 Lenka Vargová1*
Lenka Vargová1* Gabriela Mikulášková1,2
Gabriela Mikulášková1,2 Denisa Fedáková3
Denisa Fedáková3 Martin Lačný4
Martin Lačný4 Jaroslava Babjáková1
Jaroslava Babjáková1 Martina Šlosáriková1
Martina Šlosáriková1 Peter Babinčák1Ivan Ropovik5,6
Peter Babinčák1Ivan Ropovik5,6 Matúš Adamkovič1,3,6
Matúš Adamkovič1,3,6- 1Institute of Psychology, Faculty of Arts, University of Presov, Prešov, Slovakia
- 2Instytut Psychologii, Wyższa Szkoła Humanitas, Humanitas University, Sosnowiec, Poland
- 3Institute of Social Sciences of the Centre of Social and Psychological Sciences, Slovak Academy of Sciences, Bratislava, Slovakia
- 4Faculty of Arts, Institute of Political Science, University of Presov, Prešov, Slovakia
- 5Department of Preschool and Elementary Education and Psychology, Faculty of Education, University of Presov, Prešov, Slovakia
- 6Faculty of Education, Institute for Research and Development of Education, Charles University, Prague, Czechia
The changes in people’s mental health have become one of the hot topics during the COVID-19 pandemic. Parents have been said to be among the most vulnerable groups in terms of the imposed anti-pandemic measures. The present paper analyzes the trends in mental health indicators in a sample of Slovak parents (N = 363) who participated in four waves of data collection over a year and a half of the COVID-19 pandemic. The mental health indicators were represented by general levels of depression and anxiety as well as COVID-related stress and anxiety. While there were only minor changes in depression and anxiety, the dynamic in COVID-related stress and especially anxiety was more noteworthy. Besides some exceptions, the results hold even after controlling for the socioeconomic situation. The gender differences in the mental health trends were found to be negligible. Overall, we observed no substantial deterioration in the mental health indicators across the four waves of the study.
Introduction
Since the beginning of the COVID-19 pandemic, its impact on mental health has been studied intensively [e.g., (1, 2)]. There have been worldwide measures put in place to curb the spread of coronavirus. However, these have disrupted the work and family-life routines of individuals. Social isolation, closure of educational institutions, financial insecurity, and changes in health and social care have impaired the lives of families, especially those with children (3). In particular, parents have been exposed to more stressful situations which have concerned them as well as their children (4). Parents have also experienced difficulties in taking care of homeschooled children during online teaching in addition to keeping down their job. This has made them vulnerable to financial insecurity, income decrease or job loss (5). Thus, the negative impact of COVID-19 appears to have been much more significant for parents compared to non-parents (6).
The objective economic situation of many families has worsened significantly as a result of the pandemic. There has been a global increase in unemployment (7); note that jobs most-at-risk are concentrated in lagging regions, (8) in addition to no-pay leave, reduced working hours (9), liquidity constraints, income shocks and the related decrease in consumption (10). The economic slowdown has exacerbated the pre-existing health and socio-economic inequalities as the pandemic has progressed (11). In Slovakia, the unemployment rate peaked in April 2021 at 8.8% (12). In spite efforts to provide economic aid, particularly for parents with children (13), there was notably low satisfaction with the pandemic support in Slovakia and Slovaks also reported serious household difficulties making ends meet and the fear of future financial worsening (14).
Various studies have confirmed an association between both objective and subjective economic status and mental health issues [e.g., (15–19)]. Therefore, it is likely that the economic changes during the course of the pandemic have affected mental health, especially among parents. Higher levels of depression, anxiety, stress, parental burnout, and worsened family relationships have been mainly observed in parents who have suffered socio-economic hardship, low-income families and families that have experienced multiple hardships or economic losses (20–25). In addition, the deterioration of mental health has been more notable in mothers as their work-life balance has been particularly affected by the anti-pandemic measures (26–28).
Parents’ struggles, such as an increased reliance on negative coping strategies (29) or mental health worsening (30), tend to get reflected in children’s at-home education, their well-being, emotional regulation or, in severe cases, maltreatment (31–34). While it is undeniable that the pandemic has caused tremendous socio-economic changes and disrupted the functioning of many families, general evidence of how families adapt in the long term is still lacking (21). There has only been one study published (35) concerning the mental health of Slovak parents. However, the study deals with a specific context and sample (i.e., parents of children with autistic spectrum disorder, predominantly mothers). Furthermore, only a few studies have dealt with specific COVID-related measures of mental health. In some of these studies, single items concerning worry, fear, stress, or COVID-related stressors have been used (36, 37). In other studies, COVID-related mental health scales have been used [e.g., COVID-related stress or anxiety; (38–41)]. However, to the best of our knowledge, there is a lack of studies that target the dynamic of COVID-related mental health constructs in a sample of parents.
In order to address these gaps, complex and especially longitudinal evidence is needed. In contrast to cross-sectional data, a longitudinal design means it is possible to study the dynamics of mental health indicators and subsequently help to understand the rate of change. The present study thus aims to analyze the changes in Slovak parents’ mental health over a year and a half of the COVID-19 pandemic, while also accounting for the effect of the objective, as well as subjective, economic situation. In particular, we will examine the trends will be examined in four mental health indicators out of which two are general (depression and anxiety), and the other two are COVID-related (COVID-related anxiety and COVID-related stress). The study focuses on a sample of parents from a representative sample of the Slovak population across four time points. The study also examines differences between mothers and fathers in these trends.
Materials and methods
Data collection and participants
A longitudinal design with four waves of online data collection (October 2020, December 2020, December 2021, and March 2022) was implemented. The first three waves were intentionally carried out during a period of lockdown or very strict measures. The fourth wave took place during a period of eased (almost non-existent) restrictive measures.
Before the first wave of data collection, the total number of positive cases in Slovakia since the beginning of the pandemic was approximately 10,000. By October 2020, when the first wave of data collection was carried out, the number of new daily cases had grown rapidly, and at the end of October, the total number of positive cases was almost 60,000. In December 2020, during the second wave of data collection, this number exceeded 150,000 (growing rapidly – at the end of December, it exceeded 180,000). In November and December 2021, after a relatively stable period, another increase of new positive cases emerged. During the third wave of data collection (December 2021) the total number of positive cases in Slovakia since the beginning of the pandemic had reached 840,000 (end of December). Up to March 2022, when the fourth data collection was carried out, this number had continued to grow rapidly. At the end of March, the total number of positive cases crossed 1,700,000. After that, the situation stabilized (42, 43). The vaccination rate in Slovakia was low at the time of the third and the fourth wave of data collection, and remains low even today. Vaccination against COVID-19 in Slovakia started at the end of 2020 (December 26), with priority given to at-risk groups. Vaccination for all people aged 16 + was launched in May 2021. By the end of the summer, approximately 40% of the population had been fully vaccinated and by the end of 2021, the vaccination rate had reached almost 50%. In early 2022, vaccination almost stopped due to lack of interest and now, in the summer of 2022, the vaccination rate is approximately 51% (42); Ministry of Health of the Slovak Republic). For more details about the pandemic situation in Slovakia please see this overview https://osf.io/vjmfd/.
The current sample (N = 363) is a subset of a representative sample (based on quota characteristics for gender, age, education, and region) of Slovak inhabitants and consists of parents who, at the time of the third wave, had (or were taking care of) at least one child younger than 18 years. The participants took part in all four waves of data collection. About 52% of the participants were women and the mean age of the sample at T1 was 45.4 years (SD = 10.8). For more details on the demographic characteristics see Table 1.
Table 1. Demographic characteristics of the participants.
Measures
The participants were asked about demographics, economic situation (personal and household income, number of household members).
The subjective socioeconomic status (SES) was measured using a visual ladder (MacArthur scale of subjective social status (44). The instruction describes that on the top of the ladder are people with the highest socioeconomic status whereas the bottom of the ladder represents those with the lowest socioeconomic status. The participants indicate where they would place themselves on the ladder using a 10-point scale (from 1 = the lowest socioeconomic status to 10 = the highest socioeconomic status).
Income was assessed as an equivalized total net household income per month. The equivalization was done using a slightly modified OECD formula (45). This assigns a coefficient of 1 to one adult member of the family, 0.5 to all other adult members, and 0.3 to all children living in the household (U18).
Depression was measured using a QIDS-16-SR (46) questionnaire. The items cover 9 depression symptoms according to the DSM-5 (e.g., depressed mood, loss of interest or pleasure, etc.). For each item, the participants expressed the degree of symptom severity during the last 2 weeks (from 1 to 4).
Anxiety was measured using the Generalized Anxiety Disorder Screener-7 [GAD-7; (47)] which assesses the severity of generalized anxiety disorder symptoms (e.g., feeling nervous, anxious or on edge). The participants evaluated how often they had been bothered by individual symptoms (from 1 = not at all to 4 = nearly every day) during the last 2 weeks.
