 Tazio Maleitzke1,2,3
Tazio Maleitzke1,2,3 Dario Zocholl4
Dario Zocholl4 Tobias Topp5
Tobias Topp5 Annika Dimitrov-Discher1Elly Daus1Gabriel Reaux1Malin Zocholl6Rolf Nicolas Conze6
Annika Dimitrov-Discher1Elly Daus1Gabriel Reaux1Malin Zocholl6Rolf Nicolas Conze6 Moritz Kolster7
Moritz Kolster7 Philipp Weber8Florian Nima Fleckenstein3,9
Philipp Weber8Florian Nima Fleckenstein3,9 Louise Scheutz Henriksen10,11Ulrich Stöckle1
Louise Scheutz Henriksen10,11Ulrich Stöckle1 Thomas Fuchs6Denis Gümbel7Nikolai Spranger7Alexander Ringk8
Thomas Fuchs6Denis Gümbel7Nikolai Spranger7Alexander Ringk8 Sven Märdian1*
Sven Märdian1*- 1Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Center for Musculoskeletal Surgery, Berlin, Germany
- 2Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Julius Wolff Institute, Berlin, Germany
- 3Berlin Institute of Health at Charité – Universitätsmedizin Berlin, BIH Biomedical Innovation Academy, BIH Charité Clinician Scientist Program, Berlin, Germany
- 4Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Institute of Biometry and Clinical Epidemiology, Berlin, Germany
- 5Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Orthopaedic, Trauma, Hand and Reconstructive Surgery, Berlin, Germany
- 6Department of Orthopaedic, Trauma, Hand and Reconstructive Surgery, Vivantes Hospital Friedrichshain, Berlin, Germany
- 7Department of Trauma and Orthopaedic Surgery, BG Klinikum Unfallkrankenhaus Berlin gGmbH, Berlin, Germany
- 8Center for Orthopaedics and Trauma Surgery, Helios Klinikum Berlin-Buch, Berlin, Germany
- 9Department of Growth and Reproduction, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 10International Centre for Research and Training in Endocrine Disruption of Male Reproduction and Child Health (EDMaRC), Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 11Department of Growth and Reproduction, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
Background: While repeated shutdown and lockdown measures helped contain the spread of SARS-CoV-2 during the COVID-19 pandemic, social distancing and self-isolation negatively impacted global mental health in 2020 and 2021. Although suicide rates did reportedly not increase during the first months of the pandemic, long-term data, and data on the quality of serious violent suicide attempts (SVSAs) are not available to date.
Materials and methods: Orthopaedic trauma patient visits to the emergency department (ED), ED trauma team activations, and SVSAs were retrospectively evaluated from January 2019 until May 2021 in four Level-I Trauma Centers in Berlin, Germany. SVSAs were assessed for suicide method, injury pattern and severity, type of treatment, and length of hospital stay.
Results: Significantly fewer orthopaedic trauma patients presented to EDs during the pandemic (n = 70,271) compared to the control (n = 84,864) period (p = 0.0017). ED trauma team activation numbers remained unchanged. SVSAs (corrected for seasonality) also remained unchanged during control (n = 138) and pandemic (n = 129) periods, and no differences were observed for suicide methods, injury patterns, or length of hospital stay.
Conclusion: Our data emphasize that a previously reported rise in psychological stress during the COVID-19 pandemic does not coincide with increased SVSA rates or changes in quality of SVSAs.
Introduction
The COVID-19 pandemic imposed an unprecedented burden on health care systems worldwide. To effectively slow down the spread of SARS-CoV-2, governmental authorities decreed lockdown and shutdown measures of various degrees and lengths during 2020 and 2021 (1). While patients suffering from COVID-19 impacted intensive care units and hospital services, individuals and communities were additionally challenged by a rise in depression, anxiety, and acute stress symptoms resulting from quarantine and social distancing measures (2). Consistent data from the U.S. and Europe demonstrated an initial deterioration in mental health during the first months of the pandemic in March and April 2020, followed by a considerable degree of recovery during June, July, and August 2020 (3–5). Whether or not alternating states of mental health and depression may have influenced harmful behavior and suicide attempts, concerned authors since the beginning of the pandemic (6, 7), especially in the light of reports on increased suicide rates during previous healthcare crises like the SARS outbreak in Hong Kong in 2003 (8, 9).
As data on suicide rates during the pandemic slowly emerged, geographic differences became apparent. For example, while suicide rates in a majority of western countries, including Germany (10), did not increase but remain stable or decrease (11), other studies reported a rise in suicide attempts and completed suicides during the first months of the pandemic in Nepal, Italy and South Korea (12–14).
Japan also reported a rise in suicide numbers during the second wave of COVID-19 infections, following an initial decline (15). Data from the U.S. further showed ethnicity-based shifts in suicide rates during the pandemic in Maryland (16) and Connecticut (17).
While nonviolent suicide attempts (poisoning or overdosing) represent the majority of index suicide attempts, violent suicide attempts (e.g., hanging, cutting or piercing, jumping from great heights) represent the majority of completed suicides (18). Violent suicide attempts are often tied to injuries of the musculoskeletal system and have a higher prevalence among men (19). They were previously linked to ambient temperatures and a lack of sunshine hours (20, 21).
While most available studies focus on the number of suicides during the COVID-19 pandemic, reports on suicide quality remain scarce. In this study, we evaluated serious violent suicide attempts (SVSAs), defined as violent suicide attempts that would have been potentially lethal had it not been for rapid and effective emergency treatment (22). SVSAs were analyzed for suicide method, injury severity, and concomitant treatment strategies during 14 months amid the COVID-19 pandemic and a preceding 14-month control period in four Level-I Trauma Centers in Berlin, Germany.
Materials and methods
Study design and setting
Context/places
This retrospective study was conducted at four medical centers that fulfill the Level-I Trauma Center criteria, defined by the American College of Surgeons (ACS) and the German Trauma Society (DGU) (23). As part of a network of five Level-I Trauma Centers in Berlin, Germany, the four participating centers provide full 24/7 in house trauma care for the German capital and its adjacent urban areas.
