
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 20 March 2023
Sec. Anxiety and Stress Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1068255
This article is part of the Research TopicImplementation of Evidence-Based Treatments for Child Anxiety and Related Disorders Across Diverse ContextsView all 8 articles
 Hannah E. Frank1,2*
Hannah E. Frank1,2* Grace Cain1,2
Grace Cain1,2 Jennifer Freeman1,2Kristen G. Benito1,2Erin O’Connor1,2
Jennifer Freeman1,2Kristen G. Benito1,2Erin O’Connor1,2 Josh Kemp1,2
Josh Kemp1,2 Bo Kim3,4
Bo Kim3,4Background: Youth with anxiety and obsessive–compulsive disorder (OCD) rarely access exposure therapy, an evidence-based treatment. Known barriers include transportation, waitlists, and provider availability. Efforts to improve access to exposure require an understanding of the process that families take to find therapists, yet no prior studies have examined parents’ perspectives of the steps involved.
Methods: Parents of children who have received exposure therapy for anxiety and/or OCD (N = 23) were recruited from a hospital-based specialty anxiety clinic where the majority of their children previously received exposure. Recruitment was ongoing until thematic saturation was reached. Parents completed questionnaires and attended an online focus group during which they were asked to describe each step they took—from recognizing their child needed treatment to beginning exposure. A process map was created and shown in real-time, edited for clarity, and emailed to parents for member checking. Authors analyzed process maps to identify common themes.
Results: Several themes emerged, as visually represented in a final process map. Participants identified a “search-outreach” loop, in which they repeated the cycle of looking for therapists, contacting them, and being unable to schedule an appointment due to factors such as cost, waitlists, and travel time. Parents often did not know about exposure and reported feeling guilty about their lack of knowledge and inability to find a suitable provider. Parents reported frustration that medical providers did not often know about exposure and sometimes dismissed parents’ concerns. Participants emphasized the difficulty of navigating the mental health system; many reported that it took years to find an exposure therapist, and that the search was sometimes stalled due to fluctuating symptoms.
Conclusion: A common thread among identified barriers was the amount of burden placed on parents to find treatment with limited support, and the resultant feelings of isolation and guilt. Findings point to several directions for future research, such as the development of parent support groups for navigating the mental health system; enhancing coordination of care between medical and mental health providers; and streamlining referral processes.
Youth with mental health problems have limited access to evidence-based interventions (EBIs). Although nearly 14% of youth have a mental health disorder (1), a minority of adolescents with these disorders access mental health treatment (2). Furthermore, adolescents with internalizing symptoms access treatment at lower rates than those with externalizing symptoms (2), highlighting how the treatment access crisis particularly affects anxious and depressed youth. Treatment access refers to the ability “to identify healthcare needs, to seek healthcare services, to reach, to obtain or use health care services, and to actually have the need for services fulfilled” [pg., 8, (3)]. A variety of factors may impact access to care, such as lack of transportation, long waitlists, and few available providers trained in EBIs (4). Factors such as inaccurate diagnosis of symptoms (5), limited consumer knowledge about EBIs (6), and minimal provider adoption of EBIs (7–9) all contribute to the difficulties of accessing appropriate care.
Exposure therapy for anxiety disorders and obsessive–compulsive disorder (OCD) is a particular striking example of an intervention that has strong empirical support (10) but is rarely used in routine clinical care settings (11), making it challenging for families to access. Although many efforts have been made to increase provider use of exposure therapy [e.g., through training providers (12)], it is still unlikely that an individual with an anxiety disorder or OCD will be able to access exposure therapy (13) or that it will be delivered effectively in a routine clinical care setting (14). Without adequate access to effective mental health care, anxious youth continue to struggle with symptoms that often persist into adulthood (13, 15, 16). Further research is needed to address the barriers parents and youth face when seeking exposure therapy for anxiety disorders and OCD.
The field of implementation science provides guidance for addressing barriers to accessing EBIs. Implementation science is the study of how to translate research findings into routine clinical practice settings, with the goal of improving the quality of services (17). Implementation science offers a wide array of conceptual frameworks that identify barriers and facilitators, or determinants, of EBI uptake across different domains and stages of implementation (18, 19). Assessment of these determinants is well documented for a variety of EBIs. The goal of identifying determinants is to guide the selection of implementation strategies that will increase the use and availability of EBIs (20). However, the process of selecting implementation strategies and tailoring them to a unique context and population is often a difficult and ill-defined task (21, 22). When researchers spend insufficient time understanding the barriers of a context or apply implementation interventions without matching them to the barriers they seek to mitigate, implementation efforts may yield ineffective results. In other words, implementation frameworks guide the selection of strategies that may improve the process of accessing EBIs, but such framework-guided strategy selection cannot be optimized without exactly “locating” where barriers are within the process and how they vary across contexts. Although existing research has gained insight from community partners to address this concern, no existing studies have focused on understanding parents’ perspectives of determinants to accessing EBIs for anxiety disorders and OCD.
Parents and caregivers are vital players in accessing treatment for anxious youth and can provide researchers with a direct view into the barriers and facilitators families face during the treatment seeking process. For youth with anxiety and OCD, seeking mental health services is often primarily driven by parents (23–25) and research suggests that adolescent treatment seeking is influenced by others, with the strongest influence coming from parents (26). Parents who have accessed EBIs for their children may be particularly well-positioned to identify possible solutions to address barriers to treatment access given their intimate knowledge of barriers faced during their own search. Past research indicates that parents identify determinants to accessing treatment for their children in a variety of categories. A systematic review found that families identified barriers in the form of: (1) structural barriers (e.g., wait times, cost); (2) individual-level barriers including (a) family attitudes towards treatment; (b) limited family knowledge of mental health problems and how to seek and access help; and (c) family circumstances such as a family’s support network (27). In another study that asked parents about barriers to seeking outpatient services for their children, 60.3% reported lack of information about where to seek help as a barrier, 59.8% reported professionals not listening as a barrier, and 53.7% reported providers not initiating treatment or issuing referrals as a barrier (28). While past research highlights the depth of knowledge that parents hold regarding their experience seeking services for their children, no prior studies have examined the unique process families go through to access EBIs for anxiety and OCD, including the timeline and barriers involved in accessing treatment.
Process mapping (29) is one method that can be used to systematically locate determinants to treatment access and guide optimal implementation strategy selection. Process mapping, which was originally developed and applied within the fields of business and engineering, is widely used for quality improvement in health and medical settings, and it has begun to be adapted for implementation efforts (30, 31). A process map is a detailed flow chart that makes work processes visible and identifies each of the actors and their roles in a process (29). Process mapping is a data-driven approach that identifies the steps in complex, multi-step activities and allows for assessment of inefficiencies and the development of more appropriate and effective systems (31–33). Given that few tools have been successful at assessing context prior to implementation or sustainability efforts (34), process mapping may be helpful to improve the selection of strategies that are uniquely appropriate for the local context, which will in turn increase the availability of EBIs and improve access to effective treatments. Process mapping provides a method for parents to identify the distinctive determinants they faced in their process of searching for services, and for the synthesis of parent experiences to identify common “stuck-points” in the process across individuals.
