
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychiatry, 02 March 2023
Sec. Addictive Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1051528
This article is part of the Research TopicMobile Health Application in Addictive Disorders TherapyView all 8 articles
 Núria Mallorquí-Bagué1,2*
Núria Mallorquí-Bagué1,2* Alba Palazón-Llecha1,2Mercè Madre1Francesca Batlle1
Alba Palazón-Llecha1,2Mercè Madre1Francesca Batlle1 Santiago Duran-Sindreu1,3
Santiago Duran-Sindreu1,3 Joan Trujols1,3
Joan Trujols1,3Background: Cocaine use disorder (CUD) is a chronic condition that presents high relapse rates and treatment dropouts. Web-based interventions have proven to be effective when optimizing face-to-face treatments in different mental health conditions and have the potential to optimize current CUD treatments. However, web-based interventions in addictive behaviors are still limited. The aim of this study is to evaluate whether adding a web-based cognitive behavioral therapy (i.e., CBT4CBT) to standard CUD treatment, improves treatment outcomes in a Spanish sample of patients with severe CUD (which requires inpatient treatment). Additionally, we aim to explore predictive factors of treatment response and treatment gender-related differences.
Methods: All individuals coming for inpatient cocaine detoxification who meet the inclusion criteria will have the possibility to be part of the study. The participants of this open-label randomized controlled clinical trial (RCT) will be allocated to treatment as usual (TAU) or TAU+CBT4CBT after the hospitalization for cocaine detoxification. During the inpatient treatment they will all receive an individualized psychological intervention. There will be six time point assessments: at 48–72 h of starting inpatient treatment, at the end of inpatient treatment and before starting day care and outpatient treatment, at the end of the 8 weeks CTB4CBT / TAU arm treatment and at three follow-up time points (1-, 3-, and 6-months post-treatment).
Discussion: To the best of our knowledge, this is the first RCT that explores the efficacy of adding a web-based cognitive behavioral therapy to usual CUD treatment with patients of a clinical sample in Europe.
Trial registration: IIBSP-CTB-2020-116, NCT05207228. Submitted 8th of April 2021, posted 26 st of January 2022. https://clinicaltrials.gov/ct2/show/NCT05207228?cond=Cocaine+Use+Disorder&draw=2&rank=1.
Cocaine use disorder (CUD) is a complex condition with great impact and burden for patients, their relatives and society (1, 2). Due to its increasing incidence rate in Europe and US during the last decade (2, 3) and to its highly prevalent chronic course (4), where dropout rates are high and remission is often followed by relapse, there is a large and increasing need to improve current CUD treatments. Thus, far, no pharmacological approaches are yet approved for treating CUD, which often is a resistant-to-treat condition and is associated to significative morbidity and mortality rates (5, 6). Clinical evidence-based guidelines recommend psychosocial interventions as first line of treatment (1, 2) with large body of scientific knowledge suggesting that these interventions can help improve CUD; especially, contingency management (CM) and cognitive-behavioral therapy (CBT) (1, 5–8).
Systematic reviews and meta-analysis testing the effectiveness of the available psychosocial interventions for individuals with CUD, converge in reporting the efficacy of CM programs either alone (7) or in combination with community reinforcement approaches (CRA) or with other CBT approaches [such as the relapse prevention treatment developed by Carroll et al. (9–11)] by increasing the abstinence period and reducing the dropout rates, which makes CM the most reliable method to turn an active cocaine user into an abstainer (5, 6). CM and CRA are two behavioral approaches, based on the principle of operant conditioning, where the substance related behavior is understood to be reinforced or maintained by its consequences. The previous (CM), provides an arbitrary reward in face of positive behavioral changes (i.e., most frequently drug-negative urine test), which typically consists of vouchers exchangeable for foods and services, and the latter (CRA) focuses on providing natural rewards by helping people adopt a more rewarding lifestyle free of drugs. However, in clinical practice, the above mentioned approaches are not often implemented (12) in part because they require some cost-effective changes such as the need for conducting higher urine tests or providing monetary rewards such as vouchers, thus the approach of Carroll et al. (13, 14) is a good evidence-based alternative.
With the new digital era, a new intervention window emerges through the implementation of web-based treatments that can intensify and optimize the current face-to-face treatment approaches. In fact, the current challenge in the treatment of CUD is in identifying innovative ways to implement the treatment rather than developing more effective strategies (5). However, literature in clinical settings is still scarce for addictive behaviors with very few studies on the effectiveness of web-based interventions for the treatment of illegal substance use. Up until now, much of this work has been conducted in the area of smoking, in which cognitive-behavioral interventions by means of computers/ internet have demonstrated to be effective on quit rates or attempts (15, 16). Thus, far, two web-based interventions have been tested through RCTs for treating CUD with positive effects reported in their target population (17, 18).
CBT4CBT is a CBT web-based treatment for substance use disorders. Previous studies conducted in US have shown its positive impact on improving face-to-face treatment as usual (TAU) (18–20). More specifically, participants who underwent CBT4CBT were significantly more likely to attain three or more weeks of continuous abstinence during treatment compared to participants who underwent TAU (18–20). These effects endured 6 months after treatment, measured through self-reported measures and urine toxicology screens (18, 20). Additionally homework adherence in CBT4CBT is associated with less cocaine use during treatment (19) and participants who completed at least 50% of homework displayed a greater cocaine use reduction in comparison with the ones who completed <50% of homework (21). Considering previous data regarding the prognosis and standard CUD treatment approaches, the evidence suggests that CBT4CBT approach concomitant to TAU could enhance current treatments and improve the outcomes in patients with severe CUD. In order to test the add-on efficacy of the web based CBT4CBT program concomitant to TAU, the comparative and the experimental group will have the same protocol of face-to-face sessions and will only diverge with the provision of the web based CBT4CBT program at the experimental group.
