 Nerea Almeda
Nerea Almeda Irene Gómez-Gómez
Irene Gómez-Gómez
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 12 July 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.941575
This article is part of the Research Topic Mental health care worldwide: a post-pandemic recovery approach View all 5 articles
The COVID-19 pandemic has generated a global health crisis that has negatively impacted the mental health and wellbeing of the population. A large amount of scientific literature has emerged since 2019, but none of these studies have focused on assessing the impact of COVID-19 on smoking consumption. We aimed to analyse the changes in smoking consumption during the COVID-19 pandemic through longitudinal studies. This systematic review follows the PRISMA Statement. This study was registered on PROSPERO (CRD42021282235). MEDLINE, ERIC, PsycARTICLES, Scopus, Web of Science and PsycINFO databases were searched from inception to 24 October 2021. We completed an extensive assessment of all prospective cohort studies that aimed to explore the effect of the COVID-19 pandemic on tobacco consumption habits. According to the PICOS's acronym, we included all population (P) types and studies developed before and during the COVID-19 pandemic (I) with a change in nicotine consumption as the outcome (O), as well as prospective cohort studies. The risk of bias was assessed using the Newcastle–Ottawa Scale for observational studies. The results showed that 14 cohorts reported in 11 articles fulfilled the inclusion criteria. A total of 58,052 participants were included in the review. Most of the studies pointed out a reduction in the number of cigarettes and e-cigarettes consumed from baseline (before the pandemic) to follow-up (during the pandemic). Only two studies reported an increase in cigarette or e-cigarette consumption from baseline to follow-up. The majority of studies presented a low risk of bias. In conclusion, the impact of the COVID-19 pandemic on smoking behavior is complex and uncertain. The decrease in smoking consumption during the pandemic could be related to the fear of becoming infected by COVID-19, the advancement of COVID-19, and the reduction in social gatherings. In several cases, the increases in nicotine consumption can be explained by psychological distress. These findings can be used to create strategies to prevent relapses during the post-vaccination phases of the pandemic.
Systematic Review Registration: PROSPERO, identifier: CRD42021282235.
The novel coronavirus disease (COVID-19) was identified for the first time in Wuhan (China) on 31 December 2019 (1). For over 2 years, the global pandemic caused 528,816,317 confirmed cases of COVID-19 and 6,294,969 deaths on 1 June 2022, while 11,947,644,522 vaccine doses have been administered worldwide (2). During these 2 years, the governments declared lockdown and imposed several containment measures (quarantine, isolation and social distancing) to detain the spread of the virus (3–5). These measures have detained the virus contagion and have generated a worsening in mental health and impacted health behaviors (6–8).
Due to containment measures, lockdowns and the global crisis caused by the pandemic, the population has inevitably suffered from changes in health behaviors such as sleep, substance abuse, physical activity and diet, which could have long-term consequences on global health (9). It is worth highlighting that the COVID-19 pandemic has caused more than a health crisis, which has impacted society and the economy, increasing poverty and inequalities globally (10). The pandemic has also generated psychosocial and socioeconomic insecurities that impacted wellbeing (11). In this sense, socioeconomic conditions such as deprivation and low-income increase perceived stress levels and, consequently, the development of risk behaviors such as daily smoking (12).
Considering that the COVID-19 pandemic has pushed people worldwide to change their daily lives and sociodemographic conditions (loss of job and income) and has raised their mental health conditions, it is expected that the coronavirus has also had an impact on health risk behaviors such as smoking consumption. Scientific literature points out that the relationship between smoking consumption and COVID-19 is complex. Nicotine consumption can be increased during the pandemic (13). Nevertheless, other studies found that smoking consumption might have been reduced (14). Following the first assumption, several studies have shown that high anxiety levels, stress and isolation suffered during the pandemic might have increased cigarette consumption (15). Additionally, a recent study showed that although 46.7% of smokers thought about quitting because of COVID-19, most did not change their smoking habits during the pandemic (16). On the other hand, smoking consumption might have been decreased because of perceived pulmonary potential risks, lower access opportunities and lower social interactions because of the lockdowns (17). Being scared of getting infected by COVID-19 and believing coronavirus is more severe for smokers might have decreased smoking consumption (18).
Previous systematic reviews and meta-analyses have focused on evaluating the impact of smoking on COVID-19 progression and severity. The main findings pointed out that users with any smoking history (currently or in the past) had an increased and significant risk of developing severe symptoms and worse hospital outcomes in terms of mortality, disease progression and need for medical ventilation (19–22). As far as we are, concerned there is no systematic review assessing how the COVID-19 pandemic has affected smoking consumption, which is crucial to identifying risk factors for wellbeing.
The potential effect of the COVID-19 pandemic on smoking behavior is still uncertain, and a better understanding of the magnitude of nicotine consumption because of the COVID-19 pandemic is required to predict long-term consequences on global population health. Additionally, it is crucial to help health services and policy-makers cope with the impact of COVID-19 and provide an appropriate response. Therefore, the objective of this systematic review is to analyse how the patterns of nicotine consumption changed during the COVID-19 pandemic through longitudinal studies.
