD core symptoms (6). In accordance, the female phenotype of ASD is characterized by the capacity to conceal autistic symptoms. Females are likely more socially adept due to their ability to camouflage autistic symptoms, which may lead to a delayed or missing diagnosis (8). Though the underlying etiology is not attributed to a specific factor but differences in social norms and expectations from males and females, the difference in the autism severity in men and women, and neuropsychological differences have all been suggested.
Camouflage has been demonstrated and evaluated using various measures in the literature. Early evaluations have emerged from qualitative descriptions of autistic individuals, their families, and mental health providers working with them. Later works focused on quantifying camouflage regarding the discrepancy between individuals’ autistic traits and their observed behaviors. The most recent quantifying measures are self-report questionnaires which give a score for the extent of camouflage behavior one employs. Hull, Laura, et al. created the Camouflaging Autistic Traits Questionnaire (CAT-Q) to measure the extent to which autistic and non-autistic adults engage in three aspects of social camouflaging: (1) “compensation” for autism-related difficulties in social situations, such as using scripts and copying others from carefully observing other people; (2) “masking” one’s autistic characteristics, by constantly monitoring one’s own behaviors (e.g., eye contact, facial expression, gesture) to show a non-autistic persona to others; and (3) “assimilation” which describes behavioral techniques used to fit in better with others (e.g., forcing oneself to interact by performing and pretending) (17).
Although the effect of camouflage is understudied, this concept has been referred to in the literature as imitation (18), copying (8, 19, 20), masking (19–21), and compensation (21). Camouflage may impose many difficulties on autistic individuals, including depression, anxiety, and burnout. Additionally, it may also lead to delayed diagnosis, which prevents them from getting appropriate care.
Not a large number of systematic reviews have been conducted on camouflage. Three of the previous reviews studied camouflage in females only (7, 22). The most recent systematic review by Cook et al. included studies done on both males and females. However, the review is not specified to the adult population (23).
We aimed to systematically review the existing literature on camouflage in autistic adults to describe the correlates of camouflage, motivations for exhibiting camouflaging behavior, and the potential impacts of camouflage on the mental health of autistic individuals. We evaluated the strengths and weaknesses of the research base and highlighted the areas where the evidence is consistent and reliable while identifying wherever the evidence is inconsistent.
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (24, 25) checklist guidelines to conduct a systematic review. The following databases (PubMed, Scopus, and PsycInfo) were chosen for research (Figure 1).

Figure 1. Study selection. Preferred items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Out of 659 identified studies and after the application of the inclusion and exclusion criteria, 16 studies were included in the synthesis (25).
Before the screening, the following inclusion and exclusion criteria were established. Inclusion criteria were as follows: Human studies only, measurements from a minimum of one established cognitive test and English as the language of publication. Exclusion criteria were as follows: studies with participants under the age of 18, letters, editorials, reviewers, and commentaries.
The databases of PubMed and Scopus, and PsycInfo were searched for eligible studies. Studies were published between January 1st, 1980 to April 1st, 2022.
Separate search strategies were created for each database. The search terms we used to mine each thesaurus began with a mix of generic terms drawn from cognitive domains and terms drawn from our own prior knowledge. Several preliminary scoping searches were undertaken, from which a handful of essential search phrases were derived. Listed below is an example of a conclusive search method for the PubMed database.
(“adult*”[All Fields] OR (“grown”[All Fields] AND “up”[All Fields]) OR (“men”[MeSH Terms] OR “men”[All Fields] OR “man”[All Fields])) AND (“autism s”[All Fields] OR “autisms”[All Fields] OR “autistic disorder”[MeSH Terms] OR (“autistic”[All Fields] AND “disorder”[All Fields]) OR “autistic disorder”[All Fields] OR “autism”[All Fields] OR (“autism spectrum disorder”[MeSH Terms] OR (“autism”[All Fields] AND “spectrum”[All Fields] AND “disorder”[All Fields]) OR “autism spectrum disorder”[All Fields])) AND (“camouflag*”[All Fields] OR “compensat*”[All Fields] OR (“mask s”[All Fields] OR “masked”[All Fields] OR “masking”[All Fields] OR “masks”[MeSH Terms] OR “masks”[All Fields]))
The words enclosed by brackets indicate whether the term is a search term or a Medical Subject Heading (MeSH). All search queries were examined for registration as MeSH terms.