The aim of the present study is to evaluate whether adding a web-based cognitive behavioral therapy (CBT4CBT) to standard cocaine use disorder treatment improves treatment outcomes in a Spanish sample of patients with severe CUD (that require inpatient treatment). To do so, two primary outcomes are considered: (1) treatment retention (vs. dropout) and, (2) relapse (number of positive urine specimens submitted, percent negative urine screens, percent days of abstinence, self-reported frequency of cocaine use). As secondary outcomes the following variables are measured: craving, psychopathological symptoms, days of any drug use, CBT4CBT usability and treatment satisfaction.
The secondary objectives of the study are two-fold: (a) To explore differences between men and women in treatment response; (b) To explore if comorbid psychopathological symptoms, other addictive behaviors, craving and emotion regulation difficulties are predictive factors of treatment outcome at the end of inpatient treatment as well as at the end of the 8-week CBT4CBT + TAU or TAU and at follow-ups (1, 3, and 6 month).
Inpatients with a diagnosis of cocaine use disorder (DSM-5 criteria) referred for cocaine detoxification to our addictive behaviors' unit at the Hospital de la Santa Creu i Sant Pau in Barcelona (Catalonia, Spain) that are candidates for day care treatment after receiving inpatient detoxification will be asked to participate in the study.
All participants will be recruited prior to CUD treatment randomization. To enter the study participants will: (a) be aged between 18 and 65 years, (b) be hospitalized for cocaine detoxification as the main substance, (c) abstinent at the time of study assessment (from the third day of hospitalization), (d) be eligible to attend day care after hospitalization. Exclusion criteria will be: (a) indication of treatment for other substance use detoxification which is not cocaine, (b) presence of severe psychopathological or neuropsychological alterations that hinder the participation in the study, (c) opioid use disorder within 1 year prior to participation (this criteria includes maintenance treatment with methadone or another opioid substance), (d) lack of Spanish or Catalan knowledge or difficulties to read or write that hampers the participation in the study, (e) non-acceptance of the study procedures, such as the signing of informed consent.
Accepting an alpha risk of 0.05 and a beta risk of 0.2 in a two-sided test, 37 subjects are necessary in each treatment arm to recognize as statistically significant a minimum difference of 2.1 points on treatment relapse (i.e.,: Number of positive urine specimens submitted; primary outcome) between the two groups. The common deviation is assumed to be 3.1. It has been anticipated a drop-out rate of 5%. The parameters implemented to estimate the sample size are based on previous studies with similar populations (19).
This is an unicentric national open-label-randomized clinical trial focused on the improvement of cocaine use disorder treatment as usual (TAU) outcomes through the implementation of a web-based CBT treatment (CBT4CBT). The study was approved by the Research Ethics Committee of the Hospital de la Santa Creu i Sant Pau, project number IIBSP-CBT4CBT-2020-1116.
The present RCT has two arms: arm A (TAU) and arm B (TAU + CBT4CBT). All individuals with cocaine use disorder coming to our inpatient unit for cocaine detoxification will receive treatment as usual (TAU), which will consist of a multidisciplinary approach including psychiatrists, psychologists and nurses. The hospitalization for detoxification begins with the removal of all drugs and, during hospitalization, psychiatrists adjust medication in accordance to cocaine withdrawal symptoms. Additionally, individuals also receive daily psychological interventions based on motivation for change, craving management, assertive communication, problem solving skills and relapse prevention. Nursing staff carries out necessary therapeutic actions, such as taking vital signs, administering medications, provide space for emotional venting and conducting group therapies addressing motivation for change. After a mean of 14 days from admission, inpatients are discharged and placed to either TAU (day care treatment as usual + weekly outpatient follow up) or TAU + CBT4CBT (day care treatment as usual + weekly outpatient follow up and CBT4CBT). The intervention will be discontinued in case of request by the participant. Finally, to ensure adherence to intervention, after one unjustified absence rated by the psychologist, a phone call will be done (see Figure 1).
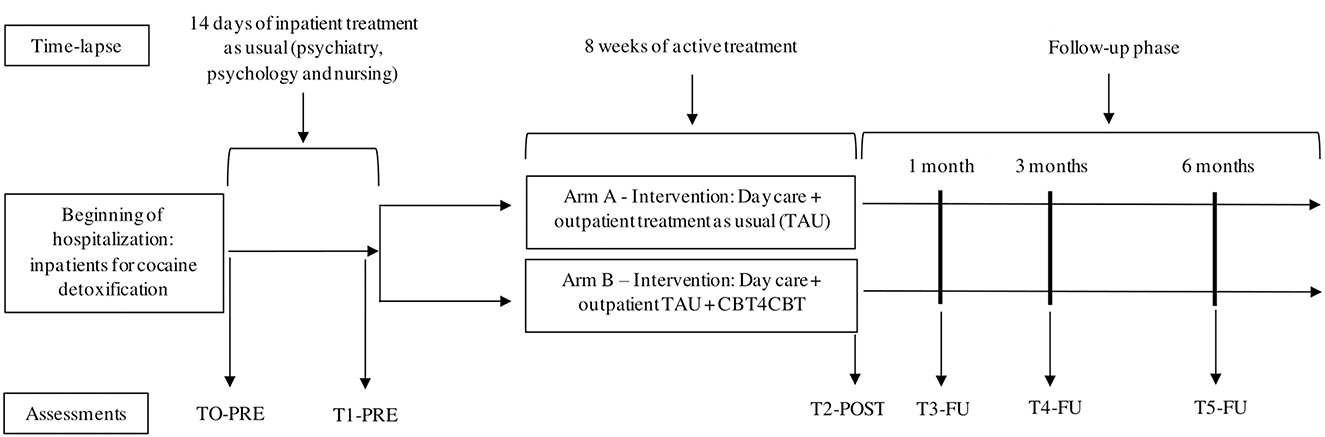
Figure 1. Study design.
