
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 10 June 2022
Sec. Mood Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.912021
This article is part of the Research Topic The Neurobiology of Suicide: The 'Suicidal Brain' View all 11 articles
 Alma Delia Genis-Mendoza1,2†
Alma Delia Genis-Mendoza1,2† Diana María Dionisio-García3†
Diana María Dionisio-García3† Thelma Beatriz Gonzalez-Castro4
Thelma Beatriz Gonzalez-Castro4 Carlos Alfonso Tovilla-Zaráte5*
Carlos Alfonso Tovilla-Zaráte5* Isela Esther Juárez-Rojop3María Lilia López-Narváez6
Isela Esther Juárez-Rojop3María Lilia López-Narváez6 Rosa Giannina Castillo-Avila3
Rosa Giannina Castillo-Avila3 Humberto Nicolini1*
Humberto Nicolini1*Background: Abnormalities in the hypothalamic-pituitary-adrenal axis (HPA) have been reported in individuals with suicide behavior. The aim of the study was to evaluate cortisol levels in peripheral plasma of individuals with more than one suicide attempt.
Methods: Cortisol concentrations in peripheral plasma were measured using the ELISA technique. Suicide attempts were evaluated by the Columbia Suicide Severity Rating Scale, while depression was evaluated by the Hamilton Depression Rating Scale.
Results: We found elevated cortisol levels in the suicide attempt group when compared with healthy controls (F = 7.26, p-value = 0.008), but no statistical differences with the psychiatric diseases group (F = 1.49, p-value = 0.22). Cortisol levels were higher in individuals with depression (F = 8.99, P = 0.004) and in individuals with two or more suicide attempts (F = 13.56, P < 0.001).
Conclusions: Cortisol levels are increased in individuals who attempt suicide and higher of cortisol concentrations in plasma regard to depression and more attempts of suicide.
Suicide is a public health problem worldwide. In 2020, 1.5 million deaths by suicide were reported (1). Epidemiology studies indicate that an estimate of 80% of these deaths were in low and middle-income countries (2, 3).
The etiology of suicide behavior is unknown; however, it has been proposed a diathesis-stress model to explain its pathogenesis. It is believed that the diathesis may have a biological origin. The literature shows that, when stress in perceived, there are clear changes in cortisol levels (4). Therefore, the stress diathesis theory of suicide postulates that there are predisposing and precipitating risk factors of suicide attempts. Genetic, inflammation, serotoninergic systems, peripheral biomarkers as cholesterol and, the alteration of the hypothalamic-pituitary-adrenal axis (HPA), could be participant in the biological diathesis of suicide behavior (5–7).
Some studies have addressed the association between altered levels of circulating cortisol and an increased risk of suicide behaviors (8); nonetheless, these studies have observed a variety of outcomes. For example, in a response to an experimental stressor in suicide attempters compared with non-suicidal individuals, a low baseline cortisol prior to the stressor was found in attempters (9). However, in veterans with and without suicide attempts, a no-significant association with cortisol levels and suicidal behavior was observed (10); similarly, no-significant association with cortisol levels was observed in individuals with psychiatric illnesses and suicide behavior (11, 12) also, higher cortisol levels were associated with increased suicidal severity and suicide attempts (13) moreover, increased cortisol response after dexamethasone suppression test have been presented in patients that were weary life (14) and in Due to the inconsistent results regarding the association of cortisol levels and suicide behavior, two meta-analyses have explored this association (15, 16) and their results suggest a possible role of cortisol levels in suicide behavior. Therefore, the need of more studies performed in other populations and the inclusion of healthy and psychiatric controls is imperative in order to determine the role of cortisol levels and suicide attempt. The objectives of the present study were to evaluate plasma cortisol levels in Mexican individuals with suicide attempt and to determine if cortisol levels differ between these individuals and those with psychiatric diseases and a healthy comparison group; and finally, to associate plasma cortisol levels with the characteristics of suicide attempt.
This is a cross-sectional study conducted from January to December, 2020, in Tabasco, Mexico. This study meets the criteria established in the Declaration of Helsinki and was approved by the ethics committee of the Regional Hospital of High Specialty of Mental Health (HRAESM/DG/UWI/351/2020). All participants signed an informed consent. None of the individual included in the study received financial compensation for their participation.
Our study group comprised a total of 143 Mexican individuals, that were recruited from February 2020 to July 2021. We included three hospitals in Tabasco State: The High Specialization Regional Hospital Dr. Gustavo A. Rovirosa Pérez in Villahermosa City, The General Hospital of Comalcalco Dr. Desiderio G. Rosado Carbajal in Comalcalco City, and The Regional Hospital of High Specialty of Mental Health in Villahermosa City.
