
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 04 July 2022
Sec. Psychological Therapy and Psychosomatics
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.915327
This article is part of the Research TopicPsychocardiology: Exploring the Brain-Heart InterfaceView all 27 articles
 Scarlett Anthony1†
Scarlett Anthony1† Rebecca Harrell1†Caroline Martin1†
Rebecca Harrell1†Caroline Martin1† Taylor Hawkins2Saleen Khan2Aditi Naniwadekar2†
Taylor Hawkins2Saleen Khan2Aditi Naniwadekar2† Samuel F. Sears1,2*†
Samuel F. Sears1,2*†Background: Atrial fibrillation occurs when rapid and disorganized electrical signals cause the atria in the heart to beat irregularly and is associated with an increased risk for stroke. Despite medical advancements, first and second line atrial fibrillation treatments exhibit significant recurrence rates. Because of this, atrial fibrillation patients often experience disease-specific fears that are not routinely assessed and targeted in clinical management. Fear of recurrence models in cancer research and other cardiac-specific fears have paved the way for a patient-centric approach to disease intervention.
Purpose: Clinical assessment focused solely on the taxonomy of anxiety disorders may miss key components unique to the atrial fibrillation patient experience. An anxiety disorder diagnosis in the presence of an arrhythmia could be misleading and ultimately fail to address patient needs. Modeled from the cancer literature, providers may benefit from a broader disease specific conceptualization for AF patients that differs from a general DSM-5 diagnosis.
Aims: The objectives of this paper are: (1) to review the medical aspects of atrial fibrillation, (2) to examine the comparability of fear of recurrence concept from cancer literature to the atrial fibrillation patient, and (3) to suggest considerations of these novel concepts in patient care.
Future Directions: Increased understanding of fear of recurrence among atrial fibrillation patients aims to define and assess fear of recurrence components, determine treatment targets, and ultimately improve patient outcomes.
Consultation liaison psychiatrists and psychologists are often called to the bedside or clinic room of a medical patient coping with multiple health challenges. The use of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5, (1)] provides the blueprint for examining psychological disorders and making diagnoses. As the evidence base grows for the psychological aspects of chronic diseases, mental health professionals are faced with evaluating patients with significant anxieties that are either consistent with, or part of, the disease process. This scenario presents a significant challenge for providers as the manifestations of disease-specific fears may be difficult to diagnose and, therefore, unresponsive to traditional treatment recommendations for DSM-5-defined anxiety disorders. Even so, illness-related anxieties surrounding fears of symptoms or conditions worsening are common for individuals with chronic conditions (2). Patients presenting with cardiac arrhythmias may experience spontaneous palpitations, shortness of breath, exercise intolerance, and other discomforts that mimic anxiety disorders. Nonetheless, the diagnosis of an anxiety disorder in the presence of an arrhythmia with similar symptoms could be misleading.
Psycho-oncology literature has rapidly deployed cancer-specific constructs in an effort to understand the patient experience of the unique aspects of living with cancer. The juxtaposition of cancer and cardiac disease constructs to describe the disease experience may provide complementary insights, as both conditions have significant impacts on perceived health and longevity, disease burden, life interruption, multiple treatment modalities, and recurrent follow-up care. Both disease states have disease-specific fears that involve patients navigating the health care system, while feeling poorly, and managing future threats. As a result, perceptions and expectations of the future become an important aspect for both disease states–specifically around the phenomenon of fear of recurrence (FoR).
Consulting psychiatrists and psychologists may increasingly be referred patients with AF. The purposes of this paper are: 1) to review the medical aspects of atrial fibrillation, 2) to examine the comparability of FoR concept from cancer literature to the AF patient, and 3) to apply these novel concepts in patient care.
Atrial fibrillation (AF) occurs when rapid and disorganized electrical signals cause the atria in the heart to irregularly beat, restricting blood flow from the atria to the ventricles (3). Over time, AF can decrease the heart's pumping ability which can lead to heart failure and is also associated with an increased risk of stroke or systemic embolism (4). In the United States alone, roughly 3 to 6 million people are impacted by AF with domestic and global prevalence expected to increase to 12.1 million by 2030 and up to 17.9 million by 2050 in Europe (5–7). Individuals aged 65 years and older are most likely to be diagnosed with AF, however, it can occur among younger patients especially if precipitated by other cardiac risk factors (e.g., hypertension, premorbid cardiovascular conditions, lifestyle and behavioral risk factors) or familial predisposition (8). Before the age of 75, men are more often diagnosed with AF compared to women (9), although women exhibit elevated risk of adverse events and AF incidence and burden (10–12). Similar patterns are demonstrated among Black and Brown patient populations with lower overall AF prevalence, but greater risk for heightened symptom burden and adverse events (13).
Presentation of AF can also vary significantly among individuals, and the presentations are categorized as paroxysmal AF (e.g., AF episodes occur spontaneously for less than a week and are often responsive to first- or second-line treatments), persistent AF (e.g., episodes occur for longer than a week and require additional intervention), and permanent AF (e.g., chronic irregular heart rhythm often unresponsive to repeated interventions). Typical symptoms reported by AF patients across all presentations include heart palpitations, lightheadedness/dizziness, tiredness/fatigue, shortness of breath, and chest pain (14). Interestingly, as much as 39% of AF patients report never having experienced any AF symptoms (15). Irrespective of symptom reporting, worsened disease progression (e.g., moving from paroxysmal to persistent to permanent presentations) can occur among AF patients with poorly managed co-morbid conditions, significant psychological distress, and behavioral risk factors among the most vulnerable (10).
