
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 17 February 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1064137
 Juliane Piasseschi de Bernardin Gonçalves1*†
Juliane Piasseschi de Bernardin Gonçalves1*† Camilla Casaletti Braghetta1†
Camilla Casaletti Braghetta1† Willyane de Andrade Alvarenga2
Willyane de Andrade Alvarenga2 Clarice Gorenstein3,4
Clarice Gorenstein3,4 Giancarlo Lucchetti5
Giancarlo Lucchetti5 Homero Vallada1
Homero Vallada1Background: Although observational studies have already shown promising results of flourishing, a broader concept of health based on positive psychology, there is still a gap in the literature regarding studies that combine different topics of flourishing in a single intervention.
Objectives: To develop a comprehensive and integrate intervention based on positive psychology gathering different topics of flourishing to improve mental health outcomes in individuals with depressive symptoms.
Methods: The following steps were performed: (1) a comprehensive literature review; (2) the designing of a 12-session group intervention based on the values, virtues, and topics of flourishing; (3) assessment of the rationale, coherence, and feasibility by a panel of healthcare professionals answering semi-structured questions, and (4) application of an e-Delphi technique including mental health experts to reach a consensus of at least 80% for each item of the protocol.
Results: A total of 25 experts participated in the study, 8 in the panel with semi-structured questions and 17 in the e-Delphi technique. A three-round e-Delphi technique was required to reach a consensus for all items. In the first round, a consensus was reached for 86.2% of the items. The remaining items (13.8%) were either excluded or reformulated. In the second round, a consensus was not obtained on one item, which was reformulated and approved in the third round. Qualitative analyses of the open questions were performed and suggestions for the protocol were considered. The final version of the intervention was composed of 12 weekly group sessions with 90-min each. The topics included in the intervention were physical and mental health, virtues and character strengths, love, gratitude, kindness, volunteering, happiness, social support, family, friends and community, forgiveness, compassion, resilience, spirituality, purpose and meaning of life, imagining the “best possible future,” and flourishing.
Conclusion: The flourishing intervention was successfully developed using an e-Delphi technique. The intervention is ready to be tested in an experimental study to verify its feasibility and effectiveness.
The mental health burden is increasing worldwide, posing several challenges to low-to-middle income countries such as Brazil. The World Health Organization (WHO) estimates that more than 300 million people have depression worldwide, and less than half have access to treatment (1).
Depression is currently the most significant cause of absenteeism and disability in the workforce (2) and the second largest cause of disability worldwide.
The incidence of depression has increased by 59.8% from 1990 to 2017, and is the most common chronic disease worldwide, at present (3). Depression treatment costed approximately US$ 236 billion in 2018 in USA, an increase of more than 35% since 2010 (4). According to recent data, at least 14% of the Brazilian population suffers from depressive symptoms, while 17% have had an episode of major depression throughout their lives (5).
The WHO defines health as “a state of complete physical, mental and social wellbeing and not only the absence of disease” (6). However, this definition does not consider the dynamic nature of human beings. Therefore, new concepts are emerging in literature. We would like to highlight a specific one called flourishing, coined by Tyler VanderWeele, which defines health as “the state in which all aspects of a person's life are good” (7). According to this concept, there are five broad domains of human life: (i) happiness and life satisfaction; (ii) health, both mental and physical; (iii) meaning and purpose; (iv) character and virtue; and (v) close social relationships and four pathways, i.e., family, work, education, and religious community (8).
Previous longitudinal studies with large samples have already shown promising effects of VanderWeele's flourishing dimensions/pathways on physical and mental health. A US national cohort with ~13,000 adults aged >50 years has shown that individuals with greater purpose of life had lower mortality risk (9) and that altruistic behaviors (e.g., volunteering) were associated with lower mortality, and better physical activity and psychosocial outcomes (10). On similar lines, a US cohort with ~60,000 nurses found that forgiveness was associated with higher levels of positive affect and social integration and lower levels of psychological distress (11), and religious attendance was related to lower risk of death (12).
This longitudinal data supports that the broader concept of health has robust scientific evidence and should be discussed by the scientific literature. Within this context, several interventions based on human values and virtues were proposed, and publications on positive mental health programs (13, 14) showed promising results toward minimizing depressive symptoms in different populations (15–18). Although there are several clinical trials regarding the effectiveness of virtues, values, and character on health outcomes (19, 20), to the best of our knowledge, there is a scarcity of studies combining different aspects of flourishing, that focus on VanderWeele's concept (8). Since the concept of flourishing embraces different dimensions which are linked to better health outcomes, promoting all of these dimensions in a single intervention may have better results than considering them separately.
The purpose of this study was to advance this field of research by creating an intervention protocol combining different aspects of flourishing to deliver in a few group sessions. Therefore, this study aimed to develop a simple, practical, and low-cost intervention protocol to promote mental health based on the conceptual framework of flourishing, through an e-Delphi technique.
The study was approved by the Research Ethics Committee of the School of Medicine of the University of Sao Paulo, Brazil, under approval number CAAE: 52554221.4.0000.0068. All respondents provided written informed consent.
The study was organized into four phases, as shown in Supplementary Figure 1.
A non-systematic review was carried out in the following scientific databases: PubMed, Web of Science and Scopus, using the keywords “Flourish*,” “Mental Health,” “Positive Psychology,” “Intervention,” “Therapy,” and “Treatment.” We selected higher hierarchy evidence studies, such as meta-analyses performed through systematic reviews, randomized clinical trials, and cohort studies.
First, we selected studies that investigated the impact of the five domains of Tyler VanderWeele's concept of flourishing, as presented in the Introduction: (i) happiness and life satisfaction; (ii) physical and mental health; (iii) purpose and meaning of life; (iv) character and virtues, and (v) social relationship. Then, we elected the specific topics that integrate these domains.
The most relevant topics related to flourishing were selected from these studies and included in our intervention. We created the structure of the intervention based on the protocols used by the clinical trial and adopted a model with the aim of gaining complexity and deepening the themes at each session. In this phase, we also defined the specific objectives to guide the group discussion within the theme of the session, and the specific dynamics and exercises related to the theme, based on previously published clinical trials.
The first version of the protocol was submitted to a committee of healthcare professionals, experts in the field of mental health, with experience in leading therapeutical groups or clinical practice related to spirituality and religiosity, for a non-systematic evaluation of its feasibility, robustness, and coherence, using a set of semi-structured questions. An email was sent to the experts explaining the flourishing intervention and inviting them to assess the attached protocol through an electronic questionnaire. After agreeing with the Informed Consent Form (ICF), they evaluated the protocol using a semi-structured questionnaire with open-ended questions about the intervention structure: content, format, target population, and intervention providers. The results obtained from the experts were used to remodel the protocol. Based on the modifications suggested by the experts, the protocol was then prepared for the structured e-Delphi phase.
In this phase, another group of experts (different from Phase 3) were invited to assess the intervention through an e-Delphi technique. This type of systematic methodology allows receiving opinions and comments from a panel of selected experts (21, 22). Thus, the opinion of experts on the subject can help point out possible topics of the intervention that need improvement or are inadequate. When the experts' answers are quantified, it serves as a guidance on the appropriateness of the evaluated item. If there is no consensus among the experts, the item should be changed or withdrawn (22).
Health professionals from medical and non-medical fields were included; they were different from those invited in the previous phase. The selection criteria were PhD holders with at least 10 years of experience in any of the following areas: mental health, spirituality/religiosity, positive psychology, or complementary health therapies. These professionals were selected based on their academic and clinical experience on themes related to the development of values and virtues in clinical practice and research, mental health care toward depressive patients and use of complementary therapies. Since there is no consensus on the sample size of experts needed for a panel adequate for an e-Delphi technique (23), the present study determined to include at least 17 individuals (22). This choice was based on the findings of a previous systematic review that investigated the median number of panel members among 76 published protocols.
Questionnaires were developed on the SurveyMonkey® platform and the link was sent by email. Experts had 45 days to respond. The e-Delphi technique was expected to be conducted for as many rounds as necessary until consensus was achieved for all items.
