
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 01 March 2023
Sec. Anxiety and Stress Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1067047
This article is part of the Research TopicImplementation of Evidence-Based Treatments for Child Anxiety and Related Disorders Across Diverse ContextsView all 8 articles
 Philip C. Kendall*
Philip C. Kendall* Julia S. NeyColleen A. MaxwellKyler R. LehrbachRafaella J. Jakubovic
Julia S. NeyColleen A. MaxwellKyler R. LehrbachRafaella J. Jakubovic Dominique S. McKnightAbbey L. Friedman
Dominique S. McKnightAbbey L. Friedman Anxiety disorders are common in youth, associated with impairments in daily functioning, and often persist into adulthood when untreated. Cognitive behavioral therapy (CBT) for youth anxiety is a well-established intervention and has been modified to fit several treatment settings. Despite decades of results supporting the efficacy of CBT, there is a large gap in access to this treatment and a need to consider how it can best be administered flexibly to increase uptake and personalization. We first discuss the core components of treatment for CBT through the lens of the Coping Cat treatment. Next, we review the empirical findings regarding adjustments made for CBT for youth anxiety delivered (a) in schools, (b) in community settings, (c) through telehealth, (d) through online computer programs, and (e) by caregivers at home. In each setting, we provide specific suggestions for how to implement CBT with flexibility while maintaining fidelity.
Anxiety disorders are the most common mental health problem for children and adolescents and have been found to be present in nearly 20% of youth (1). Youth anxiety disorders are associated with impairments in daily functioning and typically persist into adulthood when they are associated with the onset of comorbid mental health disorders (2, 3). Cognitive behavioral therapy (CBT) for youth anxiety is a well-established intervention, with meta-analyses concluding that approximately 60% of youth recover following treatment (4). In the past decade, CBT for youth anxiety has been adapted to diverse settings, including schools, community mental health centers, online programs, and telehealth, and has been administered through parent training. CBT for youth anxiety, within an upbeat therapeutic relationship, targets maladaptive anxious thinking to foster adaptive information processing, reduce anxious feelings, and enhance approach behavior (reduce avoidance) using rapport building, psychoeducation, cognitive restructuring, problem-solving, and exposure tasks (with rewards). CBT for youth anxiety can be accomplished using several empirically supported programs, one of which is the Coping Cat. Consistent with reviewer input, we are keeping the report tight with sole reference to the Coping Cat. That said, our suggestions are applicable to CBT in general. The standard protocol for this intervention includes 16 50-min sessions, which cover several key components. We first overview these key components of youth anxiety treatments that may be flexibly adapted and next discuss changes that may be made in different settings to apply CBT for youth anxiety flexibly and with fidelity.
There are treatment manuals that prescribe, with detail, the guidelines for delivering an evidence-based intervention for youth anxiety, and although there is some variability among them, several key components are consistent across those with demonstrated efficacy. Manuals and personalized approaches differ in the specific ways that the intervention is delivered (e.g., interactive activity, psychoeducational game, worksheet), often referred to as the form of the intervention, while the function, or the purpose of a given form is largely consistent across manuals. We have identified key components of evidence-based approaches to treatments for youth anxiety by their function, describe their empirical basis, and provide examples of different forms that they may take to maintain fidelity and be successful.
Therapeutic alliance has been positively, though modestly, associated with treatment outcomes for youth receiving treatment for anxiety (5, 6). Meta-analytic work has identified effect size estimates as 0.10–0.14. The results suggest that the importance of the therapeutic relationship may be stronger in the case of individual interventions, youth with mixed problem presentations, younger children, and treatment-seeking samples (7, 8). Importantly, findings also suggest that the role of the alliance was greater when measured at the beginning of treatment, suggesting that it may be important to start strong with anxious youth (7, 8). Rapport building can take numerous forms. Many youth find comfort easing into the therapeutic process by playing “get to know you” games, while older youth may prefer to simply chat. These practices can be extended throughout therapy by setting aside a few minutes at the end of a session to play a game (not necessarily therapy-related) or watch a YouTube video, with the goal that the client leaves the session feeling positive and connected. This functions as a reward and can reinforce the youth’s engagement in treatment. CBT uses rewards and praise for desired behaviors in therapy and at home. An important feature of youth therapy is the fact that the decision to attend therapy is not solely made by the youth; rather, many youth present to therapy as a result of a caregiver’s desire for treatment. As such, as part of building rapport, it can be useful for therapists to inquire about the youth’s motivation for treatment and validate any ambivalence.
Psychoeducation has been identified as a core component of CBT broadly (9). In the context of youth anxiety, it has been found that the extent to which youth engage in psychoeducational components of treatment positively predicts treatment outcomes (10). The function of psychoeducation is to increase the youth’s knowledge about anxiety, including what it feels/looks like, where it comes from, how it works, how we treat it and dispelling myths about anxiety. In practice, therapists may address the causes of anxiety by teaching the adaptive nature of anxiety. Therapists can normalize day-to-day experiences of anxiety by sharing their own examples, pointing out with the youth’s help different ways that anxiety can be helpful (e.g., stops us from running into traffic), and then discussing ways in which anxiety that gets too high can become unhelpful (e.g., so stressed for a test you can’t study). This conversation allows the therapist to set expectations for treatment: the goal of therapy is not to eliminate anxiety but to be able to cope with anxiety without letting it get in the way. To teach how anxiety works, the cognitive triangle is introduced, with particular emphasis on the connection between the emotion of anxiety and the physical symptoms it produces. Activities can be used to identify the specific physical symptoms that the youth experiences; for example, younger children may enjoy tracing their body and drawing the manifestations of their physical symptoms (e.g., butterflies in the stomach, sweaty hands), while older youth may prefer to use a list of common symptoms to identify which symptoms they feel and at what levels of anxiety they begin to experience them (e.g., shaky hands, heart racing).
Consistent with theory regarding the connection between feelings and thoughts, research on CBT for youth anxiety suggests that the cognitive restructuring component of treatment represents an active feature of change (11). A youth’s level of cognitive development is a factor that determines the relative utility of this component where older youth may derive greater benefit from mastery of these skills, and the benefits may be less for children under the age of ten or who have not yet developed meta-cognition (12). In practice, this process can be taught in three steps: (1) Catch it, (2) Check it, and (3) Change it. The Catch it step refers to the identification of thoughts, particularly when anxious physical symptoms have been detected. Youth who have difficulty distinguishing thoughts from feelings may benefit from filling in thought bubbles above drawings of themselves or others in various anxiety-provoking situations. For younger children, it may be helpful to externalize the idea of thoughts by identifying a character, such as a “worry monster” or a “guard dog,” who may be responsible for these anxious messages. Next, the Check it step involves examining whether the thought may be a cognitive distortion. Youth often benefit from a list of common thinking traps to compare with their thoughts. Youth may want to check if the thought is helpful (versus interfering). If the youth determines that the thought is not helpful or that they are falling into a thinking trap, the third step, Change it, provides an opportunity to respond to that thought with more helpful thoughts. For younger children, this may be framed as arguing back to the worry monster. For older youth, it is important that this step is not simply generating the opposite thought or telling themselves something they do not believe (e.g., I’m going to ace the test, not fail it). Rather, the function of this exercise is to achieve some level of cognitive flexibility by generating more balanced, believable thoughts (e.g., I may get a B or a C on the test but probably won’t fail it).