This study used process mapping to develop an in-depth understanding of parents’ efforts to access exposure therapy for their children, including inefficiencies and barriers encountered in the process. Developing a process map of accessing exposure therapy for anxiety is especially important given that: (1) there is robust evidence for the efficacy of exposure therapy, yet (2) significant barriers to accessing it persist. Although the barriers and facilitators to using exposure are well-documented (35), there is still disconnect between understanding barriers and identifying appropriate and effective implementation strategies to address these barriers. Process mapping may be well-suited to unpack this “black box” and understand the types of implementation strategies most appropriate to a specific context. Thus, the aim of this study was to use process mapping to identify specific barriers that parents face when trying to access exposure therapy, as well as to identify potential parent-identified solutions to address them.
Participants (N = 23) included parents of children (and one former patient) with anxiety and/or OCD who have received exposure therapy in any setting (i.e., community mental health, outpatient hospital-based clinic, and partial hospital program). Four participants were recruited from an existing parent advisory group, 12 from an outpatient hospital-based clinic study, one from a partial hospital program, and five from unknown sources. Other inclusion criteria included English-speaking and willingness to complete study procedures. There were no exclusion criteria.
Participants completed a questionnaire assessing parent and child demographic characteristics (e.g., age, sex, gender, race, and ethnicity).
Parents were asked to respond to a modified version of the CGI-S (36) in which they were asked “Please provide a rating for how severe your child’s anxiety/obsessive–compulsive disorder symptoms were at their worst” and “currently.” Responses ranged from 1 (normal, not at all a problem) to 7 (extremely ill), as consistent with the CGI-S.
The Revised Child Anxiety and Depression Scale (RCADS-25) is a 25-item parent report measure of anxiety and depressive symptoms (37). Items are rated on a four-point Likert-scale from 0 (never) to 3 (always). It yields three scores: Total Anxiety, Total Depression, and Total Anxiety and Depression. Parents were asked to rate items based on when their child’s symptoms were at their worst.
All study procedures were approved by the Lifespan Institutional Review Board. Data collection tooks place between September 2020 and March 2022.
Prior to formally recruiting participants for this study, we piloted the focus group-based process mapping methods to be used for this study (described below), as part of an existing advisory group meeting for the Improving Access to Child Anxiety Treatment (IMPACT study; PCORI/IHS-2017C1-6,400). The IMPACT study is an ongoing comparative effectiveness trial that is comparing different delivery methods for exposure therapy. The IMPACT patient and family advisory group is comprised of 12 participants, all of whom were invited by email to attend an advisory group meeting specifically focused on accessing exposure therapy. Five of the advisory group participants indicated interest, and four attended the focus group. One of these participants was a former (now adult) patient; the remainder were parents. Participants completed the Demographics Questionnaire prior to the focus group, which took place via Zoom in September 2020.
After piloting the process mapping methods with the existing advisory group, we recruited additional participants to attend focus groups and complete online questionnaires as part of the accessing exposure (ACE) study. We used several methods to recruit participants including: (1) sending emails and providing fliers to therapists who provide exposure therapy through the Pediatric Anxiety Research Center (PARC) outpatient clinic and through PARC training studies and asking them to share the study information with patients’ parents who might be interested in participating; (2) posting fliers in clinical space at Bradley Hospital; (3) posting to OCD Rhode Island social media channels; (4) contacting participants who previously completed other PARC studies and who consented to be contacted in the future for other studies conducted through PARC; and (5) asking participants to forward information about the study to parents they knew whose children have also completed exposure therapy.
Parents interested in participating in the study first completed an online study interest form via REDCap, a secure, web-based software platform designed to support data collection for research studies (38, 39). Parents then received a link to complete an electronic consent form followed by online questionnaires, which took about 15–30 min to complete. Following completion of quantitative measures, participants were scheduled to attend a focus group via Zoom. One family had two parents attend the focus group, and the remainder only had one parent per family attend. After the focus group, participants received payment (a $50 Amazon gift card) by email. Recruitment was ongoing until saturation was reached (i.e., data from additional participants did not provide new information), leading to a sample of 18 ACE study participants across six focus groups between August 2021 and March 2022. Together with the pilot focus group participants, this yielded a final study sample of 23 participants across seven focus groups between September 2020 and March 2022.
Focus groups took place online via Zoom. Meetings lasted 60–90 min and were audio recorded. Meetings took place with 2–5 parents, except for one parent who met with us individually due to scheduling constraints. Each group was led by a licensed clinical psychologist (HEF) with facilitation assistance from a trained research assistant (GC). In addition, GC took extensive field notes during each group, which were later reviewed as part of the data analytic process. The meeting agenda for each focus group included: (1) introductions of all participants and study team members; (2) a brief overview of the method and purpose of process mapping; (3) a thought exercise during which parents were given 2-min to think about their experiences and the process that they went through to access exposure therapy for their child; and (4) guided discussion of parents’ experience accessing exposure with a simultaneous display of process mapping in real time via screen share.
Focus groups followed a structured approach based on process mapping (i.e., collecting information on specific processes related to identifying and scheduling an appointment with an exposure therapist). Parents were told that they would be asked to describe the process from (a) when they made an initial attempt to seek therapy services for their child until; (b) their child began exposure therapy with a trained therapist. Specifically, we inquired about who parents initially contacted when they decided they needed treatment for their child’s anxiety and the process of seeking and following up on referrals to therapists. Parents were encouraged to provide information about what steps they followed at each stage of their search process, including who they talked to and how successful they were in finding appropriate treatment at each step along the way. As parents shared information about the steps they followed, a process map was created and screen shared in real time using Lucidchart, an online software program that allows for easy creation of diagrams and flowcharts (40). The process map displayed the combined experiences of all parents participating in each focus group. During the focus group, parents were asked to confirm whether the process map reflected the information they were sharing, including decision points and problems (e.g., gaps, uncertainties, and bottlenecks) that occurred at each step. After each group, we drafted a refined, electronic version of the process map using Lucidchart that incorporated data from their group and all previous groups (i.e., a common features process map). This common features process map included elements that were common or similar across families. Saturation was reached when no new process steps were identified. Within 1 week of each focus group, we distributed the common features process map via email to participants for their input and confirmation that it accurately represented their family’s process. No parents suggested any changes to the process map in response to these email requests.
After the completion of all focus groups, data analysis took place in three steps. Analyses were guided by participants’ experiences and themes that emerged based on what they described during focus groups. First, the first and second author (HEF and GC) reviewed field notes and the common features process map to ensure that all key steps of the process were represented. This review of notes was also used to ensure inclusion of all relevant “clouds” (i.e., gaps, bottlenecks, and uncertainties) on the process map. Using information from the common features process map and the field notes, HEF and GC created a table that expanded upon “cloud” descriptions by providing examples from the field notes. Using the field notes as a reference point, sections of the focus group audio recordings were reviewed to select representative quotes for each cloud. A visual review of the map alongside the notes also highlighted multiple “loops” that were commonly described by parents in the process of seeking treatment. HEF and GC identified these loops through discussion and consensus.