Whether this was the case, a search was run to see if it was essential, as indicated, to add the search phrase booth as a mesh term with explosion and a search term.
This was done to reduce the complexity of the search phrase while maintaining the same search results since certain databases struggled to process lengthy search strings. Similar experiments were done in all datasets.
All references were imported into EndNote 20, where duplicates were subsequently discovered and eliminated.
One reviewer collaboratively devised a data-charting form to select which variables to extract. The reviewer extracted data separately and discussed the findings in the event of a dispute. Article characteristics (author, year, country, journal, and citations) and population characteristics (autism severity, autism diagnostic tools) were extracted, along with sample size (n) and mean age and sex. Research parameters (intervention, outcome, and impact) were used for the conclusion of data extraction.
The risk of bias was evaluated using a technique developed by The Effective Public Health Practice Project (EPHPP) [21] to assess the methodological quality of primary studies using a range of research designs. There are six component ratings: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection method, and (6) withdrawals and dropouts. Each element is ranked as weak, moderate, or strong. If there are no weak ratings, the international rating is strong; if there is one poor rating, it is moderate; and if there are two or more weak ratings, it is weak. The tool was adjusted somewhat since the component domain (c) “confounders” was particularly applicable to randomized controlled research, where control for group differences is crucial. In the current research, the populations serve as their own controls, making this factor less significant. Again, the two reviewers evaluated the research separately and discussed the findings in the case of disagreement.
We included 16 articles, of which four studies were qualitative, and 11 were quantitative were included in this review. One study used a mixed method. Detailed characteristics and main findings of the studies are demonstrated in Table 1.
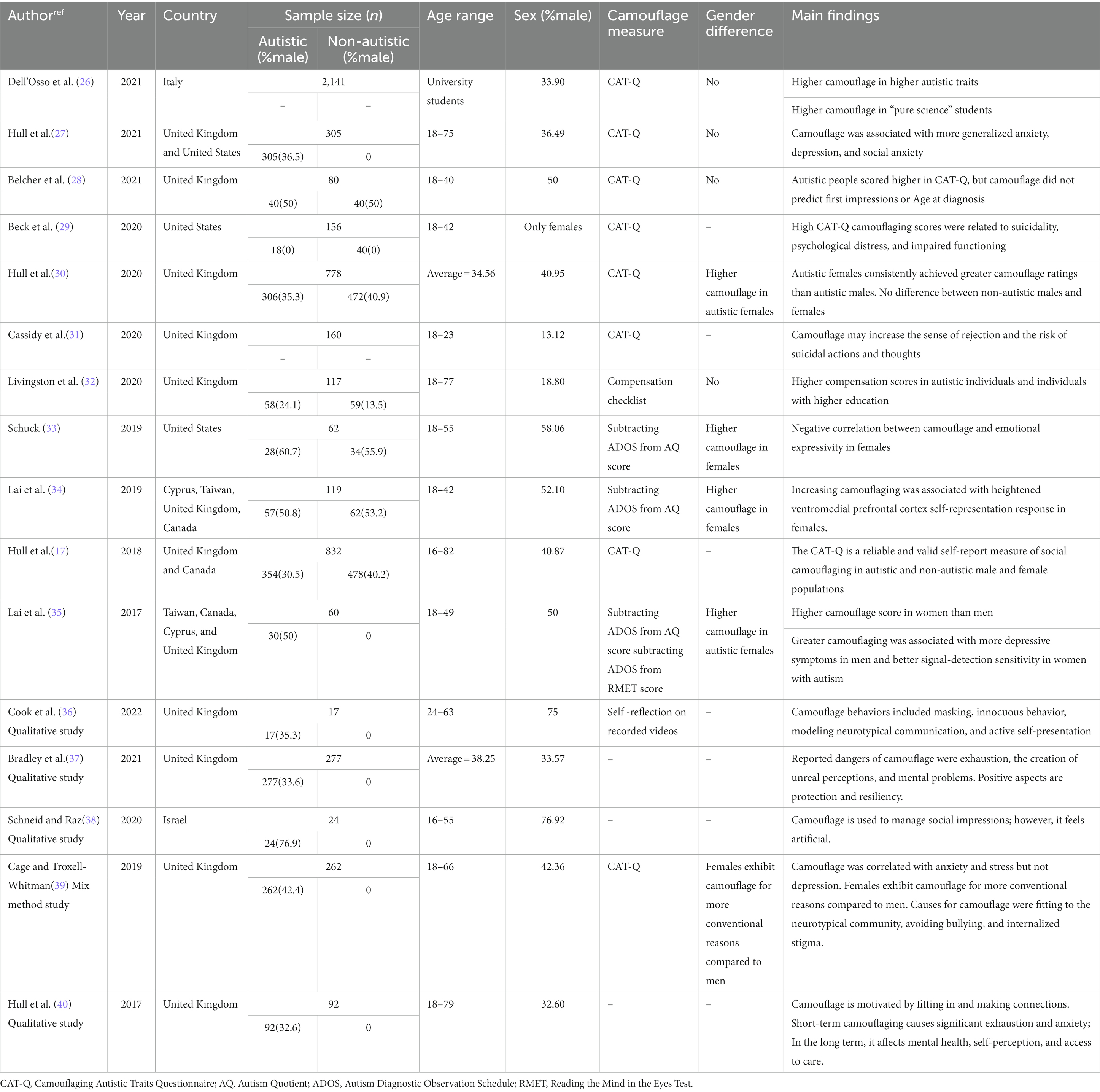
Table 1. Characteristics and main findings of studies included in the systematic review.
Camouflage was assessed using different measures. The most common tool (eight studies) was the Camouflaging Autistic Traits Questionnaire (CAT-Q) (26–31, 36, 39) which is a 25-item self-report questionnaire developed in 2018 by Hull et al. (17). One study utilized a 31-item Compensation Checklist to evaluate strategies including masking, shallow compensation, deep compensation, and accommodation in participants (32).
In some studies, camouflage was scored by subtracting Autism Diagnostic Observation Schedule (ADOS) score from Autism Quotient (AQ) score (33–35). In a number of studies screening and open questions were used to assess the extent of camouflaging (37–40). In a study by Cook et al. authors asked the participants to watch their own interactions and self-reflect on camouflaging (36).
