
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 27 June 2022
Sec. Psychopathology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.898017
 Beatriz Cerda-De la O1†
Beatriz Cerda-De la O1† Ana Lilia Cerda-Molina2*
Ana Lilia Cerda-Molina2* Lilian Mayagoitia-Novales2†
Lilian Mayagoitia-Novales2† Margarita de la Cruz-López1Marcela Biagini-Alarcón1Erika Lucia Hernández-Zúñiga1
Margarita de la Cruz-López1Marcela Biagini-Alarcón1Erika Lucia Hernández-Zúñiga1 Javier I. Borráz-León2Jesús Alfredo Whaley-Sánchez1
Javier I. Borráz-León2Jesús Alfredo Whaley-Sánchez1Background: Intimate partner violence (IPV) is one of the most prevalent forms of violence against women globally and it is considered a public health problem. Because the experience of IPV is stressful and traumatic for victims, they are at high risk of developing alteration of the Hypothalamus–Pituitary–Adrenal (HPA) axis functioning as well as anxiety and depression symptoms. The aim of this study was to compare the quality of life and changes in cortisol response to an acute stressor between women exposed to IPV and non-exposed women. Differences according to symptoms of anxiety and depression including the risk of suicide thoughts, were also analyzed.
Method: Our sample size consisted of 130 women (ages 18–68) grouped as follows: 71 women experiencing IPV and 59 women without history of IPV as control group. All participants completed a battery of questionnaires including IPV exposure, anxiety, and depression symptoms (Beck Inventories), as well as quality of life (WHOQOL-BREF). Salivary cortisol levels in response to a cognitive test with verbal, mathematical, and abstract reasoning were measured at four time points.
Results: Women exposed to IPV, with severe anxiety and depression symptoms as well as suicide thoughts, exhibited heightened cortisol response after the cognitive test and reported lower quality of life compared to (i) women experiencing IPV with moderate symptoms of anxiety and depression, who showed a blunted response, and (ii) women without history of IPV with minimal to moderate symptoms, who showed a decreased cortisol profile. Social relationships dimension was in particular the most affected aspect of quality of life.
Conclusions: Our findings highlight the role of cortisol responses as a complementary biological marker to be associated with severe psychiatric disturbances in women exposed to IPV.
Intimate partner violence (IPV) is one of the most prevalent forms of violence against women worldwide, since around one third (27%) of women aged 15–49 years has been exposed to any kind of violence at least once in their life (1). IPV is defined by the World Health Organization (WHO) (2) as “any behavior within an intimate relationship that causes physical, sexual, or psychological harm.” It includes acts of physical aggression (slapping, hitting, kicking and beating), sexual coercion (forced intercourse), emotional or psychological abuse (insults, constant humiliation, intimidation, threats of harm, or to take away children), and/or controlling behaviors (isolation from family and friends, monitoring their movements, restricting access to financial resources, employment, education or medical care) (1), which are commonly perpetrated by current or former romantic partners, even without cohabitation (3). IPV constitutes a multifactorial global public health problem affecting the quality of life of victims and their families, regardless of the country, socioeconomic status, ethnicity, or religion (4, 5). In the United States, the lifetime prevalence of IPV experienced by women is 37.3% (6) whereas the percentage is almost double in Mexico. The latest national survey in Mexico reported that 66.1% (30.7 million out of 46.5 million women) have faced violence of any kind and from any aggressor at some time in their life, whereas 43.9% have faced aggression from their current or former husband or romantic partner throughout their relationship (7). IPV affects the sense of wellbeing and causes adverse physical and mental health outcomes for victims and their families, even after the violence has ended (8, 9). For example, extensive literature has showed that being a victim of IPV is a strong risk factor for developing stress-related diseases and disorders such as gastrointestinal complains, major depressive disorder (MDD), anxiety, post-traumatic stress disorder (PTSD), substance abuse problems, and higher recurrence of suicide thoughts than women who do not suffer violence (3, 10–14). Thus, it is not surprising that the health consequences associated with IPV are among of the most common reasons for requesting medical services (8).
Stressful and traumatic life events, such as IPV are associated with alterations in the regulation of the hypothalamic-pituitary-adrenal (HPA) axis, and consequently in cortisol secretion, the end product of the HPA axis (15). For example, previous studies have evidenced either abnormally high cortisol secretion (hyper-reactivity) or reduced secretion (hypo-reactivity) in response to long-term stressors. Hyperactivation of the HPA axis has been associated with MDD (16–19) and is mainly due to an impaired negative brain feedback mechanism necessary for the recovery of basal cortisol levels after the exposure to a stressor. This altered mechanism of cortisol regulation could lead to deleterious effects on mood and cognitive performance (20). In contrast, other mental health disorders, such as PTSD, are associated with decreased responsiveness to stress and consequently with hypo-secretion of cortisol (21). Besides its function in stress regulation, cortisol has an important metabolic role necessary for the maintenance of body homeostasis (15), due to the well-characterized diurnal rhythm secretion with a normal peak around 30 min after awakening (22). Previous research on victims of IPV has focused on studying cortisol awakening response and diurnal changes, with mixed results depending on the associated mental health disorder. For instance, some studies have found lower levels of morning cortisol in women victims of IPV with psychiatric disorders such as PTSD (23), dissociative symptoms (24), or MDD (25) [but see (26) for opposite results]. Other studies have found higher levels of evening cortisol in women victims of IPV with abuse antecedents, relative to non-abused women (27), and in women with PTSD than in women without this disorder (28). Similarly, Johnson et al. (29) observed that women with PTSD had higher awakening cortisol response than women without PTSD, whereas reported chronic abuse was associated with lower levels of this hormone. To date, the only study investigating cortisol responses to a psychosocial stressor in women exposed to interpersonal violence/trauma, found higher cortisol response to the first of four tests that make up the Trier Social Stress Tests (TSST) among trauma exposed women with current PTSD than among women without PTSD (with no cortisol response) and non-traumatized controls, who showed a blunted response (30). Therefore, to contribute with the understanding of the consequences of altered HPA axis responses in women victims of IPV, we aimed to assess quality of life as well as cortisol levels in response to a cognitive test in a group of female psychiatric patients exposed to IPV with anxiety and depression symptoms, and to compare them with a group of women without history of IPV. In addition, we sought to evaluate potential differences in the results according to recurrency of suicidal thoughts. According to the literature, we expected that women experiencing IPV have a higher cortisol response, worse quality of life, and more severe symptoms of anxiety and depression than women without IPV. We also expected a much higher cortisol response in those patients with suicide thoughts.