Second, HEF and GC conducted an inductive content analysis of all field notes to identify whether additional themes emerged that were not reflected in the “clouds” or “loops.” Then, they organized all themes, including emergent themes from field notes, as well as themes represented in “clouds” and “loops” via Lucidspark, an online software for collaborative ideation and consensus-reaching. This allowed for collaborative grouping of similar themes into larger groups, yielding a total of six overarching themes for the entire dataset.
Third, in June 2022, all participants were sent an updated version of the common features process map, as well as a description of the identified “clouds” and loops for member checking. Parents were asked to confirm whether their experience was reflected in the map and whether there was anything that was wrong or missing from the materials. One parent replied with detailed feedback, and we made revisions based on that feedback. Twelve parents replied saying that they did not have any edits and the map and tables reflected their experiences.
Participants included 22 parents and one former patient from 22 families. Most families had one parent attend the focus groups with two exceptions. There was one couple that attended together whose child had received exposure therapy, and another participant was a young adult who had received exposure therapy as a child. Responses to the RCADS and CGI-S-P indicated variability in severity of children’s anxiety and OCD symptoms at their worst. Participant demographics are shown in Table 1.
Table 1. Participant demographics (N = 23).1
The process map that emerged from our discussion with participants is shown in Figure 1. In Table 2, we describe the numbered “clouds” that appear in the process map, which represent gaps, bottlenecks, and uncertainties that occurred during the process of seeking treatment. This table also provides illustrative quotes from parents. Findings in Table 2 highlight challenges across each phase of seeking treatment—from initially looking for a therapist to starting therapy with a non-exposure therapist to eventually starting treatment with an exposure therapist. Personal connections and word-of-mouth were commonly cited as ways that parents found providers more quickly. Parents highlighted how structural barriers, such as waitlists, geographical location, and type of insurance accepted had an impact at multiple stages in the treatment-seeking process, including when they were first looking for the name of a therapist and when they found a therapist and initiated treatment. Parents frequently described “begging and pleading” (3703) to get into treatment, especially if they had been looking for a long time and their child’s symptoms were worsening. This resulted in emotional distress for parents, as well as initial willingness to stretch the family’s financial and other resources to initiate therapy (e.g., paying high out of pocket costs, traveling long distances). However, maintaining engagement in therapy that was expensive or geographically distant was often not sustainable or increased stress on the family system. In addition, when an initial course of treatment ended, parents cited difficulty re-engaging in treatment with the same or a new provider due to many of the same obstacles they faced when first seeking treatment.
Figure 1. Final combined process map. Detailed descriptions of red clouds are provided in Table 2. Consistent with Kim and colleagues (31), each shape connotes a different type of step in the process: (a) Circles represent a process' start and end points; (b) Arrows between shapes depict the sequence in which events occur; (c) Rectangles indicate events that took place in the process; (d) Diamonds represent decision points in the process; and (e) Cloud shapes (referred to as "kapowies" during focus groups) represent uncertainties, gaps, bottlenecks, or inefficiencies. Loops are identified by different pattern lines: (a) the medical loop is represented by dashes and dots; (b) the search-outreach loop is represented by dashes; and (c) the parent research loop is represented by small dots.
Table 2. Description of process map “clouds”—Uncertainties, gaps, and bottlenecks.
Given the timing of data collection for this study (2020–2022), some parents mentioned the impact of COVID-19 on treatment seeking. In particular, parents described mixed reactions to the emergence of telehealth as a primary mode for treatment delivery during the pandemic. Some parents reported that it improved access to treatment by increasing ease of scheduling and reducing transportation barriers. Other participants identified challenges related to higher reliance on parents to conduct exposures rather than having a therapist guide the child through exposures in vivo. Another telehealth-related challenge was difficulty building rapport via Zoom, especially for youth with social anxiety.
In addition to the barriers to treatment seeking highlighted in Table 2, the process map contains three “loops” or stuck points that emerged. These loops are described in Table 3. First, participants identified a “search-outreach loop,” in which they repeated the cycle of looking for therapists, contacting them, and being unable to schedule an appointment due to factors such as cost, waitlists, and travel time. Second, parents identified a “medical loop” that involved repeated visits to their pediatrician or other medical provider to receive input on ways to manage anxiety/OCD symptoms. This was particularly salient among parents whose children had symptoms that required treatment by medical providers, though many parents whose children did not have medical symptoms also endorsed frequent visits to the pediatrician to seek help related to anxiety symptoms. Several participants reported that their child’s pediatrician was a source of constant support and guidance through the treatment seeking process. However, other parents expressed frustration with pediatricians and medical specialists not having sufficient knowledge or resources to support them.
Table 3. Loops.
Finally, there was a “parent research loop” that involved parents doing their own research into anxiety and OCD treatment after not receiving clear guidance from medical providers and/or therapists. Some parents mentioned that they had also sought counseling for their child through school, but that it was not sufficient to address ongoing symptoms. In response to these failed attempts at seeking adequate treatment for anxiety and OCD, several parents described efforts to do online research and to make calls to local clinics and hospitals about what treatments might work for their child. They often noted confusion about their child’s diagnosis and the use of online research to gain a better understanding of their child’s symptoms [e.g., morality OCD, Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS)]. The role of diagnostic confusion was particularly pronounced for children with OCD caused by PANDAS. This is likely due to the relative rarity of PANDAS (41) and many providers’ lack of familiarity with this etiology. Parents differed in their experiences with PANDAS, where some said that assessment for PANDAS was a distraction, whereas other expressed frustration that an immune-related etiology was not consider by pediatricians. Many parents learned about diagnoses and exposure therapy through their own research, which allowed them to engage in a more directed search for their child’s treatment.
Finally, Table 4 describes the six overarching themes that emerged based on parents’ descriptions of the process of seeking treatment. These themes were derived from focus group notes and the process map itself, and include: (1) resources and terminology related to exposure therapy, (2) identifying diagnoses to guide treatment, (3) parent-related factors in treatment-seeking, (4) child-related factors that drive treatment seeking, (5) the role of medical providers, and (6) structural and social barriers to accessing care. In terms of resources and terminology related to exposure, parents described confusion about the variety of terms used to describe psychological treatments for anxiety disorders. After having received exposure therapy for his child, one parent said, “I keep hearing CBT but honestly, I do not even know what CBT means, what it stands for” (4006). Parents also talked about the importance of identifying diagnoses to guide their next steps for treatment. One participant noted, “I called one of my close friends who works with children and adults with OCD… [she] talked through it with me how OCD and tics are often overlapping and connected. That was really helpful” (8606). This parent went on to describe how understanding that OCD might be a part of the diagnostic picture led her to finding an appropriate provider. In the process leading up to finding treatment for their children, parents described many intense emotional reactions of their own that added to the challenge of seeking treatment. One parent said, “When you go through it [seeing your child in distress and not being able to help] every day, it’s torture” (1606). Child-related factors also affected the treatment seeking process. For instance, some parents described finding a therapist, but not being able to engage their child in treatment: “[The pediatrician] gave us a list of therapists to reach out to. We did try for about 3 months. [Child] would refuse to participate. He did not speak. We just sat there…” (5105). Medical providers, particularly primary care physicians and pediatricians, were frequently mentioned as the first places families went to get information to help their child. However, there was also acknowledgement that medical providers rarely receive specialized mental health training, particularly related to OCD. As stated by one parent, “There is not a single OCD CME [continuing medical education] out there, so if you are trying to target primary care providers as a way to get in, there is nothing out there” (3703). Finally, parents identified that there are many structural barriers related to accessing care, and how many of them had the social capital (e.g., colleagues in the mental health system) to help them access treatment. One parent described, “I think about other parents out there that aren’t educated [about mental health] or do not have resources or really good health insurance… there was no person stepping into our life helping us. That’s really scary for people who do not have all the resources to get the help” (1505). Many parents identified feeling lucky to have the resources available to seek treatment at a high financial or logistical cost even if it was a burden on their families.