The comprehensive treatment of atrial fibrillation requires multidisciplinary collaboration and includes primordial anti-arrhythmic and rate control agents, catheter ablation, and lifestyle management (16). The first-line treatment option for patients requires consideration of risk factors, duration of atrial fibrillation, left atrial fibrosis, and other individual factors (17, 18). Further, the introduction of direct oral anticoagulants and the addition of left atrial appendage occlusion devices have increased the effectiveness and safety profile of stroke prophylaxis in AF. Recurrence of atrial fibrillation while taking antiarrhythmic agents is close to 40–70%, compared to 20–50% with ablation (18, 19). Initial antiarrhythmic drug therapy can reduce recurrent AF episodes for some patients; however, catheter ablation interventions have demonstrated effectiveness at reducing recurrence risk (19, 20). Even so, ablative interventions do not significantly reduce risk of adverse events when compared to pharmacological treatments (20), and in 1 year following ablation and cardioversion, up to 40% of people can still have recurrence [despite anti-arrhythmic medications (21)].
Despite all of the advancements in the treatment paradigm of atrial fibrillation, some patients can remain focused on AF recurrence with each of these approaches (22, 23). While some patients may never experience recurrence of an AF episode after the initial treatment, variables such as obesity, thyroid abnormalities, alcohol consumption and obstructive sleep apnea have all been closely linked to increased probability of recurrence of AF (24). Given the notable probability for recurrent AF episodes following first and second-line treatments and the behavioral link, identifying the role of recurrence possibility for patients is critical. Thus, contemporary management of atrial fibrillation is multi-pronged: reduction of stroke risk, prevention of AF incidents with medical, surgical, or electrical means, and reduction of recurrence to promote comprehensive symptom relief with aggressive risk factor modifications (16, 19, 22).
FoR refers to specific anxiety among medical patients with episodic disease bouts of varying intensity and causality that are resistant to forecast. In the US, cancer accounted for nearly 10 million deaths in 2020 (25) compared to approximately 26,000 caused by AF (26). Despite this difference in mortality, the possibility for adverse events (e.g., stroke and premature death) is also prominent in AF patient populations (5), and, as such, it appears that the emotional dimensions and behavioral implications of these conditions share some similarities. Similar to cancer patients in remission, AF patients may exhibit significant fears related to the possibility of recurrence. Specifically, AF symptoms and recurring episodes due to high rates of AF recurrence are anticipated by patients (27).
While this concept has yet to be translated to understanding the AF patient experience, both FoR models in cancer research and prior research regarding other well-defined cardiac-specific fears (e.g., ICD shock anxiety) have taken a two-factor approach to understanding patient fears–examining both fear of antecedents and consequences (28, 29). Similarly, (30) have recently utilized a cancer model as a framework for understanding recurrence fears among patients following acute coronary syndromes (ACS). Birk and colleagues are currently examining its impact on medication adherence and physical activity engagement in a randomized trial targeting patients fears vs. usual care. While this work will help better inform the feasibility of transferring cancer-informed ideas about FoR to cardiac populations and how to treat it, conceptualization of AF patient fears maybe more specific and centered around the AF patient experience. Clinical care of FoR among cancer patients spans reliable assessment, psychoeducation, signs and symptoms, and cognitive behavioral therapy (CBT) strategies for risk reduction and follow-up (31). Similar action-oriented interventions can be integrated into AF patient care to better target specific fears and produce considerable patient benefit.
Within populations of cancer survivors, it is estimated that roughly 30–70% of patients endorse having moderate to severe levels of recurrence fears that can persist for years following diagnosis (32). Models of FoR generally involve antecedent and consequence-focused specific fears of cancer relapse. These models have proposed that patient perception of physical sensations and identification of symptoms often serve as a trigger for elevated fears that can result in increased symptom reporting, significant psychological distress, feelings of hopelessness, and diminished quality of life (32, 33). In addition, FoR among cancer survivors has been linked to increased depressive symptoms, frequent rumination, and impairment in functioning (34). Fear of recurrence has also been associated with heightened death anxiety and intrusive and threatening thoughts about death and dying (35, 36). Patients who have experienced disease recurrence exhibit heightened fear of disease progression and fear of loss of autonomy and related emotional distress (37).
Behavioral impacts of FoR generally occur on a spectrum–with some patients becoming hypervigilant about their health (i.e., over-utilization of health care, constantly monitoring symptoms and displaying control-seeking behaviors), while others become avoidant [i.e., missing routine appointments, avoiding necessary testing, non-adherence to medications and treatment regimens; (32, 34, 38)]. Differences in FoR in cancer survivors have also emerged in regard to gender with women experiencing FoR at higher rates than men (39). In addition, patients with lower education, decreased income, and younger age are also more likely to experience FoR following cancer remission. Even so, a pattern exists between high FoR and diminished engagement in health behaviors, such as physical activities like walking or running (40). The body of literature for cancer patients is substantial, and many of these specific fears (and manifestations) are mirrored in the AF patient experience.
FoR in AF populations can also be understood as a two-factor concept-composed of both patient fears around antecedents (e.g., fear of activities that could trigger an AF episode) and consequences (e.g., fear of what may happen if an AF episode occurs). In other words, specific to this population, FoR can be conceptualized as cognitions and behaviors associated with either fear of triggering an AF episode or fear of the potential consequences of AF recurrence. Interestingly, recent research has demonstrated that only alcohol use was a reliable trigger in a study utilizing patient selected triggers for AF (41), suggesting that commonly held ideas about the triggers of caffeine, reduced sleep, exercise, lying on the left side, dehydration, large meals, and other customized triggers were not associated with the occurrence of AF.
