 Jigyansa Ipsita Pattnaik
Jigyansa Ipsita Pattnaik Udit Kumar Panda1
Udit Kumar Panda1 Susanta Padhy
Susanta Padhy- 1Department of Psychiatry, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India
- 2Child and Adolescent Psychiatry, St. Johns Medical College and Hospital, Bengaluru, India
- 3Department of Psychiatry, All India Institute of Medical Sciences Bhubaneswar, Bhubaneswar, Odisha, India
With proliferation in research on high-risk psychosis spectrum diseases, it is crucial to distinguish a prodrome or psychosis-like episode in children and adolescents from true psychosis. The limited role of psychopharmacology in such circumstances is well-documented, underlining the difficulties in diagnosing treatment resistance. To add to the confusion is emerging data on the head-to-head comparison trials for treatment-resistant and treatment-refractory schizophrenia. Clozapine, the gold-standard drug for resistant schizophrenia and other psychotic psychopathology, lacks FDA or manufacturer guidelines for use in the pediatric population. Possibly due to developmental pharmacokinetic (PK) considerations, clozapine-related side effects are more commonly seen in children than adults. Despite evidence of an increased risk for seizures and hematological problems in children, clozapine is widely used off-label. Clozapine reduces the severity of resistant childhood schizophrenia, aggression, suicidality, and severe non-psychotic illness. There is inconsistent prescribing, administration, and monitoring of clozapine, and limited database evidence-backed guidelines. Despite the overwhelming efficacy, problems remain regarding unambiguous indications of use and risk-benefits assessments. This article reviews the nuances in the diagnosis of treatment resistance psychosis in childhood and adolescents and its management, in particular highlighting the evidence base for clozapine in this population group.
1. Introduction
The phrase “childhood-onset psychosis (COP)” was initially subsumed under the description of pervasive developmental disorder (PDD). In the DSM-V or ICD-11, the symptomatology and stated definitions/criteria of psychotic illnesses remain the same for children, adolescents, and adults (1, 2). Imaginative play and fantasy are frequent in young children and early teens. Children's imaginations and fantasy lives, combined with language and cognitive development stages, influence diagnostic accuracy, particularly when distinguishing between Childhood-Onset Schizophrenia (COS), Mood Disorders such as Bipolar Affective disorder (BPAD) or Major Depressive disorder (MDD), obsessive-compulsive disorder (OCD), and Attention-Deficit/Hyperactivity Disorders (ADHD) (1). The term “Psychosis Not Otherwise Specified (PNOS)” has been used to fill diagnostic gaps in instances with an ambiguous presentation. Neurocognitive issues are common in the absence of pathognomonic symptoms. Though there are no definite biochemical or neuroimaging indicators, psychosis may be an indication of widespread brain dysfunction. Pharmacotherapy for children and adolescents is primarily based on evidence from adult psychosis research. There has been little investigation in the domain of psychosocial and psychotherapy interventions for childhood psychosis as well (3).
As a result, it is important to first comprehend the idea of Childhood psychosis, followed by concerns about management. Clozapine's role in adults with treatment-resistant psychosis is well-established; however, evidence for its usage in children is lacking. This chapter will investigate the current level of validity of the notion of treatment-resistant psychosis in children, as well as outline existing guidelines for diagnosis and therapy in this population, with a particular emphasis on the evidence base for clozapine in this cohort.
2. The construct of childhood-onset psychosis
DSM-V uses positive symptoms like delusions and hallucinations as well as disorganization in speech and behavior and negative symptoms to diagnose cases of Schizophrenia (4). Hallucinations and delusions are clinically frequently used to diagnose psychosis. But these symptoms are not exclusive to psychosis; they can also be found in trauma, seizure disorders, and other medical illnesses as well as other psychiatric condition of mood disorder and dissociative disorders. A normal child with a busy imagined life can misinterpret thoughts as real events and insist vehemently that a thought or dream occurred (1), which may the criteria for hallucination and delusion, posing diagnostic challenge.
Psychotic symptoms are difficult to distinguish from symptoms associated with other mental illnesses. The table below lists a few considerations to be kept in mind while making a diagnosis of Childhood Psychosis (1, 5, 6).
Language and cognition deficiencies compromise diagnostic precision in younger age groups. The diagnosis is typically valid for older adolescents, a time when first episodes are widespread. Non-specific symptoms such as anxiety, concentration impairments, and irritability may occur before a psychotic episode. This could result in a misdiagnosis.
2.1. Schizophrenia prodrome and psychosis-risk syndrome
The emergence of psychotic symptoms in schizophrenia is preceded by a period of mood, perception, cognitive, and social decline that can span from weeks to years. This is especially true for children and adolescents (7). Under the “At-Risk Mental State (ARMS).” Three groups have been identified.
(i) Brief Limited Psychotic Symptoms [BLIPS]- patients experiencing transient psychotic symptoms.