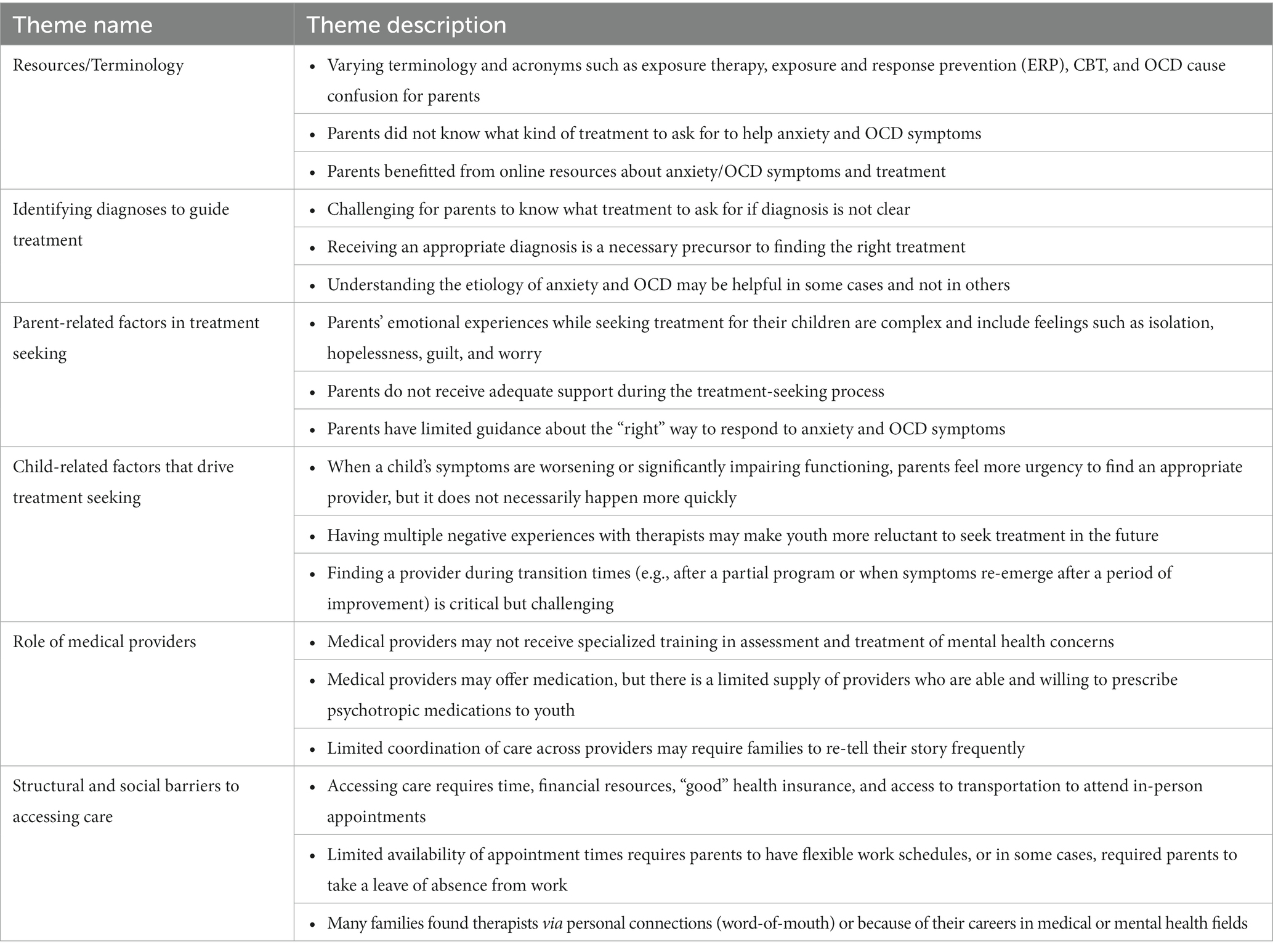
Table 4. Emergent themes.
In addition, parents emphasized how helpful the focus groups themselves were, noting that the opportunity to talk to other parents was a valuable one. One parent said, “I would have paid a million dollars to talk to you all 3 years ago… this is priceless to be able to [talk to other parents]. Hearing your stories is validating because going through it you are trying to do the best thing, but you have no idea what that is” (1606). Another parent said, “I have not had the opportunity to talk to others about this ‘cause family and friends do not know about it or understand” (1105). Parents identified that having more support from friends, family, and/or medical providers during the treatment and treatment-seeking process would have improved their ability to support their child and had a positive impact on their own mental health. This is consistent with the finding that the process of seeking treatment brought up many negative emotions for parents, including isolation, guilt, and helplessness.
This study examined parents’ experiences accessing exposure therapy for their children. Parents participated in focus groups that used process mapping to guide conversations about their experiences accessing treatment. This approach allowed for parents and researchers to visualize the barriers and facilitators faced during this process and to identify stuck points to target in future implementation efforts. Results from this study indicate that parents seeking treatment for their children found themselves caught in “loops” (i.e., a “search and outreach loop,” a “medical loop,” and a “parent research loop”) in which they engaged in repeated process steps due to the emergence of barriers. In addition, parents reported feeling reliant on guidance from pediatricians and word-of-mouth recommendations from their personal networks to gain information about treatment options. Furthermore, parents reported feelings of isolation and guilt caused by the burden of finding treatment for their children with limited support.
The three “loops” identified in the process map represent the biggest stuck-points parents faced during treatment-seeking given that the barriers maintaining these loops persisted in the face of multiple attempts by parents to bypass them. Hence, these parent-identified loops highlight clear areas for future implementation efforts. The “search and outreach loop,” in which parents repeatedly received information about potential therapists but were unable to start treatment, was maintained through logistical barriers that have been identified in prior research [(e.g., 27)]. These include parents’ lack of access to up-to-date information about available providers, long waitlists, high costs, and few providers who accept insurance. As a result, parents reported significant time and financial resources being dedicated to the search for a therapist for their child. To address the barriers maintaining the search and outreach loop, potential implementation efforts may focus on encouraging insurance companies to provide more up-to-date information about available providers, disseminating information about exposure to school-based providers, and increasing the availability of lower intensity interventions like phone consultations or single session interventions (42) that provide psychoeducation and tools for managing symptoms. The last column of Table 3 shows additional recommendations generated by participants and researchers for addressing this and other loops.