While the concept of FoR can be theorized into two distinct components, it is important to recognize that FoR is multidimensional and encompasses patient-perceived possible triggers, emotions, thoughts, behavioral reactions, and coping strategies (see Table 1). Additional value or utility of FoR includes that cardiac providers would likely be comfortable reviewing the chances and the impact of AF recurrence. Identifying patients with high FoR for AF would allow for more targeted patient education, whereas addressing more general anxiety would likely not be as responsive to patient education. Moreover, recent constructs, such as confidence in living with AF (42), provide cardiac clinics with other patient centered metrics to evaluate positive or desirable aspects of the patient experience as well. Taken together, increased theory and metrics of the AF patient experience can address both fears and the initiation of empowerment.
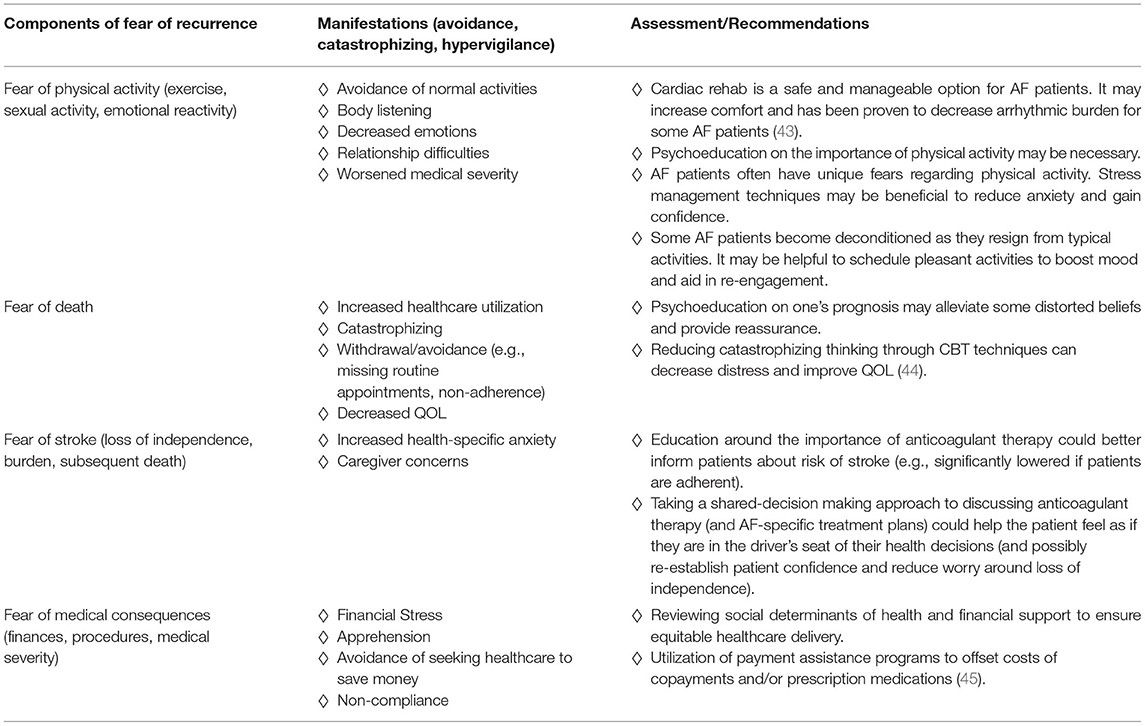
Table 1. Signs, symptoms, and steps for identifying and targeting AF patient fears.
The patient experience of AF symptoms has long included a curious component with a significant portion of patients (approximately 39%) reporting that they were asymptomatic (15). Objective metrics of the presence of AF allow for examination of both the objective and subjective components of AF symptoms. This research suggested that negative emotions were more strongly associated with AF symptom score than the presence of device-detected AF (46). More recently, observational studies using serial assessment of AF patients in a specialty clinic demonstrated that depression and anxiety were the best predictors of AF symptom severity and that symptom severity was associated with increased costs and healthcare utilization (47). These data further necessitate understanding the psychological aspects of AF symptom reporting and the AF patient experience.
Approximately 28–38% of AF patients experience significant depressive or anxious symptoms (11, 48), and the interrelationships between these symptoms and AF are multidimensional and complex (49). Those patients taking the anti-coagulant, warfarin, as a method for stroke prevention are also at an increased risk of depressive symptoms and dementia (50). These high rates of emotional reactivity may be attributed to AF specific fears, consequences, and demanded psychological adjustment (51). The combination of uncertainties regarding the cause, symptom presentation, treatment options, and outcomes of AF can be overwhelming for patients (52). AF on its own is not typically life threatening, however, AF increases the risk of stroke by nearly five times and is the most commonly reported fear by AF patients, and for good reason (53, 54). Those patients with both AF and history of stroke experience increased rates of medical and neurological complications and are more likely to face consequences such as disability and even death when compared to stroke patients without AF (55–57). The current assessment of fear of stroke revolves largely around physical functioning (e.g., mobility, memory and thinking, communication, etc.) and emotional impacts following the event rather than future, stroke-related fears (58). In addition to fear of stroke, death anxiety is a salient fear in those with chronic conditions such as AF (59, 60) and refers to feelings of discomfort, worry, or fear that may follow becoming aware of one's own mortality (61). Death anxiety in patients has been shown to be negatively related to quality of life; that is, those with higher levels of death anxiety often experience poorer quality of life (62). Collectively, psychological well-being can strongly impact AF symptom severity and patient healthcare utilization (63).
