 Dorothy Newbury-Birch
Dorothy Newbury-Birch Jennifer Ferguson
Jennifer Ferguson Natalie Connor
Natalie Connor
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 07 July 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.900186
This article is part of the Research Topic The Evidence and Practice-Gap of Screening and Brief Interventions for Substance Misuse View all 9 articles
Although the relationship is complex, there is an association between alcohol use and offending behavior with an interplay between the amount drank, the pattern of drinking and individual and contextual factors. Alcohol brief interventions have been shown to be effective in primary healthcare, however there is currently a lack of compelling evidence in the criminal justice system. We carried out a rapid systematic review of the literature, which updated our review conducted in 2016. Following systematic searches, we included 36 papers on prevalence and 13 papers on effectiveness. Between 26 and 88% of individuals in the policy custody setting scored positive for an alcohol use disorder. In the magistrates court this was 95%; 31–86% in the probation setting and between 19 and 86% in the prison system. In relation to probable dependence, between 21 and 38% of individuals were shown to have probable alcohol dependence in the police custody suite setting; 39 per cent in the magistrate court system; 17–36% in the probation setting and between 18 and 48% in the prison system. This compares to 6% in the general population. We included 13 studies of effectiveness with differing outcome measures and outcomes. We conclude more studies are needed in the field to develop the current evidence base.
An estimated 3.8% of all global deaths and 4-6% of global disability-adjusted life-years are attributable to alcohol (1). Although the relationship is complex, there is an association between alcohol use and offending behavior (2, 3), with an interplay between the amount drank, the pattern of drinking and individual and contextual factors (4). In England and Wales, alcohol-related crime is estimated to cost society £11.4 billion (5) and drugs £20 billion annually (6). Effective interventions have the potential to significantly reduce the costs relating to substance use, as well as increase individual social welfare (7).
Hazardous drinking is a repeated pattern of drinking that increases the risk of psychological or physical problems (8), whereas harmful drinking is defined by the presence of these problems (9). Drinking at hazardous or harmful levels are often categorized as risky drinking. Previous research has shown that risky drinking is more than twice as high in the criminal justice system (CJS), in comparison with the general population, in the UK, and probable dependency up to 10 times higher (10).
Alcohol brief interventions (ABIs) are a secondary prevention activity, which are aimed at those individuals who are drinking in a pattern that is likely to be harmful to health and/or well-being. They have been frequently shown to be effective in primary healthcare (11, 12), but they are typically delivered by practitioners who are not addiction specialists, to non-treatment, opportunistic populations (13).
They largely consist of two different approaches; simple structured advice, which after screening, raises awareness through provision of personalized feedback and advice on steps to reduce drinking behavior and its adverse consequences; and an extended brief intervention, which generally involves behavior change counseling. Extended brief intervention introduces and evokes change by giving the participant the opportunity to explore their alcohol use, as well as their motivations and strategies for change. Both forms share the common aim of helping people to change drinking behavior to promote health (13).
There is a wide variation in the duration and frequency of ABIs. However, typically they consist of between one and four sessions and are very short in nature (between five and 60 minutes) (14). They generally include personalized feedback on alcohol intake in relation to what the recommended limits are, discussion of both health and social risks and may include setting personal targets which can include psychological and motivational interviewing (14). One example of this is using the FRAMES (feedback, responsibility, advice, menus, empathy, self-efficacy approach (13).
They are generally delivered in an opportunistic way by practitioners other than addiction specialists, in a wide variety of settings (12). Due to the established links between risky drinking and crime and the costs to society, in both health and social care, it is important to find interventions that are effective. It has been shown that interventions that capitalize on the “teachable moment” are conducive with behavior change, where individuals consider their alcohol use within the context of their offending behavior and its punitive consequences (15, 16). However, to date, there is a dearth of evidence relating to alcohol use disorders (AUDs) and the use of brief interventions in the CJS (10, 17). Therefore, this review was proposed as a way to update and collate the evidence around the prevalence of AUDs within the CJS and to review the evidence around the efficacy of alcohol brief interventions within these populations.
The aim of this rapid review was to update our 2016 review (10) and to identify the levels of AUDs in the various stages of the CJS around the world. Secondly it aimed to narratively review worldwide studies of the effectiveness of ABIs in the various stages of the CJS.
We carried out a review of the international literature, employing the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, which ensure comprehensive reporting within systematic reviews (18). This rapid systematic review was conducted to update the review undertaken in 2016 (10). However, the original review only included prevalence in the UK, whereas this current review was extended to include worldwide literature.
Any language paper was eligible for inclusion.
Papers were included in the review if they contained information around alcohol use prevalence or were trials investigating the efficacy of ABIs, within the CJS. The following criteria were used for selection;
This review sought to identify the prevalence of AUDs in the CJS worldwide, by searching the available evidence. To ensure reliability, it was important for papers to use a screening tool that is validated when assessing the prevalence of AUDs (10). Therefore, we included papers that employed the use of the Alcohol Use Disorders Identification Test (AUDIT), which is considered to be the gold standard of tools used to identify AUDs in healthcare settings (19). The AUDIT gives prevalence data and is not a diagnostic tool.
The 10 question AUDIT is scored between 0–40. A score of 8+ for adults indicates an alcohol use disorder; 8–15 indicates hazardous drinking, 16–19 harmful drinking and a score of 20+ indicates probable dependence (20). It has been shown to have 92% sensitivity and 94% specificity (20). Furthermore, it has been shown to be effective in the various stages of the CJS (21). Any papers that did not report the use of the AUDIT, to identify prevalence, were excluded.
Using the same literature searches we also looked to include trials of ABIs in the CJS. We used the definitions of ABIs as listed in the background and sought to include studies with control groups comprising of any other intervention, no assessment, assessment only, information only or treatment as usual. We included studies that included psychosocial interventions up to a total of 3 hours of ABIs either in one or multiple sessions.
Papers predating 2000 were not considered, and searches were restricted to 2000- present (January 2022). We also excluded papers that included a drug and alcohol intervention where alcohol information could not be easily extracted.
