 Tai-Min Wu
Tai-Min Wu Qin Yang1,3
Qin Yang1,3 Lian-Zhong Liu
Lian-Zhong Liu- 1Institute of Education, China University of Geosciences (Wuhan), Wuhan, China
- 2Affiliated Wuhan Mental Health Center, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China
- 3Research Center for Psychological and Health Sciences, China University of Geosciences (Wuhan), Wuhan, China
Experiencing a serious natural disaster may place survivors at particularly high risk for post-traumatic stress disorder (PTSD); however, very limited data are available on the prevalence and clinical characteristics of PTSD among survivors of a tornado disaster. The present study examined the prevalence of PTSD and correlates and clinical symptoms of possible PTSD in survivors 1.5 months after a tornado disaster. A total of 237 survivors were recruited and administered the Structured Clinical Interview for DSM-V (SCID) to measure the prevalence of PTSD and the Essen Trauma Inventory (ETI) to measure the incidence of symptoms in each dimension. Survivors'demographic information and characteristics of exposure to the tornado were collected via self-report questionnaires. Thirty-two of the survey respondents were diagnosed with PTSD (13.6%, total =237). Correlates of PTSD in survivors were being female (OR=3.62, P = 0.023), living in an area severely affected by the tornado (OR = 3.94, P = 0.032), and having severe property damage (OR = 3.72, P = 0.010). Less common symptoms mainly focused on the avoidance dimension and included feeling alienated or distant from the people around oneself (21.90%), not being able to recall important parts of the event (28.10%), being emotionally numb (31.20%), and feeling like one's plans for the future and hopes will not come true (37.50%). In the sample of rural residents, nearly two-thirds of people with PTSD were not willing to seek psychological help; increasing the accessibility of mental health services and administering more active mental health services are necessary for this vulnerable population, whether or not they claim to need help.
Introduction
At 20:39 on 14 May 2021, a 17-magnitude tornado broke out in Wuhan City, Hubei Province. The wind speed reached a maximum of 60 m/s; some houses in the village bay were damaged, a large number of trees were fractured, and some work sheds collapsed. As of May 15, 2021, the tornado had killed 8 people and injured approximately 280 people. The disaster not only resulted in physical and tangible damage to the local people affected by the disaster but also caused serious psychological challenges. Relevant studies have shown that after major traumatic disaster events, disaster victims experience symptoms such as depression (1, 2), anxiety (1), sleep disturbance (3, 4), and symptoms of post-traumatic stress disorder (PTSD) (5). Severe cases are also diagnosed as PTSD (6), which greatly affects postdisaster reconstruction and the mental health of victims. From 23 June 2021 to 27 June 2021, members of the research team went to Zhashan, Caidian District, Wuhan City, Hubei Province, to conduct the research.
Subjects and methods
The research group went to Caidian District, Wuhan City, Hubei Province from 23 June 2021 to 27 June 2021. A total of 240 questionnaires were distributed, and 237 valid questionnaires were recovered, with an effective rate of 98.3%. This study took rural residents affected by the tornado disaster as the research sample, analyzed PTSD and its symptoms in rural residents after the disaster, and analyzed its correlating factors. The detection of the symptoms of each dimension of PTSD was explored.
Research subjects
The Respondents Were Rural Residents of three Rural Villages in Zhashan in the Tornado-affected area of Caidian District, Wuhan City. The local government classified villages according to the degree to which they were affected by the tornado: mildly affected (village A, village B, village C, village D, village E, village F, and village G) and severely affected (village H, village I and village J). According to this classification, two mildly affected villages (village B and village E) and one severely affected village (village I) of the two disaster degrees were selected as the target group by stratified sampling. In the three randomly selected villages, the method of random sampling was adopted, and 1/6 families in each village were selected as the research sample. Random sampling was carried out in each family according to the criteria of age no <12 years old and birthday close to 15 June to ensure the reliability of the sample. One sample was taken from each family.
The Institutional Review Board of Wuhan Mental Health Center approved the study protocol, and all participants signed informed consent forms.
Research methods
The investigators were postgraduates majoring in psychology and psychiatry. All investigators underwent unified centralized training and had extensive research experience. The researchers first introduced the purpose and specific methods of the assessment to the respondents and then conducted a questionnaire survey after obtaining the respondents' informed consent. The survey was conducted in a one-on-one, question-and-answer format, and all tests were conducted using uniform guidelines. The results of the questionnaires were stored in a unified and centralized manner to ensure the confidentiality of the survey data.