Similar patterns in individual and group differences identified in research regarding FoR in cancer populations may also be reflected in AF patient populations. For instance, women living with AF consistently exhibit higher rates of depression and anxiety, increased incidence of physical AF symptoms and symptom burden, and decreased quality of life when compared to their male counterparts (11, 44, 64–66). In addition, younger AF patients (i.e., <60 years old) are seemingly more impacted by health-related stress and experience depression and anxiety at higher rates than older patients (65). Patients with lower SES and diminished access to resources are at increased risk for elevated AF symptom burden and adverse events [e.g., premature death, heart failure, MI, and stroke; (67)]. Interestingly, although female patients have demonstrated diminished quality of life and worse symptoms, they are less likely to seek secondary AF treatment such as catheter ablations (68), and as such, may be particularly vulnerable to continued psychological concerns. Moreover, it is likely that women, patients of lower SES (and lower access to resources and health literacy), and younger age are also at increased risk for developing AF-specific fears contributing to worse outcomes–a notion echoed in cancer FoR literature.
The importance of patient understanding and adherence to the medical regimen is common across chronic diseases and can prompt a set of changes spanning behavioral, emotional, and medical challenges (69).
For the AF patient, ongoing clinical care includes the management of the risk factors of AF, such as adherence to medical management (e.g., rate control, rhythm control, blood pressure control, and stroke prophylaxis) and engagement in risk reduction behaviors (e.g., weight management, abstinence from smoking, avoiding or minimizing alcohol consumption, and participation in regular physical activity) (70).
Even a quick review of these risk behaviors would indicate that many of these changes are indicated as part of a healthy lifestyle for all patients. The progression of AF can be associated with the presence and combination of behavioral risk factors, and young-onset individuals may even have risk factors that are maintaining their condition (71). However, the challenges for AF patients are multiplicative because existing research in both China and in Europe suggest that as few as 4% of AF patients are engaged in a fully “healthy lifestyle” (72). Some modifiable risk factors have been shown to have distinct associations with atrial fibrillation (e.g., alcohol consumption, being overweight/obese, smoking) and the cumulative impact poses significant risk for these patients [Di (73)]. Successes and failures at making these lifestyle changes often chip away at patients' perceptions of control, daily planning to engage in valued activities, and life itself (74). Many patients fear that physical activity may trigger an AF episode which initiates a behavioral avoidance pattern to exercise/exertion (75). Finding meaning in AF symptoms, trying to “stay clear” of AF episodes, and managing unpredictable and functional limits are also common behavioral responses that can translate into increased distress and worsened quality of life (76).
A common goal of AF patient care among psychiatrists and psychologists typically involves determining if an anxiety disorder diagnosis is warranted and then providing typical recommendations or a referral for the treatment of an anxiety disorder. Considering the specificity of AF patient experiences, it may not be ideal to pursue general anxiety disorders for these patients. Although some symptoms may overlap, patient concerns are often specifically related to AF symptoms and risk factors. Moreover, a simple phobia diagnosis also does not fit the phenomena well. Many AF patients' “approach” the fear of irregular heartbeat constantly by seeking information and diagnostics in an attempt to detect AF. Similar to routine care among cancer patients, psychiatrists and psychologists can assess for FoR, provide adequate medical information, discuss signs and symptoms of recurrence, normalize patient fears, implement strategies, and provide a plan for follow-up (31). AF patients could likely benefit from a similar action-oriented plan encompassing their individual fears and providing specific treatment plans as needed for the future. The activation of therapeutic interventions, such as exercise programs, alcohol reduction, and OSA management, would be expected to be exceedingly more beneficial than a diagnosis alone.
Each AF patient likely has a unique combination of the established components of FoR in AF. It is common for AF patients to experience a spectrum of disease-specific fears such as fear of exercise, fear of death, fear of stroke, and fear of other medical consequences. Table 1 consists of these components of fear of recurrence, manifestations of those fears, and recommendations for each.
Specific action plans that can be efficiently established during regularly scheduled appointments can improve patient outcomes, improve rapport, and decrease healthcare utilization for AF patients.
The FoR model in AF is proposed to give consultation liaison psychiatrists and psychologists a broader disease-specific conceptualization related to the AF patient experience, beyond traditional anxiety disorders in AF patients in hopes to improve patient outcomes. The FoR concept in cancer has proven useful for targeting and reducing disease-specific fears among cancer patients. A similar model for AF patients may also provide utility for consultation liaison psychiatrists and psychologists to recognize and address similar fears in the AF patient. In turn, the aim is to help advance provider assessment of FoR components, possible presentations and manifestations, and specific fears that can be targeted in AF management plans. The importance of this work is highlighted in that many patients may feel misunderstood or disregarded when their fears are not recognized by providers and instead receive anxiety disorder diagnoses that are not representative of their experience (77). Overall, FoR assessment can help normalize the patient experience and provide education around rationality of fears. In addition, it can help patients balance the risk and benefits of engaging in previously feared behaviors necessary for proper AF management (e.g., physical activity). It is our belief that AF patient care involves a commitment to understanding unique patient fears outside of what can be defined by the DSM-5. We can borrow from cancer FoR assessment strategies to inform AF care by addressing disease-specific fears.
Tailored treatment therapies from FoR in cancer should also be further evaluated for applicability to help target AF patients' shared experiences. A growing number of therapeutic interventions have demonstrated effectiveness in managing FoR among cancer patients (31). Psychological interventions (e.g., CBT interventions) have been identified as efficacious treatments for alleviating FoR among cancer survivors with effects immediately following intervention and at follow-up periods. Of note, contemporary CBT interventions have demonstrated greater efficacy in treating FoR than traditional CBT interventions, indicating that treatments aimed at altering how individuals relate to inner experiences (e.g., worry, rumination, etc.) are especially advantageous (34). Similar strategies spanning behavioral, psychological, and cognitive concerns can be translated into AF-specific clinical care to improve patient outcomes. As a first step to targeted target, we are currently developing and testing a measure assessing AF FoR informed by the model presented in the current paper. This model intends to provide a blueprint for further assessment and future treatments in hopes to improve the AF experience.
