 Christian Rauschert1
Christian Rauschert1 Nicki-Nils Seitz1
Nicki-Nils Seitz1 Sally Olderbak1,2
Sally Olderbak1,2 Oliver Pogarell3
Oliver Pogarell3 Tobias Dreischulte4Ludwig Kraus1,5,6*
Tobias Dreischulte4Ludwig Kraus1,5,6*- 1Department of Epidemiology and Diagnostics, IFT Institut Für Therapieforschung, Munich, Germany
- 2Department of Psychology, University of Arizona, Tucson, AZ, United States
- 3Department of Psychiatry and Psychotherapy, Ludwig-Maximilians-Universität, Munich, Germany
- 4Department of General Practice and Family Medicine, Ludwig-Maximilians-Universität, Munich, Germany
- 5Department of Public Health Sciences, Centre for Social Research on Alcohol and Drugs, Stockholm University, Stockholm, Sweden
- 6Institute of Psychology, ELTE Eötvös Loránd University, Budapest, Hungary
Background: Owing to their pharmacological properties the use of opioid analgesics carries a risk of abuse and dependence, which are associated with a wide range of personal, social, and medical problems. Data-based approaches for identifying distinct patient subtypes at risk for prescription opioid use disorder in Germany are lacking.
Objective: This study aimed to identify distinct subgroups of patients using prescribed opioid analgesics at risk for prescription opioid use disorder.
Methods: Latent class analysis was applied to pooled data from the 2015 and 2021 Epidemiological Survey of Substance Abuse. Participants were aged 18–64 years and self-reported the use of prescribed opioid analgesics in the last year (n = 503). Seven class-defining variables based on behavioral, mental, and physical health characteristics commonly associated with problematic opioid use were used to identify participant subtypes. Statistical tests were performed to examine differences between the participant subtypes on sociodemographic variables and prescription opioid use disorder.
Results: Three classes were extracted, which were labeled as poor mental health group (43.0%, n = 203), polysubstance group (10.4%, n = 50), and relatively healthy group (46.6%, n = 250). Individuals within the poor mental health group (23.2%, n = 43) and the polysubstance group (31.1%, n = 13) showed a higher prevalence of prescription opioid use disorder compared to those of the relatively healthy group.
Conclusion: The results add further evidence to the knowledge that patients using prescribed opioid analgesics are not a homogeneous group of individuals whose needs lie in pain management alone. Rather, it becomes clear that these patients differ in their individual risk of a prescription opioid use disorder, and therefore identification of specific risks plays an important role in early prevention.
Introduction
The use of opioid analgesics (OA) is an established component of adequate pain therapy in palliative and acute medicine for patients with severe pain (1). Over the last 25 years, an increase in OA prescriptions can be observed not only internationally in the most affected countries such as the US (2) or Canada (3), but also in Germany (4–7). Based on analyses of German health insurance data, long-term prescriptions (duration ≥3 months) increased by about four percentage points between 2006 and 2015 (8). Studies showed that most of these prescriptions are for patients with chronic non-cancer pain (4), despite evidence on the effectiveness in this patient group is lacking (9). Owing to their pharmacological properties, the use of OA carries the risk of abuse and dependence (10, 11). In Germany, the 1-year prevalence of prescription opioid use disorder (pOUD) among individuals reporting use of opioids prescribed to them by their providers is currently estimated at 21.2% (12). Even though Germany may not currently be affected by an opioid epidemic (6, 13), the high prevalence of pOUD is concerning. Abuse and dependence are associated with a wide range of personal, social, and medical problems and therefore should be prevented (14). The German S3 guideline “Long-term administration of opioids for non-tumor pain” takes this into account and provides evidence-based recommendations to clinicians for appropriate treatment (15).
Among the behavioral, mental, and physical health conditions that are associated with pOUD are co-occurring alcohol use disorder, polysubstance use of illicit drugs (16, 17), depression as well as other psychiatric disorders (12, 16, 18, 19). Although many studies have identified associations between pOUD and single risk factors, little is known about the existence of specific patient subgroups and their individual risk of pOUD. Data-driven approaches to identify such groups have mainly been applied in the US (20–22) but are lacking in Germany. Identifying distinct subtypes of patients taking prescribed OA and their individual risk of pOUD may inform decisions around the need for and length of opioid use as well as strategies to prevent pOUD in patients with severe non-cancer pain.
The aim of this study was to (1) identify distinct subgroups of individuals who used prescribed OA in the past year based on behavioral, mental, and health characteristics and (2) compare the subgroups by risk of pOUD.
Methods
Study Design and Sample
The data used in this study are from the Epidemiological Survey of Substance Abuse (ESA), a representative cross-sectional study of Germany's general population on the use of substances that is conducted every 3 years [for a detailed description of the methodology and design of the single studies, see (23)]. The ESA sample was drawn from the 18- to 64-year-old German-speaking population living in private households. Random sampling was carried out using a two-stage selection procedure. First, 254 “sample points” (i.e., cities, districts, municipalities) were selected proportionally to their population size. Then individuals living in these communities were randomly selected based on personal addresses from population registers. Data were collected through the use of a questionnaire (paper-pencil, telephone interviews, or online). A weight correction (age, gender, education, federal states, and district size class) based on the Iterative Proportional Fitting Algorithm was used to weight the data (24).
We pooled data from two waves of the ESA—years 2015 (n = 9,204) and 2021 (n = 9,046)—in which information about OA was available, resulting in a total of 18,250 cases (see section Data Analysis for justification of pooling). Of the total sample 10,199 women (55.9%), 8,038 men (44.0%), and 13 who selected other (0.07%) participated in this study with an average age of 38.4 years (SD = 0.12). The ESA was approved by the ethics committee of the German Psychological Society (DGPs; Reg.-No: GBLK06102008DGPS).