(ii) Attenuated Psychotic Symptoms [APS]- patients with sub-threshold Psychotic symptoms of recent onset.
(iii) Genetic Risk Plus Functional Decline- people who have a first-degree relative (FDR) with schizophrenia and who are now experiencing a deterioration in their functional capacity, or with a diagnosis of schizotypal personality disorder.
Commonly utilized instruments include Comprehensive Assessment of “At- Risk Mental States” (CAARMS) and Structured Interview for Prodromal Symptoms (SIPS).
2.2. Prevalence of childhood psychosis as compared to childhood onset mood disorder
Epidemiological evidence implies childhood psychosis is infrequent. Schizophrenia starting in mid-to-late adolescence is 1 percent, whereas Childhood Onset Schizophrenia (COS) is 0.2–0.4 per 10,000 people (8). A landmark study on COS included 1,400 country-wide referrals during a 10-year period (9) where 71 patients met COS criteria at study entry, and 54 children (76%) retained the diagnosis at 10 years. Thus, reflecting that about a quarter of children do not retain the diagnosis after 10 years.
When it comes to affective disorder, 1% of kids and 5% of adolescents suffer from MDD, while 1–2% of people are diagnosed with BPAD. Thus, the prevalence of a pediatric mood disorder is more common.
2.3. Do psychotic symptoms imply a diagnosis of schizophrenia?
Childhood psychotic symptoms may be linked to other mental disorders than to schizophrenia (e.g., MDD, BPAD, or dissociative states) (10). A child with a bipolar episode may have hallucinations, delusions, mania, depression, or both. Children with schizophrenia show more formal thought disorder, negative symptoms (e.g., apathy and social withdrawal), and violence (10). Autism spectrum disorders (ASD) can present with oddities in thought like schizophrenia (e.g., the idea that they can talk to their favorite inanimate toys) (11, 12). Misdiagnosis of psychosis can occur with milder forms of autism, like Asperger's syndrome because of unusual perspectives, social difficulties, and concrete brain processes (12) (Table 1). Psychotherapeutic and/or social therapy can relieve psychotic symptoms in children with traumatic hallucinations (usually coupled with nightmares and trance-like states) (11).
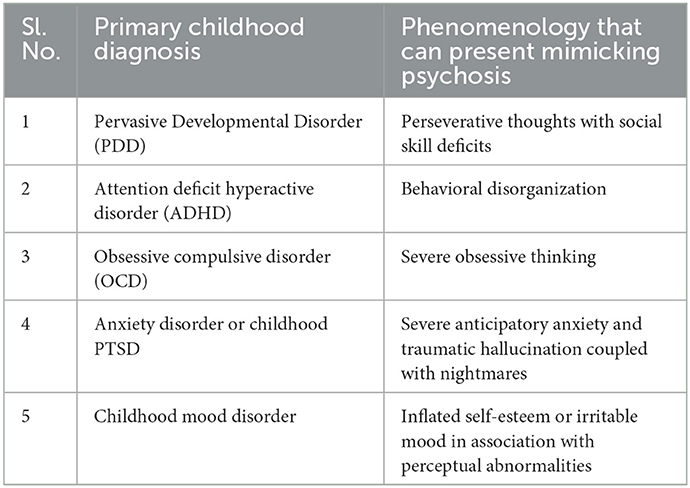
Table 1. Phenomenology in other childhood diagnosis mimicking psychosis.
2.3.1. Medical conditions presenting with psychosis
There is a wide range of medical diseases associated with psychotic symptoms. Lesions of the central nervous system, whether from disease, trauma, or drug abuse, can trigger psychosis (13). The detailed list of Medical Diagnoses related to Psychotic Episodes is beyond the scope of this chapter. However, before making a diagnosis of primary psychotic disease, it is necessary to rule out secondary causes through a comprehensive medical evaluation.
2.4. Phenomenology of childhood psychosis
• Hallucinations and delusions are common in youngsters. Psychotic symptoms aren't a benign occurrence, but they don't always indicate schizophrenia (10).
• Other mental disorders (e.g., depression, anxiety, ADHD, posttraumatic states, and autism spectrum disorders) or medical conditions can cause psychotic symptoms in children and adolescents (10). Prodromal signs often precede psychosis onset.
• For the pharmacological therapy of psychotic symptoms in children, the clinician should choose the proper medication and dose, and then monitor therapeutic results and adverse effects.
2.5. Development and cognition associated with psychosis in children
2.5.1. Neurodevelopmental delays
COS children usually exhibit early developmental difficulties. Subtle motor impairments, hypo/hypertonia, sensory processing and integration difficulties, and language delays (14). Pervasive Developmental Disorder (PDD) is indicated by hand flapping, persistent smelling, and touching. Attention difficulties, distractibility, and executive functioning impairment may signal a poor prognosis. Developmental delays and cognitive deficits are seen in schizophrenia spectrum disorders. COS children often have expressive and receptive language impairments that cause cognitive disorder and disorganization (14).