This was a cross-sectional study that included a total of 130 adult women with an age range of 18–68 years (Table 1) as follows: 74 female psychiatric patients, diagnosed with anxiety and depression, who met the inclusion criteria of being currently receptors of IPV, were recruited during the first admission at the Gender and Sexuality Clinic of the Instituto Nacional de Psiquiatría “Ramón de la Fuente Muñiz,” in Mexico City, Mexico. Three women were excluded from the sample because they did not complete the entire psychological instruments; thus, the final sample in this group was 71 women (hereinafter IPV women). As controls, female students, and administrative employees (non-involved in the clinical research and who have no contact with psychiatric patients) of the same Institute were invited to participate. A total of 59 women who met the inclusion criteria of not being exposed to IPV were included in the control group. Demographic characteristics of both groups (age, education, occupation, and marital status) can be found in Table 1. Exclusion criteria in both groups were comorbidity with psychotic disorders, intellectual disability, substance use, serious physical illness, and those conditions affecting cortisol levels such as pregnancy, using birth control pills, and current treatment with anti-inflammatories. Diagnoses were made by the Psychiatrists and Psychologists in charge of the Gender and Sexuality Clinic according to the Diagnostic and Statistical Manual Version 5 (DSM-5) (31). Before signing the informed consent letter, all participants received detailed information about the protocol and purposes of the study and were told that they had the right to finish the procedure at any time without any negative consequence for them. This study took place from 2018 to the beginning of 2020, prior to the COVID-19 pandemic which discards the effects of the pandemic on our results.
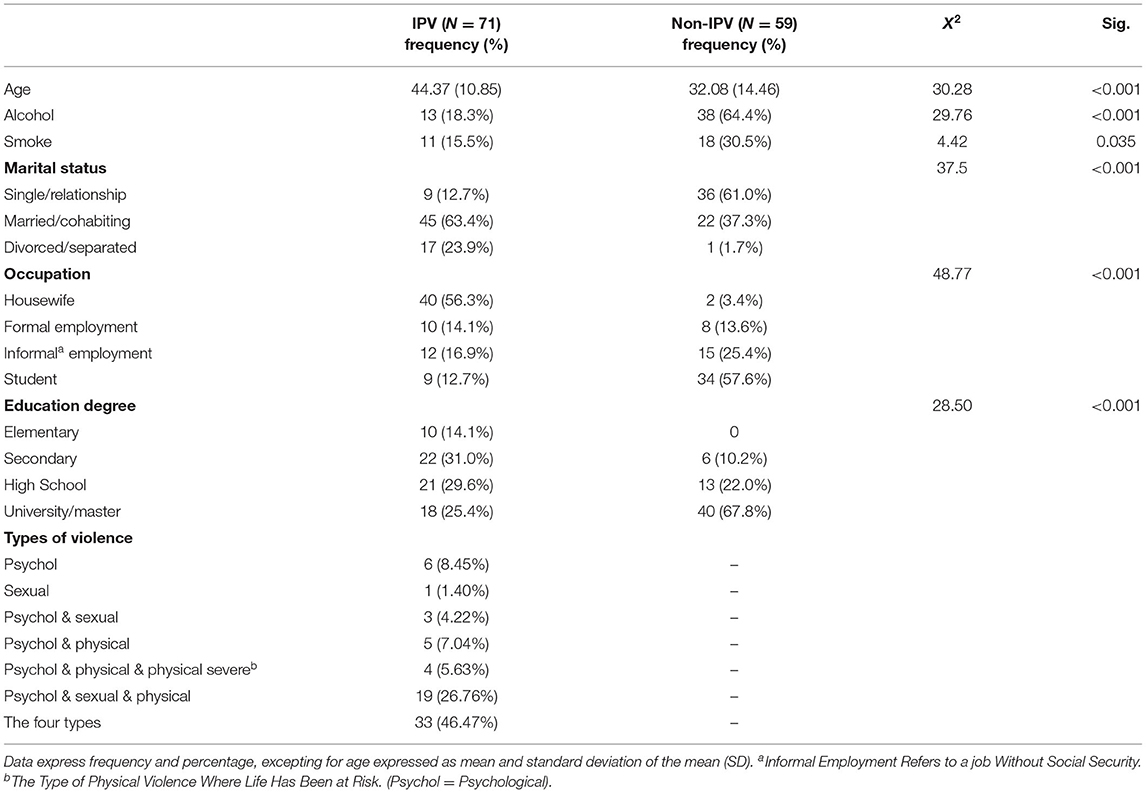
Table 1. Demographic data and descriptive statists of the participants (IPV vs. control non-IPV).
This study was approved by the Research and Ethic Committees (Project Number: SC19114.0) and conducted in compliance with the declaration of Helsinki and the National Official Norms for Research with Human Beings (NOM-012-SSA3-2012). As compensation, patients were offered to receive free psychotherapeutic interventions; control women were offered to receive their psychological and endocrine profiles and were also offered to receive free psychological assistance if needed.
Exposition to intimate partner violence was assessed using the Mexican Scale of Violence by the Male Partner Against Women (32). This is a 27-item scale (Cronbach's α = 0.99) to measure the types of violence currently experienced and their severity within the last 12 months (psychological, sexual, physical, and severe physical violence –where life has been at risk–). The severity index is calculated by summing the scores of the frequency of each event (i.e., never = 0, sometimes = 4–9, many times = 8–14, several times = 12–27). According to the weight assigned to each item, the index is classified as: no violence, moderated violence, and severe violence (Cronbach's α for the present sample = 0.89). Table 1 indicates the frequency and percentages of the types of violence reported by IPV women. Only 7 out of 71 reported one type of violence, the other patients reported two, three, and even the four types of violence.
