
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 15 July 2022
Sec. Anxiety and Stress Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.931349
This article is part of the Research Topic Assessing and Evaluating the Impact Of The Covid 19 Pandemic on Anxiety And Stress: A Global Perspective View all 16 articles
 Knut Stavem1,2,3*
Knut Stavem1,2,3* Trond Heir2,4
Trond Heir2,4 Toril Dammen2,5
Toril Dammen2,5 Eivind Brønstad6,7Tøri Vigeland Lerum2,8Michael T. Durheim2,9Kristine M. A. Lund10Bernt B. Aarli11,12
Eivind Brønstad6,7Tøri Vigeland Lerum2,8Michael T. Durheim2,9Kristine M. A. Lund10Bernt B. Aarli11,12 Gunnar Einvik1,2
Gunnar Einvik1,2Objective: To assess the trajectory of symptoms and symptom-defined post-traumatic stress disorder (PTSD) from 1.5 to 12 months after hospitalization for COVID-19 and determine risk factors for persistent symptoms and PTSD.
Methods: This was a prospective cohort study of consecutive patients discharged after hospitalization for COVID-19 before 1 June 2020 in six hospitals in Southern Norway. Symptom-defined PTSD was assessed by the post-traumatic stress disorder (PTSD) checklist for DSM-5 (PCL-5) at 1.5, 3 and/or 12 months after hospitalization, using DSM-5 criteria. Changes in PCL-5 symptom score and the prevalence of PTSD were analyzed with multivariable mixed models.
Results: In total, 388 patients were discharged alive, and 251 (65%) participated. Respondents had a mean (SD) age of 58.4 (14.2) years, and 142 (57%) were males. The prevalence of symptom-defined PTSD was 14, 8, and 9% at 1.5, 3, and 12 months, respectively. WHO disease severity for COVID-19 was not associated with PCL-5 scores. Female sex, lower age and non-Norwegian origin were associated with higher PCL-5 scores. The odds ratio (OR) (95%CI) for PTSD was 0.32 (0.12 to 0.83, p = 0.019) at 3 months and 0.38 (0.15 to 0.95, p = 0.039) at 12 months compared to 1.5 months. There was no association between PTSD and WHO severity rating.
Conclusions: The level of PTSD symptoms decreased from 1.5 to 3 months after hospitalization, but did not decrease further to 12 months, and there was no association between PTSD symptoms and COVID-19 disease severity.
Post-traumatic stress disorder (PTSD) is a chronic and debilitating mental condition that may develop in response to traumatic events that involve a life-threatening component, including acute medical diseases. A meta-analysis reported that 17–44% of critical illness survivors reported clinically important PTSD symptoms, and that symptoms of PTSD were associated with pre-ICU psychopathology, but not with age, disease severity, or ICU length of stay (1).
During the severe acute respiratory syndrome (SARS) outbreak in 2002–2004, many recovered SARS patients showed symptoms of PTSD at 1 and 3 months after discharge from hospital, and 4–5% satisfied the criteria for PTSD (2), although higher rates have been reported (3). Furthermore, the level of hypoxia is associated with PTSD symptoms (2). The prevalence of PTSD 12 months after hospitalization for the Middle East respiratory syndrome (MERS) were even higher, with 24% reporting severe or very severe PTSD (4).
Patients hospitalized for COVID-19 are characterized by fever, cough, dyspnea, chest pain, or confusion, and typically 10–20% of hospitalized patients have critical illness requiring care in the intensive unit (5, 6). Until June 2022, cumulatively 15.8% of patients hospitalized for COVID-19 in Norway required ICU care (7).
Recent studies have reported significant PTSD symptoms during and after hospitalization for COVID-19 among 2–40 % of patients with follow-up of 1–6 months, and just recently 12–15 months, in cross-sectional or cohort studies (8–20). Prevalence rates vary according to time after acute COVID-19, assessment method, sample selection, and geographical region. During follow-up, female sex and continued symptoms, but not age or disease severity, were associated with PTSD (20).