Conducting exposure tasks is considered the most critical component of CBT for youth anxiety (13, 14). In this context, exposures typically follow a graded approach in which youth, together with their caregivers and therapist, identify feared situations, rank them in terms of difficulty, begin with the easiest situation, and gradually move up the “fear hierarchy” as they progress through treatment. Recent meta-analytic work has demonstrated that across 75 studies of CBT with anxious youth, effect sizes were positively associated with the amount of in-session exposure (15). The field’s understanding of the mechanisms through which exposures affect change continues to advance, with recent findings suggesting that inhibitory learning models can be used to maximize their effectiveness (16). Specifically, this can involve emphasizing the violation of expectancies that occurs in exposure, deepening extinction by conducting exposures to distinct aspects of the feared situation first individually and then simultaneously, removing safety signals from the exposure experience, varying exposure content from week to week and across contexts, and developing retrieval cues to remind them of what they learned in exposures (e.g., holding the same paper clip in exposure practices as in real-life school presentations) (17). In practice, successful exposures can take many forms. Yet, prior to an exposure task, it is important that youth understand the reason for exposures or “challenges.” Metaphors like slowly entering a cold swimming pool can be used to describe the progressive and graded nature of exposure. Additionally, trust between the therapist and the client is important in preparation for this component of treatment. Youth should be positioned “in the driver’s seat” with assurance that they will be asked to do things they do not want to do, but they will not be forced to do anything they are not yet ready to do. In planning exposure tasks, a hierarchy of feared situations with increasing difficulty is created. To develop a hierarchy collaboratively, the therapist and youth (and can include the help of caregivers) set target behaviors that serve as the goals at the top of the hierarchy. The therapist may generate many scenarios that could approximate steps to the identified goal. The youth rank the scenarios and rate their perceived difficulty. The therapist can gain information about how to optimally design exposures by asking follow-up questions throughout this process (e.g., “Would it be easier or harder if…”). Of note, hierarchies are flexible, living documents that are adjusted as treatment progresses. Often, the first exposure identified by the youth is relatively “easy,” which may allow the youth to establish a sense of efficacy and agency when approaching exposure tasks. However, as youth progress through treatment, exposures on the hierarchy are scaffolded or adjusted so that they target moderate and increasing levels of anxiety.
When it comes time to engage in a feared situation, it is important firstly that the youth has agreed to do the task. It is helpful to set a specific and attainable goal for the exposure (e.g., “Talk to the stranger without leaving the room before the 4-minute mark” and not “Do a good job talking to a stranger”). Lastly, it is helpful to ask the youth what they expect to happen in the task so that this can be re-examined afterward, akin to a “behavioral experiment.” Throughout an exposure, the therapist tracks the youth’s distress through the use of a predetermined scale (e.g., 1–10); this information informs any adjustments that may be necessary for the therapist to make. For example, if the youth reports feeling so highly distressed that they anticipate escaping, it may be helpful to make the exposure slightly easier so as to allow the youth to meet the goal (back up but not back down). In the case that it becomes clear that the exposure is too difficult for the child, the therapist can work with the child to adjust the goal mid-exposure (e.g., “Rather than stay for 4 minutes, can you stay for 2?”). This adjustment provides an alternative response to anxious feelings that is not immediate escape, facilitating experiential learning that counters avoidance responses to anxiety. Following an exposure, youth are given an opportunity to assess their efforts, their performance in relation to the objective goal, and the accuracy of their expectations. The exposure task typically provides evidence that the youth was able to cope (e.g., achieve the objective goal) and that the anticipated catastrophe did not occur, violating their expectancy. Therapists provide ample praise, specifically focused on the effort put forth, rather than on a judgment of the outcome.
Psychoeducation (e.g., normalizing anxiety), cognitive restructuring (changing anxious self-talk), and exposure tasks (e.g., behavioral disconfirmations of anticipated catastrophes) are central features of effective CBT, but they can and are implemented in varying ways. Many forms of CBT for youth anxiety include these core components. These treatments have been studied through randomized controlled trials—and they can be implemented flexibly and with complete fidelity outside the research studies. Attention to implementation in other settings (e.g., schools, online, community mental health centers) is particularly important as we consider how to best serve historically underserved populations of youth (e.g., youth living in low-income or rural settings, youth with comorbid mental health or neurodevelopmental concerns) who may be less likely to access specialty clinics. The phrase “flexibility within fidelity” denotes the need to administer treatment personalization while adhering to research-supported protocols (18, 19). Research examining the relationship between treatment integrity (i.e., therapist adherence to protocol and therapist competence) and youth outcomes has demonstrated no link between rigid treatment fidelity and outcomes (20–22). In a recent study examining 51 youth who completed individualized CBT for anxiety, therapist adherence did not influence youth outcomes (23).
One guiding framework offered by Georgiadis et al. (24) identifies the “Who, What, When, Where and Why of Strategic Flexibility,” where the therapists considers (1) who warrants treatment flexibility; (2) what treatment components should be flexibly modified, (3) when flexibility is needed (4) where flexibility is needed, and (5) why flexibility should be applied. We organize our discussion along the lines of “where.” Specifically, we examine what is known about adjusting CBT for youth anxiety in schools, community mental health agencies, telehealth, online programs, and through caregivers at home. Our focus is on flexibility within fidelity across settings, but there are also adaptations that are appropriate for variations among participant youth (e.g., youth with comorbities).
Educational environments are a fruitful setting in which to implement a variety of interventions because they offer the opportunity to reach a broad range of youth, including individuals who may not have otherwise had access to or been knowledgeable about needed services. Interventions in school settings can provide affordable and quality services to youth who come from under-resourced communities or to youth in lower socioeconomic brackets. Further, because youth across all demographics and with a variety of risk and resilience factors attend schools, implementing interventions in this setting can offer the first line of defense in addressing youth with more severe symptomology, especially if they are initially or frequently unable to access other intervention services for a variety of reasons (e.g., income, transportation barriers, knowledge of services, etc.). Research has found that school settings are an effective environment for implementing treatment modalities that address mental health concerns, such as youth anxiety (25). Literature indicates that CBT can be successfully implemented within a school setting (26). More specifically, Coping Cat has been successfully integrated into school settings (27, 28), highlighting the flexibility of the program and its’ ability to be modified with considerations specific to the setting (see Table 1).