The sample was divided in 3 groups: (1) The suicide attempt group included 56 patients who had a diagnosis of suicide attempt, made by at least one psychiatrist using the evaluation of suicide behavior by the Columbia Suicide Severity Rating Scale (C-SSRS); they were all selected from admissions to the hospital emergency department. (2) The group of individuals with psychiatric diseases (excluding depression) and no-history of suicide behavior was formed by 31 patients; the psychiatric diagnoses (including schizophrenia) were made by at least one psychiatrist. (3) The healthy control group included 56 participants who reported no-history of suicide attempt or psychiatric illnesses. All the participants were volunteers; they were informed about the study, the procedure and the objectives; they all signed an informed consent form and agreed to the collection of the biological sample. The objective of including these three groups was to compare the cortisol levels in three types of population, since literature indicates variations among them.
Demographic characteristics such as age, sex, occupation, marital status, educational level, sample collection time, BMI (body mass index) and substance use were gathered. Additionally, we included information about their suicide behavior using the C-SSRS; to evaluate symptoms of depression we used the Hamilton Depression Scale (HAM-D). In the suicide attempt group, we also enquired about the family history of suicide attempts, number of suicide attempts, method of suicide attempt, as well as age of first and last suicide attempts.
The clinical diagnosis was made by at least one psychiatrist according to the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders 5) criteria for determining suicide attempt, and they used the C-SSRS (which is validated in Spanish and increases the ability to predict suicidal risk) full version including 16 questions with binary responses. The C-SSRS is used as an initial screening to guide clinicians in assessing suicide risk and to help stratify patients into categories of low, moderate or high lifetime patient risk. The C-SSRS is formed by four sub-scales: severity and intensity of suicidal ideation and severity and lethality of suicide behavior (17); and 20 categories: wish to be dead, with no-specific active suicidal thoughts; active suicidal ideation, with any methods, without intent to act; active suicidal ideation, with some intent to act, without specific plans; active suicidal ideation, with specific plan and intent; preparatory suicide acts or suicide behavior; aborted suicide attempt; interrupted suicide attempt; actual suicide attempt (non-fatal); and completed suicide. If one question is answered “yes”, in categories 1–5 is suicidal ideation, in categories 6–10 is suicide behavior. In the same way, information about the number of suicide attempts was collected, age when the first suicide attempt occurred, age of last suicide attempt, family history of suicide attempts and whether they suffer from any psychiatric illnesses.
The group of individuals with psychiatric diseases but without suicide attempt were diagnosed by psychiatrics according to the DSM-5. Who reported in the interviews that they did not have any previous suicide attempts and we corroborated that information in their medical records.
The control group was formed by 56 individuals (64.3% males and 35.7% females) with an age range of 18–55 years and a mean of 34.30 years of age (±10.37), who were volunteer donors from the blood bank of The High Specialization Regional Hospital Dr. Gustavo A. Rovirosa Pérez. This group received a general check-up by physicians and they reported no psychiatric illness or history of suicide attempts.
Depression symptoms were evaluated in individuals with suicide attempt using the HAM-D, consisting of 17 questions validated in Spanish and evaluates the depressive symptomatology of the patients (18). It was important to evaluate depression, since it is an important factor related to suicide attempts (19). The scale is widely available and has two common versions with either 17 or 21 items that score between 0 and 4 points. The first 17 items measure the severity of depressive symptoms and as examples the interviewer rates the level of agitation clinically noted during the interview or how the mood is impacting on an individual's work or leisure pursuits. The extra four items on the extended 21-point scale measure factors that might be related to depression, but are not thought to be measurements of severity, such as paranoia or obsessional and compulsive symptoms. The scoring is based on the 17-item scale and scores of 0–7 are considered as being normal, 8–16 suggest mild depression, 17–23 moderate depression and scores over 24 are indicative of severe depression; the maximum possible score is 52 on the 17-point scale.
Peripheral blood samples were taken from three groups and the blood was placed in EDTA (Ethylenediamine tetraacetic acid) containing tubes [BD Vacutainer, K2 EDTA (K2E)] Plus Blood Collection Tubes, placed on ice. Samples from the group of individuals with suicide attempt were taken the day after their admission to the emergency room. After the peripheral blood samples were collected, they were immediately centrifuged and plasma aliquots were made and stored at −80°C. Cortisol concentrations in plasma were determined by means of the competitive Enzyme-Linked Immunoabsorption Assay (ELISA). The samples were analyzed using a commercially available Cortisol Competitive Human ELISA kit by Invitrogen. The mean of sample collection was at 11:00 am.
Data were analyzed using the SPSS version 27.0 (IBM Corporation, Armonk, NY). Descriptive variables were expressed as means and Standard Deviation (SD) for continues variables, and frequencies and percentages for categorical variables. The initial comparison between patients with suicide attempt and the comparison groups were analyzed with X2-test also for categorical variables and with independent samples t-test for continuous variables. In continues variables, an analysis of variance followed by Bonferroni correction were performed. Cortisol levels and confounding variables were analyzed by linear regression analysis. We performed linear regression with confounding variables (age, sex, education, marital status, socioeconomic level, time of collection and body mass index) which did not present statistical differences that influenced the cortisol levels of our study group. To determine the association between cortisol levels and suicide attempt, we performed an age-adjusted linear regression analysis. Significance was established at p ≤ 0.05 for all analyses.
