
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 28 October 2022
Sec. Aging Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.954048
This article is part of the Research TopicInternational Evidence on Predictors and Outcomes of Awareness of Age-related ChangeView all 8 articles
 Fiona S. Rupprecht1*
Fiona S. Rupprecht1* Serena Sabatini2
Serena Sabatini2 Manfred Diehl3
Manfred Diehl3 Denis Gerstorf4
Denis Gerstorf4 Roman Kaspar5
Roman Kaspar5 Oliver K. Schilling6
Oliver K. Schilling6 Hans-Werner Wahl6
Hans-Werner Wahl6Although gains and losses are an integral part of human development, the experience of change and readjustment that often comes with major life events may be particularly influential for an individual's subjective aging experience and awareness of age-related change (AARC). Thus, this study focused on the role of life events in the domains of family and health for an individual's awareness of age-related gains and losses. Specifically, we differentiated between the experience of specific life events (e.g., entering a new romantic relationship; hospital stay) and the cumulative experience of multiple life events. Furthermore, we differentiated between life events experienced at an expected time in life and life events experienced relatively early or relatively late compared to established social norms. Data came from the Innovation Sample of the German Socio-Economic Panel (SOEP-IS) and consisted of 1,612 participants aged 16 to 93 years (M = 54.1; SD = 18.2). Life events were assessed annually and retrospectively for the last 2 years. Propensity score matching provided evidence for an association of specific family life events and a higher awareness of age-related gains, as well as specific health life events and a higher awareness of age-related losses. Results furthermore indicated that the cumulative experience of family life events was associated with a higher awareness of age-related gains. Conversely, the cumulative experience of health events was associated with higher awareness of both age-related losses and age-related gains. Moreover, it was not only life events happening at an expected age, but also those happening relatively early and particularly those happening late in life, which were associated with AARC. In summary, life events and the change they may bring seem to be reflected in individuals' awareness of age-related losses and awareness of age-related gains.
Both gains and losses are seen as a natural part of human development and aging (1). The awareness of age-related gains and losses (i.e., AARC-gains and AARC-losses), however, differs between individuals and has been linked to various developmental outcomes, such as psychological wellbeing, mental health, physical health, and even survival—with AARC-losses exhibiting a mostly negative association with development outcomes, and AARC-gains showing oftentimes a small but positive association (2–4). Qualitative research has pointed toward critical life events, such as new medical diagnoses or entering retirement, as potential contributors to perceiving AARC-gains or AARC-losses (5). Life events are seen as specific transitions and discontinuities in an individual's life course and elicit a general awareness of change and readjustment (6, 7). As many life events in adulthood are to some extent age-graded, it seems plausible that they may trigger a greater awareness of age-related change and, thus, contribute to both AARC-gains and AARC-losses. Therefore, the current work investigates AARC in the context of life events.
Subjective aging of which AARC is a central component refers to individuals' reflection, understanding, and identification with their personal aging processes (8, 9). AARC is defined as “all those experiences that make a person aware that [their] behavior, level of performance, or ways of experiencing [their] life have changed as a consequence of having grown older (i.e., increased chronological age)” [(10), p. 340]. In contrast to most other operationalizations of subjective aging, AARC explicitly acknowledges the coexistence of gains and losses throughout human development (1, 10). This aspect is particularly relevant when studying the context of life events, which can simultaneously come with gains and losses. For example, both negative and positive life events are seen as major stressors and challenges for an individual's wellbeing and mental health (7, 11, 12), but can also result in psychological growth (13, 14). Furthermore, AARC is conceptualized as comprising multiple dimensions, including changes in health and physical functioning, cognitive functioning, interpersonal relations, social-cognitive and social-emotional functioning, and lifestyle and engagement, allowing to capture the broad range of adaptation that is often required when dealing with life events (15, 16).
Whereas research has been accumulating on individual difference predictors of AARC (17, 18), research on the effects of context-based predictors of AARC is still very much at the beginning (19). Reasoning behind the construct of AARC itself (20) as well as other indicators of subjective aging (21, 22) point to the need to contextualize AARC and thus, to better understand how “diverse […] phenomena, events, and forces that exist outside of the developing individual” [(23), p. 84] shape the subjective experience of aging and change. Life events are usually either elicited by contexts or heavily involve (changing) contexts and are thus crucial when aiming for a contextualization of AARC. In the following, we first discuss the potential role of specific life events in the domains of family and health for AARC. Subsequently, we focus on the role of accumulating life events for AARC. Lastly, we discuss the role of timing and age-normativity of life events when it comes to their relation to AARC.
According to life script theory, specific major life events, such as the birth of a child, the death of a parent, or the diagnosis of a critical illness, are used as developmental markers and help to structure the human life course (24). Within cultures, there is often much consensus about the order and timing of life events; that is, at what age life events are considered normative (25, 26). This age-normativity of a considerable portion of major life events is closely linked to life anticipation as well as the achievement of important life goals. At the same time, such life events infuse and structure autobiographical memories and meaning-making of a person's individual development (24, 26). Because AARC is essentially one possible way to reflect and make meaning of a person's own development and strongly symbolizes that lifetime is progressing, it stands to reason that specific, age-normative life events may feature strongly in an individual's awareness of age-related gains and losses.
Prior research regarding life events and subjective aging has mostly focused on such age-normative life events and their relation to the felt age of individuals. Within this line of research, it has been argued that life events may serve as markers of aging processes and could thus affect how old people feel (22). Whereas specific life events in the family domain (e.g., marriage or death of one's spouse) have been found to be unrelated to (changes in) people's felt age (27–29), specific life events in the health domain (e.g., incident of a serious disease) were indeed linked to increases in felt age over time (27). We therefore distinguish between life events in the family domain, which involve individuals' close others and comprise experiences of both gains and losses, and life events in the health domain, which often involve losses and may be more readily attributed to the aging process (30). The existing lifespan literature argues that the social/family and health domain are among the most important drivers of development across the adult lifespan (31, 32). Consequently, we first investigate the association of specific life events in the health and family domain with AARC. This should allow us to examine whether there are life events (e.g., birth of a child for young adults, new medical diagnoses for older adults) that may serve as markers of aging and thus prompt AARC-gains or AARC-losses.
Irrespective of their potential age association, major life events often constitute transitions and discontinuities in a person's life course and everyday life routines and require instrumental, behavioral, cognitive, and emotional adaptation (7, 16). They often come with immediate changes to social networks, health, functioning, finances, and daily life, as well as new social roles, tasks, demands, and requirements and can, eventually, lead to changes in personality and the self (15, 16). Life events can thus be seen as drivers of change and challenges for psychological adaptation and development. When life events accumulate, their consequences tend to accumulate as well (33) and may profoundly affect an individual's level of adjustment and quality of life. How successfully or unsuccessfully individuals deal with this challenge of accumulated change, the associated stress, increasing constraints and a lack of control (34, 35), may generally foster a strong awareness of age-related change. For example, individuals could become aware of their age-related gains in socio-emotional functioning that now allow them to cope with the change better than they would have been able to at a younger age. It also stands to reason that life events themselves may not be linked to age, but the consequences for one's individual development, for example in health or interpersonal relations, may still be attributed to age.