This systematic review was developed following PRISMA guidelines (23, 24). The protocol of this study was previously registered at PROSPERO on October 1, 2021 (PROSPERO ID: CRD42021282235). According to the protocol, a systematic review and meta-analysis study were planned. However, due to considerable (I2 = 92.7%; 95% CI, 916% to 95%) and significant heterogeneity between the included studies (Q18 = 264.13; p < 0.001), the meta-analysis was not performed. These analyses were performed based on Cochran's Q statistic, its p-value and I2 index and its 95% CI.
The search strategies were implemented in MEDLINE (via OVID and PubMed), ERIC (via OVID), PsycARTICLES (via OVID), Scopus, Web of Science (WOS) and PsycINFO from database inception to 24 October 2021. In addition, the reference lists of included articles were reviewed manually. The search strategy included the following three sets of relevant terms: a set of words related to COVID-19, a second set made up of a combination of words related to tobacco consumption, and the third set of words related to the design of the studies. The words included within the sets were combined with the Boolean OR, while the three sets of words were combined with the Boolean AND. All words were searched by title and abstract. The search was piloted in PubMed and then adapted to run across OVID, Scopus, WOS and PsycINFO. The search strategies in all databases are shown in Supplementary Material.
The rationale for our inclusion criteria was to have an extensive assessment of all prospective cohort studies that aim to explore the effect of the COVID-19 pandemic on tobacco consumption habits. Following PICOS's acronym, we included all types of populations (P). We aimed to explore studies developed before and during the COVID-19 pandemic (I/E) regarding intervention or exposure. A comparator was not applicable (C). The outcome was a change in nicotine consumption habits (O), and the study design was exclusively prospective cohort studies. No restrictions were imposed regarding publication year, language, or study setting. Table 1 shows the inclusion and exclusion criteria.
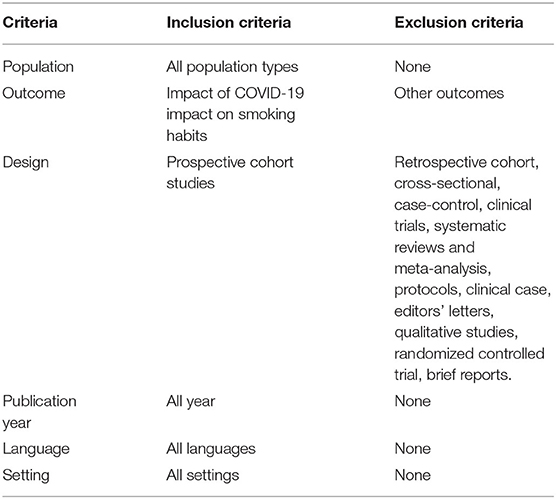
Table 1. Inclusion and exclusion criteria.
Two reviewers (NA and IGG) independently screened the studies in two phases to assess eligibility: (1) abstracts and title inspection and (2) full-text inspection. Disagreements were resolved by consensus between both reviewers (NA and IGG), and in case of disagreement, a third reviewer made the final decision. The web-based software Rayyan system was used for recording decisions (25). The initial degree of agreement between the reviewers at the abstract and title inspection phases (Cohen κ = 0.43; 95% CI, 0.227 to 0.636) and the full-text inspection phase (Cohen κ = 0.94; 95% CI, 0.810 to 1.060) was moderate and very good, respectively.
Two reviewers (NA and IGG) independently extracted all qualitative and quantitative relevant characteristics in an Excel sheet specifically created for the study. Discrepancies between reviewers were resolved by consensus. For the qualitative synthesis, first authors & publication year, region & country, target population, sex, sample size at baseline, sample size at follow-up, the main outcome, smoking consumption measure, number of smokers at baseline, number of smokers at follow-up results were extracted. The corresponding authors of the included studies were contacted to request more information when necessary.
Previous evidence suggests that the strictness of government policies taken to deal with the COVID-19 pandemic have an influence on tobacco use behaviors (26, 27). Thus, a part from the variables reported above, the COVID-19 stringency index (as a measure of country-level response to COVID-19) created by the Oxford COVID-19 Government Response Tracker (OxCGRT), was used (28) to calculate the mean daily COVID-19 stringency index. The COVID-19 stringency index uses nine criteria (school and work closures, restrictions on public gatherings, annulment of public events, closures of public transport, stay-at-home requirements, public information campaigns, restrictions on internal movements, and international travel controls) to calculate an index that ranges from 0 to 100. The higher the score, the greater the restrictive response. The mean daily COVID-19 stringency index was calculated for each study taking into account the follow-up period of each study. To do so, the daily COVID-19 stringency indexes during the periods, in which the follow-up of each study was carried out, have been sum and divided by the total number of days included in the follow-up.
The risk of bias in the included studies was measured independently by two reviewers (NA and IGG) using the Newcastle–Ottawa Scale for observational studies (NOS) (29). The NOS scale consists of eight items divided across three domains: (1) selection of the cohort, (2) comparability of the cohort and (3) outcome. Each study is evaluated through the assignment of stars. Each study can only receive one star for each item in the selection and outcome categories and a maximum of two stars for comparability. The stars designate the items with a low risk of bias. Thus, according to the NOS scale, the risk of bias in each study might be interpreted as follows: very high risk of bias (0–3 stars), high risk of bias (4–6 stars), and low risk of bias (7–9 stars) (30).
