 Neslihan Güzelsoy1,2†
Neslihan Güzelsoy1,2† Ulrike Ravens-Sieberer1*†
Ulrike Ravens-Sieberer1*† Joachim Westenhöfer2
Joachim Westenhöfer2 Janine Devine1Michael Erhart1,3,4Heike Hölling5Anne Kaman1
Janine Devine1Michael Erhart1,3,4Heike Hölling5Anne Kaman1- 1Department of Child and Adolescent Psychiatry, Psychotherapy, and Psychosomatics, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Department of Health Sciences, Faculty of Life Sciences, Competence Center Health, Hamburg University of Applied Sciences, Hamburg, Germany
- 3Department of Public Health, Alice Salomon University of Applied Science, Berlin, Germany
- 4Department of Psychology, Apollon University of Applied Science, Bremen, Germany
- 5Department of Epidemiology and Health Monitoring, Robert Koch Institute, Berlin, Germany
Background: Mental health during the COVID-19 pandemic is of particularly high relevance. Especially for children and adolescents, the pandemic and its restrictions represent a significant burden. The present study aims to identify risks and resources for depressive symptoms and anxiety in children and adolescents during the pandemic in Germany.
Materials and Methods: Self-reported data from the first wave of the longitudinal COVID-19 and Psychological Health (COPSY) study were used to investigate risks and resources among n = 811 children and adolescents aged 11–17 years. Depressive symptoms and anxiety were measured at the first follow-up 6 months later. Multivariate linear regression analyses were performed to investigate the effects of risks and resources on depressive symptoms and anxiety.
Results: Parental depressive symptoms predicted depressive symptoms and anxiety in children and adolescents 6 months later. Female gender was identified as a risk factor for anxiety during the pandemic. None of the potential resources were associated with depressive symptoms or anxiety at the follow-up.
Conclusion: The findings provide evidence of risk factors for depressive symptoms and anxiety during the COVID-19 pandemic. Children and adolescents who face risk factors need to be identified early and monitored during the pandemic. Family-based intervention programs are needed to help vulnerable children and adolescents cope with the challenges of the pandemic.
Introduction
The challenges and restrictions resulting from the COVID-19 pandemic can have a negative impact on mental health (1, 2). Studies from throughout the world have shown the adverse effects of the COVID-19 pandemic on the mental health of children and adolescents (3–6). Findings from the population-based longitudinal COVID-19 and Psychological Health (COPSY) study show that a majority of children and adolescents in Germany have felt burdened by the pandemic (1). The lack of contact with friends and homeschooling due to school closures represents an additional burden (7, 8). Family life was negatively affected as conflicts within the family increased and escalated more often (8, 9). The COPSY study found that during the pandemic health-related quality of life decreased and the stress level, sleeping problems, loneliness, hyperactivity/inattention, conduct problems, and psychosomatic symptoms increased (8, 10, 11). Of particular note is the significant increase in symptoms of depression and anxiety in children, which seem associated with pandemic measures (12–16).
Mental health problems in children may persist into adolescence and pose risk factors for the emergence of mental disorders in adulthood (17–19). Therefore, information on risk and resource factors that influence the development of mental health problems such as depressive and anxiety symptoms during the COVID-19 pandemic is crucial.
Existing research identifies risks and resources that are associated with the occurrence of mental problems such as depression and anxiety in children and adolescents. In terms of social risk and resources, studies indicate that social isolation and loneliness as well as lack of peer relationships are linked to depression and anxiety during the COVID-19 pandemic (2, 14, 20). Moreover, excessive or insufficient demands at school and educational failure have been associated with an increased risk of depression (21). School and kindergarten ideally are a resource and can provide social support, foster emotional development and coping with trauma (22, 23). Traumas like domestic violence, abuse or neglect, which increased during the COVID-19 pandemic (2, 24), can lead to adverse long-term effects such as mental problems in adulthood (25, 26). Especially for traumatized children, social and emotional support can protect against depressive symptoms (27). Studies show that peers, school and good relationships between children and teachers have a promoting effect on mental resilience (28–30).
Regarding familial risks, parental stress and psychopathology play a key role in children’s mental health (31, 32). Conflicts with parents and a negative family climate have an adverse impact on emotional health (33, 34). Children and adolescents whose mothers suffer from depression and those who have a negative mother-child relationship are at higher risk of developing internalizing problems such as depression (35–37). Conversely, a two-parent family structure, family cohesion and positive parenting are well-established resource factors for ameliorating mental problems (28, 36, 38).
Among personal factors, overall worse psychological health and preexisting psychiatric disorders present important risk factors for the deterioration of mental health (39). Quittkat et al. showed that the COVID-19 pandemic exacerbated the degree of symptom severity in children and adolescents with a history of mental problems (40). Self-esteem, a positive self-concept and an optimistic attitude (34, 38) as well as successful coping mechanisms (41, 42) can be considered resources for the mental health of youth.
Besides the psychosocial risks and resources, there are biological and sociodemographic factors associated with depressive symptoms and anxiety in youth. Female gender and puberty increase the risk of internalizing symptoms (43). Further, a low socioeconomic status as well as a migration background are strongly associated with psychological problems (8, 28, 44, 45). A study undertaken in Brazil during the COVID-19 pandemic demonstrated that anxiety rates are higher among children with parents who have essential jobs and who are separated from their parents (46). Quarantined youth living in high epidemic areas (47), who have a high-risk family member (48) or relatives infected with COVID-19 (49) also experienced higher rates of anxiety (6, 50, 51).
Overall, previous research has examined factors influencing the development of depressive symptoms and anxiety in youth before and at the beginning of the COVID-19 pandemic. However, there is a lack of knowledge regarding risks and resources for children and adolescents over the course of the pandemic based on longitudinal studies.
Therefore, the present population-based longitudinal study aims to determine which familial, personal as well as social risk and resources at the early stage of the pandemic predict depressive symptoms and anxiety over the course of the pandemic, i.e., 6 months later. Our hypotheses were that conflicts within the family, school stress and parental depressive symptoms (risk factors) predict depressive symptoms and anxiety in children and adolescents during the pandemic. Further, we assumed that a positive family climate, personal resources and social support (resource factors) are associated with fewer depressive symptoms and anxiety.
Materials and Methods
Study
The population-based longitudinal COPSY study examines the mental health and quality of life of children and adolescents aged 7–17 years during the COVID-19 pandemic in Germany. The design and methodology of the COPSY study is conceptualized based on the population-based longitudinal BELLA study. The BELLA study presents the mental health module of the German National Health Interview and Examination Survey for Children and Adolescents (KiGGS) (52). The first wave of the COPSY study was conducted from May 26th to June 10th, 2020. At that time Germany was under a partial nationwide lockdown, with educational institutions, leisure and cultural facilities partly closed or restricted. In total, n = 1,586 parents of children aged 7–17 years as well as n = 1,040 children and adolescents aged 11–17 years took part in the online survey. The second wave of the COPSY study took place from December 17th, 2020 to January 25th, 2021, during the second wave of the pandemic. At that time, there was a complete nationwide lockdown, with schools as well as leisure and cultural facilities closed. Families who had participated in the first wave of the COPSY study were re-contacted, informed about the second wave and asked for their consent. Overall, n = 1,288 families participated in the second wave (re-participation rate of 85.1%). A responder versus non-responder analysis revealed no significant differences in sociodemographic or health-related variables. The samples match the sociodemographic characteristics (age, gender, education, region) of the German population according to the Microcensus of 2018. The COPSY study was approved by the Local Psychological Ethics Committee and the Commissioner for Data Protection of the University of Hamburg. Detailed information on the design, methods and results of the first two waves of the COPSY study can be found elsewhere (1, 53).