We used the self-reporting Spanish version of the Beck Depression Inventory (BDI) (33) and Beck Anxiety Inventory (BAI) (34). The total score of both inventories ranges from 0 to 63. The validated version of BDI (Cronbach's α = 0.87) establishes 0–9 points as minimal o absent depression, 10–16 mild, 17–29 moderate, and >29 severe. Cronbach's α in the present study was 0.88. The validated version of BAI (Cronbach's α = 0.83) considers 0–5 points as minimal o absent anxiety, 6–15 mild, 16–30 moderate, and >30 severe. Cronbach's α in the present study was 0.93.
Most of the IPV patients (95.77%, N = 68) had symptoms of both anxiety and depression, and 29 patients (40.8%) answered the item 9 of the BDI scale about suicidal thoughts (see Table 2). These 29 women were at the highest limit of moderate depression (mean score 28.76 ± 9.48) but had a mean score of severe anxiety (32.03 ± 11.12). Patients without suicide thoughts had moderate symptoms (depression: 18.67 ± 6.94; anxiety: 23.60 ± 13.17). Most of the women without IPV (94.9% N = 56) had minimal/absent to moderate symptoms of both anxiety and depression (Table 2).
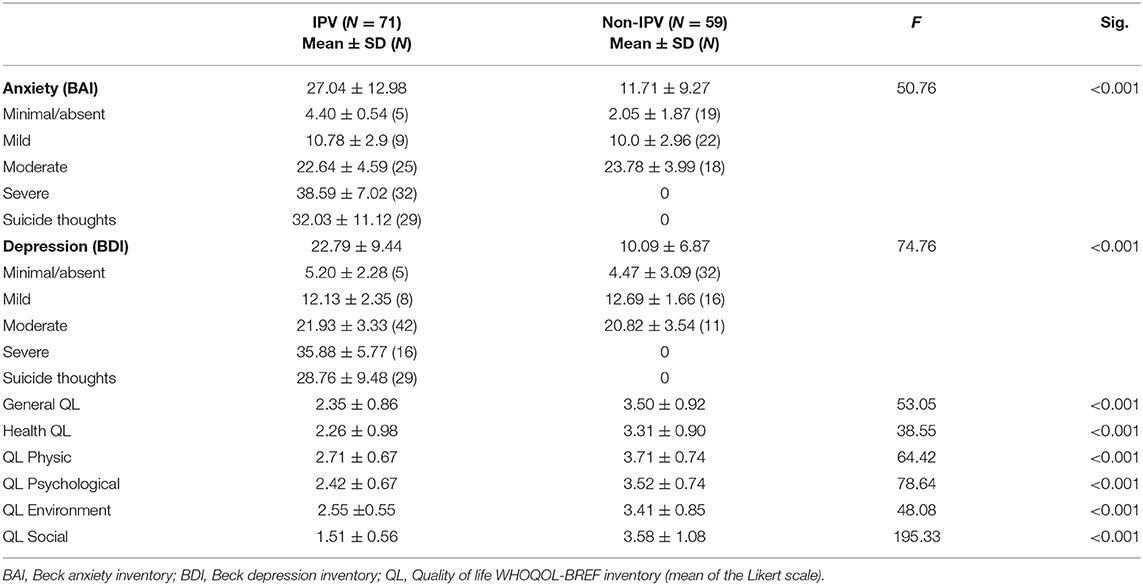
Table 2. Descriptive statistics for anxiety, depression, and quality of life applied to the participants (IPV vs. control non-IPV).
Quality of life was evaluated using the 26-item Quality of Life questionnaire (WHOQOL-BREF) (35, 36). This scale measures four health dimensions: Physical (e.g., activities of daily living, energy, and fatigue); Psychological (e.g., bodily image and appearance, positive and negative feelings); Social relations (personal relationships, social support, and sexual activity); Environment (e.g., financial resources, home environment, transport), and two general questions: (1) How do you rate your quality of life in general? (2) How satisfied are you with your health? Each item was rated on a 5-point Likert-type scale (1 = very bad/completely unsatisfied; 3 = neither unsatisfied/neither satisfied; 5 = very good/completely satisfied). This scale has an internal consistency range of 0.68–0.81 being the lowest for social relations (35). In the present sample, the internal consistencies were: total scale α = 0.88; physical health α = 0.72; psychological health α = 0.73; environment α = 0.70; social relations α = 0.60.
Saliva samples were subjected to two subsequent freeze-thaw cycles to free them from mucopolysaccharides and proteins (37). After each thawing, samples were centrifuged at 1,500 g during 30 min at 4°C; the supernatants were collected and frozen again. We measured cortisol in duplicates using commercially available kits (ENZO Life Sciences) through the ELISA technique by following the manufacturer's instructions. Cortisol concentrations were reported in pg/ml. Inter-assay and intra-assay coefficients were 9.8 and 7.1%, respectively.
Participants were previously instructed to brush their teeth before coming to the test and not to eat, smoke, drink tea, coffee, or any sweet or colored beverage (only water), for at least 2 h before the test. First, participants completed the general information questionnaire; after that they collected a first saliva sample (2-3 ml) by passive drool into a new polypropylene tube (basal sample). After the first saliva sample was collected, participants were exposed to an acute stressor as follows: they were instructed to complete a brief IQ test comprising questions about verbal, mathematical, and abstract reasoning. Participants were told that they had exactly 10 min to complete the test and that two psychiatrists would be taking care not to cheat on the test. 15, 30, and 45 min after the test, the second, third, and fourth saliva samples were collected, and volunteers completed the inventories described above. All the procedure took about 60–70 min and was performed in groups of 10–12 participants per session. Saliva samples were labeled with a code to ensure the confidentiality of the volunteer and immediately frozen and stored at −20°C until assayed.