Patient sample and key dates
Absolute numbers for orthopaedic trauma patients, trauma team activations, and SVSAs admitted to the emergency departments (EDs) of the four participating Level-I Trauma Centers in Berlin, Germany, were retrospectively assessed. The following periods were defined as 14-month pandemic and control periods:
- January 1, 2019–February 29, 2020 (control).
- April 1, 2020–May 20, 2021 (pandemic; Figure 1).
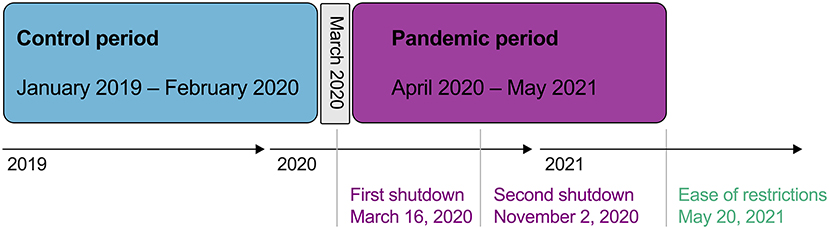
Figure 1. Longitudinal time chart of analyzed periods and COVID-19 related shutdowns implemented in Berlin, Germany during 2020 and 2021.
On March 16, 2020, the German government and the federal states announced a first temporary shutdown of public life, including schools, universities, restaurants, and bars (24). After some restrictions were lifted during the summer of 2020, a second shutdown was imposed on November 2, 2020 (25). On May 20, 2021 shutdown measures were mostly lifted in Berlin, Germany, which marks the endpoint of the pandemic period in our analyses (Figure 1). March 2020 was excluded from the analyses to allow a clear discrimination between the control and pandemic period.
Sample frame and data collection
Investigators from each center retrieved data from hospital healthcare databases [retrospective chart review employing the convenience sampling approach (26)]. First, absolute numbers for orthopaedic trauma patients, trauma team activations, and SVSAs were evaluated. Second, all SVSA cases were reviewed in detail for parameters surrounding the quality of suicide attempts (Table 1). All patients were followed up until they were discharged from hospital or deceased.
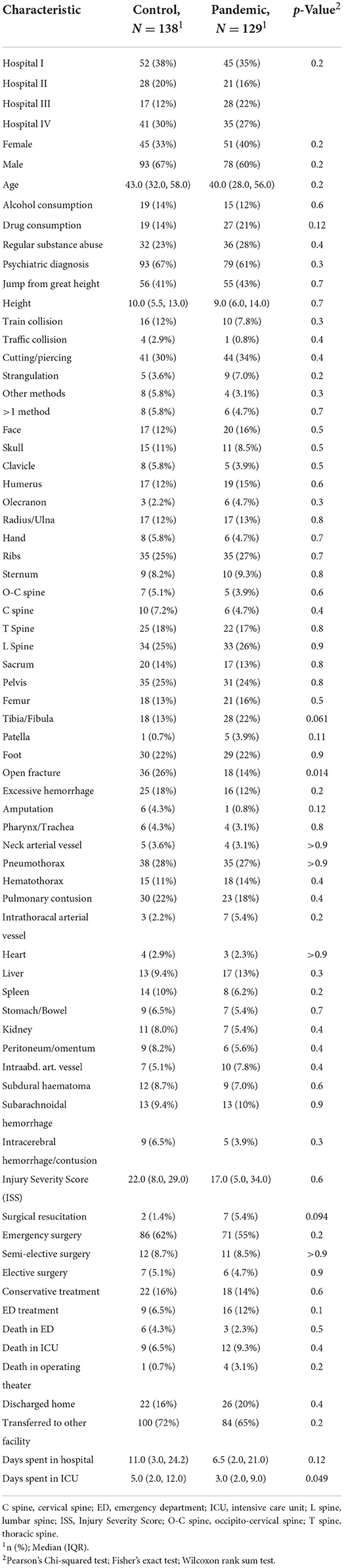
Table 1. Characteristics of patients who committed serious violent suicide attempts (SVSAs) during a 14-month COVID-19 pandemic period and a 14-month control period in Berlin, Germany.
Inclusion criteria
All orthopaedic trauma patients (defined as patients who were primarily treated by an orthopaedic trauma surgeon in the ED), and all cases where the trauma team was activated [initiated if patients met the Grade of Recommendation B-criteria (GoR-B) defined by DGU® (e.g. fall/jump from great heights, penetrating or gunshot injuries, high-velocity traffic accidents) (27)] were included. All SVSAs were included if the provided information in the medical chart indicated a suicide attempt or where a suicide intention leading to the injury could not be ruled out (e.g. in case of schizophrenia or bipolar disorder).
Exclusion criteria
For orthopaedic trauma patients and trauma team activations no exclusion criteria were required. For SVSAs we excluded patients who denied suicidal intentions and where an unintentional accident was plausible after ruling out mental health conditions.
Ethics
Ethical approval (EA1/082/20) was obtained from the local ethics committee, Ethikkommission Charité – Universitätsmedizin Berlin.
Statistical analysis
Data were analyzed primarily descriptively. Incidences were presented as absolute counts within the period of observation. For both the pandemic and the control period, specific characteristics of SVSAs were calculated and compared in an exploratory manner. In case of continuous and ordinal data, mean, median, interquartile range and standard deviation (SD) were calculated as well as the p-value from a Wilcoxon signed-rank test. For binary data, corresponding proportions were calculated as well as the p-value from Pearson's Chi-Squared test, or Fisher's exact test if the expected count in any cell was below 5. To compare variables during the pandemic vs. control period, odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. To allow for scale-independent comparisons between ORs of continuous variables, variables were standardized to a mean of 0 and an SD of 1.