Some correlates have been suggested for camouflage in a number of studies (26, 33).
Camouflaging was reported to be higher in autistic individuals compared to non-autistic individuals (28, 30). A significant positive relationship between camouflaging behavior and autism severity (higher scores in autism questionnaires) was observed in some studies (26, 28, 31, 32). Dell’Osso et al. reported a strong association between autistic traits and camouflaging in university students (26). Higher AQ10 scores and having an autism diagnosis were positively associated with total compensation and shallow compensation (32). Similarly, a significant positive relationship was found between AQ28 and CAT-Q total and subscales scores in 160 undergraduate students in the United Kingdom (31).
It has been revealed by three studies that camouflage behavior is more common in autistic females rather than males (30, 33, 35). However, some studies could not find the gender difference in the non-autistic population (26, 28, 30) or in samples of autistic adults (27, 28). Using a Compensation Checklist, Livingston et al. did not find a relationship between compensation score and sex (32).
In addition to the prevalence of camouflage behavior, a gender difference was found in the reasons for camouflaging in autistic women and men (39).
Students of pure sciences reported higher camouflaging behavior compared to applied sciences (26). This group scored higher in The Adult Autism Subthreshold Spectrum (AdAS). Livingston et al. reported that a higher educational level was associated with higher compensation in autistic and non-autistic adults (32).
One study showed a negative correlation between emotional expressivity and positive expressivity in autistic females; however, this correlation was not observed in autistic males (33). In this study, no correlation between working memory and camouflage was found. No significant correlation between IQ and camouflage was found by Lai et al. (35); However, the authors found a positive correlation between camouflage and signal detection sensitivity. Similarly, Belcher et al. reported no correlation between camouflage and executive function or theory of mind in 80 autistic participants (28).
Only one study explored the effect of camouflage on the Age of receiving ASD diagnosis and found no relationship between them (28). No correlation was found between Age and camouflage in two other studies (32, 35). However, a negative correlation between the compensation subscale of CAT-Q and Age was reported in undergraduate students in one study (31).
Only two studies explored camouflaging in relation to neuroanatomical regions or activity. One study examined the neural responses during mentalization and self-representation and found a positive correlation between camouflage and activation of the ventromedial prefrontal region during self-representation (34). Lai et al. revealed a gender difference in neuroanatomical correlates of camouflage. While no neuroanatomical association with camouflage was found in men, smaller volumes in the medial temporal and cerebellum were associated with higher camouflaging in autistic women (35).