To understand the course of stress reactions, repeated measurements of PTSD symptoms during the convalescence of COVID-19 and longer observation times are necessary (9, 17). This study investigated the course of symptoms of PTSD over 12 months after COVID-19 onset, focusing on the change in symptoms and possible association with disease severity.
This was a multicenter study, inviting patients 2–6 weeks after discharge from six major hospitals in Norway after COVID-19, before 1 June 2020. All patients >18 years of age with a discharge diagnosis (International Statistical Classification of Diseases and Related Health Problems 10) of U07.1, U07.2, or J12.x were eligible. Among all 454 survivors, we excluded 15 patients living outside the hospitals' catchment areas, 13 unable to provide informed consent, and 38 participating in a conflicting COVID-19 treatment trial. In total, 251 (65%) of 388 eligible patients provided data for this study.
The Regional Committee for Medical and Health Research Ethics, Health Region South East (no. 2020/125384) and data protection officers at participating centers approved the study. Written informed consent was obtained by mail or a secure web-form. The study is registered with ClinicalTrials.gov (NCT04535154).
As this was an observational study, clinical treatment was up to each hospital. However, during the study follow-up visits, we used a standard protocol.
Data were collected at four time points: (i) Previous medical history and data during COVID-19 hospitalization were extracted from the electronic medical records (EMR); (ii) about 1.5 month after hospitalization, participants responded to a paper or on-line questionnaire; all participants returned to the respective hospitals' outpatient clinics for a visit, including self-completed questionnaires at (iii) 3 and (iv) 12 months after hospitalization.
Basic demographics, symptoms, Charlson's comorbidity index (21), and severity of COVID-19 were extracted from the EMR by study physicians/nurses. COVID-19 severity was classified using a WHO ordinal severity score (22): 3 no oxygen supplementation, 4 oxygen supplementation, 5 high-flow oxygen or non-invasive ventilation, or 6–7 mechanical ventilation. We obtained supplementary information on socio-demographics, height, weight, and smoking history by self-report at the 3-month visit.
Symptoms of PTSD were assessed using a Norwegian version of the PCL-5 (PTSD Checklist for DSM-5) questionnaire (23). The PCL-5 contains 20 items on an ordinal scale (0 to 4), which are summed to a total score (range 0–80, with 80 denoting maximal symptoms). The PCL-5 also has an alternative scoring algorithm fitted to the five clusters of the DSM-5 PTSD criteria (24). We used the DSM-5 criteria scoring to define symptom-defined PTSD.
We analyzed data from respondents with at least one response to PCL-5 (n = 251). Descriptive statistics are presented as mean (SD), median (25th to 75th percentile) or number (%). We present PTSD symptoms as continuous scores on the PCL-5 total scale and the prevalence of PTSD using DSM-5 scoring.
We conducted longitudinal analyses using mixed models, thereby accounting for missing values and enabling us to use all available data. For PCL-5 total scores, we used a linear mixed model with random effect (intercept) at the patient level, and an unstructured covariance structure. The model was fitted using maximum likelihood. Because the distribution of PCL-5 total score was highly skewed with many subjects having a score of 0, we tried log and square-root transformations of the PCL-5 total scores. However, this did not improve the distribution of the residuals or the model fit. Therefore, we used untransformed values as the dependent variable and bootstrapping with 10,000 iterations to estimate 95% confidence intervals and p-values. We included independent variables selected a priori: occasion (1.5, 3, or 12 months), age (per year), sex (male vs. female), living alone (married/cohabiting vs. single/divorced/widowed), born in Norway (yes vs. no), education (university level vs. lower level), Charlson comorbidity score (0, 1, ≥2), and WHO ordinal severity score (3, 4, 5–7).
Adding a random effect at the hospital level to the model only marginally influenced the coefficients and did not alter the results. The intraclass correlation coefficient (ICC) at the hospital level was only 0.029 compared to 0.657 at the patient level. Therefore, we omitted the hospital level in further analysis. In a supplementary analysis, we repeated the linear mixed models for PCL-5 total scores with the same approach and the same variables.