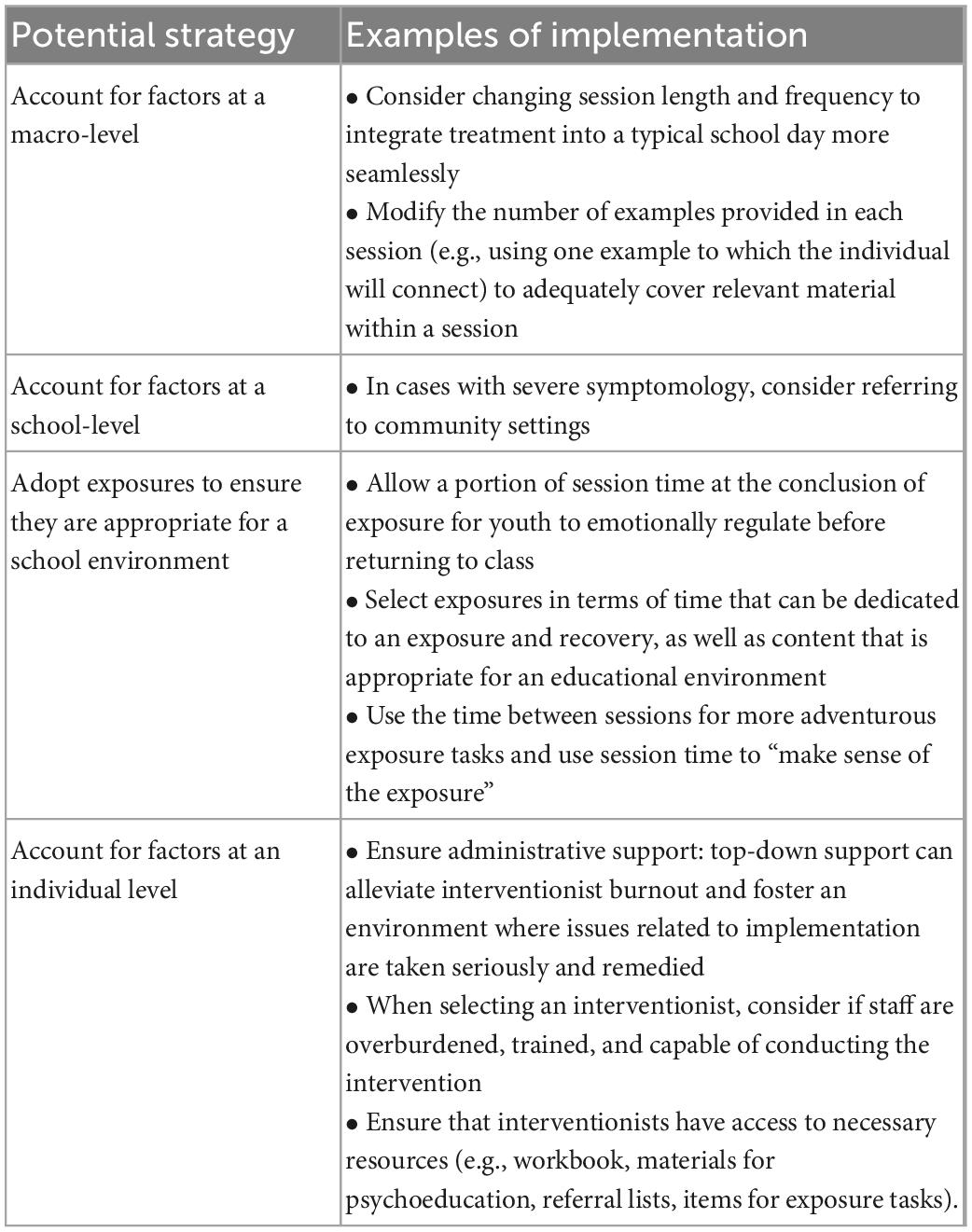
Table 1. Administering CBT for youth anxiety in schools.
There are several considerations for a school setting, in part, due to administrative and contextual issues. Domitrovich et al. (29) offered a framework: consider macro-level factors (e.g., federal, state, and district policies), school-level factors (e.g., climate, resources, decision structure), and individual-level factors (e.g., characteristics of the interventionist, attitudes toward the intervention) and how each of these may interact with the success of an intervention in schools (see Table 1). For example, at a macro-level, state/district policy can influence the allocation of funding and scheduled time to implement an intervention. Typically, the Coping Cat program is designed to accommodate 50-min weekly sessions; however, in schools, it is reasonable to modify session length to fit within a typical school schedule. When assessing the manageability of adapting the Coping Cat program into schools, Mychailyszyn et al. (30) found that it was easiest to devote 30-min sessions up to twice per week, as it more closely mirrors a routine school schedule. Coping Cat allows for flexibility in the breakdown of session information such that sessions can be split into two shorter sessions per week or, if it is not feasible to have more than one session per week, interventionists can select one activity from the session plan (preferably an activity that is expected to be of greatest interest to youth), as opposed to presenting the full gamut of activities related to the session.
A school’s organizational functioning, resources, and climate (reflected by staff impressions of their workplace) merit consideration (29). One potential barrier is implementing key components of the intervention due to constraints within the school. For example, school counselors have expressed concerns related to providing the appropriate “dosage” of the intervention, depending on symptom severity (30). Additionally, school counselors have expressed concern related to conducting exposure tasks within a school. Fortunately, there are opportunities for modifications that help to adapt the Coping Cat program to a school setting (see Table 1). It is encouraged that providers in a school setting be creative when adapting key treatment components. For example, allot time (5–10 min) at the conclusion of an exposure task to allow time for a pleasant activity, facilitating the opportunity for the youth to emotionally regulate prior to returning to class. It may also be wise to schedule longer sessions for the exposure tasks (30). If adapting certain exposure tasks does not seem conducive for a school (e.g., a specific exposure task is indicated and cannot be modified), interventions can be supplemented with outside referrals; for individuals with more severe symptomatology, one can coordinate with community-based referrals (31).
An interventionist’s attitudes (e.g., self-efficacy, experience, and psychological determinants) can contribute to the success of an intervention. In general, more positive attitudes toward the intervention and greater levels of self-efficacy are associated with more successful implementation (29). It is important to foster an environment in which an interventionist feels supported by school administration for decisions about modifying the length of sessions, session content, and appropriate exposure tasks.
Community mental health centers (CMHCs), despite being a widespread source of treatment for youth dealing with anxiety, have historically seldom used CBT to treat youth anxiety. A possible explanation for this hesitancy involves concerns about the practical implementation of efficacious treatment for youth anxiety in community settings, as these settings are often lacking specialized training and support (32). Effectiveness studies evaluate efficacious treatments within real-world settings and are important to determine if treatments have similar levels of success outside of a controlled efficacy study. Initial effectiveness studies investigating CBT treatment of youth anxiety in CMHCs found comparable and beneficial outcomes, but these studies should be interpreted cautiously, given several limitations.
Barrington et al. studied 54 anxious youth treated with CBT and treatment as usual (TAU) in Australia, but only youth participants were randomized, not clinicians (i.e., they used experienced CBT therapists) (33). Southam-Gerow et al. (34) used full randomization in their effectiveness study of 48 youths (i.e., they used therapists employed in community clinics to emulate community settings). Despite its methodological strengths, this study had several limitations, including small sample size (like in Barrington et al.) and non-adherence within the CBT condition. Of youth in the CBT condition, only 52% attended a full 16 sessions, and only 59% participated in exposures, both of which are known to be important and necessary for fidelity and youth outcomes (11, 35, 36) (see Table 2). While the authors noted that some of these limitations could be conceived as a byproduct of how community settings often function, and the CBT outcomes appeared to be comparable to prior efficacy trials, increased fidelity in community settings will inform how to best deliver treatment.
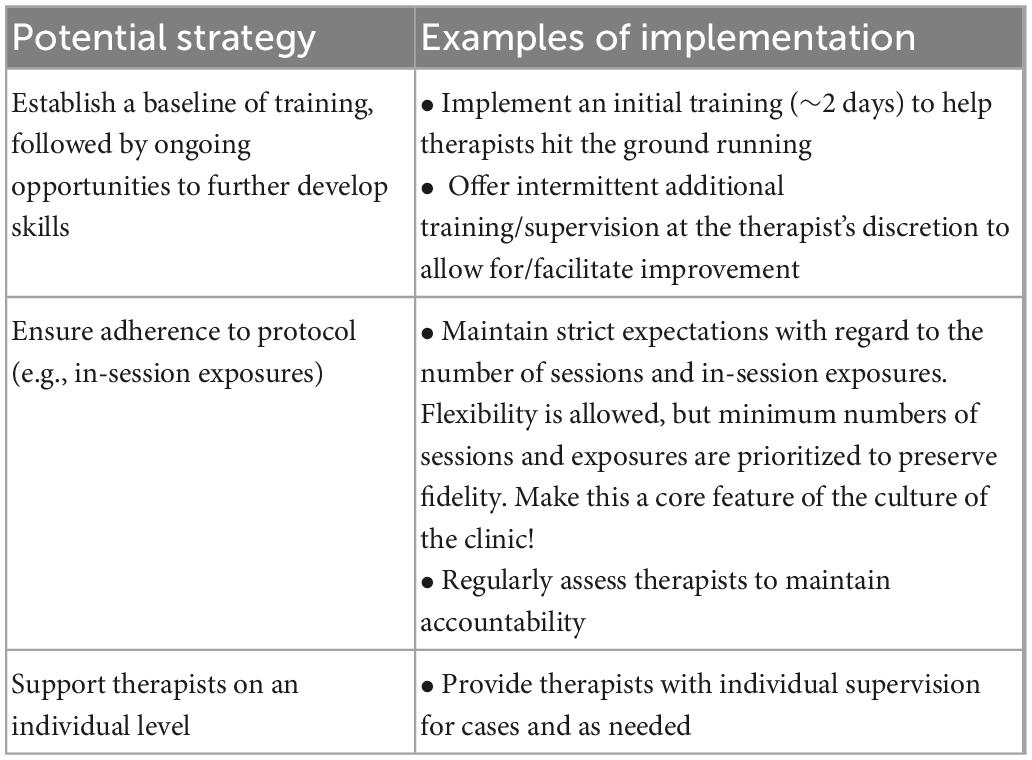
Table 2. Administering CBT for youth anxiety in CMHCs.