The questionnaire consisted of general questions about each session and specific ones for the items that were considered the most challenging by the authors. It contained multiple choice questions and open questions for extra comments. The answers were structured with a Likert score of 1 to 5 points. Although no consensus is defined for the e-Delphi evaluation criteria, most studies use levels of agreement between 60 and 80% (24). Therefore, to be rigorous with the assessment of the protocol, we adopted a cut-off point of 80% consensus with scores between 4 and 5 points. In the case of not reaching the cut-off point, an item could be eliminated or re-assessed.
Comments by the evaluators were examined, and the results of this analysis were used to improve the protocol and materials of the intervention.
The themes of the intervention's sessions were derived using the conceptual framework and the activities for Flourishing proposed by Tyler VanderWeele and collaborators in a previous publication (25). The selected topics of flourishing were: physical and mental health awareness; purpose and meaning of life; forgiveness; character strengths and virtues; kindness; volunteering; spirituality; gratitude; imagining the “best possible future”; love; compassion; social support, family, friends, and community; and happiness and resilience (25).
The framework in Figure 1 was developed to illustrate the interconnection between the pathways of flourishing, the topics selected for the intervention sessions, and domains of flourishing, demonstrating the rational used to develop the entire intervention protocol.
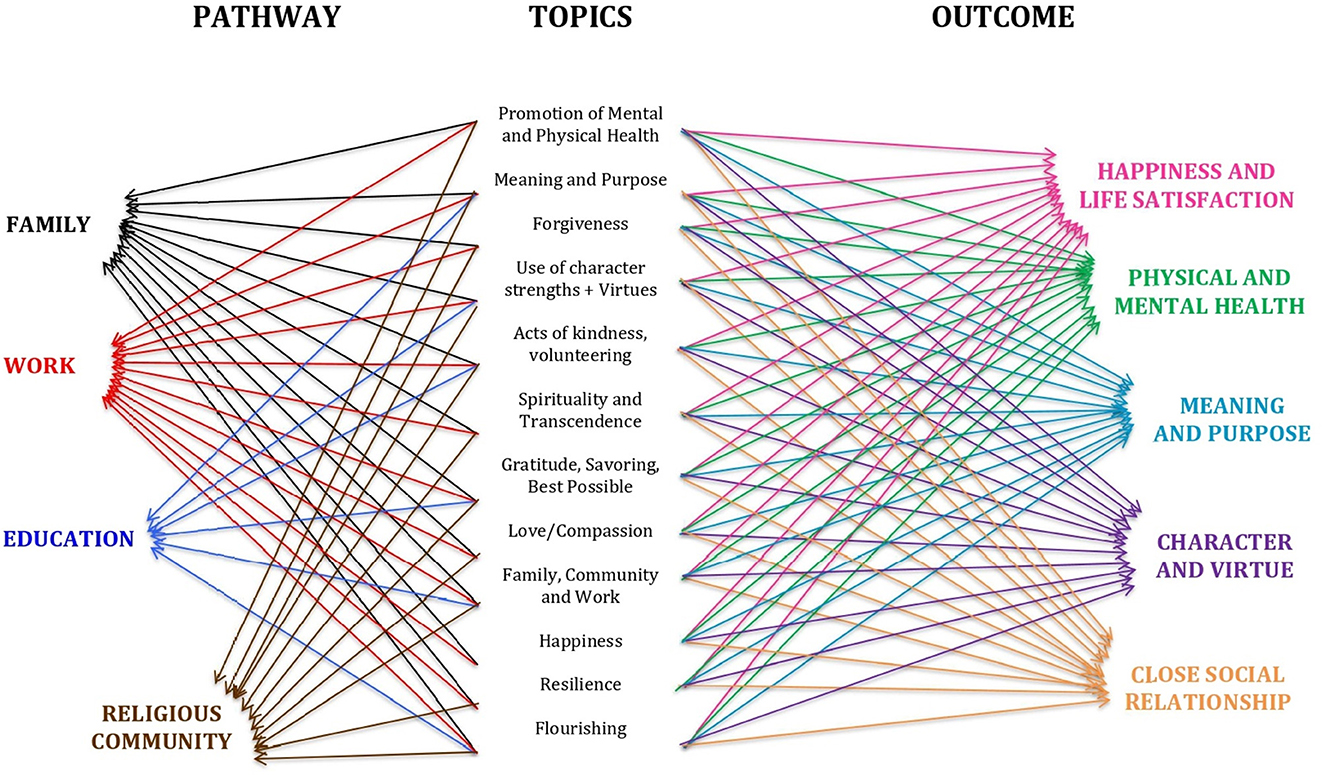
Figure 1. Flourishing framework: The pathway interconnections between the domains and the aspects.
Thereafter, we categorized the topics into three main groups to increase the complexity and enhance “human development” in the process of flourishing:
a) Health awareness and self-knowledge: Physical and mental health, virtues, character strengths, and flourishing.
b) Virtues and values that can connect the participant with the environment and others: Kindness, volunteering, gratitude, imagining the “best possible future,” love, compassion, and social support, family, friends, and community.
c) Virtues and values that connect one with self: Happiness, purpose and meaning of life, forgiveness, spirituality, and resilience.
Regarding the structural organization of the sessions, our search revealed that most positive psychology interventions varied from 1 to 20 weekly sessions (19, 20), with a duration of 1–5 h per session (19). Therefore, in accordance with the literature, we decided to distribute the topics into 12 weekly sessions, each lasting for 90 min.
Also, the intervention was to be delivered on-line. Online interventions can be effective and feasible for treating mental health disorders, such as depression and anxiety (26, 27). Advantages of such interventions include adaptability, multimedia presentations, and saving on traveling efforts. Due to these reasons and considering the traffic problems as a consequence of the population density and territorial extension of the city of São Paulo, Brazil, we decided to offer the intervention through the online format. Regarding the structure of the intervention, the sessions were to be conducted by one or two healthcare professionals where all participants could interact with the provider and among themselves.
Table 1 presents the topics in the sequential order of the initially proposed approach, goals for each session, and specific tools used to achieve the goals. All sessions aimed to promote individual reflection using different strategies such as, group discussions, writing exercises, guided meditation exercises, sharing videos and songs about the topic of the sessions, and reflective moments. Based on the theoretical model, we chose to describe the evidence found for each topic along with the design and goals proposed for the session.
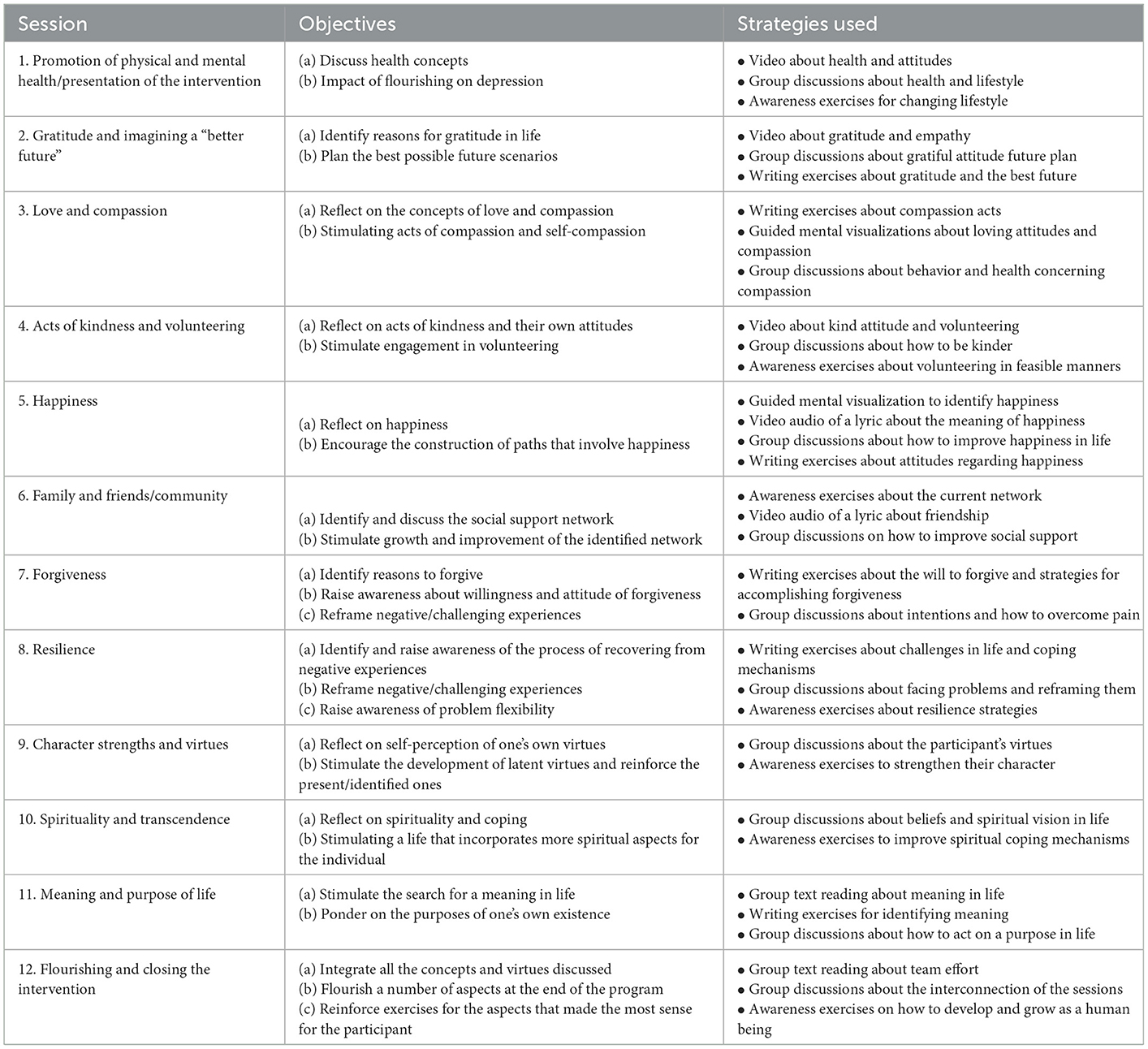
Table 1. Preliminary protocol sessions, objectives, and strategies used in each session.
