
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 11 August 2022
Sec. Adolescent and Young Adult Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.937723
 Adam Mabrouk1†
Adam Mabrouk1† Gideon Mbithi1*
Gideon Mbithi1* Esther Chongwo1
Esther Chongwo1 Ezra Too1
Ezra Too1 Ahmed Sarki2,3
Ahmed Sarki2,3 Mary Namuguzi2
Mary Namuguzi2 Joseph Atukwatse2Derrick Ssewanyana4
Joseph Atukwatse2Derrick Ssewanyana4 Amina Abubakar1,5*
Amina Abubakar1,5*Background: Globally, adolescents are vulnerable to mental health problems, particularly those from sub-Saharan Africa (SSA) due to impoverished living conditions and a higher prevalence of chronic conditions such as HIV/AIDS in the region. The COVID-19 pandemic has further exacerbated this risk. This calls for an urgent need for evidence-based adolescent mental health interventions to reduce the risk and burden of mental health problems in SSA. The review aims to identify and characterize existing adolescent mental health interventions in SSA, as well as to evaluate their implementation strategies and effectiveness.
Methods: We systematically searched PubMed, African Index Medicus, PsycINFO, Web of Science, and CINAHL databases for relevant articles. Furthermore, we searched gray literature databases, including Think Tank search, open gray, NGO search engine, and IGO search engine for additional relevant articles. The scoping review was conducted to identify original research articles on mental health interventions among adolescents in sub-Saharan Africa published from database inception to 31 December 2021. We carried out a narrative synthesis to report our findings.
Results: Our literature search generated 4,750 studies, of which 1,141 were duplicates, 3,545 were excluded after screening, and 64 articles met the inclusion criteria. The 64 studies describe a total of 57 unique mental health interventions comprising 40,072 adolescents. The nature of these interventions was diverse, encompassing various implementation strategies such as economic-based, family strengthening, psychoeducation, interpersonal psychotherapy, Cognitive Behavioral Therapy, and resilience training, among others. Most of the interventions were selective interventions that targeted adolescents at high risk of developing mental health problems including adolescents living with HIV, war-affected adolescents, orphans, adolescents from poorer backgrounds, and survivors of sexual violence. Half of the interventions were delivered by lay persons. Sixty-two of the eligible studies examined the effectiveness of the mental health interventions, of which 55 of them reported a positive significant impact on various mental health outcomes.
Conclusions: The review findings show that there exist several diverse interventions that promote mental health among adolescents in sub-Saharan Africa. These interventions can be implemented in diverse settings including schools, communities, health facilities, and camps, and can be delivered by lay persons.
Approximately 792 million people live with a mental disorder worldwide with many of these cases emerging during adolescence (1, 2). Mental health problems in adolescents have been on the rise in recent years, and they are linked to significant psychosocial, economic, and physical health burdens for affected adolescents, caregivers, and host communities (1, 3, 4). Across the world, mental health problems including, depressive disorders, anxiety disorders, and suicide, affect 10–20% of children and adolescents and account for 16% of the total burden of disease among adolescents aged 10–19 years (5). In Sub-Saharan Africa (SSA), one out of every seven children and adolescents (14.3%) suffers from major psychological problems, with nearly 10% qualifying for a psychiatric diagnosis (6).
The most recent systematic review of studies from Sub-Saharan African countries encompassing a total population of 97 616 adolescents found the following prevalence estimates; 40.8% for emotional and behavioral problems, 29.8% for anxiety disorders (29.8%), 26.9% for depression, 21.5% for PTSD, and 20.8% for suicidal thoughts (7). The prevalence rates reported from the review are high in comparison with studies from other regions (8–10).
The high burden of adolescent mental health morbidity in SSA is contributed by heightened psychosocial stressors such as exposure to chronic poverty, abuse, exposure to violence, and higher prevalence of certain conditions such as HIV/AIDS in the region (7), coupled with the rapid physical, emotional and social changes that occur during this period (11). The COVID-19 pandemic has also placed additional stress on adolescent mental health (12). The negative impacts of poor mental health in adolescents include poor educational performance, poor physical functioning, and unemployment which greatly reduces their overall quality of life (13).
Despite the high burden of mental health problems in adolescents and the associated negative consequences, the mental health of adolescents remains neglected (14). Furthermore, adolescent mental health services remain scarce, particularly in SSA (15). The high burden of mental health problems, and the scarcity of services, necessitate the need for urgent evidence-based mental health interventions to promote mental health among adolescents.
Therefore, the purpose of this scoping review was to identify interventions that have been implemented to address mental health problems among adolescents in SSA. Specifically, the review also aimed to assess the effectiveness of the identified interventions in reducing adolescent mental health problems. Lastly, the review aimed to evaluate the implementation strategies of the interventions.
This scoping review was guided by the methodological framework proposed by Arksey and O'Malley and further advanced by Levac et al. (16, 17). The framework recommends six stages to be followed in conducting scoping reviews. These stages include (i) identifying the research question (ii) identification of the relevant studies (iii) selecting the studies (iv) charting the data (v) collating, summarizing, and reporting the results, and (vi) consultation. We reported our results based on guidelines by the preferred reporting items for systematic reviews and meta-Analysis (PRISMA) statements (19).
To capture the full range of mental health interventions targeting adolescents in SSA, all peer-reviewed and non-journal articles (gray literature) were included. The eligibility criteria for including studies and documents in this review was that a component of mental health interventions targeting adolescents in SSA must have been reported. There were no limits on the date of publication or language during the search.
We systematically searched the following electronic databases: PubMed, African Index Medicus, PsycINFO, Web of Science, and CINAHL (from database inception to 31 December 2021). Additionally, we searched the following gray literature databases: think tank search, open gray, NGO search engine, and IGO search engine. For this review, the electronic literature search followed the three-step search strategy recommended by the Joanna Briggs Institute (18). The first was a preliminary search in a common online database. The search terms “Mental health”, “Intervention” and “adolescents” were used in PubMed. AM, ET, and EC analyzed the keywords used in the titles and abstracts of the identified articles.
In the second step, relevant keywords in the titles and abstracts of the identified papers were reviewed to compile a list of terms to guide in undertaking a detailed literature search in all the databases. Search terms included Medical Subject Headings (MeSH) and keywords related to mental health, mental disorders, intervention, and adolescents.
Based on preliminary searches, we combined the four search terms (“Mental health”, “Intervention”, “Adolescents”, Sub-Saharan Africa”) with the “AND” Boolean operator. Respective synonyms for these search terms were combined using the “OR” Boolean operator (Table 1). The refined final search strategy was developed in consultation with AA, DS, and an experienced librarian and applied to the databases. This was applied to fit the specifications of each database. Results from the individual database searches were retrieved and uploaded to EPPI-Reviewer (Version 4.12.2.0). Lastly, the reference lists of the selected reports and articles were further explored to identify additional studies meeting the eligibility criteria.