When taking on this perspective of accumulated life events as a challenge for development, it should not be the influence of specific (age-related) life events, but rather their accumulation: The higher the number of life events an individual has experienced within a specific time period, the more pronounced the experience of change and the required adaptation and—potentially—the increase of AARC-gains and AARC-losses. For testing this hypothesis, we utilized two count variables for life events, one for the family domain and the other for the health domain, as a measure of accumulated life events.
Whereas our investigation of single life events in relation to AARC only allows for a qualitative comparison of more or less age-normative life events (e.g., birth of a child as a highly age-normative life event for young adulthood), the analysis of accumulated life events comes with enough statistical power for a more fine-grained investigation of the timing of life events and the association of timing with AARC. One assumption would be that age-corresponding life events (i.e., life events experienced at an age, at which they are expected or normative) may feature more strongly in an individual's AARC because changes elicited by the age-corresponding life events could easily be interpreted as age-related. The contrasting assumption would, however, be that the experience of life events at a non-normative or uncommon age (either relatively early or relatively late) could make a person's diverging and non-normative aging process particularly salient and contribute to a strong individual AARC. The uncommon or non-normative timing makes life events and the associated changes less predictable and less amenable to anticipatory coping and personal control. Moreover, individuals who experience life events at a non-normative time may have less social support available to them and may be more prone to engage in unfavorable social comparisons (36–38). All of these aspects may affect the association of life events with AARC. In a third step, we thus compared the (cumulative) experience of life events happening relatively (or non-normatively) early, life events happening relatively (or non-normatively) late, and life events happening at an expected (or normative) age in respect to their relation to AARC.1 This allowed us to investigate whether the timing of (cumulative) life events plays a role for the association between life events and AARC.
The current study focused on awareness of age-related change in the context of life events. We investigated (a) whether single and specific life events were related to AARC, (b) whether the cumulative experience of life events was related to AARC, and (c) the role of timing of these life events. For all research questions, we applied a lifespan perspective on AARC and included individuals in early, middle, and late adulthood in the analyses. We do so because change in form of both gains and losses is seen as a ubiquitous phenomenon throughout the lifespan (1) and reflections upon and interpretation of aging should happen across adult development. In addition, given our argument on the role of timing of life events, a research approach including AARC in early adulthood is of particular importance.
Regarding the first research question, we started by investigating single life events and their role for AARC by propensity score matching individuals who had experienced a respective life event with highly similar individuals who had not experienced this event. We expected traditional age-related life events, such as the birth of a child, to be particularly strongly related to AARC. We investigated the second research question by using count scores for life events and assuming that a higher number of life events was associated with accumulated change and could thus be related to a higher awareness of age-related change. For the third research question, we were interested whether the point in life at which life events occurred was relevant for their association with AARC. There are arguments for both a particularly strong association between age-corresponding life events and AARC as well as a particularly strong association between relatively early or late life events and AARC. Therefore, we considered this an exploratory research question, which we also addressed using count variables for age-corresponding life events, early life events, and late life events.
Regarding the choice of life events, we decided to focus on family life events and health life events. Family life events encompass events concerning romantic relationships, children, and death, and allow for a strongly contextual perspective on AARC as all those events involve persons other than the participating individuals themselves. Health life events focus on new mental and physical health diagnoses, as well as hospital stays. Due to the often strong association between health and AARC-losses (4), we expected health life events to be more strongly related to AARC-losses. Overall, we however acknowledge that life events may feature gains and losses at the same time and thus expected them to be related with potential increases in both, AARC-losses and AARC-gains. For time distance, we focused on life events that had occurred within the 2 years before the assessment of AARC. We chose this time distance because dynamic adaptation to most life events usually takes place within 2 years after the occurrence of the event (39). All analyses controlled for the influence of age and gender, which are oftentimes related to the actual occurrence of life events. To account for resources of the participants in dealing with the life events, we furthermore controlled for their education, their number of close friends (as a social resource variable), and their previous health state, that is, the health state an individual had before the health life events occurred.
Data came from the Innovation Sample of the German Socio-Economic Panel Study (SOEP-IS). The SOEP study is a multidisciplinary and longitudinal survey covering ~11,000 German households. SOEP-IS is one of its extensions and applies innovative research questions and instruments not covered in the core survey to smaller subsamples (40). Participants in two of these subsamples answered the items on awareness of age-related change and, thus, formed the sample for the present study. The participants were 1,612 adults from 1,011 German households aged 16 to 93 years (M = 54.1 years; SD = 18.2 years), and 53% of them were women. Among the participants, 53% were married, 2% were married but lived in separation, 24% were single and never married, 12% were divorced and 9% were widowed. The sample reflected diverse educational backgrounds with 1% still being in school, 6% either not having completed school or only having completed general elementary school, 4% having completed intermediate school, 14% having a general or vocational maturity certificate, 24% having a basic vocational and 30% having intermediate vocational qualification, 5% having lower tertiary and 14% having higher tertiary education. Monthly household net incomes ranged from 129€ to 21,250€, Md = 2,700€, M = 3,043€, SD = 1,718€. 10% of the participants had direct migration background, 9% had indirect migration background (i.e., participants were born in Germany, but have at least one parent who immigrated to Germany).
Awareness of age-related gains and losses was assessed with the 10-item short form of the AARC questionnaire, which was specifically developed for large-scale studies (41). Items start with the phrase “With my increasing age, I realize that…” and conclude with a gain- or loss-specific statement reflecting one of the five domains health and physical functioning, cognitive functioning, interpersonal relations, social-cognitive and social-emotional functioning, and lifestyle and engagement. For example, for the domain of social-cognitive and social-emotional functioning the two statements are “…I have a better sense of what is important to me” and “…I find it harder to motivate myself”. Items were answered on a scale ranging from 1 (not at all) to 5 (very much). The AARC-gains and AARC-losses subscales were computed by averaging the respective five items. Awareness of age-related gains amounted to M = 3.30, SD = 0.74, and had a reliability of Cronbach's α = 0.66. Awareness of age-related losses amounted to M = 2.09, SD = 0.80, and achieved good reliability with Cronbach's α = 0.81. The two subscales were positively related to each other, r = 0.28, p < 0.001.