Research instruments
The research questionnaire used the Essen Trauma Inventory (ETI) to assess PTSD symptoms (7). The affected rural villagers were diagnosed with PTSD using the Structured Clinical Interview for DSM-V (SCID) (8) (the researcher conducting the PTSD diagnosis was trained in the SCID interview by the Wuhan Mental Health Center).
PTSD
The SCID was used to diagnose PTSD. It is the most widely used structured diagnostic tool for assessing mental illness. It can be used to assess mood disorders, psychotic disorders, substance abuse disorders, anxiety disorders, obsessive-compulsive disorders and related disorders, eating disorders, somatic symptom disorders, some sleep disorders (such as insomnia and somnolence disorders), externalizing behavior disorders (i.e., intermittent explosive disorder, gambling disorder and adult attention deficit hyperactivity disorder) and trauma and stress-related disorders.
PTSD symptoms
The validated Chinese version of the ETI was used to assess three symptom clusters of PTSD. The ETI was developed based on the DSM-IV-TR diagnostic criteria, and it has five parts with a total of 58 items. Part 1 contains a list of 14 potentially traumatic events and an open question asking about exposure to other traumatic events. Part 2 has 10 questions regarding the worst event's objective and subjective threat to life (criteria A1 and A2). Part 3 consists of 23 questions covering three symptom clusters of PTSD (intrusion [criteria B], avoidance [criteria C], and hyperarousal [criteria D]) and one additional symptom cluster for ASD (dissociation). Part 4 assesses the severity of psychological distress caused by the event [criteria F] and the duration of PTSD symptoms [criteria E]. Part 5 evaluates the severity of functional impairment caused by the event in terms of life satisfaction, school/work/job performance, household chores and duties, hobbies and leisure activities, relationships with friends, family relationships, and sexual life [criteria F].
Demographics
Demographic variables included gender, age, education, marital situation, living arrangements, personal income, smoking and alcohol consumption.
Exposure to the tornado disaster
Classification of the disaster degree and three questions were used to assess the severity of exposure to the tornado: “Did the disaster cause serious property damage?”, “Were you physically harmed by the disaster?”, and “Did you witness any injuries or deaths in the disaster?”.
Willingness to ask for psychological assistance
Two questions were used to assess the willingness to ask for psychological assistance: “Do you have any psychological troubles?”, “If so, do you need psychological assistance? (e.g., counseling, psychotherapy, and medication).”
Statistical analysis
The questionnaire data were analyzed using SPSS 21.0 statistical software. Before data analysis, the normality of the data was tested by combining histograms and P-P plots of the data distribution, and the results showed that the data generally followed a normal distribution. Detection rates for PTSD were calculated, and rates between subgroups were compared using chi-square tests based on demographic and tornado disaster exposure characteristics. Significant factors from the chi-square test were included in binary logistic regression to determine the factors associated with PTSD. Associations between correlates and PTSD were quantified using OR values and 95% confidence intervals. PTSD symptoms in affected villagers were described using frequencies and percentages. A two-sided P < 0.05 was considered statistically significant.
Results
General information of all respondents
Among the 237 affected rural villagers surveyed, information on their demographics (eight items) and tornado exposure characteristics (four items) was collected with a total of 12 items. The general information is shown in Table 1. Of all survey respondents, 32 were diagnosed with PTSD based on the SCID, accounting for 13.6% of the total survey population. Of the 95 most severely affected samples, 27 (28.4%) were diagnosed with PTSD. It was found that people with PTSD were more likely to be willing to seek psychological help (psychological counseling, psychotherapy, psychopharmacological treatment) than those without PTSD (χ2= 35.075, P < 0.001), but nearly 2/3 of people with PTSD (68.75%) still did not seek help (Table 2).