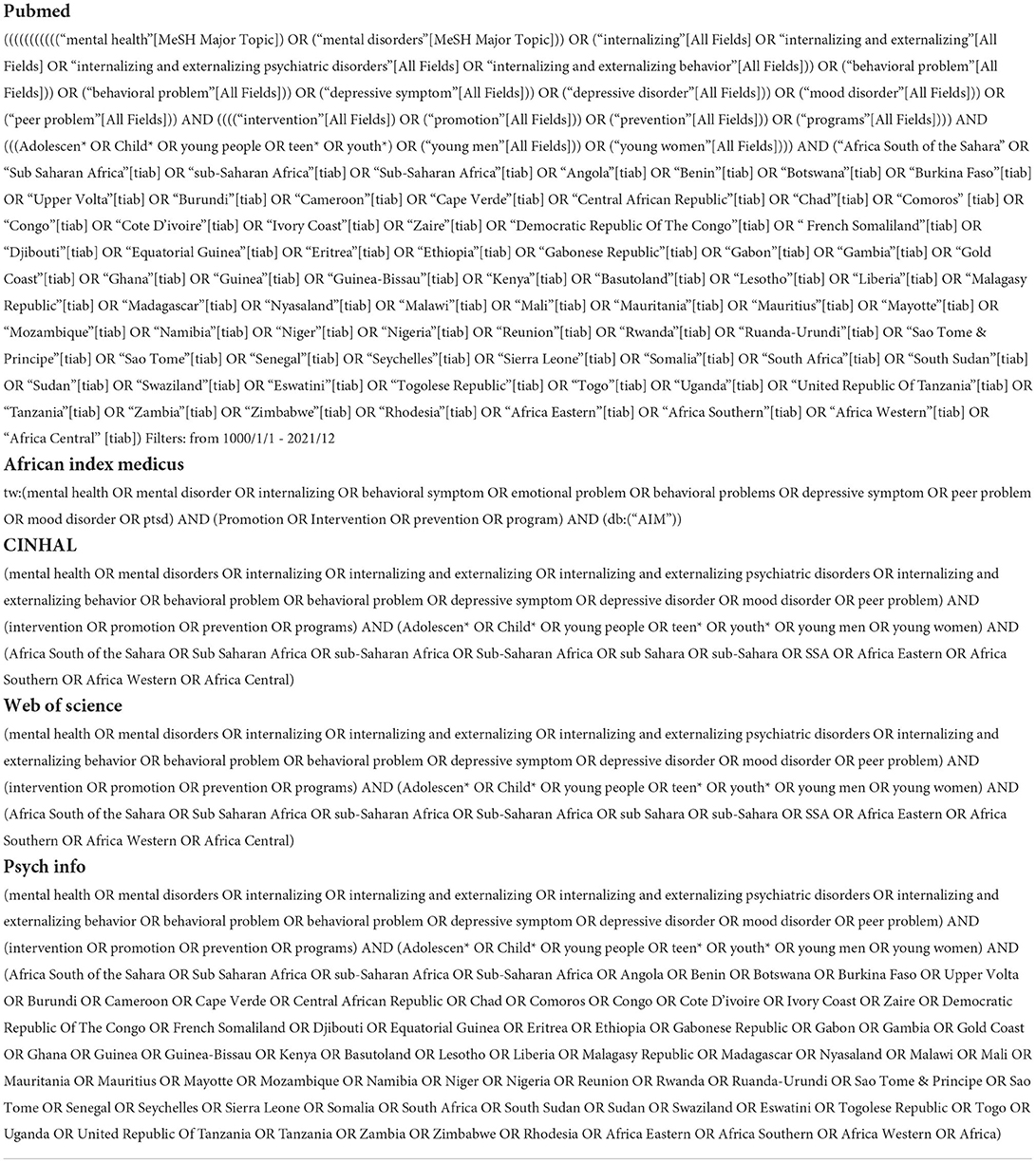
Table 1. List of search terms used.
We used EPPI-Reviewer (Version 4.12.2.0) for managing references of the identified studies and duplicates were automatically removed before commencing the two-stage selection process. Study titles and abstracts were reviewed for eligibility based on the inclusion and exclusion criteria described below. The screening was done independently by two authors (GM & AM) and disagreements were resolved by consensus. The results of the two were reviewed by the team. Full-text articles of selected abstracts were retrieved after which they were also assessed for eligibility by GM and AM.
The full inclusion criteria of the review entailed;
a. Study population: studies were included if the reported age range, and/or mean, and/or median age was between 10–19 years.
b. Outcome measures: studies were included if they reported on an intervention that targeted any mental health problem among adolescents, such as externalizing problems (hyperactivity, attention, aggression, and conduct problems), internalizing problems (anxiety, depression, somatization, and withdrawal) and psychological and social wellbeing problems (emotional, hopelessness, self-esteem, self-concept, feelings of isolation, lack of social support and resilience).
c. Geographic location: conducted in Sub-Saharan Africa.
d. Study design: any type of original empirical intervention research such as quantitative studies, including randomized controlled trials, quasi-experimental designs, pre-post evaluations, open trials, and post evaluations, intervention mapping techniques, and mixed-method studies.
Exclusion criteria included.
a. Study types: secondary literature (scoping reviews, literature reviews, systematic reviews, and meta-analysis), letters to the editor, protocols, and case series.
b. Outcome measures: studies having interventions that did not target any mental health outcome.
The data extraction form was developed by AM and piloted by AM and GM who independently extracted the data from a sample of 10% of the included articles. The results of the two reviewers were also compared and discussed by the research team. Data extraction for the remaining included studies was also independently carried out by AM and GM. Where disagreements arose, the two authors re-assessed the specific article and reached a consensus. Subsequently, we updated our search following the initial submission of our article to the journal, in which GM extracted data for additional articles identified and AA confirmed the accuracy of data extraction. We extracted the following information from the included articles: (i) study and sample characteristics (name of the first author, year of publication, country of study, study design, sample size, population targeted (i.e. general adolescent population or specific sub-populations), and age of participants), (ii) Intervention/program characteristics (name of the intervention, type of intervention, who implemented the intervention, study outcomes, delivery method, setting of delivery (i.e. clinic-based, school-based or community-based), duration of intervention, the impact of the intervention (if evaluated), and challenges faced during the implementation of the intervention.
To create a summary of the included studies, we collated findings relating to our review questions. We grouped and summarized the identified mental health interventions based on the mental health outcomes they targeted, their setting of delivery, and their impact on adolescent mental health. The results were then reported following the PRISMA extension for scoping reviews (PRISMA-ScR) guidelines (19).
Figure 1 is the PRISMA flow diagram detailing the study selection process. The literature search of the electronic databases yielded 4,672 articles. An extra search in the gray literature yielded an additional 78 articles. After the removal of 1,141 duplicate records, 3,410 articles were found to be unlikely to be relevant after being screened by title and abstract and were thus excluded. After a detailed full-text review of the remaining 199 articles, we excluded 135 studies as they did not meet our inclusion with reasons for the exclusion provided in Figure 1. Although we identified non-English studies in our search, none of them met the inclusion criteria. 64 studies describing 57 mental health interventions among adolescents in SSA were included.

Figure 1. Flowchart showing the scoping review process.
The characteristics of the 64 studies and interventions included in this review are shown in Supplementary Table 1. The included studies emanated from 15 countries with more than half (53.1%, n = 34) of these studies from only three countries in SSA (Uganda, Kenya, and South Africa). Figure 2 shows the geographical distribution of the studies. A few studies (3.1%, n = 2) were multi-country studies.
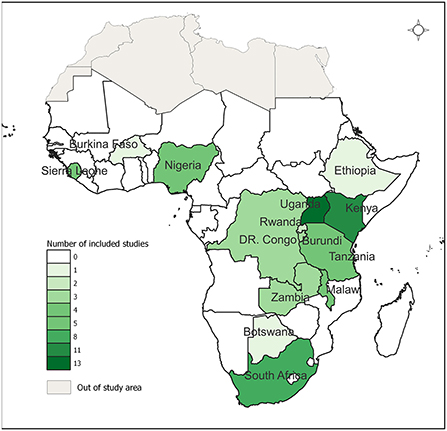
Figure 2. Geographic distribution of the studies included in the scoping review.