Differences between groups (i.e., IPV women vs. non-IPV women) in demographic data, psychiatric scales and quality of life were analyzed with X2 and one-way ANOVA. To analyze the cortisol response, we used a Generalized Equation Model (GEE) suitable for data dependency, i.e., repeated samples design (38). Cortisol levels (log transformed to normalize the distribution) were introduced as dependent variable; as independent factors we included group (IPV vs. non-IPV) and time of saliva sample (basal, 15, 30, and 45 min post-test), whereas age (in years) was included as covariate. Because anxiety and depression scores were highly correlated (Pearson r = 0.798, N = 130, p < 0.001) and most of the participants had both symptoms, we summed anxiety and depression scores of each participant, to create only one continue variable reflecting the severity of the symptoms; this variable was also included as covariate in the model. We analyzed the main effects and interactions. To compare the quality of life between IPV women with and without suicide thoughts, we used a Multivariate GLM (MGLM) analysis suitable for multiple dependent variables. The data were analyzed using SPSS version 22 (SPSS Inc., Chicago, IL, USA). We used Bonferroni as post-hoc test and significance was set at p ≤ 0.05. Results are expressed as the mean ± SD, and all the graphics express mean and 95% CI.
Statistically significant differences between women with and without IPV were found (Table 1). In general, IPV patients were older (M = 44.37 vs. 32.08 years), consumed less alcohol and tobacco than control women. Most of the IPV patients were married/cohabiting, housewives, and had middle school education. Table 2 shows that IPV patients had significantly more symptoms of anxiety and depression, ranging from moderate to severe levels, whereas most women without IPV ranged from minimal to moderate levels (none of the control women had severe symptoms or suicide thoughts). Regarding quality of life, women with IPV reported a poorer quality of life in all the domains than control women; this was especially pronounced for the “social relations” domain, reporting a mean score of 1.5, corresponding to a completely unsatisfied level (Table 2).
The GEE Model showed a significant effect of time (X2 Wald = 14.71, d.f. = 3, 129, p = 0.002), whereas the group alone did not (X2 Wald = 0.005, d.f, = 1, 129, p = 0.92); however, the interaction time × group was statistically significant (X2 Wald = 11.23, d.f. = 3, 129, p = 0.01), indicating differences in cortisol response between IPV and non-IPV women. No significant effects of age (X2 Wald = 0.18, d.f. = 1, 129, p = 0.67) or symptomatology of anxiety and depression (X2 Wald = 2.31, d.f. = 1, 129, p = 0.12) on cortisol response were found. Control non-IPV women displayed a pattern of cortisol hyporeactivity whereas IPV women showed a slight non-significant increase in cortisol levels. Figure 1 indicates a statistically significant decrease in cortisol levels 45 min after the cognitive test compared to basal cortisol level in control non-IPV women (p = 0.01). No significant changes in cortisol levels were found for IPV women.
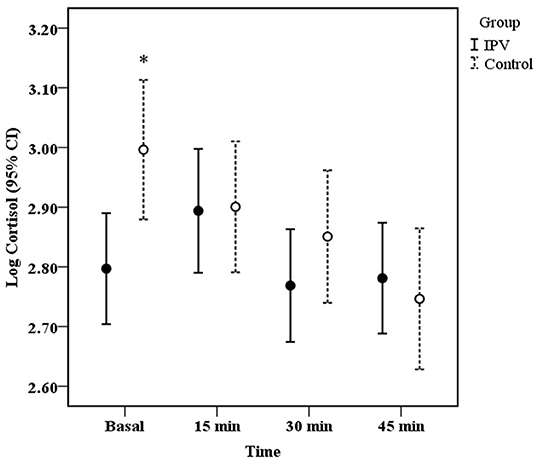
Figure 1. Mean (± 95% CI) of salivary cortisol concentration before (basal), and 15, 30, 45 min after the onset of the cognitive test in women with IPV (bold circle, N = 71) and control without IPV (open circle, N = 59). *P < 0.05 vs. 45 min.
The GEE model indicated that the interaction time × suicide thoughts was statistically significant (X2 Wald = 11.32, d.f. = 3, 71, p = 0.01). Figure 2 shows that women with suicide thoughts had a significant increase in cortisol levels 15 min after the cognitive test compared to basal and 30 min levels (p = 0.02 and p < 0.001, respectively). No significant differences in cortisol secretion were found for IPV patients without suicide thoughts.
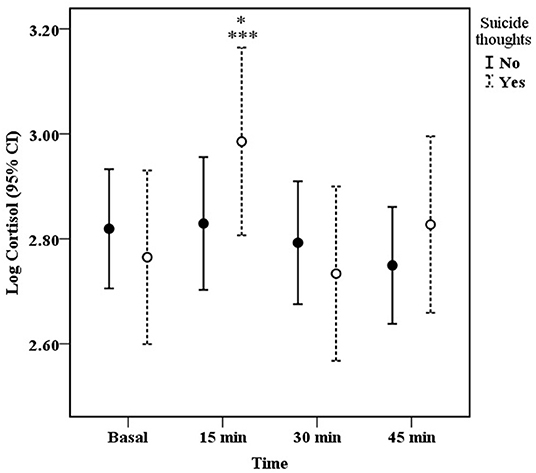
Figure 2. Mean (± 95% CI) of salivary cortisol concentration before (basal), and 15, 30, 45 min after the onset of the cognitive test in IPV exposed women with (N = 29) and without (N = 42) suicide thoughts. Suicide thoughts: ***P < 0.001 vs. 30 min, *P < 0.05 vs. basal.
The results of the MGLM indicated that IPV women with suicide thoughts had significantly worse quality of life than IPV women without these thoughts (Pillai's Trace, F = 3.15, d.f. = 6, 64, p = 0.009, η = 0.22, power = 0.89). Inter-subject analyses indicated that the dimensions of psychological, environment, and social quality of life were significantly lower in IPV women with suicide thoughts (F = 14.05, p < 0.001; F = 3.85, p = 0.05; F = 4.69, p = 0.03, respectively, see Figure 3).