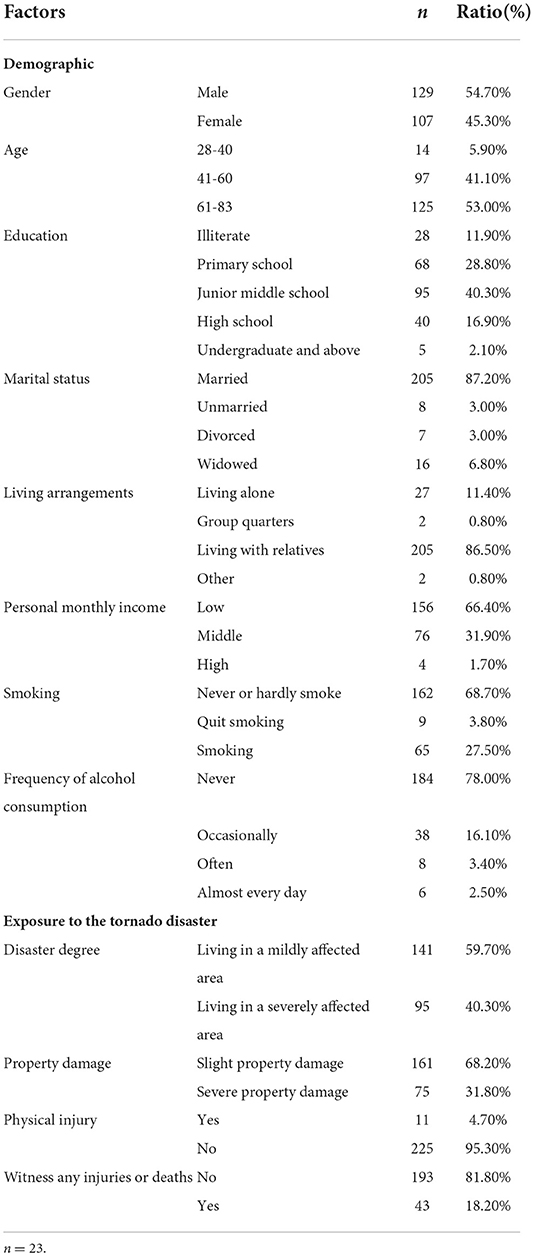
Table 1. Demographic information and characteristics of exposure to the tornado of rural residents who survived the tornado disaster.
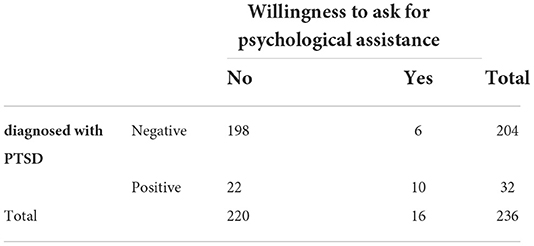
Table 2. Results of the willingness to ask for psychological assistance.
Analysis of the factors correlated with PTSD
The results of the chi-square test showed that those who were female, had severe property damage, were physically injured, were severely affected by the disaster, and witnessed injuries or deaths were more likely to have a diagnosis of PTSD. (P < 0.05) (Table 3).
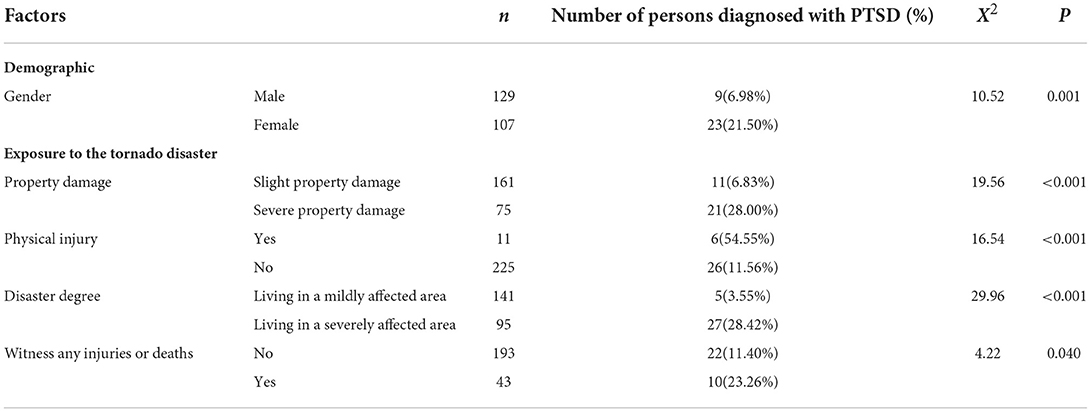
Table 3. Results of the chi-square test on collected factors in rural residents who survived the tornado disaster.
The inclusion of the factors associated with the diagnosis of PTSD from the chi-square test results in a binary logistic regression showed that being female (OR = 3.62, P = 0.023), living in area severely affected by the tornado (OR = 3.94, P = 0.032) and having severe property damage (OR = 3.72, P = 0.010) were risk factors for the diagnosis of PTSD (Table 4).