All the 64 studies were published between 2007 to 2021 with the majority (93.8%, n = 60) published over the last decade (2011–2021) while over half (51.6%, n = 33) were published in the last 5 years (2017–2021). Only one study was included from the gray literature search (20). In terms of study design, most of the studies (67.2%, n = 43) were randomized controlled trials. Five studies incorporated a mixed-methods approach (20–24) while one study used a qualitative intervention mapping technique (25). The remaining studies were either single-arm trials (15.6%, n = 10) or quasi-experimental trials (7.8%, n = 5).
The 64 eligible studies describe a total of 57 unique adolescent mental health interventions across SSA. Supplementary Table 1 provides the detailed characteristics of these interventions. Three interventions were reported in more than one study; Shamiri “thrive” (26–28), Suubi-Maka “hope for families” (29–32), and Bridges to the future (33–35). The common interventions were cognitive-behavioral therapy (CBT) (n = 20), family-based strengthening and economic empowerment interventions (n = 12), psychoeducation (n = 10, and interpersonal trauma-oriented narrative psychotherapy (n = 9).
The included studies reported a wide range of adolescents' mental health and psychosocial outcomes, with the most frequently reported outcomes being depression (n = 41), anxiety (n = 24), and post-traumatic stress disorder (PTSD) (n = 17) (Supplementary Table 1). Most of the studies (67.2%) focused on more than one mental health outcome. In addition to mental health outcomes, some studies assessed adolescent general health, as well as conduct outcomes such as violence, theft, bullying, and behavioral functioning. Three studies incorporated assessments of outcomes on parental or caregiver mental health and emotional functioning (23, 36, 37). Three studies also included outcomes on parental and adolescent bonding, connectedness and communication (23, 36, 38).
Although diverse tools were used to assess adolescent mental health outcomes, the Child Depression Inventory was the most commonly used measure of adolescent depression symptoms (29, 30, 33, 39–42) while the commonly used measures of PTSD included the University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index (UCLA-PTSD) (41, 43–48) and the Posttraumatic Stress Diagnostic Scale (21, 49–52). The Revised Children's Manifest Anxiety Scale (RCMAS) and the Child and Adolescent Symptom Inventory (CASI) Anxiety Scale were the most frequently used measures of anxiety symptoms among adolescents (36, 42, 53–55).
Five studies assessed how adolescents' knowledge of HIV transmission impacted adolescent mental health (23, 36, 40, 56, 57). A total of fourteen studies included a measure that focused on either of the following adolescent outcomes: unresolved grief, (41, 58, 59) self-esteem, (22, 26, 40, 60) hopelessness, (32–35, 61, 62) self-concept, (23, 32, 33, 35, 63) resilience (58, 60) and self-efficacy among adolescents (22, 37, 40).
There was considerable variation in the duration of the interventions, the number of sessions, and content across the included studies. Overall, the interventions lasted between 1 week to 5 years with a median duration of 3 months (Inter Quartile Range: seven weeks to 12 months). Five of the interventions lasted more than 2 years in which four (33, 34, 42, 64) involved economic strengthening and financial support for families of the adolescents, while one study (45) entailed creative play and psychotherapy (33, 34, 42, 64).
Most interventions were implemented by lay providers while 18 of them (28.0%) were implemented by professional psychologists. The lay providers included individuals without prior psychology training such as teachers, (43, 63, 65) community facilitators (48, 52), and youth ambassadors trained on the intervention component and the implementation process by psychologists who were mostly the lead researchers. Five of the interventions were cash transfer programmes implemented by the government (42, 62, 66–68) while two studies did not report on the providers of the intervention (64, 69). Only one integrated intervention that targeted reducing depression and anxiety was conducted by both lay and professional practitioners in Malawi and Tanzania (70).
The eligible studies recruited a total of 40,072 adolescents from diverse populations and varying sample sizes ranging from 11 to 5,514. Most of the interventions described in the included studies were selective interventions that targeted adolescents at high risk of developing mental health problems including HIV-affected adolescents (n = 16), war-affected adolescents (n = 12), orphans (n = 17), adolescents from a poor background (n = 4), unmarried teenage mothers (n = 2), children of migrants (n = 1) and survivors of sexual violence (n = 4). Ten of the included studies described universal interventions targeting the general population of adolescents (26, 27, 55, 62, 65, 67, 69–72). Only four of the included studies described interventions that targeted adolescents with diagnosed mental and developmental disorders including depression and anxiety, (27, 61), PTSD (73), and autism (53) (Supplementary Table 1).
The majority of the interventions (n = 44) were group interventions and entailed diverse activities implemented in schools and at the community level. They included group CBT, psychoeducation on trauma, economic strengthening, family strengthening programme, and skills acquisition programmes. Only seven of the interventions were exclusively delivered in a one-on-one environment and involved interventions tailored to the specific needs of the individual (Supplementary Table 1). One of the studies reported the use of individual-based trauma-focused narrative exposure therapy provided by local lay counselors in treating PTSD among traumatized former child soldiers in Uganda (50). The study reported that the intervention not only resulted in a significant reduction in PTSD symptoms, but also reduced depressive symptoms, and suicidal ideation among former child soldiers. Other interventions were delivered as a blend of one-on-one support and group activities, (21, 51, 56, 74) and were all associated with a significant reduction in mental health problems.
The identified interventions were implemented in diverse settings including schools, churches, camps, and health facilities, among others. Therefore, we classified the interventions into community-based interventions, school-based interventions, and facility-based interventions. Notably, some interventions were implemented in more than one setting (30, 33, 35, 38, 39, 48, 62, 64, 70, 75).
Most of the identified interventions (n = 44) among the eligible studies were community-based mental health interventions and emanated from 13 countries (Supplementary Table 1). Half (n = 22) of these interventions were implemented in only three of the 13 countries (Kenya, South Africa, and Uganda). Two studies reported on multi-country interventions (49, 70). Seven studies reporting community-based interventions reported on interventions that solely targeted girls (26, 44, 51, 57, 60, 76), while also other seven interventions targeted adolescents who were victims of war (21, 38, 43, 51, 76–79) with one of them aimed at displaced girls who had survived insurgency (76), and one targeted former female child soldiers (51). Nine studies targeted orphans and vulnerable adolescents from poor backgrounds (30, 37, 41, 62), with one of the studies focusing on AIDS orphaned adolescents (30). Overall, four interventions were aimed at improving the mental health of HIV-affected adolescents (30, 32, 40, 80). Ten of the community-based interventions were home-based and involved family meetings involving caregivers, parents, and adolescents. Psychosocial therapies and components drawn from Trauma-focused CBT were identified in fifteen studies as prominent implementation strategies employed by the community interventions.
Other interventions were carried out in camps in Sierra Leonne (81), Botswana (58), and Tanzania (22), with the duration of the intervention ranging from 1 to 4 weeks. Camp-based interventions included the use of Memory Work Therapy, group therapy, art therapy, sports or game activities and music therapy, outdoor challenge, and team-building activities (22, 58, 81).
Schools were the second most common setting in which the interventions were implemented with 19 mental health interventions implemented exclusively in schools (Supplementary Table 1). The interventions targeted diverse groups of adolescents in school settings including all students (26, 65, 82, 83), orphans and vulnerable adolescents (54, 57, 84), and students at increased risk of developing mental health problems such as those living with HIV (29, 36, 63, 85), war-affected adolescents (81, 86), and those diagnosed with mental health disorders (53, 73). The most targeted mental health outcomes by school-based interventions were depressive symptoms, PTSD, and anxiety symptoms (Supplementary Table 1).