There are different interventions to raise awareness of physical and mental health (28, 29), and evidence shows that higher awareness helps in seeking and adhering to the treatment. The objective of this session was to discuss different health concepts and ways to flourish with depressive symptoms (8, 30). Providers would help participants understand different health concepts and reflect on their attitudes and behaviors toward their own health through video and group discussions.
Previous evidence based on a meta-analysis showed that gratitude interventions were effective to improve individuals' psychological wellbeing and gratitude levels but not anxiety (31). In this context, writing lists of the things or people one is grateful for and writing letters to the people/situations were associated with better outcomes (32). Likewise, envisioning the “best possible future” was another effective strategy compared to other motivational techniques, as observed in a previous meta-analysis (33).
The goal of this session was to encourage the participants to identify situations in their lives that they were grateful for. We proposed watching a reflexive video and writing exercises regarding gratitude and plans for a “better future.”
A meta-analysis of clinical trials on self-compassion showed a significant improvement in 11 psychosocial outcomes when compared to the controls (34). The focus on compassion, however, showed a small effect size in another study (35). Loving-kindness interventions (e.g., meditation) showed a small to large effect size in daily positive emotions when compared to other groups (35). This session aimed to help the participants identify acts and feelings of love and compassion in their daily lives through guided imagery exercises for compassion and writing exercises with group discussions on loving attitudes.
Regarding kindness and altruism, a recent meta-analysis pointed out a small effect size on wellbeing (36). Another meta-analysis evidenced a reduction in mortality for individuals engaged in some voluntary work (37). This evidence motivated the development of this session that aimed to make participants aware of the influence of kindness and volunteering on their health, using video and discussions about acts of kindness and volunteering. The provider would guide the group to create new, simple, and practical ideas about volunteering in everyday life.
There is solid evidence that happiness is associated with lower mortality and better mental health outcomes (38). Based on previous intervention protocols that motivated participants to find “passion” (39, 40) and identify sources of happiness (41), the main goal of this session was to help participants reflect on how they could achieve a happier and healthier life, by making a list of what brought happiness to their lives, sharing these experiences with the group, and listening to music about the topic.
Longitudinal studies have shown that having family, friends, and a relationship are associated with a better quality of life (8, 42). Likewise, there are clinical trials proposing strategies (e.g., positive psychology) to improve relationships (43, 44) and stimulating social support networks (45, 46) with positive results.
Thus, this session was designed for the participants to identify their social support network and improve the quality and quantity of their relationships. Providers would use open-questions and a song to raise awareness of participants' current network and discuss how to expand it.
A meta-analysis evaluated the effectiveness of psychotherapeutic interventions to promote forgiveness, showing reduced levels of depression and anxiety and higher hope when compared to other treatments (47). Similarly, another meta-analysis showed that having empathy for the offender and overcoming feelings of unforgiveness were associated with lower levels of depression and anxiety (48).
Since most clinical trials use writing exercises to stimulate intention and feelings of forgiveness (49–51), we developed the session based on writing exercises to explore the participants' feelings and thoughts about forgiveness, identify reasons to forgive, and its impact on their health.
A meta-analysis showed that resilience is negatively associated with negative mental health outcomes and positively associated with positive outcomes (52). Clinical trials proposed interventions based on cognitive-behavioral exercises and mindfulness (53, 54). We based the design of this session on Steinhardt and Dolbier's model of (a) transforming stress into resilience, (b) taking responsibility, (c) focusing on empowerment interpretations, and (d) creating meaningful connections (55).
The resilience session aimed to identify the process of recovering from adversities and developing a more flexible vision of those adversities. Providers would stimulate strategies to develop better resilience in life.
A meta-analysis of character strengths interventions showed significant increases in positive affect, happiness, and life satisfaction, and lower levels of depression (56). In this context, the classic intervention proposed by Seligman (57) showed that encouraging individuals to exercise their strongest character strengths weekly, after identifying them through a questionnaire, resulted in increased happiness and decreased depressive symptoms.
We designed the session using an abbreviated version of the Seligman Strengths and Character scale for the participants to identify their strongest and weakest virtues. The main objective was to increase the participants' perception of their virtues and reinforce their strengths by sharing different perspectives.
Several studies have demonstrated the positive impact of spirituality-based interventions on mental health outcomes, such as lower levels of anxiety and depression (58, 59). Protocols are usually based on motivational group discussions addressing topics such as faith, spiritual beliefs, and peace (60, 61).
The session was based on the material developed by Hopkins et al. (62), with the objective to reflect on the influence of the individuals' beliefs on health by discussing the history of their belief system, and their connection with the sacred, others, and nature. Finally, providers would help participants on how to use these tools and spiritual practice to develop a healthier path.
Meta-analyses on the meaning of life and its impact on health have shown positive correlation with life satisfaction and negative correlation with negative affect (63, 64). Likewise, there is growing evidence that clinical trials based on meaning-centered therapies are associated with better psychological outcomes (65).
This session was developed based on an intervention proposed by Luz et al. which used different reflexive texts about meaning of life (66), allowing participants to identify their meaning in life and consider a purpose to follow. Providers would help participants with their process of identifying and creating life purposes and being able to live it by proposing discussion from the reading of a text and exchange of impressions and personal experiences.
Finally, the aim of the last session was to integrate the virtues and values of the aspects of flourishing into participants' life, reinforcing the idea of human development. The session would encourage the participants to reflect on their role in life and assume responsibility for their lives and situations through text reading and group discussions (25, 67, 68).
The panel was composed of eight experts: five women (71.4%) and three men (28.6%). Their professions were psychologists (four), physicians (two), social worker (one), and spiritual counselor (one), and all had more than 10 years of professional experience.
According to the experts, the intervention seemed to be a positive, innovative, and well-grounded proposal. They pointed out the following strengths: the scope of the themes, potential to stimulate reflection, and possibility of being replicated in different scenarios. The experts agreed with the feasibility of the intervention, emphasizing clarity and objectivity, and the applicability of the exercises. The number and duration of the sessions were considered appropriate. Most experts agreed that the providers should be healthcare professionals with previous adequate training on the subject and the sessions.
According to the experts, the population that could benefit from this intervention were adults and older adults with mild and moderate depressive symptoms. However, they discouraged the use of this intervention for individuals with severe symptoms. Furthermore, experts mentioned that individuals with low education could benefit from the intervention as well. However, they pointed out two possible challenges to be tested in practice: the writing exercises and the difficulties in understanding complex concepts such as resilience and flourishing. Finally, they reported that some conceptual adaptations and simplifications would be necessary.