Participants were asked whether the following changes occurred in their life since the beginning of 2016, or the beginning of 2017, respectively (measurement points conducted in 2017 and 2018 were used): New romantic partnership, moving in with partner, new marriage, birth of child, child moving in, child moving out, separation from partner, divorce, death of partner, death of father, death of mother, death of child, death of (another) household member, (other) change in household composition. Due to available assessment format, there is only information whether a life event occurred (1) or not occurred (0) at least once during the last 2 years. Multiple occurrences of the same life event could not be operationalized. Life events in the family domain were summed up to the count variable family life events, which ranged from 0 to 5, Md = 0, M = 0.41, SD = 0.69.
In a next step, we split the count variable family life events into three distinct count variables, one for life events happening non-normatively early (i.e., early family life events), one for life events happening within a normative age range (i.e., age-corresponding family life events), and one for life events happening non-normatively late (i.e., late family life events). Hereby, the 25% and 75% age quartiles were determined across all participants who had experienced a specific life event within the last 2 years. If a participant had experienced a specific life event themselves and their age lay below the 25% quartile it was counted as an early life event, if their age lay above the 75% quartile it was counted as a late life event, and if it lay between the 25% and the 75% quartile (i.e., in the interquartile range) it was counted as an age-corresponding life event.
Participants were asked whether a physician had diagnosed the following diseases within the last year, both in 2017 and in 2018: Sleep disorder, diabetes, asthma, cardiac disease, cancer, apoplectic stroke, migraine, depressive disorder, high blood pressure, dementia, joint disorder, chronic back pain, or any other disease. In order to unambiguously identify new medical diagnoses, we only counted diagnoses that had not yet been reported by the individual in the years of 2012 to 2015. Additionally, participants were asked whether they had been admitted to a hospital at least once in the two previous years. Multiple occurrences of the same life event were again not assessed. Life events in the health domain were summed up to the count variable health life events, which ranged from 0 to 5, Md = 0, M = 0.59, SD = 0.85. In a next step, the three variables early health events, age-corresponding health events, and late health events were formed as described for family life events.
As covariates for the regression analyses and as predicting variables in the propensity score matching, we used age, sex, education, number of close friends and prior count of medical diagnoses. Age, sex, and education were used to account for demographic characteristics of the individual. Age was coded as years since birth, sex was coded as 0 for women and 1 for men, and education was coded using the Comparative Analysis of Social Mobility in Industrial Nations (CASMIN) indicator, which ranges from in school (0) to higher tertiary education (9). The number of close friends reflects an important social resource for dealing with life events in both the health and the family domain (42). It was assessed directly with the question “How many close friends would you say you have” and subsequently reduced to a maximum number of 35, which reflects the assumed limit of close social relationships an individual can have (43). The prior count of diagnoses refers to the health state of an individual in the years between 2012 and 2015—and thus, before the health life events and family life events occurred and is based on the same list of diagnoses as the variable of health life events.
To test the role of single life events, we first identified the individuals who had experienced the specific life event within the last 2 years. We then matched these individuals who had experienced the life event (experiential group; Exp) to highly similar individuals who had not experienced the life event (control group; Con). This was done by propensity score matching, wherein each individual was assigned a probability of having experienced the respective life event using logistic regression analysis and age, sex, education, number of close friends, and prior count of diagnoses as predictors. Individuals from the experiential group were then matched to their closest neighbor from the control group. Subsequently, the individuals in the experiential and the control group were compared in their AARC-gains and AARC-losses scores using paired t-tests. As the number of individuals who had experienced a specific life event was often small, we performed power analyses beforehand to estimate the size of effects we would be able to find. Power analyses indicated that 33 pairs of individuals would be enough to detect moderate-sized effects (d = 0.50). Detecting weaker effects (d = 0.40, d = 0.30, d = 0.20) would require larger group sizes, respectively (n = 51, n = 89, n = 198). We thus only conducted the t-tests for life events with an experiential group of n ≥ 33.
To test the role of accumulated life events, we performed linear regression models with AARC-gains and AARC-losses as the respective outcome variables. In a first analysis, the two general count variables family life events and health life events served as predictors. In a second analysis, we differentiated between life events experienced at a normative age and non-normatively early/late by focusing on early family life events, age-corresponding family life events, late family life events, early health life events, age-corresponding health life events, and late health life events as predictors. Age, sex, education, number of close friends, and prior count of diagnoses served as covariates in all analyses. R version 4.1.1 was used for analyses (44).
Descriptive statistics and bivariate correlations of the study variables are shown in Table 1. At the bivariate level, the higher the number of health events (general, age-corresponding, and late), the older the age, the larger the number of close friends and the more prior diagnoses, the higher was the reported AARC-gains. Also, men reported slightly higher AARC-gains than women. The higher the number of family life events (general, early, and age-corresponding), the number of health events (general, age-corresponding, and late), the age, and the count of prior diagnoses, but the lower the education and the number of close friends, the higher was the reported AARC-losses. The experience of family life events was associated with the experience of health life events (more early health life events, but less late health life events), a younger age, a higher education, and a lower count of prior diagnoses. The experience of health life events was furthermore associated with an older age, lower education, and a higher count of prior diagnoses.
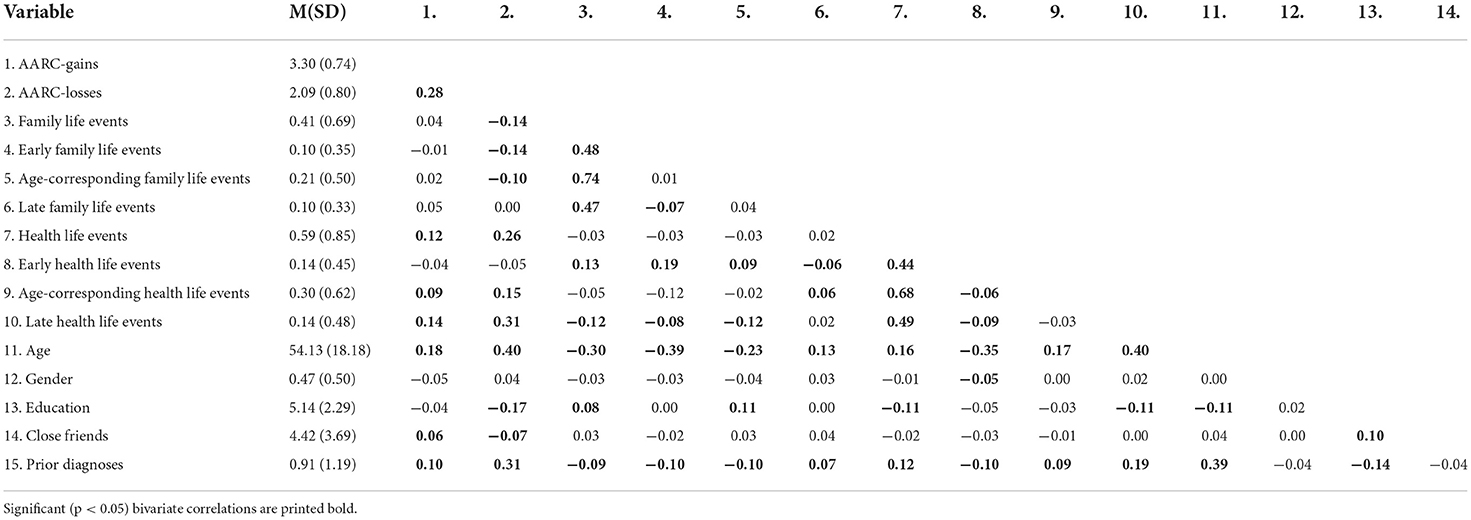
Table 1. Descriptives and bivariate correlations of the study variables (N = 1,612).