A total of 1,300 records were found through databases, and 9 records were found through other sources (reference lists inspection of the included articles in full-text screening). After eliminating duplicates, 509 records remained and were reviewed for the title and abstract inspection. Of these, 31 studies met the inclusion criteria and were reviewed for full-text inspection. Finally, 14 cohorts reported in 11 publications met the inclusion criteria for the systematic review (see Figure 1). We must note that the study of García-Esquinas et al. (31) included four different cohort studies (ENRICA cohort study, ES cohort study, TSHA cohort study and Exernet cohort study) in the same publication.
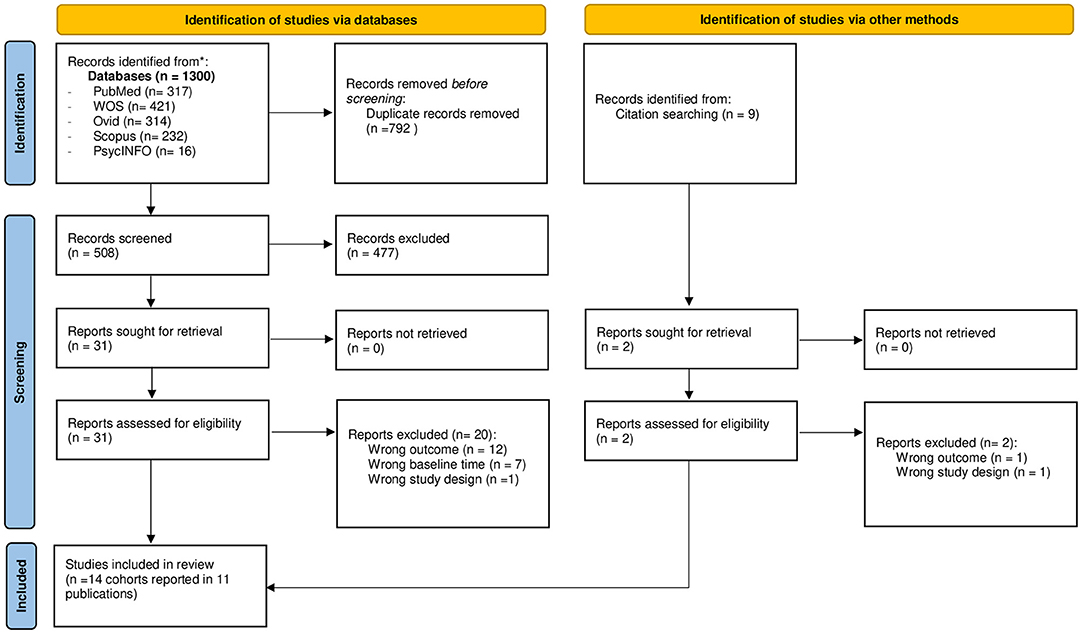
Figure 1. PRISMA 2020 flow diagram of the studies included.
Table 2 shows the qualitative characteristics of the included studies. A total of 58052 participants were included across 14 cohorts reported in 11 publications. The sample size ranged from 295 (35) to 22,823 (34) (median = 1,642). All of the included studies were published in 2021. A total of 45.5% (n = 5) of the studies were conducted in Europe (31, 33, 34, 37, 40), while 36.4% (n = 4) were conducted in the USA (32, 35, 38, 42) and 18.2% (n = 2) in Asia (39, 41).
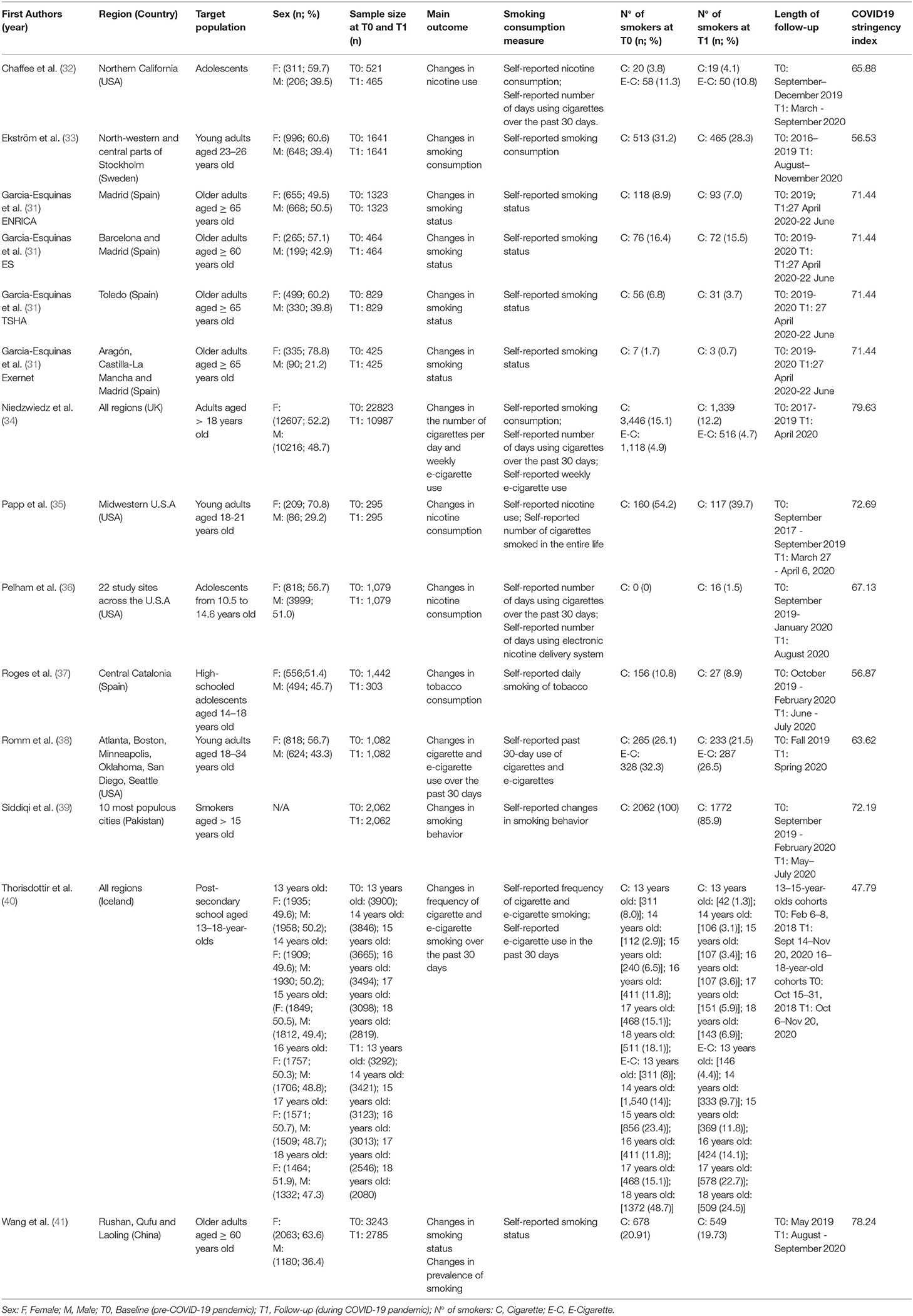
Table 2. Characteristics of the studies included in the systematic review.
Related to the target population, four (36.4%) of the studies included adolescents (32, 36, 37, 40), three (27.3%) included young adults (33, 35, 38), two (18.2%) included adults (34, 39) and two (18.2%) included older adults (31, 41).
Five studies (45.5%) reported changes in nicotine, smoking or tobacco consumption as the main outcome (32, 33, 35–37). Three studies (27.3%) reported changes in cigarette use as the main outcome (34, 38, 40), and two studies (18.2%) reported changes in smoking status (31, 41). In addition, four studies (36.4%) reported information about e-cigarette consumption (32, 34, 38, 40).