The following databases; EBSCO (Child Development & Adolescent Studies, CINAHL Complete, Criminal Justice Abstracts with Full Text, MEDLINE, APA PsycArticles, Psychology and Behavioral Sciences Collection, APA PsycInfo) and Scopus were searched using the search terms alcohol, screening, crime, police probation, court, jail, prison and variations of these in the title, keywords and abstract.
Two authors were involved in the sifting of the published papers (DNB and JF). DNB reviewed all abstracts and full papers and JF acted as the second reviewer, reviewing 20% to ascertain that all decisions matched, which they did, without the need for a third reviewer. Endnote was used to manage the data in the sifting stages, whilst data extraction was carried out using Microsoft Excel, which was again undertaken by DNB and JF reviewing 20%. Data was extracted in the same way as our previous review, using the same data extraction tables, except that the country of study was added to the prevalence extraction table (10).
Gray literature was also searched from around the world, with variations of the search terms being entered into Google and the first 300 hits were investigated by NC, AD and GW. We also interrogated our previous papers on the subject (10, 17), screened the reference lists of included papers and reached out through the International Network on Brief Interventions for Alcohol and Other Drugs (Inebria- http://inebria.net/) and Twitter to obtain any further articles, and to ensure no potentially relevant studies had been overlooked.
The relevant screening tools from the Critical Appraisal Skills Programme (CASP) were used to quality assess any included papers (22). The QA was carried out across the research team (GW, AD and NC) with 20% being double checked. High risk of bias was recorded if “no” or “unsure” was recorded for 6 or more of the 11 questions on the tool. Medium risk of bias was assigned if “no” or “unsure” was recorded for 4–5 questions and Low risk for 1–3 questions, as in our previous study (17).
In total 10,898 papers were identified from the initial searches. Following the first sift, 189 full papers were assessed for inclusion. After completion of full text screening 40 papers were deemed eligible for inclusion. Figure 1 provides a breakdown of the numbers of papers and gray literature excluded at each stage and how many papers were used in assessing the prevalence vs. the alcohol brief intervention efficacy.
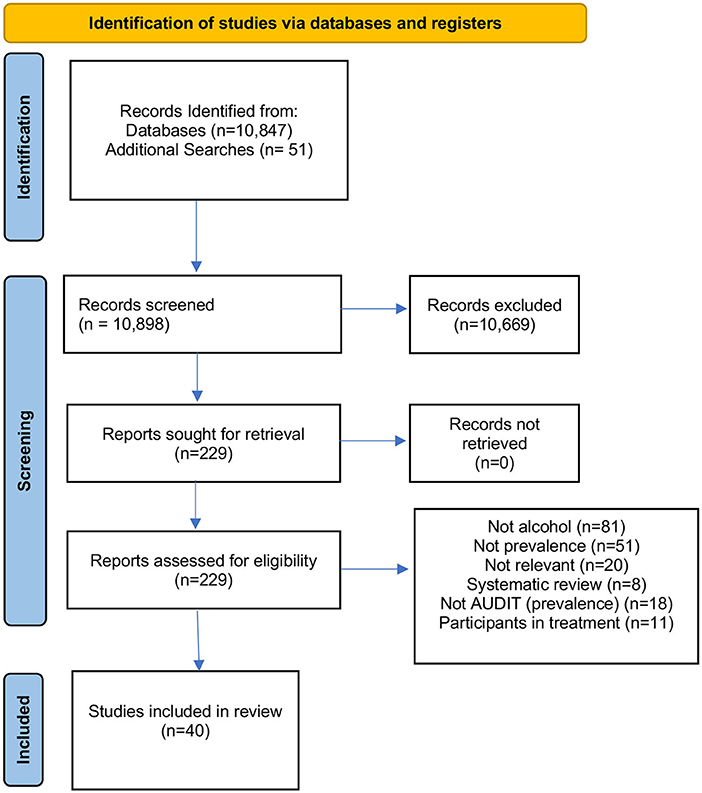
Figure 1. Data flow.
In total, 39 studies from 34 papers were included, as presented in Table 1. The majority of papers were from the UK (4, 11, 21, 23, 24, 26–32, 34–37, 39, 41–43, 47–49, 54), two from Sweden (25, 44) and one each from Australia (51), Brazil (45), Ethiopia (52), France (40), Holland (38), Norway (50), Ukraine (46) and the USA (53).

Table 1. Alcohol use disorder prevalence.
One study of low risk from England included participants from the police, probation and prison together (21). The study included 205 participants and showed that 73% had an AUD with 26% as hazardous drinkers and 75% harmful or possibly dependent.
Nine studies were found relating to the police custody suite setting (23–31). Six studies were classified as low risk (23–25, 30, 31), two as medium risk (28, 29) and one as high risk (26). Eight were conducted in England and one in Sweden (25) and included 12,897 participants (range 12–4,739) and the majority of participants were male (Table 1).
Two of the studies gave mean AUDIT scores 14.7 ± 10.19 and 14.66 ± 10.19 (25, 26). The prevalence of AUDIT positives ranged from 26 to 88% with the median being 76%. Four studies reported prevalence of probable dependence (23, 27–29). These ranged from 21 to 38% (Table 1).
One study was found (low risk) in relation to prevalence amongst those at a magistrates' court in Wales (32). Of those screened 95% scored positive for an AUD (8+ on AUDIT) and 39% as being probably dependent (20+ on AUDIT). The eligibility for the study, however, was that the participant had been sentenced for a violent crime committed whilst intoxicated. This would, in part, explain the high prevalence rates (Table 1).
Seven studies were found in the probation setting (11, 33–38). Five were classified as low risk (33–36, 38), one medium risk (37) and one high risk (11). Four were conducted in England) (11, 34–36), two in Scotland (33, 37) and one in Holland (38) and included 1,774 participants (range 32–525) and the majority of participants were male (Table 1). Two studies gave mean AUDIT scores: 11.6 ± 10.7 and 7.2 ± 8.5 (36, 38). Prevalence rates for an AUD ranged from 31 to 86% and probable dependence between 5 and 36%. Two studies gave prevalence rates for women; AUDIT positive 20 and 53%, probable dependence was 25 and 5% (34, 38).