2.5.2. Neurocognition
Literature states children with childhood-onset schizophrenia (COS) have lower IQs than normal children (14). Lower IQ scores possibly reflect a prior neurodevelopmental disorder in such children. Children with schizophrenia often have concentration, memory, and movement problems (14). MRI studies found a link between hippocampal volume and raw information subtest score, possibly reflecting a neuro-biological co-relate for impairment in cognitive function. A decrease in IQ is reported in children with COS during their adolescent period. It is described to be probably due to their inability to master new abilities and is not a regression in pre-existing cognitive reserves. The correlation of schizophrenia with IQ is however highly debated.
2.6. Assessment and diagnosis
2.6.1. Screening instruments
Screening instruments can assist discover psychiatric diseases linked with psychotic symptoms before a formal diagnosis is made. Screening instruments in children and adolescents include the Brief Psychiatric Rating Scale for Children (BPRS-C) for psychosis. Children's Depression Inventory (15) for depression and Young Mania Rating Scale (C-YMRS) for mania.
2.6.2. Semi-structured diagnostic interviews
Standardized diagnostic instruments are useful for a number of reasons, including: establishing diagnostic stability; examining symptom dimensions; defining clinical characteristics; and stating predictive validity.
The Schedule for Affective Disorders and Schizophrenia -Present and Lifetime Version (K-SADS-PL) (16), the Diagnostic Interview for Children and Adolescents (DICA) (17), and the Diagnostic Interview Schedule for Children (DISC) (18), are reliable measures for diagnosing MDD, BPAD, COS, and other psychiatric disorders.
2.6.3. Rating scales
Rating scales can help assess psychotic illness symptoms during therapy and over time once a diagnosis has been made. The Child Depression Rating Scale (CDRS) (19) and the Kiddie Version of the Positive and Negative Symptoms of Schizophrenia (K-PANSS) (20) are both effective pediatric COS rating scales. The Clinical Global Impressions-Severity and Improvement (CGI-S and CGI-I) scales, as well as the Clinical Global Assessment of Function (CGAF), assess psychiatric impairment at diagnosis and over time.
2.7. Course and prognosis of psychosis in children and adolescents
The symptoms of psychosis in children tend to fluctuate widely over time. However, they might also be a signs of an evolving syndromal psychotic disorder. A birth cohort (10) (n = 761) was administered structured diagnostic interviews at ages 11 and 26 to assess symptom prediction. The group was split based on hallucinations or delusions, their severity, and other psychotic symptoms. No child had COS. By the age of 26, those with core symptoms were 16 times more likely to have schizophreniform disorder, and 90% of them had adult occupational and social problems. Even those with mild symptoms were more likely to have adult schizophreniform illness. Forty-two percent of schizophreniform individuals diagnosed at age 26 had weak or significant symptoms at age 11.
An insidious onset pattern is more common in young children before the age of 11 or 12 and has a poorer outcome (5).
Childhood Onset Schizophrenia (COS) is severe, impairs development, and has a poor prognosis. Sixty-seven percent of COS had premorbid social, motor, and language problems, learning impairments, and mood or anxiety disorders (5). Before psychotic episodes, 27% of COS met Autism/ASD criteria. Developmental abnormalities predict prognosis and outcome (5, 21). The consequences of a wrong diagnosis of COS might be severe. Although psychotic symptoms are common (up to 5%) in otherwise healthy youngsters, a diagnosis of Schizophrenia is unlikely. About 30–50% of kids with affective or atypical symptoms are given a COS diagnosis when they shouldn't be, and 90% of kids with a COS diagnosis end up getting another diagnosis (22).
2.8. Management of psychosis in children and adolescents
There are three types of childhood psychosis that require different approaches to treatment:
(i) Childhood schizophrenia,
(ii) Depression with psychotic symptoms, and
(iii) Psychosis associated with bipolar affective disorder.
Substance-induced psychosis, medical-related psychosis, and delirium are all treated with antipsychotic medications. In cases where diagnosis is uncertain, like Psychosis NOS, that cannot be properly understood as schizophrenia or a mood illness, it important to wait and watch with close monitoring and offering psychological therapies and social intervention, however in case of severe aggression or agitation neuroleptic and other psychotropic uses should be instituted promptly.
2.8.1. Treatment of childhood onset schizophrenia (COS)
The second -generation antipsychotics are the mainstay of therapy because they cause fewer extrapyramidal symptoms in COS. The Cochrane review of six clinical trials with 256 children and adolescents found limited data to support one antipsychotic medication over another for treating EOS (23). According to the study “Treatment of Early-Onset Schizophrenia Spectrum (TEOSS),” second generation antipsychotics were equally effective in symptom improvement as first generation antipsychotics; clinicians need to be careful about the metabolic side effects of Risperidone and olanzapine in long term follow up (24).