SA contributed to the conceptualization with support from SS, RH, CM, SK, TH, and AN. SS, SA, and RH contributed to visualization. SS, SA, RH, CM, TH, and SK contributed to the writing—original draft. SA, SS, RH, TH, SK, and AN contributed to writing—review and editing. SS supervised the writing of this article. All authors contributed to the article and approved the submitted version.
SS serves as a consultant to Medtronic, Abbott, Milestone Pharmaceutical, and Zoll Medical. He has received honorarium from Medtronic, Biotronik, and Zoll Medical in the past 12 months.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Publishing (2013).
2. Lebel S, Mutsaers B, Tomei C, Leclair CS, Jones G, Petricone-Westwood D, et al. Health anxiety and illness-related fears across diverse chronic illnesses: a systematic review on conceptualization, measurement, prevalence, course, and correlates. PLoS ONE. (2020) (15, 7:234124. doi: 10.1371/journal.pone.0234124
3. Wang X, Fu Q, Song F, Li W, Yin X, Yue W, et al. Data on prevalence of atrial fibrillation and its association with stroke in low-, middle-, and high-income regions of China. Data in Brief. (2018) 19:1822–7. doi: 10.1016/j.dib.2018.06.082
4. Olson NC, Cushman M, Judd SE, McClure LA, Lakoski SG, Folsom AR. American Heart Association's Life's Simple 7 and risk of venous thromboembolism: the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. J Am Heart Assoc. (2015) 4:e001494 doi: 10.1161/JAHA.114.001494
5. D'Souza A, Butcher KS, Buck BH. The multiple causes of stroke in atrial fibrillation: thinking broadly. Can J Cardiol. (2018) 34:1503–11. doi: 10.1016/j.cjca.2018.08.036
6. Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. (2020) 127:4–20 doi: 10.1161/CIRCRESAHA.120.316340
7. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. (2021) 16:217–21. doi: 10.1177/1747493019897870
8. Aggarwal N., Selvendran S., Raphael C. E., Vassiliou V. (2015). Atrial fibrillation in the young: A neurologist's nightmare. Neurol Res Int. (2015) 2015:374352. doi: 10.1155/2015/374352
9. Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Njølstad I, et al. Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the biomarcare consortium (Biomarker for cardiovascular risk assessment in Europe). Circulation. (2017) 136:1588–97. doi: 10.1161/CIRCULATIONAHA.117.028981
10. Ladwig KH, Goette A, Atasoy S, Johar H. Psychological aspects of atrial fibrillation: a systematic narrative review: impact on incidence, cognition, prognosis, and symptom perception. Current Curr Cardiol Rep. (2020) 22:137 doi: 10.1007/s11886-020-01396-w
11. Patel D, Mc Conkey ND, Sohaney R, Mc Neil A, Jedrzejczyk A, Armaganijan L. A systematic review of depression and anxiety in patients with atrial fibrillation: The mind-heart link. Cardiovasc Psychiatry Neurol. (2013) 2013:159850. doi: 10.1155/2013/159850
12. Pothineni NV, Vallurupalli S. Gender and atrial fibrillation: Differences and disparities. US Cardiol Rev. (2018) 12:103–6. doi: 10.15420/usc.2017:39:1
13. Nanda A, Kabra R. Racial differences in atrial fibrillation epidemiology, management, and outcomes. Curr Treat Options Cardiovasc Med. (2019) 21:85. doi: 10.1007/s11936-019-0793-5
15. Freeman JV, Simon DN, Go AS, Spertus J, Fonarow GC, Gersh BJ, et al. Association between atrial fibrillation symptoms, quality of life, and patient outcomes: results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circ Cardiovasc Qual Outcomes. (2015) 8:393–402. doi: 10.1161/CIRCOUTCOMES.114.001303
16. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. Scientific Document Group. ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the european society of cardiology (ESC) developed with the special contribution of the european heart rhythm association (EHRA) of the ESC. Eur Heart J. (2020) 42:373–498 doi: 10.1093/eurheartj/ehaa612
17. Kim D, Yang P, You SC, Jang E, Yu HT, Kim T, et al. Age and outcomes of early rhythm control in patients with atrial fibrillation; nationwide cohort study. JACC Clin Electrophysiol. (2022) 8:619–32. doi: 10.1016/j.jacep.2022.02.014
18. Kirchhof P, Camm AJ, Goette A, Brandes A, Eckardt L, Elvan A. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med. (2020) 383:1305–16 doi: 10.1056/NEJMoa2019422
19. Andrade JG, Wazni OM, Kuniss M, Hawkins NM, Deyell MW, Chierchia GB, et al. Cryoballoon ablation as initial treatment for atrial fibrillation: JACC state-of-the-art review. J Am Coll Cardiol. (2021) 78:914–30. doi: 10.1016/j.jacc.2021.06.038
20. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the cabana randomized clinical trial. JAMA. (2019) 321:1261–74. doi: 10.1001/jama.2019.0693
21. Darby AE. Recurrent atrial fibrillation after catheter ablation: considerations for repeat ablation and strategies to optimize success. J Atr Fibrillation. (2016) 9:1427–1427.