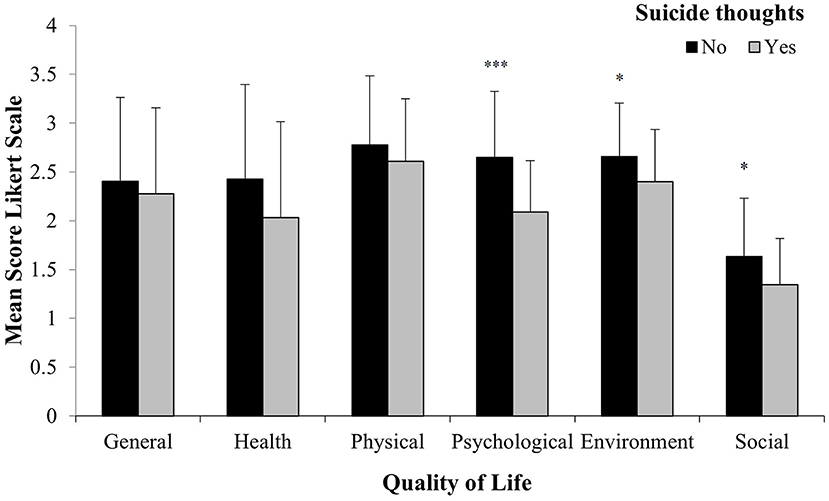
Figure 3. Mean (± SD) of quality of life level in IPV exposed women with (N = 29) and without (N = 42) suicide thoughts. ***P < 0.001, *P < 0.05 vs. suicide thoughts.
The present study aimed to compare cortisol responses between women exposed to IPV and women without IPV, with women in both groups showing symptoms of anxiety and depression. Our findings indicated that cortisol responses in IPV women depended on the exhibition of suicide thoughts and the severity of anxiety and depression symptoms. IPV women with suicide thoughts and severe anxiety and depression symptoms had an increased cortisol response 15 min after the cognitive test compared to IPV women without suicide thoughts and mild to moderate symptoms. Contrastingly, control women without IPV who exhibited minimal to moderate symptoms, showed a decreased cortisol profile. These results support the notion that the experience of IPV is highly stressful for victims (3, 10, 12). Our findings also showed a worse perception in the quality of life in IPV women compared to non-IPV ones, especially for social relationships, which may reflect potential negative effects of their social environment such as experiencing low social support. This result is consistent with previous research asserting that one strategy of batterers to exert control over their partner is to isolate them from family and /or friends, as well as to impose financial restrictions (39, 40) which can diminish their support perceptions.
Our results about cortisol responses in IPV women with suicide thoughts and severe anxiety and depression, agree with previous literature reporting that depressed patients tend to exhibit a hyperactivation of the HPA axis with increased cortisol levels, probably as a result of their psychological load (10, 41). The role of depression and anxiety as comorbidities has also been reported. For instance, Young et al. (42) found an increased activity in the HPA axis of depressed people with comorbid anxiety disorders compared to control subjects.
Our findings are also in line with those reported by Morris et al. (30) who found cortisol responses to the first stage of the TSST to be more pronounced in trauma survivors with current PTSD compared to those without PTSD and non-traumatized controls (who showed blunted responses). It has been reported that people with MDD may have impaired stress coping strategies, partly as a consequence of an increased sensitivity of the HPA axis activation along with an impairment of the negative feedback regulation responsible for ending the stress response (41, 43). In contrast, IPV women with moderate symptomatology and without suicidal thoughts had a blunted response, possibly indicating a higher sensitivity for a negative feedback regulation of cortisol which could contribute to explain the relatively better quality of life reported (44). Previous literature has informed that both exaggerated and blunted cortisol responses after acute stress exposure has been associated with adverse health outcomes (45); in the present study, IPV women indicated poor self-perceptions of general health and quality of life. These perceptions were even more pronounced in the case of IPV women with suicide thoughts and higher cortisol reactivity. This finding agrees with research associating a high degree of chronic stress with recurrent depressive episodes (46). Contrastingly, some clinical studies have associated a blunted cortisol response to stress with poor cognitive abilities, addiction, and poor self-reported health (47). Although some literature has previously discussed the implications for overall wellbeing and health of experiencing either hypo or hyper-reactivity of cortisol levels in response to acute stressors, our results indicate that higher cortisol responses (i.e., hyper-reactivity), may have more negative outcomes including the risk of suicide thoughts and higher symptoms of anxiety and depression (45). The fact that non-IPV women with minimal to moderate symptoms of anxiety and depression had a decreased cortisol secretion supports the hypothesis of an adaptive mechanism promoting rapid negative feedback regulation, which protects the brain from the negative effects of chronic high levels of cortisol (48–50). For instance, Elzinga et al., (51) has suggested that reduced cortisol response in non-clinical women could be explained by an enhanced stress resistance or a marker for resilience. Furthermore, it has been suggested that cortisol hyper-reactivity characterize the short-term effect of an acute stress at the beginning of the adversity, whereas hypo-reactivity may develop in the long-term (48). According to the allostatic load model, individuals who show greater difficulty in adapting to repeated stressors may fail to develop a proper habituation, leading to a higher allostatic load which contribute to hyper-reactivity of the HPA axis and the consequent negative effects on psychological wellbeing and general health (52, 53). In this regard, some studies have shown that most healthy subjects exhibit HPA habituation across repeated psychosocial stressors; however, individual differences may explain variations in sensitization levels (54). Contrastingly, other studies have found that diminished cortisol secretion in response to early trauma exposure increases the risk for developing some mental disorders such as PTSD (55, 56). Discrepancies in the results might be related in part to the nature of the laboratory stressor and the psychological condition of the study subjects. It has been documented that social-evaluative laboratory tests such as the TSST, are perceived as threats by interpersonal trauma survivors with some mental disorder, showing exaggerated responses compared to healthy controls. Thus, people with a history of repeated stressors or negative life events but without developing any mental disorder, might exhibit lower HPA reactivity (51, 57). This hypothesis may explain our findings for the control non-IPV women. It is important to note that our studied population had different sociodemographic characteristics, for example, whereas most IPV women were housewives, non-IPV were mainly students, and also IPV women had less education level than non-IPV. The fact that non-IPV women had symptoms of depression and anxiety could be explained by the fact that most of them were students and could be exposed to academic stress; however, none of these women presented neither severe symptoms nor suicide thoughts. The diminished cortisol response in non-IPV women supports our explanation.