Within the framework of the study and with the purpose of introducing the subsequent outpatient treatment, all patients in our inpatient unit for cocaine detoxification who are part of the study will also receive individual psychological CBT based treatment with motivational strategies, emotional regulation skills for mood symptoms and craving management, as explained previously. After completing the inpatient care (at discharge of inpatient care), patients will be randomly assigned to the CBT4CBT + TAU or to TAU. The randomization will be centralized through Clinapsis (http://www.clinapsis-estudis.com/) and all data will be handled through this same platform. Clinapsis is a friendly-user platform where all data from participants is stored. To ensure the transparency and the achievement of ethics procedures, the Central Clinical Research and Clinical Trials Unit of Research Institute of the Hospital de Sant Pau can access the platform to monitor the data collection and management. In addition, the two researchers who provide the psychological strategies during both the inpatient and outpatient treatment phase and carry out the assessments (NMB and APL) also have access to Clinapsis to check whether all data is completed and, subsequently, export it to the software Statistical Package for Social Sciences (SPSS) v. 26.0. Once the database is crated in SPSS, authors will manage the database removing duplicates, identifying missing values and setting up all the variables in order to conduct the statistical analyses in SPSS. Any imbalance in the number of participants in each treatment arm due to non-adherence to treatment protocol prior to starting CBT4CBT but after arm allocation, will also be centralized through Clinapsis.
After completing the inpatient care (at discharge), the patients randomly assigned to the experimental condition will receive the TAU + CBT4CBT a web-based treatment which, as previously stated was tested on individuals with cocaine use disorder in America by the team of Carroll et al. (18). Depending on the patients' personal situation, they will have two options for receiving the treatment: they will be provided with access to the computer program in a small private room within the addictive behaviors outpatient unit or they will be provided with code access for being able to do it from home. In all instances, a psychologist will guide participants through their initial use of the CBT4CBT program and she will be available to answer questions and assist participants each time they use the program (the CBT4CBT and TAU treatments are always explained by a woman). The participants will access the program through an identification/password system to protect confidentiality.
The CBT4CBT program is intended to be user-friendly. The multimedia style of the program is based on elementary-level computer learning games, and the material is presented in a range of formats, including graphic illustrations, videotaped examples where a story with different characters with substance addictions display common risk situations and several ways to cope with them (highlighting the most functional one), verbal instructions, audio voiceovers, interactive assessments with a dichotomous response type, and practice exercises, such as decisional balances that participants must complete with their own arguments. The program consists of six skills (understanding and changing patterns of substance use, coping with craving, refusing offers of drugs, problem-solving skills, identifying and changing thoughts about drugs and improving decision making skills) organized in seven modules of 30 min duration based on a CBT manual published by the National Institute on Drug Abuse and it covers the following core concepts: (1) recognize the triggers, (2) stand up for yourself, (3) deal with craving, (4) stop and think, (5) plan don't panic, (6) go against the flow and (7) stay safe. Each participant has its own credentials to enter the platform, and once in the web-based treatment, the first module will also provide a brief explanation of how to use and navigate the program. Following completion of the first module, the participants can access the rest of the modules (see Table 1). Additional details regarding CBT4CBT can be found elsewhere (14, 19, 22).
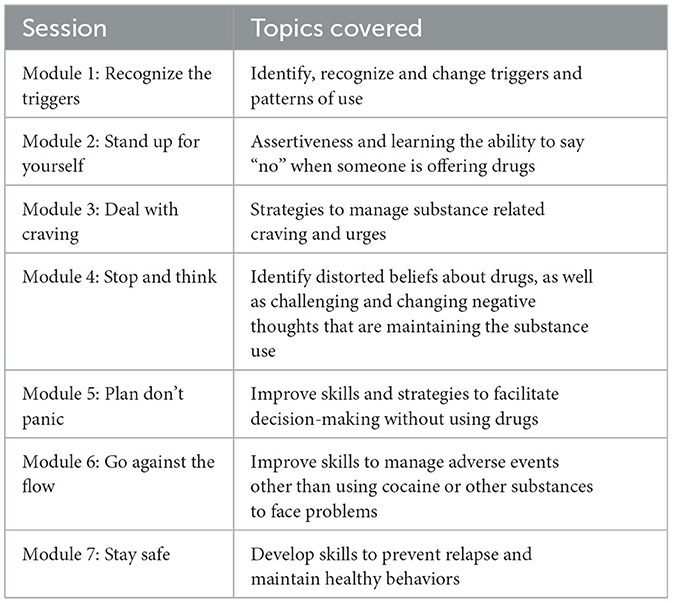
Table 1. Content of the 8-week CBT4CBT program.
Researchers NMB and APL monitor whether participants complete the modules of the CBT4CBT treatment and report it in a separate excel sheet. Also, the completion of the modules can be tracked entering to the section “providers” in the CBT4CBT website (http://www.cbt4cbt.com). Apart from whether the participant has completed or not the module, the researcher can check the percentage of completion of the module and the time spent on it.
