 Ching-Fang Sun
Ching-Fang Sun Zeeshan Mansuri
Zeeshan Mansuri Chintan Trivedi
Chintan Trivedi Ramu Vadukapuram4
Ramu Vadukapuram4 Abhishek Reddy
Abhishek Reddy
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 16 November 2022
Sec. Molecular Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.933524
This article is part of the Research Topic Comorbidity in Patients with Psychiatric Disorders: Epidemiological and Molecular Perspectives View all 9 articles
Objectives: Adolescents with a homicidal tendency is a growing concern in the United States. Studies in the past have showcased the relationship between homicidal ideation (HI) and psychiatric illnesses, but very limited information is available on the adolescent and inpatient population. We aim to evaluate the prevalence of demographic characteristics and psychiatric disorders in adolescents with and without HI.
Materials and methods: Adolescent (age 12–17) population admitted to the hospital with the diagnosis of homicidal ideation was identified from the 2016–2018 National Inpatient Sample Dataset (NISD). Patients without HI were defined as the control group. The prevalence of psychiatric comorbidities between the groups was compared by applying the Rao-Scott adjusted chi-square test. We used multivariable logistic regression to generate odds ratio (OR) of homicidal ideation as an outcome; we adjusted age, sex, race, socioeconomic status, substance use disorders, alcohol use disorders, and psychiatric comorbidities.
Results: A total of 18,935 patients (mean age: 14.5) with HI diagnosis were identified in this study. Majority of the patients were male subjects in the HI group compared to the control group (58.7 vs. 41.2%, p < 0.001). Racially, HI was more prevalent in white race (56.0 vs. 52.6%, p < 0.001) and black race (22.3 vs. 17.8%, p < 0.001), compared to Hispanic race (14.9 vs. 21.3%, p < 0.001). Major depression (Odds ratio [OR]: 2.66, p < 0.001), bipolar disorder (OR: 3.52, p < 0.001), anxiety disorder (OR: 1.85, p < 0.001), ADHD, and other conduct disorders (OR: 4.01, p < 0.001), schizophrenia (OR: 4.35, p < 0.001) are strong predictors of HI. Suicidality was prevalent in 66.9% of patients with HI.
Conclusion: We found a higher prevalence of psychiatric illnesses such as depression, anxiety, and bipolar disorder in adolescents with homicidal ideation in the inpatient setting. White and black races were more prevalent in patients with homicidal ideation. Further large-scale longitudinal research studies are warranted to establish the correlation between psychiatric disorders and homicidal ideation among adolescents.
Though the adolescent legal offense case rates in the US are generally trending down, the number of juvenile criminal homicides has conversely increased by 49% in the recent 5 years, while most offenders are older than 16 (6%), male subjects (89%), and non-Caucasian (72%) (1). The number of murder offenders peaks at the age group of 20–29, but the age group of 17–19 has the highest number (2). Homicidal events are a growing concern in the US. Homicidal events, especially those with firearms, illicit the publics’ fear about personal safety; decrease satisfaction with law enforcement and the trust of others (3). Also, violence is a form of financial burden to society. A single homicide could cost nearly $4 million (4).
Homicidal ideation in the adolescent population deserves public attention. Adolescents endorse the tendency toward rewards approach behavior with increased emotion reactivity and limited impulse control due to immature neurodevelopmental status (5–7). However, they might have to undergo the same legal process as adults. In most states in the US, the maximum age of juvenile court jurisdiction is age 17, but murder and serious violent felony cases will be excluded from juvenile court (8). Furthermore, violent and chronic young offenders are very likely to become adult delinquents (9, 10). Of note, homicidal ideation is not only related to homicidal events, but various kinds of criminal activities with higher severity (10). As a result, early identification and intervention is a reasonable, cost-effective strategy to protect both the youth and society.
Previous research has shown the correlation between HI and psychiatric illnesses in adolescents, with the evidence that students with mental health issues were arrested at a rate of 2.9 times more than their healthy counterparts (11, 12). Juvenile offenders with mental illness also have a greater risk of re-offending (13). Childhood maltreatment, conduct disorder, attention-deficit hyperactivity disorder, mood disorder, tic disorder, and abnormal neuropsychiatric findings such as learning disabilities have been proven to increase the odds of comorbid HI (12, 14–16). HI is also well-known to harbor depression and suicidal ideation (SI) (17).
Despite evidence demonstrating substantial mental health conditions predisposing to HI in adolescents, minimal information is available on the adolescent inpatient population, the most vulnerable group needs a higher level of care. Our study aims to evaluate the difference in demographic characteristics and comorbid psychiatric disorders in adolescents with and without HI in a nationwide prospect.