A recent effectiveness study (37) exemplified fidelity: a study of 165 anxious youths conducted in CMHCs throughout Norway compared individual CBT (iCBT) and group CBT (gCBT) with a waitlist condition and found similar treatment responses in iCBT and gCBT conditions compared to previous efficacy trials. These findings show that CBT can be effectively delivered by non-specialist therapists lacking previous CBT training. Other research supports this notion of effectiveness, including a 2021 meta-analysis of 58 studies that showed CBT for the treatment of anxious youth in routine clinical care settings had similar outcomes to efficacy studies (38) and a 2020 meta-analysis of 75 studies that underscored the importance of using in-session exposure tasks in community settings (15). With the evidence that CBT of anxiety can be effective when delivered properly, it is imperative that fidelity is maintained in community settings. For instance, ensuring that youth receiving CBT for anxiety meet for the minimum number of sessions and partake in enough exposure tasks (see Table 2).
Research has identified a variety of barriers to fidelity/adherence, which can guide CMHCs’ efforts. Organizational factors influence adherence to evidence-based treatments (39)—one way to address this is by the organization-level implementation of robust initial training, intermittent “booster” trainings, and ongoing assessments of adherence. Even for therapists with little to no experience with CBT, a 2-day workshop and optional boosters provide appropriate scaffolding as a beginning (see Table 2). Another potential barrier to adherence identified by research is the perceived complexity of and variability of clients and presentations. Specific guidance and individualized supervision when implementing CBT can help ensure that each case is treated with personalized flexibility (35, 40) (see Table 2).
Related, there has been several efforts to implement CBT for youth anxiety through pediatric primary care providers (PCPs). PCPs frequently screen for anxiety—in 2022, the U.S. Preventive Services Task Force released recommendations for primary care physicians to conduct anxiety screening in asymptomatic youth from ages 8 to 18 (41). A study examining barriers to implementing psychosocial treatment in primary care found that PCPs ranked the following characteristics of treatments most important: time to employ, applicability to multiple disorders, ease of use, and ease of learning (42). In a pilot study investigating a brief CBT-based anxiety intervention delivered in a behavioral healthcare setting to 25 parent-child dyads (1–4 sessions, 15–30 min in length), pediatricians found the intervention to be feasible to administer, and parents reported reduced child anxiety (43).
Prior to 2020, there were several self-guided and therapist-mediated online computerized CBT programs that had been shown to be effective, but they did not offer the same amount of therapist contact as clinic-based CBT. Before the COVID-19 pandemic, telehealth only accounted for a very small proportion of mental health services (44). However, COVID-19 necessitated clinician use of telehealth to provide access to treatment during the global pandemic. This, in turn, generated clinician creativity in modifying treatment to the telehealth format.
Telehealth is here to stay, as 6 months into the pandemic, 90% of surveyed clinical psychologists anticipated they would continue to use telehealth after the pandemic was over (44, 45). Although there have been limited studies investigating telehealth outcomes of CBT for anxiety in youth, among adults, CBT for anxiety has been found to be similarly effective through telehealth compared to in person (46). Additionally, the therapist-client alliance is an important factor in telehealth. In a study comparing CBT for youth anxiety in a telehealth format compared to an in-person clinic-based format, youth reported no difference in the strength of their therapeutic relationship; however, parents reported slightly higher working alliance with in-person therapy (47).
Our experience conducting CBT for youth anxiety through telehealth during the COVID-19 pandemic has identified strategies to combat technical difficulties, maintain youth attention during sessions, as well as uncover some advantages provided by telehealth (see Table 3). In terms of technical matters, we’ve found that it is best for the client to have sound, video, and their face on the video screen. We also have a plan for what to do if one experiences technical difficulties sorted out ahead of time. We’ve also found that frequent distractions are the rule rather than the exception; a plan to keep distractions—both physical and virtual—to a minimum is best sorted out with the child and caregiver ahead of the session.
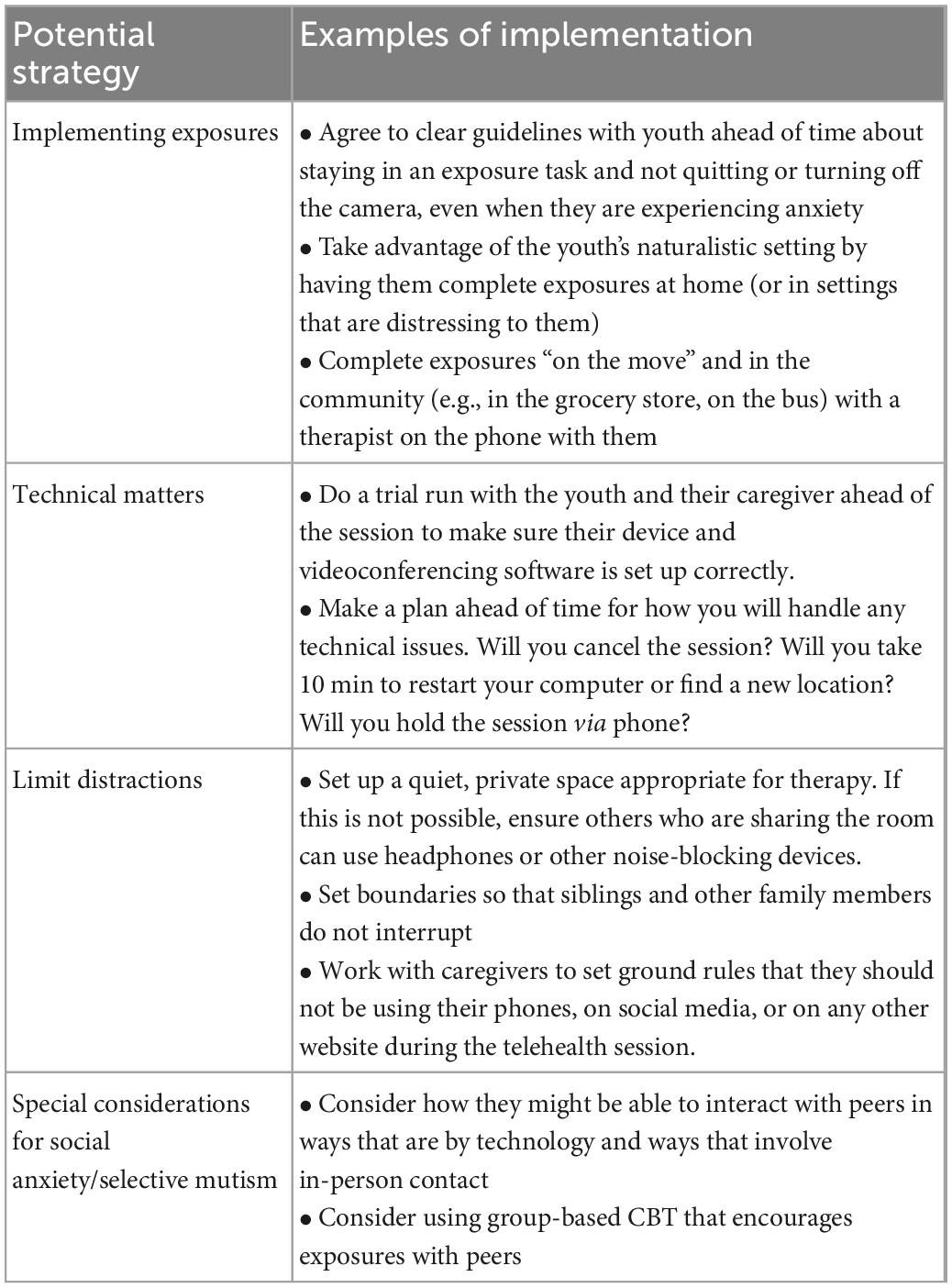
Table 3. Administering CBT for youth anxiety through telehealth.