There will be 6 time-point assessments: TO-PRE: within the inpatient unit, before starting psychological treatment but once the patients are stabilized from cocaine withdrawal; T1-PRE: after inpatient treatment before starting outpatient treatment (TAU or TAU + CBT4CBT); T2-POST: once the 8-w outpatient treatment is completed (TAU or TAU + CBT4CBT); T3-FU: 1 month follow-up; T4-FU: 3 months follow-up; T5-FU: 6 months follow-up. Additionally, the presence of benzoylecgonine (metabolite of cocaine) in urine will be assessed weekly during the 8 w period of web-based treatment (see Table 2).
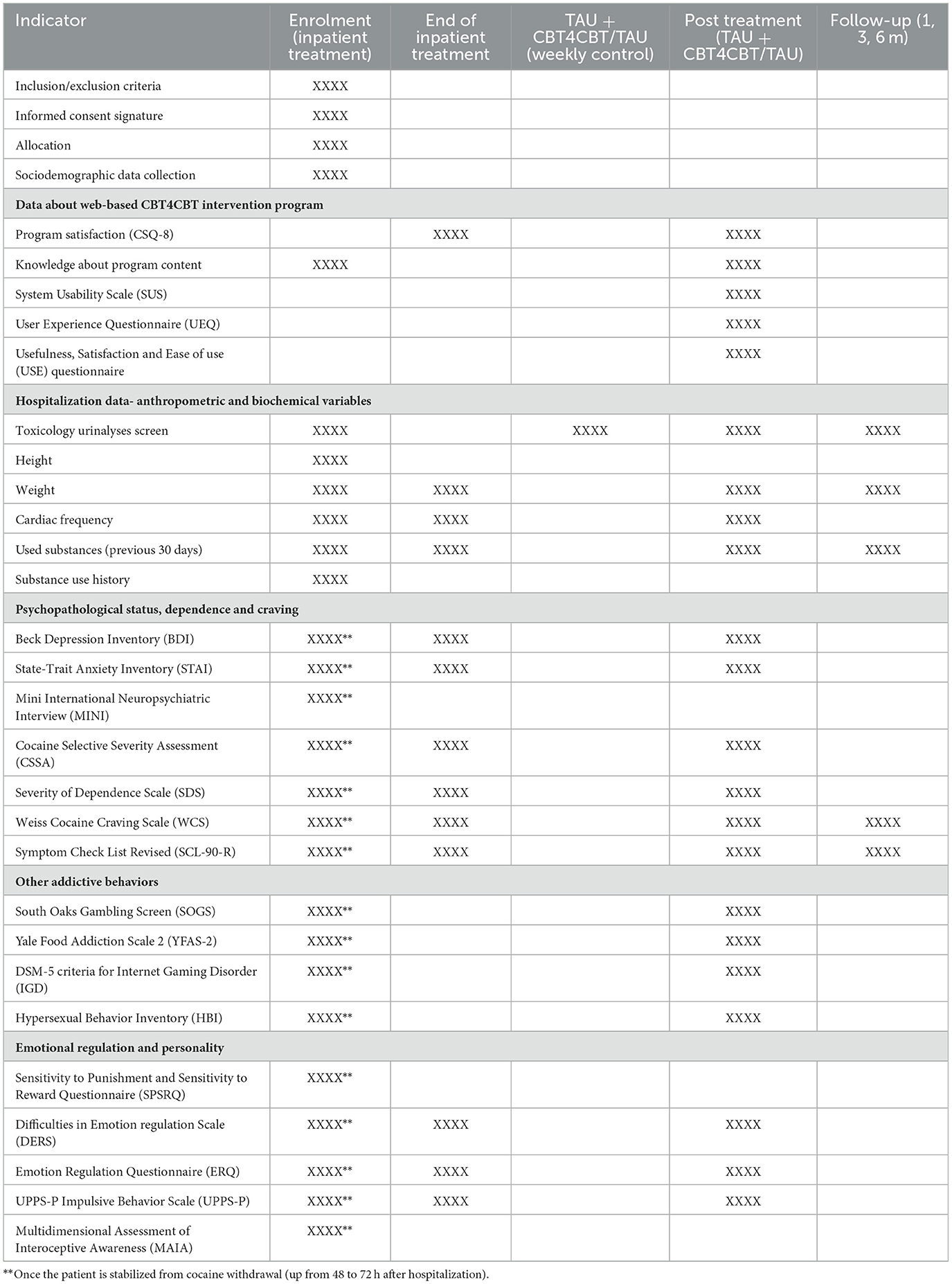
Table 2. Schedule of enrolment, interventions and assessments.
Primary outcome measures will be treatment dropout (two consecutive failures to attend and not answering the phone) and relapse (cocaine use: number of positive urine specimens submitted, percent negative urine screens, percent days of abstinence, self-reported frequency of cocaine use). Treatment dropout will be determined throughout the attendance at the appointments with the clinician (TAU or TAU + CBT4CBT), which will be carried out weekly during the 8-week period of treatment and at follow-up points. Relapse will be determined according to the participants' reports and throughout the presence of benzoylecgonine (metabolite of cocaine) in urine assessed with the Kinetic Microparticle Interaction test in a Solution (Roche Diagnostic System, Inc., Sommerville, NJ).
Secondary measures will cover sociodemographic variables and anthropometric measures (weight and high), cocaine craving, psychopathological symptoms and comorbidities, other addictive behaviors, personality traits, emotion regulation skills and CBT4CBT usability as well as treatment satisfaction.