We reviewed patient records from the Nationwide Inpatient Sample (NIS) dataset during 2016–2018. The NIS database is an administrative dataset from the Healthcare Cost and Utilization Project (HCUP) and Agency for Healthcare Research and Quality (AHRQ) (17). NIS is released annually and contains information on over 150 patient and hospital-level data elements, such as diagnoses, procedures, patient demographics (e.g., sex, age, race, median income), and discharge disposition, primary payer, length of stay, and hospital characteristics (bed size, location, and teaching status). The NIS provides weights (the trend weight prior to the year 2011 and the discharge weight after the year 2011) that allow nationally representative estimates. As NIS excludes data elements that could directly or indirectly identify individuals, this study was exempt from review by the institutional review board. Also, each record contains primary (indication for hospital admission) and secondary diagnosis information based on the International Classification of Diseases, Clinical Modification/Procedure Coding System (ICD-10-CM). Diagnoses were aggregated according to the ICD-10 code provided in Clinical Classification Software groupings of psychiatric and substance-related disorders.
The study group was defined as adolescent aged 12–17 with homicidal ideation (ICD-10 code: R45.850) by applying the ICD-10 code provided in the NIS dataset. Adolescent aged 12–17 without homicidal ideation (ICD-10 code: R45.850) were defined as the control group. We collected baseline demographic data for both the study and control group. Further, we collected data on psychiatric and substance use disorder comorbidities based on the clinical classification software grouping provided on the HCUP website.