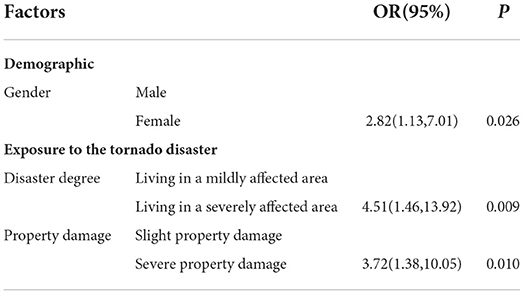
Table 4. Results of binary logistic regression on factors associated with PTSD in rural residents who survived the tornado disaster.
Detection of PTSD symptoms by symptom cluster
Table 5 shows the detection of symptoms for each dimension of PTSD among the respondents. The most common symptoms in the intrusion, avoidance and hyperarousal dimensions were feeling emotionally upset when one was reminded of the event (75.00%), trying to avoid situations that reminded one of the event (56.30%), and being overly alert (75.10%), respectively. Less common symptoms mainly focused on the avoidance dimension and included feeling alienated or distant from the people around oneself (21.90%), not being able to recall important parts of the event (28.10%), being emotionally numb (31.20%), suddenly feeling like one is living through the event again (31.30%), and feeling like one's plans for the future and hopes will not come true (37.50%). See Table 5.
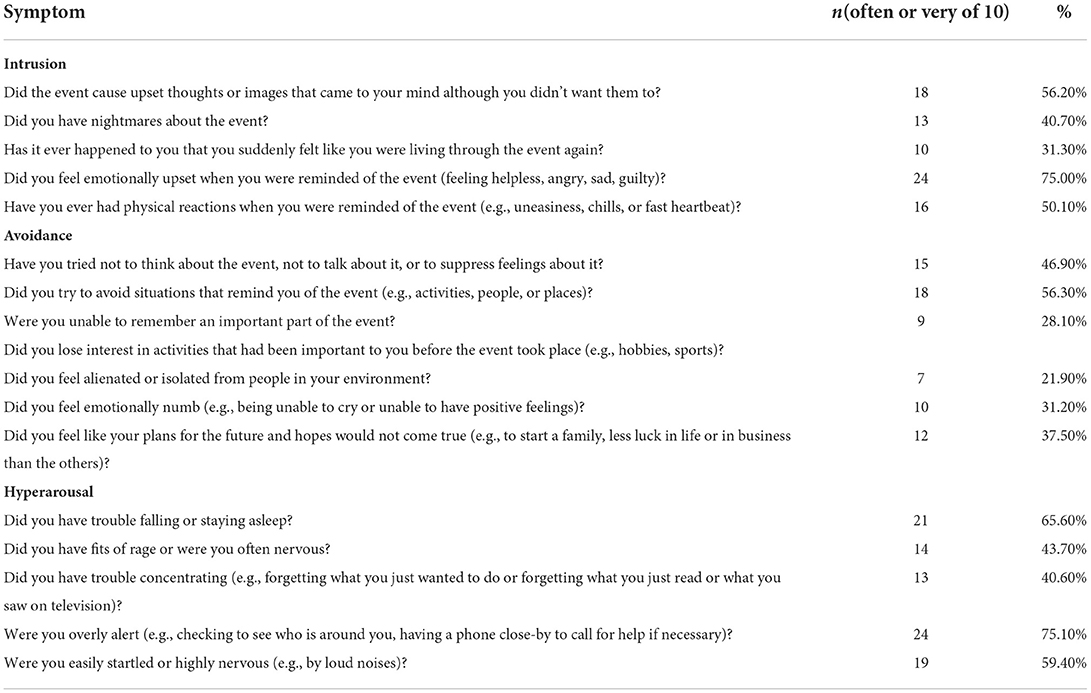
Table 5. PTSD symptoms of rural residents who survived the tornado disaster.
Discussion
This study was a field study in the affected rural villages of Caidian District conducted 1.5 months after the tornado in Caidian District, Wuhan City. The prevalences of PTSD were found to be 13.6% overall and 28.4% in the most severely affected rural villages. Risk factors for PTSD diagnosis were being female, living in a severely affected area, and having severe property damage. Compared to the typical PTSD symptoms according to the DSM-V-TR criteria, the avoidance dimension was less frequent than the other two dimensions, particularly feeling alienated or distant from the people around oneself (21.90%), not being able to recall important parts of the event (28.10%), and being emotionally numb (31.20%).