For the present analysis, only individuals reporting the use of OA within the last 12 months and receiving their medication via a prescription from a medical doctor were included. For the remainder of the manuscript, we refer to these persons as patients.
Variables for Latent Class Analysis (pOUD Risk Factors)
A review of the literature on risk factors identified several behavioral, mental, and health characteristics highly associated with pOUD, which were collected in our survey: hazardous alcohol consumption (25), daily smoking (26), consumption of cannabis (27), consumption of other illicit drugs (amphetamines, ecstasy, LSD, heroin and other opioids, cocaine, crack, hallucinogenic mushrooms) (28, 29), depression, psychological treatment (16, 17, 19, 30), and poor physical health status (31). All variables were dichotomized (yes/no). Hazardous alcohol consumption was assessed using the German version of the Alcohol Use Disorder Identification Test, a screening instrument for alcohol-related disorders with a cut-off value of 8 points out of a possible total of 40 points for having a positive screen (32–34). Daily smoking was defined as the consumption of at least one cigarette per day in the last 30 days. Self-reported information about the consumption of cannabis as well as of other illicit drugs was assessed for the last 12 months. Screening for mental health conditions such as depression as well as information on whether a participant was in treatment for mental health problems or had been diagnosed with a mental disorder was achieved using questions from the Munich Composite International Diagnostic Interview (35, 36). According to the World Health Survey (37), self-rated physical health status was measured using a five-point Likert scale ranging from 1, very good, to 5, very bad. To dichotomize the variable poor health status, the first three points of the scale were summarized and coded as “no,” whereas the last two points of the scale were summarized and coded as “yes.” These variables were used to identify distinct subgroups of individuals reporting the use of prescribed OA.
Selection of External Factors Related to Extracted Classes
The variable of highest interest, pOUD, was assessed using the written version of the Munich Composite International Diagnostic Interview (35, 36). According to the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (38), an opioid use disorder is defined as having occurred if at least two out of 11 criteria have been met in the last 12 months. However, in patients taking prescribed OA under appropriate medical supervision, only nine criteria are applicable as recommended by the DSM-5. Therefore, the criteria “tolerance” and “withdrawal” symptoms are excluded from the DSM-5 diagnosis and were not considered in the analyses in this paper. Further variables to test for class membership were sociodemographic variables including age (metric), gender (male/female; as none of the participants who selected “other” reported OA use), education (low/middle/high), currently employed (yes/no), and net household income (OECD modified equivalence scale) below the poverty threshold (yes/no). The variable education was categorized into three groups according to the International Standard Classification of Education (ISCED) as follows: low (ISCED 1 and ISCED 2), middle (ISCED 3 and ISCED 4), and high (ISCED 5) (39).
Data Analysis
To reach a sample size of n ≥ 500, which is sufficiently powered for latent class analysis (LCA) (40–42), the data from two ESA waves, years 2015 and 2021, were pooled. Before the data was pooled, it was tested whether the mean levels (or categorical proportions) and relations between all variables included in the LCA, χ2 tests, and t-tests were comparable between the waves. We found no statistical difference in the correlations between all variables between the waves. Differences in means (continuous variables) and proportions (categorical variables) were tested using independent t-tests and χ2 tests, respectively (for detailed information see Supplementary Table 1). No statistically significant differences were found (all p-values ≥ 0.132) except for the variable mode of administration (i.e., paper-pencil, telephone, or internet-based) (p-value < 0.01). However, this difference was expected due to an increased internet use from 2015 to 2021: 38.4% of the participants answered the ESA questionnaire online in 2015 whilst in 2021 61.6%.
Seven class-defining variables, as described above, were used to delineate subgroups of patients taking prescription OA using LCA. The LCA is a probabilistic model-based approach that uses multivariate categorical data as inputs to identify unobserved, mutually exclusive classes (subgroups of individuals) in a certain population. Membership of an individual in a specific class is based on similarities in individual response behavior to some chosen set of observed variables by calculating class membership probabilities (43, 44). To determine the number of latent classes, five alternative models were run, ranging from one to five classes. A complex mixture term was needed to avoid biased results resulting from the two-stage selection procedure of the ESA. To choose the best model with an optimum number of classes, goodness-of-fit-criteria such as the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), the adjusted Bayesian Information Criterion (aBIC) as well as entropy were used to compare the five models. High entropy, as well as low values of AIC, aBIC, and BIC, indicate a good class solution, where the BIC was considered the best indicator (40, 45). To evaluate the discriminatory power of the models, average class assignment probabilities were determined (45). The selection of the final model was also based on the researchers' assessment of the interpretability of the results. The LCA estimation was conducted in MPlus 6.12 (46) using maximum likelihood estimation with robust standard errors.
To identify associations between class membership and pOUD as well as sociodemographic factors (described above), statistical tests were performed. Testing for differences between the identified groups was done with χ2 tests for categorical variables and t-tests for continuous variables. An alpha level of 0.05 was considered for statistical significance. All analysis was performed using Stata 15.1 SE (Stata Corp LP; College Station, TX, USA) (47).
Results
Analysis Sample
Data were available for 537 people who reported using prescribed OA in the past year, of which 34 individuals were excluded because of missing values on key variables: pOUD (21 individuals), unemployed (10 individuals), and education according to the ISCED (3 individuals). The final analysis sample was comprised of 503 individuals.
Prevalence Distribution of Class-Defining Variables
Information about the weighted prevalence proportions (with listwise deletion of missing data) of the seven class-defining variables is shown in Table 1. Depression (60.2%), as well as daily smoking (32.2%), were the most prevalent indicators, whereas the use of other illicit drugs (9.2%) and the use of cannabis (12.9%) showed the lowest prevalence proportions. About one-fifth (18.3%) of the respondents met the criteria for hazardous alcohol consumption, and one quarter (26.7%) reported being treated for mental health problems or a diagnosed mental disorder.
