
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 09 September 2022
Sec. Digital Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.893073
This article is part of the Research Topic Digital Mental Health Research: Understanding Participant Engagement and Need for User-centered Assessment and Interventional Digital Tools View all 13 articles
 Carmen Gonzalez1,2,3,4*
Carmen Gonzalez1,2,3,4* Magaly Ramirez1,2,3,4Felicia Mata-Greve1,2,3,4Autumn Diaz1,2,3,4Miriana C. Duran1,2,3,4Morgan Johnson1,2,3,4
Magaly Ramirez1,2,3,4Felicia Mata-Greve1,2,3,4Autumn Diaz1,2,3,4Miriana C. Duran1,2,3,4Morgan Johnson1,2,3,4 Nancy Grote1,2,3,4
Nancy Grote1,2,3,4 Patricia A. Areán1,2,3,4
Patricia A. Areán1,2,3,4Background: Postpartum depression (PPD) affects one in eight women in the U.S., with rates increasing due to the COVID-19 pandemic. Given the unique circumstances of COVID-19, virtual therapy might be a unique way to overcome barriers to mental health services. The study sought to explore the acceptability of virtual therapy among women in the postpartum period.
Methods: Using an online recruitment mixed methods approach, we collected data from a U.S. national cross-sectional sample of women (N = 479) who gave birth in the last 12 months.
Findings: Results show that 66% of women endorsed items consistent with possible depression during the COVID-19 pandemic. Only 27% accessed therapy services during the postpartum period. While 88% were open to engaging in virtual therapy services, 12% identified several major concerns with virtual therapy, namely: (1) preference for in-person therapy (2) no perceived need for therapy (3) uncomfortable with virtual therapy, and (4) lack of privacy. Of note, 36% more Latinas reported dissatisfaction with quality of care received during virtual therapy compared to non-Latina participants. Despite a major shift to virtual care with COVID-19, future work is needed to make virtual mental health services more accessible for women with PPD.
Postpartum depression (PPD) is the most common pregnancy complication and affects approximately one in eight women in the U.S (1). Women of color and women from low-income backgrounds report even higher rates of PPD (2). With changes for many individuals due to mandated stay-at-home orders during the COVID-19 pandemic, rates of PPD have doubled compared to pre-pandemic rate (3). With the unique circumstances of the pandemic, digital mental health, or services delivered through technology platforms, might be a unique way to overcome barriers to care and effectively provide mental health support in the postpartum period. However, little is known about the acceptability of this form of care among postpartum women.
While postpartum mood disorders increase, there are still several barriers to postpartum mental health care as well as a shortage of providers that offer culturally appropriate services (4). For example, among 500 postpartum women from diverse backgrounds, only 4% of the sample indicated that they had no barriers to accessing mental health care (5). While many women report that common barriers to mental health care include lack of time, childcare, knowledge about PPD, stigma, and transportation concerns (4, 5), systemic inequities further affect treatment options available to women from low-income backgrounds (6), women of color (7), and women with limited English proficiency (4). Latina women often report being under- or uninsured as well as challenges with childcare, transportation, and leave (6, 8).
COVID-19 has underlined these disparities by increasing financial stress and social isolation for new parents. Home environments have also shifted during the pandemic, with mothers often taking on more care responsibilities as schools, businesses, and social services moved online (9). For postpartum women, the experience of giving birth and taking care of a newborn during a pandemic can lead to compounded trauma.
Digital mental health interventions have been proposed as a novel way to overcome barriers and shortages of postpartum mental health care. As a subset of digital mental health services, self-guided digital mental health apps have been developed and hold potential for reaching women with untreated PPD (10) as well as individuals negatively impacted by the COVID-19 pandemic (11). In fact, a recent systematic review of 21 experimental and randomized controlled trials found that perinatal women in high-income countries that used self-guided digital mental health apps and coach-guided digital mental health apps reported significantly decreased depression from pre- to post-intervention (12). These self-guided digital mental health apps might also contribute to the reduction of barriers related to transportation, childcare, time constraints, and language fluency for Latina women (13).
Fewer digital mental health services have used the feature of virtual therapy, or one-on-one contact between a patient and mental health provider in real-time (e.g., video conferencing, telepsychotherapy, and message-based care). Nair et al. (14) conducted a systematic review of 10 randomized controlled trials published between 2000 and 2018 to assess the effectiveness of virtual therapy, which included phone calls, emails, coach-guided mental health apps, and coach-guided websites to treat PPD. A majority of these studies reported significant improvement in depression scores post intervention, signaling promise for an understudied use of telemedicine. Virtual therapy can reduce barriers for postpartum mental health care, especially for women from underserved backgrounds, who are more likely to report difficulties accessing in-person therapy due to transportation, scheduling, and childcare concerns (4).
There are few studies that explore whether women in the postpartum period are receptive to virtual interventions (15). Outside of the postpartum literature, a recent study found that patients are open to virtual therapy and mental health apps with understandable apprehension surrounding privacy and quality of mental health care (16). Videoconferencing psychotherapy (VCP) specifically has been found to have similar outcomes to in person psychotherapy and is associated with positive user satisfaction (17). Thus, research is needed to understand the specific concerns of virtual therapy among women in the postpartum period, particularly during the COVID-19 pandemic and the rapid shift to telehealth.