In the general Chinese population, the 1-month prevalence of PTSD was 0.195% (9), which was significantly lower than the 1-month prevalence of PTSD in the affected villagers in this study (13.60%). Previous studies on the detection rate of PTSD after disaster events have also shown varying results, with the prevalence of PTSD after earthquakes, rockfalls, mudslides and car accidents ranging from 18.80 to 43.00% (10–13). The detection rate of PTSD among the affected villagers in this study was slightly higher than the rates after tornado disasters in previous studies (14, 15). The reasons for this phenomenon may be related to the status and older age of rural residents. First, rural elderly people have more severe mental health problems overall than urban elderly people (16). Second, the affected villagers were generally older (60.60 ± 11.70). The relationship between PTSD and age in previous studies is complex and may be related to the social, economic and cultural aspects of the affected areas (17), which may indicate that PTSD shows a positive correlation with age in rural areas of China. This also suggests that we need to consider the corresponding characteristics of the population when carrying out postdisaster psychological reconstruction.
Among the demographic factors, women were at significantly higher risk for PTSD than men, which is consistent with previous research findings (18). Evidence suggests that direct trauma from disasters is an important determinant of PTSD development (18, 19). The results of this study also suggest that the degree of the disaster and property damage from the tornado disasters are significantly associated with PTSD diagnosis. In particular, the prevalence of PTSD was significantly higher in the sample from severely affected areas with severe property damage than in the sample from mildly affected areas with mild property damage. In addition, the study also investigated the willingness of the sample to seek psychological help. The results show a low overall willingness to seek help among affected people, reflecting the fact that crisis interventions may not be well received by some rural residents in the aftermath of a tornado disaster.The results also showed that individuals diagnosed with PTSD were more likely to seek psychological assistance, which could include counseling, psychotherapy, and medication. This suggests that PTSD patients suffer from the pain generated by the illness, which to some extent motivates their willingness to seek psychological assistance. In postdisaster psychological reconstruction, it is important to focus on and properly deal with victims who need help, as they are more likely to be potential PTSD sufferers. Although people with PTSD are more likely to be willing to seek psychological help, nearly two-thirds of people with PTSD are not. This may be due to a sense of stigma or a lack of knowledge about psychological assistance. Therefore, in addition to increasing the accessibility of mental health services and administering more active mental health services after a disaster, publicity and dissemination of mental health knowledge should be enhanced in rural areas before a disaster occurs to raise rural residents' awareness of mental health and crisis intervention with a view to reducing their sense of stigma about psychological problems.
In general, symptoms of PTSD vary from person to person, but intrusion, avoidance, and hyperirritability are typical symptoms (19). In the present study, most PTSD symptoms were present among the affected villagers according to the DSM-V-TR criteria, but symptoms in the avoidance dimension were less common than other symptoms. This may be because the damage to their houses caused by the disaster, as well as physical injuries, were real situations that they needed to face continuously and could not escape. In addition, interpersonal interaction was higher in rural areas than in urban areas, and the process of interacting with each other made it easier for individuals to deal with the disaster that had occurred.
This study has some limitations. First, this study adopted a cross-sectional study design, but the development of PTSD and its influencing factors are complex processes that change over time. Therefore, a follow-up longitudinal study can be carried out. Second, the sample size of this study is small, and more samples can be included later to increase the reliability of the research results. Third, SCID can not only diagnose PTSD, but also other mental disorders. For instance, MDD is highly prevalent among individuals that were affected by a disaster. This research only discuss the PTSD situation. Future studies could include other parts of the SCID for the diagnosis of other mental disorders. Lastly, The investigators found that social support and post-disaster negative life events had a significant impact on the affected people's understanding of the disaster, so the Social Support and Post-Disaster Negative Life Events could be surveyed to explore the impact of social support and post-disaster negative life events on changes in the mental health of the affected people.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Wuhan Mental Health Center. The patients/participants provided their written informed consent to participate in this study.
Author contributions
T-MW completed the manuscript draft. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.946450/full#supplementary-material
References
1. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. an empirical review of the empirical literature, 1981-2001. Psychiatry. (2002) 65: 207–39. doi: 10.1521/psyc.65.3.207.20173
2. Shannon MP, Lonigan CJ. Finch AJ, Taylor CM. Children exposed to disaster: i epidemiology of post-traumatic symptoms and symptom profiles. J Am Acad Child Adolesc Psychiatry. (1994) 33:80–93. doi: 10.1097/00004583-199401000-00012
3. Wang Z, Sha W, Gu X, Bian J, Ye Q, Zhang X, et al. Investigation on the psychological status of the wounded and their families in Wenchuan earthquake stricken areas in Sichuan. J Psychiatry. (2009) 22:193–4.