Associations between the experience of specific family life events and awareness of age-related change are shown in Table 2. Only the start of a new romantic relationship as well as the separation from one's partner were significantly related to a higher awareness of age-related gains. No specific family life event was related to AARC-losses. Associations between the single health life events and awareness of age-related change are shown in Table 3. The new diagnosis with a sleep disorder or a cardiac disease were associated with a stronger awareness of age-related losses. Similarly, individuals who had a hospital stay within the last 2 years, reported a slightly elevated awareness of age-related losses. No specific health life event was related to AARC-gains. To indicate the age characteristics of the individuals who had experienced a specific life event, their age range, age mean, and standard deviation are provided in Tables 2, 3.
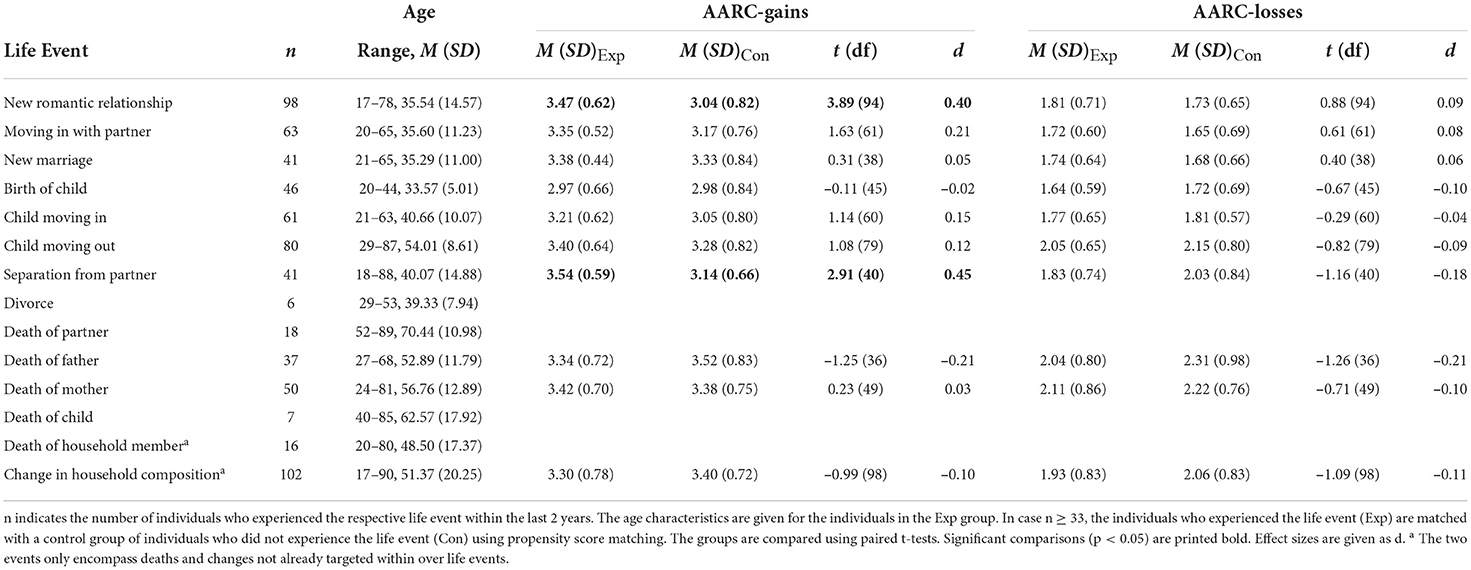
Table 2. Investigating the impact of specific life events in the family domain using propensity score matching.
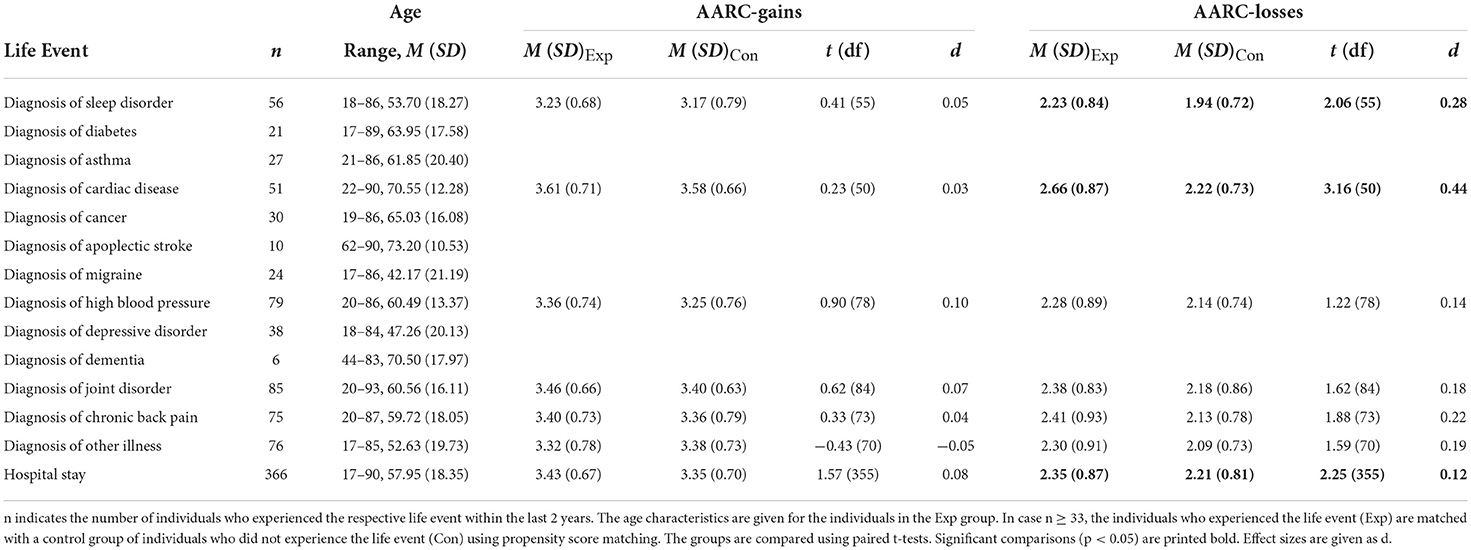
Table 3. Investigating the impact of specific life events in the health domain using propensity score matching.