Psychopathological symptoms and comorbid disorders will be assessed with a Clinical interview based on the DSM-5 diagnostic criteria for addictive behaviors, the MINI international neuropsychiatric interview (23), the Symptom CheckList-90 items-Revised (SCL-90-R) (24, 25), The State-Trait Anxiety Inventory (STAI) (26, 27) and the Beck's Depression Inventory (BDI) (28, 29). Craving and compulsive drug use will be measured with the following self-reported questionnaires: Severity of Dependence Scale (SDS) (30, 31), Cocaine Selective Severity Assessment (CSSA) (32, 33), Weiss Craving Scale (WCS) (34, 35). Other addictive behaviors will be measured, including gambling with the South Oaks Gambling Screen (SOGS) (36, 37), food with the Yale Food Addiction Scale 2 (YFAS) (38, 39), gaming with the DSM-5 criteria for internet gaming disorder (IGD) (40, 41) and sexuality with the Hypersexual Behavior Inventory (HBI) (42, 43).
Different facets of emotion regulation will be assessed with the following self-reported questionnaires: Difficulties in Emotion Regulation Scale (DERS) (44, 45), Emotion regulation questionnaire (ERQ) (46, 47), and Multidimensional Assessment of Interoceptive Awareness (MAIA) (48, 49). Impulsive related traits will be measured with the UPPS-P Impulsive Behavior Scale (50, 51) and the Sensitivity to Punishment and Sensitivity to Reward Questionnaire (SPSRQ) (52). Finally, treatment satisfaction will be assessed through the Client Satisfaction Questionnaire (CSQ-8) (53, 54), usability of the intervention will be assessed using the System Usability Scale (SUS) (55, 56), user experience will be assessed by the User Experience Questionnaire (UEQ) (57, 58) and usefulness, satisfaction and ease of use will be assessed with the Usefulness, Satisfaction and Ease of Use (USE) questionnaire (59, 60).
Statistical programs SPSS 26.0 and Stata 15.1 for Windows will be used. The primary objectives of this study will be carried out through cox regression models. In addition, repeated measures ANOVA will also be performed to assess whether there is a time effect on the primary measures (treatment dropout and/or relapse) as well as secondary (craving, psychopathological state, recent cocaine use emotion regulation scores, trait impulsivity, other addictive behaviors) measures. In addition, these scores will be compared between the two treatment groups using a mixed model of repeated measures. All statistical tests will be two-tailed and will be considered significant if p <0.05. Also, for the characterization of the differences between men and women group comparisons will be conducted by means of chi-square tests (categorical variables) and t-tests (continuous variables). Finally, generalized linear models will be implemented to assess the psychopathological factors associated with treatment response. The need for the analyses to be adjusted for potential confounding variables that could introduce a bias in the results will be considered (e.g.,: age, psychopathology, among others). Especially if the study groups present an imbalance with confounding variables reported in previous literature.
CBT4CBT is a CBT web-based treatment which concomitant to TAU has shown to improve current treatments in multiple US-based studies (18–20). However, up to date it has never been implemented in Spain.
This study aims to improve current evidence-based treatments for severe CUD (that requires inpatient treatment) through the implementation of a more intensive and extensive treatment which is grounded on a web-based CBT approach (CBT4CBT). Additionally, predictive factors for treatment outcome will be assessed. The main strength and contribution of this study will be the enhancement of CUD treatment, using a concomitant web-based treatment approach to TAU. CBT4CBT has the potential to optimize current treatments by facilitating daily access to it when needed. This study also explores different secondary measures (i.e., sociodemographic, cocaine use related variables, craving, personality traits, as well as comorbid psychopathology and other addictive behaviors) that can help to better understand predictive factors of treatment outcomes at two different clinical settings (i.e., inpatients treatment and day care treatment + CBT4CBT) and at 6 different time points (end of each treatment setting and at three different follow-up points−1, 3, and 6 months after treatment-). This can lead to the possibility of targeting specific characteristics in a population of severe CUD and to individualize treatments accordingly for aiming to a better outcome. Furthermore, this study will take into account a gender perspective and explore gender differences in predictive factors for treatment outcome and the efficacy of CBT4CBT.
The potential limitations of this study are the exclusion of patients with opioid use disorder or any other severe condition that can interfere in the participation or assessment of the study. Additionally, dropout rates are considered as treatment outcome although participants can dropout before starting CBT4CBT or TAU after arm allocation which would limit the power of the analysis. Finally, some patients will not be able to join the study if they live in a different area or attend to another treatment than day care. This is required for enabling the implementation of the full treatment and may be strength for homogeneity but it can also limit the generalization of results.
The study was approved by the Research Ethics Committee of the Hospital de la Santa Creu i Sant Pau, project number IIBSP-CBT4CBT-2020-1116. The study will be carried out in accordance with the Declaration of Helsinki and Good Clinical Practices ethical principles. All participants will be informed about the study and they will have to provide informed consent for participation before their inclusion. This study does not pose any risk to the participants. Central Clinical Research and Clinical Trials Unit of Research Institute of the Hospital de Sant Pau will monitor through periodic visits the correct progression of the project, notifying protocol deviations. They will be aware of every single step of the project.
NM-B designed the study with the collaboration of JT and SD-S. NM-B, JT, SD-S, FB, and MM were involved in the set-up of the study in the clinical settings. NM-B and AP-L drafted the manuscript. JT, SD-S, FB, and MM critically reviewed the manuscript. All authors read and approved the final version of the manuscript.