Seventeen studies provided information about intervention facilitators for school-based interventions, in which 11 interventions were delivered by trained lay providers (27–29, 35, 48, 52, 54, 57, 63, 65, 83), while six (24, 33, 53, 84, 87) were delivered by professionals (24, 33, 53, 73, 84, 87). Fourteen (24, 27–29, 33, 34, 48, 52–54, 63, 82–84, 87, 88) of the interventions were delivered in groups (24, 28, 29, 33, 48, 52–54, 63, 68, 82) while three (57, 65, 73) were delivered in one on one sessions. The common implementation strategies in school-based interventions were economic-based interventions entailing financial support such as payment of school fees (29, 30, 32–35, 38, 64, 67, 68), and CBT (38, 48, 52, 53, 69, 86).
Health facility/clinic-based interventions were the least common and were reported in three studies conducted in health care facilities in Uganda (39), Tanzania (47), and Nigeria (61). The Suubi + Adherence intervention was a multicomponent intervention that was implemented among adolescents living with HIV in Uganda (39). The intervention included sessions on setting short-term and long-term goals, financial management seminars, income-generating activity training, medical assistance, and psychosocial support. Lay counselors trained in ART counseling provided psychosocial support to patients in HIV clinics.
The Sauti ya Vijana (SYV; The Voice of Youth) intervention was aiming at addressing mental health challenges to improve HIV outcomes among adolescents admitted to two HIV clinics (47). The intervention entailed providing a safe space where participants could share their past experiences.
The Nigerian study assessed the effectiveness of CBT among adolescents with clinically diagnosed depressive disorder attending a specialist psychiatric hospital (61). The group format intervention was administered by a psychiatrist in four weekly sessions using interactive lectures and group discussions. The sessions entailed psychoeducation, promoting hope and medication adherence, and an activity schedule.
Sixty-two studies examined the effectiveness of the interventions, with 55 of them finding a positive significant impact on various mental health outcomes. Firstly, for the community-based interventions, they included a variety of activities targeted at preventing HIV, strengthening family relationships, and reconciliation in addition to supporting mental health among adolescents. Most of the community interventions entailed psychosocial therapies with components derived from Trauma-focused CBT (22, 38, 41, 44, 46, 48, 49, 58, 79, 81, 89). All the studies that reported on CBT intervention reported that CBT significantly reduced mental health problems among adolescents and their family members (Supplementary Table 1) (22, 38, 41, 44, 49, 58, 81). The Family Strengthening Intervention (FSI), for example, significantly improved the mental health outcomes of the entire household and strengthened child-caregiver interactions, family communication, HIV psychoeducation, and resource provision (38). In addition, unconditional cash transfers intervention was associated with improved psychological wellbeing among adolescents (42, 62, 66).
Results of school-based interventions showed that most interventions (17/19) were effective in improving the mental health and wellbeing of students. According to Olowokore et al. (54), the Resilience Training intervention reduced depressive symptoms and improved social connection, and self-esteem among children. However, this intervention did not have any significant effects on anxiety among the adolescents.
The Suubi (Hope) Economic Strengthening Intervention, which was implemented in Uganda and included activities such as counseling and mentorship, the provision of scholastic materials, and matched savings accounts for students, resulted in improved physical health and a decrease in depression and hopelessness (30). In addition, another study conducted in Kenya reported that school support in the form of tuition payments and the provision of scholastic materials such as school uniforms may help to cushion against the onset and exacerbation of mental health problems (64).
In addition to improved mental health outcomes, school-based mental health interventions significantly improved other positive outcomes such as school enrollment, school attendance, and discipline (38, 62, 64, 66). Other reported positive outcomes of the school-based interventions included better emotional regulation, increased prosocial support, reduced functional impairment, and reduced health risk behaviors. However, one school-based intervention had no significant impact on mental health although it improved other aspects of school outcomes such as school attendance (38).
Three healthcare-based studies reported a positive impact of the interventions on improved mental health outcomes among adolescents (39, 47, 61). Post-intervention follow-up and evaluation of the family-based economic intervention indicated that the intervention was effective in enhancing the mental health of adolescents living with HIV (39). The one-week post-intervention evaluation of the Nigerian study also indicated a statistically significant reduction in depressive symptoms and also improvements in the adolescents' knowledge of depression, hope, and attitude toward treatment adherence.
This scoping review aimed to identify and describe interventions that promote mental wellbeing among adolescents in SSA. A total of 64 studies describing 57 interventions were identified. Of the identified interventions, more than half of them (53.1%) were from only three countries in SSA (Uganda, Kenya, and South Africa). This potentially reflects a low coverage and prioritization of mental health interventions across SSA which points to an urgent need for investment in adolescent mental health promotion in the region.
Our review revealed that the existing mental health interventions in SSA targeted a variety of adolescent subpopulations (for example, adolescents living with HIV, adolescents affected by war, and adolescents from low-income families) and were implemented in diverse settings, including schools, communities, and health facilities. This is important as it shows that mental health interventions can be delivered outside conventional healthcare settings. Moreover, it is encouraging to note that most of the interventions were delivered by lay workers. This is particularly important for SSA settings where there is limited mental health infrastructure, including mental health professionals. This noted, the diversity of adolescent sub-populations requiring mental health interventions and services points to a need for evidence-based mental health promotion as well as a need for contextually appropriate tailoring of mental interventions to enhance uptake and effectiveness.
In this review, we observe that CBT is the most frequently utilized mental health promotion intervention, which may be attributable to its effectiveness as a problem-oriented strategy based on the findings from this review and elsewhere (90). First, in all the studies that utilized CBT in this review, significant reductions in mental health problems among adolescents and that of their family members were reported (see Supplementary Table 1). Second, similar findings have been observed in a systematic review on the effectiveness of CBT interventions (91). Some of the common components found in successful CBT interventions are behavioral activation, goal setting, relaxation, affective modulation, cognitive coping, trauma narrative, stress management/relaxation techniques, creating a trauma narrative, and cognitive processing. However, we could not determine which components were the most effective because they were mixed and blended in the interventions.
On the other hand, digital-based interventions were the least utilized interventions. This is despite the availability of evidence on the use and effectiveness of technology in delivering mental health interventions in other settings (92). This might be a reflection of the state of technology in SSA compared to other regions (93). Some interventions involved household economic strengthening through socio-economic empowerment programmes, such as improving access to education, credit schemes, cash transfers, savings schemes, and financial management training. The findings of the study suggest the potential of economic empowerment interventions in decreasing psychological distress among vulnerable adolescent populations.
With regards to community-based interventions in SSA, results from the included studies are promising given the positive impact that was shown by the interventions across a diverse range of mental health outcomes. Most of the community-based interventions reported improvement in mental health outcomes of adolescents following the intervention. Mostly, community-based interventions were aiming at reducing psychosocial issues by fostering parent-child relationships, improved-caregiver relationships, family communication, and parenting skills, connections to resources, and HIV psychoeducation. A key implementation strategy for community-based interventions was the use of community-based organizations and the involvement of local community members, including community health volunteers, chiefs, and religious leaders in the delivery of the intervention. One component that contributes to the success of these treatments is the collective mobilization of resources and sensitization of communities, which enhances responsiveness to adolescent needs and breaks down barriers to obtaining mental health services.
For the family-focused interventions, study implementers, including psychologists and counselors, were able to reach as many vulnerable adolescents as possible in the comfort of their homes, thus reducing barriers, such as transportation, that many poverty-stricken families face when trying to access health facility or center-based mental health interventions. Although the results of family-focused interventions are promising, future research should investigate the sustainability of such interventions.
Camp-based recreational and creative activities such as outdoor challenges, sports, and games had a positive effect not only on mental health outcomes but also on resilience, social-emotional changes, behavioral outcomes, and physical activity among adolescents. It is encouraging to note that all the camp-based interventions reported that the interventions were associated with an increase in resilience and self-esteem.