Overall, our results support previous evidence on the negative impact of IPV on women's mental health and quality of life. Particularly, we found that IPV women have markedly higher score of anxiety and depression than control women without IPV, and a poor perception of the quality of life that worsens with the exhibition of suicidal thoughts in patients with severe symptoms. The high cortisol response in those patients, might signal a reduced ability to contend with acute stressors of daily life challenges with potential long-term negative effects in their lives. The findings presented in this study are highly relevant for psychiatrist and clinicians because they highlight the need to design interdisciplinary therapeutic strategies that contemplate the inclusion of physiological variables (e.g., cortisol responses) as complementary markers of general and mental health of victims of IPV. Since there is evidence of the beneficial impact on general health resulting from the availability of social support, further research is needed to test the long-term effects of therapeutic strategies aimed to restore or increase social support in IPV women on mental health and cortisol responses.
The small sample size both in IPV patients and control women without IPV as well as the age differences between both groups may have represented a limitation in the present study. Even though we did not find a significant effect of age in the results, the hypotheses examined in this study have to be tested in future research where this limitation is taken into account. Moreover, the inclusion of sex hormones such as estradiol has to be addressed in further research since it has been shown that fluctuations in this hormone might alter the HPA axis in women with menopausal symptoms (58).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Ética en Investigación. The patients/participants provided their written informed consent to participate in this study.
BC-D, AC-M, MC-L, MB-A, and JW-S designed the proposal, recruited the participants, contributed to the analyses, and writing and interpretation of the data. LM-N measured hormones and contributed to the data analyses. EH-Z contributed to the application of the scales. JB-L contributed to the writing—original draft preparation. All authors contributed to the article and approved the submitted version.
This research did not receive any specific grant from funding agencies in the public, commercial, and not-for-profit sectors; it was completely financed by the Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the INPRFM for supporting the research and we thank the technical assistance of Dr. Alejandra Hernández-Melessio.
1. World Health Organization. Violence Against Women. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed March 16, 2022).
2. World Health Organization. Understanding and Addressing Violence Against Women: Intimate Partner Violence. (2012) Available online at: https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf (accessed March 16, 2022).
3. Lövestad S, Löve J, Vaez M, Krantz G. Prevalence of intimate partner violence and its association with symptoms of depression: a cross-sectional study based on a female population sample in Sweden. BMC Public Health. (2017) 17:1–11. doi: 10.1186/s12889-017-4222-y
4. Morris M, Okoth V, Prigmore HL, Ressler DJ, Mbeya J, Rogers A, et al. The prevalence of interpersonal violence (IPV) against women and its associated variables: an exploratory study in the Rongo Sub-County of Migori County, Kenya. J Interpers Viol. (2022) 37:2083–101. doi: 10.1177/0886260520935484
5. Mojahed A, Alaidarous N, Kopp M, Pogarell A, Thiel F, Garthus-Niegel S. Prevalence of intimate partner violence among intimate partners during the perinatal period: a narrative literature review. Front Psychiatry. (2021) 12:601236. doi: 10.3389/fpsyt.2021.601236
6. Smith SG, Basile KC, Gilbert LK, Merrick MT, Patel N, Walling M. National Intimate Partner Sexual Violence Survey (NISVS): 2010-2012 State Report. (2017). Available online at: https://stacks.cdc.gov/view/cdc/46305/cdc_46305_DS1.pdf (accessed March 16, 2022).
7. Instituto Nacional de Estadística y Geografía,. Estadística a Propósito del día Internacional de la Eliminación de la Violencia Contra la Mujer (25 de Noviembre) 2 592/19. (2019). Available online at: http://www.inegi.org.mx (accessed June 14, 2022).
8. Díaz-Olavarrieta C, Ellerston C, Paz F, Ponce de León S, Alarcón-Segovia D. Prevalence of battering among 1780 outpatients at an internal medicine institution in Mexico. Soc Sci Med. (2002) 55:1589–602. doi: 10.1016/S0277-9536(01)00293-3
9. Labrador-Encinas FJ, Fernández-Velasco MR, Rincón P. Características psicopatológicas de mujeres víctimas de violencia de pareja. Psicothema. (2010) 22:99–105.