Based on the opinions of this panel, adaptations were made in the protocol and the revised version was sent to an e-Delphi panel.
Of the 21 experts invited, 3 were not available to collaborate in due time, and 1 refused to provide consent to participate. Therefore, the final panel was composed of 17 individuals: 10 men (58.8%) and 7 women (41.2%). The average age was 52.2 (SD = 14.5) years, with an average professional experience of 25.9 (SD = 10.6) years, and all of them were PhD holders. The panel included eight physicians, four psychologists, three university professors, one physical therapist, and one nurse.
This phase was separated as follows:
(a) E-Delphi technique assessment: This included 58 items regarding specific opinions on the objectives, strategies, and interventions for each session, using a Likert scale ranging from 1 (totally disagree) to 5 (totally agree).
1st round
Table 2 presents the specific items assessed if consensus was achieved for them, and the conduct provided by the authors. Consensus was obtained on 50 out of the 58 items in the first round, representing 86.2% agreement among experts; these topics and exercises were maintained in the intervention protocol. The remaining eight items (13.8%) were from the following topics: three items from session 2 “gratitude and imagining a better future,” and one item each from session 6 “family, friends, and community,” session 7 “forgiveness,” session 10 “spirituality,” and session 11 “meaning and purpose of life.” All of these items were either excluded or reformulated and re-sent to the experts in the second e-Delphi round.
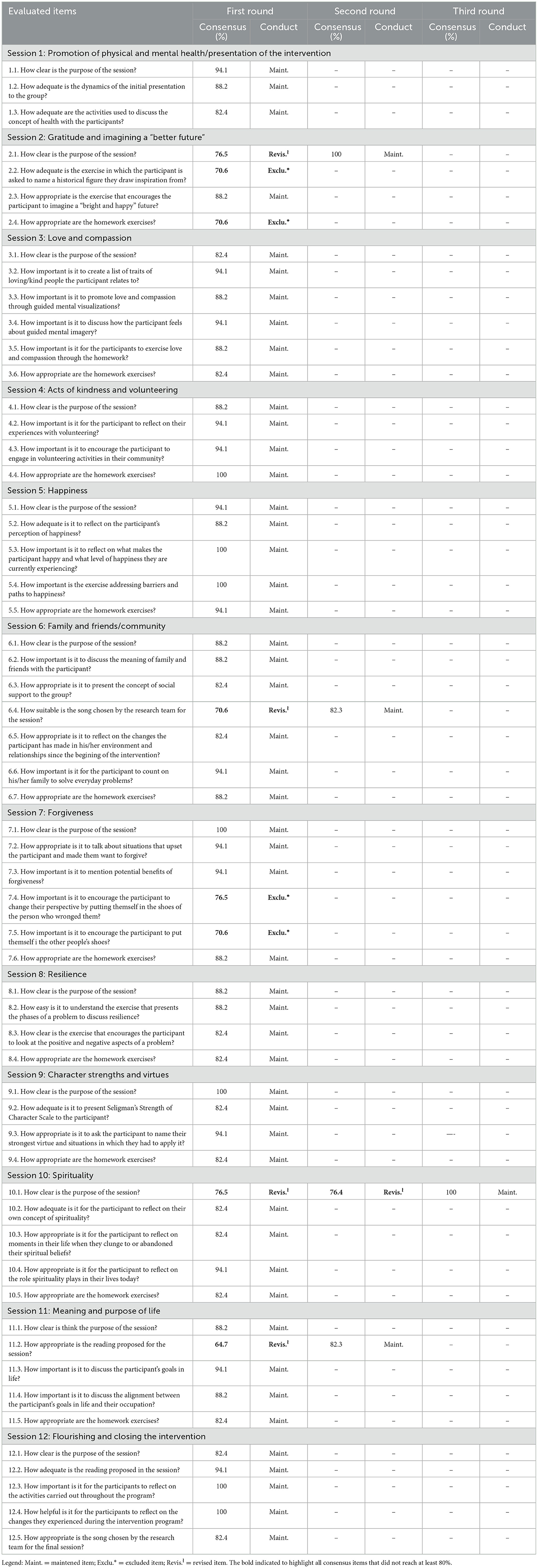
Table 2. Consensus for the items of the preliminary intervention protocol submitted to the Delphi technique.
2nd round
The authors considered the qualitative answers of the experts regarding the eight revised items and decided to exclude four items from the protocol and reformulate the other four to obtain consensus. Table 3 shows the summary of the experts' comments along with the authors' appropriate explanation for the reformulation or exclusion of the items. Only the “spirituality” objective of session 10 did not obtain a consensus and was revised again.
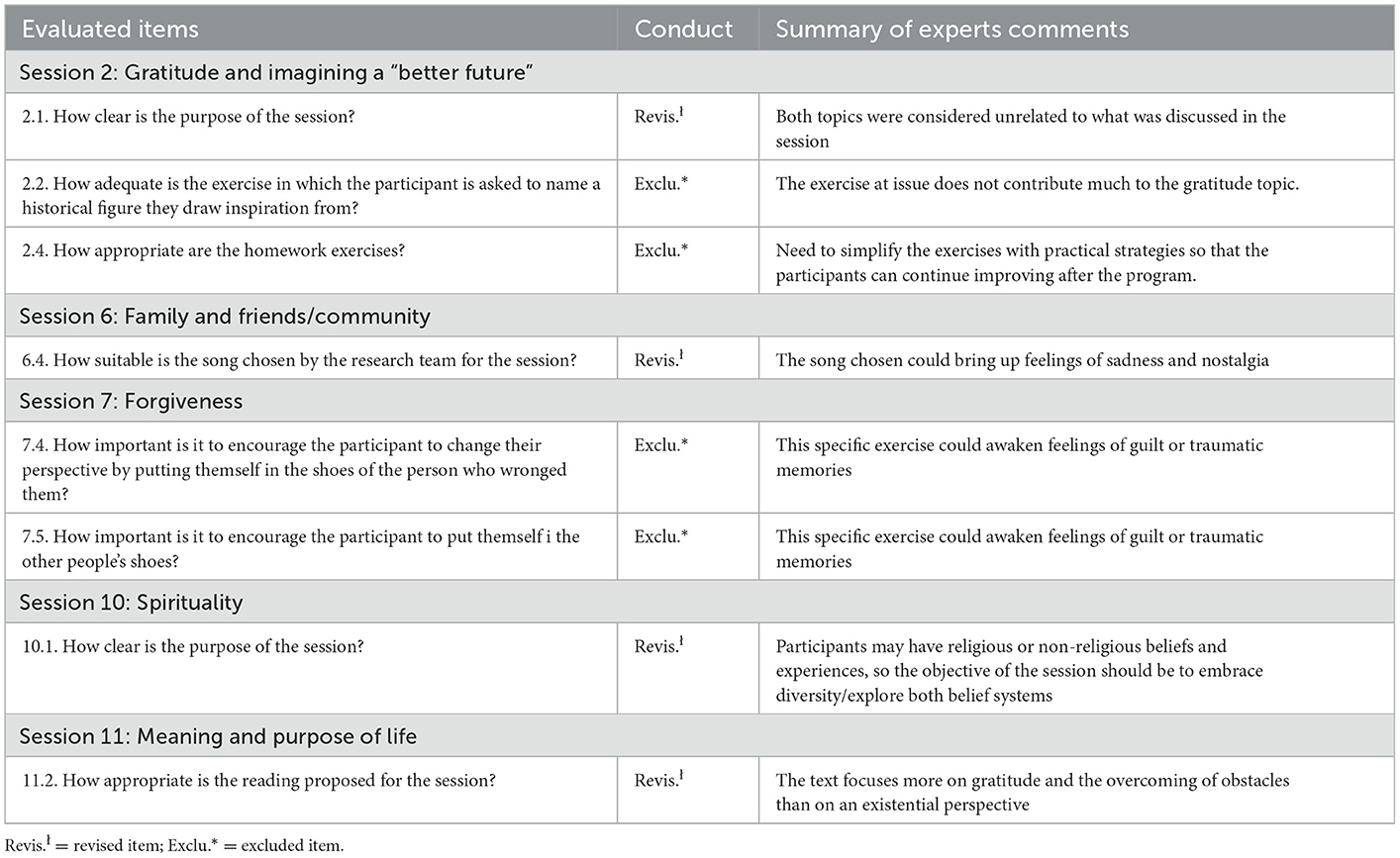
Table 3. Non-consensual items: Revisions and general comments.