Regarding the smoking consumption measure, all studies used self-reported questions about nicotine, smoking or tobacco consumption; smoking status; the number of cigarettes/e-cigarettes smoked over a specific period; and the number of days using tobacco products over a specific period. Of those, three studies (27.3%) reported both self-reported nicotine/smoking consumption and self-reported number of days using cigarettes or number of cigarettes smoked over a specific period (32, 34, 35).
The percentage of cigarette smokers at baseline (pre-COVID-19 pandemic) and follow-up (during COVID-19 pandemic) varied across studies. At baseline, it ranges from 0% (36) to 100% (39), while at follow-up, it ranges from 0.7% (García-Esquinas et al., (31) - Exernet cohort) to 85.9% (39). Regarding the number of e-cigarette smokers, a lower prevalence was observed than in traditional cigarettes. It ranged from 11.3% (32) to 48.7% (40) at baseline and from 10.8 (32) to 26.5 (38) at follow-up. The majority of the studies showed a reduction in cigarette and e-cigarette smokers from baseline to follow-up. Only two studies (18.2%) reported an increase in cigarette (36) or e-cigarette (40) consumption from baseline to follow-up.
Finally, the mean daily COVID-19 stringency index varied from 47.79 to 79.63 (Mean: 67.59; SD: 8.8). The two studies with the highest COVID-19 stringency index at follow-up were conducted in China (41) and the United Kingdom (34) and both of them showed a reduction in the percentage of cigarette and/or e-cigarette smokers.
The risk of bias in the included studies is shown in Table 3. All the studies had a low risk of bias in the categories of representative of the non-exposed cohort, selection of the non-exposed cohort, a demonstration that the outcome of interest was not present at the start of the study, and comparability of cohorts and adequate length of follow-up. In addition, all studies except one (37) had a low risk of bias in the adequacy of follow-up of the cohort category. Because self-reported measures were used in all of the studies, a high risk of bias was observed for the categories of ascertainment of exposure and assessment of outcome. By considering this, it can be concluded that all studies except one (37) presented a low risk of bias.