We found 18 studies from 16 articles (4, 34, 39–46, 48–50, 52, 53). Eleven studies were low risk (4, 34, 40, 44–46, 48–52) with the rest classified as medium risk (39, 41, 42, 47).
Of the 15 articles, four were conducted in England (34, 41, 42, 47), two in England and Wales (39, 48), two in Scotland (4, 43), one each in England and Scotland (55), France (40), Ukraine (46), Sweden (44), Brazil (45), Norway (50), Ethiopia (52) and Australia (56). The studies included 6,398 participants (range 47–1,446) (Table 1).
Two of the studies gave mean AUDIT scores 7.25 ± 10.6 and 13.87 ± 12.10 (45, 48). Three studies gave prevalence rates for women (13; 51 and 63%) (34, 39). In the same studies probable dependence for women was shown as 8, 25 and 42%. AUDIT positive rates in all studies ranged from 19–86% and probable dependence from 21 to 48% (Table 1).
Three studies from two papers of low risk were included (53, 54). One article was conducted in England (54) one in the USA (53). The studies included 536 participants (range 125–227).
Thayer et al. (53) conducted a study in juvenile justice diversion in the USA and found that 59% of the population scored 4+ on the AUDIT. Newbury-Birch et al. (35) carried out a study with young people aged 11–17 in Youth Offending Teams (YOTs) and young offenders' institutions (prison) in England. They found that when using adult cut-offs on the AUDIT (8+) 64% scored positive for an AUD. When using the cut off of 2+ on AUDIT recommended by Knight et al. (57) the majority of young people (81%) scored positive for an AUD.
In total, 13 studies were included (Tables 2, 3). Seven studies were from the UK (26, 28–30, 32, 34, 37) and six from the USA (42, 56, 58–61).
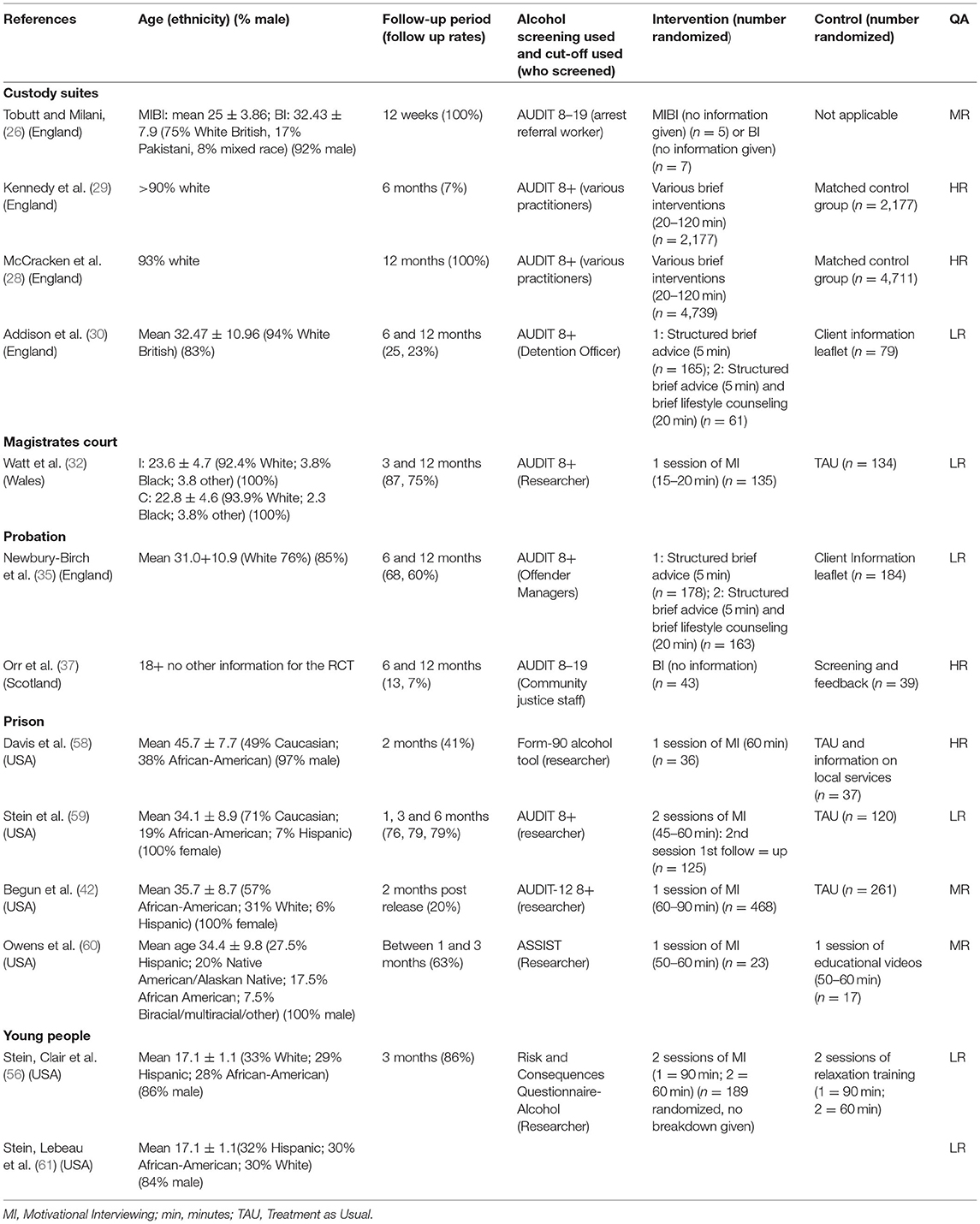
Table 2. Details of included papers.