We calculated mean and standard error to present continuous data and percent for categorical data. All tests were two-sided. A p-value of less than 0.05 was considered statistically significant. The prevalence of psychiatric comorbidities between the groups was compared by applying Rao-Scott adjusted chi-square test. Multivariable logistic regression was performed with homicidal ideation as an outcome; we adjusted age, sex, race, socioeconomic status, substance use disorders, alcohol use disorders, and psychiatric comorbidities. All statistical analyses were performed by using the SPSS version 26.0 software for Windows (IBM Software, Inc., Armonk, NY, USA).
The baseline characteristics of the study group and control group are shown in Table 1. A total of 18,935 patients (mean age: 14.5 years) with HI diagnosis were identified with a male predominant pattern (58.7 vs. 41.2%, p < 0.001). Racially, HI was more prevalent in white race (56.0 vs. 52.6%, p < 0.001) and black race (22.3 vs. 17.8%, p < 0.001) compared to Hispanic race (14.9 vs. 21.3%, p < 0.001). Patients with HI were more likely to be covered by Medicare or Medicaid insurance (59.4 vs. 50.6%, p < 0.001) with a lower household income (34.4 vs. 30.7% in the lowest 25% of household income, p < 0.001). No significant difference was found in the rural or urban area, whereas HI was more prevalent in hospitals in the Midwest and southern region of the US (33.8 vs. 23.9%; 43.4 vs. 39.9%). All the psychiatric comorbidities included in our study were more prevalent in patients with HI (Figure 1) with a p-value less than 0.001. Suicidality including suicidal ideation and suicide attempt was prevalent in 66.9% of patients with HI.
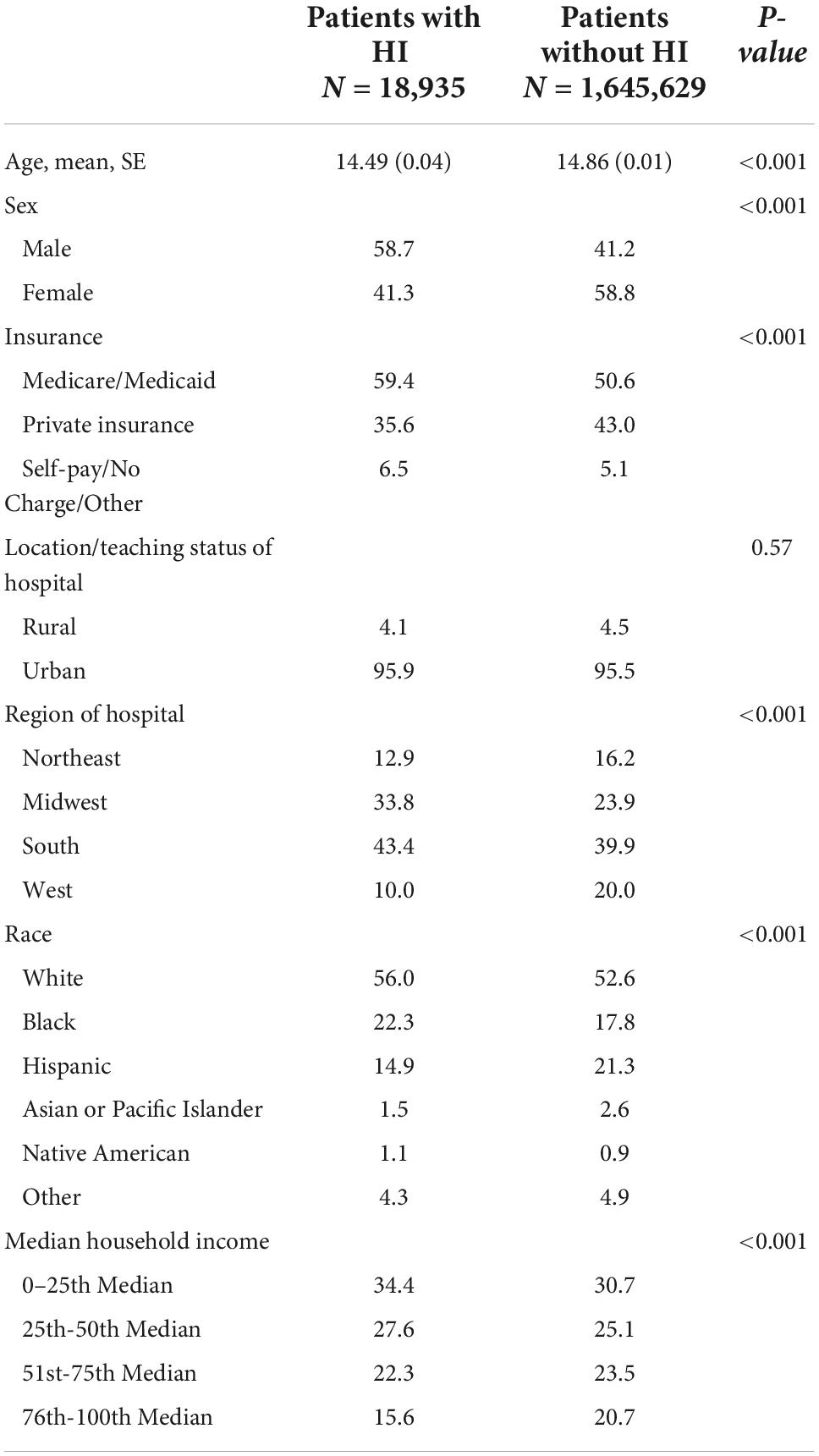
Table 1. Demographic characteristics of the patients (age 12–17) with and without homicidal ideation.
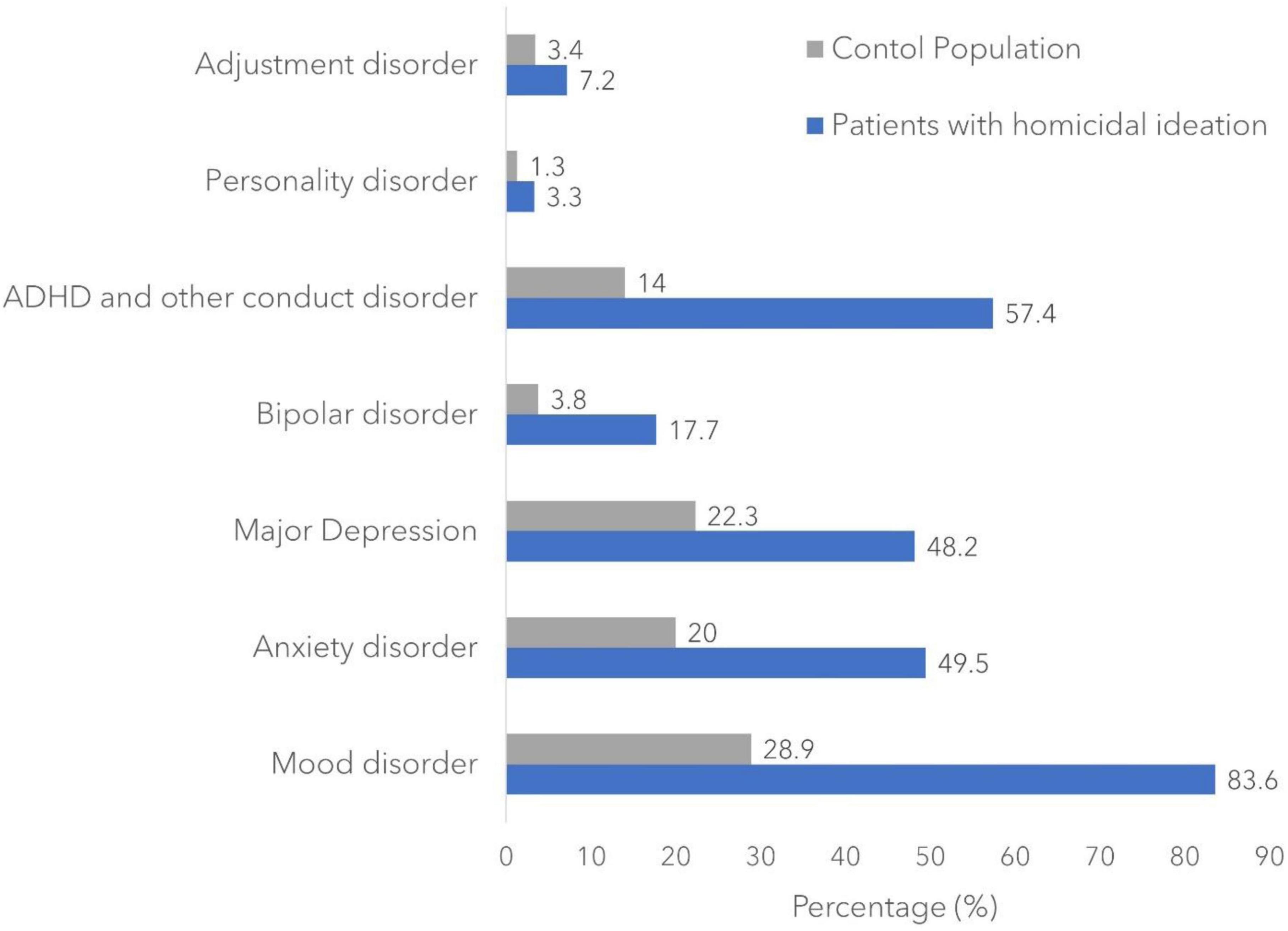
Figure 1. Incidence rate of psychiatric comorbidities among the study population.