Participants
In the present analysis, data from the baseline survey (wave 1) and the first follow-up (wave 2) of the COPSY study were used. Participants were included in the analysis if (i) they were 11–17 years old at baseline, provided self-reports, and (ii) their data of depressive and anxiety symptoms were available at follow-up. This resulted in a final sample of n = 811 children and adolescents.
Measures
Sociodemographic Variables
The self-report version of the online survey included questions on age and gender of the children and adolescents. In addition, the parent-reported version included further sociodemographic information on the educational and migration background of the parents. Socio-demographic data collected at baseline were defined as control variables in the regression analysis. Parental education was assessed in accordance with the Comparative Analyses of Social Mobility in Industrial Nations (CASMIN) classification. For this purpose, the highest academic and vocational qualifications of both parents were assessed by two items (54). A categorization into three status groups (low, medium and high parental education) was performed for sample description and further analysis. In addition, information on migration background was gathered by asking the parents two questions regarding their migration status.
Risk Factors
Conflicts within the family were assessed by one newly developed item (“To what degree did the frequency of arguments in your family change compared to before the pandemic?”) with a five-point response scale (1 = a lot more to 5 = much less). The variable was dichotomized into 0 = family conflicts did not increase (summarizing the response options much less, a little less and just as much) and 1 = family conflicts increased (combining the response options a lot more and a little more). School burden was also measured by one newly developed item (“How do you perceive schooling and learning/work now compared to a regular school or workday?”) presented with a five-point response scale (1 = a lot more difficult to 5 = much less difficult). The variable was dichotomized into 0 = school was not perceived as more stressful (combining the response options much less difficult, a little less difficult and both equal) and 1 = school was perceived as more stressful (summarizing the response options a lot more difficult and a little more difficult). Parental depressive symptoms were assessed by the eight-item Patient Health Questionnaire (PHQ-8), which is a valid diagnostic and severity measure for depressive disorders used in population-based studies (55). Each item (e.g., “Over the last week, how often have you been bothered by any of the following problems? Feeling down, depressed or hopeless”) was offered with four response options ranging from 1 = not at all to 4 = nearly every day). A scale sum score was calculated with values ranging from 0 to 24. A higher score indicates more severe depressive symptoms of parents.
Resource Factors
Personal resources were measured using five self-reported items administered in the KiGGS study (56). The scale captures individual capabilities such as self-efficacy, optimism, and a positive self-concept. The items (e.g., “I look to the future with optimism/confidence”) were provided with four-point response options (1 = not true to 4 = exactly true). The whole scale comprises total scores ranging from 5 to 20, with higher scores reflecting more pronounced personal resources. Four self-report items from the Family Climate Scale (FSC) were administered to assess family cohesion (57). The FSC collects data on sense of belonging and cohesiveness of individual family members. Each item (e.g., “In our family everybody cares about each other’s worries”) was provided with four-point response options (1 = not true to 4 = exactly true). The scale sum score ranges from 4 to 16. A higher sum score reflects a stronger family cohesion. Data on social support were collected using four self-report items from the German translation of the Social Support Scale (SSS) (58). The items (e.g., “How often has there been someone you can count on to listen to you when you need to talk”) were answered by children and adolescents using a five-point response options (1 = never to 5 = always). The scale comprises total values from 4 to 20, with higher scores demonstrating more social support.
Depressive Symptoms
The German version of the Center for Epidemiological Studies Depression Scale (CES-DC) was administered to assess self-reported depressive symptoms in children and adolescents at baseline and at follow-up 6 months later (59). The scale consists of seven items (e.g., “I felt sad”) offered with a four-point response scale (1 = rarely or not at all to 4 = mostly, all the time). A scale sum score was calculated with values ranging from 7 to 28. A higher score indicates more depressive symptoms.
Anxiety
To measure anxiety in children and adolescents at baseline and at follow-up 6 months later, the subscale for generalized anxiety from the Screen for Child Anxiety Related Disorders (SCARED) questionnaire was applied as self-report version (60). It includes nine items (e.g., “I worry about what is going to happen in the future”) presented with three response options (0 = not true or hardly ever true to 2 = very true or often true). The sum scale score ranges from 0 to 18, with higher scores indicating more anxiety.
Data Analysis
Descriptive analyses were carried out covering the calculation of frequencies, means and standard deviations of all variables. Bivariate analyses (chi-square tests, Spearman and Pearson correlations) were performed to examine associations between the predictor variables. Furthermore, linear regression analyses were conducted to determine to what degree the predictors can be considered as risk or resource factors for anxiety and depressive symptoms in children and adolescents. First, the association between each of the predictors and anxiety and depressive symptoms was examined using univariate linear regression analyses. Second, two multivariate linear regression models were carried out (one for anxiety and one for depressive symptoms). All predictor and control variables such as age, gender, parental education, and migration background were entered simultaneously into the regression models. For all regression analyses, metric variables were centered around the mean. All statistical analyses were performed using the SPSS version 25.
Results
Sample Characteristics
The analyzed sample including n = 811 children and adolescents aged 11–17 years (50.3% female) is described in Table 1. The majority of the children and adolescents were German (86.3%). The parents had a medium educational level (53.1%). The mean score for depressive symptoms at baseline was M = 11.35 and for anxiety M = 5.74. Among the risk factors, school stress was reported most often at 64.2%. Slightly more than a quarter of the children and adolescents reported an increase in family conflicts (26.4%). The mean scores of parental depressive symptoms was M = 5.17. Among the resource factors, the mean scores for personal resources were M = 15.30, for family climate M = 12.92 and for social support M = 16.35. Six months later, the mean score for depressive symptoms among the children and adolescents was M = 11.85 and M = 6.08 for anxiety.