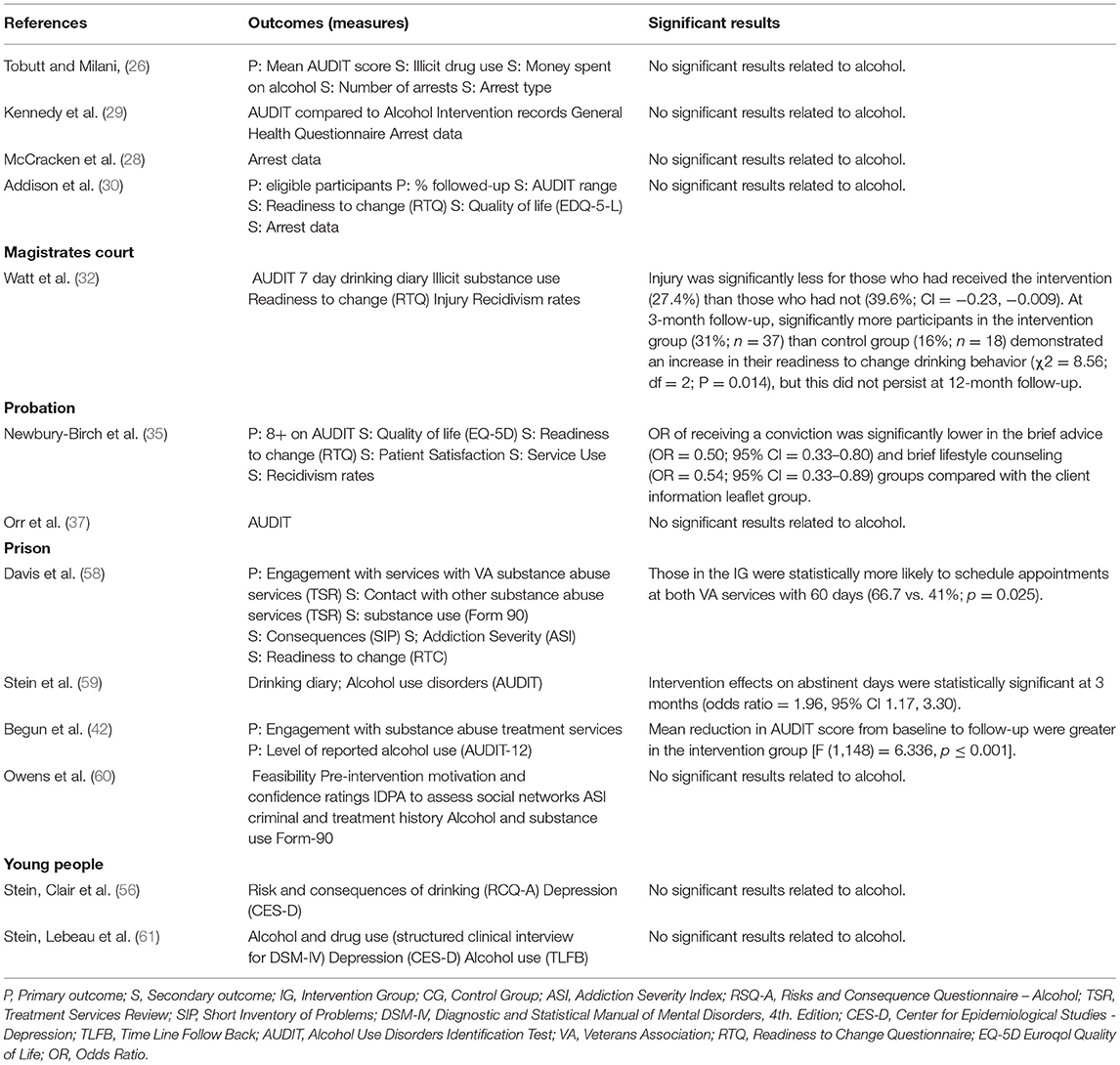
Table 3. Outcome measures and significant results of included studies.
Four studies were found in relation to the custody suite (26, 28–30). Two of the studies were from different phases of the same study (28, 29). All were from England. Three were high risk (26, 28, 29) and one low risk (30) (Tables 2, 3).
A scheme to deliver brief interventions (<30 min) in custody suites after the arrest, or in a non-custody venue, was carried out across 12 police forces in the UK between 2007 and 2010 in two phases (28, 29). Both phases used a matched control group and looked at arrest data differences. Addison et al. (30) carried out a pilot feasibility study of brief interventions in police custody suites and compared two interventions to control condition of feedback and a leaflet with a six and 12 month follow-up period. Tobutt and Milani (26) carried out a small study (n = 12) of motivational interviewing and brief intervention. They did not give information on what the intervention involved. All were followed up at 12 weeks.
No statistically significant differences were found in any of the studies (26, 28–30).
One study (low risk) was found for the magistrates' court setting (32).
Randomized Control Trial (RCT) that compared a control condition of usual care (n = 134) to a single 15–20-min manualised session of brief intervention (n = 135) in a magistrates' court in Wales, UK. The interventions were based on the work of Miller and Rollnick (13).
No significant findings were found in any of the alcohol use measures (AUDIT, total number of standard weekly drinks or number of drinking days) or recidivism. Injury was significantly less for those who had received the intervention (27.4%) than those who had not (39.6%; CI = −0.23, −0.009). At 3-month follow-up, significantly more participants in the intervention group (31%; n = 37) than control group (16%; n = 18) demonstrated an increase in their readiness to change drinking behavior (χ2 = 8.56; df = 2; P = 0.014), but this did not persist at 12-month follow-up.
Two studies were found in the probation setting. Both were from the UK (35, 37). Newbury-Birch et al. (35) had a low risk of bias and Orr et al. (37) a high risk of bias.
A pilot RCT with offenders on probation on community service orders was carried out in Scotland (37). In total, 82 offenders were randomized (no information on randomization group was given for 11 offenders). A pragmatic cluster RCT of the effectiveness of two different brief intervention strategies compared to a control condition of feedback on AUDIT score and an information leaflet at reducing risky drinking in the probation setting in England (35). Probation offender managers were recruited across three areas of England (the North East, South East and London). They were randomized to one of the three conditions—each of which built upon the previous one; feedback on screening outcome and a client information leaflet control group, 5 min of structured brief advice, and 20 min of brief lifestyle counseling.