The results of the multivariable analysis are shown in Table 2. In the multivariable analysis, major depression (OR: 2.66, p < 0.001), bipolar disorder (OR: 3.52, p < 0.001), anxiety disorder (OR: 1.85, p < 0.001), ADHD, other conduct disorders (OR: 4.01, p < 0.001), and schizophrenia (OR: 4.35, p < 0.001) were strong predictors of the outcome. No association was found between personality disorders and homicidal ideation (p = 0.27).
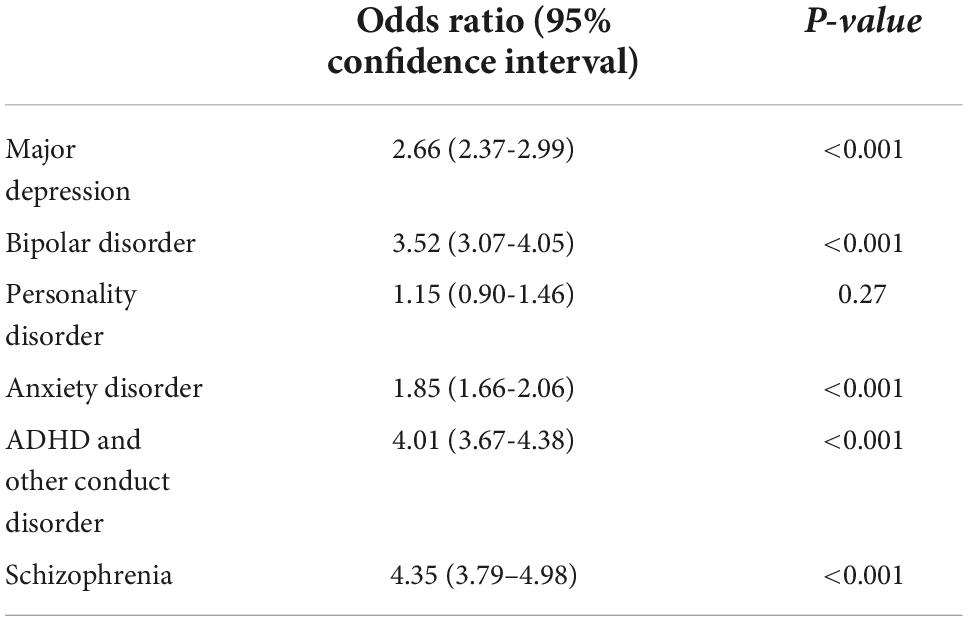
Table 2. Multivariable analysis for predictors of homicidal ideation.
The demographic feature of adolescents with HI in our study demonstrates a propensity which is similar to adolescents being arrested for murder and non-negligent manslaughter: male predominant (58.7 vs. 41.2%, p < 0.001), white (56.0 vs. 52.6%, p < 0.001), and black races (22.3 vs. 17.8%, p < 0.001) more than other races. According to the Office of Juvenile Justice and Delinquency Prevention data, 89% of minor offenders charged with murder and non-negligent manslaughter are male subjects; 47% of them are white; and 50% are black (18).
Homicidal behavior is well-known to be more prevalent in male subjects. We also want to highlight that female subjects in our study were more likely to present with HI compared to the real-world criminal statistic results. Previous studies explained our findings with evidence that female homicide offenders are more likely to have a diagnosis of mental illness (19). With a higher prevalence of mental illness, they are more likely to be hospitalized and thus included in our study.