A central aim of the analysis was the comparison of monthly incidences of SVSAs between the control and the pandemic period. To control for seasonal trends, a regression approach was chosen. The limited time period and the relatively small incidence raised concerns regarding the appropriate model fit of simple linear regression. Therefore, a sensitivity analysis also considering regression models for count data, i.e., poisson and negative binomial regression were fitted, too, and the results of each regression approach were compared.
All observations during the defined time frame within the participating Level-I Trauma Centers were included in the analysis, so no sample size calculation was conducted. Instead, an exemplarily power analysis was used to justify the chosen time frame: based on the assumption of a monthly incidence of ~10 SVSAs, the 95% CI of the pairwise difference between pre- and post-pandemic months would have an expected width of 1.0 SVSA per month.
Results
Absolute numbers and seasonality
During the pandemic period, significantly fewer orthopaedic trauma patients presented to the ED during the pandemic (n = 70,271) compared to the control (n = 84,864) period (p = 0.0017). Subgroup analyses confirmed this pattern for each center (hospital I, p = 0.0012; hospital II, p = 0.0017; hospital III, p = 0.0006; hospital IV, p = 0.0046; Figure 2A). Furthermore, the longitudinal development of orthopaedic trauma patients per month unveiled a decrease in cases, especially during spring and autumn 2020, when lockdown measures were in effect in Berlin, Germany (Figure 2B).
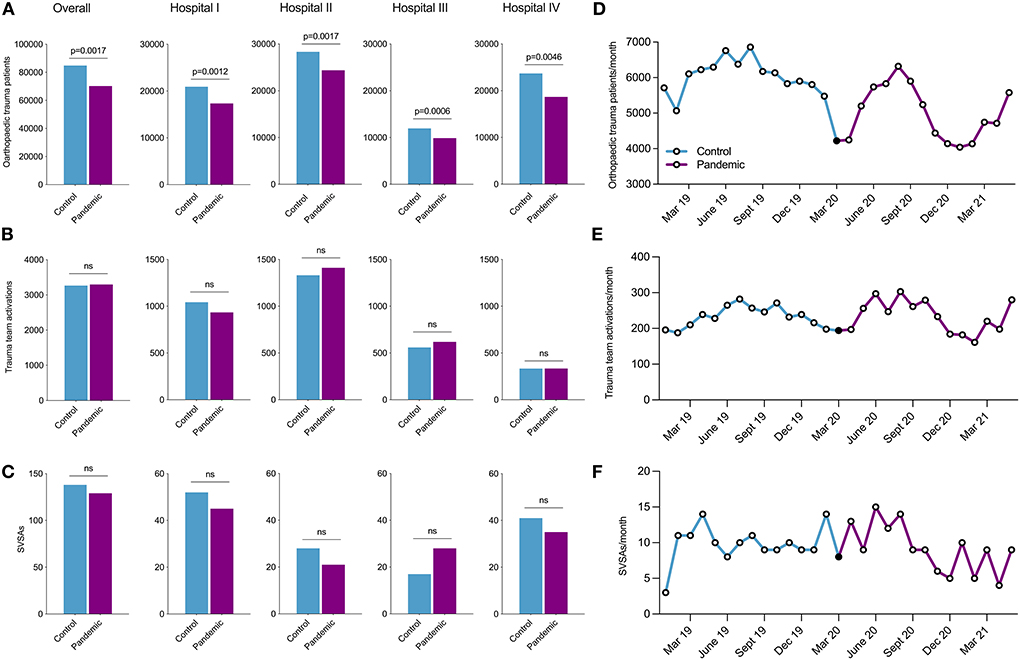
Figure 2. Overall and hospital-specific distribution of (A) orthopaedic trauma patients, (B) trauma team activations, and (C) SVSAs during the 14-month control (blue) and pandemic period (purple). Longitudinal distribution of (D) orthopaedic trauma patients, (E) trauma team activations, and (F) SVSAs per month during the control (blue) and pandemic period (purple). March 2020 (black dot) was excluded from the analyses. SVSAs, serious violent suicide attempts.
Trauma team activation numbers remained unchanged during control and pandemic periods, with 3.267 and 3.298 cases, respectively (Figure 2C). Although overall numbers of trauma team activation did not differ, decreases were observed during shutdown periods (Figure 2D). Lastly, SVSAs also remained unchanged when comparing control (n = 138) and pandemic (n = 129) periods (Figure 2E). Monthly SVSAs were evenly distributed between February 2019 and August 2020, followed by a slight decline between September 2020 and May 2021 (Figure 2F). Interestingly, SVSAs decreased in all hospitals during the pandemic period, apart from hospital III (CBF), where an increase, yet not significant, was observed (p = 0.1270; Figure 2E).
Controlling for seasons, linear regression (p = 0.427), poisson regression (p = 0.446), and negative binomial regression (p = 0.446) models showed no differences between control and pandemic periods.
Additionally, we compared two calendar-matched 12-month periods from April 2019-March 2020 (control II) to April 2020-March 2021 (pandemic II) and found similar results, where linear regression (p = 0.523), poisson regression (p = 0.595), and negative binomial regression (p = 0.595) models showed no differences between control II and pandemic II periods.
Quality of SVSAs
Demographics and suicide motivation
After assessing absolute numbers of SVSAs, changes in quality and severity of SVSAs during the control and pandemic period were evaluated. No relevant differences were observed between the two periods for all variables assessed (Table 1).
Women accounted for 33% (n = 45) of SVSAs during the control and for 40% (n = 51) of SVSAs during the pandemic period. The median (IQR) age was 43 (29;30) years during the control and 40 (28;31) years during the pandemic period. Alcohol and drug intoxications in association with SVSAs were observed during control (both 14%, n = 19) and pandemic (alcohol 12%, n = 15; other drugs 21%, n = 27) periods. Regular substance abuse was seen in 23% (n = 32) of cases during the control and in 28% (n = 36) of cases during the pandemic period.