10. Bergman B, Brismar B. Suicide attempts by battered wives. Acta Psychiatr Scand. (1991) 83:380–4. doi: 10.1111/j.1600-0447.1991.tb05560.x
11. Devries KM, Child JC, Bacchus LJ, Mak J, Falder G, Graham K, et al. Intimate partner violence victimization and alcohol consumption in women: a systematic review and meta-analysis. Addiction. (2014) 109:379–91. doi: 10.1111/add.12393
12. Chandan J, Thomas T, Bradbury-Jones C, Russell R, Bandyopadhyay S, Nirantharakumar K, et al. Female survivors of intimate partner violence and risk of depression, anxiety, and serious mental illness. Br J Psychiatry. (2019) 217:562–7. doi: 10.1192/bjp.2019.124
13. Han KM, Jee HJ, An H, Shin C, Yoon HK, Ko YH, et al. Intimate partner violence and incidence of depression in married women: a longitudinal study of a nationally representative sample. J Affec Disord. (2019) 245:305–11. doi: 10.1016/j.jad.2018.11.041
14. Ahmadabadi Z, Najman JM, Williams GM, Clavarino AM, d'Abbs P, Tran N. Intimate partner violence and subsequent depression and anxiety disorders. Soc Psychiatry Psychiatr Epidemiol. (2020) 55:611–20. doi: 10.1007/s00127-019-01828-1
15. McEwen BS, Wingfield JC. The concept of allostasis in biology and biomedicine. Horm Behav. (2003) 43:2–15. doi: 10.1016/S0018-506X(02)00024-7
16. Burke HM, Davis MC, Otte C, Mohr DC. Depression and cortisol responses to psychological stress: a meta-analysis. Psychoneuroendocrinology. (2005) 30:846–56. doi: 10.1016/j.psyneuen.2005.02.010
17. Heim C, Newport DJ, Mletzko T, Miller AH, Nemeroff CB. The link between childhood trauma and depression: insights from HPA axis studies in humans. Psychoneuroendocrinology. (2008) 33:693–710. doi: 10.1016/j.psyneuen.2008.03.008
18. Holsen LM, Lancaster K, Klibanski A, Whitfield-Gabrieli S, Cherkerzian S, Buka S, et al. HPA-axis hormone modulation of stress response circuitry activity in women with remitted major depression. Neuroscience. (2013) 250:733–42. doi: 10.1016/j.neuroscience.2013.07.042
19. Cerda-Molina AL, Borráz-León JI, Mayagoitia-Novales L, Gaspar-del Río AT. Reactividad del cortisol y salud mental en adultos expuestos a violencia temprana: revisión sistemática. Rev Panam Salud Publica. (2018) 41:e171. doi: 10.26633/RPSP.2017.171
20. Anacker C, Zunszain PA, Carvalho LA, Pariante CM. The glucocorticoid receptor: pivot of depression and of antidepressant treatment? Psychoneuroendocrinology. (2011) 36:415–25. doi: 10.1016/j.psyneuen.2010.03.007
21. Yehuda R, LeDoux J. Response variation following trauma: a translational neuroscience approach to understanding PTSD. Neuron. (2007) 561:19–32. doi: 10.1016/j.neuron.2007.09.006
22. Kirschbaum C, Kudielka BM, Gaab J, Schommer NC, Hellhammer DH. Impact of gender, menstrual cycle phase, and oral contraceptives on the activity of the hypothalamus-pituitary-adrenal axis. Psychosom Med. (1999) 61:154–62. doi: 10.1097/00006842-199903000-00006
23. Seedat S, Stein MB, Kennedy CM, Hauger RL. Plasma cortisol and neuropeptide Y in female victims of intimate partner violence. Psychoneuroendocrinology. (2003) 28:796–808. doi: 10.1016/S0306-4530(02)00086-0
24. Basu A, Levendosky AA, Lonstein JS. Trauma sequelae and cortisol levels in women exposed to intimate partner violence. Psychodyn Psychiatry. (2013) 41:247–75. doi: 10.1521/pdps.2013.41.2.247
25. Blasco-Ros C, Herbert J, Martinez M. Different profiles of mental and physical health and stress hormone response in women victims of intimate partner violence. J Acute Dis. (2014) 3:303–13. doi: 10.1016/S2221-6189(14)60066-4
26. Pinna KL, Johnson DM, Delahanty DL. PTSD, comorbid depression, and the cortisol waking response in victims of intimate partner violence: preliminary evidence. Anxiety Stress Coping. (2014) 27:253–69. doi: 10.1080/10615806.2013.852185
27. Pico-Alfonso MA, Garcia-Linares MI, Celda-Navarro N, Herbert J, Martinez M. Changes in cortisol and dehydroepiandrosterone in women victims of physical and psychological intimate partner violence. Biol Psychiatry. (2004) 56:233–40. doi: 10.1016/j.biopsych.2004.06.001
28. Inslicht SS, Marmar CR, Neylan TC, Metzler TJ, Hart SL, Otte C, et al. Increased cortisol in women with intimate partner violence-related posttraumatic stress disorder. Psychoneuroendocrinology. (2006) 31:825–38. doi: 10.1016/j.psyneuen.2006.03.007
29. Johnson DM, Delahanty DL, Pinna K. The cortisol awakening response as a function of PTSD severity and abuse chronicity in sheltered battered women. J Anxiety Disord. (2008) 22:793–800. doi: 10.1016/j.janxdis.2007.08.006
30. Morris MC, Bailey B, Hellman N, Williams A, Lannon EW. Dynamics and determinants of cortisol and alpha-amylase responses to repeated stressors in recent interpersonal trauma survivors. Psychoneuroendocrinology. (2020) 122:104899. doi: 10.1016/j.psyneuen.2020.104899
31. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-5®. Washington, DC: American Psychiatric Pub (2013).
32. Valdez-Santiago R, Híjar-Medina MC, Salgado de Snyder VN, Rivera-Rivera L, Avila-Burgos L, Rojas R. Escala de violencia e índice de severidad: una propuesta metodológica para medir la violencia de pareja en mujeres mexicanas. Salud Publica Mex. (2006) 48:s221–31. doi: 10.1590/s0036-36342006000800002
33. Jurado S, Villegas ME, Méndez L, Rodríguez F, Loperena V, Varela R. La estandarización del inventario de depresión de beck para los residentes de la Ciudad de México. Salud Mental. (1998) 21:26–31.
34. Robles R, Varela R, Jurado S, Páez F. Versión mexicana del inventario de ansiedad de beck: propiedades psicométricas. Rev Mex Psicol. (2001) 18:211–8.