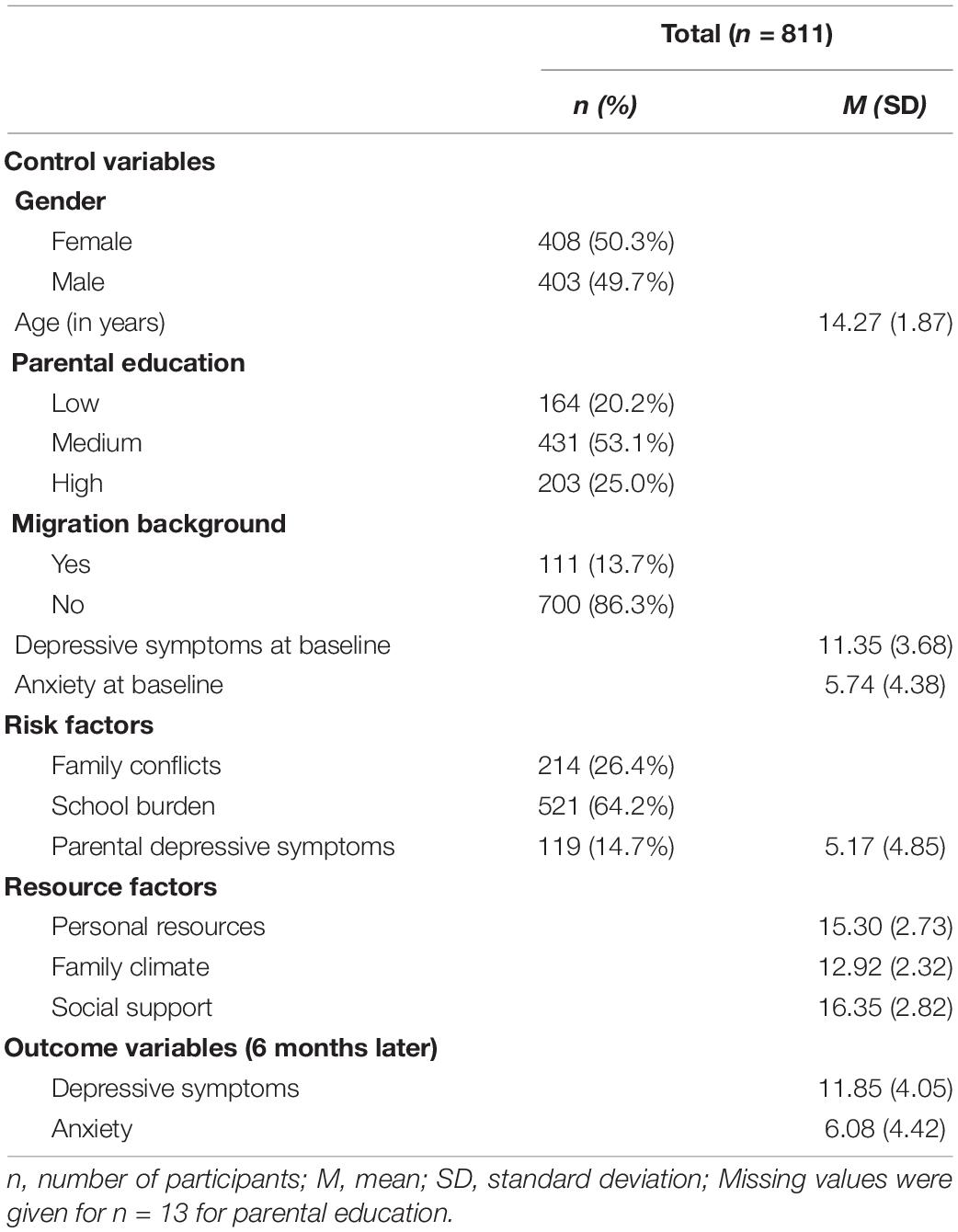
Table 1. Description of the analyzed sample of children and adolescents.
Correlations Between Predictors
The correlations between the control and predictor variables are shown in Table 2. The sociodemographic variables showed only weak associations with one another and with the risk and resource factors, with correlation coefficients less than r = 0.20. Depressive symptoms at baseline were strongly correlated with anxiety at baseline (r = 0.600, p < 0.001). Both depressive symptoms at baseline (r = –0.552, p < 0.001) as well as anxiety at baseline (r = –0.458, p < 0.001) showed strong correlations with personal resources. Among the risk factors, the highest intercorrelation was found between family conflicts and family climate (r = –0.291, p < 0.001) and between parental depressive symptoms and children’s depressive symptoms at baseline (r = 0.399, p < 0.001). In terms of resource factors, the strongest positive relationships were detected between family climate and personal resources (r = 0.486, p < 0.001) and between family climate and social support (r = 0.567, p < 0.001).
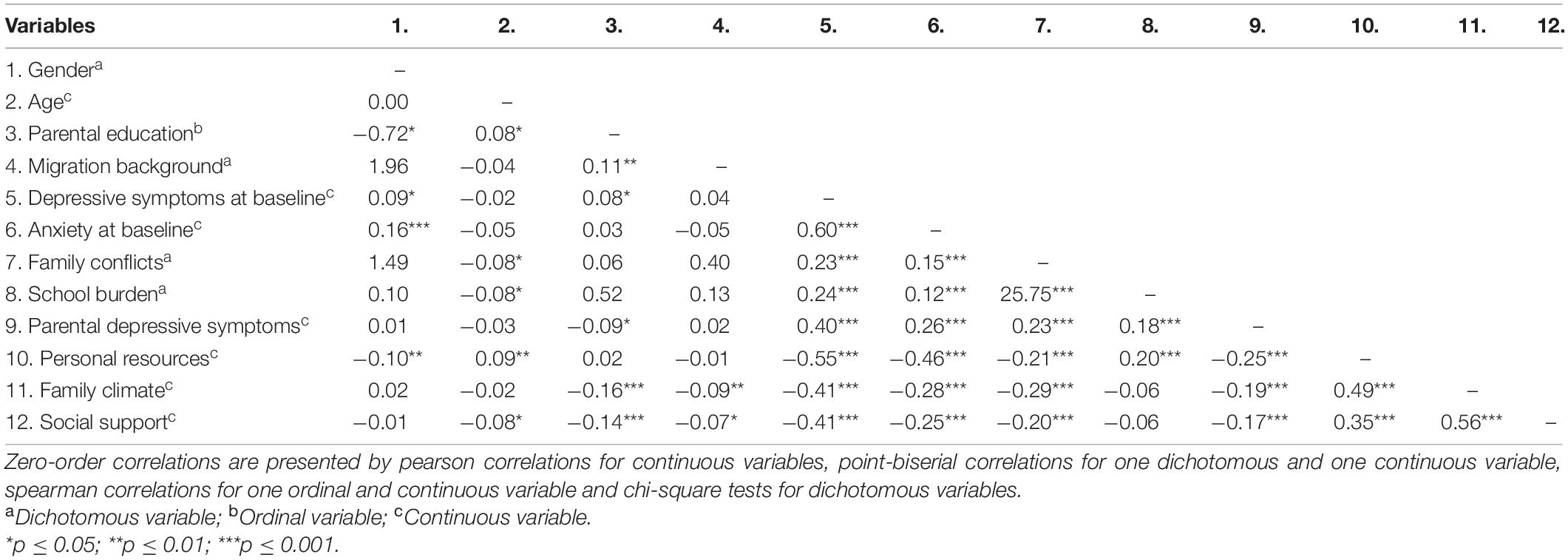
Table 2. Zero-order correlations among predictor variables.
Univariate Linear Regression Analyses
The results of the univariate regression analyses are presented in Supplementary Tables 1 and 2. The findings indicate that among the sociodemographic variables, only female gender was significantly associated with depressive symptoms (ß = 0.11, p = 0.002) and anxiety (ß = 0.16, p < 0.001) 6 months later. Depressive symptoms at baseline (ß = 0.60, p < 0.001) and anxiety at baseline (ß = 0.45, p < 0.001) were positively associated with depressive symptoms at follow-up. In addition, depressive symptoms at baseline (ß = 0.48, p < 0.001) and anxiety at baseline (ß = 0.64, p < 0.001) also showed positive associations with anxiety at follow-up. An examination of the risk factors revealed that all the risk factors proved to be significant predictors of later depressive symptoms and anxiety. Parental depressive symptoms were most strongly associated with depressive symptoms (ß = 0.39, p ≤ 0.001) and anxiety (ß = 0.27, p ≤ 0.001) at follow-up. In terms of resource factors, all were associated with fewer depressive symptoms and anxiety 6 months later. Personal resources demonstrated the strongest negative association with depressive symptoms (ß = –0.41, p ≤ 0.001) and anxiety (ß = –0.39, p ≤ 0.001) at follow-up.