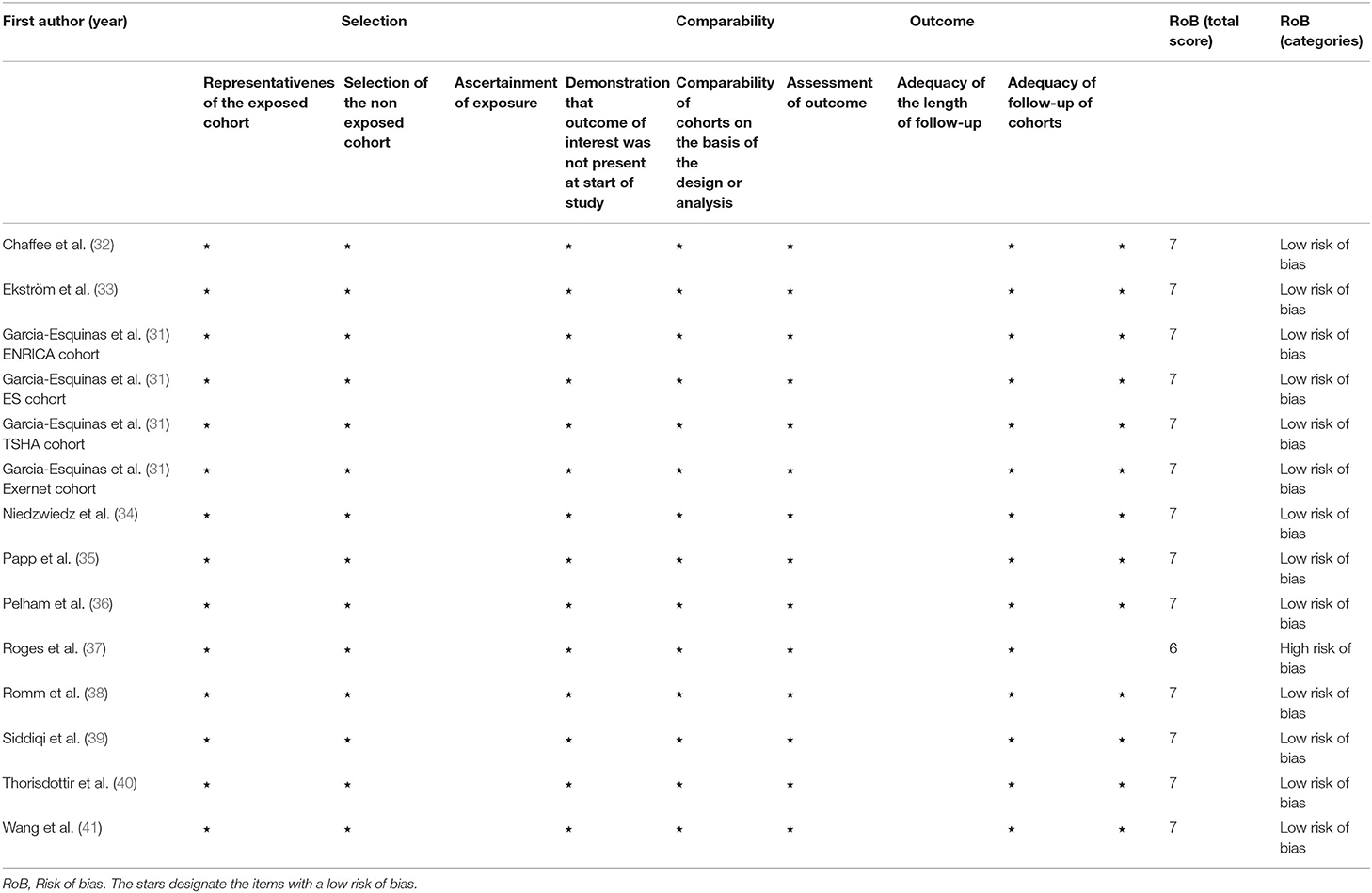
Table 3. Risk of bias of the included studies.
In this systematic review, we aimed to analyse how the patterns of nicotine consumption changed during the COVID-19 pandemic through longitudinal studies.
To the best of our knowledge, this is the first systematic review assessing the impact of COVID-19 on smoking consumption behavior. Global results of this systematic review evidenced that the pattern of tobacco use have decreased during the pandemic. Most smokers decreased the number of cigarettes and e-cigarettes consumed from baseline (before the COVID-19 pandemic) to follow-up (during the COVID-19 pandemic). Consistent with previous research, reductions in smoking consumption might be explained by less difficulty in quitting smoking and higher motivation to quit because of fear of the pandemic and COVID-19 negative progression (14, 18, 43). In this sense, the pandemic and fear of being infected by COVID-19 have motivated patients to quit or reduce smoking (44). Additionally, lockdowns worldwide and a reduction in social activities might have reduced the opportunities for social smoking or even the accessibility to buy cigarettes (45). In this line, we have to note that the studies with the highest COVID-19 mean daily stringency index presented reductions in the percentage of cigarette and/or e-cigarette smokers. According to this, United Kingdom, China (Rushan, Qufu and Laoling regions), Midwestern U.S.A (USA), Pakistan and Spain (Barcelona, Madrid, Toledo, Aragón and Castilla-La Mancha) showed the highest COVID-19 mean daily stringency index and an evidenced reduction in smoking consumption. However, a previous meta-analysis did not find an association between prevalence of smoking and mean daily stringency indexes (46).
Therefore, the evolution of the pandemic might have positively impacted population wellbeing in terms of smoking consumption.
Iceland and USA (22 study sites across the U.S.A) showed an increment in tobacco consumption in comparison with pre-pandemic level (36, 40). It is worthy to highlight the case of USA, which can show patterns variations in smoking consumption across different states. This increase might be caused by feelings of boredom during the lockdown (47). Additionally, smoking can be considered an unhealthy strategy to cope with stress, where people feel that they do not control the number of cigarettes they consume (48).