3rd round
The third round of the e-Delphi comprised a revised aim of the spirituality session. The experts' suggestions were mainly to highlight the aspects of spirituality related to transcendence, promote the meaning and experience of connection, and emphasize that the session goal should be more inclusive and cover religious and non-religious people. The item was reformulated, and the session renamed to broaden the complexity of the concept of spirituality adopted for the session. The item was then submitted for a third round of evaluation and was approved with 100% consensus.
The agreement for the ratings of all Delphi items between experts (inter-rater reliability) were assessed using the intra-class correlation coefficients (ICC) (two-way mixed model, consistency, average-measures ICC), yielding a coefficient of 0.48 (CI 95%: 0.25–0.66, p < 0.001).
(b) General protocol organizational opinions: This included 10 items concerning organizational aspects of the protocol, such as target public, number and duration of sessions, multimedia presentation, and the provider's guide, using multiple choice questions and Likert scale ranging from 1 (totally disagree) to 5 (totally agree).
Figure 2 shows the opinions of the experts regarding the structure and implementation of the protocol. Experts highlighted the appropriateness of the overall process of flourishing, target population of those with mild depressive symptoms, 12 weekly online delivery sessions, use of the audiovisual resources, and the guideline created for the providers. However, some experts raised two points of warning: implementing the intervention for individuals with moderate depressive symptoms and duration of the sessions.
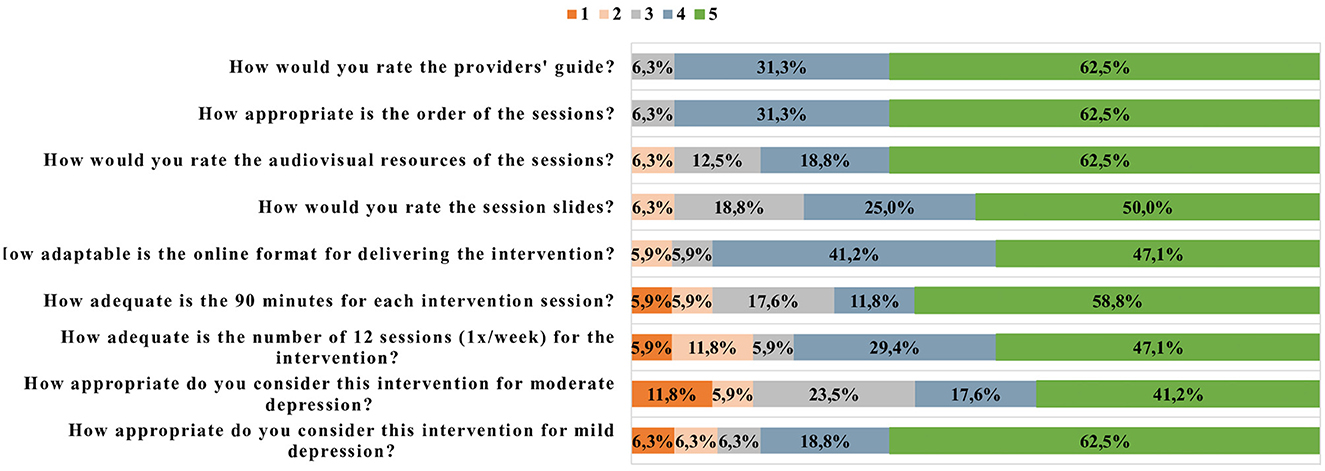
Figure 2. Experts' opinions about the structure and implementation of the protocol.
It is important to emphasize that changes were necessary to improve the coherence of the intervention as a whole. This included the changes related only to the structure (writing and distribution), and not to the content of the items, and the opinions on the e-Delphi technique were respected during this process. Another aspect that should be highlighted is that despite the reorganization of the themes, the protocol remained of 12 sessions.
(c) Experts' suggestions: Experts were allowed to suggest and comment in support of their opinions concerning the questions they were asked. They provided practical suggestions regarding group dynamics for the implementation of the protocol, that were included in the final manual created by the authors for the training of healthcare providers of the intervention in future.
The complementary exercises of the sessions were gathered in a single file, and it was decided to provide this material to the participants at the end of the intervention (post-intervention material), so that they could continue following the proposals and exercises in their daily lives, resulting in continuation of its flourishing process. Experts mentioned the importance of a strategy to ensure continuity of exercises for constant personal improvement, even after of the intervention ended.
The present study successfully developed an intervention protocol based on the flourishing concept of health using a comprehensive literature review and the opinion of experts through the e-Delphi technique. The protocol consists of sharing therapeutic tools during online sessions in collaboration with trained healthcare professionals to conduct the sessions. Though there are other mental health programs focusing on positive aspects, but in this intervention, we specifically sough to adopt the VanderWeele's concept of flourishing and combine its various topics into the sessions offered (13, 14). This intervention is different from others because it combines all virtues and values in a single intervention, resulting in a more holistic and comprehensive approach.
For the development of this protocol, our study followed previous articles that used Delphi or e-Delphi to develop an intervention (21, 22, 69). Delphi is a technique that can impact ways of thinking or decision making through the convergence of opinions and comments of experts' assessments (21). The main advantage of using such a technique is the possibility of exploring underlying assumptions regarding a specific topic (69).
According to the literature, one of the most important aspects of Delphi is the choice of experts. Our experts were mostly from the field of mental health, and this choice was made considering the main outcome of our intervention (reducing depressive symptoms and promoting mental health) and the experience of the experts in the precepts of positive psychology. However, it is important to highlight that, to improve the public health feasibility of this protocol, professionals from other healthcare fields were also included. Another important choice for our panel selection was to include experienced PhD holders for the e-Delphi. This choice guaranteed that well-qualified experts with expertise in both clinical practice and research were included, which was supported by previous studies (21, 22).
An important choice in the development of our protocol was the use of an online e-Delphi technique, instead of a Delphi technique. The e-Delphi has some important advantages such as time and cost savings, convenience for experts and the research team, and data management facility (21, 22). The individualized communication with experts and their blindness regarding the other experts' answers during the process may have contributed to the impartiality of scores, ideas, and suggestions provided.
Regarding the protocol, the experts favored the online format of the interventions. The advantages of using this type of approach include the use of multimedia for the participants, facilitating access to complex content, time and cost savings, and the possibility of engaging with others (26, 27). The use of an online approach is supported by previous studies where clinical trials of brief online intervention programs showed better long-term clinical effects compared to face-to-face therapies for different mental health conditions, especially when the technique included the support of a healthcare professional (70).
As verified through the results, experts reached consensus for ~90% of the items, revealing that the intervention was consistent with the proposal of flourishing. However, it is important to highlight that one item was subjected to three rounds of e-Delphi to reach consensus: the objective of the spirituality session. To achieve the goal for this session the following concept mentioned by Puchalski (71) was adopted: “spirituality is the aspect of humanity that refers to the way individuals seek and express meaning and purpose and the way they experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred.” Some experts argued that spirituality should be related to the sacred or an immortal being and not to the connectedness to the moment, self, or others. Since our main goal in this session was to be inclusive, Puchalski's definition was chosen because it provides a more comprehensive understanding of this construct, in which individuals can recognize their beliefs and values, and identify which connections are meaningful to them, regardless of sacred or religious beliefs. Most experts highlighted the notions of transcendence and connection as relevant aspects to be addressed in this session. In the third round a consensus was reached and the session was renamed “Spirituality and Inner Connection.”
Another important highlight by the experts was the order of the topics of flourishing. The experts did not initially agree to address gratitude and imagining your “best future” in the same session, even though both topics could stimulate an individual to connect with the environment and with others. Comments included that the exercises proposed should be provided separately to achieve their personal goals, and that imagining a “better future” could be more useful at the end of the intervention to synthesize the concept of flourishing. The authors revisited the order of the topics maintaining the rationale initially proposed, to achieve an increase in complexity of the virtues and values of the process of flourishing (8).