During the control period, psychiatric diagnoses were evaluated for 67% (n = 93) and during the pandemic for 61% (n = 79) of patients committing SVSAs (Figure 3A and Table 1).
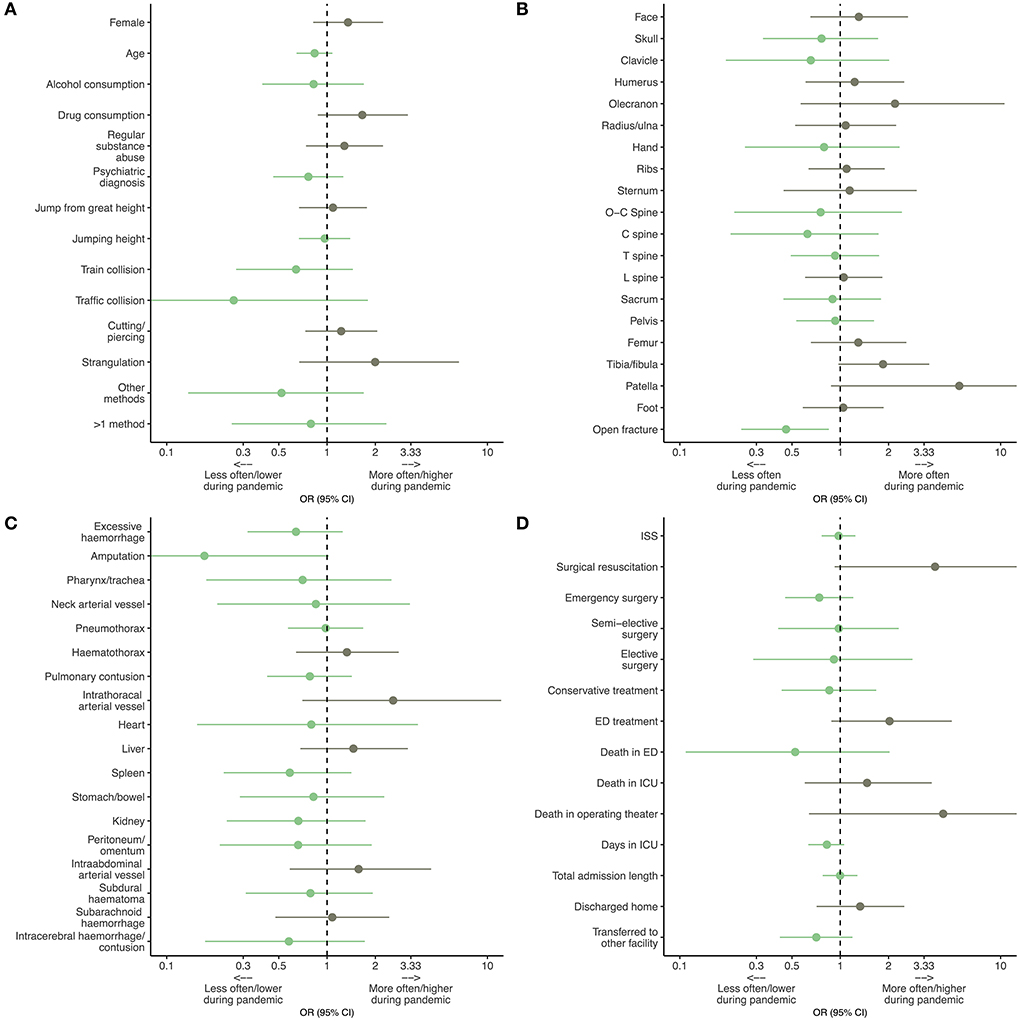
Figure 3. Odds ratios (ORs) for (A) demographics and suicide methods, (B) osseous injury patterns, (C) non-osseous injury patterns, (D) Injury Severity Score (ISS), treatment and outcomes of patients who undertook serious violent suicide attempts (SVSAs) during the COVID-19 pandemic and a proceeding control period. Green confidence intervals (95% CIs) indicate an event happening less often during the pandemic, whereas gray 95% CIs represent events happening more often during the pandemic. To obtain symmetric CIs, a log-scaled x-axis was used (few, very wide CIs were cut for proper display). ED, emergency department; C spine, cervical spine; ICU, intensive care unit, L spine, lumbar spine, O-C spine, occipito-cervical spine, T spine, thoracic spine.
Methods of SVSAs
With 41% (n = 56) and a median (IQR) height of 10 (5.5;13) meters and 43% (n = 55) and a median height of 9 (6;14) meters, jumps from great heights were the most common suicide method observed during control and pandemic periods, respectively. Cutting and piercing injuries were seen in 30% (n = 41) and 34% (n = 33) of cases during the control and pandemic period. SVSAs including subway train collisions were observed in 12% (n = 16) of cases during the control and in 7.8% (n = 10) of cases during the pandemic period. Strangulations were evident in 3.6% (n = 5) of cases during the control and in 7.0% (n = 9) of cases during the pandemic period. SVSAs including more than 1 method were observed in 5.8% (n = 8) of cases during the control and in 4.7% (n = 6) of cases during the pandemic period (Figure 3A and Table 1).
Injury patterns following SVSAs
Please refer to Table 1 and Figures 3B, C for a detailed overview of osseus and non-osseus injury patterns. No relevant changes were observed apart from open fractures, which were seen significantly less often during the pandemic period with 14% (n = 18) compared to the control period with 25% (n = 36) (p = 0.014). In addition, the median (IQR) ISS during the control period was 22 (8, 31) compared to 17 (5, 32) during the pandemic period.
Treatment of SVSAs
Resuscitation surgery was performed twice during the control period and seven times during the pandemic period. Sixty-two percent (n = 68) and 55% (n = 71) of patients required emergency surgery and 8.7% (n = 12) and 8.5% (n = 11) semi-elective and 5.1% (n = 7) and 4.7 (n = 6) elective surgery during the control and pandemic period. Sixteen percent (n = 22) and 14% (n = 18) of patients were treated conservatively and 6.5% (n = 9) and 12% (n = 16) of patients received ED treatment during respective control and pandemic periods (Figure 3D and Table 1).