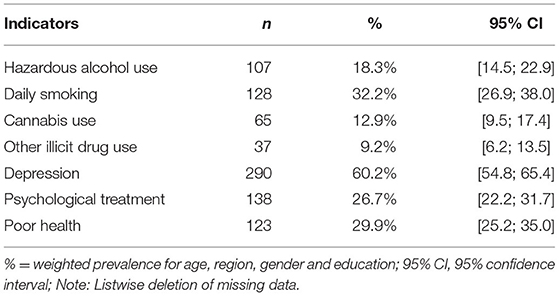
Table 1. Weighted prevalence proportions of class-defining variables (n = 503).
Identifying Subgroups With LCA
A review of the goodness-of-fit indicators revealed contradictory recommendations regarding the appropriate number of classes. We ultimately decided on the three-class solution because it had the best fit according to two of the fit indices (BIC and aBIC), a better distribution of class prevalence (average class assignment probability was >0.8), and the subtypes were associated with meaningful and clearly distinct subgroups values (Table 2). The assumption of conditional independence in all three classes was met (45).
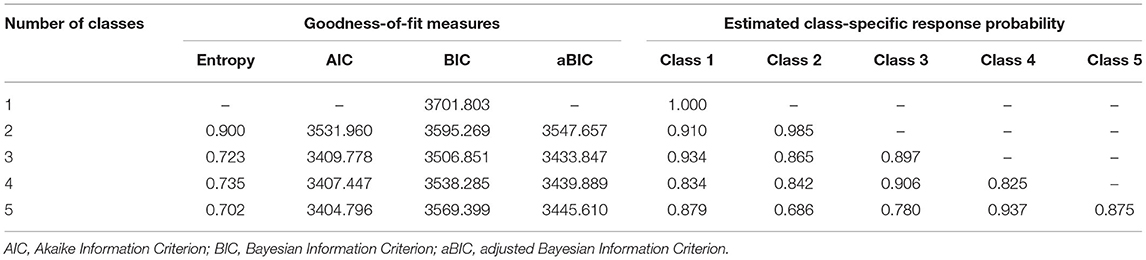
Table 2. Goodness-of-fit-measures and class-specific response probabilities of the five investigated models for deciding the number of classes (n = 503).
Estimated class-specific response probabilities indicating patterns of three distinct subgroups of individuals using prescription OA are presented in Figure 1. The first class (43.0%, n = 203) showed the highest value for poor health (60.1%) of all classes and very low values for cannabis use (6.3%) and other illicit drug use (0.01%). On account of the highest values for depression (95.7%) and psychological treatment (55.4%) compared with the other classes and low to moderate values in all other class-defining variables, this class was characterized as the “poor mental health group”.
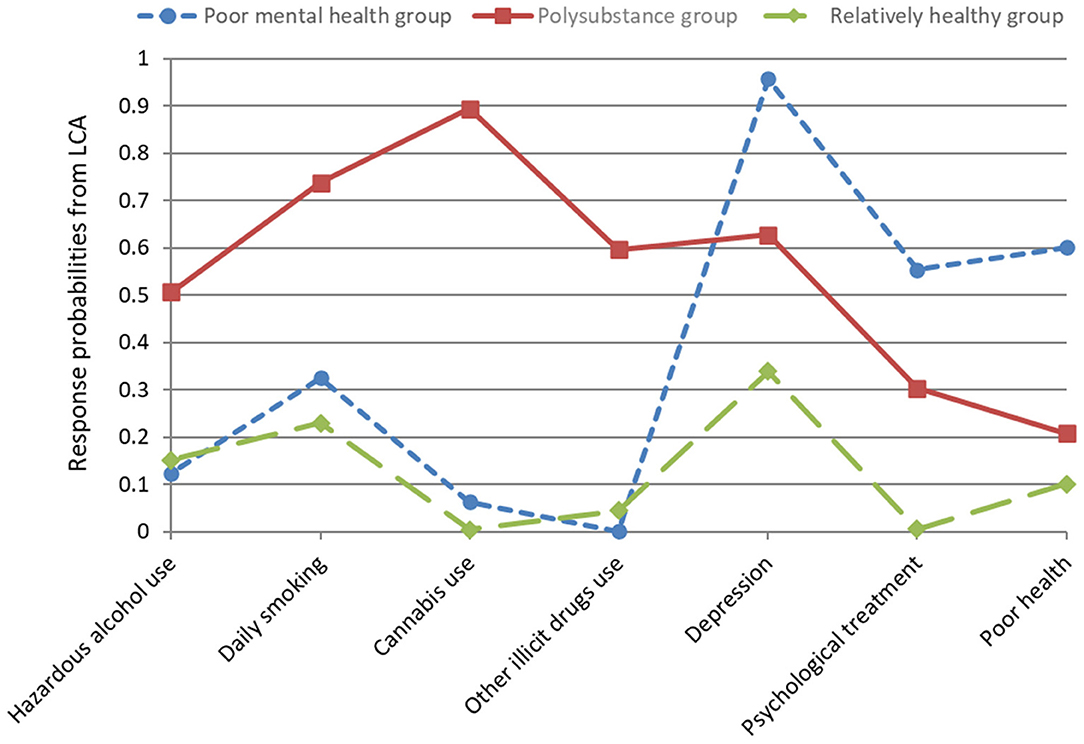
Figure 1. Estimated class-specific response probabilities for seven pOUD risk factors. A high score indicates a high probability of a particular risk factor.