Covid-related anxiety was measured using the Covid-related anxiety stress scale [items from PAS; (48)], and consecutively modified according to (49). The items are formulated as statements measuring anxiety related to COVID-19 (e.g., worries about catching COVID-19.) The participants answered on a 5-point Likert scale (from 1 = not at all to 5 = completely).
Covid-related stress was measured using the Covid-related stress scale [adapted from the COVIDiSTRESS survey; (50)]. The items are formulated as statements assessing the presence of concerns and difficulties in various areas possibly affected by the COVID-19 pandemic (e.g., concerns about the socio-economic situation, daily functioning, etc.). The participants answered on a 7-point Likert scale (1 = no concerns at all; 7 = great concerns).
Statistical analysis
Given the longitudinal nature of the data, the four waves of data collection were combined and the respondents who participated in all of them were matched. Out of the general population, participants who indicated they have (or take care of) at least one child under 18 years of age were selected. This item was available in the third wave of data collection. The data were screened for improbable values and careless participants as part of general data wrangling for the purposes of the research project APVV-20-0319 “Behavioural aspects of COVID-19: Mapping the COVID-related behaviours, and psychological, social, and economic consequences of the pandemic”). The reliabilities of the scales were checked using the omega total coefficient. The estimated omega total coefficients ranged from 0.84 to 0.96. We proceeded with calculations of a sum score for each of the mental health constructs at each timepoint and divided it by the number of items forming the construct. For descriptive purposes, descriptive statistics were also calculated, and the correlation matrix examined. To examine the sensitivity of our design to a range of hypothetical effect sizes, we carried out a power analysis and found that, given the sample size of N = 363, alpha level of 0.05, and the usage of two-sided test, our design had 48% power to detect an effect of r = 0.10, 97% power to detect an effect of r = 0.2, and almost 100% power to detect correlations larger than 0.3. For the mental health indicators, as well as for the socioeconomic indicators, a trend line was visualized for each participant and an average trend line was plotted (without any smoothing). In order to answer the research question (i.e., how the indicators of parents’ mental health changed over the four time points), three unconstrained linear growth models were run for each mental health indicator. The first of the three models did not include any of the covariates. In terms of accounting for one’s socio-economic situation, a time-varying covariate represented by one’s subjective perception of SES and the objective economic situation was included in the second and the third model, respectively. From each estimated model, the latent intercept, latent slope, their variances and intercept-slope covariance, including the SEs and p-values of these parameters were extracted. The models were estimated using the MLR estimator (Maximum Likelihood with Robust standard errors) and the missing data were imputed using FIML (Full Information Maximum Likelihood). The analysis was performed in R, using the lavaan package, version 0.6-8 (51).
Results
The descriptive statistics of the scales are available in Table 2. The correlation matrix with the diagonal representing the reliabilities of the scales is available in Figure 1. There are two things worth noting. Firstly, it is possible to see medium-to-high positive correlations between the mental health indicators. This indicates high comorbidity between the mental health issues and their (usually high) within-person stability in time. Secondly, there is a clear pattern of almost universally negative correlations between the socio-economic situation and mental health variables. The visualizations of the trend lines of mental health indicators, as well as participants’ socio-economic situation, are presented in Figure 2.
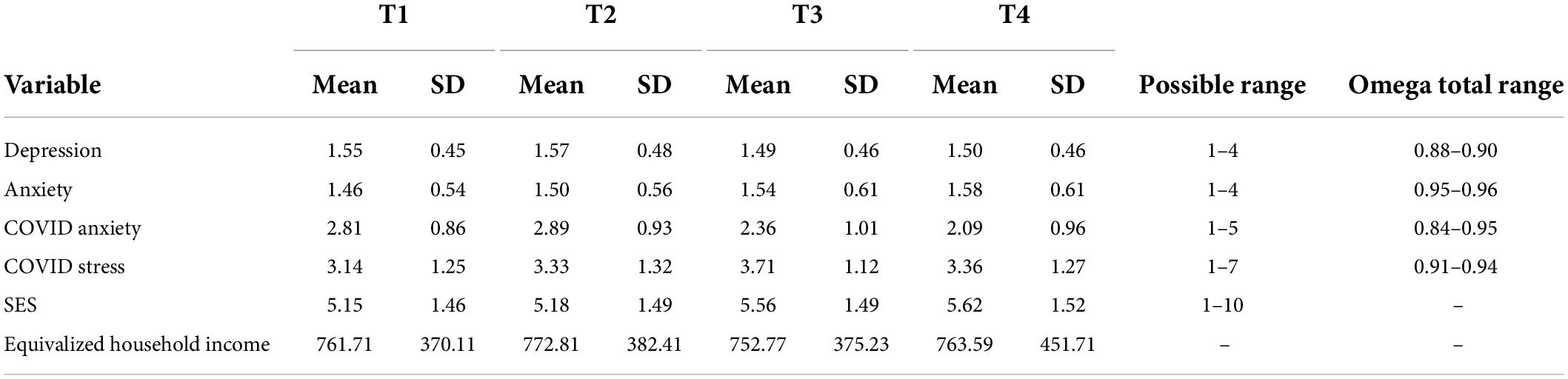
Table 2. Descriptive statistics and reliabilities.
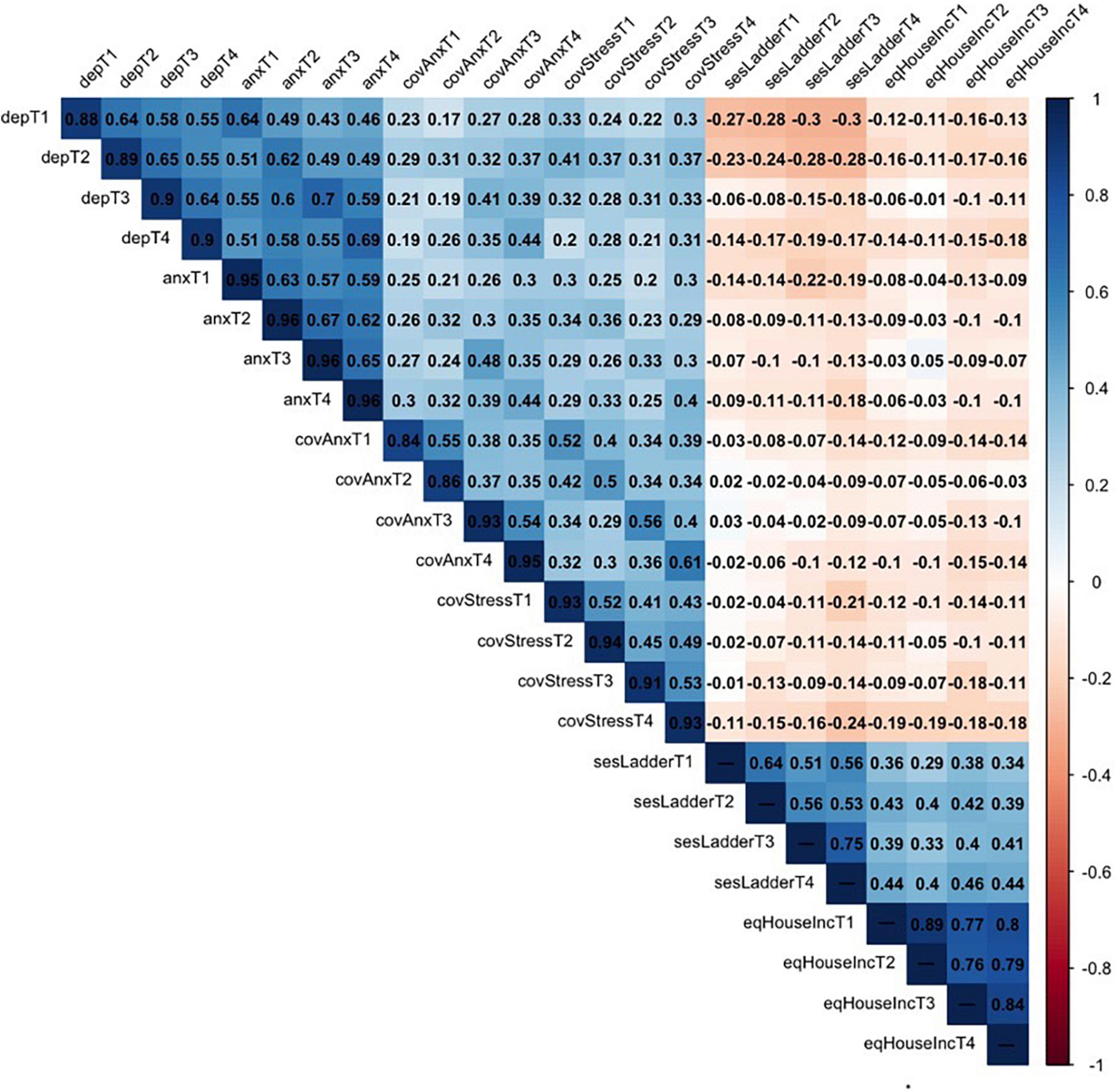
Figure 1. Correlation matrix and reliabilities. The reliablilities of the scales are presented on the diagonal.