2.8.2. Treatment of psychosis related to pediatric bipolar disorder
Risperidone showed improvement in both psychotic and mood symptoms (25). Use of Olanzapine in children with mania is promising (25). Because atypical antipsychotics have shown good antimanic efficacy in adults, we anticipate similar results for their use in pediatric BPAD.
Divalproex, lithium, and carbamazepine exhibited adequate clinical responses in an open label trial of 42 children and adolescents (aged 8–18 years) with BPAD (25).
2.8.3. Treatment of major depression with psychotic features in childhood
We could not find any open-label study to propose any recommendation for treating psychotic depression in children. A combination of an SSRI like fluoxetine or sertraline in combination with an atypical antipsychotic like olanzapine or risperidone appears to be the rational pharmaceutical approach to treat psychotic depression (26). NICE guidelines recommend intensive psychological therapies along with fluoxetine, augmented with a second-generation antipsychotic medication as the treatment of psychotic depression in children (1, 27).
3. Treatment resistant psychosis in children and adolescents
Treatment Resistant Schizophrenia (TRS) is defined as no significant improvement in positive symptoms following treatment with two non-clozapine antipsychotics at adequate dose, duration, and adherence (28).
The landmark study, Treatment of Early Onset Schizophrenia Spectrum Disorders (TEOSS), concluded that more than half of the study participants did not show improvement after 8 weeks of therapy (24).
According to studies on individuals with schizophrenia, response rates to subsequent non-clozapine antipsychotic medication are lower for patients whose disease did not improve with the first antipsychotic. Up to 30% of chronic schizophrenia patients fulfill criteria for TRS, failing to react to 2 non-clozapine antipsychotics (28, 29). Childhood Schizophrenia studies are scarce. Genetic and imaging correlates show childhood-onset schizophrenia has been a continuum with adult-onset schizophrenia, with a persistent, treatment-resistant illness of insidious onset and chronic morbidity (28). Thus, the criteria used for adults with TRS has been extended and used for studies with TRS among children as well.
Contrary to the agreement on primary features of the TRS definition, guidelines differ on definitions of a lack of treatment response and the target clinical outcome measures for treatment response. The concept of pseudo-resistance can complicate determining treatment response (28). Medication non-adherence, pharmacokinetic issues (e.g., drug-drug interactions), and other comorbidities (e.g., substance use disorders, and other medical conditions) might cause pseudo-resistance. This may be more relevant for childhood schizophrenia.
TRS patients who don't respond to clozapine with good compliance or Electro-convulsive Therapy (ECT) are a subset; these are clozapine-resistant and ECT-resistant schizophrenia. No clear criteria exist for treatment resistance psychosis in childhood onset schizophrenia.
4. Clozapine in children and adolescents
4.1. Clozapine use in treatment-refractory schizophrenia
Very early onset schizophrenia (VEOS) comprises 1% of schizophrenia diagnoses, however they are at significant risk of mortality and disability if treatment is not given efficiently and judiciously. About half of patients with very early-onset schizophrenia (VEOS) do not show adequate clinical response to first line antipsychotics, where clozapine may be useful (23). Despite clozapine's better efficacy for TRS, strangely it has not received not approval from FDA for children and adolescents. Clozapine is the only medicine that helps EOS with treatment resistance, with a better efficacy compared to Olanzapine or Halopreidol (23, 30). Additionally, clozapine has a far reduced risk of extrapyramidal symptoms (EPS) than other antipsychotics. After trying two antipsychotics for 6–8 weeks without improvement, clozapine can be tried. Studies show clozapine is usually utilized after three antipsychotics trial (23). When clozapine is indicated, the hesitancy on the part of psychiatrists for a very rare side effect of bone marrow suppression. there is lack of the lack of substantial evidence-base in children and adolescents regarding the idiosyncratic side effect of agranulocytosis (31).
In past double blind studies, FDA-approved antipsychotic medications such as olanzapine, haloperidol, and quetiapine have been compared with clozapine. Clozapine outperformed quetiapine and risperidone in terms of positive and negative symptom treatment as well as adherence (23). The addition of aripiprazole to clozapine medication may be beneficial in adolescent schizophrenia. Clozapine is recommended for first-episode psychosis (FEP) patients who have not responded well to first-line antipsychotic medications. If patients are not adhering to first-line antipsychotic medications due to side effects or a lack of symptomatic control of psychotic symptoms, initiating Clozapine can be considered (23). Patients with FEP who fail a first-line drug trial are more likely to fail a second drug trial. Given this information and clozapine's demonstrated superiority over other antipsychotics in the treatment of EOS (23), Tungaraza et al. proposed that clozapine be used as a second-line treatment (30, 32). Clozapine significantly reduced hospitalization, suicidality, and substance abuse. Clozapine is usually chosen as the fourth medication, according to studies, and it takes an average of 19.5 months to begin clozapine therapy (30, 32). Early clozapine treatment reduces suicidal behavior and improves cognitive and behavioral outcome.