Multivariate Linear Regression Analyses
The results of the multivariate linear regression analyses are presented in Tables 3 and 4. Among the sociodemographic variables, female gender proved to be a significant risk factor for later anxiety (ß = 0.07, p = 0.012). Findings from both models indicated that parental depressive symptoms were significantly positively associated with depressive symptoms (ß = 0.18, p < 0.001) and anxiety (ß = 0.08, p = 0.011) among youth 6 months later, which is in line with results of the univariate analysis. In addition, depressive symptoms at baseline (ß = 0.38, p < 0.001) as well as anxiety as baseline (ß = 0.13, p < 0.001) significantly predicted later depressive symptoms. Anxiety at baseline (ß = 0.53, p < 0.001) was strongly associated with anxiety at follow-up. Among the resource factors, none were significantly associated with depressive symptoms or anxiety 6 months later.
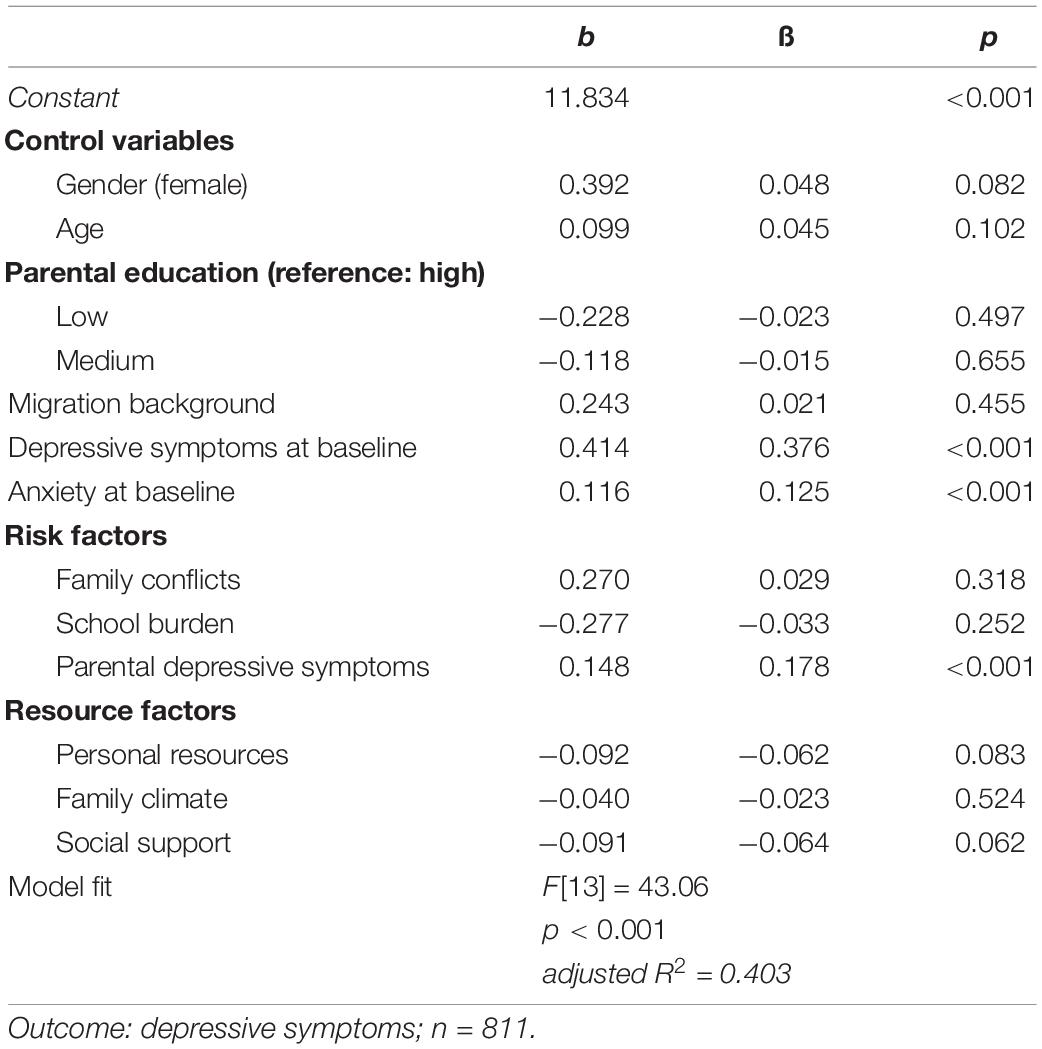
Table 3. Results of the multivariate linear regression analyses; risk and resource factors in children and adolescents predicting depressive symptoms 6 months later.
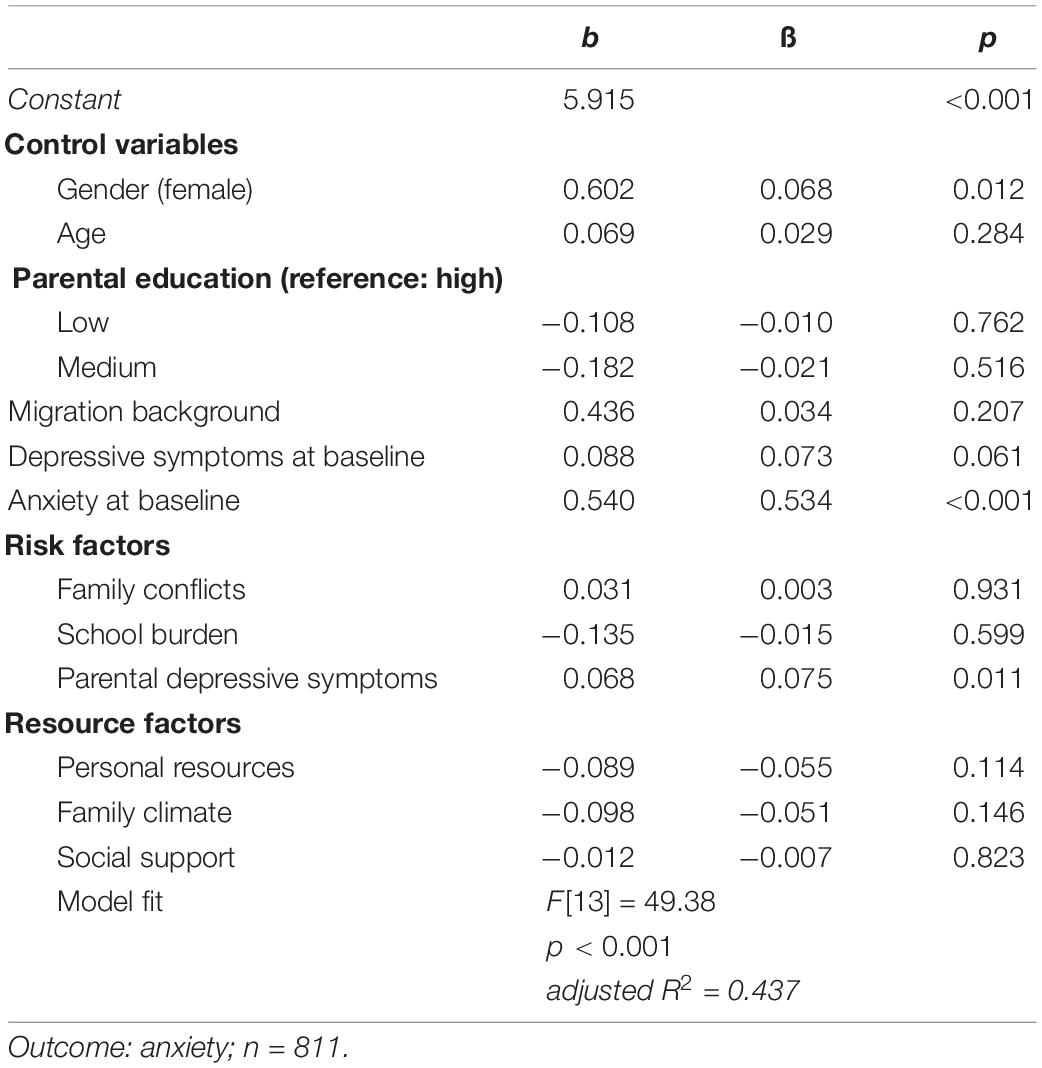
Table 4. Results of the multivariate linear regression analyses; risk and resource factors in children and adolescents predicting anxiety 6 months later.