No effectiveness data was available in the Orr et al. (37) study as they only followed 22% of participants up (37). In the Newbury-Birch study 68 and 60% of participants were followed up at 6 and 12 months respectively (35). No significant differences between groups were found in relation to AUDIT status. Those in the brief advice and brief lifestyle counseling intervention groups were statistically significantly less likely to reoffend (36 and 38%, respectively) than those in the information leaflet group (50%) in the year following intervention (35).
Four studies from the USA were found for the prison system (42, 58–60). One was assessed as low risk (59), two as medium risk (42, 60) and one as high risk (58).
Davis et al. (58) carried out an RCT of veterans in a USA county jail. Participants were recruited in the month prior to leaving jail. Despite various attempts to contact people at the two-month follow-up period, only 41% of participants were followed up. An RCT to evaluate brief intervention for alcohol use and risky sexual behavior among women in a prison in the USA was carried out by Stein et al. (59). Women were eligible for the trial if they had consumed alcohol at a hazardous level (four or more drinks on at least three occasions in the previous 3 months or identified as a hazardous drinker in the past year using the AUDIT) and if they had recently engaged in risky sexual behavior. The first session of motivational interviewing was delivered in prison with the second taking place approximately one to three months after leaving prison. Participants were followed up at 3 and 6 months. Owens and McCrady (60) carried out a pilot RCT with adult males in a large detention center in the USA with individuals who were drinking at a moderate or high level in the 12 months prior to incarceration. The two conditions both had active ingredients. Participants were randomized to either take part in a 50–60 min in-person motivational interview intervention or were asked to watch two educational videos. Participants were followed up at 3 months post intervention.
In the Davis et al. (58) study no differences were found between groups for any alcohol measures. Those in the intervention group were more likely to schedule appointments at a veterans' addiction clinic following their release (67 vs. 41%; p < 0.03) (58). Stein et al. (59) found motivational interview intervention effects on abstinent days was statistically significant at 3 months (OR = 1.96, 95% CI 1.17,3.30). Although, this effect was not maintained at 6-month follow-up. There was no significant difference between participant groups for the number of drinks consumed per drinking day. The study suggests that brief motivational interviewing may be effective at reducing the frequency of alcohol use in the short term but further sessions may be necessary to maintain the effect in the longer term. Begun et al. (42) found a mean reduction in AUDIT score greater in intervention group [F (1,148) = 6.336, p ≤ 0.001. Owens and McCrady (60) did not find any statistical differences and because of a low-response rate (20%) Begun et al. (42) could not test any effectiveness of the intervention.
Two studies with a low risk of bias were found from the USA from the same author (56, 61).
Comparison of two sessions of motivational interviewing compared to relaxation therapy for young people in juvenile correctional facilities (56, 61). The studies were designed to evaluate the effective of depression on reducing alcohol and marijuana use.
Stein, Clair et al. (56) did not find any significant effects between group however Stein, Lebeau et al. (61) found that those in the motivational interview group reported a significantly lower average number of drinks consumed per day, a lower prevalence of heavy drinking days and a lower percentage of days that more than five drinks were drank at three months post-release. Participants were also automatically enrolled into a substance misuse programme which involved 2 h per week of psycho-education for alcohol and drug use for a period of 8 weeks. It is unclear if and how this contributed to the results (61).
In the prevalence section 39 studies (36 papers) were included. The majority of papers were from the UK (4, 11, 21, 23, 24, 26–32, 34–37, 39, 41–43, 47–49, 54), two from Sweden (25, 44) and one each from Australia (51), Brazil (45), Ethiopia (52), France (40), Holland (38), Norway (50), Ukraine (46) and the USA (53).
Using the AUDIT screening tool on the whole samples, between 26 and 88% of individuals in the policy custody setting scored positive for an AUD. In the magistrates court this was 95%; 31–86% in the probation setting and between 19 and 86% in the prison system. In relation to probable dependence, between 21 and 38% of individuals were shown to have probable alcohol dependence in the police custody suite setting; 39 per cent in the magistrate court system; 17–36 % in the probation setting and between 18 and 48% in the prison system. This compares to 6% in the general population (62). Furthermore, for young people, levels of AUD, using the adult cut-off on AUDIT, are high (64%) and levels of probable dependence were also high (30%). We found levels high across the world in the CJS and indicates similarity across different points of the CJS.
In the efficacy section we included 13 studies which was three more than in our 2016 review (10), however this still shows a scarcity of studies in this area. There are a number of reasons why this may be, including “how to measure alcohol consumption when someone has been in prison for a period of time” and the ethical arrangements needed for carrying out research in the CJS (10).
Although the evidence base relating to prevalence rates of AUDS in the CJS globally is increasing, there is still very little evidence of efficacy or effectiveness in the CJS and because there are so few studies it is impossible to assess fully withing different settings in the CJS. Since our last review, we were only able to identify three more published studies, with the majority of studies coming from the USA. This is primarily because of the issues related to when and how you measure alcohol consumption, when someone is incarcerated for a long period of time. Although there are some promising findings within the included studies, we believe more robust evidence is needed in relation to all of the stages in the CJS.
Similarly to healthcare settings, the lack of available evidence in the CJS can be attributed to issues such as workload and the time needed to undertake robust studies (10, 24, 35, 63). More work is also needed around identifying who the best people, in each of the CJS, are to deliver alcohol screening and brief interventions. Another of the main issues experienced when conducting trials in the CJS is being able to successfully follow up participants. This is in large due to the population being “hard to reach” and often falling victim to their chaotic lifestyles (37).
We found, as other studies have (10, 17), that studies examining the effectiveness of risky drinking interventions are still scarce. Another challenge associated with conducting research in the CJS is the necessity of using self-report follow-up data (10, 17, 64). Another fundamental issue is that studies include different measurement tools and outcomes, with outcomes decided upon based on the research funding. We have recently published a Core Outcome Set for Alcohol Brief Interventions to improve the measurement of alcohol-related change (65–67) which will help researchers use the same measurements in studies of brief interventions in the future. Another concern is the differences found in different studies on the active ingredients of different control groups which is an issue that effects both health and criminal justice research (35, 68, 69).