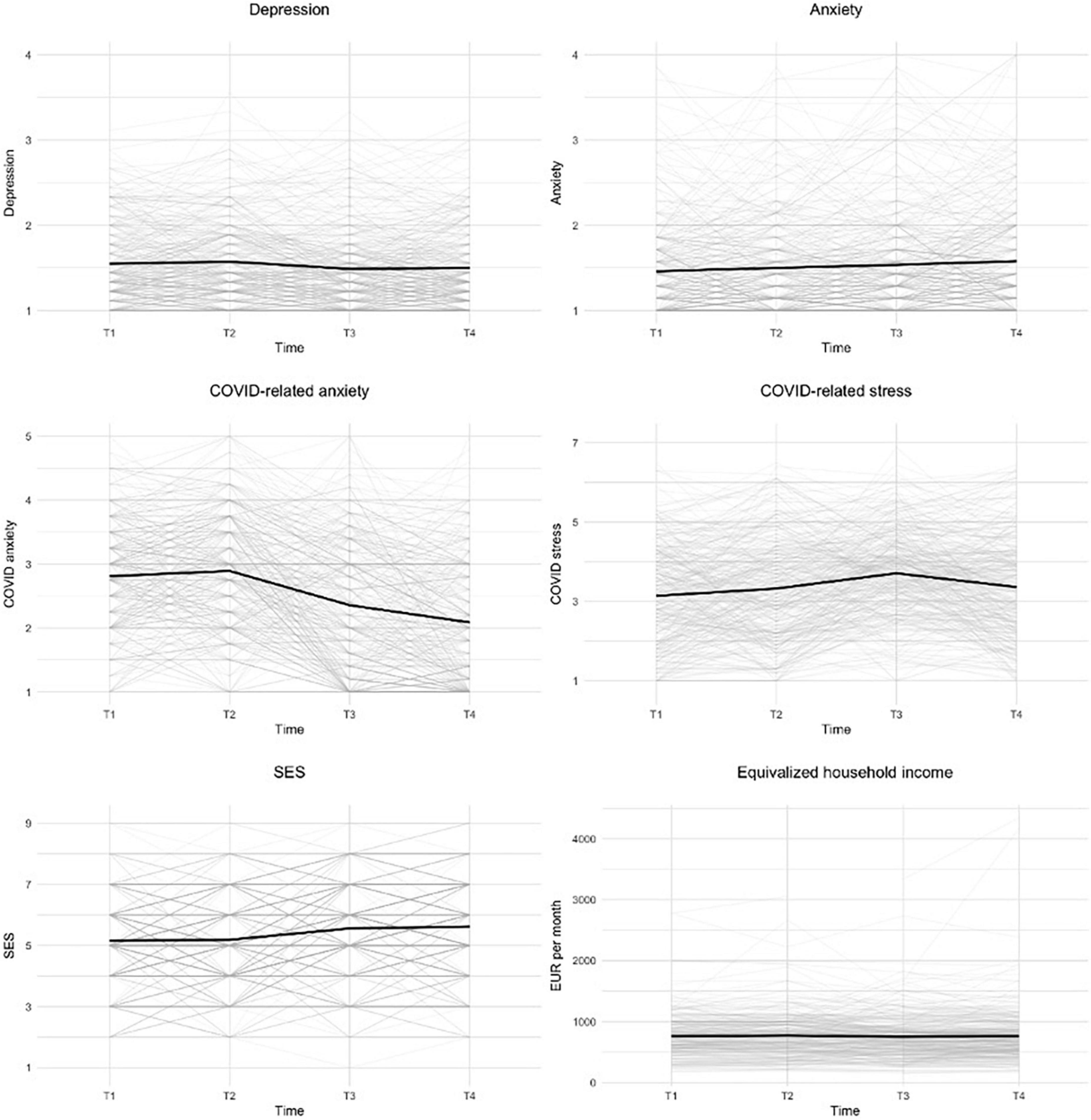
Figure 2. Visualization of the dynamic of mental health indicators and economic situation. Trend lines for each participant and average trend lines are plotted.
In order to answer our research question (i.e., how the indicators of parents’ mental health changed over the four time points), three linear growth models were run for each mental health indicator.
The results of the linear growth models suggest the following patterns. There was a very small decrease observed in the level of depression (slope = −0.02, p = 0.006). This became more visible when controlling for SES (slope = −0.13, p < 0.001). On the other hand, a very small increase in anxiety was observed across the four time points (slope = 0.04, p < 0.001). This increase was more pronounced when the model controlled for income (slope = 0.11, p = 0.011). There was a substantial decrease in COVID-related anxiety observed in the model without any covariates (slope = −0.25, p < 0.001) as well as for the model that controlled for SES (slope = −0.23, p = 0.008). The decrease was slower for parents with a high initial level of COVID-anxiety (I-S covariances ranged from −0.08 to −0.09, ps < 0.001). Conversely, a notable increase was observed in COVID-related stress (slope = 0.11, p < 0.001). This was further amplified when a covariate was added into the model (slopes = 0.31 and 0.37; ps = 0.001 and.135; note the high SEs when income was controlled for in these models). For more detailed results, see Table 3.
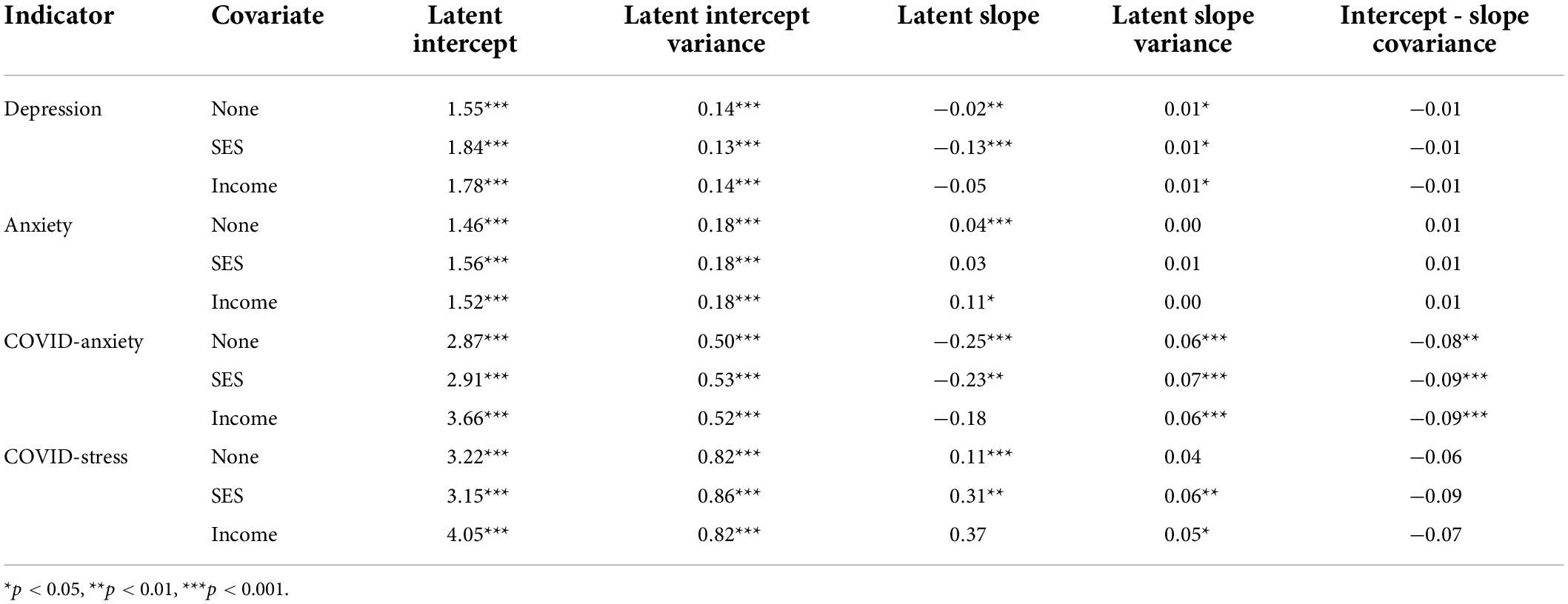
Table 3. Results of the linear growth models.