The second major loop was a “medical loop,” which involved frequently re-engaging with medical providers to manage anxiety-related medical symptoms. For some youth, the medical loop led to medical intervention (e.g., antibiotics to treat PANDAS; weight restoration) while for others it ultimately led to the discovery that symptoms were somatic (e.g., gastrointestinal distress caused by anxiety). Parents whose children required medical intervention noted that better coordination among medical and mental health providers [e.g., via integrated care teams; (43)] would have reduced their need to repeatedly explain their story and seek help from multiple providers. To address delays in obtaining an accurate diagnosis for medical symptoms that are secondary to anxiety, parents advocated for an increased focus on educating medical providers (primary care physicians and specialists) about anxiety, OCD, and exposure therapy. This may involve increased dissemination of information about identification of and recommended treatments for pediatric anxiety disorders and OCD, as well as additional training opportunities for medical providers. These results also further highlight parents’ interest in models that promote the integration of behavioral health services into primary care settings, which have shown promise for their effectiveness (44).
Finally, the “parent research loop,” in which parents and sometimes adolescents did their own research into symptoms and possible treatment options, was maintained by the limited available information about symptom presentations of and EBIs for anxiety and OCD. Parents reported feeling guilty about their lack of knowledge and inability to find a suitable provider, which motivated them to engage in their own research. Parents also emphasized the difficulty of navigating the mental health system; many reported that it took years to find an exposure therapist. One strategy to reduce time that parents spend in this loop is to disseminate information in a cohesive and user-centered manner such that parents can easily learn about EBIs and use this information to request their desired treatment by name. This is in line with calls for direct-to-consumer marketing as a strategy to increase provider use of EBIs for anxiety disorders (45). Parents also expressed a strong interest in family support groups in which families who have already accessed treatment advise families going through the process. Warmlines—confidential and often free peer-support lines staffed by volunteers (46)—may offer a personalized peer-guidance option for parents. Warmlines may be particularly helpful given that they may address both the “search and outreach cycle” and the “parent research loop” by providing emotional and logistical support during the treatment-seeking process.
An overarching emotion that arose repeatedly in focus groups was the presence of confusion throughout the treatment seeking process. Specifically, parents endorsed ongoing diagnostic uncertainty and confusion about what EBIs for anxiety and OCD entail, which in turn brought about feelings of guilt, hopelessness, and worry. A particularly consequential finding in this study was that multiple parents expressed confusion about what treatment to ask for due to the number of terms used to describe EBIs for anxiety and OCD (e.g., exposure therapy, ERP, and CBT). Other parents who felt confident about the meaning of relevant terms expressed frustration and uncertainty about how to ensure their child’s provider was really offering the treatment they advertised (e.g., providers delivering CBT but not doing exposure). These findings further highlight the need for increased dissemination about EBIs for anxiety and OCD to parents to increase demand, as well as increased training and consultation for therapy providers. It also underscores the importance of considering the end-user, or consumer, of EBIs when it comes to intervention development and implementation (47). Related to this, efforts to “rebrand” exposure should consider terminology that will be more intuitive and less confusing to parents and families (48).
One theme that has relevance to all of the identified “loops” is the role of medical providers. One concern was that physicians do not have adequate training to diagnose or determine effective treatments for mental health disorders. Indeed, prior research suggests that pediatricians may not be well trained in recognizing mental health disorders, including OCD (5, 49). However, parents’ distress about mental health symptoms during primary care visits may increase provider recognition of mental health disorders (49). Although this highlights the importance of advocating for their children, some parents reported that their child’s anxiety or OCD symptoms were dismissed by medical providers. This is in line with past research suggesting that supportiveness or dismissiveness from professionals is a determinant to accessing treatment (27). At the same time, physicians face significant barriers to providing parents with mental health support. A systematic review found that pediatricians identified low confidence and knowledge about mental health, limited time, low reimbursement, and lack of resources as the biggest barriers to recognition of mental health problems in their youth patients (50). Furthermore, barriers to pediatricians making referrals to specialist services are similar to those faced by parents and include lack of providers and resources, waiting times, and insurance coverage (50). These findings indicate that even if pediatricians have the knowledge to identify mental health symptoms, healthcare system barriers prevent them from making referrals that parents find helpful. Ultimately, in addition to pediatricians’ understanding of mental health disorders, their perceptions of parents and their own access to resources (e.g., a referral database) impact their clinical decisions. Additional research is needed to assess physicians’ perspectives related to providing mental health assessment and referrals, which can guide the development of implementation strategies to address this area of need.
As noted above, implementing integrated behavioral health services in primary care physicians’ offices is one strategy to address barriers related to communication between physicians and therapists (43). For instance, integrated behavioral health providers (therapists) can provide consultation directly to primary care physicians about mental health assessment. In addition, this model supports consultation to patients via “warm handoffs” from physicians to behavioral health providers, as well as increased coordination of care between medical providers and behavioral health providers. The ability to receive brief behavioral health interventions in primary care physicians’ offices addresses barriers of finding an appropriate provider and reduces the number of times families must retell their story and start over with a new provider. In addition, by providing services within a clinic where the family is already accessing care, it is likely to reduce structural barriers such as treatment costs and transportation. Although there are some families for whom the brief care provided in primary care offices will not be sufficient, integrated behavioral health providers tend to be well positioned to provide appropriate community referrals.
Study participants identified several equity considerations that warrant further consideration in efforts to improve access to care for youth. Parents’ concerns are consistent with the literature on disparities to accessing treatment, particularly among youth who are minoritized and underserved. For instance, previous research indicates that Black and Latinx youth are significantly less likely to receive needed mental health treatment compared to White youth (51–53). Race and ethnicity were not explicitly mentioned by parents during focus groups; however, inclusion criteria for this study required that families received exposure therapy. The relatively low rates of racial/ethnic minoritized participants in this study may in part reflect the fact that fewer racial/ethnic minoritized youth access effective therapy due to a range of socio-ecological factors (54, 55).
Sociodemographic variables, including poverty, have also been demonstrated to predict patterns of service use, with lower rates of adequate care for individuals living in high-poverty areas (56, 57). Consistent with Lu and colleagues’ (55) systematic review findings related to the contextual/structural and social/cultural levels of the Social Ecological model, several parents in this study specifically acknowledged that they had the resources to overcome common barriers to accessing mental health treatment. For instance, parents were able to overcome geographical barriers, such as where providers’ offices are located. Multiple parents discussed the need to go out of state for treatment, with at least two parents relocating for a period to access treatment for their children.