Results of AARC's prediction by the general count variables are shown in Table 4. Awareness of age-related gains was stronger when individuals had experienced an overall higher number of both family and health life events in the two previous years. Furthermore, AARC-gains was positively associated with an older age, female sex, and a higher number of close friends. After accounting for covariates, the two general count variables for life events accounted for an additional 1.5% of variance in AARC-gains, which indicates a small effect size.
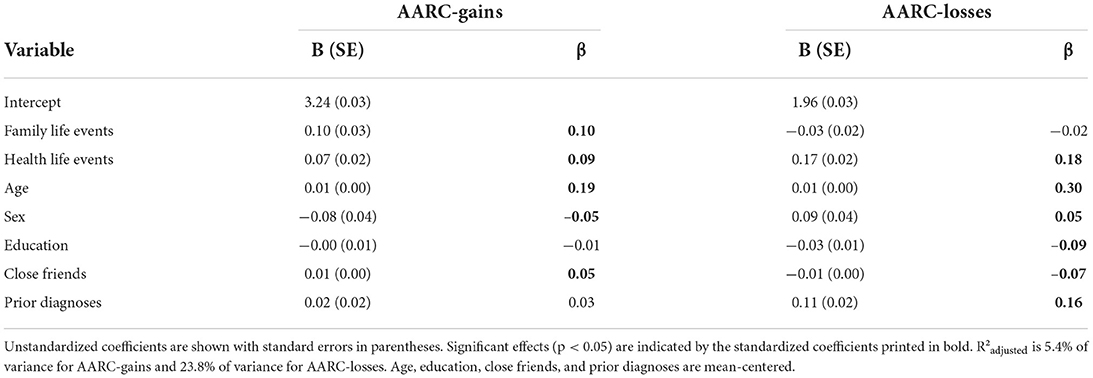
Table 4. Investigating the predictive effects of accumulating life events for awareness of age-related change.
Awareness of age-related losses was stronger when individuals had experienced an overall higher number of health life events in the two previous years. AARC-losses was not associated with the general number of family life events experienced. Instead, AARC-losses was positively associated with an older age, male sex, lower education, a lower number of close friends, and more prior diagnoses. After accounting for covariates, the two general count variables for life events accounted for an additional 2.9% of variance in AARC-losses, which again indicates a small effect size.
Table 5 presents the regression analyses with the count variables for (non-normatively) early, age-corresponding, and (non-normatively) late life events instead of the general count variables as predictors of AARC. For AARC-gains, these differentiated count variables did not account for significantly more variance than the general count variables. Still, whereas early and age-corresponding family life events predicted stronger AARC-gains, late family life events did not. In the health domain, age-corresponding and late life events predicted stronger AARC-gains, but early health life events did not. Figure 1 depicts the associations between general, early, age-corresponding, and late life events with AARC-gains.
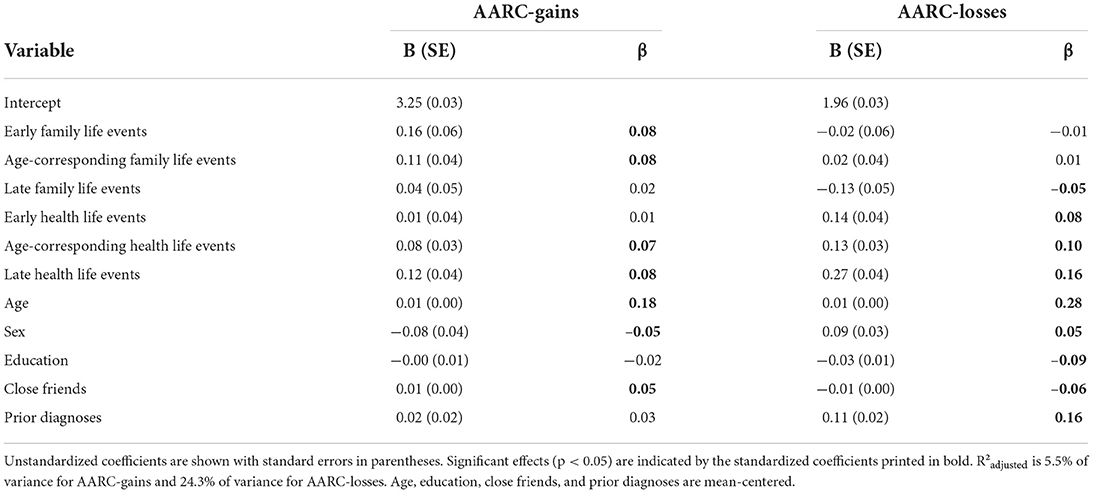
Table 5. Investigating the predictive effects of relatively early, age-corresponding, and relatively late life events for awareness of age-related change.
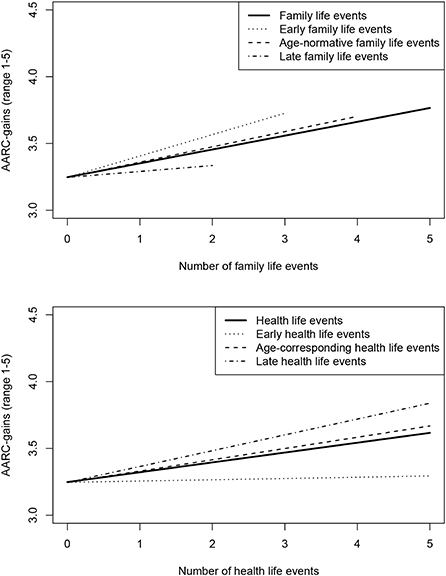
Figure 1. Number of life events and awareness of age-related gains. Regression lines cover the maximum number of life events occurring in the sample.
For AARC-losses, the variance accounted for by the differentiated count variables was slightly higher than the variance accounted for by the general count variables (+0.5%). In the family domain, only late life events were associated with a lower AARC-losses. There was no association between AARC-losses and early and age-corresponding family life events. In the health domain, early, age-corresponding, and late life events were all associated with higher AARC-losses. However, the regression coefficients point toward the strongest association of late health life events with AARC-losses. Figure 2 depicts the associations between general, early, age-corresponding, and late life events with AARC-losses.
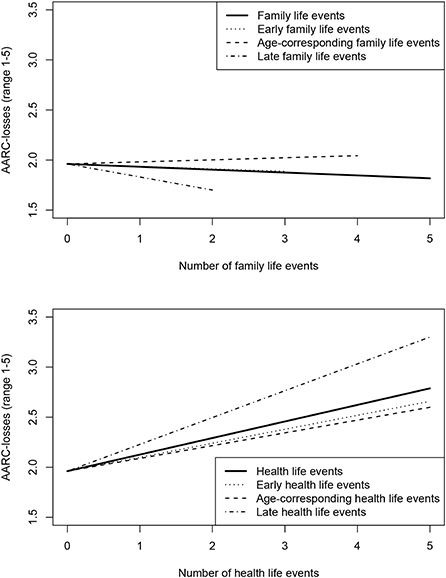
Figure 2. Number of life events and awareness of age-related losses. Regression lines cover the maximum number of life events occurring in the sample.