As an additional goal of the study, we examined the trends in the mental health outcomes separately for mothers and fathers. It was found that although mothers tend to score higher in most of the measures (models without a covariate), the group differences in changes in the mental health indicators over the course of the study were negligible. After accounting for SES, notable exceptions in this pattern occurred. In particular, depression in mothers decreased more sharply (slope difference = −0.10), anxiety decreased (slope difference -0.13), while the increase in COVID-related stress was less steep compared to fathers (slope difference = −0.11). After controlling for one’s household income, mothers got lower scores in depression (intercept difference = −0.17) and anxiety (intercept difference = 0.52) compared to fathers. Fathers’ scores for COVID-related anxiety (slope difference = 0.38) and COVID-related stress (slope difference = 0.69) rose compared to mothers. The observed increase was very steep, especially in the case of COVID-related stress. More detailed results are available in Table 4.
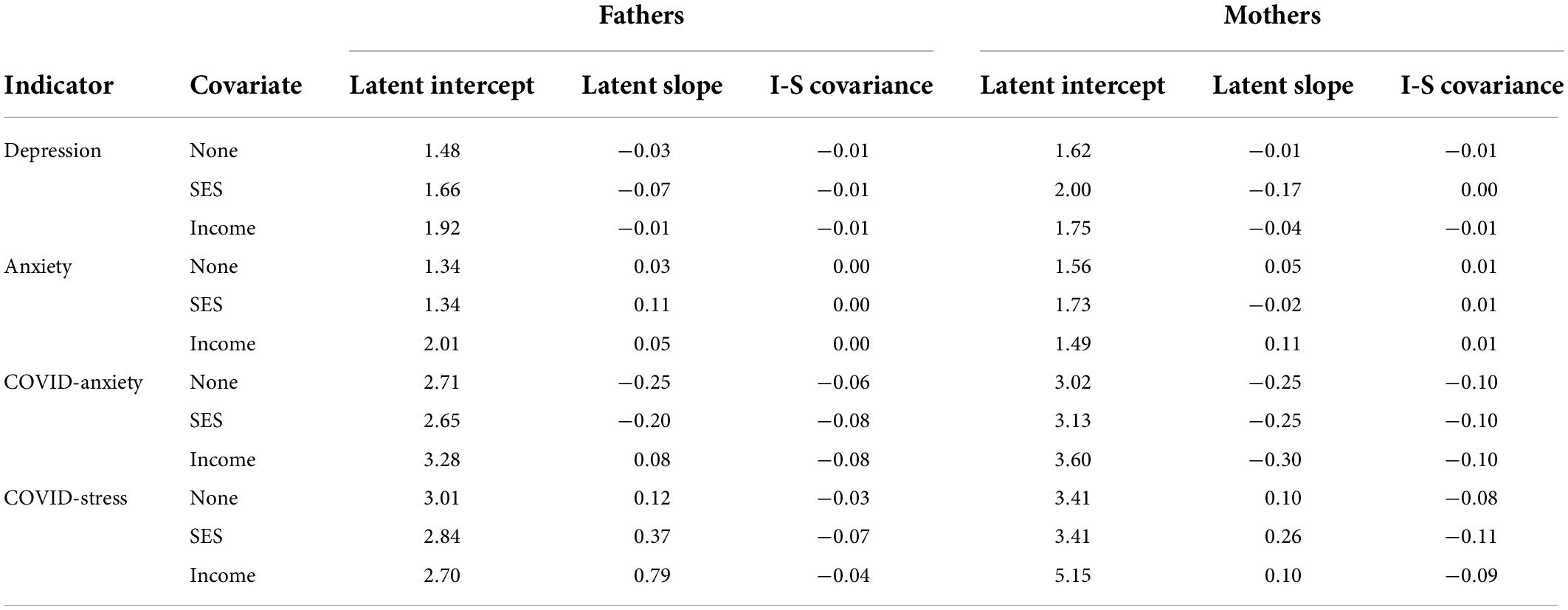
Table 4. Gender differences in (changes in) mental health indicators.
Discussion
Although the initial evidence has suggested a severe impact of the COVID-19 pandemic on mental health in the general population [e.g., (52–54), and parents in particular (23, 36, 55)], the present results have mostly indicated minor changes in parents’ mental health over the course of the study. The notable exceptions are a decrease in COVID-related anxiety and an increase in COVID-related stress after controlling for parents’ socio-economic situation.
At the beginning of the COVID-19 pandemic, there was little information about the virus or the situation in general available (56). In its initial phase, a worsening in mental health could be seen (57, 58). However, as both the amount of available information and people’s experience with the virus has increased, people have likely adapted to the situation and their mental health has stabilized or improved (59). On top of that, some people have ceased to think about COVID-19 being a serious threat or re-evaluated their perspective as a result of increased fake news and politicization of the situation (60). Concerns about health have played an important role in mental health during the pandemic (61). Although the population of parents has experienced more stress compared to non-parents (4), similar to the general population (62), the stress got lower as the perceived threat and severity of the situation decreased. In addition, the availability of vaccines and their efficiency has likely lowered the worries about health (63), helping to mitigate the negative impact of the pandemic situation on mental health.
With regard to the specific aspects of mental health measured in the current study, the results have shown a small decrease in the level of depression. Several studies have reported an increase in the depression rate due to the COVID-19 pandemic [e.g., (64–66)]. However, this increase was observed during the first few months of the pandemic. Fancourt et al. (67) have found that after depression peaked during the first few months, its level has tended to decrease and stabilize during later months. This is consistent with Kwong et al. (68) who observed no changes in the level of depression measured in April and May 2020, compared to the pre-pandemic level. The current results suggest that in the population of Slovak parents, reactive grief from an objective situation could have occurred instead of an increase in clinical depression. As such, the pandemic could be regarded as a temporary situation and people will learn how to cope with it. Although Martin et al. (69) have pointed out that people with higher pre-pandemic levels of depression are much more vulnerable to depression developing further, the study found no clear pattern suggesting that parents with higher initial levels of depression would get even worse or get better more slowly.
Valero-Moreno et al. (70) have found no increase in anxiety in the initial stages of the pandemic. Further evidence has also suggested a stabilization or even decline in the level of anxiety over time (67). In the present study, there was a small increase in anxiety observed across the four time points. Even though the results only indicate a minor impact of the pandemic on the changes in the level of anxiety, three important points can be discussed. Firstly, the data collection for the present study started in late 2020. While an increase in mental health issues seems to have occurred in the initial phase of the pandemic, there is no data to support or contradict this claim. Following other studies (57, 58, 67), it can be assumed that after the initial increase in the level of anxiety, a stabilizing trend is likely to have occurred. On the other hand, the pandemic situation during the first months was significantly better in Slovakia (the infection rate was one of the world’s lowest) compared to other countries. This might have caused a faster stabilization rate in the case of Slovakia.
Secondly, although stabilization was probably the most common mental health response to the pandemic, some subgroups may have also experienced worsening or improving mental health issues (71). As baseline data and information on pre-existing mental health status are not a part of the current study, interpretations should be made with some caution. While our data reflect a stabilizing trend, there is also a possibility that the levels of mental health issues found in the current study could reflect an increase which remained the same over time. More specifically, after the outbreak of the pandemic, an increase in mental health issues may have occurred and stayed at that higher level during our data collection. Alternatively, a worsening may have occurred in that subgroup of people with pre-existing mental health issues who were at higher risk of mental health deterioration (72). However, there is no data that could help clarify the possible heterogeneity of mental health responses to the pandemic in the current study (see limitations).
Thirdly, the measurement of mental health indicators should be taken into account. Many studies that have found modest changes in mental health during the COVID-19 pandemic assessed mental health using general measures [e.g., (71, 73, 74)]. However, it seems there is a qualitative difference between conventional mental health constructs and COVID-related mental health issues. This has been highlighted by Kubb and Foran (38) who discuss that findings concerning traditional measures of mental health should not be generalized to COVID-related mental health problems. The issue of COVID-related mental health and its consequences has been often neglected by researchers (75).
The present findings indicate a substantially higher dynamic of COVID-related mental health constructs compared to generally oriented depression or anxiety. In particular, the findings indicate that COVID-related anxiety started to decrease significantly after the first two waves of data collection. On the contrary, COVID-related stress increased over time, with its peak being observed in the third wave of data collection (late 2021). Stressors, their intensity as well as their qualitative aspects have changed during the pandemic (see (76, 77), and a fluctuation of stress related to the pandemic is thus natural (78). Consequently, there is a possibility of an interplay between COVID-related stress and COVID-related anxiety. In particular, the initial fear related to the pandemic can, through the inability to cope with stressors, develop into COVID-related anxiety. This is also supported by the strong bivariate relationships (rs > 0.50) between the constructs across all time points.