4.2. Review of evidence of clozapine use in children and adolescents
Few randomized controlled trials on clozapine in children exist, but each provides high level of evidence (33–36) (Table 2).
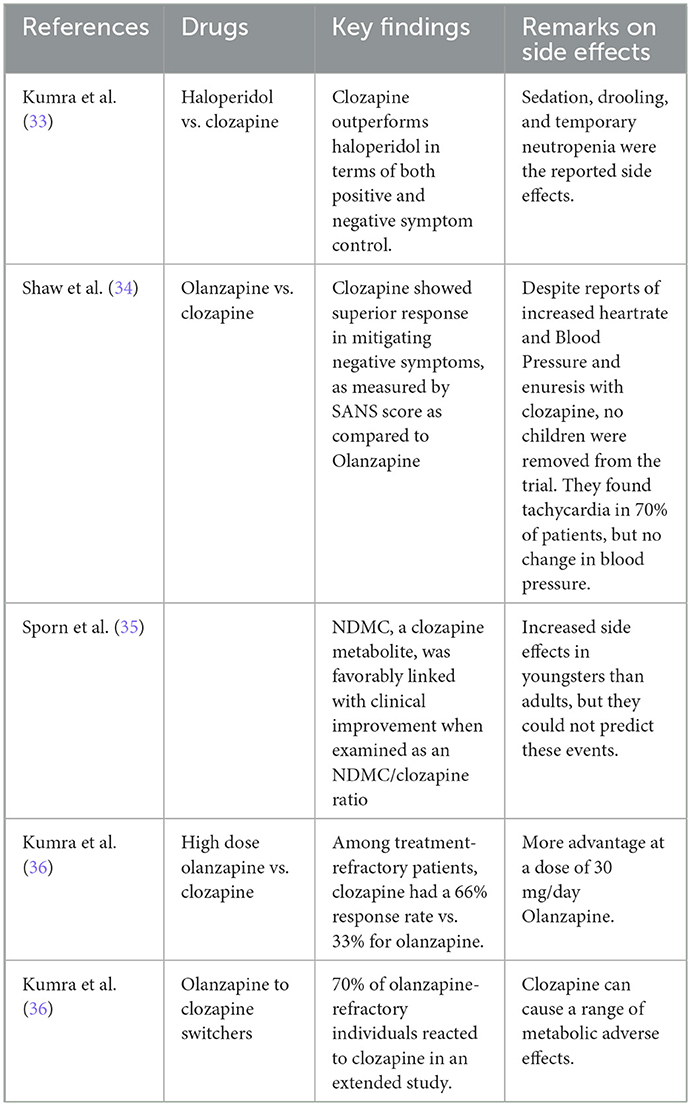
Table 2. Review of evidence of clozapine use in childhood psychosis.
4.3. ADR of clozapine in children and adolescents
Literature states the risk of cardiac and metabolic adverse effects in children taking clozapine is higher than that of the other atypical antipsychotics (aripiprazole, olanzapine, quetiapine, and risperidone) (23, 30). Clozapine related Pediatric and adult pharmacokinetics are similar (23). Clozapine causes higher behavioral problems and white blood cell disorders in children. Despite the gap in reported side effects and the tendency for children to develop metabolic syndrome, children are less likely than adults or elderly patients to encounter any side-event with clozapine (24, 29, 30). Clozapine produces less EPS, neuromotor dysfunction, hyperprolactinemia, and liver damage than other antipsychotics (23, 31, 37). Clozapine-induced cardiomyopathy has led to the discontinuation of the drug (23). In adolescent olanzapine and risperidone causes more weight gain than clozapine according to a study of 51 teens (23, 31). Uncertain side effect profile and incidence of metabolic syndrome, sedation, and drooling are expected with clozapine use (23). However, the available literature is limited to a few case series only; and large, controlled studies are suggested to understand population-based side effects of clozapine.
4.4. Long term use of clozapine
Few studies are available on long-term clozapine use in children (30). 96.2% of Korean patients had fewer hospital days after a year of clozapine (23, 31). Nearly 70% of 24-year cohort trial patients were compliant after 2 years of maintenance (23, 31). Other trials claim safety up to a year without major side effects.