One of the biggest adjustments in conducting CBT for child anxiety through telehealth is adapting the in-session exposure tasks. Telehealth can provide the opportunity to conduct an exposure within a naturalistic context. For example, the youth bring an electronic device into the real-world exposure setting. This gives a “window into the patient’s own world” (48) and may facilitate the generalizability of the benefit of the exposure. Not only can therapists conduct exposures in a youth’s own home, but a therapist can also consider being on the phone with a client as they conduct an exposure in their community.
Treating youth with social anxiety disorder (SAD) and selective mutism (SM) benefits from special considerations, such as providing opportunities to practice socializing. However, CBT has been successfully delivered in telehealth group-based formats for individuals with SAD and SM (49) (see Table 3). Telehealth can be used to provide CBT in a group format with a group of youth. Although telehealth allows for easier access to groups of individuals with similar difficulties, it also makes it potentially more difficult to complete in-person exposures.
There has been a flourishing of computer- and Internet-based therapy programs geared toward youth. Existing programs that deliver CBT for youth range widely with regard to the platform (e.g., from CD-ROMs to mobile applications), targeted age range (e.g., from preschool through adolescence), degree of customization possible (e.g., in terms of content, pacing, duration), and degree of therapist monitoring and contact (e.g., from “computer-based” programs with no therapist involvement to “computer-assisted” programs with abbreviated, regularly scheduled live sessions). All of these programs have the potential to increase the accessibility of quality mental healthcare for youth while circumventing or reducing common barriers to receiving evidence-based mental health treatment in traditional settings [e.g., limited availability of therapists with training in empirically supported models, therapist and client time constraints, lack of insurance or inability to afford high fees, lack of transportation and/or childcare, the stigma associated with seeing a therapist; (50)]. These benefits may be particularly salient for historically underserved populations of youth, including low-income youth, youth with marginalized identities, and youth residing in rural areas. When possible, we recommend a high degree of customization and flexibility in the mode and frequency of therapist contact to suit the needs of a greater number of youth and families (see Table 4 for specific suggestions).
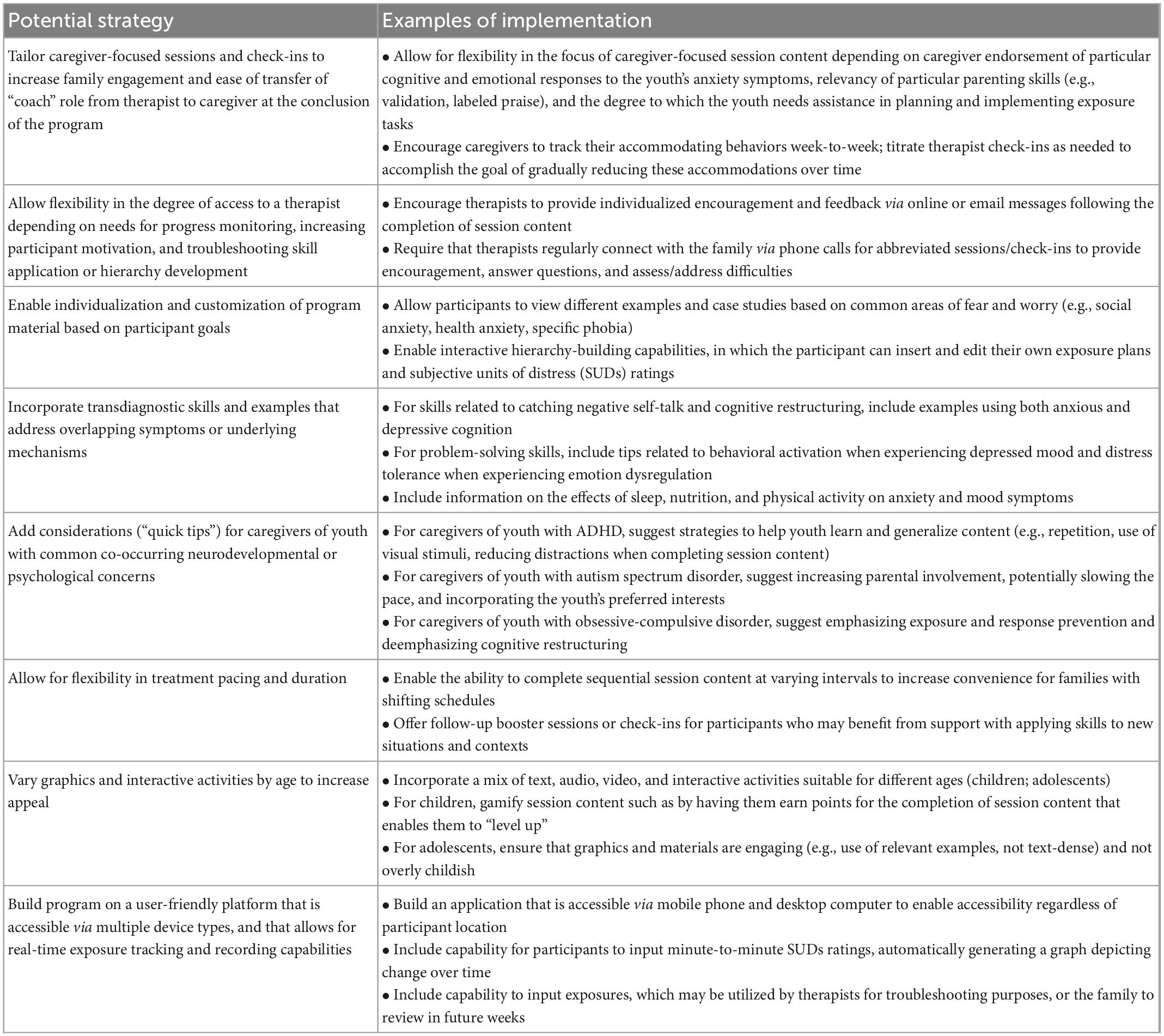
Table 4. Administering CBT for youth anxiety through online computer programs.