Response probabilities of individuals in class 2 (10.4%, n = 50) were very high in all substance use variables, with cannabis use showing the highest value (89.4%). Although patients in this class showed a high value for depression, this class was defined as the “polysubstance group”.
Class 3 (46.6%, n = 250) comprised individuals who were less likely to have poor health (10.1%), less likely to be in psychological treatment (0.5%), and less likely to be engaging in hazardous alcohol use (15.2%), cannabis use (0.4%), or the use of other illicit drugs (4.5%). They also had moderate values for daily smoking (23.0%) and depression (33.9%). Thus, the third class was labeled as the “relatively healthy group”.
Baseline Characteristics of Extracted Subgroups
Information about weighted proportions of sociodemographic data and pOUD over all three subgroups is displayed in Table 3. Individuals in the poor mental health group were predominantly female (68.9%, n = 156) with an average age of 46.0 years (SD = 0.93), and the majority had a middle level of education (53.9%, n = 104). In this subgroup, 22.4% (n = 44) reported having a net household income below the poverty threshold and 34.4% (n = 71) were unemployed. Diagnostic criteria for pOUD were met in 23.2% (n = 43) of patients.
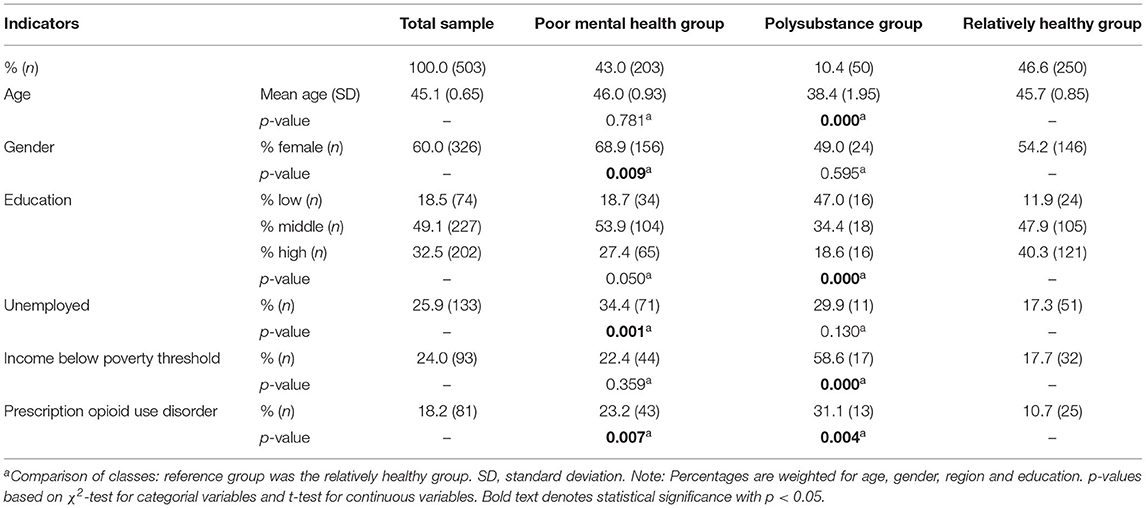
Table 3. Baseline characteristics of the extracted classes.
Patients in the polysubstance group were on average 38.4 years old (SD = 1.95), and 49.0% (n = 24) were female. The level of education in this subgroup was predominantly low (47.0%, n = 16), 29.9% (n = 11) were unemployed, and 58.6% (n = 17) had an income below the poverty threshold. pOUD was detected in 31.1% (n = 13) of patients.
The relatively healthy group was marked by individuals with an average age of 45.7 years (SD = 0.85). More than half of all patients in this subgroup were female (54.2%, n = 146), and the majority had a middle level of education (47.9%, n = 105). The proportion of unemployed individuals in this subgroup was 17.3% (n = 51), and 17.7% (n = 32) had a net household income below the poverty threshold. pOUD occurred in 10.7% (n = 25) of patients.
Differences Between Subgroups on External Factors
Individuals in the poor mental health group showed significantly higher proportions of pOUD compared with the relatively healthy group (23.2% vs. 10.7%). Moreover, patients in this subgroup were more likely to be female (68.9% vs. 54.2%) and unemployed (25.5% vs. 17.3%) compared to those in the relatively healthy group. A higher proportion of individuals within the polysubstance group had a diagnosis of pOUD compared with the relatively healthy group (31.1% vs. 10.7%). Additionally, members of this subgroup were more likely to be younger, with a lower level of education (47.0% vs. 11.9%) as well as a net household income below the poverty threshold (58.6% vs. 17.7%) compared with those in the relatively healthy group.
Discussion
The present study investigated pooled cross-sectional data from the ESA for the years 2015 and 2021 to identify distinct subgroups of patients using prescribed OA, based on behavioral, mental, and physical health characteristics commonly considered to be relevant to problematic OA use. The study aimed to address differences in the prevalence of pOUD between the single subgroups. Latent class analysis revealed that a three-class model best fitted the data. Subgroups were labeled as poor mental health group (43.0%, n = 203), polysubstance group (10.4%, n = 50), and relatively healthy group (46.6%, n = 250). Testing for group differences indicated that individuals in the poor mental health subgroup as well as individuals in the polysubstance group showed a higher prevalence of pOUD compared to the relatively healthy group. Furthermore, patients in the poor mental health group were more likely to be female and unemployed. Against that, patients of the polysubstance group were more likely to be younger, with a lower level of education and a net household income below the poverty threshold. To our knowledge, this is the first study using a model-based approach to identify distinct subgroups of individuals reporting the use of prescribed OA on a population-based level in Germany. The results add further evidence to the knowledge that patients using prescribed OA are a heterogeneous group of individuals, many of whom are likely to have needs beyond pain management alone. It becomes clear that patients using prescribed OAs differ in their individual risk of pOUD.