Regarding the structure of the intervention, the experts agreed on the 12 weekly sessions; however, not all experts agreed with the duration of 90-min. Since online interventions have operational challenges, such as speed of connection and learning of operating the multimedia (70), a loss of therapeutic time should be considered. Also, group sessions including 10–15 participants need adequate time to allow everyone to express their ideas and opinions. Therefore, this program needs to be tested in clinical practice so that its viability can be confirmed. The experts were also consulted regarding the general use of the multimedia resources, slides for the sessions, and proposed items to include a variety of tools to ensure a better group dynamic, and most opinions were favorable.
Concerning the target population, people with mild and moderate depressive symptoms tend to respond well to most psychotherapy approaches, irrespective of whether those are self-help or cognitive-behavioral therapy (CBT) interventions (72–74). There are, however, reports of lower effects and high rates of treatment dropout when no human therapeutic support is offered, and the patient has only access to the content generated by the electronic platform (74, 75). There is clear evidence that the computer cannot fully replace human contact (76). Therefore, our intervention was developed as a synchronous online approach including full support of the healthcare professionals throughout the program for the participants, making it a relevant therapeutic alliance (73).
Finally, it is noteworthy that most studies investigating mood disorders and web-based treatments do not deal with major depression diagnoses, but with symptoms of depression (72, 77). Given the evidence found in the literature, our intervention was designed for individuals with depressive symptoms and not for those with a diagnosis of major depression. Most experts agreed that this intervention could be used for mild to moderate depressive symptoms, which is supported by the previous literature. Future studies using this protocol should explore which group of participants will benefit the most through this intervention.
The study has some limitations. First, the experts who evaluated the protocol were invited to participate through the authors' professional relationship network. Purposive sampling was used to recruit professionals to serve in the expert committee. However, experts were form different institutions, had different backgrounds, and experiences in the field. Second, the intervention was developed in Portuguese language. Although we had an English version translated by a professional native English speaker translator, no cross-cultural adaptation was carried out. This protocol should be tested in other languages and cultures to verify if the sessions are feasible and meaningful, aiming to make the flourishing intervention culturally sensitive.
The development of the flourishing intervention aims to fill the gap in public health approaches since it is a practical and low-cost intervention. Interventions in groups have an advantage of providing greater efficiency and cost-effectiveness to health services (78), besides the benefits to patients (79), as they facilitate the exchange of experiences and support by expanding the social support network.
Furthermore, the flourishing intervention aims to train healthcare professionals from different backgrounds and expertise, providing fundamental skills to conduct the intervention as a new healthcare tool. Investment in continuous education of multidisciplinary teams has proved to be a significant resource for implementing technical innovations, which aim to change practices in health systems and, consequently, in communities (80). The authors developed a guide for the providers on specific information for conducting the sessions, such as troubleshooting and managing therapeutic groups. The experts had access to this material and highlighted its relevance. The providers' guide is an accessible material for healthcare professionals to understand the exercises and tools proposed for the sessions. The intention is to allow this to be reproducible in different healthcare contexts. A study pointed out that it is important for professionals conducting online interventions to have clinical experience, empathy, and robust knowledge of the technique used, otherwise the intervention may have less effect (26). Therefore, adequate material and training are essential to ensure the best use and effectiveness of the intervention.
The development of the intervention based on the concept of flourishing obtained consensus from the experts. Necessary adjustments were made by the team, and the protocol reformulation proved to be successful. The intervention is ready to be tested in an experimental study to verify its feasibility and effectiveness.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was approved by the Research Ethics Committee of the School of Medicine of the University of Sao Paulo, Brazil, under approval number CAAE: 52554221.4.0000.0068. All respondents provided written informed consent. The patients/participants provided their written informed consent to participate in this study.
JG: conception and design of the work, data collection, data analysis and interpretation, drafting the article, and final approval of the version to be published. CB: data collection, data analysis and interpretation, drafting the article, and final approval of the version to be published. WA: data analysis and interpretation, critical revision of the article, and final approval of the version to be published. CG: data interpretation, critical revision of the article, and final approval of the version to be published. GL: conception and design of the work, data analysis and interpretation, critical revision of the article, and final approval of the version to be published. HV: conception and design of the work, data interpretation, critical revision of the article, and final approval of the version to be published. All authors contributed to the article and approved the submitted version.
This work was sponsored by FAPESP (2022/05018-4). GL and HV are research productivity grantees of the Brazilian Council for Scientific and Technological Development (CNPq). Received financial support from IHPV.
We are very grateful for the experts' contribution to this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1064137/full#supplementary-material
1. Marcus M, Yasamy M, van Ommeren M, Chisholm D, Saxena S. Depression: A Global Public Health Concern. WHO Department of Mental Health Substance Abuse. (2012). Available online at: http://www.who.int/mental_health/management/depression/%0Awho_paper_depression_wfmh_2012.pdf
2. Gordon BR, McDowell CP, Hallgren M, Meyer JD, Lyons M, Herring MP. Association of efficacy of resistance exercise training with depressive symptoms: meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry. (2018) 75:566–76. doi: 10.1001/jamapsychiatry.2018.0572
3. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res. (2020) 126:134–40. doi: 10.1016/j.jpsychires.2019.08.002
4. Greenberg PE, Fournier A-A, Sisitsky T, Simes M, Berman R, Koenigsberg SH, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. (2021) 39:653–65. doi: 10.1007/s40273-021-01019-4
5. Silva MT, Galvao TF, Martins SS, Pereira MG. Prevalence of depression morbidity among Brazilian adults: a systematic review and meta-analysis. Rev Bras Psiquiatr. (2014) 36:262–70. doi: 10.1590/1516-4446-2013-1294
6. Larson JS. The World Health Organization's definition of health: Social vs. spiritual health. Soc Indic Res. (1996) 38:181–92.
7. VanderWeele TJ, McNeely E, Koh HK. Reimagining health—flourishing. JAMA. (2019) 321:1667–8. doi: 10.1001/jama.2019.3035
8. VanderWeele TJ. On the promotion of human flourishing. Proc Natl Acad Sci. (2017) 114:8148–56. doi: 10.1073/pnas.1702996114
9. Shiba K, Kubzansky LD, Williams DR, VanderWeele TJ, Kim ES. Associations between purpose in life and mortality by SES. Am J Prev Med. (2021) 61:e53–61. doi: 10.1016/j.amepre.2021.02.011