Outcomes following SVSAs
Six patients died in the ED, nine in the ICU and one in the operating theater (11.6%; n = 16) during the control period and three in the ED, 12 in the ICU and four in the operating theater during the pandemic period (14.7%; n = 19).
Sixteen percent (n = 22) of patients could be discharged to their homes during the control and 20% (n = 26) during the pandemic period. The remaining patients (72%; n = 100 during the control and 65%; n = 84 during the pandemic) were transferred to other specialized psychiatric or rehabilitation facilities.
Overall, SVSA patients spent a median (IQR) of 11 (3;24) days in hospital during the control period and 6.5 (2;21) days during the pandemic period. This included a median (IQR) of five (2;12) and three (2;9) days in the ICU during respective periods (Figure 3D and Table 1).
Discussion
The present study demonstrates a constant rate of SVSAs and trauma team activations during a 14-month period during the COVID-19 pandemic compared to a preceding control period. Furthermore, we were able to show that the quality of SVSAs, including suicide method, injury severity, type of treatment, and admission time did not change between the two assessed periods. Yet, the total number of orthopaedic trauma patients decreased significantly, in the EDs of four Level-I Trauma Centers in Berlin, Germany.
While previous studies reported an increase in depression and suicidal ideation during the COVID-19 pandemic (28, 31, 33, 34), most high volume data on actual suicide attempts failed to show a concomitant increase in suicides (10, 11, 32, 35–37). Our data are in line with these findings and we were able to show that violent suicide attempts did not increase during the first 14 months of the pandemic in Berlin, Germany. Nevertheless, few studies with limited patient numbers have demonstrated an increase in suicide rates during specific periods amid the COVID-19 pandemic in 2020 (12–15). Previous health crises, including the SARS epidemic in Hong Kong and the Ebola virus epidemic in Guinea led to an increase in suicide attempts and completed suicides (39), however, thus far this has not been the case for the COVID-19 pandemic.
While previous health crises, including the SARS epidemic in Hong Kong, and the Ebola virus epidemic in Guinea led to an increase in suicide attempts and completed suicides (38), thus far this has not been the case for the COVID-19 pandemic.
Reasons for this may have been prompt economical support programs, implemented in Germany, which helped to reduce financial losses for individuals and companies (39). While recessions have previously been linked to increased suicide rates, the effect seemed to be less pronounced in countries with larger social welfare spending (40–42).
Second, access to healthcare during the COVID-19 pandemic was perceived as reasonably good among the German population (43). Notably, access to healthcare has previously also been shown to be a crucial factor in suicide prevention (44, 45).
It is however too early to finalize conclusions on suicide rates during the COVID-19 pandemic, which is still ongoing in various countries worldwide. Although the majority of currently published studies on the topic could not show an increase in suicide attempts and completed suicides during the pandemic (10, 11, 32, 35–37), suicides may still rise with a certain delay, as previously seen in periods following natural catastrophes in the US (46).
In a Swedish registry-based study, cutting or piercing accounted for 35.6% of violent index suicide attempts and only for 4.8% of completed violent suicides (18). In line with these findings, we observed cutting or piercing in 29.7% of cases (n = 41) during the control, and in 34.1% of cases (n = 44) during the pandemic period.
While we saw jumps from great heights in 40.6% (n = 56) of the study population during the control and in 42.6% (n = 55) of cases during the pandemic period, they only accounted for 9.5% of violent index attempts and 8% of completed violent suicides in the Swedish registry-based study (18). This marked difference may be attributed to our study population, exclusively derived from an urban environment. It was previously described that the accessibility to lethal methods, including living in higher buildings, determines the method of suicide (47).
One study from South Korea reported a decline in violent suicide attempts (“self-harm injury”) from 82.6% before the pandemic (January–October 2019) to 30% during the pandemic (January–October 2020), while they observed a rise in drug overdoses from 13.3 to 66.6% (14).
Marked differences can be observed between suicide completers, where hanging is the most prevalent method, and suicide attempters, where poisoning is most commonly observed (48). The method chosen at the index suicide attempt also predicts the chances of suicide completion at a later point. Suicide completers most commonly chose the same method during an index suicide attempt (90% for hanging) (49).
Effects of seasonality, weather, and temperature on suicide rates have been extensively reported in previous decades. While suicide peaks were described for spring and late summer in the 1960s−1980s (50, 51) more recent data indicate that seasonal patterns have diminished regarding suicide rates. Reasons identified are an increased intensity of communal life and technological developments (52–54). Accordingly, our data showed no differences in SVSA rates, when controlled for seasonality.
While incidences of neuro-psychiatric diagnoses rose during the COVID-19 pandemic, in both, patients suffering from COVID-19 (55) and healthy individuals (28), early reports also suspected a direct translation into suicide attempts (30, 56). In a commentary, Sher reported a high probability of patients suffering from post-COVID-19 syndrome to show an increase in suicidal ideation and behavior due to long-term psychiatric, neurological, and physical illness (57). To date, most data could not confirm concerns about increased suicide rates during the COVID-19 pandemic, raised in various editorials, reviews and commentaries.
Reporting on suicidal behavior must be conducted with caution, as misleading data and sensational media coverage may considerably influence suicide intentions and imitations. Scientific reporting is obligated to be conducted in a precise and balanced manner and should focus on facts rather than speculations (29, 58).