This study presents some limitations. First, following the PROSPERO register, a systematic review and meta-analysis study was planned. However, it was impossible to perform the study's meta-analytic part due to the high heterogeneity between studies. Regarding smoking status measures, all of the studies evaluated smoking status by self-reported questions. This might be explained by many of the studies assessing smoking as a secondary outcome. In addition, most of the studies collected data through online surveys due to the exceptional circumstances derived from the COVID-19 pandemic. Regarding population, we must note that many of the studies were focused on young populations. Therefore, our conclusions apply mainly to this population profile. Despite these limitations, this systematic review addressed a novel topic. To the best of our knowledge, we must note that all previous systematic reviews aimed to explore the effect of smoking on COVID-19 severity (19, 20, 49–51). Apart from that, we must note that this study explore the most relevant databases in the area combined with extensive supplementary hand searching. Moreover, many participants from different countries and continents were included, supporting its external validity. In addition, Supplementary Material about the COVID-19 pandemic situation in each country during the follow-up periods was included by using the COVID-19 stringency index. Regarding methodology, study selection, data extraction and risk of bias assessment were performed by two independent reviewers following the PRISMA statement.
The impact of the COVID-19 pandemic on smoking behavior is complex and unclear. The results from this systematic review indicate that, in most cases, smoking consumption has decreased during the COVID-19 pandemic, while this global health crisis has been considered a good opportunity to reduce or quit smoking. Fear of becoming infected by COVID-19 and developing a maladaptive progression of the infection have motivated people to drop out of this habit. Lockdown and social restrictions have also played a crucial role in decreasing nicotine consumption. Nevertheless, in some cases, the pandemic has negatively affected smoking behavior. In these cases, the increase in nicotine consumption during the pandemic may be caused by boredom, stress and anxiety. These findings support the development of prevention and intervention strategies during the recovery phase of the pandemic to help people reduce smoking and avoid relapses in people who have quit.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
NA and IG-G designed and conducted the study, prepared the initial protocol draft, and revised the manuscript. IG-G supervised the methodology. All authors read, provided feedback, discussed and approved the final manuscript.
This study was supported by the Universidad Loyola Andalucía.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the Universidad Loyola Andalucía for their support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.941575/full#supplementary-material
1. World Health Organization. Brote de enfermedad por coronavirus (COVID-19). (2021). Available online at: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019 (accessed April 2022).
2. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. (2021). Available online at: https://covid19.who.int/ (accessed April 2022).
3. World Health Organization. Considerations for quarantine of contacts of COVID-19 cases. Interim guidance. (2021). Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-IHR-Quarantine-2021.1 (accessed April 2022).
4. Islam N, Sharp SJ, Chowell G, Shabnam S, Kawachi I, Lacey B, et al. Physical distancing interventions and incidence of coronavirus disease 2019: natural experiment in 149 countries. BMJ. (2020) 370:m2743. doi: 10.1136/bmj.m2743
5. Jarvis CI, Gimma A, van Zandvoort K, Wong KLM, Abbas K, Villabona-Arenas CJ, et al. The impact of local and national restrictions in response to COVID-19 on social contacts in England: a longitudinal natural experiment. BMC Med. (2021) 19:52. doi: 10.1186/s12916-021-01924-7
6. McBride E, Arden MA, Chater A, Chilcot J. The impact of COVID-19 on health behaviour, well-being, and long-term physical health. Br J Health Psychol. (2021) 26:259–70. doi: 10.1111/bjhp.12520
7. Quittkat HL, Düsing R, Holtmann F-J, Buhlmann U, Svaldi J, Vocks S. Perceived Impact of Covid-19 Across Different Mental Disorders: A Study on Disorder-Specific Symptoms, Psychosocial Stress and Behavior. Front Psychol. (2020) 11:586246. doi: 10.3389/fpsyg.2020.586246
8. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
9. Arora T, Grey I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J Health Psychol. (2020) 25:1155–63. doi: 10.1177/1359105320937053
10. United Nations Development Programme. COVID-19 SOCIO-ECONOMIC IMPACT. (2021). Available online at: https://www.undp.org/coronavirus/socio-economic-impact-covid-19 (accessed April 2022).
11. Bodrud-Doza M, Shammi M, Bahlman L, Islam ARMT, Rahman MM. Psychosocial and Socio-Economic Crisis in Bangladesh Due to COVID-19 Pandemic: A Perception-Based Assessment. Front Public Heal. (2020) 8:341. doi: 10.3389/fpubh.2020.00341
12. Algren MH, Ekholm O, Nielsen L, Ersbøll AK, Bak CK, Andersen PT. Associations between perceived stress, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: a cross-sectional study. BMC Public Health. (2018) 18:250. doi: 10.1186/s12889-018-5170-x
13. Gendall P, Hoek J, Stanley J, Jenkins M, Every-Palmer S. Changes in Tobacco Use During the 2020 COVID-19 Lockdown in New Zealand. Nicotine Tob Res. (2021) 23:866–71. doi: 10.1093/ntr/ntaa257
14. Rebollar Álvarez A, Nuez Vicente C, Lozano Polo A, Pérez Ríos M, Pola Ferrández E, Furió Martínez AM, et al. Tobacco use in Spain during COVID-19 lockdown: an evaluation through social media. Rev Esp Salud Publica. (2021) 95:e1–11.