When interpreting the findings in relation to previously published work, several of the results could be confirmed. For example, Cochran et al. also identified three subtypes of individuals using prescribed OA while analyzing community pharmacy data in southwestern Pennsylvania (20). Subgroups in this study were labeled as hazardous alcohol group, mental health group, and poor health group, and patients in the mental health group showed the highest risk of opioid misuse. Another study performing LCA among individuals using prescribed OA in the US population also identified a group with mental health issues, labeled as the depressed class (22). Patients in this class were more likely to be female which was in coincidence with the findings of the present study. In the same study, the authors found higher rates of pOUD in patients with comorbid psychopathological disorders. A link between mental disorders and a higher risk of pOUD was also found in other studies (17–19, 48, 49). These findings can be confirmed by the results of the present study, by showing a significant relationship between membership of the poor mental health group and a positive diagnosis of pOUD compared to the relatively healthy group. As in the present study individuals in the poor mental health group also showed signs of a higher prevalence of unemployment compared to patients in the relatively healthy group, this association could be confirmed by previous studies (50, 51).
As mental health problems and physical disorders often exacerbate each other and pain management, more sophisticated interdisciplinary therapy approaches are needed (20, 52, 53). Psychosocial interventions such as cognitive behavioral therapy, in combination with medical pain management, represent an important resource for patients in this subgroup (54). As individuals in this specific subgroup also showed a high prevalence of unemployment, additional linking of these patients to services in the community to address social determinants of health (e.g., vocational services) might be considered for enhancement of treatment (55). Our findings also indicated that individuals in the poor mental health group are more likely to be female, therefore gender-specific treatment programs should be considered in an integrated healthcare setting. This might lower the barriers for some individuals to access substance abuse treatment with enhancing overall treatment outcomes (56).
Identifying individuals in the poor mental health subgroup might enable early intervention strategies such as referral to specialized care for these patients (20, 57).
Besides mental health problems, the use of illicit drugs as well as alcohol abuse and smoking are also serious problems in pain patients taking prescription OA that are associated with a higher risk of pOUD (16, 19, 58–61). The results of the present study are in line with those of Afshar et al. who also detected a polysubstance group in hospitalized patients with opioid misuse (21). Patients in this subgroup also showed lower socioeconomic status, which could be confirmed by the present result of a very low net household income in the polysubstance group. Larger studies with sample sizes reaching from 19,000 to 26,000 individuals enrolled in substance abuse treatment programs also identified subtypes of individuals using prescribed OA with polysubstance use and therefore match our labeling for this group (62, 63). Patients in this subgroup might require access to comprehensive addiction services, such as professional addiction counseling and therapy, in addition to appropriate pain treatment. Further, the present findings indicate that patients in the polysubstance group differed significantly in sociodemographic factors compared with the relatively healthy group. Therefore, we strongly support the recommendation from the German S3 guideline “Medikamentenbezogene Störungen” [Medication-Related Disorders] for early screening for psychosocial and substance use characteristics at the very beginning of opioid therapy (64).
The present findings also identified a large group of patients using prescribed OA showing no noticeable behavioral, mental or physical health characteristics on most of the indicator variables. Due to moderate values on daily smoking and depression, this class was labeled as the relatively healthy group. However, these levels of depression and smoking are comparable to the general German population (65, 66). While Green et al. also identified a medically healthy subgroup in their analysis (63), individuals in the present analysis differed in low proportions of substance use (alcohol, cannabis, illicit drugs) and mental health problems. Statistical testing showed that patients in the relatively healthy group, relative to the other subgroups, also had the lowest proportion of a positive pOUD diagnosis (10.7%). Individuals in this subgroup reported the use of OA but hardly showed signs of poor health. It may be possible that these individuals had already overcome successful opioid therapy before answering the survey questionnaire. Assuming that pain reduction is the primary concern in these patients and appropriate medication adherence is ensured, this may lower the risk of pOUD.
Limitations
The present findings are subject to several limitations. As the data in the study are based on self-reports, validity is strongly dependent on the response behavior of the individuals interviewed. Biases resulting from lack of memory and response tendencies resulting from social desirability can neither be quantified nor excluded. Regarding the representativeness of the results, it should be noted that, with the present study design, certain population groups are not or hardly reached. These are mainly individuals older than 64 years, homeless people as well as inmates or people who are accommodated in medical institutions (67). The last category primarily concerns palliative patients. In the case of chronic and acute diseases, the influence of possible hospitalization is quite small as the survey periods lasted about 6 months.
Future studies should provide a deeper investigation into the variables that may help to predict pOUD. For instance, the duration of exposure, information about the pain condition treated, as well as information about who was the prescriber of the OA (i.e., specialty vs. general medical prescriber). Unfortunately, these questions were not possible to address in the current paper, because this data was not collected in either ESA wave.
Because of the pooling of two cross-sectional surveys, the participation of individuals in both ESA surveys cannot be fully excluded. The two-stage random sampling design, however, essentially eliminates this possibility.
Finally, there is also the possibility that people misusing their prescribed OA were included in our analysis sample, which might affect our findings regarding patients being treated for pain conditions. Although not completely impossible, the inclusion of individuals misusing opioids under a prescription regime is very unlikely given the rather strict German prescription regulations (64).