As COVID-related worries are determined by different stressors of different severity during different phases of the pandemic, COVID-related stress tends to get higher in the early phases of the pandemic or at its peak (78). In the current data, this is reflected by an increase in COVID-related stress in late 2021. This was when strict anti-pandemic measures were imposed in Slovakia and the infection and mortality rates were failing to decrease. More specifically, the infection rate and number of new daily cases were extremely high while the vaccination rate was low (see description of data collection). Furthermore, a new COVID-19 variant – Omicron – appeared in late 2021 and increased parents’ worries about their children’s vulnerability to this mutation (79). With an increased infection rate among children, parents were further exposed to the difficulties of ensuring care during the time of homeschooling, while also meeting other work-related needs. The available evidence has confirmed that children being in quarantine and parents’ difficulties in managing quarantine contributed to an increase in parental stress (33). With isolation from the wider family and teachers, parents were often left alone to take care of and educate their children. Childcare without sufficient external support is known to be stressful (80). The instability of the current pandemic situation and the associated difficulties in daily life has likely exacerbated the stress further (6).
We further analyzed the trends in mental health also after controlling for the subjective economic status and equivalized household income. The results indicate that a decrease in depression became more visible when the model controlled for the subjective SES. This result corresponds with the findings of Hoebel et al. (81) who have pointed out that the association between the objective economic situation and depressive symptoms is partially mediated through subjective SES for both men and women. The increase in general anxiety was more pronounced when the model controlled for income. For COVID-related anxiety, it seems that controlling for the socioeconomic situation does not affect its dynamics. On the other hand, a notable increase in COVID-related stress was amplified by both subjective SES and income. Various studies have confirmed the association between the economic situation and mental health issues during the initial phase of the pandemic (see (82). Indeed, parents tend to question their role and ability to take financial care of their family (83, 84).
In terms of the bivariate correlations between the constructs, it can be concluded that the relationships between the economic situation and mental health issues are almost uniformly negative. Valero-Moreno et al. (70) have noted a higher level of stress in parents at the beginning of the pandemic. The present data do not cover the initial phases of the pandemic and thus it is not known the extent to which parents’ level of stress at the end of the year 2020 differed from the levels in the early months. This raises the question as to whether the stabilization of COVID-related stress will follow the stabilization of the economic situation. This is especially after people have realized that economic worsening may not be as damaging as expected (85) or that it is reversible as the pandemic situation can improve [for example during the summer, even if the improvement is temporary; (86, 87)].
Given the aim of the study, gender differences can be discussed in the context of changes in depression, anxiety and stress separately. The results have confirmed that mothers tend to score higher in most measurements (models without covariates) and this corresponds to epidemiological data from 23 EU countries which all report a higher incidence of depression in women (88). On the other hand, the group differences between fathers and mothers in changes in mental health indicators during the pandemic were negligible although gender differences are observable when SES is taken into account. This may relate to socio-economic stratification across genders resulting from a variety of factors including differences in education choices, preferred job and industry, horizontal and vertical occupational gender segregation, work experience, number of hours worked, breaks in employment (such as for bearing and raising children), as well as gendered income disparity [see, e.g., (89, 90)]. The reduction in the symptoms of depression of mothers compared to fathers can be explained by the higher level of involvement in the education of their children during the pandemic period. The improvement in maternal depressive symptoms can be further explained by the higher presence of the father in the family (88) which is connected to better social support in their partnership (91). The results further showed that COVID-related anxiety and COVID-related stress increased in the group of fathers after controlling for household income. The increase was very sharp, especially in the case of COVID-related stress. It is likely that cultural expectations of the role of the father in the family in terms of providing income for the family will put more pressure on fathers.
Limitations
The limitations of the present study can be interpreted on several levels such as limits related to the design of data collection, parental characteristics, social and personal context, and children’s characteristics. Participants were not asked about their pre-morbid status such as pre-existing mental health issues, medication or using supplements. Therefore, the evaluation of changes in people with pre-existing mental health issues [e.g., worsening of symptoms; recurrence, etc.; (92) is lacking in the present analyses]. Despite the longitudinal design of this study, the findings are limited to the changes that happened after the first several months of the pandemic and do not capture the initial dynamic in parents’ mental health (93). Furthermore, even though the data collection procedure was set to collect data from a representative sample of the Slovak population (based on quota characteristics for gender, age, education, and region), parents with lower SES (94) or parents below the poverty threshold are less likely to participate in the survey as they are known to have limited access to technology and internet. Moreover, specific financial concerns that could have affected the levels of (especially) stress were not assessed in detail. Future research could thus focus on these variables and examine which financial constraints have the strongest effect on parents’ mental health. At the same time, there was also no data on social support in the context of partnerships (80) nor on the level of resilience (95). These could both have affected the levels of stress and anxiety. It is possible that in some families the differences are caused by the parental role rather than by gender (96). Broader environmental and contextual factors could also have shaped the results. For instance, the strict anti-pandemic measures, including the obligatory quarantine, likely caused higher levels of mental health issues in the first two or possibly three waves of data collection. Moreover, factors like personal experience with the virus (e.g., the severity of the course of the infection, hospitalization, death of a close one, etc.) would have had an impact on one’s mental health but were not captured in the present study. For future research, it would be useful to take a look at social isolation due to the obligatory periods of quarantine. If a person has a positive attitude toward quarantine (considers it as protection from the virus), it might help them to cope with the situation better. The reduction in social activities has lowered the likelihood of getting infected. Thus, people that were more likely to adhere to the anti-pandemic measures, like social distancing, could have experienced less stress and fear about their health (97). Moreover, some people could have changed their lifestyle to handle the situation and stress related to the pandemic, restrictions, or lockdown (see (98). In addition, it could be of interest to examine if information about COVID-19 has been correctly presented. Clear and unbiased information and instructions can serve as a protective factor in alleviating mental health issues (65, 99, 100). Lastly, parents’ mental health could be determined by the characteristics of their children. In particular, the level of experienced stress in parents is associated with the perceived failure in taking care of their children, even more so if the child has special needs.
Implications
The presented findings provide several fundamental proposals that could help improve health and social policies. We highly recommend paying more attention to parents’ mental health and especially to those who have a high baseline level of mental health issues. Moreover, parents’ mental health is mirrored in the well-being of their children. In terms of social policies, it seems to be of importance to pay extra attention to parents’ feelings and worries as their level of stress increases once they get concerned about their children’s safety, work-life balance and household income (20, 36, 84). Overall, the imposed anti-pandemic measures should also take into account the factors related to people’s mental health. In addition, governments should ensure easily accessible psychological or psychiatric aid to help alleviate the growing levels of stress. Social support programs, stress management training, and easy-to-implement interventions on emotional regulation strategies [e.g., reappraisal interventions; (101)] could positively affect parents’ ability to cope with the pandemic situation.
Conclusion
Throughout the COVID-19 pandemic, societies and individuals have had to deal with a long-term crisis and intensive demands on safety and quality of life. This period of time has been accompanied by financial insecurity, job loss, or income reductions that could have occurred as a consequence of the pandemic. As parents’ mental health can have a wider impact, especially on their children (31), the current study aimed to look at the mental health of parents over a year and a half of the COVID-19 pandemic. In addition, differences between mothers and fathers were analyzed. The current results do not support the initial notions that the pandemic has a huge impact on mental health [e.g., (102–105)]. Indeed, the longitudinal evidence, including the presented study, has suggested that the deterioration of mental health has been small or negligible in both the general population (74) and population of parents (70). These results indicate that, in general, parents have adapted to the pandemic situation. In comparison to pre-pandemic times, a decrease in mental health issues has also been observed (64). The current study mostly found minor changes in parents’ mental health over the course of the study. Gender differences were also mostly negligible. There were some exceptions observed after controlling for the subjective and especially objective economic situation. However, more attention should be paid to COVID-related mental health issues and stressors which are likely to change over the course of the pandemic.
Data availability statement
Data and the analytic script can be found at https://osf.io/epmt7/.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee at the Faculty of Arts, University of Presov. The patients/participants provided their written informed consent to participate in this study.
Author contributions
LV: data curation, conceptualization, investigation, writing – original draft, and writing – review and editing. GM: conceptualization, investigation, writing – original draft, and writing – review and editing. DF: conceptualization, investigation, supervision, writing – original draft, and writing – review and editing. ML: investigation, writing – original draft, and writing – review and editing. JB: conceptualization, writing – original draft, and writing – review and editing. MŠ: writing – original draft and writing – review and editing. PB: data curation, conceptualization, and writing – review and editing. IR: formal analysis, methodology, and writing – review and editing. MA: conceptualization, investigation, supervision, formal analysis, methodology, and writing – review and editing. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Slovak Research and Development Agency (APVV-17-0418 and APVV-20-0319), the Research Grant Agency of the Ministry of Education, Science, Research and Sport of the Slovak Republic and Slovak Academy of Science (VEGA 1/0559/21 and VEGA 1/0719/20), project PRIMUS/20/HUM/009, and NPO Systemic Risk Institute LX22NPO5101.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
A detailed description of measures can be found at https://osf.io/bskr4/. A chronological overview of the pandemic situation and anti-pandemic measures in Slovakia is available at https://osf.io/vjmfd/. The full version of Table 3 is available at https://osf.io/ydq56.