Another potential benefit of computerization is greater assurance of fidelity and adherence compared to live therapy, given that at least a portion of online and computer-based program content is systematically delivered (51, 52). However, concerns have been raised regarding the ability of these standardized programs to flexibly address the complex needs of youth and families. We propose ways for online CBT interventions for youth anxiety to facilitate greater flexibility and thus more effectively serve the needs of diverse youth and families. Considerations for increasing flexibility begin when developing program design and capabilities and continue through to roles assigned to therapists or “coaches” (see Table 4). We caution online intervention developers to remain vigilant about issues of fidelity by ensuring that core treatment elements are incorporated in some manner for all participants and, accordingly, encourage incorporating “check-ins” on participants’ experiences throughout the program.
One computer-assisted program for youth with anxiety ages 7–13 is Camp Cope-A-Lot [CCAL; (53)] based on the Coping Cat treatment program (28, 53). The development team included researchers, child psychologists, programmers, and graphic designers, and worked with the goal of creating a program that may be used in settings such as private practices, CMHC, schools, and ultimately in youths’ homes with caregiver assistance (53). Parent input was incorporated in the design of the intervention as well. CCAL is experiential, interactive, and designed to engage youth in middle childhood and early adolescence. In the context of prior research, CCAL included assistance from mental health providers who served as “coaches” for participants, with responsibilities including symptom monitoring, encouraging compliance, and maintaining the integrity of core CBT program elements (51). Of note, several opportunities for flexibility were built into CCAL, including participant ability to customize their own exposure tasks, move through program content at their own pace, and choose between options of theme music and video game rewards. A randomized clinical trial (51) found that both in-person and computer-delivered treatment was effective; there were no statistical differences in gains among youth assigned to CCAL versus those assigned to individual CBT delivered in a traditional manner at both posttreatment and follow-up time points. Both interventions outperformed a computer-assisted education, support, and attention condition. CCAL, as well as Child Anxiety Tales, a web-based program for parents, are now available as online programs (54).
Traditionally, much work in youth anxiety is done in the therapist’s office, but both experience and data attest to the importance of generalizing to the home environment. Participation in and compliance with treatment is best when it continues after leaving the clinic. It is encouraged (e.g., via homework) that children and adolescents continue to work toward treatment goals at home, often with the help of caregivers or others who live with them, for example, through the elimination of accommodations and by practicing exposures.
Accommodations in the home are usually done by caregivers, though others living in the house could also contribute. A common form of accommodation in the home reported by caregivers is changing the child’s or the family’s schedules, routines, or expectations to avoid the child’s discomfort and avoid a possible emotional/behavioral outburst. In a study of 313 parents seeking treatment for their child’s anxiety, it was found that parents who believe accommodation helps maintain behavioral/emotional control accommodate more (55). A study of 73 youths (ages 7–12) quantified these results, showing that reduced accommodation predicted progress in the child overcoming anxiety (56). There are treatments designed specifically for parents that focus on eliminating accommodation in the home (57–59) that were found to be comparably efficacious as individual CBT. Table 5 includes examples of ways caregivers could reduce accommodation in the home. We encourage recommending a reduction or elimination of accommodations in the home to allow for increased mastery or the development of confidence in the child’s abilities to tackle new and challenging situations on their own.
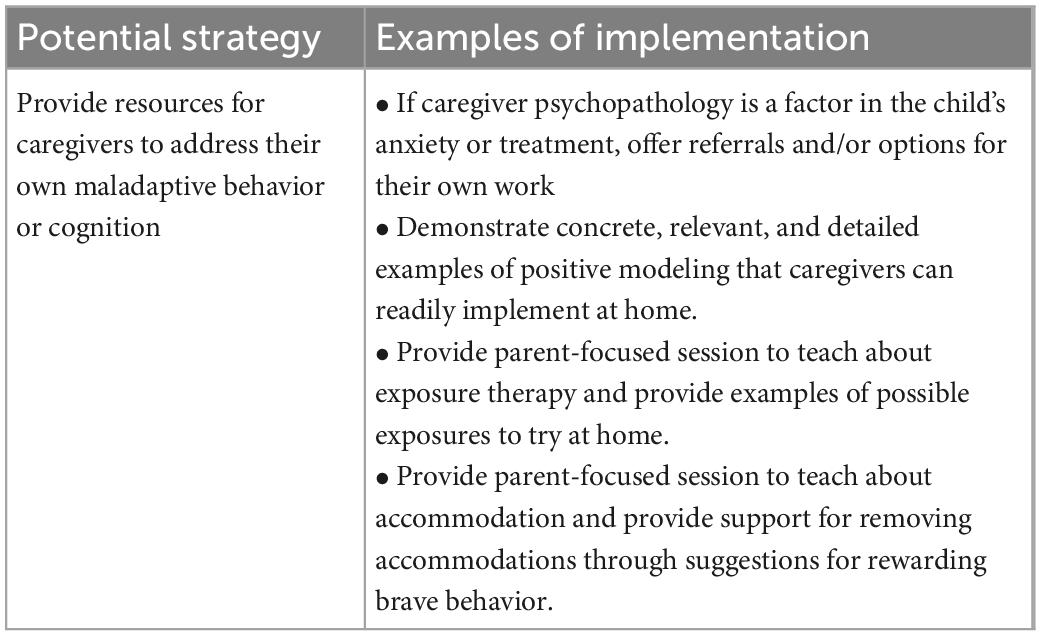
Table 5. Administering CBT for youth anxiety with caregivers.
Some anxious youth may experience less anxiety in the home, where they feel safe and comfortable. This experience is often the case with social anxiety and certain phobias. However, there are also children who experience a great deal of anxiety in the home (e.g., worries about bedtime for those who struggle with separation anxiety or a fear of the dark, worries about home invasions). Exposure tasks are one way therapists generalize treatment to other settings, such as the home. Exposures at home, much like in any other environment, are critical to treating anxiety, and caregiver involvement is necessary for effective youth participation (60). However, parents may want to maintain their role as parents and rely on a professional for treatment (61), creating an obstacle for generalizing treatment to the home. A session dedicated to parental psychoeducation about exposures and how best to implement an exposure at home is helpful (see Table 5) in ensuring treatment is generalized to the home (62).
PK and JN contributed to the conceptualization. All authors contributed to the writing, editing, and approval of the submitted version.