This study was financed by a governmental grant from the Spanish Ministry of Science, Innovation and Universities, Instituto Carlos III (ISCIII) (FIS PI20/00929) and co-funded by FEDER funds a way to build Europe, and Fundació Privada Hospital de la Santa Creu i Sant Pau (Pla d'acció social 2020). The funding sources have played no role in the study design or preparation of this protocol and will have no role in the execution of the study, analyses and interpretation of data, or decision to submit results for publication.
We thank all the addictive behaviors unit team of Hospital de la Santa Creu i Sant Pau that run the treatment as usual for the patients of the unit, thus without their work the present study would not be feasible.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CUD, cocaine use disorder; TAU, treatment as usual; CBT, cognitive behavioral therapy; CBT4CBT, specific web-based cognitive behavioral therapy; CM, contingency management; RCT, randomized controlled clinical trial; WHO, World Health Organization; UNODC, United Nations Office on Drugs and Crime; SCL-90-R, Symptom Checklist-Revised; STAI, State-Trait Anxiety Inventory; BDI, Beck Depression Inventory; SDS, Severity of Dependence Scale; CSSA, Cocaine Selective Severity Assessment; WCS, Weiss Cocaine Craving Scale; SOGS, South Oaks Gambling Screen; YFAS, Yale Food Addiction Scale; IGD, Internet Gaming Disorder; HBI, Hypersexual Behavior Inventory; SPSRQ, Sensitivity to Punishment and Sensitivity to Reward Questionnaire; UPPS-P, UPPS-P Impulsive Behavior Scale; DERS, Difficulties in Emotional Regulation Scale; ERQ, Emotion Regulation Questionnaire; MAIA, Multidimensional Assessment for Interoceptive Awareness; CSQ-8, Client Satisfaction Questionnaire; SUS, System of Usability Scale; UEQ, User Experience Questionnaire; USE, Usefulness, Satisfaction and Ease of Use (USE).
1. Clinical Guidelines on Drug Misuse Dependence Update 2017 Independent Expert Working Group. Drug Misuse and Dependence: UK guidelines on clinical management. Medical Pharmacology at a Glance (2017). p. 68–9. Available online at: https://www.gov.uk/government/publications/drug-misuse-and-dependence-uk-guidelines-on-clinical-management
2. World Health Organization & United Nations Office on Drugs and Crime. International Standards for the Treatment of Drug Use Disorders: Revised Edition Incorporating Results of Field-Testing (2020). p. 121–228.
3. European Monitoring Centre for Drugs and Drug Addiction. European Drug Report. Trends and Developments (2021). Office of the European Union, Luxembourg (2021).
4. UNODC. Drug Market Trends : Cocaine Amphetamine-. United Nations publication, Sales No. E.21.XI.8 (2021). Booklet 4.
5. Kampman KM. The treatment of cocaine use disorder. Sci Adv. (2019) 5:1–8. doi: 10.1126/sciadv.aax1532
6. Chan B, Kondo K, Freeman M, Ayers C, Montgomery J, Kansagara D. Pharmacotherapy for cocaine use disorder—a systematic review and meta-analysis. J Gen Intern Med. (2019) 34:2858–73. doi: 10.1007/s11606-019-05074-8
7. Bentzley BS, Han SS, Neuner S, Humphreys K, Kampman KM, Halpern CH. Comparison of treatments for cocaine use disorder among adults: a systematic review and meta-analysis. JAMA Netw Open. (2021) 4:1–22. doi: 10.1001/jamanetworkopen.2021.8049
8. Petitjean SA, Dürsteler-MacFarland KM, Krokar MC, Strasser J, Mueller SE, Degen B, et al. A randomized, controlled trial of combined cognitive-behavioral therapy plus prize-based contingency management for cocaine dependence. Drug Alcohol Depend. (2014) 145:94–100. doi: 10.1016/j.drugalcdep.2014.09.785
9. Carroll KM, Rounsaville BJ. Contrast of treatment-seeking and untreated cocaine abusers. Arch Gen Psychiatry. (1992) 49:464–71. doi: 10.1001/archpsyc.1992.01820060044007
10. De Crescenzo F, Ciabattini M, D'Alò GL, De Giorgi R, Del Giovane C, Cassar C, et al. Comparative efficacy and acceptability of psychosocial interventions for individuals with cocaine and amphetamine addiction: a systematic review and network meta-analysis. PLoS Med. (2018) 15:e1002715. doi: 10.1371/journal.pmed.1002715
11. Carroll KM, Rounsaville BJ, Gawin FH. A comparative trial of psychotherapies for ambulatory cocaine abusers: relapse prevention and interpersonal psychotherapy. Am J Drug Alcohol Abuse. (1991) 17:229–47. doi: 10.3109/00952999109027549
12. Trujols J, Luquero E, Siñol N, Bañuls E, Tejero A, Batlle F, et al. Técnicas de intervención cognitivo-conductuales para el tratamiento de la dependencia a la cocaína. Actas Españolas Psiquiatr. (2007) 35:190–8.