This study has several limitations. We were able to analyze ED records of four Level-I Trauma Centers, yet, our data is merely representative for the urban area of Berlin, Germany. While conclusions could be relevant for other capital regions, they may fall short when looking at provincial areas or countries with alternate urban environments (47). Second, shutdown measures varied greatly between regions and countries. Therefore, data may be interpreted with caution and should always be put in perspective to available international evidence. Third, the retrospective character of our study does not allow assumptions about causation, but rather about associations between the COVID-19 pandemic and suicidal behavior. Finally, this study only covered the first 14 months of the COVID-19 pandemic and conclusions for the pandemic as a whole are not valid at this point. Most studies reporting on suicide numbers and rates have however covered shorter time periods and long-term data is still scarce.
To address a potential selection bias based on hospital location, we included four Level-I Trauma Centers that geographically form a string spanning from West to East Berlin. We thereby anticipated to minimize a geographical or socioeconomical selection of patients.
Retrospective chart review studies often include a relevant documentation bias (data entry, data collection, and data quality assurance). We employed a standardized data retrieval sheet (Microsoft Excel) for all four participating centers to ensure obtained data are of similar quality. Following the guide of Gearing et al. (26), sections for each variable in the data retrieval sheet were created using simple and unambiguous response options. Nonetheless, documentation of e.g., alcohol consumption or history of mental illness is highly dependent on the documenting physician and may be a relevant source of bias.
The COVID-19 pandemic may have just surpassed its peak and new virus variants, including Omicron, seem to cause milder symptoms in affected individuals compared to previous virus strains. Nonetheless, lockdown and shutdown measures are still in place in numerous countries to date. Recent data indicated that restrictions and subsequent self-isolation related to COVID-19 correlated with a rise in psychiatric diagnoses. Whether this would also impact suicide attempts was discussed by a number of authors.
This study was able to demonstrate that violent suicide attempts did not change in quantity nor in quality during the COVID-19 pandemic compared to a control period prior to the SARS-CoV-2 outbreak in 2019/2020. These data may help to map out “collateral damage” scenarios resulting from social distancing, while preparing for future pandemics. Whether current lockdown and shutdown measures have an impact on long-term mental health and suicidal behavior remains to be seen.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without unduereservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethikkommission der Charité – Universitätsmedizin Berlin. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
TM and SM designed and conceived the study. TM, TT, ADD, ED, GR, MZ, RC, MK, PW, and FF provided, selected, assembled, analyzed, and interpreted data. DZ and LSH provided statistical, graphical and software support. TT, US, TF, DG, NS, AR, and SM curated data and provided project administration. TM drafted the original manuscript. All authors agree to be accountable for the work as a whole and ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors critically reviewed and edited the final manuscript and have read and confirmed the final version, submitted to Frontiers in Psychiatry.
Acknowledgments
TM is a fellow of the BIH Charité Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin, and the Berlin Institute of Health at Charité (BIH).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Haug N, Geyrhofer L, Londei A, Dervic E, Desvars-Larrive A, Loreto V, et al. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat Hum Behav. (2020) 4:1303–12. doi: 10.1038/s41562-020-01009-0
2. Wang Y, Shi L, Que J, Lu Q, Liu L, Lu Z, et al. The impact of quarantine on mental health status among general population in China during the COVID-19 pandemic. Mol Psychiatry. (2021) 26:4813–822. doi: 10.1038/s41380-021-01019-y
3. Pierce M, McManus S, Hope H, Hotopf M, Ford T, Hatch SL, et al. Mental health responses to the COVID-19 pandemic: a latent class trajectory analysis using longitudinal UK data. Lancet Psychiatry. (2021) 8:610–19. doi: 10.2139/ssrn.3784647
4. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. (2021) 8:141–9. doi: 10.1016/S2215-0366(20)30482-X
5. Daly M, Robinson E. Psychological distress and adaptation to the COVID-19 crisis in the United States. J Psychiatr Res. (2021) 136:603–9. doi: 10.1016/j.jpsychires.2020.10.035
6. Gunnell D, Appleby L, Arensman E, Hawton K, John A, Kapur N, et al. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:468–71. doi: 10.1016/S2215-0366(20)30171-1
7. John A, Eyles E, Webb RT, Okolie C, Schmidt L, Arensman E, et al. The impact of the COVID-19 pandemic on self-harm and suicidal behaviour: update of living systematic review. F1000Res. (2020) 9:1097. doi: 10.12688/f1000research.25522.1
8. Cheung YT, Chau PH, Yip PS. A revisit on older adults suicides and severe acute respiratory syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry. (2008) 23:1231–8. doi: 10.1002/gps.2056