Higher prevalence of HI in white adolescents may result from racial/ethnic disparity in health services. White adolescents are more likely to be recognized with HI because healthcare is more approachable. The racial demographic data in adolescents with HI are also comparable to adolescent suicidality. More white adolescents endorsed SI, while more black adolescents attempted suicide (20). Black adolescents had a higher rate of suicide attempts compared to their white counterparts. The ideation-to-action model of suicidal behavior could possibly explain this phenomenon (21). We assume that the same model could be applied to homicidal behavior. Not every aggression consequently develops into homicidal ideation. Repetitive exposure to trauma and violence cause habituation of aggression which later could escalate into homicidal ideation. Black adolescents are more likely to experience inequitable sociopolitical contexts (e.g., police hostility) and microsystem (e.g., unsafe neighborhoods). Due to the increased psychosocial burden, the incubation period for aggression to escalate might be shorter and thus less likely to be detected. Hispanic adolescents with HI might be underdiagnosed due to similar reasons (22). Previous studies showed that black people are more likely to be both the offender and victim of homicide/assault (23). The necessity of self-defense and the violent drive from the fear of being killed should also be taken into consideration.
Although we could not obtain the exact family social economic status of our patient population, our data showed that patients with HI were more likely to be covered by public insurance (Medicare or Medicaid) with a lower household income. The insurance type and income could at least provide a glimpse of the undesirable financial environment in certain patient populations. Low social economic status indicates stressful life situations, higher rate of behavior issues, and psychopathology (24, 25). Adolescents from a household struggling financially are also more likely to be a victim of bully (26). Adverse childhood events including school bullying are significantly related to the development of HI (27–29).
Neuroimaging shows that depressive symptoms and impulsivity in children and adolescents share common features, including reduced cortical thickness in the ventromedial prefrontal cortex and medial orbitofrontal cortex. Moreover, impulsivity is specifically associated with reduced cortical thickness in the lateral prefrontal region and frontal pole (30). Children and adolescents with bipolar disorder and aggressive behavior also have cortical thinning in prefrontal and parietal cortices (31). Additionally, depression, bipolar, anxiety, and aggression shared many common physiological characteristics including dysregulated hypothalamic–pituitary–adrenal (HPA) axis, abnormal serotonin system, and chronic inflammation (32–34).
Anxiety increases indirect aggression like anger and hostility, also physical aggression in the context of high impulsivity in adolescents (35, 36). As a part of early programming for humans to survive an aversive situation, anxiety is associated with a fight and flight response and thereby coexists with aggression as an adaptive reaction toward threats in nature. Anxiety and aggression have multiple overlapping brain pathways involving the HPA axis, arginine vasopressin, gamma-aminobutyric acid, testosterone, and serotonin (37). The fact that admitting anxiolytics decreases aggression also supports the anxiety-aggression correlation (38). These evidence explained the higher prevalence of anxiety in adolescents with HI.
Attention-deficit/hyperactivity disorder and conduct disorder were associated with homicidal ideation, so as personality disorders (39). Not every ADHD child endorsed the tendency of violence. However, ADHD was known to be related to impulsive and risky decision making (40). Conduct disorder is a strong predictor of antisocial personality disorder later in life, while both are related to increased risk of HI and being an offender of homicidal events (10, 41).
Previous studies showed increased HI in patients with personality disorders which include antisocial personality disorder, borderline personality disorder, paranoid personality disorder, obsessive-compulsive personality disorder, and avoidant personality disorder (41). Among all the personality disorders, the literature review showed a significant correlation between antisocial personality disorder and HI (41–43). We did not find personality disorders as a strong predictor of HI in the adolescent population, which might be a result of underdiagnosis. Considering the similarity of certain personality features and normal adolescent behavior, mental health professionals tend not to diagnose personality in adolescents (44). Another reason for clinicians to avoid diagnosing adolescents with personality disorders is to avoid stigmatizing patients with a long-lasting, treatment-resistant condition (44, 45).
We found that HI was commonly present with SI, which was also seen in previous studies. The co-occurrence of HI and SI may be explained by the pathophysiology shared by depression, bipolar, and anxiety. It could also be illustrated from a psychoanalytic standpoint. According to Karl Menninger, there are three wishes binding together to push a person to suicide: the wish to kill, the wish to be killed, and the wish to die (46). Thus, we can postulate that there is a relationship between SI and HI.
The projective-introjective cycling of aggressive impulse is another explanation of HI accompanied by a suicidal wish (47). Children’s and adolescents’ concept of self is not completely formed. Thus, they are more likely to experience blurring boundaries of self and others, especially with those raised by abusive parents (47). While experiencing chronic stress and emotional suffering, they would have difficulty attributing the psychological content. The direction of aggression thereby vacillates between self and others. In other words, they become alternatively suicidal and homicidal (48).