13. Milligan CO, Nich C, Carroll KM. Ethnic differences in substance abuse treatment retention, compliance, and outcome from two clinical trials. Psychiatr Serv. (2004) 55:167–73. doi: 10.1176/appi.ps.55.2.167
14. Carroll K. Terapy Manuals for Drug Addiction, Manual 1: A Cognitive-Behavioral Approach: Treating Cocaine Addiction. National Institute on Drug Abuse. (1998). doi: 10.1037/e597502007-001
15. Strecher VJ, Shiffman S, West R. Randomized controlled trial of a web-based computer-tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction. (2005) 100:682–8. doi: 10.1111/j.1360-0443.2005.01093.x
16. Japuntich SJ, Zehner ME, Smith SS, Jorenby DE, Valdez JA, Fiore MC, et al. Smoking cessation via the internet: a randomized clinical trial of an internet intervention as adjuvant treatment in a smoking cessation intervention. Nicotine Tob Res. (2006) 8:59–67. doi: 10.1080/14622200601047900
17. Schaub M, Sullivan R, Haug S, Stark L. Web-based cognitive behavioral self-help intervention to reduce cocaine consumption in problematic cocaine users: randomized controlled trial. J Med Internet Res. (2012) 14:e166. doi: 10.2196/jmir.2244
18. Carroll KM, Kiluk BD, Nich C, Gordon MA, Portnoy GA, Marino DR, et al. Computer-assisted delivery of cognitive-behavioral therapy: efficacy and durability of cbt4cbt among cocaine-dependent individuals maintained on methadone. Am J Psychiatry. (2014) 171:436–44. doi: 10.1176/appi.ajp.2013.13070987
19. Carroll KM, Ball SA, Martino S, Nich C, Babuscio TA, Nuro KF, et al. Computer-assisted delivery of cognitive-behavioral therapy for addiction: a randomized trial of CBT4CBT. Am J Psychiatry. (2008) 165:881–8. doi: 10.1176/appi.ajp.2008.07111835
20. Carroll KM, Ball SA, Martino S, Nich C, Babuscio TA, Rounsaville BJ. Enduring effects of a computer-assisted training program for cognitive behavioral therapy: a 6-month follow-up of CBT4CBT. Drug Alcohol Depend. (2009) 100:178–81. doi: 10.1016/j.drugalcdep.2008.09.015
21. Decker SE, Kiluk BD, Frankforter T, Babuscio T, Nich C, Carroll KM. Just showing up is not enough: homework adherence and outcome in cognitive-behavioral therapy for cocaine dependence. J Consult Clin Psychol. (2016) 84:907–12. doi: 10.1037/ccp0000126
22. Carroll KM, Ph D. Cognitive-Behavioral Coping Skills Treatment for Cocaine Dependence. Yale University Psychotherapy Development Center (1997).
23. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59:22–33.
24. Derogatis L, Cleary PA. Confirmation of the dimensional structure of the scl-90: a study in construct validation. J Clin Psychol. (1977) 33:981–9.
25. Londoño NH, Agudelo DM, Marínez E, Anguila D, Aguirre DC, Arias JF. Validación del cuestionario de 90 síntomas SCL-90-R de Derogatis en una muestra clínica colombiana. MedUNAB. (2018) 21:45–9. doi: 10.29375/01237047.2807
27. Spielberger CD, Gorsuch RL, y, Lushene RE. Manual STAI, cuestionario de ansiedad estado rasgo.adaptación española. Tea Ediciones (1997). p. 7–16. Available online at: http://www.web.teaediciones.com/Ejemplos/STAI-Manual-Extracto.pdf
28. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression the difficulties inherent in obtaining. Arch Gen Psychiatry. (1960) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
29. Sanz J, Luis A, Carmelo P, Resumen V. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. propiedades psicométricas en población general. Clínica y Salud. (2003) 14:249−80.
30. Gossop M, Darke S, Griffiths P, Hando J, Powis B, Hall W, et al. The severity of dependence scale (SDS): psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction. (1995) 90:607–14. doi: 10.1046/j.1360-0443.1995.9056072.x
31. Vélez-Moreno A, González-Saiz F, Ramírez López J, Torrico Linares E, Fernández-Calderón FJ, Rojas A, et al. Adaptación al español de la Substance Dependence Severity Scale: resultados preliminares. Adicciones. (2013) 25:339. doi: 10.20882/adicciones.36
32. Pérez de los Cobos J, Trujols J, Siñol N, Vasconcelos e Rego L, Iraurgi I, Batlle F. Psychometric properties of the Spanish version of the cocaine selective severity Assessment to evaluate cocaine withdrawal in treatment-seeking individuals. J Subst Abuse Treat. (2014) 47:189–96. doi: 10.1016/j.jsat.2014.05.004
33. Kampman KM, Volpicelli JR, McGinnis DE, Alterman AI, Weinrieb RM, D'Angelo L, et al. Reliability and validity of the cocaine selective severity assessment. Addict Behav. (1998) 23:449–61. doi: 10.1016/S0306-4603(98)00011-2
34. Weiss RD, Griffin ML, Hufford C. Craving in hospitalized cocaine abusers as a predictor of outcome. Am J Drug Alcohol Abuse. (1995) 21:289–301. doi: 10.3109/00952999509002698
35. Tejero A, Trujols J, Siñol N. Evaluación del craving de cocaína. In:Pérez de los Cobos J, Tejero A, Trujols J, , editor. Instrumentos clínicos para la evauación de la dependencia de la cocaína. Barcelona: Ars Médica (2003). p. 23–50.
36. Echeburúa-Odriozola E, Báez-Gallo C, Fernández-Montalvo J, Páez-Rovida D. Cuestionario De Juego Patologico De South Oaks (SOGS): Validacion Española. Análisis y Modif Conduct. (1994) 20:769–91.