In the Table 1 are shown the characteristics of the study population. The majority in the overall population were men n = 79 (55.6%) and unemployed n = 75; the majority were not-married n = 74 (51.7%) and had studied more than 6 years n = 116 (81.1%). As for substances use, most of them did not consume alcohol n = 75 (52.4%), neither cannabis n = 133 (93%) nor smoke cigarettes n = 123 (88.35%).
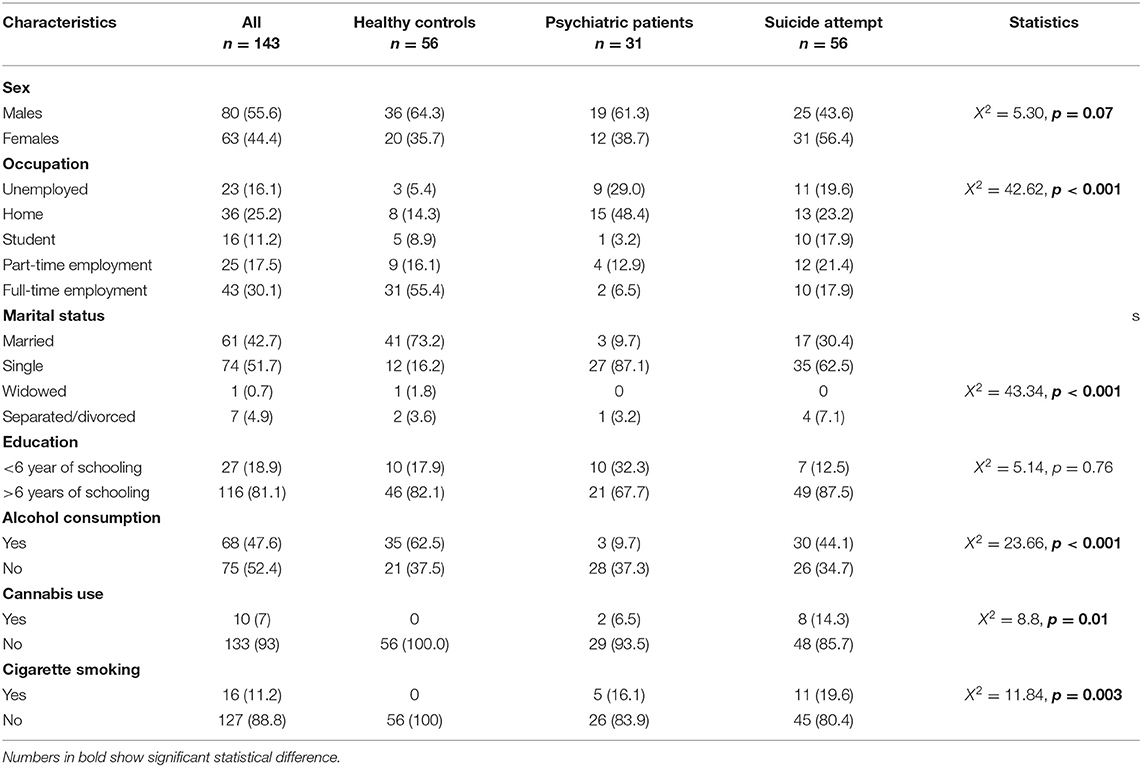
Table 1. Sociodemographic characteristics of suicide attempters, patients with psychiatric diseases and healthy individuals in a Mexican population.
The suicide attempt group included more women n = 31 (56.4), unemployed n = 34 (60.7%), mostly single n = 39 (69.6%), and with an education of more than 6 years n = 49 (87.5). The majority consumed alcohol n = 30 (44.1), but not cannabis n = 45 (85.7%) and no cigarette smoking n = 44 (80%), and the mean cortisol level was 14.68 μg/dL (SD 15.36).
The psychiatric diseases group included more men n = 19 (61.3%), single n = 27 (87.1%), and who had more than 6 years of schooling n = 21 (67.7%). Most of them, did not consume alcohol n = 28 (90.3%), neither cannabis n = 29 (93.5%) and no cigarette smoking n = 24 (82.8%).
In the healthy control group there were more men n = 36 (64.3%), unemployed n = 16 (64%), and married n = 41 (73.2%). The majority had studied more than 6 years n = 46 (82.1%). As for the substances abuse, most of them used alcohol n = 35 (62.5%) but not cannabis n = 56 (100%) and no cigarette smoking n = 56 (100%).
Comparison of groups using the cortisol levels are show in the Table 2. We observed difference between groups. In accordance with post-hoc comparisons, healthy controls and suicide attempt groups reported statistically significant. Since, the suicide attempt groups showed a higher cortisol levels that healthy controls groups. However, the post-hoc analysis of healthy controls and psychiatric controls not differences were observed.