As research moves forward, it could be argued that the stages in the CJS described above are analogous to the health care system. Police stations are busy and chaotic, much like accident and emergency departments. Probation is similar to primary care, appointments made and an emphasis on dealing with the underlying issues, whereas prison is similar to hospital wards in as much as often the person is there for a period of time (10, 17). This information and analogy can help us identify key strengths and weaknesses that can be learned in these settings.
This present study shows that levels of AUDs and probable dependence are high across all stages of the CJS. We need more robust research studies across all stages of the CJS in order to ascertain efficacy of alcohol screening and brief interventions.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
DN-B wrote the first draft of the article. All authors contributed to the final article, design, and the carrying out of the systematic review. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. (2009) 373:2233–33. doi: 10.1016/S0140-6736(09)60746-7
2. Boden J, Fergusson D, Horwood L. Alcohol misuse and violent behavior: Findings from a 30-year longitudinal study. Drug Alcohol Depend. (2012) 122:135–41. doi: 10.1016/j.drugalcdep.2011.09.023
3. Richardson A, Budd T. Alcohol, Crime and Disorder: a Study of Young Adults. London: Home Office Research, Development and Statistics Directorate. Report No.: Home Office Research Study (2003). p. 263.
4. Graham L, Heller-Murphy S, Aitken L. A M. Alcohol problems in a remand Scottish prisoner population. Int J Prison Health. (2012) 8:51–9. doi: 10.1108/17449201211277174
5. Commission on Alcohol Harm. “It's everywhere” - Alcohol's Public Face and Private Hard. (2020). Available online at: https://lordslibrary.parliament.uk/commission-on-alcohol-harm-its-everywhere-alcohols-public-face-and-private-harm/#:~:text=The%20commission%20published%20its%20findingsthough%20often%20hidden%20from%20view%E2%80%9D
7. Raistrick D, Heather N, Godfrey C. Review of the Effectiveness Of Treatment For Alcohol Problems. National Treatment Agency for Substance Misuse, London (2006).
8. Saunders J, Lee N. Hazardous alcohol use: its delineation as a subthreshold disorder, and approaches to its diagnosis and management. Compr Psychiatry. (2000) 41:95–103. doi: 10.1016/S0010-440X(00)80015-2
9. World Health Organisation. The Role of General Practice Settings in the Prevention and Management of the Harm Done by Alcohol. Copenhagen: World Health Organisation Regional Office for Europe (1992).
10. Newbury-Birch D, McGovern R, Birch J, O'Neill G, Kaner H, Sondhi A, et al. A rapid systematic review of what we know about alcohol use disorders and brief interventions in the criminal justice system. Int J Prison Health. (2016) 12:57–70. doi: 10.1108/IJPH-08-2015-0024
11. Fitton L, Bates A, Hayes A, Fazel S. Psychiatric disorders, substance use, and executive functioning in older probationers. Crim Behav Ment Health. (2018) 28:447–59. doi: 10.1002/cbm.2094
12. Kaner EFS, Beyer FR, Muirhead C, Campbell F, Pienaar ED, Bertholet N, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. 2018(2). doi: 10.1002/14651858.CD004148.pub4
13. Miller W, Rollnick S. Motivational Interviewing; Preparing People to Change Addictive Behavior. New York, NY: Guildford Press (1991).
14. Haighton CA, Newbury-Birch D, Kaner EFS. Haighton CA, Newbury-Birch D, Kaner EFS. Screening and interventions in medical setting including brief feedback-focused interventions. In Miller PM, ed. Interventions for Addiction - Comprehensive Addictive Behaviors and Disorders. V3. Academic Press: London. doi: 10.1016/B978-0-12-398338-1.00030-0
15. Babor TF, Grant M. From clinical research to secondary prevention: international collaboration in the development of the alcohol use disorders identification test (AUDIT). Alcohol Health Res World. (1989) 13:371–4.
16. Haighton C, Newbury-Birch D, Durlik C, Sallis A, Chadbourn T, Porter L, et al. Optimising Making Every Contact Count (MECC) interventions: a strategic behavioural analysis. Health Psychol. (2021) 40:960–73. doi: 10.1037/hea0001100
17. Newbury-Birch D, Ferguson J, Landale S, Giles EL, McGeechan GJ, Gill C, et al. A systematic review of the efficacy of alcohol interventions for incarcerated people. Alcohol Alcohol. (2018) 53:412–25. doi: 10.1093/alcalc/agy032
18. Rethlefsen M, Kirtley S, Waffenschmidt S, Ayala A, Moher D, Page M, et al. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst Rev. (2021) 10:39. doi: 10.1186/s13643-020-01542-z
19. Hodgson R, Alwyn T, John B, Thom B, Smith A. The FAST alcohol screening test. Alcohol Alcohol. (2002) 37:61–6. doi: 10.1093/alcalc/37.1.61
20. Saunders JB, Aasland OG, Babor TF, De La Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. Addiction. (1993) 88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x
21. Coulton S, Newbury-Birch D, Cassidy P, Dale V, Deluca P, Gilvarry E, et al. Screening for alcohol use in criminal justice settings: an exploratory study. Alcohol Alcohol. (2012) 47:423–7. doi: 10.1093/alcalc/ags048
23. Hopkins M, Sparrow P. Sobering up: Arrest referral and brief intervention for alcohol users in the custody suite. Criminol Crim Justice. (2006) 6:389–410. doi: 10.1177/1748895806068576
24. Brown N, Newbury-Birch D, McGovern R, Phinn E, Kaner E. Alcohol screening and brief intervention in a policing context: a mixed methods feasibility study. Drug Alcohol Rev. (2010) 29:647–54. doi: 10.1111/j.1465-3362.2010.00223.x
25. Durbeej N, Berman AH, Gumpert CH, Palmstierna T, Kristiansson M, Alm C. Validation of the alcohol use disorders identification test and the drug use disorders identification test in a swedish sample of suspected offenders with signs of mental health problems: results from the mental disorder, substance abuse and crime study. J Subst Abuse Treat. (2010) 39:364–77. doi: 10.1016/j.jsat.2010.07.007
26. Tobutt C, Milani R. Comparing two counselling styles for hazardous drinkers charged with alcohol-related offences in a police custody suite: piloting motivational interviewing brief intervention or a standard brief intervention to reduce alcohol consumption. Adv Dual Diagn. (2010) 3:20–33. doi: 10.5042/add.2011.0189
27. Barton A. Screening and brief intervention of detainees for alcohol use: a social crime prevention approach to combating alcohol-related crime? Howard J. (2011) 50:62–74. doi: 10.1111/j.1468-2311.2010.00647.x
28. McCracken K, McMurran M, Winlow S, Sassi F, McCarthy K. Evaluation of Alcohol Arrest Referral Pilot Schemes (Phase 2). London: Home Office (2012).