PK receives royalties from the sales of materials related to the treatment of anxiety in youth.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. (2021) 175:1142–50. doi: 10.1001/jamapediatrics.2021.2482
2. Beesdo-Baum K, Knappe S. Developmental epidemiology of anxiety disorders. Child Adolesc Psychiatr Clin. (2012) 21:457–78. doi: 10.1016/j.chc.2012.05.001
3. Swan AJ, Kendall PC. Fear and missing out: youth anxiety and functional outcomes. Clin Psychol. (2016) 23:417. doi: 10.1111/cpsp.12169
4. Warwick H, Reardon T, Cooper P, Murayama K, Reynolds S, Wilson C, et al. Complete recovery from anxiety disorders following cognitive behavior therapy in children and adolescents: a meta-analysis. Clin Psychol Rev. (2017) 52:77–91. doi: 10.1016/j.cpr.2016.12.002
5. Cummings CM, Caporino NE, Settipani CA, Read KL, Compton SN, March J, et al. The therapeutic relationship in cognitive-behavioral therapy and pharmacotherapy for anxious youth. J Consult Clin Psychol. (2013) 81:859. doi: 10.1037/a0033294
6. Marker CD, Comer JS, Abramova V, Kendall PC. The reciprocal relationship between alliance and symptom improvement across the treatment of childhood anxiety. J Clin Child Adolesc Psychol. (2013) 42:22–33. doi: 10.1080/15374416.2012.723261
7. Bose D, Proenza DA, Costales G, Viswesvaran C, Bickman L, Pettit JW. Therapeutic alliance in psychosocial interventions for youth internalizing disorders: a systematic review and preliminary meta-analysis. Clin Psychol. (2022) 29:124. doi: 10.1037/cps0000052
8. McLeod BD. Relation of the alliance with outcomes in youth psychotherapy: a meta-analysis. Clin Psychol Rev. (2011) 31:603–16. doi: 10.1016/j.cpr.2011.02.001
9. Compton SN, March JS, Brent D, Albano AM, Weersing VR, Curry J. Cognitive-behavioral psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry. (2004) 43:930–59. doi: 10.1097/01.chi.0000127589.57468.bf
10. Chiappini EA, Gosch E, Compton SN, Olino TM, Birmaher B, Sakolsky D, et al. In-session involvement in anxious youth receiving CBT with/without medication. J. Psychopathol Behav Assess. (2020) 42:615–26. doi: 10.1007/s10862-020-09810-x
11. Peris TS, Compton SN, Kendall PC, Birmaher B, Sherrill J, March J, et al. Trajectories of change in youth anxiety during cognitive—behavior therapy. J Consult Clin Psychol. (2015) 83:239. doi: 10.1037/a0038402
12. Waite P, Codd J, Creswell C. Interpretation of ambiguity: differences between children and adolescents with and without an anxiety disorder. J Affect Disord. (2015) 188:194–201. doi: 10.1016/j.jad.2015.08.022
13. Higa-McMillan CK, Francis SE, Rith-Najarian L, Chorpita BF. Evidence base update: 50 years of research on treatment for child and adolescent anxiety. J Clin Child Adolesc Psychol. (2016) 45:91–113. doi: 10.1080/15374416.2015.1046177
14. Kendall PC, Robin JA, Hedtke KA, Suveg C, Flannery-Schroeder E, Gosch E. Considering CBT with anxious youth? Think exposures. Cogn Behav Pract. (2005) 12:136–48. doi: 10.1016/S1077-7229(05)80048-3
15. Whiteside SPH, Sim LA, Morrow AS, Farah WH, Hilliker DR, Murad MH, et al. A meta-analysis to guide the enhancement of CBT for childhood anxiety: exposure over anxiety management. Clin Child Fam Psychol Rev. (2020) 3:102–21. doi: 10.1007/s10567-019-00303-2
16. Banneyer KN, Bonin L, Price K, Goodman WK, Storch EA. Cognitive behavioral therapy for childhood anxiety disorders: a review of recent advances. Curr Psychiatry Rep. (2018) 20:1–8. doi: 10.1007/s11920-018-0924-9
17. Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. (2014) 58:10–23. doi: 10.1016/j.brat.2014.04.006
18. Kendall PC, Gosch E, Furr JM, Sood E. Flexibility within fidelity. J. Am. Acad. Child Adolesc Psychiatry. (2008) 47:987–93. doi: 10.1097/CHI.0b013e31817eed2f
19. Kendall PC, Frank HE. Implementing evidence-based treatment protocols: flexibility within fidelity. Clin Psychol. (2018) 25:40. doi: 10.1111/cpsp.12271
20. Ginsburg GS, Becker KD, Drazdowski TK, Tein J-Y. Treating anxiety disorders in inner city schools: results from a pilot randomized controlled trial comparing CBT and usual care. Child Youth Care Forum. (2012) 41:1–19. doi: 10.1007/s10566-011-9156-4
21. Liber JM, McLeod BD, van Widenfelt BM, Goedhart AW, van der Leeden AJM, Utens EMWJ, et al. Examining the relation between the therapeutic alliance, treatment adherence, and outcome of cognitive behavioral therapy for children with anxiety disorders. Behav Ther. (2010) 41:172–86. doi: 10.1016/j.beth.2009.02.003
22. Podell JL, Kendall PC, Gosch EA, Compton SN, March JS, Albano A-M, et al. Therapist factors and outcomes in CBT for anxiety in youth. Prof Psychol. (2013) 44:89. doi: 10.1037/a0031700
23. Southam-Gerow MA, Chapman JE, Martinez RG, McLeod BD, Hogue A, Weisz JR, et al. Are therapist adherence and competence related to clinical outcomes in cognitive-behavioral treatment for youth anxiety? J Consult Clin Psychol. (2021) 89:188. doi: 10.1037/ccp0000538
24. Georgiadis C, Peris TS, Comer JS. Implementing strategic flexibility in the delivery of youth mental health care: a tailoring framework for thoughtful clinical practice. Evid Based Pract Child Adolesc Ment Health. (2020) 5:215–32. doi: 10.1080/23794925.2020.1796550
25. Feiss R, Dolinger SB, Merritt M, Reiche E, Martin K, Yanes JA, et al. A systematic review and meta-analysis of school-based stress, anxiety, and depression prevention programs for adolescents. J Youth Adolesc. (2019) 48:1668–85. doi: 10.1007/s10964-019-01085-0
26. Chiu AW, Langer DA, McLeod BD, Har K, Drahota A, Galla BM, et al. Effectiveness of modular CBT for child anxiety in elementary schools. School Psychol Q. (2013) 28:141. doi: 10.1037/spq0000017
27. Hajmohammadi Z, Haji Alizadeh K, Aeini B. The effectiveness of a coping cat program on symptoms of anxiety disorders in primary schools. Int J Pediatr. (2021) 9:14801–11.
28. Kendall PC, Hedtke KA. Cognitive-Behavioral Therapy for Anxious Children: Therapist Manual. Ardmore, PA: Workbook Publishing (2006).
29. Domitrovich CE, Bradshaw CP, Poduska JM, Hoagwood K, Buckley JA, Olin S, et al. Maximizing the implementation quality of evidence-based preventive interventions in schools: a conceptual framework. Adv School Ment Health Promot. (2008) 1:6–28. doi: 10.1080/1754730X.2008.9715730
30. Mychailyszyn MP, Beidas RS, Benjamin CL, Edmunds JM, Podell JL, Cohen JS, et al. Assessing and treating child anxiety in schools. Psychol Sch. (2011) 48:223–32. doi: 10.1002/pits.20548
31. Lenz AS. Meta-analysis of the coping cat program for decreasing severity of anxiety symptoms among children and adolescents. J Child Adolesc Counsel. (2015) 1:51–65. doi: 10.1080/23727810.2015.1079116
32. Schoenwald SK, Hoagwood K. Effectiveness, transportability, and dissemination of interventions: What matters when? Psychiatr Serv. (2001) 52:1190–7. doi: 10.1176/appi.ps.52.9.1190
33. Barrington J, Prior M, Richardson M, Allen K. Effectiveness of CBT versus standard treatment for childhood anxiety disorders in a community clinic setting. Behav Change. (2005) 22:29–43. doi: 10.1375/bech.22.1.29.66786
34. Southam-Gerow MA, Weisz JR, Chu BC, McLeod BD, Gordis EB, Connor-Smith JK. Does cognitive behavioral therapy for youth anxiety outperform usual care in community clinics? An initial effectiveness test. J Am Acad Child Adolesc Psychiatry. (2010) 49:1043–52. doi: 10.1016/j.jaac.2010.06.009
35. Peterman JS, Read KL, Wei C, Kendall PC. The art of exposure: putting science into practice. Cognit Behav Pract. (2015) 22:379–92. doi: 10.1016/j.cbpra.2014.02.003
36. Rapee RM, Wignall A, Hudson JL, Schniering CA. Treating Anxious Children and Adolescents: An Evidence-Based Approach. Oakland, CA: New Harbinger Publications (2000).