9. Chan SM, Chiu FK, Lam CW, Leung PY, Conwell Y. Elderly suicide and the 2003 SARS epidemic in Hong Kong. Int J Geriatr Psychiatry. (2006) 21:113–8. doi: 10.1002/gps.1432
10. Radeloff D, Papsdorf R, Uhlig K, Vasilache A, Putnam K, von Klitzing K. Trends in suicide rates during the COVID-19 pandemic restrictions in a major German city. Epidemiol Psychiatr Sci. (2021) 30:e16. doi: 10.1017/S2045796021000019
11. Pirkis J, John A, Shin S, DelPozo-Banos M, Arya V, Analuisa-Aguilar P, et al. Suicide trends in the early months of the COVID-19 pandemic: an interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry. (2021) 8:579–88. doi: 10.1016/S2215-0366(21)00091-2
12. Shrestha R, Siwakoti S, Singh S, Shrestha AP. Impact of the COVID-19 pandemic on suicide and self-harm among patients presenting to the emergency department of a teaching hospital in Nepal. PLoS ONE. (2021) 16:e0250706. doi: 10.1371/journal.pone.0250706
13. Chevallard G, Veronese G, Giudici R, Pressato L, Pozzi F, Compagnone C, et al. Facing increased suicide attempts during COVID-19 pandemic lockdown: the experience from the major trauma center in Lombardy, Italy. Minerva Anestesiol. (2021) 87:243–5. doi: 10.23736/S0375-9393.20.14970-8
14. Kang JH, Lee SW Ji JG, Yu JK, Jang YD, Kim SJ, et al. Changes in the pattern of suicide attempters visiting the emergency room after COVID-19 pandemic: an observational cross sectional study. BMC Psychiatry. (2021) 21:571. doi: 10.1186/s12888-021-03570-y
15. Tanaka T, Okamoto S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat Hum Behav. (2021) 5:229–38. doi: 10.1038/s41562-020-01042-z
16. Bray MJC, Daneshvari NO, Radhakrishnan I, Cubbage J, Eagle M, Southall P, et al. Racial differences in statewide suicide mortality trends in maryland during the Coronavirus Disease 2019 (COVID-19) pandemic. JAMA Psychiatry. (2021) 78:444–7. doi: 10.1001/jamapsychiatry.2020.3938
17. Mitchell TO, Li L. State-level data on suicide mortality during COVID-19 quarantine: early evidence of a disproportionate impact on racial minorities. Psychiatry Res. (2021) 295:113629. doi: 10.1016/j.psychres.2020.113629
18. Stenbacka M, Jokinen J. Violent and non-violent methods of attempted and completed suicide in Swedish young men: the role of early risk factors. BMC Psychiatry. (2015) 15:196. doi: 10.1186/s12888-015-0570-2
19. Mergl R, Koburger N, Heinrichs K, Szekely A, Toth MD, Coyne J, et al. What are reasons for the large gender differences in the lethality of suicidal acts? An epidemiological analysis in four European countries. PLoS ONE. (2015) 10:e0129062. doi: 10.1371/journal.pone.0129062
20. Vyssoki B, Kapusta ND, Praschak-Rieder N, Dorffner G, Willeit M. Direct effect of sunshine on suicide. JAMA Psychiatry. (2014) 71:1231–7. doi: 10.1001/jamapsychiatry.2014.1198
21. Lin HC, Chen CS, Xirasagar S, Lee HC. Seasonality and climatic associations with violent and nonviolent suicide: a population-based study. Neuropsychobiology. (2008) 57:32–7. doi: 10.1159/000129664
22. Gvion Y, Levi-Belz Y. Serious suicide attempts: systematic review of psychological risk factors. Front Psychiatry. (2018) 9:56. doi: 10.3389/fpsyt.2018.00056
23. Southern AP, Celik DH. EMS, Trauma Center Designation. StatPearls. Treasure Island, FL: StatPearls Publishing. Copyright © 2021, StatPearls Publishing LLC (2021).
24. Maleitzke T, Pumberger M, Gerlach UA, Herrmann C, Slagman A, Henriksen LS, et al. Impact of the COVID-19 shutdown on orthopaedic trauma numbers and patterns in an academic Level I Trauma Center in Berlin, Germany. PLoS ONE. (2021) 16:e0246956. doi: 10.1371/journal.pone.0246956
25. Schuppert A, Polotzek K, Schmitt J, Busse R, Karschau J, Karagiannidis C. Different spreading dynamics throughout Germany during the second wave of the COVID-19 pandemic: a time series study based on national surveillance data. Lancet Reg Health Eur. (2021) 6:100151. doi: 10.1016/j.lanepe.2021.100151
26. Gearing RE, Mian IA, Barber J, Ickowicz A. A methodology for conducting retrospective chart review research in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry. (2006) 15:126–34.
27. Hagebusch P, Faul P, Naujoks F, Klug A, Hoffmann R, Schweigkofler U. Trauma-team-activation in Germany: how do emergency service professionals use the activation due to trauma mechanism? Results from a nationwide survey. Eur J Trauma Emerg Surg. (2020) 48:393–99. doi: 10.1007/s00068-020-01425-x
28. Zhou SJ, Wang LL Qi M, Yang XJ, Gao L, Zhang SY, et al. Depression, anxiety, and suicidal ideation in Chinese University students during the COVID-19 pandemic. Front Psychol. (2021) 12:669833. doi: 10.3389/fpsyg.2021.669833
29. Hawton K, Marzano L, Fraser L, Hawley M, Harris-Skillman E, Lainez YX. Reporting on suicidal behaviour and COVID-19-need for caution. Lancet Psychiatry. (2021) 8:15–7. doi: 10.1016/S2215-0366(20)30484-3
30. Sher L. An infectious disease pandemic and increased suicide risk. Braz J Psychiatry. (2020) 42:239–40. doi: 10.1590/1516-4446-2020-0989
31. Ammerman BA, Burke TA, Jacobucci R. McClure K. Preliminary investigation of the association between COVID-19 and suicidal thoughts and behaviors in the US. J Psychiatr Res. (2021) 134:32–8. doi: 10.1016/j.jpsychires.2020.12.037
32. Appleby L, Richards N, Ibrahim S, Turnbull P, Rodway C, Kapur N. Suicide in England in the COVID-19 pandemic: early observational data from real time surveillance. Lancet Reg Health Eur. (2021) 4:100110. doi: 10.1016/j.lanepe.2021.100110
33. Brailovskaia J, Teismann T, Friedrich S, Schneider S, Margraf J. Suicide ideation during the COVID-19 outbreak in German university students: comparison with pre-COVID 19 rates. J Affect Disord Rep. (2021) 6:100228. doi: 10.1016/j.jadr.2021.100228