4. North CS, Nixon SJ. Shariat S, Mallonee S, McMillen JC, Spitznagel EL, et al. Psychiatric disorders among survivors of the Oklahoma City Bombing. JAMA. (1999) 282:755–62. doi: 10.1001/jama.282.8.755
5. Ge F, Fan F, Zhang L. 18 months after the Wenchuan earthquake, adolescents in Dujiangyan area suffered from PTSD, depression and anxiety. Chin J Clin Psychol. (2012) 20:172–5. doi: 10.16128/j.cnki.1005-3611.2012.02.036
6. Zhou X, Wu X, Yuan X, Chen J, Chen Q. The relationship between trauma exposure and post-traumatic stress disorder in adolescents – the role of core belief challenge, subjective fear and invasive rumination. J Psychol. (2015) 47:455–65. doi: 10.3724/SP.J.1041.2015.00455
7. First MB. Structured clinical interview for the DSM (SCID). In: The Encyclopedia of Clinical Psychology. (2014). p. 1–6. doi: 10.1002/9781118625392.wbecp351
8. Huang Y, Wang YU, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
9. Zhou J, Jin C, Zhang S, Wu C, Li F. Investigation report on mental reaction after rock avalanche and suspension bridge events in Wuxi County. Chin Mental Health J. (1988) 02:72–5.
10. He M, Wu R, Zhang X, Ji S, Chu M, Yang D. Post-traumatic stress disorder among rollover survivors. Chin Mental Health J. (1993) 190:148–51.
11. Zhao G, Yang Y, Zhang Q, Zhang S, Deng H, Zhu Y, et al. Incidence and influencing factors of post-traumatic stress disorder in community residents in Wenchuan earthquake stricken areas. Chin Mental Health J. (2009) 23:478–83. doi: 10.3969/j.issn.1000-6729.2009.07.008
12. Shi T, Jiang C, Jia S, Liu Q, Zhang J, Qi X. Evaluation scale of post-traumatic stress disorder in severe acute respiratory syndrome. Clin Rehabil. (2005) 9:44–7.
13. Adams ZW, Sumner JA, Danielson CK, McCauley JL, Resnick HS, et al. Prevalence and predictors of PTSD and depression among adolescent victims of the Spring 2011 tornado outbreak. J Child Psychol Psychiatry. (2014) 55: 1047–55. doi: 10.1111/jcpp.12220
14. Wang B, Wang X, Zhao F, Zhang L. Investigation on post-traumatic stress disorder of tornado wounded. J PLA Hospital Manag. (2020) 28:408–10. doi: 10.16770/J.cnki.1008-9985.2021.05.003
15. Ye B, Chen L, Gao J, Fu H. Relationship between perception of age discrimination and depressive symptoms in middle-aged and elderly people in rural areas. Chin Mental Health J. (2019) 33:524–9. doi: 10.3969/j.issn.1000-6729.2019.07.011
16. Norris FH, Kaniasty K, Conrad ML, Inman GL, Murphy AD. Placing age differences in cultural context: a comparison of the effects of age on PTSD after disasters in the United States, Mexico, and Poland. J Clin Geropsychol. (2002) 8:153–73. doi: 10.1023/A:1015940126474
17. Sareen J. Post-traumatic stress disorder in adults: impact, comorbidity, risk factors, and treatment. Can J Psychiatry. (2014) 59:460–7. doi: 10.1177/070674371405900902
18. Scott ST. Multiple traumatic experiences and the development of post-traumatic stress disorder. J Interpers Violence. (2007) 22:932–8. doi: 10.1177/0886260507301226
Keywords: tornado disaster, post-traumatic stress disorder, structured clinical interview for DSM-V (SCID), symptoms, correlates, prevalence
Citation: Wu T-M, Yang Q, Huang Y-J, Zhong B-L, Zhang J and Liu L-Z (2022) Prevalence and correlates of post-traumatic stress disorder and its symptomatology in tornado-affected rural residents. Front. Psychiatry 13:946450. doi: 10.3389/fpsyt.2022.946450
Received: 17 May 2022; Accepted: 11 July 2022;
Published: 08 August 2022.
Edited by:
Antonio Vita, University of Brescia, ItalyReviewed by:
Liang Zhou, Guangzhou Medical University, ChinaHongxian Shen, Central South University, China
Copyright © 2022 Wu, Yang, Huang, Zhong, Zhang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lian-Zhong Liu, MTg0OTIzMDQ3QHFxLmNvbQ==; Juan Zhang, ZHVvZHVvemh1MDExMDA5QDE2My5jb20=