37. Villabø MA, Narayanan M, Compton SN, Kendall PC, Neumer S-P. Cognitive–behavioral therapy for youth anxiety: an effectiveness evaluation in community practice. J Consult Clin Psychol. (2018) 86:751. doi: 10.1037/ccp0000326
38. Wergeland GJH, Riise EN, Öst L-G. Cognitive behavior therapy for internalizing disorders in children and adolescents in routine clinical care: a systematic review and meta-analysis. Clin Psychol Rev. (2021) 83:101918. doi: 10.1016/j.cpr.2020.101918
39. Beidas RS, Marcus S, Aarons GA, Hoagwood KE, Schoenwald S, Evans AC, et al. Individual and organizational factors related to community clinicians’ use of therapy techniques in a large public mental health system. JAMA Pediatr. (2015) 169:374.
40. Ringle VA, Read KL, Edmunds JM, Brodman DM, Kendall PC, Barg F, et al. Barriers to and facilitators in the implementation of cognitive-behavioral therapy for youth anxiety in the community. Psychiatr Serv. (2015) 66:938–45. doi: 10.1176/appi.ps.201400134
41. U.S. Preventative Services Task Force. Screening for anxiety in children and adolescents: US preventative services task force recommendation statement. JAMA. (2022) 328:1438–44. doi: 10.1001/jama.2022.16936
42. Arora PG, Stephan SH, Becker KD, Wissow L. Psychosocial interventions for use in pediatric primary care: an examination of providers’ perspectives. Fam Syst Health. (2016) 34:414. doi: 10.1037/fsh0000233
43. Ginsburg GS, Drake KL, Winegrad H, Fothergill K, Wissow LS. An open trial of the anxiety action plan (AxAP): a brief pediatrician-delivered intervention for anxious youth. Child Youth Care Forum. (2016) 45:19–32. doi: 10.1007/s10566-015-9320-3
44. Comer JS. Rebooting mental health care delivery for the COVID-19 pandemic (and beyond): guiding cautions as telehealth enters the clinical mainstream. Cogn Behav Pract. (2021) 28:743–8. doi: 10.1016/j.cbpra.2021.09.002
45. Sammons MT, Elchert DM, Martin JN. Mental health service provision during COVID-19: results of the third survey of licensed psychologists. J Health Serv Psychol. (2021) 47:119–27. doi: 10.1007/s42843-021-00044-3
46. Khatri N, Marziali E, Tchernikov I, Shepherd N. Comparing telehealth-based and clinic-based group cognitive behavioral therapy for adults with depression and anxiety: a pilot study. Clin Intervent Aging. (2014) 9:765. doi: 10.2147/CIA.S57832
47. Anderson REE, Spence SH, Donovan CL, March S, Prosser S, Kenardy J. Working alliance in online cognitive behavior therapy for anxiety disorders in youth: comparison with clinic delivery and its role in predicting outcome. J Med Internet Res. (2012) 14:e1848. doi: 10.2196/jmir.1848
48. Comer JS, Timmons AC. The other side of the coin: computer-mediated interactions may afford opportunities for enhanced empathy in clinical practice. Clin Psychol. (2019) 26:e12308. doi: 10.1111/cpsp.12308
49. Hong N, Herrera A, Furr JM, Georgiadis C, Cristello J, Heymann P, et al. Remote intensive group behavioral treatment for families of children with selective mutism. In: A Mary editor. Evidence-Based Practice in Child and Adolescent Mental Health. London: Routledge (2022). p. 1–20. doi: 10.1080/23794925.2022.2062688
50. Vigerland S, Lenhard F, Bonnert M, Lalouni M, Hedman E, Ahlen J, et al. Internet-delivered cognitive behavior therapy for children and adolescents: a systematic review and meta-analysis. Clin Psychol Rev. (2016) 50:1–10. doi: 10.1016/j.cpr.2016.09.005
51. Khanna MS, Kendall PC. Computer-assisted cognitive behavioral therapy for child anxiety: results of a randomized clinical trial. J Consult Clin Psychol. (2010) 78:737. doi: 10.1037/a0019739
52. Stasiak K, Fleming T, Lucassen MFG, Shepherd MJ, Whittaker R, Merry SN. Computer-based and online therapy for depression and anxiety in children and adolescents. J Child Adolesc Psychopharmacol. (2016) 26:235–45. doi: 10.1089/cap.2015.0029
53. Khanna MS, Kendall PC. Computer-assisted CBT for child anxiety: the coping cat CD-ROM. Cognit Behav Pract. (2008) 15:159–65. doi: 10.1016/j.cbpra.2008.02.002
54. Khanna MS, Carper MM, Harris MS, Kendall PC. Web-based parent-training for parents of youth with impairment from anxiety. Evid Based Pract Child Adolesc Ment. Health. (2017) 2:43–53. doi: 10.1080/23794925.2017.1283548
55. Meyer JM, Clapp JD, Whiteside SP, Dammann J, Kriegshauser KD, Hale LR, et al. Predictive relationship between parental beliefs and accommodation of pediatric anxiety. Behav Ther. (2018) 49:580–93. doi: 10.1016/j.beth.2017.11.004
56. Salloum A, Andel R, Lewin AB, Johnco C, McBride NM, Storch EA. Family accommodation as a predictor of cognitive-behavioral treatment outcome for childhood anxiety. Fam Soc. (2018) 99:45–55. doi: 10.1177/1044389418756326
57. Lebowitz ER, Marin C, Martino A, Shimshoni Y, Silverman WK. Parent-based treatment as efficacious as cognitive-behavioral therapy for childhood anxiety: a randomized noninferiority study of supportive parenting for anxious childhood emotions. J Am Acad Child Adolesc Psychiatry. (2020) 59:362–72. doi: 10.1016/j.jaac.2019.02.014
58. Silverman WK, Marin CE, Rey Y, Kurtines WM, Jaccard J, Pettit JW. Group-versus parent-involvement CBT for childhood anxiety disorders: treatment specificity and long-term recovery mediation. Clin Psychol Sci. (2019) 7:840–55. doi: 10.1177/2167702619830404
59. Lebowitz ER, Omer H, Hermes H, Scahill L. Parent training for childhood anxiety disorders: the SPACE program. Cogn Behav Pract. (2014) 21:456–69. doi: 10.1016/j.cbpra.2013.10.004
60. Crawford EA, Frank HE, Palitz SA, Davis JP, Kendall PC. Process factors associated with improved outcomes in CBT for anxious youth: therapeutic content, alliance, and therapist actions. Cogn Ther Res. (2018) 42:172–83. doi: 10.1007/s10608-017-9864-7
61. Lundkvist-Houndoumadi I, Thastum M, Nielsen K. Parents’ difficulties as co-therapists in CBT among non-responding youths with anxiety disorders: parent and therapist experiences. Clin Child Psychol Psychiatry. (2016) 21:477–90. doi: 10.1177/1359104515615641
Keywords: cognitive behavioral therapy (CBT), anxiety, youth, flexibility, adaptation
Citation: Kendall PC, Ney JS, Maxwell CA, Lehrbach KR, Jakubovic RJ, McKnight DS and Friedman AL (2023) Adapting CBT for youth anxiety: Flexibility, within fidelity, in different settings. Front. Psychiatry 14:1067047. doi: 10.3389/fpsyt.2023.1067047
Received: 11 October 2022; Accepted: 30 January 2023;
Published: 01 March 2023.
Edited by:
Juventino Hernandez Rodriguez, The University of Texas Rio Grande Valley, United StatesReviewed by:
Emily Becker-Haimes, University of Pennsylvania, United StatesCopyright © 2023 Kendall, Ney, Maxwell, Lehrbach, Jakubovic, McKnight and Friedman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philip C. Kendall, cGtlbmRhbGxAdGVtcGxlLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.