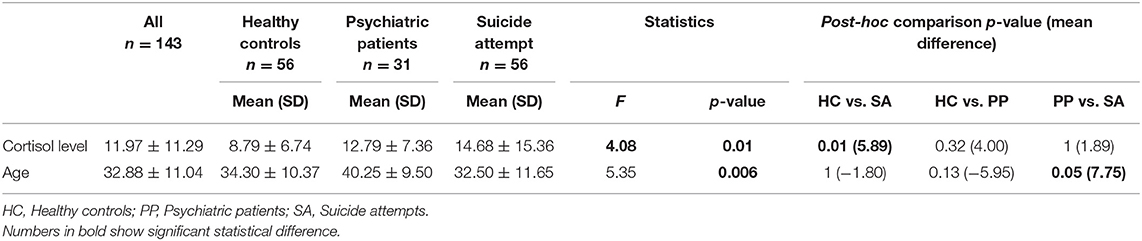
Table 2. Comparison of cortisol levels and age among groups.
Table 3 shows the characteristics of the suicide attempts in the cases group, most of them had one suicide attempt n = 37 (66.1%), did not have familiar history of suicide attempts n = 24 (75%), the mean age of the first suicide attempt was at 29.28 years old ±12.90 and the last suicide attempt was at 31.64 years old ±13.82. Where the characteristics were compared between men and women, there were no statistical differences, in our study group sex was not related to suicide phenotypes.
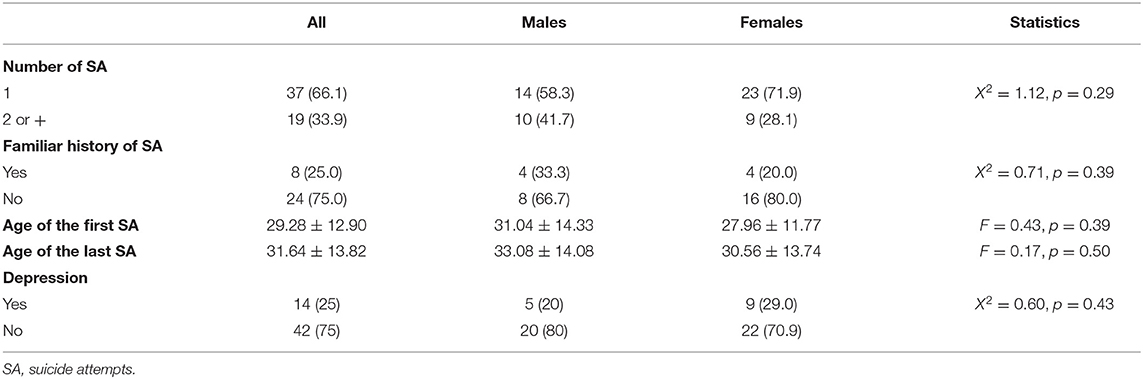
Table 3. Characteristics of suicide attempt among males and females in Mexican population.
In Table 4, we show the levels of cortisol in plasma μg/dL) in subgroups of suicide attempters and the comparison groups (healthy individuals or with psychiatric diseases) in a Mexican population.
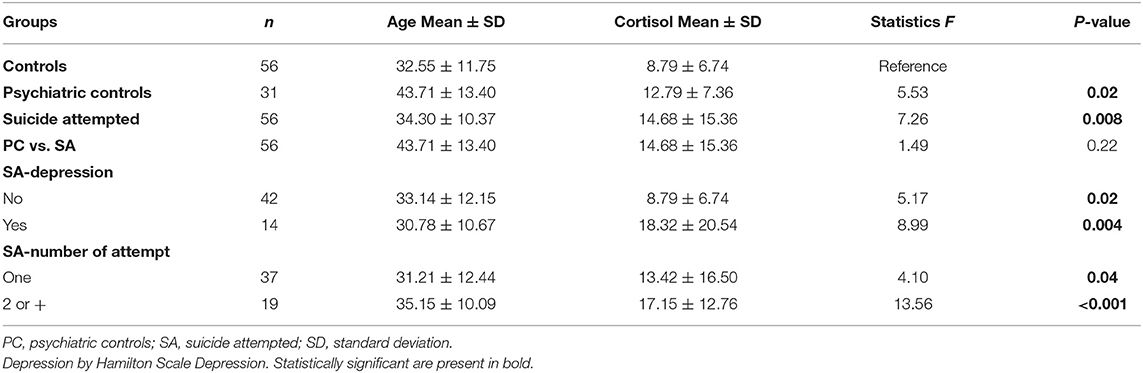
Table 4. Level of plasma cortisol (μg/dL) in subgroups of suicide attempters and comparison groups (health and psychiatric group) in a Mexican population.
The results of the linear regression analysis were statistically significant when we compared cortisol levels between healthy controls and individuals with suicide attempt (F = 7.26, P-value = 0.008) (Table 3). But no statistically significant differences were observed when comparing with the psychiatric diseases group (F = 1.49, p = 0.22). Subsequently, we evaluated differences in the presence of symptoms of depression. We found that individuals with (F = 8.99, P = 0.004) and without depression showed increased cortisol levels in comparison with healthy controls and/or individuals with psychiatric diseases.