References
1. Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. (2021) 281:91–8. doi: 10.1016/j.jad.2020.11.117
2. Nochaiwong S, Ruengorn C, Thavorn K, Hutton B, Awiphan R, Phosuya C, et al. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: a systematic review and meta-analysis. Sci Rep. (2021) 11:10173. doi: 10.1038/s41598-021-89700-8
3. Gadermann AC, Thomson KC, Richardson CG, Gagné M, McAuliffe C, Hirani S, et al. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: findings from a national cross-sectional study. BMJ Open. (2021) 11:e042871. doi: 10.1136/bmjopen-2020-042871
4. Adams EL, Smith D, Caccavale LJ, Bean MK. Parents are stressed! Patterns of parent stress across COVID-19. Front Psychiatry. (2021) 12:626456. doi: 10.3389/fpsyt.2021.626456
5. Ananat, E, Gassman-Pines A. Snapshot of the COVID Crisis Impact on Working Families. (2020). Available online at: https://digitalcommons.wcl.american.edu/wlpeconomy/8 (accessed February 01, 2022).
6. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Int Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
7. Hyman M, Mark C, Imteaj A, Ghiaie H, Rezapour S, Sadri AM, et al. Data analytics to evaluate the impact of infectious disease on economy: case study of COVID-19 pandemic. Patterns (New York, N.Y.). (2021) 2:100315. doi: 10.1016/j.patter.2021.100315
8. Sanchez, DG, Parra NG, Ozden C, Rijkers B. Which Jobs are Most Vulnerable to COVID-19? What an Analysis of the European Union reveals. (2020). Available online at: https://papers.ssrn.com/abstract=3602354 (accessed February 16, 2022).
9. Shen M, Xiao Y, Yuan Y, Chen X, Li J. Perceived stress links income loss and urticaria activity during the coronavirus disease 2019 pandemic. Ann Allergy Asthma Immunol. (2021) 126:89–90. doi: 10.1016/j.anai.2020.08.019
10. Li J, Song Q, Peng C, Wu Y. COVID-19 pandemic and household liquidity constraints: Evidence from micro data. Emerg Markets Financ Trade. (2020) 56:3626–34. doi: 10.1080/1540496x.2020.1854721
11. Mikolai J, Keenan K, Kulu H. Intersecting household-level health and socio-economic vulnerabilities and the COVID-19 crisis: an analysis from the UK. SSM – Populat Health. (2020) 12:100628. doi: 10.1016/j.ssmph.2020.100628
12. OECD. Unemployment rate (indicator). (2022). Available online at: https://data.oecd.org/unemp/unemployment-rate.htm. (accessed January 27, 2022).
13. Buchel, O, Fašungová L, Hábel B, Hlaváč M, Komadel J, Veselková M. First Aid” for Slovakia: Updated report on the economic policy response to the COVID-19 pandemic. Gov.Sk. (2020). Available online at: https://www.employment.gov.sk/files/slovensky/ministerstvo/analyticke-centrum/analyticke-komentare/isp_first_aid_nov2020.pdf (accessed February 10, 2022).
14. Ahrendt D, Mascherini M, Nivakoski S, Saìndor E. Living, Working and COVID-19 (Update April 2021): Mental Health and Trust Decline Across EU as Pandemic Enters Another Year. Brussels: European Union (2021).
15. Hudson CG. Socioeconomic status and mental illness: tests of the social causation and selection hypotheses. Am J Orthopsychiatry. (2005) 75:3–18. doi: 10.1037/0002-9432.75.1.3
16. Wang JL, Schmitz N, Dewa CS. Socioeconomic status and the risk of major depression: the Canadian National Population Health Survey. J Epidemiol Commun Health. (2010) 64:447–52. doi: 10.1136/jech.2009.090910
17. Fryers T, Melzer D, Jenkins R. Social inequalities and the common mental disorders: a systematic review of the evidence. Soc Psychiatry Psychiatr Epidemiol. (2003) 38:229–37. doi: 10.1007/s00127-003-0627-2
18. Businelle MS, Mills BA, Chartier KG, Kendzor DE, Reingle JM, Shuval K. Do stressful events account for the link between socioeconomic status and mental health? J Public Health (Oxford, England). (2014) 36:205–12. doi: 10.1093/pubmed/fdt060
19. Sasaki Y, Shobugawa Y, Nozaki I, Takagi D, Nagamine Y, Funato M, et al. Association between depressive symptoms and objective/subjective socioeconomic status among older adults of two regions in Myanmar. PLoS One. (2021) 16:e0245489. doi: 10.1371/journal.pone.0245489
20. Kerr ML, Rasmussen HF, Fanning KA, Braaten SM. Parenting during COVID-19: a study of parents’ experiences across gender and income levels. Fam Relat. (2021) 70:1327–42. doi: 10.1111/fare.12571
21. Lim-Soh JW, Tan PL. Weathering the storm: longitudinal evidence on women’s changing family relationships during COVID-19. J Fam Issues. (2022). doi: 10.1177/0192513X221087721
22. Gassman-Pines A, Ananat EO, Fitz-Henley J II. COVID-19 and parent-child psychological well-being. Pediatrics. (2020) 146:e2020007294. doi: 10.1542/peds.2020-007294
23. Cheng Z, Mendolia S, Paloyo AR, Savage DA, Tani M. Working parents, financial insecurity, and childcare: mental health in the time of COVID-19 in the UK. Rev Econ Household. (2021) 19:123–44. doi: 10.1007/s11150-020-09538-3
24. Viola TW, Nunes ML. Social and environmental effects of the COVID-19 pandemic on children. J Pediatr. (2022) 98(Suppl 1):S4–12. doi: 10.1016/j.jped.2021.08.003
25. Orsini A, Corsi M, Pedrinelli V, Santangelo A, Bertelloni C, Dell’Oste V, et al. Post-traumatic stress, anxiety, and depressive symptoms in caregivers of children tested for COVID-19 in the acute phase of the Italian outbreak. J Psychiatr Res. (2021) 135:256–63. doi: 10.1016/j.jpsychires.2021.01.024
26. Meyer B, Zill A, Dilba D, Gerlach R, Schumann S. Employee psychological well-being during the COVID-19 pandemic in Germany: a longitudinal study of demands, resources, and exhaustion. Int J Psychol. (2021) 56:532–50. doi: 10.1002/ijop.12743
27. Adamson MM, Phillips A, Seenivasan S, Martinez J, Grewal H, Kang X, et al. International prevalence and correlates of psychological stress during the global COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:9248. doi: 10.3390/ijerph17249248
28. Johnson, MS, Skjerdingstad N, Ebrahimi OV, Hoffart A, Johnson SU. Parenting in a pandemic: parental stress, anxiety and depression among parents during the government-initiated physical distancing measures following the first wave of COVID-19. Stress Health. (2021): doi: 10.1002/smi.3120 [Epub ahead of print].