Conclusion
The findings of the present study add new evidence to the classification of individuals using prescribed OA and the prevalence of pOUD on a nationally representative level in Germany. Two specific subgroups with a high prevalence of pOUD, labeled as the poor mental health group and polysubstance group were identified. While individuals in the poor mental health group were more likely to be female and unemployed, patients in the polysubstance group were marked by younger age with a low level of education and a net household income below the poverty threshold. Clinicians treating patients in opioid therapy should be aware of these specific subtypes and their highly related risk of pOUD during medical history. Using data-based approaches to delineate patient subgroups from different data sources is highly recommended in further research to gain urgently needed insight into subtype characteristics. Stratification of these subtypes enables targeted early intervention from a clinical as well as a public health perspective.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.esa-survey.de/ergebnisse/datenzugang.html.
Ethics Statement
The studies involving human participants were reviewed and approved by German Psychological Society (DGPs). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
CR analyzed and interpreted the data and wrote the initial draft of the manuscript. LK designed the study. All authors gave important feedback in revising the manuscript, commented on various versions of the article, and approved the final version.
Funding
The Epidemiological Survey of Substance Abuse (ESA) was supported by funding from the German Federal Ministry of Health (project no. ZMVI1-2520DSM203).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.918371/full#supplementary-material
References
2. Ballantyne JC. Opioid therapy in chronic pain. Phys Med Rehabil Clin N Am. (2015) 26:201–18. doi: 10.1016/j.pmr.2014.12.001
3. Belzak L, Halverson J. The opioid crisis in Canada: a national perspective. Health Promot Chronic Dis Prev Can. (2018) 38:224–33. doi: 10.24095/hpcdp.38.6.02
4. Schubert I, Ihle P, Sabatowski R. Increase in opiate prescription in Germany between 2000 and 2010: a study based on insurance data. Dtsch Arztebl Int. (2013) 110:45–51. doi: 10.3238/arztebl.2013.0045
5. Buth S, Holzbach R, Rosenkranz M, Verthein U. The use of prescription drugs with dependence potential in Germany: a prospective analysis of prescriptions in the public healthcare system between 2006 and 2010. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2017) 60:865–72. doi: 10.1007/s00103-017-2571-4
6. Rosner B, Neicun J, Yang JC, Roman-Urrestarazu A. Opioid prescription patterns in Germany and the global opioid epidemic: systematic review of available evidence. PLoS ONE. (2019) 14:e0221153. doi: 10.1371/journal.pone.0221153
7. Verthein U, Buth S, Daubmann A, Martens MS, Schulte B. Trends in risky prescriptions of opioid analgesics from 2011 to 2015 in Northern Germany. J Psychopharmacol. (2020) 34:1210–17. doi: 10.1177/0269881120936544
8. Buth S, Holzbach R, Martens M-S, Neumann-Runde E, Meiners O, Verthein U. Problematic medication with benzodiazepines, “Z-drugs”, and opioid analgesics. Dtsch Arztebl Int. (2019) 116:607–14. doi: 10.3238/arztebl.2019.0607
9. Reinecke H, Weber C, Lange K, Simon M, Stein C, Sorgatz H. Analgesic efficacy of opioids in chronic pain: recent meta-analyses. Br J Pharmacol. (2015) 172:324–33. doi: 10.1111/bph.12634
10. Els C, Jackson TD, Hagtvedt R, Kunyk D, Sonnenberg B, Lappi VG, et al. High-dose opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database Syst Rev. (2017) 10:CD012299. doi: 10.1002/14651858.CD012299
11. Wolter D. Schmerzen und Schmerzmittelabhängigkeit im Alter. Die Gerontopsychiatrische Perspektive. Stuttgart: Kohlhammer (2017).
12. Just JM, Scherbaum N, Specka M, Puth MT, Weckbecker K. Rate of opioid use disorder in adults who received prescription opioid pain therapy-a secondary data analysis. PLoS ONE. (2020) 15:e0236268. doi: 10.1371/journal.pone.0236268
13. Marschall U, L'Hoest H, Radbruch L, Hauser W. Long-term opioid therapy for chronic non-cancer pain in Germany. Eur J Pain. (2016) 20:767–76. doi: 10.1002/ejp.802
14. Wu L-T, Woody GE, Yang C, Blazer DG. Subtypes of nonmedical opioid users: results from the national epidemiologic survey on alcohol and related conditions. Drug Alcohol Depend. (2010) 112:69–80. doi: 10.1016/j.drugalcdep.2010.05.013
15. Häuser W. 2. Aktualisierung der S3 Leitlinie “Langzeitanwendungen von Opioiden bei chronischen nicht-tumorbedingten Schmerzen” LONTS. Der Schmerz. (2020) 34:204–44. doi: 10.1007/s00482-020-00472-y
16. Turk DC, Swanson KS, Gatchel RJ. Predicting opioid misuse by chronic pain patients: a systematic review and literature synthesis. Clin J Pain. (2008) 24:497–508. doi: 10.1097/AJP.0b013e31816b1070
17. Rice JB, White AG, Birnbaum HG, Schiller M, Brown DA, Roland CL. A model to identify patients at risk for prescription opioid abuse, dependence, and misuse. Pain Med. (2012) 13:1162–73. doi: 10.1111/j.1526-4637.2012.01450.x
18. Edlund MJ, Steffick D, Hudson T, Harris KM, Sullivan M. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. (2007) 129:355–62. doi: 10.1016/j.pain.2007.02.014
19. Edlund MJ, Martin BC, Fan MY, Devries A, Braden JB, Sullivan MD. Risks for opioid abuse and dependence among recipients of chronic opioid therapy: results from the TROUP study. Drug Alcohol Depend. (2010) 112:90–8. doi: 10.1016/j.drugalcdep.2010.05.017
20. Cochran G, Hruschak V, Bacci JL, Hohmeier KC, Tarter R. Behavioral, mental, and physical health characteristics and opioid medication misuse among community pharmacy patients: a latent class analysis. Res Soc Administr Pharm. (2017) 13:1055–61. doi: 10.1016/j.sapharm.2016.11.005
21. Afshar M, Joyce C, Dligach D, Sharma B, Kania R, Xie M, et al. Subtypes in patients with opioid misuse: a prognostic enrichment strategy using electronic health record data in hospitalized patients. PLoS ONE. (2019) 14:e0219717. doi: 10.1371/journal.pone.0219717
22. De Nadai AS, Little TB, McCabe SE, Schepis TS. Diverse diagnostic profiles associated with prescription opioid use disorder in a nationwide sample: one crisis, multiple needs. J Consult Clin Psychol. (2019) 87:849–58. doi: 10.1037/ccp0000429
23. IFT Institut für Therapieforschung München. Der Epidemiologische Suchtsurvey. (2022). Available online at: https://www.esa-survey.de/ (accessed February 26, 2022).