4.5. Recommendations for clozapine use
A recent systematic review (30) and meta-analysis which included four double-blind RCTs, four open label studies, seven observational studies, and three case reports, stated clozapine was well-tolerated and superior in efficacy to other antipsychotics in both short term and long term use, with improvement that sustained during long term follow up. The side-effect profile included sedation, hyper salivation and weight gain commonly and no fatalities reported (30). Severe adverse effects in adolescents are infrequent and outweighed by benefits. Thus, the following recommendations are made:
a. Clozapine should be used for TRS among Children and Adolescents and in some first-line failure patients.
b. Reluctance in clozapine-initiation has been attributed to the risk perceived by clinicians related to use of clozapine, despite evidence that it's safe in children and adolescents. Thus, robust long term follow up studies need to be designed to increase the evidence on safety of use in this cohort.
c. More research is needed on clozapine use in children to develop a consensus or protocol for identifying the target population, minimizing delay in initiation of clozapine and developing a child specific side-effect monitoring checklist.
5. Conclusion
Treatment Resistant Psychosis in children and adolescents poses a challenge in diagnosis and management. A comprehensive clinical history helps clarify diagnostic ambiguities. Majority of patients VEOS who do not respond to first-line anti-psychotics are unlikely to benefit from a second non-clozapine antipsychotic. The hazards of delaying therapy when psychotic-symptoms are not immediately managed with a considerable unwanted rise in morbidity and disability has been highlighted often. When other antipsychotics fail, early access to clozapine improves efficacy in risk–benefit analyses. Clozapine is well-tolerated and superior in efficacy to other antipsychotics in both short term and long term use, with improvement that sustained during long term follow up. Long-term clozapine use in young people increases the risk of metabolic side effects include obesity, insulin resistance, diabetes, and dyslipidemia. These side effects damage life quality, although not as much as untreated psychosis. Clozapine long-term use shows promise but needs additional research.
Author contributions
JP, JR, and UP contributed to the conception and design of the paper. JP, UP, and SC wrote the first draft of the manuscript. All authors wrote different sections of the manuscript, contributed to manuscript revision, read, and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Courvoisie H, Labellarte MJ, Riddle MA. Psychosis in children: Diagnosis and treatment. Dialog Clin Neurosci. (2001) 3:79–92. doi: 10.31887/DCNS.2001.3.2/hcourvoisie
2. Munir KM. The co-occurrence of mental disorders in children and adolescents with intellectual disability/intellectual developmental disorder. Curr Opin Psychiatry. (2016) 29:95–102. doi: 10.1097/YCO.0000000000000236
3. Morrison AP, Pyle M, Byrne R, Broome M, Freeman D, Johns L, et al. Psychological intervention, antipsychotic medication, or a combined treatment for adolescents with a first episode of psychosis: The maps feasibility three-arm RCT. Health Technol Assess. (2021) 25:1–124. doi: 10.3310/hta25040
4. Biedermann F, Fleischhacker WW. Psychotic disorders in DSM-5 and ICD-11. CNS Spectr. (2016) 21:349–54. doi: 10.1017/S1092852916000316
5. Kendhari J, Shankar R, Young-Walker L. A review of childhood-onset schizophrenia. Focus. (2016) 14:328–32. doi: 10.1176/appi.focus.20160007
6. Sheffield JM, Karcher NR, Barch DM. Cognitive deficits in psychotic disorders: A lifespan perspective. Neuropsychol Rev. (2018) 28:509–33. doi: 10.1007/s11065-018-9388-2
7. Gonçalves AM, Dantas Cde, Banzato CE. Values and DSM-5: Looking at the debate on attenuated psychosis syndrome. BMC Medical Ethics. (2016) 17:8. doi: 10.1186/s12910-016-0090-8
8. Gogtay N, Vyas NS, Testa R, Wood SJ, Pantelis C. Age of onset of schizophrenia: Perspectives from structural neuroimaging studies. Schizophr Bull. (2011) 37:504–13. doi: 10.1093/schbul/sbr030
9. Gordon CT, Frazier JA, McKenna K, Giedd J, Zametkin A, Kaysen D, et al. Childhood-onset schizophrenia: An NIMH study in progress. Schizophr Bullet. (1994) 20:697–712. doi: 10.1093/schbul/20.4.697