In this study, we evaluated plasma cortisol levels in individuals with suicide attempt in comparison with two groups, healthy individuals and individuals with psychiatric diseases (excluding depression). Up to date, research has not delivered conclusive outcomes that determine if cortisol levels are decreased or increased in individuals who attempt suicide (15, 20, 21). We also analyzed cortisol levels according to clinical and sociodemographic variables; to our knowledge, this is the first study that evaluates cortisol levels in Mexican individuals who have attempted suicide.
We found significantly elevated cortisol levels in the suicide attempt group in comparison with the healthy control group. Our results agree with other studies that have observed high cortisol levels in suicide attempt groups when compared with individuals without suicide behavior (22–29). Sociodemographic characteristics of cases and comparison groups in our population studied were very similar; however, their circulating cortisol levels differed significantly. Hence, we could assume that cortisol levels are related with an alteration of the stress regulation system in patients with suicide attempt (30). In the case of the individuals with psychiatric diseases (excluding depression), cortisol levels were not significantly different when compared with the suicide attempt group. Nevertheless, both groups had higher cortisol levels then the healthy individuals group. Some studies have concluded that individuals with psychiatric diseases (excluding suicide behavior and depression) show different cortisol levels than patients with suicide behavior (15). Other reports found that subjects with psychiatric disorders have shown HPA axis hyperactivity and alterations in cortisol levels (31, 32); furthermore, individuals with suicide attempt could have a more active HPA axis than individuals with other psychiatric disorders (11, 12).
On the other hand, we observed statistical differences when we analyzed the characteristics of the suicide attempt group associated with cortisol levels such as the presence or absence of depression. Significantly elevated cortisol levels were observed in the group of individuals who had attempted suicide, in comparison with the baseline cortisol levels of the healthy group, as some previous studies have recorded (23, 27, 33). Our results suggest that cortisol levels could be a phenotype of suicide attempters because of an alteration in the HPA axis, and this could be increased in the presence of depression or the number of suicide attempts.
A conclusive description of the increased levels of cortisol in patient with suicide attempt has not been reached yet. However, some explanations have been proposed: some studies correlate 5-HT1A receptors of serotonin (5-HT) with cortisol levels, stress and suicide attempt (34, 35). In this sense, the altered serotonin is associated with suicide behavior, making people more aggressive and more susceptible to mood disorders (36, 37). Also, the hippocampus plays an important role in feedback mechanisms of the HPA axis (38, 39), as well as in the levels of 5HT1A receptors. The hyperactivity of the HPA axis produced by chronic exposure to stress generates an elevation of plasma corticosteroids, including cortisol (40). Having high levels of cortisol reduces the mRNA of 5HT1A receptors, decreasing their levels, resulting in low rates of serotonin metabolism, but when serotonin dysfunction occurs there is a risk of suicidal behavior (41–43). Another way in which high cortisol levels have been related to a decrease in 5-HT, is due to the increased tryptophan 2,3-dioxugenase (TDO) (20, 21); this enzyme is involved in the degradation of tryptophan (TRP) via the kynurenine pathway, which synthesizes 5-HT (44). With lower levels of TRP, there is not enough TRP available in brain to synthesize 5-HT, as there are more enzymes that metabolize TRP (45), and decreased amounts of the 5-HT neurotransmitter are associated with attempted suicide (46, 47).
The HPA hyperactivity in our group with psychiatric diseases is presumed to be different from our suicide attempt group, because one of the factors that contribute in the development of suicide ideation and suicide attempt is the presence of psychiatric illness (48–50) such as schizophrenia disorder (51, 52). In our results, suicide attempt group and psychiatric control group showed high cortisol levels, which indicates that there was hyperactivity of the HPA axis in both groups. But even if there were no significant differences between these groups, the suicide attempt group showed the highest cortisol levels. We assumed that this is a duality, where apart from suicidal behavior, a psychiatric illness is present, and both situations increased cortisol levels in patients who attempted suicide. Considering that cortisol levels in suicide attempt subjects were much higher when in presence of psychiatric illness and suicide ideation, it was important for us to include a control group with psychiatric illness to see any difference in cortisol levels. Our results support that we can use cortisol as a particular biomarker of suicidal attempt.
Some limitations in this study should be noted. First, we did not determine menstrual cycle, contraceptive use or hormone replacement in women who participated in the study. Second, the sample size could be considered small. However, it is the first study that explores cortisol levels in a Mexican population with suicide attempt. Third, this is a cross sectional study, then longitudinal studies that measure cortisol levels are needed. Also, we did not include the use of medications and if they received psychotherapy or some medication. Further, we did not aboard if the study population had been received psychological treatment in their childhood, neither, the evaluation of resilience capacity, or if they had some stressful life events, among other evaluations that could have been of great value for our study to include.