22. Shan Q, Xinxin S, Zhijuan X, Rongjing D, Minjie Z. Effects of cognitive behavior therapy on depression, illness perception, and quality of life in atrial fibrillation patients. Front Psychiatry. (2022) 13:830363. doi: 10.3389/fpsyt.2022.830363
23. Camm AJ, Naccarelli GV, Mittal S, Crijns HJGM, Hohnloser SH, Ma C, et al. The increasing role of rhythm control in patients with atrial fibrillation; JACC state-of-the-art review. J Am Coll Cardiol. (2022) 79:1932–48. doi: 10.1016/j.jacc.2022.03.337
24. Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res. (2014) 114:1453–68. doi: 10.1161/CIRCRESAHA.114.303211
25. Weller M, Cloughesy T, Perry JR, Wick W. Standards of care for treatment of recurrent glioblastoma-are we there yet? Neuro Oncol. (2013) 15:4–27. doi: 10.1093/neuonc/nos273
26. Center for Disease Control. Atrial Fibrillation. (2021). Available online at: https://www.cdc.gov/heartdisease/atrial_fibrillation.htm (accessed November 30, 2021).
27. Vizzardi E, Curnis A, Latini MG, Salghetti F, Rocco E, Lupi L, et al. Risk factors for atrial fibrillation recurrence: a literature review. J Cardiovasc Med (Hagerstown). (2014) 15:235–53. doi: 10.2459/JCM.0b013e328358554b
28. Kuhl EA, Dixit NK, Walker RL, Conti JB, Sears SF. Measurement of patient fears about implantable cardioverter defibrillator shock: an initial evaluation of the Florida shock anxiety scale. PACE. (2006) 29:614–8. doi: 10.1111/j.1540-8159.2006.00408.x
29. Tripp C, Huber NL, Kuhl EA, Sears SF. Measuring ICD shock anxiety: status update on the Florida Shock Anxiety Scale after over a decade of use. PACE. (2019) 42:1294–301. doi: 10.1111/pace.13793
30. Birk JL, Cumella R, Lopez-Veneros D, Jurado A, Romero EK, Lazarov A, et al. Intervening on fear after acute cardiac events: Rationale and design of the INFORM randomized clinical trial. Health Psychol. (2020) 39:736–44. doi: 10.1037/hea0000853
31. Butow P, Sharpe L, Thewes B, Turner J, Gilchrist J, Beith J. Fear of cancer recurrence: a practical guide for clinicians. Oncology (United States). (2018) 32:32–8. Available online at: https://www.cancernetwork.com/view/fear-cancer-recurrence-practical-guide-clinicians
32. Hall DL, Jimenez RB, Perez GK, Rabin J, Quain K, Yeh GY, et al. Fear of cancer recurrence: a model examination of physical symptoms, emotional distress, and health behavior change. J Oncol Pract. (2019) 15:E787–97. doi: 10.1200/JOP.18.00787
33. Mehnert A, Koch U, Sundermann C, Dinkel A. Predictors of fear of recurrence in patients one year after cancer rehabilitation: a prospective study. Acta Oncol. (2013) 52:1102–9. doi: 10.3109/0284186X.2013.765063
34. Tauber NM, O'Toole MS, Dinkel A, Galica J, Humphris G, Lebel S, et al. Effect of psychological intervention on fear of cancer recurrence: a systematic review and meta-analysis. J Clin Onco. (2019) 37:2899–2915. doi: 10.1200/JCO.19.00572
35. Curran L, Sharpe L, MacCann C, Butow P. Testing a model of fear of cancer recurrence or progression: the central role of intrusions, death anxiety and threat appraisal. J Behav Med. (2020) 43:225–36. doi: 10.1007/s10865-019-00129-x
36. Sharpe L, Curran L, Butow P, Thewes B. Fear of cancer recurrence and death anxiety. Psychooncology. (2018) 27:2559–65. doi: 10.1002/pon.4783
37. Shim EJ, Shin YW, Oh DY, Hahm BJ. Increased fear of progression in cancer patients with recurrence. Gen Hosp Psychiatry. (2010) 32:169–75. doi: 10.1016/j.genhosppsych.2009.11.017
38. Palas JMC, Hyland KA, Nelson AM, Small BJ, Jim HSL, Jacobsen PB. An examination of the relationship of patient modifiable and non-modifiable characteristics with fear of cancer recurrence among colorectal cancer survivors. Support Care Cancer. (2020) 29:869–76. doi: 10.1007/s00520-020-05552-4
39. Pang C, Humphris G. The relationship between fears of cancer recurrence and patient gender: a systematic review and meta-analysis. Front Psychol. (2021) 12:1–13. doi: 10.3389/fpsyg.2021.640866
40. Leclair CS, Lebel S, Westmaas JL. The relationship between fear of cancer recurrence and health behaviors: a nationwide longitudinal study of cancer survivors. Health Psychol. (2019) 38:596–605. doi: 10.1037/hea0000754
41. Marcus GM, Modrow MF, Schmid CH, Sigona K, Nah G, Yang J, et al. Individualized studies of triggers of paroxysmal atrial fibrillation: The I-STOP-AFib randomized clinical trial. JAMA Cardiol. (2022) 7:167–74. doi: 10.1001/jamacardio.2021.5010
42. Tripp C, Gehi AK, Rosman L, Anthony S, Sears SF. Measurement of patient confidence in self-management of atrial fibrillation: Initial validation of the Confidence in Atrial fibriLlation Management (CALM) Scale. J Cardiovasc Electrophysiol. (2021) 32:1640–5. doi: 10.1111/jce.15050