Parents identified additional facilitators they experienced, such as having financial or social resources to allow them to follow a path to accessing treatment. For instance, many parents noted that personal or professional connections with providers allowed them to get into treatment more quickly. This parent-reported dependence on their own networks and social capital further showcases how the gap between high-resource and low-resource families is maintained, given that higher income individuals are more likely to have greater health literacy and comfort navigating the medical system (58, 59). Thus, future research examining access to treatment should work to include the perspectives of parents from a range of cultural and socio-economic backgrounds that may not have the social or cultural capital to circumvent barriers. This can inform tailored approaches to addressing barriers to treatment access. For instance, community outreach programs for youth who are underserved and from racial/ethnic minoritized groups may improve social network support and improve word-of-mouth referrals to culturally responsive exposure therapists (55).
Strengths of this study include its focus on obtaining data informed by parents’ perspectives and the novel application of the process mapping approach to obtain detailed information about barriers to accessing mental health treatment. A strength of process mapping itself is its ability to showcase the timing in which a barrier arises during a process and the steps that both precede and follow that barrier. Process mapping is complementary to “group model building” (GMB), a system dynamics-based method in which contributors develop a causal loop diagram that models problems and opportunities for improvement (22, 60). The identification of barriers through process mapping can help inform GMB and causal loop diagrams, which in turn will further improving tailoring of implementation strategies to match determinants (22). Process mapping may be a method particularly well-suited to presenting parents’ and patients’ perspectives, as it allows participants the opportunity to see their story represented visually and to provide feedback and clarifications in real-time.
In addition to these strengths, this study had multiple limitations. Recruitment was geographically restricted to families seeking treatment in Rhode Island and Massachusetts; thus, participants may have experienced barriers or facilitators to treatment access specific to New England. Additionally, we had some difficulty scheduling participants due to their work schedules. Although we offered a variety of times for focus groups, some parents were unable to predict work schedules in advance to commit to any meeting time. This is a major limitation given that the available participants had the flexibility in their schedules to attend the focus groups, and therefore, likely had similar resources that increased their access to treatment. This limitation was referenced by many participants themselves, who noted that they could not imagine the obstacles faced by parents who had less time and fewer resources. Consequently, this study may also be inherently skewed toward the perspectives of families with greater resources, as we recruited parents who had already accessed exposure therapy for their children. In particular, this sample had a preponderance of White, highly educated parents with relatively high incomes, which does not represent the larger population of people who may seek treatment for mental health concerns. Another limitation of this study is that it focused only on families who successfully received exposure therapy; future research is needed to understand the perspectives of families who have not been able to receive exposure therapy or other types of therapy. Furthermore, except for one former patient, participants in this study were parents. Additional input is needed from youth to understand their perspectives on accessing treatment, including how they perceive the role of their parents in the treatment-seeking and utilization process.
The results of this study, along with its strengths and limitations, highlight future opportunities for research to help tailor implementation strategies to improve access to mental health care. While this study focused specifically on access to exposure therapy for youth with anxiety and OCD, it is likely that process mapping can highlight stuck points requiring intervention for other disorders and their EBIs. Our findings point to several directions for future interventions such as the creation of a streamlined referral process and user-friendly database of available providers, and the development of parent support groups or Warmlines to help families navigate the mental health system. Additional interventions may focus on enhanced coordination of care between medical and mental health providers by testing education programs for pediatricians and by examining collaboration efforts between medical and mental health providers. Future research with parents who are actively in the treatment seeking process could also shed light on the perspectives of more families including those who may not have the resources to readily access treatment. In addition, future research might benefit from explicitly asking parents to identify the relative importance of each barrier to prioritize the barriers that most urgently need to be addressed.
Using process mapping, this study identified determinants to accessing exposure therapy for parents of youth with anxiety and OCD. Findings highlight priority areas to improve access to care, including: (1) lack of clarity regarding diagnosis, treatment, and terminology related to anxiety disorders and OCD; (2) parents’ experience of repeatedly encountering the same barriers during their attempts to access treatment and resultant feelings of guilt, shame, and helplessness; (3) inequitable access to care that relies on parents’ use of their own personal connections, flexible work schedules, and high costs for care; and (4) overreliance on medical providers, and particularly pediatricians, to solve issues related to accessing mental health treatment for anxiety and OCD. Although we specifically inquired about treatment for anxiety and OCD, many of these barriers likely expand to other populations. Future work should identify how barriers to accessing care are similar or different for other presenting problems and underserved populations. Furthermore, in partnership with parents and other key community members, future research should develop dissemination and implementation strategies specifically focused on addressing these barriers to accessing care.
The data presented in this article are not publicly available due to the highly sensitive nature of focus group data and risk of identifying research participants. Requests to access the datasets should be directed to the first author, HEF, aGFubmFoX2ZyYW5rQGJyb3duLmVkdQ==.
The studies involving human participants were reviewed and approved by Rhode Island Hospital Institutional Review Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
HEF, KGB, and BK contributed to the conception and design of the study. HEF, EO’C, JK, and GC participated in the collection of study data. HEF and GC analyzed the study data and wrote the initial draft of the manuscript. HEF, GC, BK, and JF wrote and edited sections of the manuscript. All authors contributed to the article and approved the submitted version.