PTSD was analyzed using a logistic mixed model, with random effect (intercept) at the patient level, and an unstructured covariance structure. Here we only used occasion (1.5, 3, or 12 months) and WHO ordinal severity score as covariates, because of the low number of events.
We used Stata version 17.0 (Stata Corporation, College Station, TX) or R (The R Foundation for Statistical Computing) for all statistical analyses. We chose a 5% significance level.
The participants had a mean age of 58.4 years, range 16.6 to 91.3 years. Overall, 35/142 men (25%) and 13/109 women (12%) had been admitted to the ICU. Further demographic and clinical characteristics of the participants are shown in Table 1.
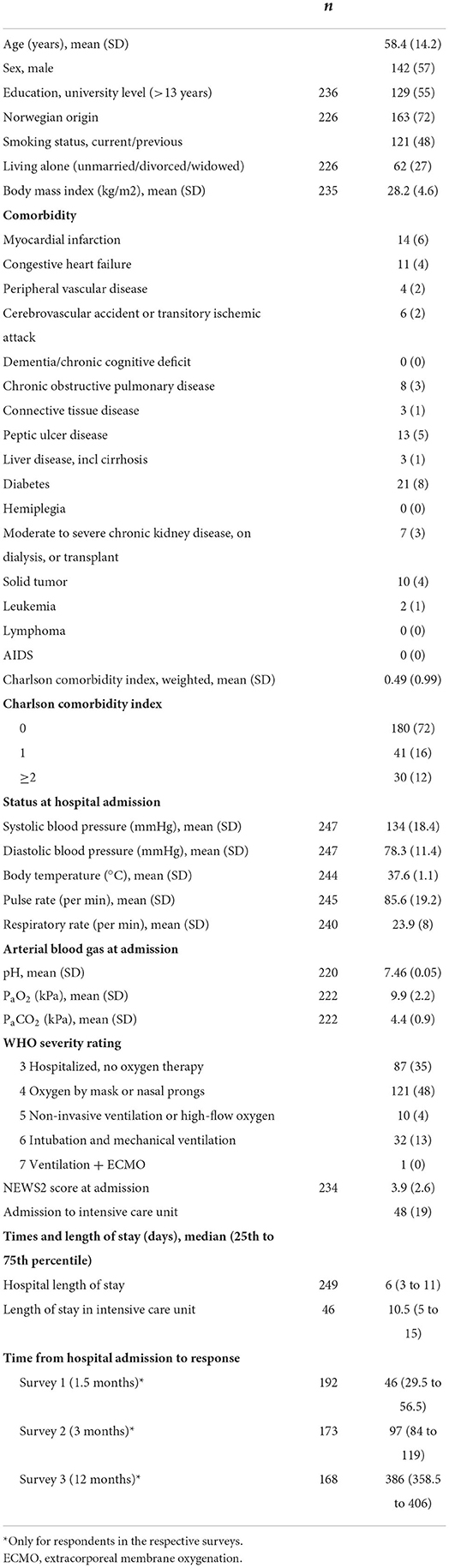
Table 1. Descriptive statistics for respondents (N = 251), number (%) unless otherwise stated.
The mean (SD) PCL-5 total scores were 14.2 (14.2), 11.2 (12.9), and 10.4 (12.4) at 1.5, 3, and 12 months, respectively. Symptom-defined PTSD was present in 27 (14%), 18 (8%), and 19 (9%) of the patients at the same time points, but there was no association with disease severity (Figure 1).