37. Stinchfield R. Reliability, validity, and classification accuracy of the South Oaks Gambling Screen (SOGS). Addict Behav. (2002) 27:1–19. doi: 10.1016/S0306-4603(00)00158-1
38. Gearhardt AN, Corbin WR, Brownell KD. Preliminary validation of the yale food addiction scale. Appetite. (2009) 52:430–6. doi: 10.1016/j.appet.2008.12.003
39. Stengel A, Von Wietersheim J, Albayrak Ö, Jiménez-Murcia S, Fernández-Aranda F, Granero R, et al. Validation of the Spanish version of the yale food addiction scale 2. 0 (YFAS 20) and clinical correlates in a sample of eating disorder, gambling disorder, and healthy control participants spanish validation of YFAS 20. Front Psychiatry. (2018) 1:208. doi: 10.3389/fpsyt.2018.00208
40. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th edition. American Psychiatric Publishing (2013). doi: 10.1176/appi.books.9780890425596
41. Asociación Americana de. Psiquiatría. Manual diagnóstico y estadístico de los trastornos mentales (DSM-5) 5a edición Editorial Médica Panamericana. (2014).
42. Ballester-Arnal R, Castro-Calvo J, Gil-Juliá B, Giménez-García C, Gil-Llario MD. A validation study of the Spanish version of te Hypersexual Behavior Inventory (HBI): paper-and-pencil versus online administration. J sex Marital Ther. (2019) 45:283–302. doi: 10.1080/0092623X.2018.1518886
43. Reid RC, Garos S, Carpenter BN. Reliability, validity, and psychometric development of the hypersexual behavior inventory in an outpatient sample of men. Sex Addict Compulsivity. (2011) 18:30–51. doi: 10.1080/10720162.2011.555709
44. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
45. Hervás G, Jódar R. The Spanish version of the difficulties in emotion regulation scale. Clin y Salud. (2008) 19:139–56.
46. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. (2003) 85:348–62. doi: 10.1037/0022-3514.85.2.348
47. Cabello R, Salguero JM, Fernández-Berrocal P, Gross JJ. A Spanish adaptation of the emotion regulation questionnaire. Eur J Psychol Assess. (2013) 29:234–40. doi: 10.1027/1015-5759/a000150
48. Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, Stewart A. The Multidimensional assessment of interoceptive awareness (MAIA). PLoS ONE. (2012) 7:48230. doi: 10.1371/journal.pone.0048230
49. Valenzuela-Moguillansky C, Reyes-Reyes A. Psychometric properties of the multidimensional assessment of interoceptive awareness (MAIA) in a Chilean population. Front Psychol. (2015) 6:120. doi: 10.3389/fpsyg.2015.00120
50. Verdejo-García A, Lozano Ó, Moya M, Alcázar MÁ, Pérez-García M. Psychometric properties of a spanish version of the UPPS-P impulsive behavior scale: reliability, validity and association with trait and cognitive impulsivity. J Pers Assess. (2010) 92:70–7. doi: 10.1080/00223890903382369
51. Whiteside SP, Lynam DR, Miller JD, Reynolds SK. Validation of the UPPS impulsive behaviour scale: a four-factor model of impulsivity. Eur J Pers. (2005) 19:559. doi: 10.1002/per.556
52. Torrubia R, Avila C, Molto J, Caseras X. The sensitivity to punishment and sensitivity to reward questionnaire. Pers Individ Dif. (2001) 31:837–62. doi: 10.1016/S0191-8869(00)00183-5
53. Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD. Assessment of client/patient satisfaction: development of a general scale. Eval Program Plann. (1979) 2:197–207. doi: 10.1016/0149-7189(79)90094-6
54. Roberts RE, Attkisson CC. Assessing client satisfaction among hispanics. Eval Program Plann. (1983) 6:401–13. doi: 10.1016/0149-7189(83)90019-8
55. Del Rocio Sevilla-Gonzalez M, Loaeza LM, Lazaro-Carrera LS, Ramirez BB, Rodríguez AV, Peralta-Pedrero ML, et al. Spanish version of the system usability scale for the assessment of electronic tools: development and validation. JMIR Hum Factors. (2020) 7:1–7. doi: 10.2196/21161
56. Jordan PW, Thomas B, Weerdmeester BA, McClelland IL. Usability Evaluation In Industry. Taylor & Francis (1996). doi: 10.1201/9781498710411
57. Laugwitz B, Held T, Schrepp M. Construction and evaluation of a user experience questionnaire. HCI Usability Educ Work. (2008) 5298:63–76. doi: 10.1007/978-3-540-89350-9_6
58. Rauschenberger M, Schrepp M, Perez-Cota M, Olschner S, Thomaschewski J. Efficient measurement of the user experience of interactive products. how to use the user experience questionnaire (UEQ)example: Spanish language version. Int J Interact Multimed Artif Intell. (2013) 2:39–45. doi: 10.9781/ijimai.2013.215
Keywords: cocaine use disorder, treatment, cognitive behavioral therapy, treatment outcome, gender, predictive factors, clinical trial, protocol
Citation: Mallorquí-Bagué N, Palazón-Llecha A, Madre M, Batlle F, Duran-Sindreu S and Trujols J (2023) CBT4CBT web-based add-on treatment for cocaine use disorder: Study protocol for a randomized controlled trial. Front. Psychiatry 14:1051528. doi: 10.3389/fpsyt.2023.1051528
Received: 22 September 2022; Accepted: 13 February 2023;
Published: 02 March 2023.
Edited by:
Yasser Khazaal, Université de Lausanne, SwitzerlandReviewed by:
Miriam Engels, Open University of the Netherlands, NetherlandsCopyright © 2023 Mallorquí-Bagué, Palazón-Llecha, Madre, Batlle, Duran-Sindreu and Trujols. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Núria Mallorquí-Bagué, bm1hbGxvcnF1aUBsaXZlLmNvbQ==; bnVyaWEubWFsbG9ycXVpQHVkZy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.