This investigation of AARC in the context of life events found a higher number of life events in the family domain to be related to a stronger awareness of age-related gains. A higher number of life events in the health domain was predominantly associated with a stronger awareness of age-related losses but also weakly with a stronger awareness of age-related gains. Associations were particularly evident for life events happening at an age-normative or relatively late time, indicating that the point in life at which a life event was experienced might indeed be relevant. Associations between AARC and single life events were only sporadic but pointed toward a relation between specific family life events and higher AARC-gains and specific health life events and higher AARC-losses. Thus, the distinction between family life events and health life events appeared particularly wellsuited to capture the differential content and relational patterns of AARC-gains and AARC-losses.
The cumulative experience of life events was overall associated with a heightened awareness of age-related change. This indicates that individuals might have interpreted at least part of the change driven by life events as a change also driven by their increasing age. Importantly, this change was not only in the form of losses, but also in the form of gains, hinting toward the growth that can follow even from highly stressful life events (13). Aside from this cumulative effect, we found few single life events that were significantly associated with AARC, that is, new romantic relationship and separation from partner in the family domain, and diagnosis of sleep disorder, diagnosis of cardiac disease, and hospital stay in the health domain. Apart from new romantic relationship, which is a developmental task traditionally assigned to young adulthood (46), none of the life events seem particularly normative for a certain age group. This finding provides only limited evidence for the role of specific, age-corresponding life events as markers of aging and AARC. This is mostly in line with prior empirical research on single life events outside the health domain which were also unrelated to felt age as a different indicator of subjective aging (27–29). In contrast, the cumulative experience of age-corresponding life events was indeed associated with AARC—though life events happening relatively late in life also appeared of relevance.
The accumulation of life events in the family domain was found to be positively related to AARC-gains. Individuals who experienced (multiple) transitions within their closest relationships and their families seemed to perceive growth and to associate this growth with their own aging. Many life events in the family domain follow from long-term investments (e.g., marriage or child moving out). Experiencing these life events and witnessing the results of such long-term investments may make individuals particularly aware of the gains in their development. This finding highlights the importance to contextualize AARC and to account for individuals' experiences in their families and social networks, which can be one source of positive aging experiences. When differentiating between age-corresponding, relatively early, and relatively late family life events, the two former event types were associated with higher AARC-gains, whereas the latter type was associated with lower AARC-losses. In general, family life events seemed to have positive influences overall, but the exact influences may depend on the point in life at which they are experienced. With regard to specific family life events, only the beginning and ending of a romantic relationship were directly associated with a higher awareness of age-related gains. Changes in the relationship status may come with new experiences, the opportunity to gain new self-knowledge, a heightened appreciation of existing social ties, and overall psychological growth (47) and may thereby raise the awareness of age-related gains.
Somewhat unexpectedly, the negative family life events, which were mainly deaths in the immediate family, were unrelated to both AARC-gains and AARC-losses. However, important moderating aspects, such as the emotional closeness to the person who had died, as well as the circumstances of death could not be examined as this information was not available. Also, there were only very few individuals who reported the death of their spouse and information on the death of other same-aged individuals, such as friends, colleagues, or siblings, was not available. The death of a peer may affect AARC in different and more pronounced ways than for example the death of a parent.
Accumulated life events in the health domain were associated with higher AARC-losses and higher AARC-gains. Regarding the former association, (multiple) diagnoses and health events can signal a deterioration of health, can come with a loss of functioning and independence and may raise an individual's awareness of age-related losses. The close association between health (declines) and a more negative subjective aging experience has been documented in several prior studies (4, 45, 48). The association between health life events and AARC-losses appeared regardless of when they happened—though it appeared strongest for health life events happening particularly late considering the age distribution of the sample.
Regarding single health life events, a new diagnosis with a sleep disorder was related to heightened AARC-losses. This finding is congruent with a recent study linking poor self-reported sleep to higher AARC-losses (49). It also seems important to highlight the weak, though significant impact a hospital stay seemed to have on AARC-losses. Hospital stays are often acute and unexpected and may, thus, be associated with a feeling of vulnerability and lack of controllability. Overall, results suggest that a close monitoring of the aging experience of individuals facing major transitions in the health domain (i.e., multiple diagnoses, hospital stays) could be beneficial, so that losses do not become overwhelming and negatively influence other aspects of life, such as psychological wellbeing (2, 50).
In this vein, the present results offer one potential way of coping with negative life events in the health domain, that is, a parallel awareness of age-related gains. Results indicated that the positive association of health life events with both AARC-losses and AARC-gains could only be found for age-corresponding or late, but not for early life events. Nevertheless, this finding highlights that awareness of growth can happen in the face of health declines and other adversities (13, 14) and that such perceived growth could be explicitly encouraged and supported.
A first limitation of our research concerns the operationalization of AARC and life events. To our knowledge, the SOEP-IS 2018 provided the first opportunity to assess and investigate AARC in early adulthood. We acknowledge that the assessment of AARC in early adulthood needs more research in the future. However, unpublished psychometric analyses are supporting measurement invariance of the AARC short version across the full adult lifespan (Kaspar et al., in preparation). Life events within the family domain were not necessarily representative for old age and particularly positive life events normative for old age (e.g., birth of a grandchild) were missing. Overall, the distinction between family and health life events proved meaningful in regard to their specific relations to AARC-gains vs. AARC-losses. However, life events in other domains (e.g., work, leisure) could similarly provide distinct influences on AARC and should be investigated in future research. In the framework of SOEP-IS 2018, such other life events were either not assessed or were only applicable for subsamples with fairly limited age ranges (e.g., graduation or retirement). Additionally, the non-occurrence of certain life events (e.g., not receiving medical diagnoses as an older adult or not becoming a parent as a young adult) or the multiple occurrence of the same life event (e.g., new romantic relationship) within 2 years may also be impactful for AARC but could not be examined within this study.
A second limitation concerns the fact that only cross-sectional data were available for AARC. Though information on other variables and life events was available from the years before, AARC was only assessed at a single occasion in 2018. Thus, actual increases and decreases in AARC as a consequence of the experience of life events could not be examined. Relations in the opposing direction, that is AARC as a predicting variable of single life events (e.g., high AARC-gains as a predictor of starting a new romantic relationship; high AARC-losses as a predictor for new medical diagnoses) could also not be ruled out. Future research should concentrate on longitudinal data in AARC (with at least one wave of data collection of AARC before the occurrence of the life events) to disentangle the potentially complex mechanisms in its association with life events.