Discussion
The aim of this study was to identify risk and resource factors for depressive symptoms and anxiety in children and adolescents during the COVID-19 pandemic. Findings of the population-based longitudinal COPSY study revealed that parental depressive symptoms were associated with stronger depressive symptoms and anxiety in children and adolescents during the pandemic. Other than expected none of the potential resources were associated with depressive symptoms or anxiety during the pandemic in our multivariate model.
Findings of the univariate regression analyses showed that the examined risk factors such as family conflicts, school burden and parental depressive symptoms were positively associated with stronger depressive symptoms and anxiety in children and adolescents during the pandemic. However, most of the identified risk factors did not predict later depressive symptoms and anxiety in our multivariate analysis. This might be due to the fact that in the interaction of several risk factors, family conflicts and school burden lose their significance. Further, controlling for depression and anxiety scores at baseline means that we modelled the change in depression and anxiety scores from baseline to follow-up. Thus, it is likely that predictors that are important for the occurrence of depression or anxiety per se might not turn out to be significant regarding the change in these outcomes.
In the multivariate model, only parental depressive symptoms emerged as a risk factor for depressive symptoms and anxiety in children and adolescents 6 months later. This finding is in line with previous studies investigating the relationship between parental psychopathology and mental disorders in children and adolescents (32, 36, 37).
In the univariate regression analyses, the examined factors such as personal resources, family climate and social support were significantly associated with fewer depressive symptoms and anxiety 6 months later. However, we found no direct effects of those resource factors in our multivariate model. Nevertheless, the important role of family cohesion in the context of internalizing mental health problems has been well examined in previous studies (35, 61, 62). Our results of the univariate regression analyses thus underline the importance of family-based intervention programs during the COVID-19 pandemic to support a positive family climate and strengthen family cohesion to mitigate the adverse effects of potential risk factors. Furthermore, special mental health counseling and support services should be offered for parents with depressive symptoms or mental health issues as well as for children and adolescents with pre-existing psychological health problems to cope with the additional burden of the pandemic.
Regarding the examined control variables, we found that depressive symptoms and anxiety at baseline were associated with depressive symptoms at follow-up. Moreover, anxiety at baseline predicted anxiety at follow-up. This finding is in line with the fact that mental disorders are highly recurrent and persistent and often last into adulthood (63). In addition, female gender was significantly associated with stronger symptoms of anxiety at follow-up, which is consistent with previous studies on gender distribution in internalizing disorders indicating that females are about twice as likely to experience anxiety compared to males (64, 65).
The present study shows the following limitations. The variables included in our multivariate regression analyses explained 40.3% of the variance in depressive symptoms and 43.7% of the variance in anxiety. Although this is a sizeable proportion, these findings may suggest that the development of depressive symptoms and anxiety during the COVID-19 pandemic is related to other important factors that we did not take into account in our models. These factors can be genetic risks, environmental aspects such as living conditions or the experience of stressful life events, domestic violence, and abuse (66). These aspects should be investigated in future studies. Moreover, it should be noted that the population-based COPSY study cannot identify causal relationships, as it is an observational study that only detects associations between risk and resource factors. Furthermore, it cannot be ruled out that other events occurred between the baseline and follow-up that influenced the development of depressive symptoms and anxiety during the pandemic. With regard to the assessment of depressive symptoms and anxiety measured by established and validated screening questionnaires it should be noted that these instruments are mostly not suitable for clinical diagnoses of mental health problems. The results of the COPSY study are neither generalizable nor transferable to other countries due to possible differences in study design and methodology as well as existing differences in conditions during the pandemic such as infection rates, lockdown measures and access to health care services.
The present study has the following strengths. First of all, the COPSY study is one of the first population-based longitudinal studies on health-related quality of life and mental health in children and adolescents with two measurement points during the COVID-19 pandemic. The study provides important findings on psychosocial risks and resources for the development of depressive symptoms and anxiety in children and adolescents during the pandemic, that are highly relevant for prevention, clinical practice and policy. The strengths of the COPSY study include the wide age range of the participants and the longitudinal analysis over a pandemic time period of 6 months. We examined a large population-based sample of n = 811 children and adolescents including their parents. Established self- and proxy-report measures were used to assess a range of psychosocial risk and resource factors. The self-reported data allowed insight into the perspective of children and young people.
Overall, the findings of the present study revealed that parental depressive symptoms were associated with stronger depressive symptoms and anxiety in children and adolescents during the COVID-19 pandemic. Given the high number of adults affected by depression and anxiety during the pandemic, the overall poorer mental health of parents is of particular concern for the emotional health of children and young people. Compared to pre-pandemic data showing a prevalence of 10.1% for depression among adults in Germany (67), the prevalence in this study, also assessed with the PHQ-8, is slightly higher at 14.7% during the pandemic. Other studies have also shown that parents reported higher rates of depression and anxiety during the pandemic compared to pre-pandemic estimates (68, 69). Mothers seem to be particularly impacted, most likely due to a higher burden caused by household chores, homecare/schooling and home office during lockdown phases (70, 71). These results are in line with several studies from Germany (72–74) as well as international reviews (75–78) reporting high prevalence rates for depression and anxiety in the general population during the pandemic.