10. Kim ES, Whillans A V, Lee MT, Chen Y, VanderWeele TJ. Volunteering and subsequent health and well-being in older adults: an outcome-wide longitudinal approach. Am J Prev Med. (2020) 59:176–86. doi: 10.1016/j.amepre.2020.03.004
11. Long KNG, Worthington ELJ, VanderWeele TJ, Chen Y. Forgiveness of others and subsequent health and well-being in mid-life: a longitudinal study on female nurses. BMC Psychol. (2020) 8:104. doi: 10.1186/s40359-020-00470-w
12. Chen Y, Koh HK, Kawachi I, Botticelli M, VanderWeele TJ. Religious service attendance and deaths related to drugs, alcohol, and suicide among US health care professionals. JAMA Psychiatry. (2020) 77:737–44. doi: 10.1001/jamapsychiatry.2020.0175
13. Eisenstadt M, Liverpool S, Infanti E, Ciuvat RM, Carlsson C. Mobile apps that promote emotion regulation, positive mental health, and well-being in the general population: systematic review and meta-analysis. JMIR Ment Heal. (2021) 8:e31170. doi: 10.2196/31170
14. Carr A, Cullen K, Keeney C, Canning C, Mooney O, Chinseallaigh E, et al. Effectiveness of positive psychology interventions: a systematic review and meta-analysis. J Posit Psychol. (2021) 16:749–69. doi: 10.1080/17439760.2020.1818807
15. Breitbart W, Rosenfeld B, Gibson C, Pessin H, Poppito S, Nelson C, et al. Meaning-centered group psychotherapy for patients with advanced cancer: a pilot randomized controlled trial. Psychooncology. (2010) 19:21–8. doi: 10.1002/pon.1556
16. Kelly JF, Stout RL, Magill M, Tonigan JS, Pagano ME. Spirituality in recovery: a lagged mediational analysis of alcoholics anonymous' principal theoretical mechanism of behavior change. Alcohol Clin Exp Res. (2011) 35:454–63. doi: 10.1111/j.1530-0277.2010.01362.x
17. Koenig HG, Pearce MJ, Nelson B, Daher N. Effects of religious vs. standard cognitive-behavioral therapy on optimism in persons with major depression and chronic medical illness. Depress Anxiety. (2015) 32:835–42. doi: 10.1002/da.22398
18. Lucchetti AL, Peres MF, Vallada HP, Lucchetti G. Spiritual treatment for depression in brazil: an experience from spiritism. Exploration. (2015) 11:377–86. doi: 10.1016/j.explore.2015.07.002
19. Casellas-Grau A, Font A, Vives J. Positive psychology interventions in breast cancer. A systematic review. Psychooncology. (2014) 23:9–19. doi: 10.1002/pon.3353
20. Meyers MC, van Woerkom M, Bakker AB. The added value of the positive: a literature review of positive psychology interventions in organizations. Eur J Work Organ Psychol. (2013) 22:618–32. doi: 10.1080/1359432X.2012.694689
21. Laustsen S, Brahe L. Applying the Delphi method to generate interventions to reduce unnecessary interruptions in clinical nursing. Nord J Nurs Res. (2015) 35:249–55. doi: 10.1177/0107408315603630
22. Sampaio FMC, Sequeira C, Lluch Canut T. Content validity of a psychotherapeutic intervention model in nursing: a modified e-Delphi study. Arch Psychiatr Nurs. (2017) 31:147–56. doi: 10.1016/j.apnu.2016.09.007
23. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS ONE. (2011) 6:e20476. doi: 10.1371/journal.pone.0020476
24. Santos O, Lopes E, Virgolino A, Stefanovska-Petkovska M, Dinis A, Ambrósio S, et al. Defining a brief intervention for the promotion of psychological well-being among unemployed individuals through expert consensus. Front Psychiatry. (2018) 9:13. doi: 10.3389/fpsyt.2018.00013
25. VanderWeele TJ. Activities for flourishing: an evidence-based guide. J Posit Sch Psychol. (2020) 4(1 SE):79–91. Avaiable online at: https://hfh.fas.harvard.edu/files/pik/files/activitiesforflourishing_jppw.pdf
26. Andersson G. Using the internet to provide cognitive behaviour therapy. Behav Res Ther. (2009) 47:175–80. doi: 10.1016/j.brat.2009.01.010
27. Rathbone AL, Clarry L, Prescott J. Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: systematic review. J Med Internet Res. (2017) 19:e399. doi: 10.2196/jmir.8598
28. Teng EJ, Friedman LC. Increasing mental health awareness and appropriate service use in older Chinese Americans: a pilot intervention. Patient Educ Couns. (2009) 76:143–6. doi: 10.1016/j.pec.2008.11.008
29. Livingston JD, Tugwell A, Korf-Uzan K, Cianfrone M, Coniglio C. Evaluation of a campaign to improve awareness and attitudes of young people towards mental health issues. Soc Psychiatry Psychiatr Epidemiol. (2013) 48:965–73. doi: 10.1007/s00127-012-0617-3
30. Silva MJS, Schraiber LB, Mota A. The concept of health in Collective Health: contributions from social and historical critique of scientific production. Physis Revista de Saúde Coletiva. (2019) 29:102. doi: 10.1590/s0103-73312019290102
31. Davis DE, Choe E, Meyers J, Wade N, Varjas K, Gifford A, et al. Thankful for the little things: a meta-analysis of gratitude interventions. J Couns Psychol. (2016) 63:20–31. doi: 10.1037/cou0000107
32. Froh JJ, Bono G, Fan J, Emmons RA, Henderson K, Harris C, et al. Nice thinking! An educational intervention that teaches children to think gratefully. School Psych Rev. (2014) 43:132–52. doi: 10.1080/02796015.2014.12087440
33. Malouff JM, Schutte NS. Can psychological interventions increase optimism? A meta-analysis. J Posit Psychol. (2017) 12:594–604. doi: 10.1080/17439760.2016.1221122
34. Ferrari M, Hunt C, Harrysunker A, Abbott MJ, Beath AP, Einstein DA. Self-compassion interventions and psychosocial outcomes: a meta-analysis of RCTs. Mindfulness. (2019) 10:1455–73. doi: 10.1007/s12671-019-01134-6
35. Zeng X, Chiu CPK, Wang R, Oei TPS, Leung FYK. The effect of loving-kindness meditation on positive emotions: a meta-analytic review. Front Psychol. (2015) 6:1693. doi: 10.3389/fpsyg.2015.01693
36. Curry OS, Rowland LA, Van Lissa CJ, Zlotowitz S, McAlaney J, Whitehouse H. Happy to help? A systematic review and meta-analysis of the effects of performing acts of kindness on the well-being of the actor. J Exp Soc Psychol. (2018) 76:320–9. doi: 10.1016/j.jesp.2018.02.014
37. Okun MA, Yeung EW, Brown S. Volunteering by older adults and risk of mortality: a meta-analysis. Psychol Aging. (2013) 28:564–77. doi: 10.1037/a0031519
38. Koopmans TA, Geleijnse JM, Zitman FG, Giltay EJ. Effects of happiness on all-cause mortality during 15 years of follow-up: the arnhem elderly study. J Happiness Stud. (2010) 11:113–24. doi: 10.1007/s10902-008-9127-0
39. Weiss LA, Westerhof GJ, Bohlmeijer ET. Nudging socially isolated people towards well-being with the “Happiness Route”: design of a randomized controlled trial for the evaluation of a happiness-based intervention. Health Qual Life Outcomes. (2013) 11:159. doi: 10.1186/1477-7525-11-159
40. Weiss LA, Oude Voshaar MAH, Bohlmeijer ET, Westerhof GJ. The long and winding road to happiness: a randomized controlled trial and cost-effectiveness analysis of a positive psychology intervention for lonely people with health problems and a low socio-economic status. Health Qual Life Outcomes. (2020) 18:162. doi: 10.1186/s12955-020-01416-x
41. Lambert D'raven LT, Moliver N, Thompson D. Happiness intervention decreases pain and depression, boosts happiness among primary care patients. Prim Heal Care Res Dev. (2015) 16:114–26. doi: 10.1017/S146342361300056X
42. Waldinger RJ, Cohen S, Schulz MS, Crowell JA. Security of attachment to spouses in late life: concurrent and prospective links with cognitive and emotional wellbeing. Clin Psychol Sci J Assoc Psychol Sci. (2015) 3:516–29. doi: 10.1177/2167702614541261
43. Doss BD, Cicila LN, Georgia EJ, Roddy MK, Nowlan KM, Benson LA, et al. A randomized controlled trial of the web-based OurRelationship program: effects on relationship and individual functioning. J Consult Clin Psychol. (2016) 84:285–96. doi: 10.1037/ccp0000063
44. Halford WK, Doss BD. New frontiers in the treatment of couples. Int J Cogn Ther. (2016) 9:124–39. doi: 10.1521/ijct.2016.9.2.124
45. Leung P, Orrell M, Orgeta V. Social support group interventions in people with dementia and mild cognitive impairment: a systematic review of the literature. Int J Geriatr Psychiatry. (2015) 30:1–9. doi: 10.1002/gps.4166