Some reasons mentioned for camouflaging by autistic individuals included helping them to access the social world and social opportunities and making friends, being accepted by others, maintaining safety, and building resiliency (37, 40). Different reasons for camouflage were described in one study; while women engage in camouflage to serve a functional purpose in the workplace or education, men camouflage to be more comfortable in social interactions (39).
Some studies reported the consequences of camouflage in autistic and neurotypical individuals (27, 29, 35). According to a study in 2020, camouflaging was a predictor of psychological distress (measured by The Depression Anxiety Stress Scales 21) and functional challenges (measured by The World Health Organization Disability Assessment Schedule, Second Edition) but not suicidality in women. Though in the high camouflage group, a significant relationship between CAT-Q score and suicidality was found (29). Cassidy et al. found an increased risk of experiencing thwarted belongingness and lifetime suicidality in undergraduate students with higher camouflaging autistic traits (31).
In a similar vein, Hull et al. demonstrated an association between camouflage and generalized anxiety, social anxiety, and to a smaller extent between camouflage and depression in a sample of 305 autistic adults (27). The effect of camouflage on anxiety and stress was replicated in the study of Cage and Troxell-Whitman (39). Lai et al. reported a correlation between depression and camouflage in autistic men but not women. Such correlation was not observed for anxiety (35).
Moreover, the impacts of camouflage have been investigated through open questions about the experience of autistic individuals and further thematic analyses (37, 40). Exhaustion, depression, and anxiety, making unreal perceptions of others were the consequences stated by autistic adults. For some individuals, camouflaging affected their self-perception and gave them a feeling of deception, which led to anxiety, isolation, and a sense of alienation (38, 40).
We did a systematic review of empirical studies of camouflage phenomena in autistic adults. Social camouflage is an emerging topic of research with an increasing number of studies over the last decade. Camouflage research has also included various concepts of masking, compensation, copying, or imitation in different studies (23, 26).
Recent attempts to develop an index (33, 34) and questionnaires (17, 32) with gender-sensitive criteria for camouflage have made this field of research more interesting. Almost all the measures are self-reports through questionnaires. In one study, autistic individuals were asked to report camouflage behaviors when watching their own video recordings (36). Assessing camouflage with objective measures is not studied and needs further attention. In one study, autistic individuals were asked to report camouflage behaviors when watching their own video recordings. It should be noted that some autistic individuals might engage in camouflaging while they are not aware of it and do not report it, respectively.
In synthesizing the literature, we conclude that camouflage seems to be more common among females who report more autistic symptoms themselves (26, 28, 32) and are perhaps more aware of their challenges in social situations. This self-awareness and continuous effort to mask their symptoms would naturally lead to more negative emotional outcomes (27, 29).
There are various correlates of camouflage that makes it more interesting, as follows:
There are a number of studies suggesting camouflage to be a characteristic of females with ASD or reporting it to be more common among this group of female patients (30, 33, 35). It is noteworthy to mention that not all the studies found such a difference.
A number of studies evaluated cognitive profiles of adult ASD, and a subset of these studies looked into those patients who present with camouflaging (28, 33, 35). Higher vocal expression, behavior involvement in social behavior (41), and higher education (32) have been reported in these studies. There are also studies that found those with camouflaging reporting more autistic symptoms (26).
There are very few studies reporting on neuroanatomical correlates of camouflaging. In those reports, activation of the ventromedial prefrontal region and smaller volumes of medial temporal and cerebellum were associated with higher camouflaging.
As it is described, the correlates of camouflage are not widely studied, and there exist many inconsistencies, and many questions have remained unanswered.
Not many studies explored the reasons and motivations for camouflage. In general, autistic individuals use camouflage as a tool to help them to fit better in neurotypical communities (37, 40). Further qualitative studies about the lived experiences of autistic individuals about different types of camouflaging, the situations which provoke camouflaging, and the objectives that they seek when they camouflage would be warranted to make the reasons behind camouflaging more clear.