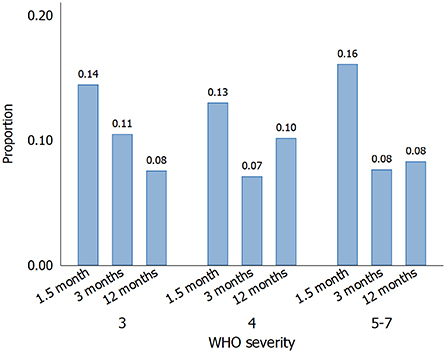
Figure 1. Proportions of hospitalized COVID-19 patients with symptom-defined PTSD (DSM-5 scoring) over time, according to WHO disease severity: 3, no oxygen requirement (n = 87); 4, oxygen by mask or nasal prongs (n = 121); 5–7, high-flow oxygen, non-invasive ventilation or intubation/mechanical ventilation (n = 43).
In multivariable analysis of continuous PCL-5 scores, 3-month and 12-month scores were lower than 1.5-month scores, but there was no association with COVID-19 severity (Table 2, Figure 2). However, female gender, non-Norwegian origin, and lower age were associated with increased PCL-5 total scores.
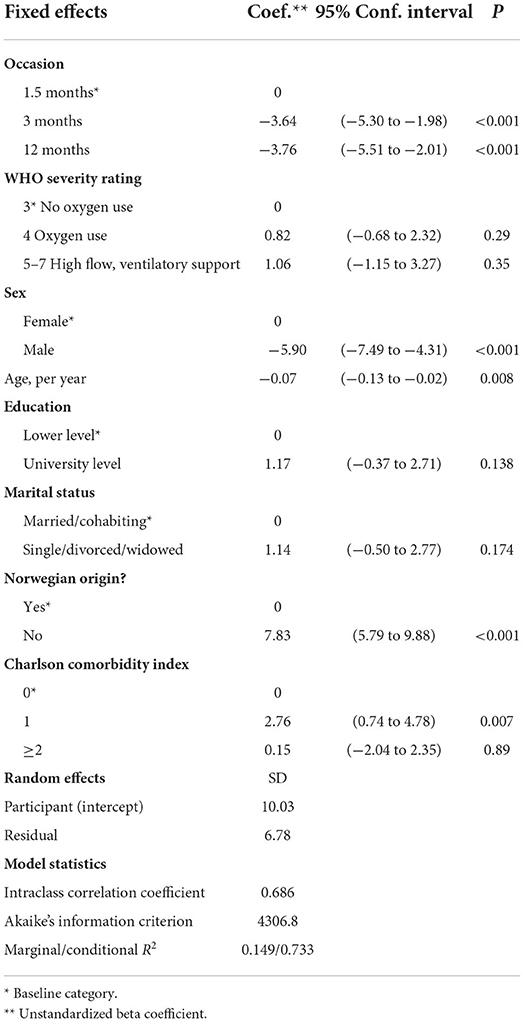
Table 2. Predictors of PCL-5 total symptom score, multivariable linear mixed model (n =565 observations, 225 patients).
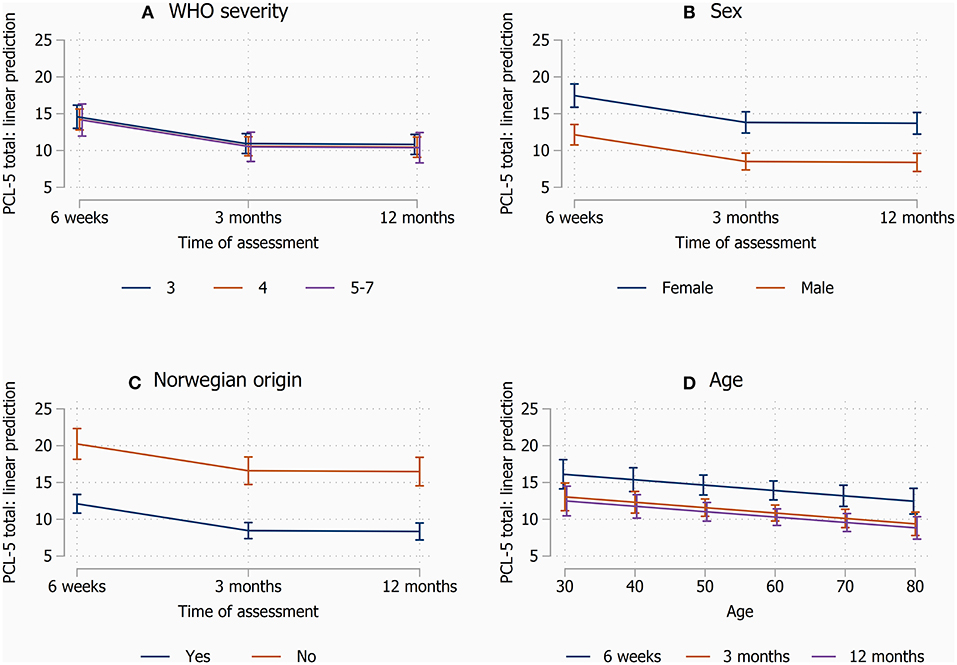
Figure 2. Margin plots from the linear mixed models, illutrating the effects of covariates on estimated PCL-5 scores over time. (A) WHO ordinal disease severity, (B) sex, (C) Norwegian origin, and (D) age. Other covariates than those shown were kept at mean values.