Further, girls seem to be at higher risk than boys for developing anxiety during the pandemic. Special focus should also be placed on children and adolescents who have already shown depressive symptoms and anxiety at the start of the pandemic. These children and adolescents at higher risk for developing mental health problems during the COVID-19 pandemic need to be detected at an early stage to avoid mental health problems exacerbate into clinical mental disorders. Based on our findings, we recommend the implementation of low-threshold prevention and intervention measures such as resource-oriented and family-based as well as parent support programs in communities, kindergartens and schools to target this high risk youth. In addition, in the planning of lockdown measures such as school closures or social distancing, the mental health of children and adolescents should be carefully taken into account. Particularly politicians as well as education and healthcare professionals should be aware of the importance of preventive measures for child and adolescent mental health during the COVID-19 pandemic. The latter need to be empowered by financial resources to plan and implement such measures. Future research is needed to identify further risk and resource factors for the development of mental health problems in children and adolescents over the course of the pandemic, so that prevention and intervention measures can be adapted to the specific burden and needs of children and adolescents to help them cope with these challenging times.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The COPSY study was approved by the Local Psychological Ethics Committee and the Commissioner for Data Protection of the University of Hamburg, Germany. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
NG performed the statistical analyses, interpreted the data, and wrote the first draft of the manuscript. UR-S and AK were principle investigators of the COPSY study, responsible for its design, funding, general decisions of measurement, supervised data cleaning and preparation, and revised the manuscript critically. JW, JD, ME, and HH revised the manuscript critically. All authors contributed to the article and approved the final manuscript.
Funding
The COPSY study was funded by the Kroschke Child Foundation and the Fritz and Hildegard Berg Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or the preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all children, adolescents and their parents who participated in this study for their time and involvement.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.901783/full#supplementary-material
References
1. Ravens-Sieberer U, Kaman A, Erhart M, Devine J, Schlack R, Otto C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur Child Adolesc Psychiatry. (2021) 31:879–89. doi: 10.1007/s00787-021-01726-5
2. Witt A, Ordóñez A, Martin A, Vitiello B, Fegert JM. Child and adolescent mental health service provision and research during the COVID-19 pandemic: challenges, opportunities, and a call for submissions. Child Adolesc Psychiatry Mental Health. (2020) 14:19. doi: 10.1186/s13034-020-00324-8
3. Adıbelli D, Sümen A. The effect of the coronavirus (COVID-19) pandemic on health-related quality of life in children. Child Youth Serv Rev. (2020) 119:105595. doi: 10.1016/j.childyouth.2020.105595
4. Bignardi G, Dalmaijer ES, Anwyl-Irvine AL, Smith TA, Siugzdaite R, Uh S, et al. Longitudinal increases in childhood depression symptoms during the COVID-19 lockdown. Arch Dis Child. (2021) 106:791–7. doi: 10.1136/archdischild-2020-320372
5. Wang G, Zhang Y, Zhao J, Zhang J, Jiang F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet. (2020) 395:945–7. doi: 10.1016/S0140-6736(20)30547-X
6. Xie X, Xue Q, Zhou Y, Zhu K, Liu Q, Zhang J, et al. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei province, China. JAMA Pediatr. (2020) 174:898–900. doi: 10.1001/jamapediatrics.2020.1619
7. Ezpeleta L, Navarro JB, de la Osa N, Trepat E, Penelo E. Life conditions during COVID-19 lockdown and mental health in Spanish adolescents. Int J Environ Res Public Health. (2020) 17:7327. doi: 10.3390/ijerph17197327
8. Ravens-Sieberer U, Otto C, Kaman A, Adedeji A, Devine J, Napp A-K, et al. Mental health and quality of life in children and adolescents during the COVID-19 pandemic. Dtsch Aerztebl Online. (2020) 117:828–9.
9. Langmeyer A, Guglhör-Rudan A, Naab T, Urlen M, Winklhofer U. Kindsein in Zeiten von Corona Erste Ergebnisse zum veränderten Alltag und zum Wohlbefinden von Kindern. München: Deutsches Jugendinstitut (2020).
10. Chi X, Becker B, Yu Q, Willeit P, Jiao C, Huang L, et al. Prevalence and psychosocial correlates of mental health outcomes among Chinese college students during the coronavirus disease (COVID-19) pandemic. Front Psychiatry. (2020) 11:803. doi: 10.3389/fpsyt.2020.00803
11. Orgilés M, Morales A, Delvecchio E, Mazzeschi C, Espada JP. Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Front Psychol. (2020) 11:579038. doi: 10.3389/fpsyg.2020.579038
12. Fegert JM, Vitiello B, Plener PL, Clemens V. Challenges and burden of the coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Mental Health. (2020) 14:20. doi: 10.1186/s13034-020-00329-3
13. Jones EAK, Mitra AK, Bhuiyan AR. Impact of COVID-19 on mental health in adolescents: a systematic review. Int J Environ Res Public Health. (2021) 18:2470. doi: 10.3390/ijerph18052470
14. Loades ME, Chatburn E, Higson-Sweeney N, Reynolds S, Shafran R, Brigden A, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. (2020) 59:1218–1239.e3. doi: 10.1016/j.jaac.2020.05.009
15. Ma L, Mazidi M, Li K, Li Y, Chen S, Kirwan R, et al. Prevalence of mental health problems among children and adolescents during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. (2021) 293:78–89. doi: 10.1016/j.jad.2021.06.021
16. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19. JAMA Pediatr. (2021) 175:1142–50. doi: 10.1001/jamapediatrics.2021.2482
17. Angold A, Egger HL. Preschool psychopathology: lessons for the lifespan. J Child Psychol Psychiatry. (2007) 48:961–6. doi: 10.1111/j.1469-7610.2007.01832.x
18. Anselmi L, Barros FC, Teodoro MLM, Piccinini CA, Menezes AMB, Araujo CL, et al. Continuity of behavioral and emotional problems from pre-school years to pre-adolescence in a developing country. J Child Psychol Psychiatry. (2008) 49:499–507. doi: 10.1111/j.1469-7610.2007.01865.x
19. Costello EJ, Egger H, Angold A. 10-Year research update review: the epidemiology of child and adolescent psychiatric disorders: i. Methods and public health Burden. J Am Acad Child Adolesc Psychiatry. (2005) 44:972–86. doi: 10.1097/01.chi.0000172552.41596.6f
20. Imran N, Zeshan M, Pervaiz Z. Mental health considerations for children & adolescents in COVID-19 Pandemic. Pak J Med Sci. (2020) 36:S67–672. doi: 10.12669/pjms.36.COVID19-S4.2759
21. Mehler-Wex C, Kölch M. Depression in children and adolescents. Dtsch Aerztebl Online. (2008) 105:149–55. doi: 10.3238/arztebl.2008.0149
22. Green JG, McLaughlin KA, Alegría M, Costello EJ, Gruber MJ, Hoagwood K, et al. School mental health resources and adolescent mental health service use. J Am Acad Child Adolesc Psychiatry. (2013) 52:501–10. doi: 10.1016/j.jaac.2013.03.002