In conclusion, we found increased levels of plasma cortisol in individuals with suicide attempt. The level of cortisol is higher in presence of depression and in individuals with more than two attempts suicide. Then, levels of cortisol in individuals who attempt to die by suicide could be considered when searching for a biomarker of suicide attempts and become part of the preventing measures of this global problem.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by HRAESM/DG/UWI/351/2020. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Conceptualization, writing-original draft preparation, and supervision: DD-G, TG-C, CT-Z, AG-M, IJ-R, ML-N, and RC-A. Methodology: DD-G, TG-C, CT-Z, and IJ-R. Formal analysis and investigation: DD-G, TG-C, and CT-Z. Editing: DD-G, TG-C, CT-Z, and RC-A. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.912021/full#supplementary-material
1. WHO. Suicide. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed January 27, 2021).
2. WHO. Suicide Worldwide in 2019: Global Health Estimates. Geneva: World Health Organization (2019).
3. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. (2016) 387:1227–39. doi: 10.1016/S0140-6736(15)00234-2
4. van Heeringen K, Mann JJ. The neurobiology of suicide. The Lancet Psychiatry. (2014) 1:63–72. doi: 10.1016/S2215-0366(14)70220-2
5. Serafini G, Parisi VM, Aguglia A, Amerio A, Sampogna G, Fiorillo A, et al. A specific inflammatory profile underlying suicide risk? Systematic review of the main literature findings. Int J Environ Res Public Health. (2020) 17:393. doi: 10.3390/ijerph17072393
6. Aguglia A, Amerio A, Asaro P, Caprino M, Conigliaro C, Giacomini G, et al. High-lethality of suicide attempts associated with platelet to lymphocyte ratio and mean platelet volume in psychiatric inpatient setting. World J Biol Psychiatry. (2021) 22:119–27. doi: 10.1080/15622975.2020.1761033
7. Aguglia A, Solano P, Giacomini G, Caprino M, Conigliaro C, Romano M, et al. The association between dyslipidemia and lethality of suicide attempts: a case-control study. Front Psychiatry. (2019) 10:70. doi: 10.3389/fpsyt.2019.00070
8. Giurgiuca A, Nemes B, Schipor S, Caragheorgheopol A, Boscaiu V, Cozman D, et al. Cortisol levels and suicide in bipolar I disorder. Acta Endocrinol. (2017) 13:188–94. doi: 10.4183/aeb.2017.188
9. Melhem NM, Keilp JG, Porta G, Oquendo MA, Burke A, Stanley B, et al. Blunted HPA axis activity in suicide attempters compared to those at high risk for suicidal behavior. Neuropsychopharmacology. (2016) 41:1447–56. doi: 10.1038/npp.2015.309
10. Sher L, Bierer LM, Flory J, Hill MN, Makotkine I, Yehuda R. Endogenous cannabinoid levels and suicidality in combat veterans. Psychiatry Res. (2020) 287:112495. doi: 10.1016/j.psychres.2019.112495
11. Kamali M, Saunders EF, Prossin AR, Brucksch CB, Harrington GJ, Langenecker SA, et al. Associations between suicide attempts and elevated bedtime salivary cortisol levels in bipolar disorder. J Affect Disord. (2012) 136:350–8. doi: 10.1016/j.jad.2011.11.027
12. Green MJ, Girshkin L, Teroganova N, Quidé Y. Stress, schizophrenia and bipolar disorder. Curr Top Behav Neurosci. (2014) 18:217–35. doi: 10.1007/7854_2014_290
13. Choi W, Kang HJ, Kim JW, Kim HK, Kang HC, Lee JY, et al. Associations of serum cortisol levels, stress perception, and stressful events with suicidal behaviors in patients with depressive disorders. J Affect Disord. (2022) 297:602–9. doi: 10.1016/j.jad.2021.10.054
14. Hennings JM, Ising M, Uhr M, Holsboer F, Lucae S. Effects of weariness of life, suicide ideations and suicide attempt on HPA axis regulation in depression. Psychoneuroendocrinology. (2021) 131:105286. doi: 10.1016/j.psyneuen.2021.105286
15. Hernandez-Diaz Y, Gonzalez-Castro TB, Tovilla-Zarate CA, Juarez-Rojop IE, Lopez-Narvaez ML, Perez-Hernandez N, et al. The role of peripheral cortisol levels in suicide behavior: a systematic review and meta-analysis of 30 studies. Psychiatry Res. (2020) 293:113448. doi: 10.1016/j.psychres.2020.113448
16. O'Connor DB, Green JA, Ferguson E, O'Carroll RE, O'Connor RC. Effects of childhood trauma on cortisol levels in suicide attempters and ideators. Psychoneuroendocrinology. (2018) 88:9–16. doi: 10.1016/j.psyneuen.2017.11.004