Stratified analysis according to sex, showed a similar development in PTSD symptoms over time for men and women, and more PTSD symptoms with non-Norwegian origin (Supplementary Table 1). However, the results for educational level seemed inconsistent, with more symptoms with higher education among women, but less symptoms with higher education among men. Being single/divorced was associated with more symptoms only among men. Finally, the association for Charlson comorbidity index was different for men and women, with score ≥2 being associated with less PTSD symptoms only among men.
The multivariable logistic model (n = 618 observations, 221 patients) showed odds ratios (OR) (95%CI) for PTSD of 0.32 (0.12 to 0.83, p = 0.019) at 3 months and 0.38 (0.15 to 0.95, p = 0.039) at 12 months compared to 1.5 months, and 0.93 (0.26 to 3.29) for WHO severity rating 4 and 1.01 (0.19 to 5.38) for severity 5–7 compared to severity 3, respectively. ICC was 0.745.
This study has shown a prevalence of PTSD of 14% at 1.5 months, declining to 8–9% after 3–12 months. Furthermore, there was no association between the severity of acute COVID-19 and PTSD symptoms or prevalence at follow-up.
The prevalence of PTSD in this study was in line with studies with similar populations 2–12 months after hospitalization for COVID-19 (10, 11, 13–17), but lower than in some populations with more severe disease (8, 12, 18, 25). However, rates of PTSD disorders following COVID-19 as low as 3.8% has been reported in combined hospitalized/non-hospitalized samples (26).
The differences in prevalence of PTSD between our study and some other studies may possibly be explained by the use of different assessment methods, or populations.
The present study recruited a large proportion of all hospitalized patients in strict geographical catchment areas and may therefore be less affected by selection bias, e.g., healthy non-participant bias in studies recruiting based on lasting symptoms. This, and some other studies (11, 13, 15–17), may therefore be more representative of all hospitalized patients.
Symptoms of PTSD improved from 1.5 to 3 months, in line with reports from some studies from 1 to 2, or 1 to 3 months (17, 27–29), but not in others (30). There is less information on change in PTSD symptoms over as long as 12 months. One study reported the presence of moderate PTSD symptoms in 12% and severe in 6.5% 12 months after hospitalization, and these rates were unchanged from 4 months after hospitalization (16), as from 3 to 12 months in the present study. In contrast, studies have reported an increase in PTSD symptoms scores from 3 to 6 months after hospitalization (31), or from baseline to follow-up after 24–60 weeks in subjects recruited from advertisements or referrals in the community (32). Recently Mazza et al. reported a reduction in PTSD symptoms over time from 1 month to 12 months, although the change from 6 to 12 months seemed to be small (18).
In the present study we found no significant association between the severity of COVID-19 during hospitalization, i.e., graded requirement for oxygen treatment, and the total score of PCL-5 during the follow-up. This, however, supports previous reports of no association between disease severity and adverse mental outcomes in COVID-19 (20).