23. Phelps C, Sperry LL. Children and the COVID-19 pandemic. Psychol Trauma. (2020) 12:S73–5. doi: 10.1037/tra0000861
24. Walker DM, Tolentino VR. COVID-19: the impact on pediatric emergency care. Pediatr Emerg Med Pract. (2020) 17:1–27.
25. Copeland WE, Shanahan L, Hinesley J, Chan RF, Aberg KA, Fairbank JA, et al. Association of childhood trauma exposure with adult psychiatric disorders and functional outcomes. JAMA Netw Open. (2018) 1:e184493. doi: 10.1001/jamanetworkopen.2018.4493
26. de Bellis MD, Zisk A. The biological effects of childhood trauma. Child Adolesc Psychiatr Clin N Am. (2014) 23:185–222. doi: 10.1016/j.chc.2014.01.002
27. Brinker J, Cheruvu VK. Social and emotional support as a protective factor against current depression among individuals with adverse childhood experiences. Prev Med Rep. (2017) 5:127–33. doi: 10.1016/j.pmedr.2016.11.018
28. Costello DM, Swendsen J, Rose JS, Dierker LC. Risk and protective factors associated with trajectories of depressed mood from adolescence to early adulthood. J Consul Clin Psychol. (2008) 76:173–83. doi: 10.1037/0022-006X.76.2.173
29. Miller-Lewis LR, Searle AK, Sawyer MG, Baghurst PA, Hedley D. Resource factors for mental health resilience in early childhood: an analysis with multiple methodologies. Child Adolesc Psychiatry Mental Health. (2013) 7:6. doi: 10.1186/1753-2000-7-6
30. Shin KM, Cho S-M, Shin YM, Park KS. Effects of early childhood peer relationships on adolescent mental health: a 6- to 8-year follow-up study in South Korea. Psychiatry Invest. (2016) 13:383–8. doi: 10.4306/pi.2016.13.4.383
31. Crum KI, Moreland AD. Parental stress and children’s social and behavioral outcomes: the role of abuse potential over time. J Child Fam Stud. (2017) 26:3067–78. doi: 10.1007/s10826-017-0822-5
32. McLaughlin KA, Gadermann AM, Hwang I, Sampson NA, Al-Hamzawi A, Andrade LH, et al. Parent psychopathology and offspring mental disorders: results from the WHO world mental health surveys. Br J Psychiatry. (2012) 200:290–9. doi: 10.1192/bjp.bp.111.101253
33. Naab S, Kunkel J, Fumi M, Voderholzer U. Psychosoziale risikofaktoren für psychische störungen im jugendalter. DNP Der Neurol Psychiater. (2017) 18:26–32. doi: 10.1007/s15202-017-1674-y
34. Wille N, Bettge S, Ravens-Sieberer U. Risk and protective factors for children’s and adolescents’ mental health: results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17:133–47. doi: 10.1007/s00787-008-1015-y
35. Kaman A, Otto C, Klasen F, Westenhöfer J, Reiss F, Hölling H, et al. Risk and resource factors for depressive symptoms during adolescence and emerging adulthood – a 5-year follow-up using population-based data of the BELLA study. J Affect Disord. (2021) 280:258–66. doi: 10.1016/j.jad.2020.11.036
36. Klasen F, Otto C, Kriston L, Patalay P, Schlack R, Ravens-Sieberer U. Risk and protective factors for the development of depressive symptoms in children and adolescents: results of the longitudinal BELLA study. Eur Child Adolesc Psychiatry. (2015) 24:695–703. doi: 10.1007/s00787-014-0637-5
37. Kötter C, Stemmler M, Lösel F, Bühler A, Jaursch S. Mittelfristige effekte des präventionsprogramms EFFEKT-E für emotional belastete mütter und ihre kinder unter besonderer berücksichtigung psychosozialer risikofaktoren. Z Gesundheitspsychol. (2011) 19:122–33. doi: 10.1026/0943-8149/a000043
38. Job A-K, Dalkowski L, Hahlweg K, Muschalla B, Schulz W. Resilienz: längsschnittliche betrachtung von kindern mit risikofaktoren. Prax Kinderpsychol Kinderpsychiatr. (2020) 69:749–67. doi: 10.13109/prkk.2020.69.8.749
39. Lee J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc Health. (2020) 4:421. doi: 10.1016/S2352-4642(20)30109-7
40. Quittkat HL, Düsing R, Holtmann F-J, Buhlmann U, Svaldi J, Vocks S. Perceived impact of COVID-19 across different mental disorders: a study on disorder-specific symptoms, psychosocial stress and behavior. Front Psychol. (2020) 11:586246. doi: 10.3389/fpsyg.2020.586246
41. Duan L, Shao X, Wang Y, Huang Y, Miao J, Yang X, et al. An investigation of mental health status of children and adolescents in china during the outbreak of COVID-19. J Affect Disord. (2020) 275:112–8. doi: 10.1016/j.jad.2020.06.029
42. Mohammadzadeh F, Delshad Noghabi A, Khosravan S, Bazeli J, Armanmehr V, Paykani T. Anxiety severity levels and coping strategies during the COVID-19 pandemic among people aged 15 years and above in Gonabad, Iran. Arch Iran Med. (2020) 23:633–8. doi: 10.34172/aim.2020.76
43. Belhadj Kouider E, Petermann F. Gemeinsame risikofaktoren von depressiver und ängstlicher symptomatik im kindes- und jugendalter: ein systematisches review aus transdiagnostischer perspektive. Fortschr Neurol Psychiatr. (2015) 83:321–33. doi: 10.1055/s-0035-1553089
44. Klasen F, Meyrose A-K, Otto C, Reiss F, Ravens-Sieberer U. Psychische auffälligkeiten von kindern und jugendlichen in Deutschland. Monatsschr Kinderheilkd. (2017) 165:402–7. doi: 10.1007/s00112-017-0270-8
45. Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med. (2013) 90:24–31. doi: 10.1016/j.socscimed.2013.04.026
46. Garcia de Avila M, Hamamoto Filho P, Jacob F, Alcantara L, Berghammer M, Jenholt Nolbris M, et al. Children’s anxiety and factors related to the COVID-19 pandemic: an exploratory study using the children’s anxiety questionnaire and the numerical rating scale. Int J Environ Res Public Health. (2020) 17:5757. doi: 10.3390/ijerph17165757
47. Jiao WY, Wang LN, Liu J, Fang SF, Jiao FY, Pettoello-Mantovani M, et al. Behavioral and emotional disorders in children during the COVID-19 epidemic. J. Pediatr. (2020) 221: 264–266.e1. doi: 10.1016/j.jpeds.2020.03.013
48. Khademian F, Delavari S, Koohjani Z, Khademian Z. An investigation of depression, anxiety, and stress and its relating factors during COVID-19 pandemic in Iran. BMC Public Health. (2021) 21:275. doi: 10.1186/s12889-021-10329-3
49. Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. (2020) 287:112934. doi: 10.1016/j.psychres.2020.112934
50. Meyer J, McDowell C, Lansing J, Brower C, Smith L, Tully M, et al. Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. Int J Environ Res Public Health. (2020) 17:6469. doi: 10.3390/ijerph17186469
51. Saurabh K, Ranjan S. Compliance and psychological impact of quarantine in children and adolescents due to COVID-19 pandemic. Indian J Pediatr. (2020) 87:532–6. doi: 10.1007/s12098-020-03347-3
52. Ravens-Sieberer U, Kurth B-M. The mental health module (BELLA study) within the German health interview and examination survey of children and adolescents (KiGGS): study design and methods. Eur Child Adolesc Psychiatry. (2008) 17:10–21. doi: 10.1007/s00787-008-1002-3
53. Ravens-Sieberer U, Kaman A, Erhart M, Otto C, Devine J, Löffler C, et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: results of a two-wave nationwide population-based study. Eur Child Adolesc Psychiatry. (2021) 30:1–14. doi: 10.1007/s00787-021-01889-1
54. Brauns H, Scherer S, Steinmann S. The CASMIN educational classification in international comparative research. In: JHP Hoffmeyer-Zlotnik, C Wolf editors. Advances in Cross-National Comparison. (Boston, MA: Springer US) (2003). doi: 10.1007/978-1-4419-9186-7_11
55. Kroenke K, Strine TW, Spitzer RL, Williams JBW, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. (2009) 114:163–73. doi: 10.1016/j.jad.2008.06.026
56. Erhart M, Hölling H, Bettge S, Ravens-Sieberer U, Schlack R. Der kinder– und Jugendgesundheitssurvey (KiGGS): risiken und ressourcen für die psychische entwicklung von kindern und jugendlichen. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2007) 50:800–9. doi: 10.1007/s00103-007-0243-5
57. Schneewind K, Beckmann M, Hecht-Jackl A. Familienklima-Skalen. Bericht 8.1 und 8.2.. Institut für Psychologie–Persönlichkeitspsychologie und Psychodiagnostik. München: Ludwig Maximilians Universität (1985).