This work was support by the National Institute of Mental Health [T32MH019927]. The funding source did not have any direct involvement in the study design, data collection, analysis, or writing of this report.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Polanczyk, GV, Salum, GA, Sugaya, LS, Caye, A, and Rohde, LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. (2015) 56:345–65. doi: 10.1111/jcpp.12381
2. Merikangas, KR, He, J-P, Burstein, M, Swendsen, J, Avenevoli, S, Case, B, et al. Service utilization for lifetime mental disorders in US adolescents: results of the National Comorbidity Survey–Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. (2011) 50:32–45. doi: 10.1016/j.jaac.2010.10.006
3. Levesque, J-F, Harris, MF, and Russell, G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. (2013) 12:18. doi: 10.1186/1475-9276-12-18
4. Katzow, MW, Steinway, C, and Jan, S. Telemedicine and health disparities during COVID-19. Pediatrics. (2020) 146. doi: 10.1542/peds.2020-1586
5. Glazier, K, Swing, M, and McGinn, LK. Half of obsessive-compulsive disorder cases misdiagnosed: vignette-based survey of primary care physicians. J Clin Psychiatry. (2015) 76:e761–7. doi: 10.4088/JCP.14m09110
6. Becker, SJ, Helseth, SA, Tavares, TL, Squires, DD, Clark, MA, Zeithaml, VA, et al. User-informed marketing versus standard description to drive demand for evidence-based therapy: a randomized controlled trial. Am Psychol. (2020) 75:1038–51. doi: 10.1037/amp0000635
7. Harned, MS, Dimeff, LA, Woodcock, EA, and Contreras, I. Predicting adoption of exposure therapy in a randomized controlled dissemination trial. J Anxiety Disord. (2013) 27:754–62. doi: 10.1016/j.janxdis.2013.02.006
8. Morris, ZS, Wooding, S, and Grant, J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. (2011) 104:510–20. doi: 10.1258/jrsm.2011.110180
9. Reid, AM, Bolshakova, MI, Guzick, AG, Fernandez, AG, Striley, CW, Geffken, GR, et al. Common barriers to the dissemination of exposure therapy for youth with anxiety disorders. Community Ment Health J. (2017) 53:432–7. doi: 10.1007/s10597-017-0108-9
10. Higa-McMillan, CK, Francis, SE, Rith-Najarian, L, and Chorpita, BF. Evidence base update: 50 years of research on treatment for child and adolescent anxiety. J Clin Child Adolesc Psychol. (2016) 45:91–113. doi: 10.1080/15374416.2015.1046177
11. Wolitzky-Taylor, K, Zimmermann, M, Arch, JJ, De Guzman, E, and Lagomasino, I. Has evidence-based psychosocial treatment for anxiety disorders permeated usual care in community mental health settings? Behav Res Ther. (2015) 72:9–17. doi: 10.1016/j.brat.2015.06.010
12. Frank, HE, Becker-Haimes, EM, and Kendall, PC. Therapist-training in evidence-based practices for mental health: A review of training approaches and outcomes. Clin Psychol Sci Pract. (2020) doi: 10.1111/cpsp.12330
13. Allen, KB, Benningfield, M, and Blackford, JU. Childhood anxiety—if we know so much, why are we doing so little? JAMA Psychiat. (2020) 77:887–8. doi: 10.1001/jamapsychiatry.2020.0585
14. Higa-McMillan, CK, Kotte, A, Jackson, D, and Daleiden, EL. Overlapping and non-overlapping practices in usual and evidence-based Care for Youth Anxiety. J Behav Health Serv Res. (2017) 44:684–94. doi: 10.1007/s11414-016-9502-2
15. Kendall, PC, Safford, S, Flannery-Schroeder, E, and Webb, A. Child anxiety treatment: outcomes in adolescence and impact on substance use and depression at 7.4-year follow-up. J Consult Clin Psychol. (2004) 72:276–87. doi: 10.1037/0022-006X.72.2.276
16. Pine, DS, Cohen, P, Gurley, D, Brook, J, and Ma, Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. (1998) 55:56–64. doi: 10.1001/archpsyc.55.1.56
17. Eccles, MP, and Mittman, BS. Welcome to Implementation Science. Implementation Science. (2006) 1:1. doi: 10.1186/1748-5908-1-1
18. Aarons, GA, Hurlburt, M, and Horwitz, SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Adm Policy Ment Health Ment Health Serv Res. (2011) 38:4–23. doi: 10.1007/s10488-010-0327-7
19. Damschroder, LJ, Aron, DC, Keith, RE, Kirsh, SR, Alexander, JA, and Lowery, JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:50. doi: 10.1186/1748-5908-4-50
20. Powell, BJ, Waltz, TJ, Chinman, MJ, Damschroder, LJ, Smith, JL, Matthieu, MM, et al. A refined compilation of implementation strategies: results from the expert recommendations for implementing change (ERIC) project. Implement Sci. (2015) 10:21. doi: 10.1186/s13012-015-0209-1
21. Harrington, NG, and Noar, SM. Reporting standards for studies of tailored interventions. Health Educ Res. (2012) 27:331–42. doi: 10.1093/her/cyr108
22. Powell, BJ, Beidas, RS, Lewis, CC, Aarons, GA, McMillen, JC, Proctor, EK, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. (2017) 44:177–94. doi: 10.1007/s11414-015-9475-6
23. Bickman, L, Heflinger, CA, Northrup, D, Sonnichsen, S, and Schilling, S. Long term outcomes to family caregiver empowerment. J Child Fam Stud. (1998) 7:269–82. doi: 10.1023/A:1022937327049
24. Macdonald, K, Fainman-Adelman, N, Anderson, KK, and Iyer, SN. Pathways to mental health services for young people: a systematic review. Soc Psychiatry Psychiatr Epidemiol. (2018) 53:1005–38. doi: 10.1007/s00127-018-1578-y
25. Sayal, K, Taylor, E, Beecham, J, and Byrne, P. Pathways to care in children at risk of attention-deficit hyperactivity disorder. Br J Psychiatry. (2002) 181:43–8. doi: 10.1192/bjp.181.1.43
26. Wahlin, T, and Deane, F. Discrepancies between parent-and adolescent-perceived problem severity and influences on help seeking from mental health services. Austral New Zealand J Psychiatry. (2012) 46:553–60. doi: 10.1177/0004867412441929
27. Reardon, T, Harvey, K, Baranowska, M, O’Brien, D, Smith, L, and Creswell, C. What do parents perceive are the barriers and facilitators to accessing psychological treatment for mental health problems in children and adolescents? A systematic review of qualitative and quantitative studies. Eur Child Adolesc Psychiatry. (2017) 26:623–47. doi: 10.1007/s00787-016-0930-6
28. Hansen, AS, Telléus, GK, Mohr-Jensen, C, and Lauritsen, MB. Parent-perceived barriers to accessing services for their child’s mental health problems. Child Adolesc Psychiatry Ment Health. (2021) 15:1–11. doi: 10.1186/s13034-021-00357-7
30. Broder-Fingert, S, Qin, S, Goupil, J, Rosenberg, J, Augustyn, M, Blum, N, et al. A mixed-methods process evaluation of family navigation implementation for autism spectrum disorder. Autism. (2019) 23:1288–99. doi: 10.1177/1362361318808460
31. Kim, B, McCullough, MB, Simmons, MM, Bolton, RE, Hyde, J, Drainoni, ML, et al. A novel application of process mapping in a criminal justice setting to examine implementation of peer support for veterans leaving incarceration. Health Justice. (2019) 7:3. doi: 10.1186/s40352-019-0085-x
32. Antonacci, G, Reed, JE, Lennox, L, and Barlow, J. The use of process mapping in healthcare quality improvement projects. Health Serv Manag Res. (2018) 31:74–84. doi: 10.1177/0951484818770411
33. Johnson, JK, Farnan, JM, Barach, P, Hesselink, G, Wollersheim, H, Pijnenborg, L, et al. Searching for the missing pieces between the hospital and primary care: mapping the patient process during care transitions. BMJ Qual Saf. (2012) 21:i97–i105. doi: 10.1136/bmjqs-2012-001215
34. McCreight, MS, Rabin, BA, Glasgow, RE, Ayele, RA, Leonard, CA, Gilmartin, HM, et al. Using the practical, robust implementation and sustainability model (PRISM) to qualitatively assess multilevel contextual factors to help plan, implement, evaluate, and disseminate health services programs. Transl Behav Med. (2019) 9:1002–11. doi: 10.1093/tbm/ibz085
35. Wolitzky-Taylor, K, Chung, B, Bearman, SK, Arch, J, Grossman, J, Fenwick, K, et al. Stakeholder perceptions of the barriers to receiving and delivering exposure-based cognitive behavioral therapy for anxiety disorders in adult community mental health settings. Community Ment Health J. (2019) 55:83–99. doi: 10.1007/s10597-018-0250-z
36. Guy, W. Clinical global impressions In:. ECDEU Asessment Manual for Psychopharmacology. National Institute for Mental Health: Rockville, MD. ed. W. Guy (1976). 218–22.