10. Stevens JR, Prince JB, Prager LM, Stern TA. Psychotic disorders in children and adolescents: A primer on contemporary evaluation and management. Prim Care Companion CNS Disord. (2014) 2014:13f01514. doi: 10.4088/PCC.13f01514
11. Datta SS, Daruvala R, Kumar A. Psychological interventions for psychosis in adolescents. Cochr Datab Systemat Rev. (2020) 2020:CD009533. doi: 10.1002/14651858.CD009533.pub2
12. Trevisan DA, Foss-Feig JH, Naples AJ, Srihari V, Anticevic A, McPartland JC. Autism spectrum disorder and schizophrenia are better differentiated by positive symptoms than negative symptoms. Fronti Psychiatr. (2020) 11:fpsyt.2020.00548. doi: 10.3389/fpsyt.2020.00548
13. Joyce EM. Organic psychosis: The pathobiology and treatment of delusions. CNS Neurosci Ther. (2018) 24:598–603. doi: 10.1111/cns.12973
14. Niemi LT, Suvisaari JM, Tuulio-Henriksson A, Lönnqvist JK. Childhood developmental abnormalities in schizophrenia: Evidence from high-risk studies. Schizophr Res. (2003) 60:239–58. doi: 10.1016/S0920-9964(02)00234-7
16. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for affective disorders and schizophrenia for school-age children-present and Lifetime version (K-SADS-PL): Initial reliability and validity data. J Am Acad Child Adolesc Psychiatr. (1997) 36:980–8. doi: 10.1097/00004583-199707000-00021
17. Reich W. Diagnostic interview for children and adolescents (DICA). J Am Acad Child Adolesc Psychiatr. (2000) 39:59–66. doi: 10.1097/00004583-200001000-00017
18. Shaffer D, Fisher P, Lucas C, Dulcan M, Schwab-Stone M. NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatr. (2000) 39:28–38. doi: 10.1097/00004583-200001000-00014
19. Mayes TL, Bernstein IH, Haley CL, Kennard BD, Emslie GJ. Psychometric properties of the children's depression rating scale–revised in adolescents. J Child Adolesc Psychopharmacol. (2010) 20:513–6. doi: 10.1089/cap.2010.0063
20. Craddock KES, Zhou X, Liu S, Gochman P, Dickinson D, Rapoport JL. Symptom dimensions and subgroups in childhood-onset schizophrenia. Schizophr Res. (2018) 197:71–7. doi: 10.1016/j.schres.2017.10.045
21. Brisch R, Saniotis A, Wolf R, Bielau H, Bernstein H-G, Steiner J, et al. The role of dopamine in schizophrenia from a neurobiological and evolutionary perspective: Old Fashioned, but still in Vogue. Front Psychiatr. (2014) 5:fpsyt.2014.00047. doi: 10.3389/fpsyt.2014.00110
22. Driver DI, Gogtay N, Rapoport JL. Childhood onset schizophrenia and early onset schizophrenia spectrum disorders. Child Adolesc Psychiatr Clin N Am. (2013) 22:539–55. doi: 10.1016/j.chc.2013.04.001
23. Kennedy E, Kumar A, Datta SS. Antipsychotic medication for childhood-onset schizophrenia. Cochr Datab Systemat Rev. (2007) 2007:CD004027. doi: 10.1002/14651858.CD004027.pub2
24. Mcclellan J, Sikich L, Findling R, Frazier J, Vitiello B, Hlastala S, et al. Treatment of early-onset schizophrenia spectrum disorders (TEOSS): Rationale, design, and methods. J Am Acad Child Adolesc Psychiatr. (2007) 46:969–78. doi: 10.1097/CHI.0b013e3180691779
25. Chaudhury S, Singh RK, Sinha VK. Effect size of lithium, carbamazepine, and sodium valproate in child and adolescent bipolar 1 disorder during manic phase: A prospective open-label study. Indus Psychiatr J. (2019) 28:185. doi: 10.4103/ipj.ipj_3_19
26. Jureidini JN, Doecke CJ, Mansfield PR, Haby MM, Menkes DB, Tonkin AL. Efficacy and safety of antidepressants for children and adolescents. Br Med J. (2004) 328:879–83. doi: 10.1136/bmj.328.7444.879
27. Geller B, Chestnut EC, Farooki ZQ, Cooper TB. Dose and plasma levels of nortriptyline and chlorpromazine in delusionally depressed adolescents and of Nortriptyline in nondelusionally depressed adolescents. Am J Psychiatry. (1985) 142:336–8. doi: 10.1176/ajp.142.3.336
28. Lally J, Gaughran F, Timms P, Curran S. Treatment-resistant schizophrenia: Current insights on the pharmacogenomics of antipsychotics. Pharmacogenom Personalized Med. (2016) 9:117–29. doi: 10.2147/PGPM.S115741
29. Kane JM, Agid O, Baldwin ML, Howes O, Lindenmayer J-P, Marder S, et al. Clinical guidance on the identification and management of treatment-resistant schizophrenia. J Clin Psychiatr. (2019) 80:12123. doi: 10.4088/JCP.18com12123