The impacts of camouflaging on the mental health of autistic individuals have been described in some studies. It can be summarized that although camouflage could provide some advantages to better fit in society can lead to some disadvantages like anxiety, depression, and exhaustion. Kim et al. conducted a meta-regression analysis of correlates of quality of life in autistic individuals (42). They did not find a significant effect size for IQ or autism severity. Nevertheless, they found a significant effect size for social functioning and quality of life. They suggested that camouflaging can have positive impacts on social functioning as individuals can reach their short-term goals by using camouflage. However, the short-term benefits of camouflage should be weighed against the long-term costs of camouflage, such as depression and exhaustion. Accordingly, the impacts of camouflage on the quality of life of autistic individuals should be considered in a multilayered and deeper view. Effects of camouflage on daily life measures of individuals such as employment, university graduation, relationship, financial status, and quality of life should be studied with more detail in future studies. The impact of camouflage on service delivery, misdiagnosis, and delayed diagnosis are other understudied areas that should be addressed when exploring camouflage in autism (43).
In conclusion, camouflage is apparently a set of strategies and self-control skills (44) used by autistic females who are more self-aware of their autistic symptoms (28, 32). This also explains why camouflage correlates positively with university education. These continuous efforts to mask symptoms are mentally costly for them and lead to mental health challenges (27, 37, 40). Further research is needed as to why this phenomenon is more prevalent in females, with implications for gender-related cognitive and neuroanatomical differences. Camouflaging is also important clinically, as health professionals are not familiar enough to diagnose adult ASD, particularly those who camouflage. Better understanding of the phenomenon would decrease the long-term consequences of non-diagnosis or misdiagnosis in this population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
JA-r contributed in idea creation, design of the study, categorizing and synthesizing the data, and drafting. AH-H contributed in idea creation, databases search, categorizing the data, and drafting. MM contributed in idea creation, design of the study, databases search, categorizing and synthesizing the data, and drafting. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer EC declared a past collaboration with author JA-r to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Psychiatric Association, D., & American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR Washington, DC: American Psychiatric Association Publishing (2013)5.
2. Psychiatrists RCo. The Psychiatric Management of Autism in Adults (CR228). England and Wales: Royal College of Psychiatrists (2020).
3. Baio, J, Wiggins, L, Christensen, DL, Maenner, MJ, Daniels, J, Warren, Z, et al. Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill Summ. (2018) 67:1–23. doi: 10.15585/mmwr.ss6706a1
4. Malik-Soni, N, Shaker, A, Luck, H, Mullin, AE, Wiley, RE, Lewis, MES, et al. Tackling healthcare access barriers for individuals with autism from diagnosis to adulthood. Pediatr Res. (2022) 91:1028–35. doi: 10.1038/s41390-021-01465-y
5. Lai, MC, Lombardo, MV, Pasco, G, Ruigrok, AN, Wheelwright, SJ, Sadek, SA, et al. A behavioral comparison of male and female adults with high functioning autism spectrum conditions. PLoS One. (2011) 6:e20835. doi: 10.1371/journal.pone.0020835
6. Tubio-Fungueirino, M, Cruz, S, Sampaio, A, Carracedo, A, and Fernandez-Prieto, M. Social camouflaging in females with autism Spectrum disorder: a systematic review. J Autism Dev Disord. (2021) 51:2190–9. doi: 10.1007/s10803-020-04695-x
7. Allely, CS. Understanding and recognizing the female phenotype of autism spectrum disorder and the “camouflage” hypothesis: a systematic PRISMA review. Adv Autism. (2018) 5:14–37. doi: 10.1108/AIA-09-2018-0036