A recent study on juvenile delinquents showed that suicidal ideation was correlated with certain features in psychopathy: carefree non-planfulness, blame externalization, and rebellious non-conformity (49). Thereby, sharing similar behavioral and lifestyle features of psychopathy might explain the co-occurrence of HI and SI.
A limitation of our study lies in the fact that we only include the inpatient population. Besides depression and anxiety, homicidal ideation is also prevalent in adolescents with an autism spectrum disorder (50). While most patients with autism spectrum disorders are more likely to be managed outpatient, they might be excluded from our study. Adolescents with mild personality traits who are predisposed to HI are even less likely to be assessed in an inpatient medical setting.
Some other limitations are derived from the nature of our database. The ICD coding system was established mainly for billing purposes. Thus, the ICD codes may not truly reflect patients’ overall situation. It is also not possible for us to see the severity of HI and its context. Additionally, the NISD did not provide vital information that would significantly affect adolescents’ mental health, such as family history, attachment style, early-childhood experience, history of emotional/physical/sexual abuse, or neglect. Last but not least, our result only demonstrated the propensity of correlation between HI and diagnoses but not the causality.
Our study provides updated demographic data of adolescents with HI in an inpatient setting: male subjects, the white race was more prevalent in the homicidal group. We also found a higher prevalence of psychiatric illnesses such as depression, anxiety, and bipolar disorder in adolescents with HI. Our result is also consistent with previous findings that HI is highly comorbid with SI. Further large-scale longitudinal research studies are warranted to establish the correlation between psychiatric disorders and homicidal ideation among adolescents.
Publicly available datasets were analyzed in this study. This data can be found here: https://www.hcup-us.ahrq.gov/.
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with national legislation and institutional requirements.
AR, ZM, and CT contributed to the idea, writing, editing, and reviewing of the manuscript. C-FS and RV contributed to the writing, editing, and reviewing of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Juvenile Court Statistics 2019. Office of Justice Programs. (n.d.). Available online at: https://www.ojp.gov/library/publications/juvenile-court-statistics-2019 (accessed October 29, 2022).
2. U.S. Department of Justice, Federal Bureau of Investigation, Criminal Justice Information Service Division. Expanded Homicide Data Table 3: Murder Offenders by Age, Sex, Race, and Ethnicity, 2019. Uniform Crime Reporting (UCR) Program. Washington, D.C: Federal Bureau of Investigation (2019).
3. Sorenson SB, Manz JG, Berk RA. News media coverage and the epidemiology of homicide. Am J Public Health. (1998) 88:1510–4. doi: 10.2105/AJPH.88.10.1510
4. Predicting and preventing homicide. A cost-effective empirical approach from infancy to adulthood. Preface. Psychol Rep. (2009) 104:5–7.
5. Blakemore SJ, Robbins TW. Decision-making in the adolescent brain. Nat Neurosci. (2012) 15:1184–91. doi: 10.1038/nn.3177
6. Casey BJ, Heller AS, Gee DG, Cohen AO. Development of the emotional brain. Neurosci Lett. (2019) 693:29–34. doi: 10.1016/j.neulet.2017.11.055
7. Cohen AO, Bonnie RJ, Tt Kim, Casey BJ. When does a juvenile become an adult: implications for law and policy. Temp L Rev. (2015) 88:769.
8. Teigen A. Juvenile Age of Jurisdiction and Transfer to Adult Court Laws. Washington, D.C: National Conference of State Legislatures (NCSL) (2021).
9. Kempf-Leonard K, Tracy PE, Howell JC. Serious, violent, and chronic juvenile offenders: the relationship of delinquency career types to adult criminality. Just Q. (2001) 18:449–78. doi: 10.1080/07418820100094981
10. DeLisi M, Tahja K, Drury AJ, Caropreso D, Elbert M, Heinrichs T. The criminology of homicidal ideation: associations with criminal careers and psychopathology among federal correctional clients. Am J Crim Just. (2017) 42:554–73. doi: 10.1007/s12103-016-9371-5
11. American Civil Liberties Union. Cops and No Counselors. (n.d.). Available online at: https://www.aclu.org/report/cops-and-no-counselors (accessed October 30, 2022).