With regards to the school-based interventions, the findings demonstrate that school-based programs implemented across SSA can have a significant positive impact on adolescent wellbeing, including reduced PTSD, depression, and anxiety, as well as enhanced coping strategies. Most of the school-based interventions were delivered by trained teachers (26, 28, 29, 35, 52, 54, 57, 63, 65), with the remaining interventions implemented by professionals, particularly psychiatrists and psychologists (33, 53, 73, 86). This suggests that trained teachers can effectively deliver mental health promotion interventions. The use of teachers to implement school-based interventions may be a long-term and low-cost strategy for improving mental health outcomes in children since they may continue making use of some of the interventions' components even after the research project is completed.
Another group of interventions targeted adolescents in health care facilities, particularly in HIV clinics and psychiatric hospitals. One of the interventions included psychoeducation and incorporated components of CBT on adolescents with clinically diagnosed depressive disorders under treatment with antidepressants (61). It is difficult to determine the more effective treatment of mental health problems between the use of medication and psychosocial interventions. Studies that combined the two treatment options yielded promising results, implying that combining psychosocial interventions such as psychoeducation and CBT with antidepressant medication is viable, acceptable, and can provide a more positive impact on depressed youths in the region.
This review's main strength was its rigorous and comprehensive nature in which we searched five major databases, including an African-based database, as well as a search of gray literature. Another strength of the review lies in its ability to explore a timely research theme in a geographical context where evidence synthesis on this subject is still limited yet critical for informing interventions.
This review also has limitations worth highlighting. Although most of the studies used randomized study designs, differences in terms of study settings, types of interventions, length of interventions, sample size, and measures made direct comparisons and pooling of effects of the interventions challenging, thus a narrative synthesis was undertaken.
Lastly, another limitation of the current review worth noting is a challenge common to scoping reviews. The quality and the risk of bias of the included studies were not assessed and therefore, the level of certainty on the effectiveness of the interventions is limited. Lastly, the adolescent population is a heterogeneous age group (e.g. early and late adolescence) which may experience the effects of the interventions differently. However, we were unable to disaggregate our findings by the adolescent age sub-categories.
Overall, in regards to informing future research, this scoping review informs mental health programmers of the variety of mental health interventions among which suitable choices can be adapted to settings and developmental stages to optimize effectiveness. The scoping review points to a need for developmentally appropriate interventions considering that the adolescent period includes both early and late adolescence, whose mental health needs and burdens may differ and thus require a targeted approach.
We identified 57 unique adolescent mental health interventions across SSA. These interventions can be administered to diverse sub-populations and can be implemented in a variety of contexts, including schools, communities, camps, and clinical settings. They can also be administered by different providers, including lay workers, which is particularly important for SSA. Most of the interventions were reported to be effective against the targeted mental health outcomes. However, it is difficult to ascertain the strength of this evidence as we did not assess the quality of the included studies.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
AA conceptualized the study. AA, AM, ET, GM, and EC refined the search terms. GM and AM did the database search. GM and AM screened the articles and did the data extraction of included studies, while AA provided guidance throughout the process. The first draft of this article was written by AM, while GM, EC, ET, AS, MN, JA, DS, and AA critically reviewed and contributed to all the subsequent manuscript revisions. All the authors except the late Adam Mabrouk read, reviewed, and approved the final manuscript.
This publication was produced with the financial support of the European Union (Contract No: CSO-LA - 2020 / 418 - 235). Its contents are the sole responsibility of the authors and do not necessarily reflect the views of the European Union. The funders had no role in the study's design, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.937723/full#supplementary-material
1. Twenge JM, Cooper AB, Joiner TE, Duffy ME, Binau SG. Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005–2017. J Abnorm Psychol. (2019) 128:185. doi: 10.1037/abn0000410
2. Saloni D, Ritchie H, Roser M. Mental Health. (20121). Available online at: https://ourworldindata.org/mental-health (accessed June 16, 2022).
3. World Health Organization. Adolescent Mental Health 2020. Available online at: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed November 17, 2020).
4. Trautmann S, Rehm J, Wittchen HU. The economic costs of mental disorders: Do our societies react appropriately to the burden of mental disorders? EMBO Rep. (2016) 17:1245–9. doi: 10.15252/embr.201642951
5. Erskine H, Baxter A, Patton G, Moffitt T, Patel V, Whiteford H, et al. The global coverage of prevalence data for mental disorders in children and adolescents. Epidemiol Psychiatr Sci. (2017) 26:395–402. doi: 10.1017/S2045796015001158
6. Cortina MA, Sodha A, Fazel M, Ramchandani PG. Prevalence of child mental health problems in sub-Saharan Africa: a systematic review. Arch Pediatr Adolesc Med. (2012) 166:276–81. doi: 10.1001/archpediatrics.2011.592
7. Jörns-Presentati A, Napp A-K, Dessauvagie AS, Stein DJ, Jonker D, Breet E, et al. The prevalence of mental health problems in sub-Saharan adolescents: a systematic review. PLoS One. (2021) 16:e0251689. doi: 10.1371/journal.pone.0251689
8. McKinnon B, Gariépy G, Sentenac M, Elgar FJ. Adolescent suicidal behaviours in 32 low-and middle-income countries. Bull World Health Organ. (2016) 94:340. doi: 10.2471/BLT.15.163295
9. Yatham S, Sivathasan S, Yoon R, da Silva TL, Ravindran AV. Depression, anxiety, and post-traumatic stress disorder among youth in low and middle income countries: a review of prevalence and treatment interventions. Asian J Psychiatr. (2018) 38:78–91. doi: 10.1016/j.ajp.2017.10.029
10. Zarafshan H, Mohammadi M-R, Salmanian M. Prevalence of anxiety disorders among children and adolescents in Iran: a systematic review. Iran J Psychiatry. (2015) 10:1.
11. Nyundo A, Manu A, Regan M, Ismail A, Chukwu A, Dessie Y, et al. Factors associated with depressive symptoms and suicidal ideation and behaviours amongst sub-Saharan African adolescents aged 10-19 years: cross-sectional study. Trop Med Int Health. (2020) 25:54–69. doi: 10.1111/tmi.13336
12. Jones EA, Mitra AK, Bhuiyan AR. Impact of COVID-19 on mental health in adolescents: a systematic review. Int J Environ Res Public Health. (2021) 18:2470. doi: 10.3390/ijerph18052470
13. Agnafors S, Barmark M, Sydsjö G. Mental health and academic performance: a study on selection and causation effects from childhood to early adulthood. Soc Psychiatry Psychiatr Epidemiol. (2020) 56:857–66. doi: 10.1007/s00127-020-01934-5
14. Vreeman RC, McCoy BM, Lee S. Mental health challenges among adolescents living with HIV. J Int AIDS Soc. (2017) 20:21497. doi: 10.7448/IAS.20.4.21497
15. Atilola O, Ola B, Abiri G, Sahid-Adebambo M, Odukoya O, Adewuya A, et al. Status of mental-health services for adolescents with psychiatric morbidity in youth correctional institutions in Lagos. J Child Adolesc Ment Health. (2017) 29:63–83. doi: 10.2989/17280583.2017.1321550
16. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
17. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implementation science. (2010) 5:69. doi: 10.1186/1748-5908-5-69
18. Joanna Briggs Institute. (2017). Available online at: https://wiki.joannabriggs.org/display/MANUAL/Chapter+11%3A+Scoping+reviews (accessed June 16, 2022).
19. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
20. Building Resilience and Resistance to Child Early and Forced Marriage through Acquiring Skills (2019).
21. Jordans MJ, Komproe IH, Smallegange E, Ntamatumba P, Tol WA, De Jong JT. Potential treatment mechanisms of counseling for children in Burundi: a series of n=1 studies. Am J Orthopsychiatry. (2012) 82:338–48. doi: 10.1111/j.1939-0025.2012.01171.x
22. Harding R, Wei G, Gwyther L, Miti E. Improving psychological outcomes for orphans living with HIV in Tanzania through a novel intervention to improve resilience: findings from a pilot RCT. AIDS Care. (2019) 31:340–8. doi: 10.1080/09540121.2018.1533630
23. Bhana A, Mellins CA, Petersen I, Alicea S, Myeza N, Holst H, et al. The VUKA family program: Piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care. (2014) 26:1–11. doi: 10.1080/09540121.2013.806770
24. Betancourt TS, Ng LC, Kirk CM, Munyanah M, Mushashi C, Ingabire C, et al. Family-based prevention of mental health problems in children affected by HIV and AIDS: an open trial. AIDS. (2014) 28:S359. doi: 10.1097/QAD.0000000000000336
25. Leerlooijer Joanne N, Kok G, Weyusya J, Bos Arjan ER, Ruiter Robert AC, Rijsdijk Liesbeth E, et al. Applying Intervention Mapping to develop a community-based intervention aimed at improved psychological and social well-being of unmarried teenage mothers in Uganda. Health Educ Res. (2014) 29:598–610. doi: 10.1093/her/cyu020
26. Osborn TL, Rodriguez M, Wasil AR, Venturo-Conerly KE, Gan J, Alemu RG, et al. Single-session digital intervention for adolescent depression, anxiety, and well-being: Outcomes of a randomized controlled trial with Kenyan adolescents. J Consult Clin Psychol. (2020) 88:657–68. doi: 10.1037/ccp0000505
27. Osborn TL, Wasil AR, Venturo-Conerly KE, Schleider JL, Weisz JR. Group intervention for adolescent anxiety and depression: outcomes of a randomized trial with adolescents in Kenya. Behav Ther. (2020) 51:601–15. doi: 10.1016/j.beth.2019.09.005
28. Osborn Tom L, Venturo-Conerly Katherine E, Arango GS, Roe E, Rodriguez M, Alemu Rediet G, et al. Effect of shamiri layperson-provided intervention vs study skills control intervention for depression and anxiety symptoms in adolescents in kenya a randomized clinical trial. JAMA psychiatry. (2021).
29. Han CK, Ssewamala FM, Wang JS. Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: evidence from a randomised evaluation in southwestern Uganda. J Epidemiol Community Health. (2013) 67:225–30. doi: 10.1136/jech-2012-201601
30. Ssewamala Fred M, Neilands Torsten B, Waldfogel J, Ismayilova L. The impact of a comprehensive microfinance intervention on depression levels of AIDS-orphaned children in Uganda. Journal of Adolescent Health. (2012) 50:346–52. doi: 10.1016/j.jadohealth.2011.08.008
31. Cavazos-Rehg P, Byansi W, Doroshenko C, Neilands TB, Anako N, Sensoy Bahar O, et al. Evaluating potential mediators for the impact of a family-based economic intervention (Suubi+Adherence) on the mental health of adolescents living with HIV in Uganda. Soc Sci Med. (2021) 280:113946. doi: 10.1016/j.socscimed.2021.113946
32. Ssewamala Fred M, Karimli L, Torsten N, Wang Julia S-H, Han C-K, Ilic V, et al. Applying a family-level economic strengthening intervention to improve education and health-related outcomes of school-going AIDS-orphaned children: lessons from a randomized experiment in Southern Uganda. Prevention Science. (2016) 17:134–43. doi: 10.1007/s11121-015-0580-9
33. Karimli L, Ssewamala FM, Neilands TB, Wells CR, Bermudez LG. Poverty, economic strengthening, and mental health among AIDS orphaned children in Uganda: Mediation model in a randomized clinical trial. Soc Sci Med. (2019) 228:17–24. doi: 10.1016/j.socscimed.2019.03.003
34. Ssewamala FM, Shu-Huah Wang J, Brathwaite R, Sun S, Mayo-Wilson LJ, Neilands TB, et al. Impact of a family economic intervention (Bridges) on health functioning of adolescents orphaned by HIV/AIDS: a 5-year (2012–2017) cluster randomized controlled trial in Uganda. Am J Public Health. (2021) 111:504–13. doi: 10.2105/AJPH.2020.306044
35. Ssewamala FM, Wang JS-H, Neilands TB, Bermudez LG, Garfinkel I, Waldfogel J, et al. Cost-effectiveness of a savings-led economic empowerment intervention for AIDS-affected adolescents in Uganda: implications for scale-up in low-resource communities. J Adol Health. (2018) 62 (Suppl. 1):S29–36. doi: 10.1016/j.jadohealth.2017.09.026
36. Bell CC, t Gibbons R, McKay MM. Building protective factors to offset sexually risky behaviors among black youths: a randomized control trial. J Natl Med Assoc. (2008) 100:936–44.
37. Thurman TR, Nice J, Luckett B, Visser M. Can family-centered programing mitigate HIV risk factors among orphaned and vulnerable adolescents? Results from a pilot study in South Africa. AIDS care. (2018) 30:1135–43. doi: 10.1080/09540121.2018.1455957
38. Betancourt TS, McBain R, Newnham EA, Akinsulure-Smith AM, Brennan RT, Weisz JR, et al. A behavioral intervention for war-affected youth in Sierra Leone: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. (2014) 53:1288–97. doi: 10.1016/j.jaac.2014.09.011
39. Cavazos-Rehg P, Byansi W, Xu C, Nabunya P, Sensoy B, Borodovsky J, et al. The impact of a family-based economic intervention on the mental Health of HIV-infected adolescents in Uganda: results from Suubi + Adherence. J Adolesc Health. (2021) 68:742–9. doi: 10.1016/j.jadohealth.2020.07.022
40. Mueller J, Alie C, Jonas B, Brown E, Sherr L. A quasi-experimental evaluation of a community-based art therapy intervention exploring the psychosocial health of children affected by HIV in South Africa. Trop Med Int Health. (2011) 16:57–66. doi: 10.1111/j.1365-3156.2010.02682.x
41. O'Donnell K, Dorsey S, Gong W, Ostermann J, Whetten R, Cohen JA, et al. Treating maladaptive grief and posttraumatic stress symptoms in orphaned children in Tanzania: group-based trauma-focused cognitive-behavioral therapy. J Trauma Stress. (2014) 27:664–71. doi: 10.1002/jts.21970
42. Shangani S, Operario D, Genberg B, Kirwa K, Midoun M, Atwoli L, et al. Unconditional government cash transfers in support of orphaned and vulnerable adolescents in western Kenya: is there an association with psychological wellbeing? PLoS ONE. (2017) 12:e0178076. doi: 10.1371/journal.pone.0178076
43. McMullen J, O'Callaghan P, Shannon C, Black A, Eakin J. Group trauma-focused cognitive-behavioural therapy with former child soldiers and other war-affected boys in the DR Congo: a randomised controlled trial. J Child Psychol Psychiatry. (2013) 54:1231–41. doi: 10.1111/jcpp.12094
44. O'Callaghan P, McMullen J, Shannon C, Rafferty H, Black A. A randomized controlled trial of trauma-focused cognitive behavioral therapy for sexually exploited, war-affected Congolese girls. J Am Acad Child Adolesc Psychiatry. (2013) 52:359–69. doi: 10.1016/j.jaac.2013.01.013