30. Adnan M, Motiwala F, Trivedi C, Sultana T, Mansuri Z, Jain S. Clozapine for management of childhood and adolescent-onset schizophrenia: A systematic review and meta-analysis. J Child Adolesc Psychopharmacol. (2022) 32:2–11. doi: 10.1089/cap.2021.0092
31. Kasoff LI, Ahn K, Gochman P, Broadnax DD, Rapoport JL. Strong treatment response and high maintenance rates of clozapine in childhood-onset schizophrenia. J Child Adolesc Psychopharmacol. (2016) 26:428–35. doi: 10.1089/cap.2015.0103
32. Tungaraza TE, Ahmed W, Chira C, Turner E, Mayaki S, Nandhra HS, et al. Prescribing pattern of clozapine and other antipsychotics for patients with first-episode psychosis: A cross-sectional survey of early intervention teams. Therapeut Adv Psychopharmacol. (2016) 7:103–11. doi: 10.1177/2045125316683151
33. Kumra S, Oberstar JV, Sikich L, Findling RL, McClellan JM, Vinogradov S, et al. Efficacy and tolerability of second-generation antipsychotics in children and adolescents with schizophrenia. Schizophr Bull. (2007) 34:60–71. doi: 10.1093/schbul/sbm109
34. Shaw P, Sporn A, Gogtay N, Overman GP, Greenstein D, Gochman P, et al. Childhood-onset schizophrenia. Arch Gen Psychiatry. (2006) 63:721. doi: 10.1001/archpsyc.63.7.721
35. Sporn A, Vermani A, Greenstein D, Bobb A, Spencer E, Clasen L, et al. Clozapine treatment of childhood-onset schizophrenia: Evaluation of effectiveness, adverse effects, and long-term outcome. J Am Acad Child Adolesc Psychiatr. (2007) 46:1349–56. doi: 10.1097/chi.0b013e31812eed10
36. Kumra S, Kranzler H, Gerbino-Rosen G, Kester HM, DeThomas C, Cullen K, et al. Clozapine vs. “high-dose” olanzapine in refractory early-onset schizophrenia: An open-label extension study. J Child Adolesc Psychopharmacol. (2008) 18:307–16. doi: 10.1089/cap.2007.0089
37. West AE, Celio CI, Henry DB, Pavuluri MN. Child mania rating scale-parent version: A valid measure of symptom change due to pharmacotherapy. J Affect Disord. (2011) 128:112–9. doi: 10.1016/j.jad.2010.06.013
Glossary
ADHD, Attention-Deficit/Hyperactivity disorders; APS, Attenuated Psychotic Symptoms; ARMS, At-Risk Mental State; ASD, Autism spectrum disorders; BLIPS, Brief Limited Psychotic Symptoms; BPAD, Bipolar Affective disorder; BPRS-C, Brief Psychiatric Rating Scale for Children; C-YMRS, Childrens' Young Mania Rating Scale; CAARMS, Comprehensive Assessment of “At- Risk Mental States;” CDRS, Child Depression Rating Scale; CGAF, Clinical Global Assessment of Function; CGI-S and CGI-I, Clinical Global Impressions-Severity and Improvement; COP, childhood-onset psychosis; COS/EOS, Childhood-Onset Schizophrenia/Early Onset Schizophrenia; DICA, Diagnostic Interview for Children and Adolescents; DISC, Diagnostic Interview Schedule for Children; DSM-V, Diagnostic and Statistical Manual-5th Edition; ECT, Electro-convulsive Therapy; EPS, Extra-pyramidal Symptoms; FDR, first-degree relative; FEP, first-episode psychosis; ICD-11, International Classification of Diseases-11th edition; IQ, Intelligence Quotient; K-PANSS, Kiddie Version of the Positive and Negative Symptoms of Schizophrenia; K-SADS-PL, Kiddie's Schedule for Affective Disorders and Schizophrenia—Present and Lifetime Version; MDD, Major Depressive disorder; NICE, National Institute for Health and Care Excellence; OCD, obsessive-compulsive disorder; PDD, pervasive developmental disorder; PNOS, Psychosis Not Otherwise Specified; SIPS, Structured Interview for Prodromal Symptoms; TEOSS, Treatment of Early-Onset Schizophrenia Spectrum; TRS, Treatment Resistant Schizophrenia; VEOS, Very early onset schizophrenia.
Keywords: childhood psychosis, treatment resistance, childhood onset schizophrenia, early onset psychosis, early onset schizophrenia
Citation: Pattnaik JI, Panda UK, Chandran S, Padhy S and Ravan JR (2023) Treatment resistant psychosis in children and adolescents and clozapine: Nuances. Front. Psychiatry 14:1014540. doi: 10.3389/fpsyt.2023.1014540
Received: 08 August 2022; Accepted: 25 January 2023;
Published: 24 February 2023.
Edited by:
Santanu Nath, All India Institute of Medical Sciences, Deoghar (AIIMS Deoghar), IndiaReviewed by:
Sydney Moirangthem, National Institute of Mental Health and Neurosciences (NIMHANS), IndiaCopyright © 2023 Pattnaik, Panda, Chandran, Padhy and Ravan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jayaprakash Russell Ravan,  amF5YXByYWthc2hydXNzZWxsLnJhdmFuQGtpbXMuYWMuaW4=
amF5YXByYWthc2hydXNzZWxsLnJhdmFuQGtpbXMuYWMuaW4=