In contrast, female sex was associated with higher symptom score, in line with findings in other studies (20) and PTSD in general (33). It is possible that young people are less prepared for being affected by acute severe illness (34), and that birth place outside Norway may be related to higher probability of previous PTSD, lower confidence in authorities or information given, or language difficulties.
A Charlson comorbidity index of 1, but not of ≥ 2, was associated with PCL-5 scores, which was most marked in the analysis in males. We do not have a good explanation for this. It could be by chance, content of the medical records, or coding issues. Some of the comorbidities might also be more important in this context, than what is reflected in the weights in this index. In the stratified analysis, this inconsistency was present only among men, who constituted 57% of the sample, and an even larger percentage of those with severe disease requiring ICU admission. In the stratified analyses, the statistical power was smaller, in particular among women, which limits conclusions to be made.
Strengths of the study are the prospective design with multiple assessments, inclusion of several large centers covering approximately 50% of the Norwegian population, and the long follow-up. The use of questionnaires and symptom-defined PTSD, instead of diagnostic interviews for assessment of PTSD represents a limitation, as in most other studies. The response rate among participants was not optimal, and may have caused a bias, and the number of patients with severe disease was small, reducing the statistical power. We did not register whether PTSD was present prior to COVID-19. However, the PCL-5 items were specifically linked to the infectious disease.
In this study the prevalence of PTSD was low. There was an early improvement in symptoms of PTSD, but no further improvement beyond 3 months. In general, about half of PTSD cases remit within 6 months, and the probability of remission does not vary much across exposure types (35). A similar remission rate of PTSD symptoms over a much shorter time period in our study suggests that COVID-19 PTSD may have a better prognosis than PTSD from most other causes.
In conclusion, the symptom load of PTSD declined from 1.5 to 3 months, with no further decline from 3 to 12 months. Symptoms of PTSD were not associated with COVID-19 severity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Regional Committee for Medical and Health Research Ethics, Health Region South East. The patients/participants provided their written informed consent to participate in this study.
GE and KS conceived and designed the study, with assistance from TD and TH. EB, TL, MD, KL, and BA contributed to data collection. KS, GE, and TH conducted data analysis. KS, GE, TH, and TD contributed to interpretation of the data. KS, GE, TD, TH, EB, TL, MD, KL, and BA critically reviewed and commented on the paper. All authors approved the final version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.931349/full#supplementary-material
1. Parker AM, Sricharoenchai T, Raparla S, Schneck KW, Bienvenu OJ, Needham DM. Post-traumatic stress disorder in critical illness survivors: a meta analysis. Crit Care Med. (2015) 43:1121–9. doi: 10.1097/CCM.0000000000000882
2. Wu KK, Chan SK, Ma TM. Post-traumatic stress after SARS. Emerg Infect Dis. (2005) 11:1297–300. doi: 10.3201/eid1108.041083
3. Ahmed H, Patel K, Greenwood DC, Halpin S, Lewthwaite P, Salawu A, et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalization or ICU admission: a systematic review and meta-analysis. J Rehabil Med. (2020) 52:jrm00063. doi: 10.2340/16501977-2694
4. Park HY, Park WB, Lee SH, Kim JL, Lee JJ, Lee H, et al. Posttraumatic stress disorder and depression of survivors 12 months after the outbreak of Middle East respiratory syndrome in South Korea. BMC Public Health. (2020) 20:605. doi: 10.1186/s12889-020-08726-1
5. Guan WJ Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