24. Gelman A, Carlin J. Poststratification and weighting adjustments. In: Groves R, Dillman D, Eltinge J, Little R, editors. Survey Nonresponse. New York, NY: Wiley (2002). p. 289–303.
25. Votaw VR, McHugh RK, Witkiewitz K. Alcohol use disorder and motives for prescription opioid misuse: a latent class analysis. Subst Use Misuse. (2019) 54:1558–68. doi: 10.1080/10826084.2019.1594904
26. John WS, Zhu H, Mannelli P, Subramaniam GA, Schwartz RP, McNeely J, et al. Prevalence and patterns of opioid misuse and opioid use disorder among primary care patients who use tobacco. Drug Alcohol Depend. (2019) 194:468–75. doi: 10.1016/j.drugalcdep.2018.11.011
27. Olfson M, Wall MM, Liu SM, Blanco C. Cannabis use and risk of prescription opioid use disorder in the United States. Am J Psychiatry. (2018) 175:47–53. doi: 10.1176/appi.ajp.2017.17040413
28. Cochran G, Rosen D, McCarthy RM, Engel RJ. Risk factors for symptoms of prescription opioid misuse: do older adults differ from younger adult patients? J Gerontol Soc Work. (2017) 60:443–57. doi: 10.1080/01634372.2017.1327469
29. Cochran G, Bacci JL, Ylioja T, Hruschak V, Miller S, Seybert AL, et al. Prescription opioid use: patient characteristics and misuse in community pharmacy. J Am Pharm Assoc. (2016) 56:248–56.e6. doi: 10.1016/j.japh.2016.02.012
30. Brown JL, Cochran G, Bryan MA, Charron E, Winhusen TJ. Associations between elevated depressive symptoms and substance use, prescription opioid misuse, overdose history, pain, and general health among community pharmacy patients prescribed opioids. Subst Abuse. (2022) 43:1110–5. doi: 10.1080/08897077.2022.2060450
31. Groenewald CB, Law EF, Fisher E, Beals-Erickson SE, Palermo TM. Associations between adolescent chronic pain and prescription opioid misuse in adulthood. J Pain. (2019) 20:28–37. doi: 10.1016/j.jpain.2018.07.007
32. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. Audit. The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care. Geneva: World Health Organization (2001).
33. Rist F, Scheuren B, Demmel R, Hagen J, Aulhorn I. Der Münsteraner Alcohol Use Disorders Identification Test (AUDIT-GM). Mannheim: Zentrum für Umfragen, Methoden und Analysen e.V (2003).
34. Conigrave KM, Hall WD, Saunders JB. The AUDIT questionnaire: choosing a cut-off score. Alcohol Use Disorder Identification Test. Addiction. (1995) 90:1349–56. doi: 10.1111/j.1360-0443.1995.tb03552.x
35. Wittchen H-U, Beloch E, Garczynski E, Holly A, Lachner G, Perkonigg A, et al. Manual zum Münchener Composite International Diagnostic Interview (M-CIDI, Paper-Pencil 2.0, 1/95). München: Max-Planck-Institut für Psychiatrie, Kunisches Institut (1995).
36. Lachner G, Wittchen H-U, Perkonigg A, Holly A, Schuster P, Wunderlich U, et al. Structure, content and reliability of the Munich-Composite International Diagnostic Interview (M-CIDI) substance use sections. Eur Addict Res. (1998) 4:28–41. doi: 10.1159/000018922
38. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-5. 5th ed. Arlington, VA: American Psychiatric Publishing (2013).
39. Schroedter JH, Lechert Y, Lüttinger P. Die Umsetzung der Bildungsskala ISCED-1997 für die Volkszählung 1970, die Mikrozensus-Zusatzerhebung 1971 und die Mikrozensen 1976-2004 (Version 1). (ZUMAMethodenbericht, 2006/08) (2006). Mannheim: Zentrum für Umfragen, Methoden und Analysen -ZUMA-. Available online at: https://www.ssoar.info/ssoar/bitstream/handle/document/26239/ssoar-2006-schroedter_et_al-die_umsetzung_der_bildungsskala_isced-1997.pdf?sequence=1 (accessed March 31, 2022).
40. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equat Model Multidiscipl J. (2007) 14:535–69. doi: 10.1080/10705510701575396
41. Finch WH, Bronk KC. Conducting confirmatory latent class analysis using Mplus. Struct Equat Model Multidiscip J. (2011) 18:132–51. doi: 10.1080/10705511.2011.532732
42. Weller BE, Bowen NK, Faubert SJ. Latent class analysis: a guide to best practice. J Black Psychol. (2020) 46:287–311. doi: 10.1177/0095798420930932
43. Porcu M, Giambona F. Introduction to latent class analysis with applications. J Early Adolesc. (2017) 37:129–58. doi: 10.1177/0272431616648452
44. Collins LM, Lanza ST. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences. Hoboken, NJ: John Wiley & Sons Inc. (2010).