43. Robaye B, Lakiss N, Dumont F, Laruelle C. Atrial fibrillation and cardiac rehabilitation: an overview. Acta Cardiol. (2020) 75:116–20. doi: 10.1080/00015385.2019.1565663
44. Frasure-Smith N, Lespérance F, Talajic M, Khairy P, Dorian P, O'Meara E, et al. Anxiety sensitivity moderates prognostic importance of rhythm-control versus rate-control strategies in patients with atrial fibrillation and congestive heart failure insights from the atrial fibrillation and congestive heart failure trial. Circ Heart Fail. (2012) 5:322–30. doi: 10.1161/CIRCHEARTFAILURE.111.964122
45. McMullen L. Patient assistance programs: easing the burden of financial toxicity during cancer treatment. Clin J Oncol Nurs. (2019) 23:36–40. doi: 10.1188/19.CJON.S2.36-40
46. Sears SF, Serber ER, Alvarez LG, Schwartzman DS, Hoyt RH, Ujhelyi MR. Understanding atrial symptom reports: objective versus subjective predictors. PACE. (2005) 28:801–7. doi: 10.1111/j.1540-8159.2005.00171.x
47. Thompson TS, Barksdale DJ, Sears SF, Mounsey JP, Pursell I, Gehi AK. The effect of anxiety and depression on symptoms attributed to atrial fibrillation. PACE. (2014) 37:439–46. doi: 10.1111/pace.12292
48. Polikandrioti M, Koutelekos I, Vasilopoulos G, Gerogianni G, Gourni M, Zyga S, et al. Anxiety and depression in patients with permanent atrial fibrillation: prevalence and associated factors. Cardiol Res Pract. (2018) 2018:7408129. doi: 10.1155/2018/7408129
49. Koleck TA, Mitha SA, Biviano A, Caceres BA, Corwin EJ, Goldenthal I, et al. Exploring depressive symptoms and anxiety among patients with atrial fibrillation and/or flutter at the time of cardioversion or ablation. J Cardiovasc Nurs. (2021) 36:470–81. doi: 10.1097/JCN.0000000000000723
50. Rizzi SA, Knight S, May HT, Woller SC, Stevens SM, Steinberg BA, et al. Depression as a driving force for low time in therapeutic range and dementia in patients with and without atrial fibrillation. Am J Cardiol. (2021) 153:58–64. doi: 10.1016/j.amjcard.2021.05.021
51. McCabe PJ, Schumacher K, Barnason SA. Living with atrial fibrillation: a qualitative study. J Cardiovasc Nurs. (2011) 26:336–44. doi: 10.1097/JCN.0b013e31820019b9
52. Piccini JP, Simon DN, Steinberg BA, Thomas L, Allen LA, Fonarow GC, et al. Differences in clinical and functional outcomes of atrial fibrillation in women and men: two-year results from the ORBIT-AF registry. JAMA Cardiology. (2016) 1:282–91. doi: 10.1001/jamacardio.2016.0529
53. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: The framingham study. Stroke. (1991) 22:983–8. doi: 10.1161/01.STR.22.8.983
54. Ozeke O, Aras S, Baser K, Sen F, Kirbas O, Cay S, et al. Defensive medicine due to different fears by patients and physicians in geriatric atrial fibrillation patients and second victim syndrome. Int J Cardiol. (2016) 212:251–2. doi: 10.1016/j.ijcard.2016.03.093
55. Steger C, Pratter A, Martinek-Bregel M, Avanzini M, Valentin A, Slany J, et al. Stroke patients with atrial fibrillation have a worse prognosis than patients without: data from the Austrian Stroke registry. Eur Heart J. (2004) 25:1734–40. doi: 10.1016/j.ehj.2004.06.030
56. Jørgensen HS, Nakayama H, Reith J, Raaschou HO, Olsen TS. Acute stroke with atrial fibrillation. Stroke. (1996) 27:1765–9. doi: 10.1161/01.STR.27.10.1765
57. Saxena R, Lewis S, Berge E, Sandercock PAG, Koudstaal PJ. Risk of early death and recurrent stroke and effect of heparin in 3169 patients with acute ischemic stroke and atrial fibrillation in the International Stroke Trial. Stroke. (2001) 32:2333–7. doi: 10.1161/hs1001.097093
58. Belgen B, Beninato M, Sullivan PE, Narielwalla K. The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke. Arch Phys Med Rehabil. (2006) 87:554–61. doi: 10.1016/j.apmr.2005.12.027
59. Soleimani MA, Lehto RH, Negarandeh R, Bahrami N, Chan YH. Death anxiety and quality of life in iranian caregivers of patients with cancer. Cancer Nurs. (2017) 40:E1–E10. doi: 10.1097/NCC.0000000000000355
60. Soleimani MA, Lehto RH, Negarandeh R, Bahrami N, Nia HS. Relationships between death anxiety and quality of life in iranian patients with cancer. Asia Pac J Oncol Nurs. (2016) 3:183–91. doi: 10.4103/2347-5625.182935
61. MacLeod R, Crandall J, Wilson D, Austin P. Death anxiety among New Zealanders: the predictive role of gender and marital status. Mental Health, Religion Culture. (2016) 19:339–49. doi: 10.1080/13674676.2016.1187590
62. Lau BHP, Wong DFK, Fung YL, Zhou J, Chan CLW, Chow AYM. Facing death alone or together? Investigating the interdependence of death anxiety, dysfunctional attitudes, and quality of life in patient-caregiver dyads confronting lung cancer. Psychooncology. (2018) 27:2045–51. doi: 10.1002/pon.4773