58. Donald CA, Ware JE. The measurement of social support. Res Commun Mental Health. (1984) 4:325–370.
59. Barkmann C, Erhart M, Schulte-Markwort M. The German version of the centre for epidemiological studies depression scale for children: psychometric evaluation in a population-based survey of 7 to 17 years old children and adolescents – results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17:116–24. doi: 10.1007/s00787-008-1013-0
60. Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M. Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry. (1999) 38:1230–6. doi: 10.1097/00004583-199910000-00011
61. Queen AH, Stewart LM, Ehrenreich-May J, Pincus DB. Mothers’ and fathers’ ratings of family relationship quality: associations with preadolescent and adolescent anxiety and depressive symptoms in a clinical sample. Child Psychiatry Hum Dev. (2013) 44:351–60. doi: 10.1007/s10578-012-0329-7
62. Sze T-M, Lin S-H, Hsieh P-J, Chen I-J. Sex differences in the development of perceived family cohesion and depressive symptoms in Taiwanese adolescents. Psychol Rep. (2013) 113:1066–84. doi: 10.2466/10.02.PR0.113x18z2
63. Kessler RC, Avenevoli S, Costello EJ, Georgiades K, Green JG, Gruber MJ, et al. Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry. (2012) 69:372–80. doi: 10.1001/archgenpsychiatry.2011.160
64. Klasen F, Petermann F, Meyrose A-K, Barkmann C, Otto C, Haller A-C, et al. Verlauf psychischer auffälligkeiten von kindern und jugendlichen. Kindheit Entwickl. (2016) 25:10–20. doi: 10.1026/0942-5403/a000184
65. Winkler D, Pjrek E, Kasper S. Gender-specific symptoms of depression and anger attacks. J Mens Health Gender. (2006) 3:19–24. doi: 10.1016/j.jmhg.2005.05.004
66. Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. (2012) 379:1056–67. doi: 10.1016/S0140-6736(11)60871-4
67. Bretschneider J, Kuhnert R, Hapke U. Depressive symptoms in adults in Germany. J Health Monit. (2017) 2:81–88. doi: 10.17886/RKI-GBE-2017-058
68. Wu KK, Chan SK, Ma TM. Posttraumatic stress, anxiety, and depression in survivors of severe acute respiratory syndrome (SARS). J Trauma Stress. (2005) 18:39–42. doi: 10.1002/jts.20004
69. Westrupp EM, Bennett C, Berkowitz T, Youssef GJ, Toumbourou JW, Tucker R, et al. Child, parent, and family mental health and functioning in Australia during COVID-19: comparison to pre-pandemic data. Eur Child Adolesc Psychiatry. (2021) 30:1–14. doi: 10.1007/s00787-021-01861-z
70. Racine N, Hetherington E, McArthur BA, McDonald S, Edwards S, Tough S, et al. Maternal depressive and anxiety symptoms before and during the COVID-19 pandemic in Canada: a longitudinal analysis. Lancet Psychiatry. (2021) 8:405–15. doi: 10.1016/S2215-0366(21)00074-2
71. Cameron EE, Joyce KM, Delaquis CP, Reynolds K, Protudjer JLP, Roos LE. Maternal psychological distress & mental health service use during the COVID-19 pandemic. J Affect Disord. (2020) 276:765–74. doi: 10.1016/j.jad.2020.07.081
72. Calvano C, Engelke L, di Bella J, Kindermann J, Renneberg B, Winter SM. Families in the COVID-19 pandemic: parental stress, parent mental health and the occurrence of adverse childhood experiences – results of a representative survey in Germany. Eur Child Adolesc Psychiatry. (2021) 30:1–13. doi: 10.1007/s00787-021-01739-0
73. Beutel ME, Hettich N, Ernst M, Schmutzer G, Tibubos AN, Braehler E. Mental health and loneliness in the German general population during the COVID-19 pandemic compared to a representative pre-pandemic assessment. Sci Rep. (2021) 11:14946. doi: 10.1038/s41598-021-94434-8
74. Jacob L, Smith L, Koyanagi A, Oh H, Tanislav C, Shin JIl, et al. Impact of the coronavirus 2019 (COVID-19) pandemic on anxiety diagnosis in general practices in Germany. J Psychiatr Res. (2021) 143:528–33. doi: 10.1016/j.jpsychires.2020.11.029
75. Lakhan R, Agrawal A, Sharma M. Prevalence of depression, anxiety, and stress during COVID-19 pandemic. J Neurosci Rural Pract. (2020) 11:519–25. doi: 10.1055/s-0040-1716442
76. Luo M, Guo L, Yu M, Jiang W, Wang H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – a systematic review and meta-analysis. Psychiatry Res. (2020) 291:113190. doi: 10.1016/j.psychres.2020.113190
77. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatry. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
Keywords: COVID-19, mental health, risk factors, resource factors, children and adolescents
Citation: Güzelsoy N, Ravens-Sieberer U, Westenhöfer J, Devine J, Erhart M, Hölling H and Kaman A (2022) Risks and Resources for Depressive Symptoms and Anxiety in Children and Adolescents During the COVID-19 Pandemic – Results of the Longitudinal COPSY Study. Front. Psychiatry 13:901783. doi: 10.3389/fpsyt.2022.901783
Received: 22 March 2022; Accepted: 20 June 2022;
Published: 07 July 2022.
Edited by:
Jean Marc Guile, University of Picardie Jules Verne, FranceReviewed by:
Eva Skoda, LVR-University Hospital Essen, GermanyVitale Elsa, Bari Local Health Authority, Italy
Copyright © 2022 Güzelsoy, Ravens-Sieberer, Westenhöfer, Devine, Erhart, Hölling and Kaman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulrike Ravens-Sieberer, cmF2ZW5zLXNpZWJlcmVyQHVrZS5kZQ==
†These authors have contributed equally to this work and share first authorship