29. Kennedy A, Dunbar I, Boath M, Beynon C, Duffy P, Stafford J, et al. Evaluation of Alcohol Arrest Referral Pilot Schemes (Phase 1). London: Home Office (2012).
30. Addison M, McGovern R, Angus C, Becker F, Brennan A, Brown H, et al. Alcohol screening and brief intervention in police custody suites: pilot cluster randomised controlled trial (AcCePT). Alcohol Alcohol. (2018) 53:548–59. doi: 10.1093/alcalc/agy039
31. Samele C, McKinnon I, Brown P, Srivastava S, Arnold A, Hallett N, et al. The prevalence of mental illness and unmet needs of police custody detainees. Crim Behav Ment Health. (2021) 31:80–95. doi: 10.1002/cbm.2193
32. Watt K, Shepherd J, Newcombe R. Drunk and dangerous: A randomised controlled trial of alcohol brief intervention for violent offenders. J Exp Criminol. (2008) 4:1–19. doi: 10.1007/s11292-007-9048-7
33. MacAskill S, Parkes T, Brooks O, Graham L, McAuley A, Brown A. Assessment of alcohol problems using AUDIT in a prison setting: more than an 'aye or no' question. BMC Public Health. (2011) 11:865. doi: 10.1186/1471-2458-11-865
34. Newbury-Birch D, Harrison B, Brown N, Kaner E. Sloshed and sentenced: a prevalence study of alcohol use disorders among offenders in the North East of England. Int J Prison Health. (2009) 5:201–11. doi: 10.1080/17449200903343183
35. Newbury-Birch D, Coulton S, Bland M, Cassidy P, Dale V, Deluca P, et al. Alcohol screening and brief interventions for offenders in the probation setting (SIPS Trial): a pragmatic multicentre cluster randomised controlled trial. Alcohol Alcohol. (2014) 49:540–8. doi: 10.1093/alcalc/agu046
36. Pluck G, Brooker C, Blizard R, Moran P. Personality disorder in a probation cohort: Demographic, substance misuse and forensic characteristics. Crim Behav Ment Health. (2015) 25:403–15. doi: 10.1002/cbm.1938
37. Orr K, McCoard S, Canning S, McCartney P, Williams J. Delivery Alcohol Brief Interventions in the Community Justice Setting: Evaluation of a Pilot Project. Edinburgh: NHS Health Scotland (2011).
38. Hildebrand M, Noteborn MGC. Exploration of the (Interrater) reliability and latent factor structure of the Alcohol Use Disorders Identification Test (AUDIT) and the Drug Use Disorders Identification Test (DUDIT) in a sample of dutch probationers. Subst Use Misuse. (2015) 50:1294–306. doi: 10.3109/10826084.2014.998238
39. Lader D, Singleton N, Meltzer H. Psychiatric Morbidity among Young Offenders in England and Wales. London: Office for National Statistics (2000).
40. Maggia B, Martin S, Crouzet C, Richard P, Wagner P, Balmès J-L, et al. Variation in AUDIT (Alcohol Use [correction of Used] Disorder Identification Test) scores within the first weeks of imprisonment. Alcohol Alcohol. (2004) 39:247–50. doi: 10.1093/alcalc/agh044
41. McMurran M, Cusens B. Alcohol and violent and non-violent acquisitive offending. Addict Res Theory. (2005) 13:439–43. doi: 10.1080/16066350500096058
42. Begun A, Rose L, LeBel T. Intervening with women in jail around alcohol and substance abuse during preparation for community reentry. Alcohol Treat Q. (2011) 29:453–78. doi: 10.1080/07347324.2011.608333
43. Parkes T, MacAskill S, Brooks O, Jepson R, Atherton I, Doi L, et al. Prison health needs assessment for alcohol problems. Edinburgh: NHS Health Scotland (2011).