12. Vaughn MG, Carbone J, DeLisi M, Holzer KJ. Homicidal ideation among children and adolescents: evidence from the 2012-2016 Nationwide emergency department sample. J Pediatr. (2020) 219:216–22. doi: 10.1016/j.jpeds.2019.12.045
13. Underwood LA, Washington A. Mental illness and juvenile offenders. Int J Environ Res Public Health. (2016) 13:228. doi: 10.3390/ijerph13020228
14. Cavaiola AA, Schiff M. Behavioral sequelae of physical and/or sexual abuse in adolescents. Child Abuse Negl. (1988) 12:181–8. doi: 10.1016/0145-2134(88)90026-9
15. Su P-Y, Han AZ, Wang GF, Wang LH, Zhang GB, Xu N, et al. Is childhood maltreatment associated with murderous ideation and behaviors in adolescents in China? Psychiatry Res. (2018) 270:467–73. doi: 10.1016/j.psychres.2018.10.024
16. Myers WC, Kemph JP. Characteristics and treatment of four homicidal adolescents. J Am Acad Child Adolesc Psychiatry. (1988) 27:595–9. doi: 10.1097/00004583-198809000-00013
17. Harter S, Low SM, Whitesell NR. What have we learned from Columbine: the impact of the self-system on suicidal and violent ideation among adolescents. J School Viol. (2003) 2:3–26. doi: 10.1300/J202v02n03_02
19. Hachtel H, Nixon M, Bennett D, Mullen P, Ogloff J. Motives, offending behavior, and gender differences in murder perpetrators with or without psychosis. J Interpers Viol. (2021) 36:3168–90. doi: 10.1177/0886260518774304
20. Child Trends. Teen Suicide. (2021). Available online at: https://www.childtrends.org/?indicators=suicidal-teens (accessed February 10, 2021).
21. Lee CS, Wong YJ. Racial/ethnic and gender differences in the antecedents of youth suicide. Cult Diver Ethnic Minor Psychol. (2020) 26:532. doi: 10.1037/cdp0000326
22. Brenes F. Hispanics, mental health, and suicide: brief report. Hispanic Health Care Int. (2019) 17:133–6. doi: 10.1177/1540415319843072
23. Willis S, Dongarwar D, Atkinson J, Taylor J, Lockett D, Williams E, et al. Comparing homicidal ideations with homicides/assaults victimization among various racial/ethnic groups in the United States. Int J Trans Med Res Public Health. (2021) 5:160–72. doi: 10.21106/ijtmrph.334
24. Peverill M, Dirks MA, Narvaja T, Herts KL, Comer JS, McLaughlin KA, et al. Socioeconomic status and child psychopathology in the United States: a meta-analysis of population-based studies. Clin Psychol Rev. (2021) 83:101933. doi: 10.1016/j.cpr.2020.101933
25. Reiss F, Meyrose AK, Otto C, Lampert T, Klasen F, Ravens-Sieberer U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: results of the German BELLA cohort-study. PLoS One. (2019) 14:e0213700. doi: 10.1371/journal.pone.0213700
26. Hosozawa M, Bann D, Fink E, Elsden E, Baba S, Iso H, et al. Bullying victimisation in adolescence: prevalence and inequalities by gender, socioeconomic status and academic performance across 71 countries. EClinicalMedicine. (2021) 41:101142. doi: 10.1016/j.eclinm.2021.101142
27. Heirigs MH. The role of psychopathy and childhood maltreatment in homicidal ideation. J Crim Just. (2021) 74:101810. doi: 10.1016/j.jcrimjus.2021.101810
28. Yuan M-Y, Li YH, Chang JJ, Wang GF, Su PY. Suicidal and homicidal ideation among Chinese undergraduates with precollege school bullying experiences: sensitive periods and exposure trajectories. Asian J Psychiatry. (2022) 70:e103047–103047. doi: 10.1016/j.ajp.2022.103047
29. Yuan M-Y, Li YH, Chang JJ, Zhang TT, Wang GF, Su PY. Exploring the correlates of homicidal ideation in Chinese early adolescents: a network analysis. J Affect Disord. (2022) 314:241–8. doi: 10.1016/j.jad.2022.07.032
30. Merz EC, He X, Noble KG. Anxiety, depression, impulsivity, and brain structure in children and adolescents. NeuroImage Clin. (2018) 20:243–51. doi: 10.1016/j.nicl.2018.07.020
31. Simonetti A, Kurian S, Saxena J, Verrico CD, Restaino A, Di Nicola M, et al. Cortical correlates of impulsive aggressive behavior in pediatric bipolar disorder. Front Psychiatry. (2021) 12:674707. doi: 10.3389/fpsyt.2021.674707
32. Lopez-Duran NL, Olson SL, Hajal NJ, Felt BT, Vazquez DM. Hypothalamic pituitary adrenal axis functioning in reactive and proactive aggression in children. J Abnorm Child Psychol. (2009) 37:169–82. doi: 10.1007/s10802-008-9263-3