8. Lai, MC, Lombardo, MV, Auyeung, B, Chakrabarti, B, and Baron-Cohen, S. Sex/gender differences and autism: setting the scene for future research. J Am Acad Child Adolesc Psychiatry. (2015) 54:11–24. doi: 10.1016/j.jaac.2014.10.003
9. Tint, A, and Weiss, JA. A qualitative study of the service experiences of women with autism spectrum disorder. Autism. (2018) 22:928–37. doi: 10.1177/1362361317702561
10. Dean, M, Harwood, R, and Kasari, C. The art of camouflage: gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism. (2017) 21:678–89. doi: 10.1177/1362361316671845
11. Giarelli, E, Wiggins, LD, Rice, CE, Levy, SE, Kirby, RS, Pinto-Martin, J, et al. Sex differences in the evaluation and diagnosis of autism spectrum disorders among children. Disabil Health J. (2010) 3:107–16. doi: 10.1016/j.dhjo.2009.07.001
12. Begeer, S, Mandell, D, Wijnker-Holmes, B, Venderbosch, S, Rem, D, Stekelenburg, F, et al. Sex differences in the timing of identification among children and adults with autism spectrum disorders. J Autism Dev Disord. (2013) 43:1151–6. doi: 10.1007/s10803-012-1656-z
13. Ratto, AB, Kenworthy, L, Yerys, BE, Bascom, J, Wieckowski, AT, White, SW, et al. What about the girls? Sex-based differences in autistic traits and adaptive skills. J Autism Dev Disord. (2018) 48:1698–711. doi: 10.1007/s10803-017-3413-9
14. Wood-Downie, H, Wong, B, Kovshoff, H, Mandy, W, Hull, L, and Hadwin, JA. Sex/gender differences in camouflaging in children and adolescents with autism. J Autism Dev Disord. (2021) 51:1353–64. doi: 10.1007/s10803-020-04615-z
15. Loomes, R, Hull, L, and Mandy, WPL. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. (2017) 56:466–74. doi: 10.1016/j.jaac.2017.03.013
16. Werling, DM. The role of sex-differential biology in risk for autism spectrum disorder. Biol Sex Differ. (2016) 7:58. doi: 10.1186/s13293-016-0112-8
17. Hull, L, Mandy, W, Lai, MC, Baron-Cohen, S, Allison, C, Smith, P, et al. Development and validation of the camouflaging autistic traits questionnaire (CAT-Q). J Autism Dev Disord. (2019) 49:819–33. doi: 10.1007/s10803-018-3792-6
18. Lai, MC, and Baron-Cohen, S. Identifying the lost generation of adults with autism spectrum conditions. Lancet Psychiatry. (2015) 2:1013–27. doi: 10.1016/S2215-0366(15)00277-1
19. Baldwin, S, and Costley, D. The experiences and needs of female adults with high-functioning autism spectrum disorder. Autism. (2016) 20:483–95. doi: 10.1177/1362361315590805
20. Mandy, W. Social Camouflaging in Autism: Is It Time to Lose the Mask?. (2019). London: SAGE Publications 1879–1881.
21. Mandy, W, Chilvers, R, Chowdhury, U, Salter, G, Seigal, A, and Skuse, D. Sex differences in autism spectrum disorder: evidence from a large sample of children and adolescents. J Autism Dev Disord. (2012) 42:1304–13. doi: 10.1007/s10803-011-1356-0
22. Hull, L, Petrides, K, and Mandy, W. The female autism phenotype and camouflaging: a narrative review. Rev J Autism Dev Disord. (2020) 7:306–17. doi: 10.1007/s40489-020-00197-9
23. Cook, J, Hull, L, Crane, L, and Mandy, W. Camouflaging in autism: a systematic review. Clin Psychol Rev. (2021) 89:102080. doi: 10.1016/j.cpr.2021.102080
24. Moher, D, Shamseer, L, Clarke, M, Ghersi, D, Liberati, A, Petticrew, M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
25. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:1–11. doi: 10.1186/s13643-021-01626-4
26. Dell'Osso, L, Cremone, IM, Chiarantini, I, Arone, A, Massimetti, G, Carmassi, C, et al. Autistic traits and camouflaging behaviors: a cross-sectional investigation in a university student population. CNS Spectr. (2021) 27:740–6. doi: 10.1017/S1092852921000808
27. Hull, L, Levy, L, Lai, M-C, Petrides, K, Baron-Cohen, S, Allison, C, et al. Is social camouflaging associated with anxiety and depression in autistic adults? Mol Autism. (2021) 12:1–13. doi: 10.1186/s13229-021-00421-1
28. Belcher, HL, Morein-Zamir, S, Mandy, W, and Ford, RM. Camouflaging intent, first impressions, and age of ASC diagnosis in autistic men and women. J Autism Dev Disord. (2022) 52:3413–26. doi: 10.1007/s10803-021-05221-3