45. van Westrhenen N, Fritz E, Vermeer A, Boelen P, Kleber R. Creative arts in psychotherapy for traumatized children in South Africa: an evaluation study. PLoS One. (2019) 14:e0210857. doi: 10.1371/journal.pone.0210857
46. Murray LK, Familiar I, Skavenski S, Jere E, Cohen J, Imasiku M, et al. An evaluation of trauma focused cognitive behavioral therapy for children in Zambia. Child Abuse Negl. (2013) 37:1175–85. doi: 10.1016/j.chiabu.2013.04.017
47. Dow DE, Mmbaga BT, Gallis JA, Turner EL, Gandhi M, Cunningham CK, et al. A group-based mental health intervention for young people living with HIV in Tanzania: results of a pilot individually randomized group treatment trial. BMC Public Health. (2020) 20:1–13. doi: 10.1186/s12889-020-09380-3
48. Murray LK, Skavenski S, Kane JC, Mayeya J, Dorsey S, Cohen JA, et al. Effectiveness of trauma-focused cognitive behavioral therapy among trauma-affected children in Lusaka, Zambia: a randomized clinical trial. JAMA Pediatr. (2015) 169:761–9. doi: 10.1001/jamapediatrics.2015.0580
49. Dorsey S, Lucid L, Martin P, King KM, O'Donnell K, Murray LK, et al. Effectiveness of task-shifted trauma-focused cognitive behavioral therapy for children who experienced parental death and posttraumatic stress in Kenya and Tanzania: a randomized clinical trial. JAMA Psychiatry. (2020) 77:464–73. doi: 10.1001/jamapsychiatry.2019.4475
50. Ertl V, Pfeiffer A, Schauer E, Elbert T, Neuner F. Community-implemented trauma therapy for former child soldiers in Northern Uganda: a randomized controlled trial. Jama. (2011) 306:503–12. doi: 10.1001/jama.2011.1060
51. Robjant K, Koebach A, Schmitt S, Chibashimba A, Carleial S, Elbert T. The treatment of posttraumatic stress symptoms and aggression in female former child soldiers using adapted Narrative Exposure therapy - a RCT in Eastern Democratic Republic of Congo. Behav Res Ther. (2019) 123:103482. doi: 10.1016/j.brat.2019.103482
52. Tol WA, Komproe IH, Jordans MJ, Ndayisaba A, Ntamutumba P, Sipsma H, et al. School-based mental health intervention for children in war-affected Burundi: a cluster randomized trial. BMC Med. (2014) 12:56. doi: 10.1186/1741-7015-12-56
53. Ireri NW, White SW, Mbwayo AW. Treating anxiety and social deficits in children with autism spectrum disorder in two schools in Nairobi, Kenya. J Autism Dev Disord. (2019) 49:3309–15. doi: 10.1007/s10803-019-04045-6
54. Olowokere AE, Okanlawon FA. The effects of a school-based psychosocial intervention on resilience and health outcomes among vulnerable children. J Sch Nurs. (2014) 30:206–15. doi: 10.1177/1059840513501557
55. Puffer ES, Green EP, Sikkema KJ, Broverman SA, Ogwang-Odhiambo RA, Pian J, et al. church-based intervention for families to promote mental health and prevent HIV among adolescents in rural Kenya: results of a randomized trial. J Consult Clin Psychol. (2016) 84:511–25. doi: 10.1037/ccp0000076
56. Jani N, Vu L, Kay L, Habtamu K, Kalibala S. Reducing HIV-related risk and mental health problems through a client-centred psychosocial intervention for vulnerable adolescents in Addis Ababa, Ethiopia. J Int AIDS Soc. (2016) 19 (Suppl. 4):20832. doi: 10.7448/IAS.19.5.20832
57. Thurman TR, Luckett BG, Nice J, Spyrelis A, Taylor TM. Effect of a bereavement support group on female adolescents' psychological health: a randomised controlled trial in South Africa. Lancet Glob Health. (2017) 5:e604–e14. doi: 10.1016/S2214-109X(17)30146-8
58. Katisi M, Jefferies P, Dikolobe O, Moeti O, Brisson J, Ungar M. Fostering resilience in children who have been orphaned: preliminary results from the botswana balekane EARTH program. Child Youth Care Forum. (2019) 48:585–601. doi: 10.1007/s10566-019-09497-6
59. Thurman Tonya R, Nice J, Taylor Tory M, Luckett B. Mitigating depression among orphaned and vulnerable adolescents: a randomized controlled trial of interpersonal psychotherapy for groups in South Africa. Child Adolesc Ment Health. (2017) 22:224–31. doi: 10.1111/camh.12241
60. Kachingwe M, Chikowe I, van der Haar L, Dzabala N. Assessing the impact of an intervention project by the young women's christian association of Malawi on psychosocial well-being of adolescent mothers and their children in Malawi. Front Public Health. (2021) 9:585517. doi: 10.3389/fpubh.2021.585517
61. Isa EW, Ani C, Bella-Awusah T, Omigbodun O. Effects of psycho-education plus basic cognitive behavioural therapy strategies on medication-treated adolescents with depressive disorder in Nigeria. J Child Adolesc Ment Health. (2018) 30:11–8. doi: 10.2989/17280583.2018.1424634
62. Kilburn K, Thirumurthy H, Halpern CT, Pettifor A, Handa S. Effects of a large-scale unconditional cash transfer program on mental health outcomes of young people in Kenya. J Adolesc Health. (2016) 58:223–9. doi: 10.1016/j.jadohealth.2015.09.023
63. Kumakech E, Cantor-Graae E, Maling S, Bajunirwe F. Peer-group support intervention improves the psychosocial well-being of AIDS orphans: cluster randomized trial. Soc Sci Med. (2009) 68:1038–43. doi: 10.1016/j.socscimed.2008.10.033
64. Green EP, Cho H, Gallis J, Puffer ES. The impact of school support on depression among adolescent orphans: a cluster-randomized trial in Kenya. J Child Psychol Psychiatry. (2019) 60:54–62. doi: 10.1111/jcpp.12955
65. Musuva R, Shen Y, Wei X, Binder S, Ivy JA, Secor WE, et al. Change in children's school behavior after mass administration of praziquantel for Schistosoma mansoni infection in endemic areas of western Kenya: a pilot study using the Behavioral Assessment System for Children (BASC-2). PLoS ONE. (2017) 12:e0181975. doi: 10.1371/journal.pone.0181975
66. Angeles G, de Hoop J, Handa S, Kilburn K, Milazzo A, Peterman A. Government of Malawi's unconditional cash transfer improves youth mental health. Soc Sci Med. (2019) 225:108–19. doi: 10.1016/j.socscimed.2019.01.037
67. Baird S, De Hoop J, Özler B. Income shocks and adolescent mental health. J Human Res. (2013) 48:370–403. doi: 10.3368/jhr.48.2.370
68. Kilburn K, Hughes JP, MacPhail C, Wagner RG, Gómez-Olivé FX, Kahn K, et al. Cash transfers, young women's economic well-being, and HIV risk: evidence from HPTN 068. AIDS Behav. (2019) 23:1178–94. doi: 10.1007/s10461-018-2329-5
69. Ugwuanyi CS, Ede MO, Onyishi CN, Ossai OV, Nwokenna EN, Obikwelu LC, et al. Effect of cognitive-behavioral therapy with music therapy in reducing physics test anxiety among students as measured by generalized test anxiety scale. Medicine. (2020) 99:e16406. doi: 10.1097/MD.0000000000016406
70. Kutcher S, Perkins K, Gilberds H, Udedi M, Ubuguyu O, Njau T, et al. Creating evidence-based youth mental health policy in sub-saharan africa: a description of the integrated approach to addressing the issue of youth depression in Malawi and Tanzania. Front Psychiatry. (2019) 10:542. doi: 10.3389/fpsyt.2019.00542