45. Geiser C. Data Analysis With Mplus [Original title: Datenanalyse mit Mplus]. Wiesbaden: VS Verlag für Sozialwissenschaften (2010).
48. Bedene A, Lijfering WM, Niesters M, van Velzen M, Rosendaal FR, Bouvy ML, et al. Opioid prescription patterns and risk factors associated with opioid use in the Netherlands. JAMA Netw Open. (2019) 2:e1910223. doi: 10.1001/jamanetworkopen.2019.10223
49. Volkow ND, Jones EB, Einstein EB, Wargo EM. Prevention and treatment of opioid misuse and addiction: a review. JAMA Psychiatry. (2019) 76:208–16. doi: 10.1001/jamapsychiatry.2018.3126
50. Amiri S. Unemployment associated with major depression disorder and depressive symptoms: a systematic review and meta-analysis. Int J Occup Saf Ergon. (2021) 1–13. doi: 10.1080/10803548.2021.1954793
51. Compton MT, Shim RS. The social determinants of mental health. Focus. (2015) 13:419–25. doi: 10.1176/appi.focus.20150017
52. Hooten WM. Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. (2016) 91:955–70. doi: 10.1016/j.mayocp.2016.04.029
53. Goesling J, Lin LA, Clauw DJ. Psychiatry and pain management: at the intersection of chronic pain and mental health. Curr Psychiatry Rep. (2018) 20:12. doi: 10.1007/s11920-018-0872-4
54. Hruschak V, Cochran G, Wasan AD. Psychosocial interventions for chronic pain and comorbid prescription opioid use disorders: a narrative review of the literature. J Opioid Manag. (2018) 14:345–58. doi: 10.5055/jom.2018.0467
55. McGinty EE, Daumit GL. Integrating mental health and addiction treatment into general medical care: the role of policy. Psychiatr Serv. (2020) 71:1163–9. doi: 10.1176/appi.ps.202000183
56. Green CA. Gender and use of substance abuse treatment services. Alcohol Res Health. (2006) 29:55–62.
57. Cochran G, Field C, Lawson K. Pharmacists who screen and discuss opioid misuse with patients: future directions for research and practice. J Pharm Pract. (2015) 28:404–12. doi: 10.1177/0897190014522064
58. Webster LR. Risk factors for opioid-use disorder and overdose. Anesth Analg. (2017) 125:1741–8. doi: 10.1213/ANE.0000000000002496
59. Lin LA, Bohnert ASB, Blow FC, Gordon AJ, Ignacio RV, Kim HM, et al. Polysubstance use and association with opioid use disorder treatment in the US Veterans Health Administration. Addiction. (2021) 116:96–104. doi: 10.1111/add.15116
60. Cheatle MD, Falcone M, Dhingra L, Lerman C. Independent association of tobacco use with opioid use disorder in patients of European ancestry with chronic non-cancer pain. Drug Alcohol Depend. (2020) 209:107901. doi: 10.1016/j.drugalcdep.2020.107901
61. Young-Wolff KC, Klebaner D, Weisner C, Von Korff M, Campbell CI. Smoking status and opioid-related problems and concerns among men and women on chronic opioid therapy. Clin J Pain. (2017) 33:730–7. doi: 10.1097/AJP.0000000000000461
62. Fong C, Matusow H, Cleland CM, Rosenblum A. Characteristics of non-opioid substance misusers among patients enrolling in opioid treatment programs: a latent class analysis. J Addict Dis. (2015) 34:141–50. doi: 10.1080/10550887.2015.1059226
63. Green TC, Black R, Grimes Serrano JM, Budman SH, Butler SF. Typologies of prescription opioid use in a large sample of adults assessed for substance abuse treatment. PLoS ONE. (2011) 6:e27244. doi: 10.1371/journal.pone.0027244
64. Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde, (DGPPN), Deutsche Gesellschaft für Suchtforschung und Suchttherapie, (DG-Sucht). S3-Leitlinie Medikamentenbezogene Störungen – 1. Auflage. Version 01, 2020 (2021). Available online at: https://www.awmf.org/uploads/tx_szleitlinien/038-025l_S3_Medikamtenbezogene-Stoerungen_2021-01.pdf (accessed February 21, 2022).
65. Wittchen H-U, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jönsson B, et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. (2011) 21:655–79. doi: 10.1016/j.euroneuro.2011.07.018
66. Atzendorf J, Rauschert C, Seitz NN, Lochbühler K, Kraus L. The use of alcohol, tobacco, illegal drugs and medicines: an estimate of consumption and substance-related disorders in Germany. Dtsch Arztebl Int. (2019) 116:577–84. doi: 10.3238/arztebl.2019.0577
Keywords: opioid analgesics, opioid use disorder, prescription, latent class analysis, epidemiological survey, DSM-5
Citation: Rauschert C, Seitz N-N, Olderbak S, Pogarell O, Dreischulte T and Kraus L (2022) Subtypes in Patients Taking Prescribed Opioid Analgesics and Their Characteristics: A Latent Class Analysis. Front. Psychiatry 13:918371. doi: 10.3389/fpsyt.2022.918371
Received: 12 April 2022; Accepted: 01 June 2022;
Published: 08 July 2022.
Edited by:
Matthew S. Ellis, Washington University in St. Louis, United StatesReviewed by:
Dieter J. Meyerhoff, University of California, San Francisco, United StatesCaitlin Martin, Virginia Commonwealth University, United States
Mary Jo Larson, Brandeis University, United States
Copyright © 2022 Rauschert, Seitz, Olderbak, Pogarell, Dreischulte and Kraus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ludwig Kraus, bHVkd2lnLmtyYXVzQHN1LnNl