44. Konstenius M, Larsson H, Lundholm L, Philips B, van de Glind G, Jayaram-Lindström N, et al. An epidemiological study of ADHD, substance use, and comorbid problems in incarcerated women in Sweden. J Atten Disord. (2012) 19:44–52. doi: 10.1177/1087054712451126
45. Nunes AdM, Baltieri DA. Substance misuse subtypes among women convicted of homicide. Subst Abus. (2013) 34:169–78. doi: 10.1080/08897077.2012.730121
46. Azbel L, Wickersham J, Grishaev Y, Dvoryak S, Altice F. Burden of infectious diseases, substance use disorders, and mental illness among Ukrainian prisoners transitioning to the community. PLoS ONE. (2013) 8:e59643. doi: 10.1371/journal.pone.0059643
47. Kissell A, Taylor P, Walker J, Lewis E, Hammond A, Amos T. Disentangling alcohol-related needs among pre-trial prisoners: a longitudinal study. Alcohol Alcohol. (2014) 49:639–44. doi: 10.1093/alcalc/agu056
48. Wainwright V, Lennox C, McDonnell S, Shaw J, Senior J. The mental health and substance misuse needs of male ex-armed forces personnel in prison. J Forens Psychiatry Psychol. (2018) 29:146–62. doi: 10.1080/14789949.2017.1352012
49. Holloway A, Ferguson J, Parker R, Sheikh A, Guthrie V, Newbury-Birch D. Alcohol brief interventions for male remand prisoners: a mixed-methods feasibility and acceptability study. Lancet. (2019) 394:S53. doi: 10.1016/S0140-6736(19)32850-8
50. Pape H, Rossow I, Bukten A. Alcohol problems among prisoners: subgroup variations, concurrent drug problems, and treatment needs. Eur Addict Res. (2021) 27:179–88. doi: 10.1159/000511253
51. Kerslake M, Simpson M, Richmond R, Albany H, Butler T. Risky alcohol consumption prior to incarceration: A cross-sectional study of drinking patterns among Australian prison entrants. Drug Alcohol Rev. (2020) 39:694–703. doi: 10.1111/dar.13127
52. Haile YG, Kebede KB, Limenhe A, Habatmu K, Alem A. Alcohol use disorder among prisoners in Debre Berhan prison. Ethiopia: a cross-sectional study. Subst Abuse Treat Prev Policy. (2020) 15:26. doi: 10.1186/s13011-020-00270-w
53. Thayer RE, Callahan TJ, Weiland BJ, Hutchison KE, Bryan AD. Associations between fractional anisotropy and problematic alcohol use in juvenile justice-involved adolescents. Am J Drug Alcohol Abuse. (2013) 39:365–71. doi: 10.3109/00952990.2013.834909
54. Newbury-Birch D, Jackson K, Hodgson T, Gilvarry E, Cassidy P, Coulton S, et al. Alcohol-related risk and harm amongst young offenders aged 11-17. Int J Prison Health. (2015) 11:75–86. doi: 10.1108/IJPH-08-2013-0041
55. O'Donnell A, Kaner E, Newbury-Birch D, Schulte B, Schmidt C, Reimer J, et al. The impact of brief interventions in primary healthcare: A systematic review of reviews. Alcohol and Alcoholism. (2014) 49:66–78. doi: 10.1093/alcalc/agt170
56. Stein LAR, Clair M, Lebeau R, Colby SM, Barnett NP, Golembeske C, et al. Motivational interviewing to reduce substance-related consequences: Effects for incarcerated adolescents with depressed mood. Drug Alcohol Depend. (2011) 118:475–8. doi: 10.1016/j.drugalcdep.2011.03.023
57. Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcoholism. (2003) 27:67–73. doi: 10.1111/j.1530-0277.2003.tb02723.x
58. Davis T, Baer J, Saxon A, Kivlahan D. Brief motivational feedback improves post-incarceration treatment contact among veterans with substance use disorders. Drug Alcohol Depend. (2003) 69:197–203. doi: 10.1016/S0376-8716(02)00317-4
59. Stein M, Caviness C, Anderson B, Hebert M, Clarke J. A brief alcohol intervention for hazardously drinking incarcerated women. Addiction. (2010) 105:466–75. doi: 10.1111/j.1360-0443.2009.02813.x
60. Owens M, McCrady B. A pilot study of a brief motivational intervention for incarcarated drinkers. J Subst Abuse Treat. (2016) 68:1–10. doi: 10.1016/j.jsat.2016.05.005
61. Stein LAR, Lebeau R, Colby SM, Barnett NP, Golembeske C, Monti PM. Motivational interviewing for incarcerated adolescents: effects of depressive symptoms on reducing alcohol and marijuana use after release. J Stud Alcohol Drugs. (2011) 72:497–506. doi: 10.15288/jsad.2011.72.497
62. NHS Information Centre. Statistics on Alcohol: England, 2008. London: NHS Information Centre for health and social care (2009).
63. Anderson P, Bendtsen P, Spak F, Reynolds J, Drummond C, Colom J, et al. Improving the delivery of brief interventions for heavy drinking in primary health care: outcome results of the Optimzing Delivery of Health Care Intervention (OHDIN) five-country cluster randomized factorial trial. Addiction. (2016) 111:1935–45. doi: 10.1111/add.13476
64. Shorter G, Bray J, Heather N, Berman A, Giles E, Clarke M, et al. The “Outcome Reporting in Brief Intervention Trials: Alcohol” (ORBITAL) core outcome set: international consensus on outcomes to measure in efficacy and effectiveness trials of alcohol brief interventions. J Stud Alcohol Drugs. (2021) 82:638–46. doi: 10.15288/jsad.2021.82.638
65. Shorter G, Heather N, Bray J, Giles E, Holloway A, Barbosa C, et al. The ‘Outcome Reporting in Brief Intervention Trials: Alcohol' (ORBITAL) framework: protocol to determine a core outcome set for efficacy and effectiveness trials of alcohol screening and brief intervention. Trials. (2018) 18:611. doi: 10.1186/s13063-017-2335-3
66. Shorter GW, Bray JW, Giles EL, O'donnell AJ, Berman AH, Holloway A, et al. The variability of outcomes used in efficacy and effectiveness trials of alcohol brief interventions: a systematic review. J Stud Alcohol Drugs. (2019) 80:286–98. doi: 10.15288/jsad.2019.80.286
67. Shorter GW, Heather N, Bray JW, Berman AH, Giles EL, O'Donnell AJ, et al. Prioritization of outcomes in efficacy and effectiveness of alcohol brief intervention trials: International multi-stakeholder e-delphi consensus study to inform a core outcome set. J Stud Alcohol Drugs. (2019) 80:299–309. doi: 10.15288/jsad.2019.80.299
68. Kaner E, Bland M, Cassidy P, Coulton S, Dale V, Deluca P, et al. Effectiveness of screening and brief alcohol intervention in primary care (SIPS trial): pragmatic cluster randomised controlled trial. BMJ. (2013) 346:e8501. doi: 10.1136/bmj.e8501
Keywords: criminal justice, offending, alcohol, brief intervention, systematic review
Citation: Newbury-Birch D, Ferguson J, Connor N, Divers A and Waller G (2022) A Rapid Systematic Review of Worldwide Alcohol Use Disorders and Brief Alcohol Interventions in the Criminal Justice System. Front. Psychiatry 13:900186. doi: 10.3389/fpsyt.2022.900186
Received: 20 March 2022; Accepted: 31 May 2022;
Published: 07 July 2022.
Edited by:
Marc N. Potenza, Yale University, United StatesReviewed by:
Gallus Bischof, University of Lübeck, GermanyCopyright © 2022 Newbury-Birch, Ferguson, Connor, Divers and Waller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dorothy Newbury-Birch, ZC5uZXdidXJ5LWJpcmNoQHRlZXMuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.