71. Dorsey S, Lucid L, Murray L, Bolton P, Itemba D, Manongi R, et al. A qualitative study of mental health problems among orphaned children and adolescents in Tanzania. J Nerv Ment Dis. (2015) 203:864–70. doi: 10.1097/NMD.0000000000000388
72. Richards J, Foster C, Townsend N, Bauman A. Physical fitness and mental health impact of a sport-for-development intervention in a post-conflict setting: randomised controlled trial nested within an observational study of adolescents in Gulu, Uganda. BMC Public Health. (2014) 14:619. doi: 10.1186/1471-2458-14-619
73. Rossouw J, Yadin E, Alexander D, Seedat S. Prolonged exposure therapy and supportive counselling for post-traumatic stress disorder in adolescents: task-shifting randomised controlled trial. Br J Psychiatry. (2018) 213:587–94. doi: 10.1192/bjp.2018.130
74. Ismayilova L, Karimli L, Sanson J, Gaveras E, Nanema R, Tô-Camier A, et al. Improving mental health among ultra-poor children: two-year outcomes of a cluster-randomized trial in Burkina Faso. Soc Sci Med. (2018) 208:180–9. doi: 10.1016/j.socscimed.2018.04.022
75. Amone-P'olak K, Garnefski N, Kraaij V. Adolescents caught between fires: cognitive emotion regulation in response to war experiences in Northern Uganda. J Adolesc. (2007) 30:655–69. doi: 10.1016/j.adolescence.2006.05.004
76. Walker JA. Building Resilience and Resistance to Child, Early, Forced Marriage through Acquiring Skills Findings from Implementation Research in Nigeria. (2019). Available online at: https://www.brookings.edu/wp-content/uploads/2019/08/Findings-from-Implementation-Research-in-Nigeria-FINAL.pdf
77. Bolton P, Bass J, Betancourt T, Speelman L, Onyango G, Clougherty KF, et al. Interventions for depression symptoms among adolescent survivors of war and displacement in northern Uganda: a randomized controlled trial. Jama. (2007) 298:519–27. doi: 10.1001/jama.298.5.519
78. Newnham EA, McBain RK, Hann K, Akinsulure-Smith AM, Weisz J, Lilienthal GM, et al. The youth readiness intervention for war-affected youth. J Adolesc Health. (2015) 56:606–11. doi: 10.1016/j.jadohealth.2015.01.020
79. Fine SL, Malik A, Guimond M-F, Nemiro A, Temu G, Likindikoki S, et al. Improving mental health in low-resource settings: A feasibility randomized controlled trial of a transdiagnostic psychological intervention among Burundian refugee adolescents and their caregivers. Behav Res Ther. (2021) 145:103944. doi: 10.1016/j.brat.2021.103944
80. Chory A, Callen G, Nyandiko W, Njoroge T, Ashimosi C, Aluoch J, et al. A pilot study of a mobile intervention to support mental health and adherence among adolescents living with HIV in Western Kenya. AIDS Behav. (2022) 26:232–42. doi: 10.1007/s10461-021-03376-9
81. Gupta L, Zimmer C. Psychosocial intervention for war-affected children in Sierra Leone. Br J Psychiatry. (2008) 192:212–6. doi: 10.1192/bjp.bp.107.038182
82. Osborn Tom L, Venturo-Conerly Katherine E, Wasil Akash R, Rodriguez M, Roe E, Alemu R, et al. The Shamiri group intervention for adolescent anxiety and depression: study protocol for a randomized controlled trial of a lay-provider-delivered, school-based intervention in Kenya. Trials. (2020) 21:938. doi: 10.1186/s13063-020-04732-1
83. McMullen JD, McMullen N. Evaluation of a teacher-led, life-skills intervention for secondary school students in Uganda. Soc Sci Med. (2018) 217:10–7. doi: 10.1016/j.socscimed.2018.09.041
84. Mutiso V, Tele A, Gitonga I, Musau A, Musyimi C, Ndetei D. Effectiveness of life skills education and psychoeducation on emotional and behavioral problems among adolescents in institutional care in Kenya: a longitudinal study. Child Adolesc Ment Health. (2018) 23:351–8. doi: 10.1111/camh.12232
85. Ssewamala FM, Sensoy Bahar O, Nakasujja N, Abente B, Nabunya P, Peer L, et al. Child mental health in HIV-impacted low-resource settings in developing countries-global research fellowship: a research training program protocol. Front Public Health. (2021) 9:632800. doi: 10.3389/fpubh.2021.632800
86. McBain RK, Salhi C, Hann K, Kellie J, Kamara A, Salomon JA, et al. Improving outcomes for caregivers through treatment of young people affected by war: a randomized controlled trial in Sierra Leone. Bull World Health Organ. (2015) 93:834–41. doi: 10.2471/BLT.14.139105
87. McBain Ryan K, Salhi C, Hann K, Salomon Joshua A, Kim Jane J, Betancourt Theresa S. Costs and cost-effectiveness of a mental health intervention for war-affected young persons: decision analysis based on a randomized controlled trial. Health Policy Plan. (2016) 31:415–24. doi: 10.1093/heapol/czv078
88. Bella-Awusah T, Adedokun B, Dogra N, Omigbodun O. The impact of a mental health teaching programme on rural and urban secondary school students' perceptions of mental illness in southwest Nigeria. J Child Adolesc Ment Health. (2014) 26:207–15. doi: 10.2989/17280583.2014.922090
89. Kane JC, Murray LK, Cohen J, Dorsey S, Skavenski van Wyk S, Galloway H, et al. Moderators of treatment response to trauma-focused cognitive behavioral therapy among youth in Zambia. J Child Psychol Psychiatry. (2016) 57:1194–202. doi: 10.1111/jcpp.12623‘
90. Coull G, Morris PG. The clinical effectiveness of CBT-based guided self-help interventions for anxiety and depressive disorders: a systematic review. Psychol Med. (2011) 41:2239–52. doi: 10.1017/S0033291711000900
91. Oud M, De Winter L, Vermeulen-Smit E, Bodden D, Nauta M, Stone L, et al. Effectiveness of CBT for children and adolescents with depression: a systematic review and meta-regression analysis. Eur Psychiatry. (2019) 57:33–45. doi: 10.1016/j.eurpsy.2018.12.008
92. Farrer L, Gulliver A, Chan JK, Batterham PJ, Reynolds J, Calear A, et al. Technology-based interventions for mental health in tertiary students: systematic review. J Med Internet Res. (2013) 15:e2639. doi: 10.2196/jmir.2639
Keywords: mental health, intervention, adolescents, scoping review, sub-Saharan Africa
Citation: Mabrouk A, Mbithi G, Chongwo E, Too E, Sarki A, Namuguzi M, Atukwatse J, Ssewanyana D and Abubakar A (2022) Mental health interventions for adolescents in sub-Saharan Africa: A scoping review. Front. Psychiatry 13:937723. doi: 10.3389/fpsyt.2022.937723
Received: 06 May 2022; Accepted: 11 July 2022;
Published: 11 August 2022.
Edited by:
Theresa (Terry) Fleming, Victoria University of Wellington, New ZealandReviewed by:
Sonia Lewycka, Oxford University Clinical Research Unit in Vietnam (OUCRU), VietnamCopyright © 2022 Mabrouk, Mbithi, Chongwo, Too, Sarki, Namuguzi, Atukwatse, Ssewanyana and Abubakar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amina Abubakar, YW1pbmEuYWJ1YmFrYXJAYWt1LmVkdQ==; Gideon Mbithi, Z2lkZW9uLm1iaXRoaUBha3UuZWR1
†Passed away on 4th March 2022 after he had conducted the review and written the first draft of the manuscript
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.