37. Ebesutani, C, Korathu-Larson, P, Nakamura, BJ, Higa-McMillan, C, and Chorpita, B. The revised child anxiety and depression scale 25–parent version: scale development and validation in a school-based and clinical sample. Assessment. (2016) 24:712–28. doi: 10.1177/1073191115627012
38. Harris, PA, Taylor, R, Thielke, R, Payne, J, Gonzalez, N, and Conde, JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
39. Harris, PA, Taylor, R, Minor, BL, Elliott, V, Fernandez, M, O’Neal, L, et al. REDCap consortium, The REDCap consortium: Building an international community of software partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
40. Faulkner, A. Lucidchart for easy workflow mapping. Ser Rev. (2018) 44:157–62. doi: 10.1080/00987913.2018.1472468
41. Jaspers-Fayer, F, Han, SHJ, Chan, E, McKenney, K, Simpson, A, Boyle, A, et al. Prevalence of acute-onset subtypes in pediatric obsessive-compulsive disorder. J Child Adolesc Psychopharmacol. (2017) 27:332–41. doi: 10.1089/cap.2016.0031
42. Schleider, JL, Dobias, M, Sung, J, Mumper, E, and Mullarkey, MC. Acceptability and utility of an open-access, online single-session intervention platform for adolescent mental health. JMIR Ment Health. (2020) 7:e20513. doi: 10.2196/20513
43. Mautone, JA, Wolk, CB, Cidav, Z, Davis, MF, and Young, JF. Strategic implementation planning for integrated behavioral health services in pediatric primary care. Implement Res Pract. (2021) 2:263348952098755. doi: 10.1177/2633489520987558
44. Asarnow, JR, Rozenman, M, Wiblin, J, and Zeltzer, L. Integrated medical-behavioral care compared with usual primary Care for Child and Adolescent Behavioral Health: a meta-analysis. JAMA Pediatr. (2015) 169:929–37. doi: 10.1001/jamapediatrics.2015.1141
45. Gallo, KP, Comer, JS, and Barlow, DH. Direct-to-consumer marketing of psychological treatments for anxiety disorders. J Anxiety Disord. (2013) 27:793–801. doi: 10.1016/j.janxdis.2013.03.005
46. Dalgin, RS, Maline, S, and Driscoll, P. Sustaining recovery through the night: impact of a peer-run warm line. Psychiatr Rehabil J. (2011) 35:65–8. doi: 10.2975/35.1.2011.65.68
47. Lyon, AR, and Koerner, K. User-centered design for psychosocial intervention development and implementation. Clin Psychol. (2016) 23:180–200. doi: 10.1111/cpsp.12154
48. Becker-Haimes, EM, Stewart, RE, and Frank, HE. It’s all in the name: why exposure therapy could benefit from a new one. Curr Psychol. (2022):1–7. doi: 10.1007/s12144-022-03286-6
49. Sayal, K, and Taylor, E. Detection of child mental health disorders by general practitioners. Br J Gen Pract. (2004) 54:348–52.
50. O'Brien, D, Harvey, K, Howse, J, Reardon, T, and Creswell, C. Barriers to managing child and adolescent mental health problems: a systematic review of primary care practitioners' perceptions. Br J Gen Pract. (2016) 66:e693–707. doi: 10.3399/bjgp16X687061
51. Cummings, JR, Ji, X, Lally, C, and Druss, BG. Racial and ethnic differences in minimally adequate depression care among Medicaid-enrolled youth. J Am Acad Child Adolesc Psychiatry. (2019) 58:128–38. doi: 10.1016/j.jaac.2018.04.025
52. Marrast, L, Himmelstein, DU, and Woolhandler, S. Racial and ethnic disparities in mental health Care for Children and Young Adults:a National Study. Int J Health Serv. (2016) 46:810–24. doi: 10.1177/0020731416662736
53. Rodgers, CRR, Flores, MW, Bassey, O, Augenblick, JM, and Cook, BL. Racial/ethnic disparity trends in Children's mental health care access and expenditures from 2010-2017: disparities remain despite sweeping policy reform. J Am Acad Child Adolesc Psychiatry. (2022) 61:915–25. doi: 10.1016/j.jaac.2021.09.420
54. Castro-Ramirez, F, Al-Suwaidi, M, Garcia, P, Rankin, O, Ricard, JR, and Nock, MK. Racism and poverty are barriers to the treatment of youth mental health concerns. J Clin Child Adolesc Psychol. (2021) 50:534–46. doi: 10.1080/15374416.2021.1941058
55. Lu, W, Todhunter-Reid, A, Mitsdarffer, ML, Muñoz-Laboy, M, Yoon, AS, and Xu, L. Barriers and facilitators for mental health service use among racial/ethnic minority adolescents: a systematic review of literature. Front Public Health. (2021) 9:641605. doi: 10.3389/fpubh.2021.641605
56. Carson, NBLC, and Alegria, M. Social determinants of mental health treatment among Haitian, African American, and white youth in community health centers. J Health Care Poor Underserved. (2010) 21:32–48. doi: 10.1353/hpu.0.0297
57. Santiago, CD, Kaltman, S, and Miranda, J. Poverty and mental health: how do low-income adults and children fare in psychotherapy? J Clin Psychol. (2013) 69:115–26. doi: 10.1002/jclp.21951
58. Griese, L, Berens, EM, Nowak, P, Pelikan, JM, and Schaeffer, D. Challenges in navigating the health care system: development of an instrument measuring navigation health literacy. Int J Environ Res Public Health. (2020) 17. doi: 10.3390/ijerph17165731
59. Rikard, RV, Thompson, MS, McKinney, J, and Beauchamp, A. Examining health literacy disparities in the United States: a third look at the National Assessment of adult literacy (NAAL). BMC Public Health. (2016) 16:975. doi: 10.1186/s12889-016-3621-9
60. Muttalib, F, Ballard, E, Langton, J, Malone, S, Fonseca, Y, Hansmann, A, et al. Application of systems dynamics and group model building to identify barriers and facilitators to acute care delivery in a resource limited setting. BMC Health Serv Res. (2021) 21:1–10. doi: 10.1186/s12913-020-06014-7
Keywords: exposure therapy, anxiety, obsessive-compulsive disorder, dissemination, treatment access, qualitative, parents
Citation: Frank HE, Cain G, Freeman J, Benito KG, O’Connor E, Kemp J and Kim B (2023) Parent-identified barriers to accessing exposure therapy: A qualitative study using process mapping. Front. Psychiatry. 14:1068255. doi: 10.3389/fpsyt.2023.1068255
Edited by:
Juventino Hernandez Rodriguez, The University of Texas Rio Grande Valley, United StatesReviewed by:
Danielle Adams, Washington University in St. Louis, United StatesCopyright © 2023 Frank, Cain, Freeman, Benito, O’Connor, Kemp and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hannah E. Frank, SGFubmFoX2ZyYW5rQGJyb3duLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.