15. Kowitt SD, Cornacchione Ross J, Jarman KL, Kistler CE, Lazard AJ, Ranney LM, et al. Tobacco quit intentions and behaviors among cigar smokers in the United States in response to COVID-19. Int J Environ Res Public Health. (2020) 17:5368. doi: 10.3390/ijerph17155368
16. Gravely S, Craig L V, Cummings KM, Ouimet J, Loewen R, Martin N, et al. Smokers' cognitive and behavioural reactions during the early phase of the COVID-19 pandemic: Findings from the 2020 ITC Four Country Smoking and Vaping Survey. PLoS ONE. (2021) 16:e0252427. doi: 10.1371/journal.pone.0252427
17. Tattan-Birch H, Perski O, Jackson S, Shahab L, West R, Brown J. COVID-19, smoking, vaping and quitting: a representative population survey in England. Addiction. (2021) 116:1186–95. doi: 10.1111/add.15251
18. Bommelé J, Hopman P, Hipple Walters B, Geboers C, Croes E, Fong GT, et al. The double-edged relationship between COVID-19 stress and smoking: implications for smoking cessation. Tob Induc Dis. (2020) 18:63. doi: 10.18332/tid/125580
19. Reddy RK, Charles WN, Sklavounos A, Dutt A, Seed PT, Khajuria A. The effect of smoking on COVID-19 severity: a systematic review and meta-analysis. J Med Virol. (2021) 93:1045–56. doi: 10.1002/jmv.26389
20. Patanavanich R, Glantz SA. Smoking is associated with COVID-19 progression: a meta-analysis. Nicotine Tob Res. (2020) 22:1653–6. doi: 10.1093/ntr/ntaa082
21. Umnuaypornlert A, Kanchanasurakit S, Lucero-Prisno DEI, Saokaew S. Smoking and risk of negative outcomes among COVID-19 patients: a systematic review and meta-analysis. Tob Induc Dis. (2021) 19:9. doi: 10.18332/tid/132411
22. Shastri MD, Shukla SD, Chong WC KC R, Dua K, Patel RP, Peterson GM, et al. Smoking and COVID-19: what we know so far. Respir Med. (2021) 176:106237. doi: 10.1016/j.rmed.2020.106237
23. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
24. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
25. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–10. doi: 10.1186/s13643-016-0384-4
26. Milovanovi I, Bakala P. Maintaining everyday life praxis in the time of COVID-19 pandemic measures (ELP-COVID-19 survey). Eur J Public Health. (2020) 30:1181–6. doi: 10.1093/eurpub/ckaa157
27. Jackson SE, Brown J, Beard E, Angus C, Field M. Moderators of changes in smoking, drinking and quitting behaviour associated with the first COVID-19 lockdown in England. Addiction. (2022) 117:772–83. doi: 10.1111/add.15656
28. Hale T, Angrist N, Goldszmidt R, Kira B, Petherick A, Phillips T, et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. (2021) 5:529–38. doi: 10.1038/s41562-021-01079-8
29. Wells G, Shea B, O'Connell D, Peterson J, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (2018). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed April 2022).
30. Lo CKL, Mertz D, Loeb M. Newcastle-Ottawa Scale: Comparing reviewers' to authors' assessments. BMC Med Res Methodol. (2014) 14:1–5. doi: 10.1186/1471-2288-14-45
31. García-Esquinas E, Ortolá R, Gine-Vázquez I, Carnicero JA, Mañas A, Lara E, et al. Changes in health behaviors, mental and physical health among older adults under severe lockdown restrictions during the covid-19 pandemic in spain. Int J Environ Res Public Health. (2021) 18:7067. doi: 10.3390/ijerph18137067
32. Chaffee BW, Cheng J, Couch ET, Hoeft KS, Halpern-Felsher B. Adolescents' substance use and physical activity before and during the COVID-19 pandemic. JAMA Pediatr. (2021) 175:715. doi: 10.1001/jamapediatrics.2021.0541
33. Ekström S, Andersson N, Lövquist A, Lauber A, Georgelis A, Kull I, et al. COVID-19 among young adults in Sweden: self-reported long-term symptoms and associated factors. Scand J Public Health. (2021) 50:85–93. doi: 10.1177/14034948211025425
34. Niedzwiedz CL, Green MJ, Benzeval M, Campbell D, Craig P, Demou E, et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: longitudinal analyses of the UK Household Longitudinal Study. J Epidemiol Community Health. (2021) 75:224–31. doi: 10.1101/2020.06.21.20136820
35. Papp LM, Kouros CD. Effect of COVID-19 disruptions on young adults' affect and substance use in daily life. Psychol Addict Behav. (2021) 35:391–401. doi: 10.1037/adb0000748
36. Pelham WE, Tapert SF, Gonzalez MR, McCabe CJ, Lisdahl KM, Alzueta E, et al. Early adolescent substance use before and during the COVID-19 pandemic: a longitudinal survey in the ABCD study cohort. J Adolesc Health. (2021) 69:390–7. doi: 10.1016/j.jadohealth.2021.06.015