6. Docherty AB, Harrison EM, Green CA, Hardwick HE, Pius R, Norman L, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO clinical characterization protocol: prospective observational cohort study. BMJ. (2020) 369:m1985. doi: 10.1136/bmj.m1985
7. Folkehelseinstituttet. COVID-19, influensa og andre luftveisinfeksjoner. Rapport – uke 21 og 22, onsdag 8. juni 2022: FHI; 2022 [updated 08.06.2022]. Available online at: https://www.fhi.no/contentassets/8a971e7b0a3c4a06bdbf381ab52e6157/vedlegg/2022/ukerapport-for-uke-21-og-22-30.05-−05.06.22.pdf
8. Janiri D, Carfi A, Kotzalidis GD, Bernabei R, Landi F, Sani G, et al. Post-traumatic stress disorder in patients after severe COVID-19 infection. JAMA Psychiatry. (2021) 78:567–9. doi: 10.1001/jamapsychiatry.2021.0109
9. Nagarajan R, Krishnamoorthy Y, Basavarachar V, Dakshinamoorthy R. Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: a systematic review and meta-analysis. J Affect Disord. (2021) 299:52–9. doi: 10.1016/j.jad.2021.11.040
10. Rass V, Ianosi BA, Zamarian L, Beer R, Sahanic S, Lindner A, et al. Factors associated with impaired quality of life three months after being diagnosed with COVID-19. Qual Life Res. (2021) 3:1–4. doi: 10.1007/s11136-021-02998-9
11. Tarsitani L, Vassalini P, Koukopoulos A, Borrazzo C, Alessi F, Di Nicolantonio C, et al. Post-traumatic stress disorder among COVID-19 survivors at 3-month follow-up after hospital discharge. J Gen Intern Med. (2021) 36:1702–7. doi: 10.1007/s11606-021-06731-7
12. Writing Committee for the CSG Morin L Savale L Pham T Colle R Figueiredo S . 4-month clinical status of a cohort of patients after hospitalization for COVID-19. JAMA. (2021) 325:1525-34. doi: 10.1001/jama.2021.3331
13. Naidu SB, Shah AJ, Saigal A, Smith C, Brill SE, Goldring J, et al. The high mental health burden of “Long COVID” and its association with on-going physical and respiratory symptoms in all adults discharged from hospital. Eur Respir J. (2021) 57:2020. doi: 10.1183/13993003.04364-2020
14. Einvik G, Dammen T, Ghanima W, Heir T, Stavem K. Prevalence and risk factors for post-traumatic stress in hospitalized and non-hospitalized COVID-19 patients. Int J Environ Res Public Health. (2021) 18:2079. doi: 10.3390/ijerph18042079
15. Simani L, Ramezani M, Darazam IA, Sagharichi M, Aalipour MA, Ghorbani F, et al. Prevalence and correlates of chronic fatigue syndrome and post-traumatic stress disorder after the outbreak of the COVID-19. J Neurovirol. (2021) 27:154–9. doi: 10.1007/s13365-021-00949-1
16. Bellan M, Baricich A, Patrucco F, Zeppegno P, Gramaglia C, Balbo PE, et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci Rep. (2021) 11:22666. doi: 10.1038/s41598-021-01215-4
17. Horn M, Wathelet M, Fovet T, Amad A, Vuotto F, Faure K, et al. Is COVID-19 associated with posttraumatic stress disorder? J Clin Psychiatry. (2020) 82:13641. doi: 10.4088/JCP.20m13641
18. Mazza MG, Palladini M, De Lorenzo R, Bravi B, Poletti S, Furlan R, et al. 1-year mental health outcomes in a cohort of COVID-19 survivors. J Psychiatr Res. (2021) 145:118–24. doi: 10.1016/j.jpsychires.2021.11.031
19. Huang X, Liu L, Eli B, Wang J, Chen Y, Liu Z. Mental Health of COVID-19 Survivors at 6 and 12 Months post-diagnosis: a cohort study. Front Psychiatry. (2022) 13:863698. doi: 10.3389/fpsyt.2022.863698
20. Sun LL, Wang J, Wang YS, Pan X, Luo J, Liu H, et al. 15-Month health outcomes and the related risk factors of hospitalized COVID-19 patients from onset: a cohort study. Front Med. (2022) 9:854788. doi: 10.3389/fmed.2022.854788
21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
22. Novel Coronavirus COVID-19 Therapeutic Trial Synopsis. Geneva, Switzerland: WHO (2020). Available online at: https://www.who.int/blueprint/priority-diseases/key-action/COVID-19_Treatment_Trial_Design_Master_Protocol_synopsis_Final_18022020.pdf
23. Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL. The post-traumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J Trauma Stress. (2015) 28:489–98. doi: 10.1002/jts.22059