Lastly, future research may include further constructs and research questions to (a) investigate for whom and under which circumstances life events affect AARC, and (b) investigate mediating variables and potential consequences of the association between life events and AARC. Regarding the former, aspects of coping, personality, control, social and instrumental support, upward and downward social comparisons, but also characteristics of the life event itself could be of relevance (17, 50). Regarding the latter, a high awareness of age-related losses could for example function as a mediator in the association between life events in the health domain and mental health (2).
When investigating AARC in the context of life events in an adult lifespan sample, we found evidence that the cumulative experience of life events was related to a higher awareness of both age-related gains and age-related losses. The experience of life events in the family domain featured prominently in the awareness of age-related gains, whereas the experience of life events in the health domain featured more strongly in the awareness of age-related losses. The experience of life events and the associated change may impact how individuals perceive their aging process, may challenge the subjective experience of age-related losses, but may also foster the subjective experience of age-related gains.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was a secondary analysis of anonymized data, and therefore an ethics approval was not required. Detailed information on ethical clearance related to the German Socio-Economic Panel (SOEP) can be found on their website (https://www.diw.de/soep).
FR: conception and design of the work, analyses, and writing. SS: contribution to conception and design of the work and analyses. MD, DG, RK, OS, and H-WW: conceptual contribution, acquisition and interpretation of data, and revising the work. All authors contributed to the article and approved the submitted version.
The data used in this publication were made available to us by the German Socio-Economic Panel Study (SOEP) at the German Institute for Economic Research (DIW), Berlin.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^For example, based on age distributions of the current data, losing one's mother (life event death of mother) was most common between the ages of 50 and 65 years (= interquartile range of the age of all participants reporting the life event) and would be rated as age-corresponding when occurring within this interval. It would be rated as relatively early when occurring before the age of 50 and as relatively late when occurring after the age of 65.
1. Heckhausen J, Dixon RA, Baltes PB. Gains and losses in development throughout adulthood as perceived by different adult age groups. Dev Psychol. (1989) 25:109–21. doi: 10.1037/0012-1649.25.1.109
2. Dutt AJ, Gabrian M, Wahl HW. Awareness of age-related change and depressive symptoms in middle and late adulthood: longitudinal associations and the role of self-regulation and calendar age. J Gerontol: Series B, Psychologic Sci Soc Sci. (2018) 73:944–53. doi: 10.1093/geronb/gbw095
3. Kaspar R, Wahl HW, Diehl M. Awareness of age-related change as a behavioral determinant of survival time in very old age. Front Psychol. (2021) 12:727560. doi: 10.3389/fpsyg.2021.727560
4. Sabatini S, Silarova B, Martyr A, Collins R, Ballard C, Anstey KJ, et al. Associations of awareness of age-related change with emotional and physical wellbeing: a systematic review and meta-analysis. Gerontologist. (2020) 60:e477–90. doi: 10.1093/geront/gnz101
5. Sabatini S, Ukoumunne OC, Ballard C, Collins R, Corbett A, Brooker H, et al. Exploring awareness of age-related changes among over 50s in the UK: findings from the PROTECT study. Int Psychogeriatric. (2021) 21:1–15. doi: 10.1017/S104161022100123X
6. Hopson B, Adams J. Toward an understanding of transition: defining some boundaries of transition dynamics, In:, editors Adams J, Hayes J, Hopson B, . Transition: Understanding and Managing Personal Change, London: Allanheld, Osmun and Co. (1976). pp. 3–25.
7. Luhmann M, Hofmann W, Eid M, Lucas RE. Subjective wellbeing and adaptation to life events: a meta-analysis. J Pers Soc Psychol. (2012) 102:592–615. doi: 10.1037/a0025948
8. Diehl M, Wahl HW, Barrett AE, Brothers AF, Miche M, Montepare JM, et al. Awareness of aging: theoretical considerations on an emerging concept. Develop Rev DR. (2014) 34:93–113. doi: 10.1016/j.dr.2014.01.001
9. Kornadt AE, Kessler EM, Wurm S, Bowen CE, Gabrian M, Klusmann V. Views on ageing: a lifespan perspective. Euro J Ageing. (2020) 17:387–401. doi: 10.1007/s10433-019-00535-9
10. Diehl M, Brothers AF, Wahl HW. Self-perceptions and awareness of aging: past, present, and future (Handbook of the Psychology of Aging). London: Elsevier, (2021). pp. 155–179.
11. Betz LT, Penzel N, Kambeitz-Ilankovic L, Rosen M, Chisholm K, Stainton A, et al. General psychopathology links burden of recent life events and psychotic symptoms in a network approach. Npj Schizophrenia. (2020) 6:40. doi: 10.1038/s41537-020-00129-w
12. Kendler KS, Karkowski LM, Prescott CA. Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry. (1999) 156:837–41. doi: 10.1176/ajp.156.6.837
13. Park CL, Helgeson VS. Introduction to the special section: Growth following highly stressful life events–current status and future directions. J Consult Clin Psychol. (2006) 74:791–6. doi: 10.1037/0022-006X.74.5.791
14. Sears SR, Stanton AL, Danoff-Burg S. The yellow brick road and the emerald city: Benefit finding, positive reappraisal coping and posttraumatic growth in women with early-stage breast cancer. Health Psychol. (2003) 22:487–97. doi: 10.1037/0278-6133.22.5.487
15. Bleidorn W, Hopwood CJ, Lucas RE. Life events and personality trait change. J Pers. (2018) 86:83–96. doi: 10.1111/jopy.12286
16. Diehl M. Self-development in adulthood and aging: the role of critical life events. In:Ryff CD, Marshall VM, , editors The Self and Society in Aging Processes. New York, NY : Springer Pub (1999). p. 150–83.
17. Rupprecht FS, Dutt AJ, Wahl HW, Diehl MK. The role of personality in becoming aware of age-related changes. GeroPsych. (2019) 32:57–67. doi: 10.1024/1662-9647/a000204
18. Sabatini S, Siebert JS, Diehl M, Brothers A, Wahl HW. Identifying predictors of self-perceptions of aging based on a range of cognitive, physical, and mental health indicators: twenty-year longitudinal findings from the ILSE study. Psychol Aging. (2021) Advance online publication. doi: 10.1037/pag0000668
19. English AN, Bellingtier JA, Neupert SD. It's “the Joneses”: The influence of objective and subjective socioeconomic status on subjective perceptions of aging. Eur J Ageing. (2019) 16:121–8. doi: 10.1007/s10433-018-0475-2
20. Diehl M, Wahl HW. Awareness of age-related change: Examination of a (mostly) unexplored concept. J Gerontol Series B: Psychologic Sci Soc Sci. (2010) 65B:340–50. doi: 10.1093/geronb/gbp110
21. Hughes ML, Touron DR. Aging in context: incorporating everyday experiences into the study of subjective age. Front Psychiatr. (2021) 12:633234. doi: 10.3389/fpsyt.2021.633234
22. Montepare JM. Subjective age: toward a guiding lifespan framework. Int J Behav Dev. (2009) 33:42–6. doi: 10.1177/0165025408095551
23. Dannefer D. On the conceptualization of context in developmental discourse: Four meanings of context and their implications. In:Featherman DL, Lerner RM, and Perlmutter M, , editors. Life-Span Development and Behavior. London: Psychology Press (1993). pp. 84–105.