29. Beck, JS, Lundwall, RA, Gabrielsen, T, Cox, JC, and South, M. Looking good but feeling bad: "camouflaging" behaviors and mental health in women with autistic traits. Autism. (2020) 24:809–21. doi: 10.1177/1362361320912147
30. Hull, L, Lai, MC, Baron-Cohen, S, Allison, C, Smith, P, Petrides, KV, et al. Gender differences in self-reported camouflaging in autistic and non-autistic adults. Autism. (2020) 24:352–63. doi: 10.1177/1362361319864804
31. Cassidy, S, Gould, K, Townsend, E, Pelton, M, Robertson, A, and Rodgers, J. Is camouflaging autistic traits associated with suicidal thoughts and behaviours? Expanding the interpersonal psychological theory of suicide in an undergraduate student sample. J Autism Dev Disord. (2020) 50:3638–48. doi: 10.1007/s10803-019-04323-3
32. Livingston, LA, Shah, P, Milner, V, and Happé, F. Quantifying compensatory strategies in adults with and without diagnosed autism. Mol Autism. (2020) 11:15. doi: 10.1186/s13229-019-0308-y
33. Schuck, RK, Flores, RE, and Fung, LK. Brief report: sex/gender differences in symptomology and camouflaging in adults with autism Spectrum disorder. J Autism Dev Disord. (2019) 49:2597–604. doi: 10.1007/s10803-019-03998-y
34. Lai, MC, Lombardo, MV, Chakrabarti, B, Ruigrok, AN, Bullmore, ET, Suckling, J, et al. Neural self-representation in autistic women and association with 'compensatory camouflaging'. Autism. (2019) 23:1210–23. doi: 10.1177/1362361318807159
35. Lai, MC, Lombardo, MV, Ruigrok, AN, Chakrabarti, B, Auyeung, B, Szatmari, P, et al. Quantifying and exploring camouflaging in men and women with autism. Autism. (2017) 21:690–702. doi: 10.1177/1362361316671012
36. Cook, J, Crane, L, Hull, L, Bourne, L, and Mandy, W. Self-reported camouflaging behaviours used by autistic adults during everyday social interactions. Autism. (2022) 26:406–21. doi: 10.1177/13623613211026754
37. Bradley, L, Shaw, R, Baron-Cohen, S, and Cassidy, S. Autistic adults' experiences of camouflaging and its perceived impact on mental health. Autism Adulthood. (2021) 3:320–9. doi: 10.1089/aut.2020.0071
38. Schneid, I, and Raz, AE. The mask of autism: social camouflaging and impression management as coping/normalization from the perspectives of autistic adults. Soc Sci Med. (2020) 248:112826. doi: 10.1016/j.socscimed.2020.112826
39. Cage, E, and Troxell-Whitman, Z. Understanding the reasons, contexts and costs of camouflaging for autistic adults. J Autism Dev Disord. (2019) 49:1899–911. doi: 10.1007/s10803-018-03878-x
40. Hull, L, Petrides, K, Allison, C, Smith, P, Baron-Cohen, S, Lai, M-C, et al. “Putting on my best normal”: social camouflaging in adults with autism spectrum conditions. J Autism Dev Disord. (2017) 47:2519–34. doi: 10.1007/s10803-017-3166-5
41. Corbett, BA, Schwartzman, JM, Libsack, EJ, Muscatello, RA, Lerner, MD, Simmons, GL, et al. Camouflaging in autism: examining sex-based and compensatory models in social cognition and communication. Autism Res. (2021) 14:127–42. doi: 10.1002/aur.2440
42. Kim, SY, and Bottema-Beutel, K. A meta regression analysis of quality of life correlates in adults with ASD. Res Autism Spectr Disord. (2019) 63:23–33. doi: 10.1016/j.rasd.2018.11.004
43. Green, RM, Travers, AM, Howe, Y, and McDougle, CJ. Women and autism Spectrum disorder: diagnosis and implications for treatment of adolescents and adults. Curr Psychiatry Rep. (2019) 21:22. doi: 10.1007/s11920-019-1006-3
Keywords: adult autism, camouflage, compensation, autism spectrum disorder, masking behavior
Citation: Alaghband-rad J, Hajikarim-Hamedani A and Motamed M (2023) Camouflage and masking behavior in adult autism. Front. Psychiatry. 14:1108110. doi: 10.3389/fpsyt.2023.1108110
Edited by:
Marco Colizzi, University of Udine, ItalyReviewed by:
Aldina Venerosi, National Institute of Health (ISS), ItalyCopyright © 2023 Alaghband-rad, Hajikarim-Hamedani and Motamed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mahtab Motamed, bW90YW1lZDg4QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.