33. Pavlov KA, Chistiakov DA, Chekhonin VP. Genetic determinants of aggression and impulsivity in humans. J Appl Genet. (2012) 53:61–82. doi: 10.1007/s13353-011-0069-6
34. Fico G, Anmella G, Pacchiarotti I, Verdolini N, Sagué-Vilavella M, Corponi F, et al. The biology of aggressive behavior in bipolar disorder: a systematic review. Neurosci Biobehav Rev. (2020) 119:9–20. doi: 10.1016/j.neubiorev.2020.09.015
35. Chung JE, Song G, Kim K, Yee J, Kim JH, Lee KE, et al. Association between anxiety and aggression in adolescents: a cross-sectional study. BMC Pediatr. (2019) 19:115. doi: 10.1186/s12887-019-1479-6
36. Hatfield J, Dula CS. Impulsivity and physical aggression: examining the moderating role of anxiety. Am J Psychol. (2014) 127:233–43. doi: 10.5406/amerjpsyc.127.2.0233
37. Neumann ID, Veenema AH, Beiderbeck DI. Aggression and anxiety: social context and neurobiological links. Front Behav Neurosci. (2010) 4:12. doi: 10.3389/fnbeh.2010.00012
38. Kendrick JG, Goldman RD, Carr RR. Pharmacologic management of agitation and aggression in a pediatric emergency department - a retrospective cohort study. J Pediatr Pharmacol Ther. (2018) 23:455–9. doi: 10.5863/1551-6776-23.6.455
39. Carbone JT, Testa A, Vaughn MG, Jackson DB. Fledgling psychopathy meets social determinants of health: evidence of childhood homicidal ideation among pediatric emergency department patients. J Crim Just. (2022):101926. doi: 10.1016/j.jcrimjus.2022.101926
40. Dekkers TJ, de Water E, Scheres A. Impulsive and risky decision-making in adolescents with attention-deficit/hyperactivity disorder (ADHD): the need for a developmental perspective. Curr Opin Psychol. (2022) 44:330–6. doi: 10.1016/j.copsyc.2021.11.002
41. Carbone JT, Holzer KJ, Vaughn MG, DeLisi M. Homicidal ideation and forensic psychopathology: evidence from the 2016 Nationwide emergency department sample (n.d.). J Forens Sci. (2020) 65:154–9. doi: 10.1111/1556-4029.14156
42. Nichita EC, Buckley PF. Comorbidities of antisocial personality disorder: prevalence and implications. In: Felthous AR, Saß H editors. The Wiley International Handbook on Psychopathic Disorders and the Law. Hoboken, NJ: John Wiley & Sons Ltd (2020). p. 645–70. doi: 10.1002/9781119159322.ch28
43. Lindberg N, Lindberg N, Laajasalo T, Holi M, Putkonen H, Weizmann-Henelius G, et al. Psychopathic traits and offender characteristics–a nationwide consecutive sample of homicidal male adolescents. BMC Psychiatry. (2009) 9:18. doi: 10.1186/1471-244X-9-18
44. Sharp C, Vanwoerden S, Wall K. Adolescence as a sensitive period for the development of personality disorder. Psychiatr Clin. (2018) 41:669–83. doi: 10.1016/j.psc.2018.07.004
45. Laurenssen EM, Hutsebaut J, Feenstra DJ, Van Busschbach JJ, Luyten P. Diagnosis of personality disorders in adolescents: a study among psychologists. Child Adolesc Psychiatry Ment Health. (2013) 7:1–4. doi: 10.1186/1753-2000-7-3
46. Ronningstam E, Weinberg I, Maltsberger JT. Psychoanalytic theories of suicide. In: Wasserman D, Wasserman C editors. Oxford Textbook of Suicidology and Suicide Prevention. Oxford: OUP Oxford (2020). 147 p. doi: 10.1093/med/9780198834441.003.0020
47. Dutton DG, Yamini S. Adolescent parricide: an integration of social cognitive theory and clinical views of projective-introjective cycling. Am J Orthopsychiatry. (1995) 65:39–47. doi: 10.1037/h0079594
49. Heirigs MH, Heirigs MH, DeLisi M, Fox B, Dhingra K, Vaughn MG. Psychopathy and suicidal thoughts and behaviors revisited: results from a statewide population of institutionalized youth. Int J Offend Ther Comp Criminol. (2019) 63:874–95. doi: 10.1177/0306624X18812533
Keywords: homicide, psychiatric comorbidity, adolescents, depression, bipolar disorder, anxiety
Citation: Sun C-F, Mansuri Z, Trivedi C, Vadukapuram R and Reddy A (2022) Homicidal ideation and psychiatric comorbidities in the inpatient adolescents aged 12–17. Front. Psychiatry 13:933524. doi: 10.3389/fpsyt.2022.933524
Received: 01 May 2022; Accepted: 10 October 2022;
Published: 16 November 2022.
Edited by:
Yezhe Lin, Virginia Tech Carilion, United StatesReviewed by:
Yamin Zhang, Sichuan University, ChinaCopyright © 2022 Sun, Mansuri, Trivedi, Vadukapuram and Reddy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zeeshan Mansuri, WmVlc2hhbk1hbnN1cmlAZ21haWwuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.