17. Al-Halabi S, Saiz PA, Buron P, Garrido M, Benabarre A, Jimenez E, et al. Validation of a spanish version of the Columbia-suicide severity rating scale (C-SSRS). Rev Psiquiatr Salud Ment. (2016) 9:134–42. doi: 10.1016/j.rpsmen.2016.06.004
18. Ramos-Brieva JA, Cordero-Villafafila A. A new validation of the hamilton rating scale for depression. J Psychiatr Res. (1988) 22:21–8. doi: 10.1016/0022-3956(88)90024-6
19. Indu PS, Anilkumar TV, Pisharody R, Russell PSS, Raju D, Sarma PS, et al. Prevalence of depression and past suicide attempt in primary care. Asian J Psychiatr. (2017) 27:48–52. doi: 10.1016/j.ajp.2017.02.008
20. O'Connor DB, Ferguson E, Green JA, O'Carroll RE, O'Connor RC. Cortisol levels and suicidal behavior: a meta-analysis. Psychoneuroendocrinology. (2016) 63:370–9. doi: 10.1016/j.psyneuen.2015.10.011
21. O'Connor DB, Green JA, Ferguson E, O'Carroll RE, O'Connor RC. Cortisol reactivity and suicidal behavior: investigating the role of hypothalamic-pituitary-adrenal axis responses to stress in suicide attempters and ideators. Psychoneuroendocrinology. (2017) 75:183–91. doi: 10.1016/j.psyneuen.2016.10.019
22. Inder WJ, Donald RA, Prickett TC, Frampton CM, Sullivan PF, Mulder RT, et al. Arginine vasopressin is associated with hypercortisolemia and suicide attempts in depression. Biol Psychiatry. (1997) 42:744–7. doi: 10.1016/S0006-3223(97)00301-6
23. Tripodianakis J, Markianos M, Sarantidis D, Leotsakou C. Neurochemical variables in subjects with adjustment disorder after suicide attempts. Eur Psychiatry. (2000) 15:190–5. doi: 10.1016/S0924-9338(00)00226-1
24. Brunner J, Stalla GK, Stalla J, Uhr M, Grabner A, Wetter TC, et al. Decreased corticotropin-releasing hormone (CRH) concentrations in the cerebrospinal fluid of eucortisolemic suicide attempters. J Psychiatr Res. (2001) 35:1–9. doi: 10.1016/S0022-3956(01)00007-3
25. Brunner EJ, Hemingway H, Walker BR, Page M, Clarke P, Juneja M, et al. Adrenocortical, autonomic, and inflammatory causes of the metabolic syndrome: nested case-control study. Circulation. (2002) 106:2659–65. doi: 10.1161/01.CIR.0000038364.26310.BD
26. Markianos M, Tripodianakis J, Istikoglou C, Rouvali O, Christopoulos M, Papageorgopoulos P, et al. Suicide attempt by jumping: a study of gonadal axis hormones in male suicide attempters versus men who fell by accident. Psychiatry Res. (2009) 170:82–5. doi: 10.1016/j.psychres.2008.08.001
27. Chatzittofis A, Nordstrom P, Hellstrom C, Arver S, Asberg M, Jokinen J, et al. 5-HIAA, cortisol and DHEAS levels in suicide attempters. Eur Neuropsychopharmacol. (2013) 23:1280–7. doi: 10.1016/j.euroneuro.2013.02.002
28. Płocka-Lewandowska M, Araszkiewicz A, Rybakowski JK. Dexamethasone suppression test and suicide attempts in schizophrenic patients. Eur Psychiatry. (2001) 16:428–31. doi: 10.1016/S0924-9338(01)00602-2
29. Brown RP, Mason B, Stoll P, Brizer D, Kocsis J, Stokes PE, et al. Adrenocortical function and suicidal behavior in depressive disorders. Psychiatry Res. (1986) 17:317–23. doi: 10.1016/0165-1781(86)90079-X
30. O'Connor DB, Thayer JF, Vedhara K. Stress and health: a review of psychobiological processes. Annu Rev Psychol. (2021) 72:663–88. doi: 10.1146/annurev-psych-062520-122331
31. Zorn JV, Schur RR, Boks MP, Kahn RS, Joels M, Vinkers CH. Cortisol stress reactivity across psychiatric disorders: a systematic review and meta-analysis. Psychoneuroendocrinology. (2017) 77:25–36. doi: 10.1016/j.psyneuen.2016.11.036
32. Coulon N, Brailly-Tabard S, Walter M, Tordjman S. Altered circadian patterns of salivary cortisol in individuals with schizophrenia: a critical literature review. J Physiol Paris. (2016) 110:439–47. doi: 10.1016/j.jphysparis.2017.05.002
33. Lewitzka U, Bauer M, Ripke B, Bronisch T, Gunther L. Impulsivity and saliva cortisol in patients with suicide attempt and controls. Neuropsychobiology. (2017) 75:162–8. doi: 10.1159/000484664
34. Porter RJ, Gallagher P, Watson S, Young AH. Corticosteroid-serotonin interactions in depression: a review of the human evidence. Psychopharmacology. (2004) 173:1–17. doi: 10.1007/s00213-004-1774-1
35. Berardelli I, Serafini G, Cortese N, Fiasche F, O'Connor RC, Pompili M. The involvement of hypothalamus-pituitary-adrenal (HPA) axis in suicide risk. Brain Sci. (2020) 10:653. doi: 10.3390/brainsci10090653