63. Gehi AK, Sears S, Goli N, Walker TJ, Chung E, Schwartz J, et al. Psychopathology and symptoms of atrial fibrillation: Implications for therapy. J Cardiovasc Electrophysiol. (2012) 23:473–8. doi: 10.1111/j.1540-8167.2011.02264.x
64. Frasure-Smith N, Lesperance F, Habra M, Talajic M, Khairy P, Dorian P, et al. Elevated depression symptoms predict long-term cardiovascular mortality in patients with atrial fibrillation and heart failure. Circulation. (2009) 120:134–40. doi: 10.1161/CIRCULATIONAHA.109.851675
65. Gleason KT, Himmelfarb CRD, Ford DE, Lehmann H, Samuel L, Jain S, et al. Association of sex and atrial fibrillation therapies with patient-reported outcomes. Heart. (2019) 105:1642–8. doi: 10.1136/heartjnl-2019-314881
66. von Eisenhart Rothe A, Hutt F, Baumert J, Breithardt G, Goette A, Kirchhof P, et al. Depressed mood amplifies heart-related symptoms in persistent and paroxysmal atrial fibrillation patients: A longitudinal analysis–data from the german competence network on atrial fibrillation. Europace. (2015) 17:1354–62. doi: 10.1093/europace/euv018
67. LaRosa AR, Claxton J, O'Neal WT, Lutsey PL, Chen LY, Bengtson L, et al. Association of household income and adverse outcomes in patients with atrial fibrillation. Heart. (2020) 106:1679–85. doi: 10.1136/heartjnl-2019-316065
68. Bazemore TC, Bolger LE, Sears SF, Sadaf MI, Gehi AK. Gender differences in symptoms and functional status in patients with atrial fibrillation undergoing catheter ablation. PACE. (2019) 42:224–9. doi: 10.1111/pace.13577
69. Lewandowska A, Religioni U, Czerw A, Deptała A, Karakiewicz B, Partyka O, et al. Medication adherence and the role of pictograms in medication counselling of chronic patients: a review. Front Pharmacology. (2021) 12:582200. doi: 10.3389/fphar.2021.582200
70. Chung MK, Eckhardt LL, Chen LY, Ahmed HM, Gopinathannair R, Joglar JA, et al. Lifestyle and risk factor modification for reduction of atrial fibrillation: a scientific statement from the American Heart Association. Circulation. (2020) 141:e750–72. doi: 10.1161/CIR.0000000000000748
71. Pluymaekers NAHA, Hermans ANL, Middeldorp ME, Kadhim K, Crijns HJGM, et al. Gender differences and daily variation in atrial fibrillation risk factor profiles: considerations for risk factor management. Int J Cardiol Heart Vasc. (2019) 25:20–2. doi: 10.1016/j.ijcha.2019.100442
72. Jiang C, Lan DH, Du X, Geng YP, Chang SS, Zheng D, et al. Prevalence of modifiable risk factors and relation to stroke and death in patients with atrial fibrillation: a report from the China atrial fibrillation registry study. J Cardiovasc Electrophysiol. (2019) 30:2759–66. doi: 10.1111/jce.14231
73. Benedetto D, Michels L, Luben G, Khaw RKT, Pfister R. Individual and combined impact of lifestyle factors on atrial fibrillation in apparently healthy men and women: The EPIC-Norfolk prospective population study. Eur J Prevent Cardiol. (2018) 25:1374–83. doi: 10.1177/2047487318782379
74. Stanton AL, Revenson TA, Tennen H. Health psychology: psychological adjustment to chronic disease. Annu Rev Psychol. (2007) 58:565–92. doi: 10.1146/annurev.psych.58.110405.085615
75. Skielboe AK, Bandholm TQ, Hakmann S, Mourier M, Kallemose T, Dixen U. Cardiovascular exercise and burden of arrhythmia in patients with atrial fibrillation -A randomized controlled trial. PLoS ONE. (2017) 12:1–17. doi: 10.1371/journal.pone.0170060
76. McCabe PJ, Barnason SA, Houfek J. Illness beliefs in patients with recurrent symptomatic atrial fibrillation. PACE. (2011) 34:810–20. doi: 10.1111/j.1540-8159.2011.03105.x
77. Locke AB, Kirst N, Shultz CG. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am Fam Physician. (2015) 91:617–24. Available online at: https://www.aafp.org/pubs/afp/issues/2015/0501/p617.html
Keywords: atrial fibrillation, cardiac electrophysiology, cardiac psychology, fear of recurrence, health anxiety
Citation: Anthony S, Harrell R, Martin C, Hawkins T, Khan S, Naniwadekar A and Sears SF (2022) Fear of Recurrence of Atrial Fibrillation: Translating a Cancer Fear Model to the Atrial Fibrillation Patient Experience. Front. Psychiatry 13:915327. doi: 10.3389/fpsyt.2022.915327
Received: 22 April 2022; Accepted: 09 June 2022;
Published: 04 July 2022.
Edited by:
Kai G. Kahl, Hannover Medical School, GermanyReviewed by:
David Duncker, Hannover Medical School, GermanyCopyright © 2022 Anthony, Harrell, Martin, Hawkins, Khan, Naniwadekar and Sears. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samuel F. Sears, c2VhcnNzQGVjdS5lZHU=
†ORCID: Samuel F. Sears orcid.org/0000-0002-7863-3591
Scarlett Anthony orcid.org/0000-0003-0154-8388
Rebecca Harrell orcid.org/0000-0003-1318-0736
Caroline Martin orcid.org/0000-0002-4813-8098
Aditi Naniwadekar orcid.org/0000-0002-0880-405X
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.