24. Using the PTSD Checklist for DSM-5. Washington D.C.: National Center for PTSD, Veterans Administration (2022).
25. Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav Immun. (2020) 89:594–600. doi: 10.1016/j.bbi.2020.07.037
26. Khademi M, Vaziri-Harami R, Shams J. Prevalence of mental health problems and its associated factors among recovered COVID-19 patients during the pandemic: a single-center study. Front Psychiatry. (2021) 12:602244. doi: 10.3389/fpsyt.2021.602244
27. De Lorenzo R, Conte C, Lanzani C, Benedetti F, Roveri L, Mazza MG, et al. Residual clinical damage after COVID-19: a retrospective and prospective observational cohort study. PLoS ONe. (2020) 15:e0239570. doi: 10.1371/journal.pone.0239570
28. Mazza MG, Palladini M, De Lorenzo R, Magnaghi C, Poletti S, Furlan R, et al. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun. (2021) 94:138–47. doi: 10.1016/j.bbi.2021.02.021
29. Vlake JH, Wesselius S, van Genderen ME, van Bommel J. Boxma-de Klerk B, Wils EJ. Psychological distress and health-related quality of life in patients after hospitalization during the COVID-19 pandemic: A single-center, observational study. PLoS ONE. (2021) 16:e0255774. doi: 10.1371/journal.pone.0255774
30. De Lorenzo R, Cinel E, Cilla M, Compagnone N, Ferrante M, Falbo E, et al. Physical and psychological sequelae at three months after acute illness in COVID-19 survivors. Panminerva Med. (2021). doi: 10.23736/S0031-0808.21.04399-8
31. Tu Y, Zhang Y, Li Y, Zhao Q, Bi Y, Lu X, et al. Post-traumatic stress symptoms in COVID-19 survivors: a self-report and brain imaging follow-up study. Mol Psychiatry. (2021). doi: 10.1038/s41380-021-01223-w
32. Kyzar EJ, Purpura LJ, Shah J, Cantos A, Nordvig AS, Yin MT. Anxiety, depression, insomnia, and trauma-related symptoms following COVID-19 infection at long-term follow-up. Brain Behav Immun Health. (2021) 16:100315. doi: 10.1016/j.bbih.2021.100315
33. Schou TM, Joca S, Wegener G, Bay-Richter C. Psychiatric and neuropsychiatric sequelae of COVID-19 - A systematic review. Brain Behav Immun. (2021) 97:328–48. doi: 10.1016/j.bbi.2021.07.018
34. Varma P, Junge M, Meaklim H, Jackson ML. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: a global cross-sectional survey. Prog Neuropsychopharmacol Biol Psychiatry. (2021) 109:110236. doi: 10.1016/j.pnpbp.2020.110236
Keywords: post-traumatic stress disorder (PTSD), COVID-19, PCL-5 questionnaire, cohort, follow-up, medium-term
Citation: Stavem K, Heir T, Dammen T, Brønstad E, Lerum TV, Durheim MT, Lund KMA, Aarli BB and Einvik G (2022) The course and determinants of post-traumatic stress over 12 months after hospitalization for COVID-19. Front. Psychiatry 13:931349. doi: 10.3389/fpsyt.2022.931349
Received: 28 April 2022; Accepted: 24 June 2022;
Published: 15 July 2022.
Edited by:
Vsevolod Konstantinov, Penza State University, RussiaReviewed by:
Cleoputri Yusainy, University of Brawijaya, IndonesiaCopyright © 2022 Stavem, Heir, Dammen, Brønstad, Lerum, Durheim, Lund, Aarli and Einvik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Knut Stavem, a251dC5zdGF2ZW1AbWVkaXNpbi51aW8ubm8=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.