35. Skevington S, Lotfy M, O'Connell K. The world health organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL Group. Qual Life Res. (2004) 13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00
36. Huerta JAL, Romo RAG, Tayabas JMT. Propiedades psicométricas de la versión en español de la Escala de Calidad de Vida WHO QoL BREF en una muestra de adultos mexicanos. Rev Iberoam Diagn Eval Aval Psicol. (2017) 2:105–15. doi: 10.21865/RIDEP44.2.09
37. Schultheiss OC, Dargel A, Rohde W. Implicit motives and gonadal steroid hormones: effects of menstrual cycle phase, oral contraceptive use, and relationship status. Horm Behav. (2003) 43:293–301. doi: 10.1016/S0018-506X(03)00003-5
38. Pekár S, Brabec M. Generalized estimating equations: a pragmatic and flexible approach to the marginal GLM modelling of correlated data in the behavioural sciences. Ethology. (2018) 124:86–93. doi: 10.1111/eth.12713
39. Agoff C, Herrera C, Castro R. The weakness of family ties and their perpetuating effects on gender violence: a qualitative study in Mexico. Viol Against Women. (2007) 13:1206–20. doi: 10.1177/1077801207307800
40. Choi SY, Cheung YW, Cheung AK. Social isolation and spousal violence: comparing female marriage migrants with local women. J Marriage Fam. (2012) 74:444–61. doi: 10.1111/j.1741-3737.2012.00963.x
41. Heim C, Newport D J, Heit S, Graham YP, Wilcox M, Bonsall R. Pituitary-adrenal and autonomic responses to stress in women after sexual and physical abuse in childhood. JAMA. (2000) 284:592–7. doi: 10.1001/jama.284.5.592
42. Young EA, Abelson JL, Cameron OG. Effect of comorbid anxiety disorders on the hypothalamic-pituitary-adrenal axis response to a social stressor in major depression. Biol Psychiatry. (2004) 56:113–20. doi: 10.1016/j.biopsych.2004.03.017
43. Fernandez-Guasti A, Fiedler JL, Herrera L, Handa RJ. Sex, stress, and mood disorders: at the intersection of adrenal and gonadal hormones. Horm Metab Res. (2012) 44:607–18. doi: 10.1055/s-0032-1312592
44. Fries E, Hesse J, Hellhammer J, Hellhammer DH. A new view on hypocortisolism. Psychoneuroendocrinology. (2005) 30:1010–6. doi: 10.1016/j.psyneuen.2005.04.006
45. De Rooij SR, Roseboom TJ. Further evidence for an association between self-reported health and cardiovascular as well as cortisol reactions to acute psychological stress. Psychophysiology. (2010) 47:1172–5. doi: 10.1111/j.1469-8986.2010.01023.x
46. Gunnar MR, Vazquez DM. Low cortisol and a flattening of expected daytime rhythm: potential indices of risk in human development. Dev Psychopathol. (2001) 13:515–38. doi: 10.1017/S0954579401003066
47. Raison CL, Miller AH. When not enough is too much: the role of insufficient glucocorticoid signaling in the pathophysiology of stress-related disorders. Am J Psychiatry. (2003) 160:1554–65. doi: 10.1176/appi.ajp.160.9.1554
48. Miller GE, Chen E, Zhou ES. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol Bull. (2007) 133:25–45. doi: 10.1037/0033-2909.133.1.25
49. Borráz-León JI, Cerda-Molina AL, Mayagoitia-Novales L. Stress and cortisol responses in men: differences according to facial symmetry. Stress. (2017) 20:573–9. doi: 10.1080/10253890.2017.1378341
50. Reyes-Mota AR, Cerda-Molina AL, Mayagoitia-Novales L, Viveros-Sandoval ME, Borráz-León JI. Reduced cortisol response to traumatic images, self-esteem and stress levels in emergency medical technicians from the red cross. Pers Indiv Diff. (2021) 179:110929. doi: 10.1016/j.paid.2021.110929
51. Elzinga BM, Roelofs K, Tollenaar MS, Bakvis P, van Pelt J, Spinhoven P. Diminished cortisol responses to psychosocial stress associated with lifetime adverse events: a study among healthy young subjects. Psychoneuroendocrinology. (2008) 33:227–37. doi: 10.1016/j.psyneuen.2007.11.004
52. McEwen BS. Protection and damage from acute and chronic stress: allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann NY Acad Sci. (2004) 1032:1–7. doi: 10.1196/annals.1314.001
53. Liberzon I, Abelson JL. Context processing and the neurobiology of post-traumatic stress disorder. Neuron. (2016) 92:14–30. doi: 10.1016/j.neuron.2016.09.039
54. Wüst S, Federenko IS, van Rossum EF, Koper JW, Hellhammer DH. Habituation of cortisol responses to repeated psychosocial stress—further characterization and impact of genetic factors. Psychoneuroendocrinology. (2005) 30:199–211. doi: 10.1016/j.psyneuen.2004.07.002
55. Yehuda R. Current status of cortisol findings in post-traumatic stress disorder. Psychiatric Clinics. (2002) 25:341–68. doi: 10.1016/S0193-953X(02)00002-3
56. Morris MC, Hellman N, Abelson JL, Rao U. Cortisol, heart rate, and blood pressure as early markers of PTSD risk: a systematic review and meta-analysis. Clin Psychol Rev. (2016) 49:79–91. doi: 10.1016/j.cpr.2016.09.001
57. Steudte-Schmiedgen S, Kirschbaum C, Alexander N, Stalder T. An integrative model linking traumatization, cortisol dysregulation and posttraumatic stress disorder: insight from recent hair cortisol findings. Neurosci Biobehav Rev. (2016) 69:124–35. doi: 10.1016/j.neubiorev.2016.07.015
Keywords: intimate partner violence, cortisol response, anxiety, depression, quality of life, suicide thoughts
Citation: Cerda-De la O B, Cerda-Molina AL, Mayagoitia-Novales L, de la Cruz-López M, Biagini-Alarcón M, Hernández-Zúñiga EL, Borráz-León JI and Whaley-Sánchez JA (2022) Increased Cortisol Response and Low Quality of Life in Women Exposed to Intimate Partner Violence With Severe Anxiety and Depression. Front. Psychiatry 13:898017. doi: 10.3389/fpsyt.2022.898017
Received: 16 March 2022; Accepted: 06 June 2022;
Published: 27 June 2022.
Edited by:
Ravi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), IndiaReviewed by:
Roberto Ariel Abeldaño Zuñiga, University of the South Sierra, MexicoCopyright © 2022 Cerda-De la O, Cerda-Molina, Mayagoitia-Novales, de la Cruz-López, Biagini-Alarcón, Hernández-Zúñiga, Borráz-León and Whaley-Sánchez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Lilia Cerda-Molina, YWxjbUBpbXAuZWR1Lm14
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.