37. Rogés J, Bosque-Prous M, Colom J, Folch C, Barón-Garcia T, González-Casals H, et al. Consumption of alcohol, cannabis, and tobacco in a cohort of adolescents before and during COVID-19 confinement. Int J Environ Res Public Health. (2021) 18:1–14. doi: 10.3390/ijerph18157849
38. Romm KF, Patterson B, Crawford ND, Posner H, West CD, Wedding D, et al. Changes in young adult substance use during COVID-19 as a function of ACEs, depression, prior substance use and resilience. Subst Abus. (2021) 43:212–21. doi: 10.1080/08897077.2021.1930629
39. Siddiqi K, Siddiqui F, Khan A, Ansaari S, Kanaan M, Khokhar M, et al. The impact of COVID-19 on smoking patterns in pakistan: findings from a longitudinal survey of smokers. Nicotine Tob Res. (2021) 23:765–9. doi: 10.1093/ntr/ntaa207
40. Thorisdottir IE, Asgeirsdottir BB, Kristjansson AL, Valdimarsdottir HB, Jonsdottir Tolgyes EM, Sigfusson J, et al. Depressive symptoms, mental wellbeing, and substance use among adolescents before and during the COVID-19 pandemic in Iceland: a longitudinal, population-based study. Lancet Psychiatry. (2021) 8:663–72. doi: 10.1016/S2215-0366(21)00156-5
41. Wang Y, Fu P, Li J, Jing Z, Wang Q, Zhao D, et al. Changes in psychological distress before and during the COVID-19 pandemic among older adults: the contribution of frailty transitions and multimorbidity. Age Ageing. (2021) 50:1011–8. doi: 10.1093/ageing/afab061
42. Peckham E, Allgar V, Crosland S, Heron P, Johnston G, Newbronner E, et al. Investigating smoking and nicotine dependence among people with severe mental illness during the COVID-19 pandemic: analysis of linked data from a UK Closing the Gap cohort. BJPsych Open. (2021) 7:1–3. doi: 10.1192/bjo.2021.45
43. Duong HT, Massey ZB, Churchill V, Popova L. Are smokers scared by COVID-19 risk? How fear and comparative optimism influence smokers' intentions to take measures to quit smoking. PLoS ONE. (2021) 16:e0260478. doi: 10.1371/journal.pone.0260478
44. Gold AK, Hoyt DL, Milligan M, Hiserodt ML, Samora J, Leyro TM, et al. The role of fear of COVID-19 in motivation to quit smoking and reductions in cigarette smoking: a preliminary investigation of at-risk cigarette smokers. Cogn Behav Ther. (2021) 50:295–304. doi: 10.1080/16506073.2021.1877340
45. Filby S, van der Zee K, van Walbeek C. The temporary ban on tobacco sales in South Africa: lessons for endgame strategies. Tobacco Control. (2021) 1–7. doi: 10.1136/tobaccocontrol-2020-056209
46. Sarich P, Cabasag CJ, Liebermann E, Vaneckova P, Carle C, Hughes S, et al. Tobacco smoking changes during the fi rst pre- vaccination phases of the COVID-19 pandemic : A systematic review and meta-analysis. eClinicalMedicine. (2022) 47:101375. doi: 10.1016/j.eclinm.2022.101375
47. Vanderbruggen N, Matthys F, Van Laere S, Zeeuws D, Santermans L, Van den Ameele S, et al. Self-Reported Alcohol, Tobacco, and Cannabis Use during COVID-19 Lockdown Measures: Results from a Web-Based Survey. Eur Addict Res. (2020) 26:309–15. doi: 10.1159/000510822
48. Maloney SF, Combs M, Scholtes RL, Underwood M, Kilgalen B, Soule EK, et al. Impacts of COVID-19 on cigarette use, smoking behaviors, and tobacco purchasing behaviors. Drug Alcohol Depend. (2021) 229:109144. doi: 10.1016/j.drugalcdep.2021.109144
49. Umnuaypornlert A, Kanchanasurakit S, Lucero-Prisno III DE, Saokaew S. Smoking and Risk of Negative Outcomes Among COVID-19 patients: a systematic review and meta-analysis. SSRN Electron J. (2020) 19:6–8. doi: 10.2139/ssrn.3634871
50. Mo X, Jian W, Su Z, Chen M, Peng H, Peng P, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J. (2020) 55:2001217. doi: 10.1183/13993003.01217-2020
Keywords: COVID-19, smoking, prospective cohort studies, systematic review, mental health, tobacco
Citation: Almeda N and Gómez-Gómez I (2022) The Impact of the COVID-19 Pandemic on Smoking Consumption: A Systematic Review of Longitudinal Studies. Front. Psychiatry 13:941575. doi: 10.3389/fpsyt.2022.941575
Received: 11 May 2022; Accepted: 09 June 2022;
Published: 12 July 2022.
Edited by:
S. M. Yasir Arafat, Enam Medical College, BangladeshReviewed by:
Zainab Alimoradi, Qazvin University of Medical Sciences, IranCopyright © 2022 Almeda and Gómez-Gómez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene Gómez-Gómez, aWdvbWV6Z0B1bG95b2xhLmVz
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.