36. Oquendo MA, Russo SA, Underwood MD, Kassir SA, Ellis SP, Mann JJ, et al. Higher postmortem prefrontal 5-HT2A receptor binding correlates with lifetime aggression in suicide. Biol Psychiatry. (2006) 59:235–43. doi: 10.1016/j.biopsych.2005.06.037
37. Mann JJ, Currier D. A review of prospective studies of biologic predictors of suicidal behavior in mood disorders. Arch Suicide Res. (2007) 11:3–16. doi: 10.1080/13811110600993124
38. Herman JP, Patel PD, Akil H, Watson SJ. Localization and regulation of glucocorticoid and mineralocorticoid receptor messenger RNAs in the hippocampal formation of the rat. Molecular endocrinology. (1989) 3:1886–94. doi: 10.1210/mend-3-11-1886
39. Herman JP, McKlveen JM, Ghosal S, Kopp B, Wulsin A, Makinson R, et al. Regulation of the hypothalamic-pituitary-adrenocortical stress response. Compr Physiol. (2016) 6:603–21. doi: 10.1002/cphy.c150015
40. Brady LS, Whitfield HJ Jr, Fox RJ, Gold PW, Herkenham M. Long-term antidepressant administration alters corticotropin-releasing hormone, tyrosine hydroxylase, and mineralocorticoid receptor gene expression in rat brain therapeutic implications. J Clin Invest. (1991) 87:831–7. doi: 10.1172/JCI115086
41. Meijer OC, Williamson A, Dallman MF, Pearce D. Transcriptional repression of the 5-HT1A receptor promoter by corticosterone via mineralocorticoid receptors depends on the cellular context. J Neuroendocrinol. (2000) 12:245–54. doi: 10.1046/j.1365-2826.2000.00445.x
42. Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci. (2003) 4:819–28. doi: 10.1038/nrn1220
43. Mann JJ, Brent DA, Arango V. The neurobiology and genetics of suicide and attempted suicide: a focus on the serotonergic system. Neuropsychopharmacology. (2001) 24:467–77. doi: 10.1016/S0893-133X(00)00228-1
44. Comai S, Costa CV, Ragazzi E, Bertazzo A, Allegri G. The effect of age on the enzyme activities of tryptophan metabolism along the kynurenine pathway in rats. Clin Chim Acta. (2005) 360:67–80. doi: 10.1016/j.cccn.2005.04.013
45. Sublette ME, Galfalvy HC, Fuchs D, Lapidus M, Grunebaum MF, Oquendo MA, et al. Plasma kynurenine levels are elevated in suicide attempters with major depressive disorder. Brain Behav Immun. (2011) 25:1272–8. doi: 10.1016/j.bbi.2011.05.002
46. Messaoud A, Mensi R, Douki W, Neffati F, Najjar MF, Gobbi G, et al. Reduced peripheral availability of tryptophan and increased activation of the kynurenine pathway and cortisol correlate with major depression and suicide. World J Biol Psychiatry. (2019) 20:703–11. doi: 10.1080/15622975.2018.1468031
47. Mann JJ. The serotonergic system in mood disorders and suicidal behaviour. Philos Trans R Soc Lond B Biol Sci. (2013) 368:20120537. doi: 10.1098/rstb.2012.0537
48. Harmer B, Lee S, Duong TVH, Saadabadi A. Suicidal Ideation. Treasure Island, FL: StatPearls Publishing Copyright (2022).
49. Breet E, Kidd M, McGregor NW, Stein DJ, Lochner C. Suicide ideation and attempts in obsessive-compulsive disorder. Ann Clin Psychiatry. (2019) 31:192–9. doi: 10.2174/1570159X16666180620155941
50. Bae SM, Lee YJ, Cho IH, Kim SJ, Im JS, Cho SJ. Risk factors for suicidal ideation of the general population. J Korean Med Sci. (2013) 28:602–7. doi: 10.3346/jkms.2013.28.4.602
51. Hor K, Taylor M. Suicide and schizophrenia: a systematic review of rates and risk factors. J Psychopharmacol. (2010). 24(Suppl. 4):81–90. doi: 10.1177/1359786810385490
Keywords: suicide attempt, cortisol, HPA axis, suicide behavior, stress, suicide
Citation: Genis-Mendoza AD, Dionisio-García DM, Gonzalez-Castro TB, Tovilla-Zaráte CA, Juárez-Rojop IE, López-Narváez ML, Castillo-Avila RG and Nicolini H (2022) Increased Levels of Cortisol in Individuals With Suicide Attempt and Its Relation With the Number of Suicide Attempts and Depression. Front. Psychiatry 13:912021. doi: 10.3389/fpsyt.2022.912021
Received: 03 April 2022; Accepted: 16 May 2022;
Published: 10 June 2022.
Edited by:
E. Erdal Erşan, Nigde Ömer Halisdemir University, TurkeyReviewed by:
Andrea Aguglia, University of Genoa, ItalyCopyright © 2022 Genis-Mendoza, Dionisio-García, Gonzalez-Castro, Tovilla-Zaráte, Juárez-Rojop, López-Narváez, Castillo-Avila and Nicolini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Alfonso Tovilla-Zaráte, YWxmb25zb190b3ZpbGxhekB5YWhvby5jb20ubXg=; Humberto Nicolini, aG5pY29saW5pQGlubWVnZW4uZ29iLm14
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.