29. Achterberg M, Dobbelaar S, Boer OD, Crone EA. Perceived stress as mediator for longitudinal effects of the COVID-19 lockdown on wellbeing of parents and children. Sci Rep. (2021) 11:2971. doi: 10.1038/s41598-021-81720-8
30. Brown SM, Doom JR, Lechuga-Peña S, Watamura SE, Koppels T. Stress and parenting during the global COVID-19 pandemic. Child Abuse Neglect. (2020) 110(Pt 2):104699. doi: 10.1016/j.chiabu.2020.104699
31. Alonzo D, Popescu M, Zubaroglu Ioannides P. Mental health impact of the COVID-19 pandemic on parents in high-risk, low income communities. Int J Soc Psychiatry. (2022) 68:575–81. doi: 10.1177/0020764021991896
32. Lee SJ, Ward KP, Chang OD, Downing KM. Parenting activities and the transition to home-based education during the COVID-19 pandemic. Child Youth Serv Rev. (2021) 122:105585. doi: 10.1016/j.childyouth.2020.105585
33. Spinelli M, Lionetti F, Pastore M, Fasolo M. Parents’ stress and children’s psychological problems in families facing the COVID-19 outbreak in Italy. Front Psychol. (2020) 11:1713. doi: 10.3389/fpsyg.2020.01713
34. Köhler-Dauner F, Clemens V, Lange S, Ziegenhain U, Fegert JM. Mothers’ daily perceived stress influences their children’s mental health during SARS-CoV-2-pandemic-an online survey. Child Adolesc Psychiatry Ment Health. (2021) 15:31. doi: 10.1186/s13034-021-00385-3
35. Polónyiová K, Belica I, Celušáková H, Janšáková K, Kopčíková M, Szapuová Ž, et al. Comparing the impact of the first and second wave of COVID-19 lockdown on Slovak families with typically developing children and children with autism spectrum disorder. Autism. (2021):13623613211051480. doi: 10.1177/13623613211051480
36. Westrupp EM, Stokes MA, Fuller-Tyszkiewicz M, Berkowitz TS, Capic T, Khor S, et al. Subjective wellbeing in parents during the COVID-19 pandemic in Australia. J Psychosomat Res. (2021) 145:110482. doi: 10.1016/j.jpsychores.2021.110482
37. Crasta D, Daks JS, Rogge RD. Modeling suicide risk among parents during the COVID-19 pandemic: psychological inflexibility exacerbates the impact of COVID-19 stressors on interpersonal risk factors for suicide. J Contextu Behav Sci. (2020) 18:117–27. doi: 10.1016/j.jcbs.2020.09.003
38. Kubb C, Foran HM. Measuring COVID-19 related anxiety in parents: Psychometric comparison of four different inventories. JMIR Ment Health. (2020) 7:e24507. doi: 10.2196/24507
39. Calvano C, Engelke L, Di Bella J, Kindermann J, Renneberg B, Winter SM. Families in the COVID-19 pandemic: parental stress, parent mental health and the occurrence of adverse childhood experiences-results of a representative survey in Germany. Eur Child Adolesc Psychiatry. (2021) 1:1–13. doi: 10.1007/s00787-021-01739-0
40. Russell BS, Tambling RR, Horton AL, Hutchison M, Tomkunas AJ. Clinically significant depression among parents during the COVID-19 pandemic: examining the protective role of family relationships. Couple Fam Psychol. (2021) 10:190–201. doi: 10.1037/cfp0000175
41. Liu CH, Smiley PA, Vicman JM, Wong GTF, Doan SN. The roles of life stress and preventive health behaviors on parent mental health during the COVID-19 pandemic. J Health Psychol. (2022) 27:1470–83. doi: 10.1177/13591053211026742
42. National Health Information Center. COVID-19 Vaccination and number of positive cases. (2022). Available online at: https://covid-19.nczisk.sk/en?csrt=4131811601970157949 (accessed July 1, 2022).
43. Ministry of Health of the Slovak Republic. Press releases. (2022). Available online at: https://www.health.gov.sk/Clanky?tlacove-spravy&stranka=1 (accessed July 1, 2022).
44. Giatti L, Camelo L, do V, Rodrigues JF, de C, Barreto SM. Reliability of the macarthur scale of subjective social status – brazilian longitudinal study of adult health (ELSA-Brasil). BMC Public Health. (2012) 12:1096. doi: 10.1186/1471-2458-12-1096
45. Hagenaars AJM, De Vos K, Zaidi A. Poverty Statistics in the Late 1980s: Research Based on Micro-Data. Luxembourg: Office for official publications of the European Union (1994).
46. Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. (2003) 54:573–83. doi: 10.1016/s0006-3223(02)01866-8
47. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7: The GAD-7. Arch Int Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
48. McElroy E, Patalay P, Moltrecht B, Shevlin M, Shum A, Creswell C, et al. Demographic and health factors associated with pandemic anxiety in the context of COVID-19. Br J Health Psychol. (2020) 25:934–44. doi: 10.1111/bjhp.12470
49. Silva WAD, de Sampaio Brito TR, Pereira CR. COVID-19 anxiety scale (CAS): development and psychometric properties. Curr Psychol. (2020) 1–10. doi: 10.1007/s12144-020-01195-0 [Epub ahead of print].
50. Yamada Y, Ćepulić D-B, Coll-Martín T, Debove S, Gautreau G, Han H, et al. COVIDiSTRESS Global Survey dataset on psychological and behavioural consequences of the COVID-19 outbreak. Sci Data. (2021) 8:3. doi: 10.1038/s41597-020-00784-9
51. Rosseel Y. lavaan: AnRPackage for Structural Equation Modeling. J Statist Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
52. Roy A, Singh AK, Mishra S, Chinnadurai A, Mitra A, Bakshi O. Mental health implications of COVID-19 pandemic and its response in India. Int J Soc Psychiatry. (2021) 67:587–600. doi: 10.1177/0020764020950769
53. Fruehwirth JC, Biswas S, Perreira KM. The COVID-19 pandemic and mental health of first-year college students: examining the effect of COVID-19 stressors using longitudinal data. PLoS One. (2021) 16:e0247999. doi: 10.1371/journal.pone.0247999
54. Faisal RA, Jobe MC, Ahmed O, Sharker T. Mental health status, anxiety, and depression levels of Bangladeshi university students during the COVID-19 pandemic. Int J Mental Health Addict. (2021) 20:1500–15. doi: 10.1007/s11469-020-00458-y
55. Wu S. Effects of pandemics-related uncertainty on household consumption: evidence from the cross-country data. Front Public Health. (2020) 8:615344. doi: 10.3389/fpubh.2020.615344
56. Fauci AS, Lane HC, Redfield RR. COVID-19 – navigating the uncharted. New Engl J Med. (2020) 382:1268–9. doi: 10.1056/NEJMe2002387
57. O’Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, et al. Mental health and well-being during the COVID-19 pandemic: longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br J Psychiatry. (2021) 218:326–33. doi: 10.1192/bjp.2020.212
58. Aknin LB, De Neve J-E, Dunn EW, Fancourt DE, Goldberg E, Helliwell JF, et al. Mental health during the first year of the COVID-19 pandemic: a review and recommendations for moving forward. Perspect Psychol Sci. (2022) 17:915–36. doi: 10.1177/17456916211029964
59. Daly M, Robinson E. Anxiety reported by US adults in 2019 and during the 2020 COVID-19 pandemic: Population-based evidence from two nationally representative samples. J Affect Disord. (2021) 286:296–300. doi: 10.1016/j.jad.2021.02.054
60. Stroebe W, vanDellen MR, Abakoumkin G, Lemay EP Jr., Schiavone WM, Agostini M, et al. Politicization of COVID-19 health-protective behaviors in the United States: longitudinal and cross-national evidence. PLoS One. (2021) 16:e0256740. doi: 10.1371/journal.pone.0256740
61. Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJG. Development and initial validation of the COVID Stress Scales. J Anxiety Disord. (2020) 72:102232. doi: 10.1016/j.janxdis.2020.102232
62. Han L, Zhan Y, Li W, Xu Y, Xu Y, Zhao J. Associations between the perceived severity of the COVID-19 pandemic, cyberchondria, depression, anxiety, stress, and lockdown experience: cross-sectional survey study. JMIR Public Health Surveillance. (2021) 7:e31052. doi: 10.2196/31052
63. Andersson O, Campos-Mercade P, Meier AN, Wengström E. Anticipation of COVID-19 vaccines reduces willingness to socially distance. J Health Econ. (2021) 80:102530. doi: 10.1016/j.jhealeco.2021.102530
64. Hyland P, Shevlin M, McBride O, Murphy J, Karatzias T, Bentall RP, et al. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr Scand. (2020) 142:249–56. doi: 10.1111/acps.13219
65. Bueno-Notivol J, Gracia-García P, Olaya B, Lasheras I, López-Antón R, Santabárbara J. Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. Int J Clin Health Psychol IJCHP. (2021) 21:100196. doi: 10.1016/j.ijchp.2020.07.007
66. Perlis RH, Ognyanova K, Santillana M, Baum MA, Lazer D, Druckman J, et al. Association of acute symptoms of COVID-19 and symptoms of depression in adults. JAMA Netw Open. (2021) 4:e213223. doi: 10.1001/jamanetworkopen.2021.3223
67. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. (2021) 8:141–9. doi: 10.1016/S2215-0366(20)30482-X
68. Kwong ASF, Pearson RM, Adams MJ, Northstone K, Tilling K, Smith D, et al. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br J Psychiatry. (2021) 218:334–43. doi: 10.1192/bjp.2020.242
69. Martin A, Partika A, Castle S, Horm D, Johnson AD, Tulsa Seed Study Team. Both sides of the screen: Predictors of parents’ and teachers’ depression and food insecurity during COVID-19-related distance learning. Early Child Res Q. (2022) 60:237–49. doi: 10.1016/j.ecresq.2022.02.001
70. Valero-Moreno S, Lacomba-Trejo L, Tamarit A, Pérez-Marín M, Montoya-Castilla I. Psycho-emotional adjustment in parents of adolescents: a cross-sectional and longitudinal analysis of the impact of the COVID pandemic. J Pediatr Nurs. (2021) 59:e44–51. doi: 10.1016/j.pedn.2021.01.028
71. Shevlin M, McBride O, Murphy J, Miller JG, Hartman TK, Levita L, et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open. (2020) 6:e125. doi: 10.1192/bjo.2020.109
72. Hampshire A, Trender W, Grant JE, Mirza MB, Moran R, Hellyer PJ, et al. Item-level analysis of mental health symptom trajectories during the COVID-19 pandemic in the UK: associations with age, sex and pre-existing psychiatric conditions. Comp Psychiatry. (2022) 114:152298. doi: 10.1016/j.comppsych.2022.152298
73. Pappa S, Chen J, Barnett J, Chang A, Dong RK, Xu W, et al. A systematic review and meta-analysis of the mental health symptoms during the COVID-19 pandemic in Southeast Asia. Psychiatry Clin Neurosci. (2022) 76:41–50. doi: 10.1111/pcn.13306
74. Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. (2022) 296:567–76. doi: 10.1016/j.jad.2021.09.098
75. Ransing R, Ramalho R, Orsolini L, Adiukwu F, Gonzalez-Diaz JM, Larnaout A, et al. Can COVID-19 related mental health issues be measured? Brain Behav Immunity. (2020) 88:32–4. doi: 10.1016/j.bbi.2020.05.049
76. Graupensperger, S, Calhoun BH, Patrick ME, Lee CM. Longitudinal effects of COVID-19-related stressors on young adults’ mental health and wellbeing. Appl Psychol Health Well-Being. (2022): doi: 10.1111/aphw.12344 [Epub ahead of print].