46. Sebern MD, Sulemanjee N, Sebern MJ, Garnier-Villarreal M, Whitlatch CJ. Does an intervention designed to improve self-management, social support and awareness of palliative-care address needs of persons with heart failure, family caregivers and clinicians? J Clin Nurs. (2018) 27:e643–57. doi: 10.1111/jocn.14115
47. Wade NG, Hoyt WT, Kidwell JEM, Worthington EL. Efficacy of psychotherapeutic interventions to promote forgiveness: a meta-analysis. J Consult Clin Psychol. (2014) 82:154–70. doi: 10.1037/a0035268
48. Recine AC. Designing forgiveness interventions: guidance from five meta-analyses. J Holist Nurs Off J Am Holist Nurses Assoc. (2015) 33:161–7. doi: 10.1177/0898010114560571
49. Wade NG, Worthington JEL. Overcoming interpersonal offenses: is forgiveness the only way to deal with unforgiveness? J Couns Dev. (2003) 81:343–53. doi: 10.1002/j.1556-6678.2003.tb00261.x
50. Goldman DB, Wade NG. Comparison of forgiveness and anger-reduction group treatments: a randomized controlled trial. Psychother Res. (2012) 22:604–20. doi: 10.1080/10503307.2012.692954
51. Baskin TW, Rhody M, Schoolmeesters S, Ellingson C. Supporting special-needs adoptive couples: assessing an intervention to enhance forgiveness, increase marital satisfaction, and prevent depression ψ. Couns Psychol. (2011) 39:933–55. doi: 10.1177/0011000010397554
52. Hu T, Zhang D, Wang J. A meta-analysis of the trait resilience and mental health. Pers Individ Differ. (2015) 76:18–27. doi: 10.1016/j.paid.2014.11.039
53. Joyce S, Shand F, Tighe J, Laurent SJ, Bryant RA, Harvey SB. Road to resilience: a systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open. (2018) 8:e017858. doi: 10.1136/bmjopen-2017-017858
54. Bennett JB Aden CA, Broome K, Mitchell K, Rigdon WD. Team resilience for young restaurant workers: research-to-practice adaptation and assessment. J Occup Health Psychol. (2010) 15:223–36. doi: 10.1037/a0019379
55. Steinhardt M, Dolbier C. Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. J Am Coll Health. (2008) 56:445–53. doi: 10.3200/JACH.56.44.445-454
56. Schutte NS, Malouff JM. The impact of signature character strengths interventions: a meta-analysis. J Happiness Stud. (2019) 20:1179–96. doi: 10.1007/s10902-018-9990-2
57. Seligman MEP, Steen TA, Park N, Peterson C. Positive psychology progress: empirical validation of interventions. Am Psychol. (2005) 60:410–21. doi: 10.1037/0003-066X.60.5.410
58. Goncalves JPB, Lucchetti G, Menezes PR, Vallada H. Religious and spiritual interventions in mental health care: a systematic review and meta-analysis of randomized controlled clinical trials. Psychol Med. (2015) 45:2937–49. doi: 10.1017/S0033291715001166
59. Moreira-Almeida A, Koenig HG, Lucchetti G. Clinical implications of spirituality to mental health: review of evidence and practical guidelines. Rev Bras Psiquiatr. (2014) 36:176–82. doi: 10.1590/1516-4446-2013-1255
60. Breitbart W, Poppito S, Rosenfeld B, Vickers AJ, Li Y, Abbey J, et al. Pilot randomized controlled trial of individual meaning-centered psychotherapy for patients with advanced cancer. J Clin Oncol. (2012) 30:1304–9. doi: 10.1200/JCO.2011.36.2517
61. Morita T, Murata H, Kishi E, Miyashita M, Yamaguchi T, Uchitomi Y, et al. Meaninglessness in terminally ill cancer patients: a randomized controlled study. J Pain Symptom Manag. (2009) 37:649–58. doi: 10.1016/j.jpainsymman.2008.04.017
62. Hopkins E, Kelley R, Bentley K. Working With Groups on Spiritual Themes: Structured Exercises in Healing. 2nd ed. Duluth: Whole Person Associates (1995). p. 148.
63. Czekierda K, Banik A, Park CL, Luszczynska A. Meaning in life and physical health: systematic review and meta-analysis. Health Psychol Rev. (2017) 11:387–418. doi: 10.1080/17437199.2017.1327325
64. Li J-B, Dou K, Liang Y. The relationship between presence of meaning, search for meaning, and subjective well-being: a three-level meta-analysis based on the meaning in life questionnaire. J Happiness Stud. (2021) 22:467–89. doi: 10.1007/s10902-020-00230-y
65. Wong P. From logotherapy to meaning-centered counseling and therapy. In:The The Human Quest for Meaning: Theories Research and Applications. 2nd, ed. New York, NY: Routledge/Taylor & Francis Group (2012). p. 619–47.
66. Luz JMO, Murta SG, Aquino TAA. Avaliação de Resultados e Processo de uma Intervenção para Promoção de Sentido da Vida em Adolescentes. Trends Psychol. (2017) 25:1795–811. doi: 10.9788/TP2017.4-14Pt
67. Norriss H. Flourishing, positive mental health and well-being: how can they be increased? Int J Leadersh Public Serv. (2010) 6:46–50. doi: 10.5042/ijlps.2010.0638
68. W?ziak-Białowolska D, McNeely E, VanderWeele TJ. Human flourishing in cross cultural settings. Evidence from the United States, China, Sri Lanka, Cambodia, and Mexico. Front Psychol. (2019) 10:1269. doi: 10.3389/fpsyg.2019.01269
69. Kim MJ, Sung E, Choi EY, Ju Y-S, Park E-W, Cheong Y-S, et al. Delphi survey for designing a intervention research study on childhood obesity prevention. Korean J Fam Med. (2017) 38:284–90. doi: 10.4082/kjfm.2017.38.5.284
70. Andersson G. Internet interventions: past, present and future. Internet Interv. (2018) 12:181–8. doi: 10.1016/j.invent.2018.03.008
71. Puchalski CM, Vitillo R, Hull SK, Reller N. Improving the spiritual dimension of whole person care: reaching national and international consensus. J Palliat Med. (2014) 17:642–56. doi: 10.1089/jpm.2014.9427
72. Schröder J, Berger T, Westermann S, Klein JP, Moritz S. Internet interventions for depression: new developments. Dialog Clin Neurosci. (2016) 18:203–12. doi: 10.31887/DCNS.2016.18.2/jschroeder
73. Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, et al. Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms: a meta-analysis of individual participant data. JAMA Psychiatry. (2017) 74:351–9. doi: 10.1001/jamapsychiatry.2017.0044
74. Klein JP, Berger T, Schröder J, Späth C, Meyer B, Caspar F, et al. Effects of a psychological internet intervention in the treatment of mild to moderate depressive symptoms: results of the EVIDENT study, a randomized controlled trial. Psychother Psychosom. (2016) 85:218–28. doi: 10.1159/000445355
75. Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomised controlled trial. BMJ. (2004) 328:265. doi: 10.1136/bmj.37945.566632.EE
76. Palmqvist B, Carlbring P, Andersson G. Internet-delivered treatments with or without therapist input: does the therapist factor have implications for efficacy and cost? Expert Rev Pharmacoecon Outcomes Res. (2007) 7:291–7. doi: 10.1586/14737167.7.3.291
77. Kleiboer A, Donker T, Seekles W, van Straten A, Riper H, Cuijpers P, et al. randomized controlled trial on the role of support in Internet-based problem solving therapy for depression and anxiety. Behav Res Ther. (2015) 72:63–71. doi: 10.1016/j.brat.2015.06.013
78. Hedman E, El Alaoui S, Lindefors N, Andersson E, Rück C, Ghaderi A, et al. Clinical effectiveness and cost-effectiveness of Internet- vs. group-based cognitive behavior therapy for social anxiety disorder: 4-year follow-up of a randomized trial. Behav Res Ther. (2014) 59:20–9. doi: 10.1016/j.brat.2014.05.010
79. Fawcett E, Neary M, Ginsburg R, Cornish P. Comparing the effectiveness of individual and group therapy for students with symptoms of anxiety and depression: a randomized pilot study. J Am Coll Health. (2020) 68:430–7. doi: 10.1080/07448481.2019.1577862
Keywords: depressive symptoms, flourishing, mental health, intervention protocol, positive psychology, e-Delphi technique
Citation: Gonçalves JPB, Braghetta CC, Alvarenga WA, Gorenstein C, Lucchetti G and Vallada H (2023) Development of a comprehensive flourishing intervention to promote mental health using an e-Delphi technique. Front. Psychiatry 14:1064137. doi: 10.3389/fpsyt.2023.1064137
Received: 07 October 2022; Accepted: 30 January 2023;
Published: 17 February 2023.
Edited by:
Maryam Salmanian, Tehran University of Medical Sciences, IranReviewed by:
Daniela Rodrigues Recchia, Universität Witten/Herdecke, GermanyCopyright © 2023 Gonçalves, Braghetta, Alvarenga, Gorenstein, Lucchetti and Vallada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juliane Piasseschi de Bernardin Gonçalves,  anVsaWFuZS5wYmdAYWx1bW5pLnVzcC5icg==
anVsaWFuZS5wYmdAYWx1bW5pLnVzcC5icg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.