24. Berntsen D, Rubin DC. Cultural life scripts structure recall from autobiographical memory. Memory Cogn. (2004) 32:427–42. doi: 10.3758/BF03195836
25. Baltes PB, Reese HW, Lipsitt LP. Life-span developmental psychology. Annu Rev Psychol. (1980) 31:65–110. doi: 10.1146/annurev.ps.31.020180.000433
26. Berntsen D, Bohn A. Cultural life scripts and individual life stories. In:Poyer P, Wertsch JV., , editors, (Hg.) 2009 – Memory in Mind and Culture. Cambridge: Cambridge University (2009). p. 62–82.
27. Schafer MH, Shippee TP. Age identity in context. Soc Psychol Q. (2010) 73:245–64. doi: 10.1177/0190272510379751
28. Ward RA. Change in perceived age in middle and later life. Int J Aging Hum Develop. (2013) 76:251–67. doi: 10.2190/AG.76.3.e
29. Westerhof GJ, Barrett AE. Age identity and subjective wellbeing: a comparison of the United States and Germany. J Gerontol Series B, Psychologic Sci Soc Sci. (2005) 60:S129–36. doi: 10.1093/geronb/60.3.S129
30. Stewart TL, Chipperfield JG, Perry RP, Weiner B. Attributing illness to 'old age:' consequences of a self-directed stereotype for health and mortality. Psychol Health. (2012) 27:881–97. doi: 10.1080/08870446.2011.630735
31. Baltes MM, Silverberg SB. The dynamics between dependency and autonomy: illustrations across the life span. In: Life-Span Development and Behavior. (1994). p. 41–90.
32. Lang FR, Fingerman KL. Advances in Personal Relationships. Growing Together: Personal Relationships Across the Life Span. Cambridge: Cambridge University Press (2004). Available online at: https://search.ebscohost.com/login.aspx?direct=trueandscope=siteanddb=nlebkanddb=nlabkandAN=161153
33. Näsman M, Niklasson J, Saarela J, Nygård M, Olofsson B, Conradsson M, et al. Five-year change in morale is associated with negative life events in very old age. Aging Ment Health. (2019) 23:84–91. doi: 10.1080/13607863.2017.1393795
34. Hovenkamp-Hermelink JHM, Jeronimus BF, van der Veen DC, Spinhoven P, Penninx BWJH, Schoevers RA, et al. Differential associations of locus of control with anxiety, depression and life-events: A five-wave, nine-year study to test stability and change. J Affect Disord. (2019) 253:26–34. doi: 10.1016/j.jad.2019.04.005
35. Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. (2004) 130:601–30. doi: 10.1037/0033-2909.130.4.601
36. Baltes PB, Lindenberger U, Staudinger UM. Life span theory in developmental psychology. In: Handbook of Child Psychology. New York, NY: John Wiley and Sons, Inc (2007).
37. Rook KS, Catalano R, Dooley D. The timing of major life events: effects of departing from the social clock. Am J Community Psychol. (1989) 17:233–58. doi: 10.1007/BF00931009
38. Wrosch C, Freund AM. Self-regulation of normative and non-normative developmental challenges. Hum Dev. (2001) 44:264–83. doi: 10.1159/000057066
39. Uglanova EA, Staudinger UM. Zooming in on life events: is hedonic adaptation sensitive to the temporal distance from the event? Soc Indic Res. (2013) 111:265–86. doi: 10.1007/s11205-012-0004-1
40. Richter D, Schupp J. The SOEP Innovation Sample (SOEP IS). Schmollers Jahrbuch. (2015) 135:389–99. doi: 10.3790/schm.135.3.389
41. Kaspar R, Gabrian M, Brothers A, Wahl HW, Diehl M. Measuring awareness of age-related change: development of a 10-item short form for use in large-scale surveys. The Gerontol. (2019) 59:e130–40. doi: 10.1093/geront/gnx213
42. Billings AG, Moos RH. The role of coping responses and social resources in attenuating the stress of life events. J Behav Med. (1981) 4:139–57. doi: 10.1007/BF00844267
43. Hill RA, Dunbar RIM. Social network size in humans. Human Nat. (2003) 14:53–72. doi: 10.1007/s12110-003-1016-y
44. R Core Team. R: A language environment for statistical computing Computer software. Vienna, Austria: R Foundation for Statistical Computing (2021). Available online at: https://www.R-project.org/
45. Sabatini S, Ukoumunne OC, Ballard C, Collins R, Corbett A, Brooker H, et al. The cross-sectional relationship between pain and awareness of age-related changes. Br J Pain. (2021) 15:335–44. doi: 10.1177/2049463720961798
47. Tashiro T, Frazier P. “I'll never be in a relationship like that again”: personal growth following romantic relationship breakups. Person Relation. (2003) 10:113–28. doi: 10.1111/1475-6811.00039
48. Schönstein A, Dallmeier D, Denkinger M, Rothenbacher D, Klenk J, Bahrmann A, et al. Health and subjective views on aging: longitudinal findings from the ActiFE Ulm Study. J Gerontol Series B: Psychologic Sci Soc Sci. (2021) 76:1349–59. doi: 10.1093/geronb/gbab023
49. Sabatini S, Ukoumunne OC, Ballard C, Collins R, Corbett A, Brooker H, et al. Cross-sectional and longitudinal associations between subjective sleep difficulties and self-perceptions of aging. Behav Sleep Med. (2021) 21:1–30. doi: 10.1080/15402002.2021.1994405
Keywords: subjective aging, family events, health events, lifespan development, developmental change, developmental gains, developmental losses
Citation: Rupprecht FS, Sabatini S, Diehl M, Gerstorf D, Kaspar R, Schilling OK and Wahl H-W (2022) Awareness of age-related change in the context of major life events. Front. Psychiatry 13:954048. doi: 10.3389/fpsyt.2022.954048
Received: 26 May 2022; Accepted: 07 October 2022;
Published: 28 October 2022.
Edited by:
Gianfranco Spalletta, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Anson Kai Chun Chau, The Chinese University of Hong Kong, ChinaCopyright © 2022 Rupprecht, Sabatini, Diehl, Gerstorf, Kaspar, Schilling and Wahl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fiona S. Rupprecht, ZmlvbmEucnVwcHJlY2h0QHVuaXZpZS5hYy5hdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.