77. Chandola, T, Kumari M, Booker CL, Benzeval M. The mental health impact of COVID-19 and lockdown-related stressors among adults in the UK. Psychol Med. (2020):1–10. doi: 10.1017/S0033291720005048
78. Asmundson GJG, Rachor G, Drakes DH, Boehme BAE, Paluszek MM, Taylor S. How does COVID stress vary across the anxiety-related disorders? Assessing factorial invariance and changes in COVID Stress Scale scores during the pandemic. J Anxiety Disord. (2022) 87:102554. doi: 10.1016/j.janxdis.2022.102554
79. Kozlov M. Does Omicron hit kids harder? Scientists are trying to find out. Nat. News. (2022). Available online at: https://doi.org/10.1038/d41586-022-00309-x (accessed March 1, 2022).
80. Sprang G, Silman M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med Public Health Prep. (2013) 7:105–10. doi: 10.1017/dmp.2013.22
81. Hoebel J, Maske UE, Zeeb H, Lampert T. Social inequalities and depressive symptoms in adults: the role of objective and subjective socioeconomic status. PLoS One. (2017) 12:e0169764. doi: 10.1371/journal.pone.0169764
82. Wang Y, Kala MP, Jafar TH. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: a systematic review and meta-analysis. PLoS One. (2020) 15:e0244630. doi: 10.1371/journal.pone.0244630
83. Bassuk EL, Beardslee WR. Depression in homeless mothers: addressing an unrecognized public health issue. Am J Orthopsychiatry. (2014) 84:73–81. doi: 10.1037/h0098949
84. McDonald A, Thompson AJ, Perzow SED, Joos C, Wadsworth ME. The protective roles of ethnic identity, social support, and coping on depression in low-income parents: a test of the adaptation to poverty-related stress model. J Consult Clin Psychol. (2020) 88:504–15. doi: 10.1037/ccp0000477
85. Heeren A, Hanseeuw B, Cougnon L-A, Lits G. Excessive worrying as a central feature of anxiety during the first COVID-19 lockdown-phase in Belgium: insights from a network approach. Psychol Belgica. (2021) 61:401–18. doi: 10.5334/pb.1069
86. Wang J, Tang K, Feng K, Lin X, Lv W, Chen K, et al. Impact of temperature and relative humidity on the transmission of COVID-19: a modelling study in China and the United States. BMJ Open. (2021) 11:e043863. doi: 10.1136/bmjopen-2020-043863
87. Demongeot J, Flet-Berliac Y, Seligmann H. Temperature decreases spread parameters of the new covid-19 case dynamics. Biology. (2020) 9:94. doi: 10.3390/biology9050094
88. Van de Velde S, Bracke P, Levecque K. Gender differences in depression in 23 European countries. cross-national variation in the gender gap in depression. Soc Sci Med. (2010) 71:305–13. doi: 10.1016/j.socscimed.2010.03.035
89. American Psychological Association. Report of the APA Task Force on Socioeconomic Status. Washington, DC: American Psychological Association (2007).
90. Entmacher J, Robbins KG, Vogtman J, Frohlich L. Insecure and unequal: Poverty and Income Among Women and Families 2000-2012. Washington, DC: National Women’s Law Center (2013).
91. Mercer RT. Becoming a mother versus maternal role attainment. J Nurs Scholarsh. (2004) 36:226–32. doi: 10.1111/j.1547-5069.2004.04042.x
92. Chatterjee SS, Barikar CM, Mukherjee A. Impact of COVID-19 pandemic on pre-existing mental health problems. Asian J Psychiatry. (2020) 51:102071. doi: 10.1016/j.ajp.2020.102071
93. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in us adults before and during the COVID-19 Pandemic. JAMA Netw Open. (2020) 3:e2019686. doi: 10.1001/jamanetworkopen.2020.19686
94. Freeman A, Tyrovolas S, Koyanagi A, Chatterji S, Leonardi M, Ayuso-Mateos JL, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. (2016) 16:1098. doi: 10.1186/s12889-016-3638-0
95. Southwick SM, Vythilingam M, Charney DS. The psychobiology of depression and resilience to stress: implications for prevention and treatment. Ann Rev Clin Psychol. (2005) 1:255–91. doi: 10.1146/annurev.clinpsy.1.102803.143948
96. Beehr TA, Farmer SJ, Glazer S, Gudanowski DM, Nair VN. The enigma of social support and occupational stress: source congruence and gender role effects. J Occupat Health Psychol. (2003) 8:220–31. doi: 10.1037/1076-8998.8.3.220
97. Sfendla A, Hadrya F. Factors associated with psychological distress and physical activity during the COVID-19 pandemic. Health Secur. (2020) 18:444–53. doi: 10.1089/hs.2020.0062
98. van der Werf ET, Busch M, Jong MC, Hoenders HJR. Lifestyle changes during the first wave of the COVID-19 pandemic: a cross-sectional survey in the Netherlands. BMC Public Health. (2021) 21:1226. doi: 10.1186/s12889-021-11264-z
99. Luo M, Guo L, Yu M, Jiang W, Wang H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – A systematic review and meta-analysis. Psychiatry Res. (2020) 291:113190. doi: 10.1016/j.psychres.2020.113190
100. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. (2020) 16:1–11. doi: 10.1186/s12992-020-00589-w
101. Wang K, Goldenberg A, Dorison CA, Miller JK, Uusberg A, Lerner JS, et al. A multi-country test of brief reappraisal interventions on emotions during the COVID-19 pandemic. Nat Hum Behav. (2021) 5:1089–110. doi: 10.1038/s41562-021-01173-x
102. Hossain MM, Tasnim S, Sultana A, Faizah F, Mazumder H, Zou L, et al. Epidemiology of mental health problems in COVID-19: a review. F1000Research. (2020) 9:636. doi: 10.12688/f1000research.24457.1
103. Kumar A, Nayar KR. COVID 19 and its mental health consequences. J Ment Health. (2021) 30:1–2. doi: 10.1080/09638237.2020.1757052
104. Pfefferbaum B, North CS. Mental health and the covid-19 pandemic. New Engl J Med. (2020) 383:510–2. doi: 10.1056/NEJMp2008017
Keywords: parents, mental health, depression, anxiety, stress, COVID-19, pandemic, economic situation
Citation: Vargová L, Mikulášková G, Fedáková D, Lačný M, Babjáková J, Šlosáriková M, Babinčák P, Ropovik I and Adamkovič M (2022) Slovak parents’ mental health and socioeconomic changes during the COVID-19 pandemic. Front. Psychiatry 13:934293. doi: 10.3389/fpsyt.2022.934293
Received: 02 May 2022; Accepted: 20 July 2022;
Published: 18 August 2022.
Edited by:
Sabina Kapetanovic, University West, SwedenReviewed by:
Haitham Jahrami, Arabian Gulf University, BahrainNorhamizan Hamzah, University of Malaya, Malaysia
Copyright © 2022 Vargová, Mikulášková, Fedáková, Lačný, Babjáková, Šlosáriková, Babinčák, Ropovik and Adamkovič. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lenka Vargová, bGVua2EudmFyZ292YUBzbWFpbC51bmlwby5zaw==