34. Mayne SL, Hannan C, Davis M, Young JF, Kelly MK, Powell M, et al. COVID-19 and adolescent depression and suicide risk screening outcomes. Pediatrics. (2021) 148:e2021051507. doi: 10.1542/peds.2021-051507
35. Leske S, Kolves K, Crompton D, Arensman E, de Leo D. Real-time suicide mortality data from police reports in Queensland, Australia, during the COVID-19 pandemic: an interrupted time-series analysis. Lancet Psychiatry. (2021) 8:58–63. doi: 10.1016/S2215-0366(20)30435-1
36. Clapperton A, Spittal MJ, Dwyer J, Garrett A, Kolves K, Leske S, et al. Patterns of suicide in the context of COVID-19: evidence from three Australian States. Front Psychiatry. (2021) 12:797601. doi: 10.3389/fpsyt.2021.797601
37. Yoshioka E, Hanley SJB, Sato Y, Saijo Y. Impact of the COVID-19 pandemic on suicide rates in Japan through December 2021: an interrupted time series analysis. Lancet Reg Health West Pac. (2022) 24:100480. doi: 10.1016/j.lanwpc.2022.100480
38. Zortea TC, Brenna CTA, Joyce M, McClelland H, Tippett M, Tran MM, et al. The impact of infectious disease-related public health emergencies on suicide, suicidal behavior, and suicidal thoughts. Crisis. (2021) 42:474–87. doi: 10.1027/0227-5910/a000753
39. Cantillon B, Seeleib-Kaiser M, van der Veen R. The COVID-19 crisis and policy responses by continental European welfare states. Soc Policy Adm. (2021) 55:326–38. doi: 10.1111/spol.12715
40. Baumbach A, Gulis G. Impact of financial crisis on selected health outcomes in Europe. Eur J Public Health. (2014) 24:399–403. doi: 10.1093/eurpub/cku042
41. Stuckler D, Basu S, Suhrcke M, Coutts A, McKee M. The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet. (2009) 374:315–23. doi: 10.1016/S0140-6736(09)61124-7
42. Toffolutti V, Suhrcke M. Assessing the short term health impact of the Great Recession in the European Union: a cross-country panel analysis. Prev Med. (2014) 64:54–62. doi: 10.1016/j.ypmed.2014.03.028
43. Hajek A, De Bock F, Wieler LH, Sprengholz P, Kretzler B, König H-H. Perceptions of health care use in Germany during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:9351. doi: 10.3390/ijerph17249351
44. Tondo L, Albert MJ, Baldessarini RJ. Suicide rates in relation to health care access in the United States: an ecological study. J Clin Psychiatry. (2006) 67:517–23. doi: 10.4088/JCP.v67n0402
45. Hester RD. Lack of access to mental health services contributing to the high suicide rates among veterans. Int J Ment Health Syst. (2017) 11:47. doi: 10.1186/s13033-017-0154-2
46. Adiamah A, Moody N, Blackburn L, Dickson E, Thompson A, Reilly JJ, et al. ICON trauma (impact of COVID-19 on major trauma workload) study. Br J Surg. (2020) 107:e412–e3. doi: 10.1002/bjs.11855
47. Chung KH, Lee HC, Kao S, Lin HC. Urbanicity and methods of suicide: a nationwide population-based study. J Urban Health. (2008) 85:136–45. doi: 10.1007/s11524-007-9238-7
48. Lim M, Lee SU, Park JI. Difference in suicide methods used between suicide attempters and suicide completers. Int J Ment Health Syst. (2014) 8:54. doi: 10.1186/1752-4458-8-54
49. Runeson B, Tidemalm D, Dahlin M, Lichtenstein P, Långström N. Method of attempted suicide as predictor of subsequent successful suicide: national long term cohort study. BMJ. (2010) 341:c3222. doi: 10.1136/bmj.c3222
50. Lester D, Frank ML. Sex differences in the seasonal distribution of suicides. Br J Psychiatry. (1988) 153:115–7. doi: 10.1192/bjp.153.1.115
51. Barraclough BM, White SJ. Monthly variation of suicide and undetermined death compared. Br J Psychiatry. (1978) 132:275–8. doi: 10.1192/S0007125000283347
52. Yip PS, Chao A, Chiu CW. Seasonal variation in suicides: diminished or vanished. experience from England and Wales, 1982-1996. Br J Psychiatry. (2000) 177:366–9. doi: 10.1192/bjp.177.4.366
53. Yip PS, Chao A, Ho TP. A re-examination of seasonal variation in suicides in Australia and New Zealand. J Affect Disord. (1998) 47:141–50. doi: 10.1016/S0165-0327(97)00135-3
54. Yang CT, Yip PSF, Cha ES, Zhang Y. Seasonal changes in suicide in South Korea, 1991 to 2015. PLoS ONE. (2019) 14:e0219048. doi: 10.1371/journal.pone.0219048
55. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. (2021) 8:416–27. doi: 10.1016/S2215-0366(21)00084-5
56. Reger MA, Stanley IH, Joiner TE. Suicide mortality and coronavirus disease 2019-a perfect storm? JAMA Psychiatry. (2020) 77:1093–4. doi: 10.1001/jamapsychiatry.2020.1060
Keywords: injury, death, mortality, SARS-CoV-2, violent suicide attempts, COVID-19
Citation: Maleitzke T, Zocholl D, Topp T, Dimitrov-Discher A, Daus E, Reaux G, Zocholl M, Conze RN, Kolster M, Weber P, Fleckenstein FN, Scheutz Henriksen L, Stöckle U, Fuchs T, Gümbel D, Spranger N, Ringk A and Märdian S (2022) Quality and quantity of serious violent suicide attempts during the COVID-19 pandemic. Front. Psychiatry 13:927696. doi: 10.3389/fpsyt.2022.927696
Received: 24 April 2022; Accepted: 27 June 2022;
Published: 19 July 2022.
Edited by:
Georgios D. Floros, Aristotle University of Thessaloniki, GreeceReviewed by:
Giacomo Veronese, University of Milano-Bicocca, ItalyHaitham Jahrami, Arabian Gulf University, Bahrain
Birgit Ludwig, Medical University of Vienna, Austria
Copyright © 2022 Maleitzke, Zocholl, Topp, Dimitrov-Discher, Daus, Reaux, Zocholl, Conze, Kolster, Weber, Fleckenstein, Scheutz Henriksen, Stöckle, Fuchs, Gümbel, Spranger, Ringk and Märdian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sven Märdian, c3Zlbi5tYWVyZGlhbkBjaGFyaXRlLmRl