The objectives of this mixed-methods cross-sectional study included: (a) to describe experiences with mental health services among women in the postpartum period during the COVID-19 pandemic, and (b) to explore the specific concerns of virtual therapy among women in the postpartum period. Because overwhelming evidence has demonstrated how COVID-19 has disproportionately affected Latinx populations in the U.S., we also examined how these experiences and concerns varied between Latina and non-Latina women (1). The findings from this study will inform how to address specific concerns of virtual therapy in future development of virtual mental health support.
Participants completed the online cross-sectional survey between 7/16/20 and 8/28/20 through Prolific.co., an online platform that allows users to complete surveys and experiments (18). During the study period various states were still under stay at home, shelter in place, or social distancing orders that aimed to slow the spread of COVID-19. Survey participants included those that are: female, U.S. residents, with at least one child, 18–50 YO. In addition, participants completed an eligibility questionnaire to determine whether they had given birth in the last 12 months. Survey items were piloted and refined during five practice interviews. This study was reviewed and approved by an Institutional Review Board.
The survey took an average of 10 min to complete. Survey responses were captured using Research Electronic Data Capture (REDCap) (19, 20), a secure web application developed to capture data for research that complies with HIPAA standards. Prolific.co ID numbers were stored with the survey to avoid duplicate responses. Personal data were not collected with the exception of women who voluntarily provided their contact information (which was stored in a password protected computer at the home institution) for a follow-up interview. Participants received $5 compensation for their participation in the survey.
Participants completed a demographic questionnaire, which assessed age, assigned sex at birth, employment status, marital status, race, ethnicity, and English proficiency.
Survey questions were developed by the authors (experts in mental health, health services, health information and communication technology) to understand the experiences of women seeking mental health services in the postpartum period and their concerns with using virtual therapy during the COVID-19 pandemic. These questions asked about prior experiences with therapy, their willingness to consult a therapist, their preference for in-person or virtual therapy, and potential challenges to talking to a therapist online. Some items were open-ended (e.g., “Can you tell us a bit about your experience with receiving emotional support from a professional during your pregnancy?”) and some provided response options [e.g., “To what extent would you agree or disagree with the following statement: I am satisfied with the quality of care I received during virtual (therapy) interactions (strongly agree, agree, disagree, or strongly disagree)”].
Participants completed the Edinburgh Postnatal Depression Scale (EPDS) (21, 22), a 10-item questionnaire that screens for PPD. Participants indicate whether they have experienced symptoms of depression (e.g., “I have blamed myself unnecessarily when things went wrong”). Summary scores are calculated (range from 0 to 30). We categorized respondents into four categories based on scoring guidelines outlined by Cox et al. (21): depression not likely (<8), depression possible (9–11), fairly high possibility of depression (12–13), and probable depression (14 and higher). We grouped women into depression not likely (score of 8 or below) and depression possible (score of 9 or above). In the current study, internal consistency reliability was excellent (Cronbach α = 0.90; omega = 0.90). Participants who reported suicidality were sent a follow up email with a list of postpartum and suicide prevention resources.
Means and frequencies were used to document demographic information, postpartum mental health outcomes, experiences with mental health services in the postpartum period, and concerns with virtual therapy. Percentages reported in the results do not reflect missingness (N = 479). To further explore how COVID-19 has disproportionately affected the Latinx population in the U.S., we assessed for differences in experiences and concerns between Latina and non-Latina participants using Fisher's exact chi-square tests, chi-square tests, and independent t-tests. We only present results when there is a statistically significant difference between Latina and non-Latina participants. All quantitative statistical analyses were performed with SAS version 9.4.
We conducted a thematic analysis of the responses to an open-ended question about reasons why participants would not be open to consulting a therapist virtually. Textual responses to the open-ended questions varied from a few words to a few sentences, with participants writing an average of 50 words. For theme identification, we first used an inductive approach that involved two authors pile-sorting each participants' response into categories based on affinity (i.e., the reason for why they were not interested in virtual therapy). Affinity diagramming, a user-centered design approach, is an exploratory qualitative analysis method that facilitates the creation of a codebook; a pile sort is a grouping of similar thoughts, perspectives, or statements (23). This process identified four salient categories: (1) preference for in-person therapy, (2) no perceived need for therapy, (3) not comfortable speaking to a therapist, and (4) lack of privacy at home. To identify subthemes, the two authors further pile-sorted responses within each of the four categories. We provide a description of each category and include representative quotes from participants' responses. All qualitative analyses were performed using Dedoose coding software.
See Table 1 for characteristics of study participants. There were 2416 individuals who were interested in completing the survey. In total, 479 women were screened eligible and completed the survey. The average age was 30.3 years. Most (72%) of the sample identified as White, and ~7% of the sample identified as Latina. Most participants (97%) indicated that they spoke English “very well.” Participants reported residing in state across the U.S., with larger states such as California, Florida, and New York more highly represented. Approximately two-thirds of the sample were in the “depression possible” range for PPD.
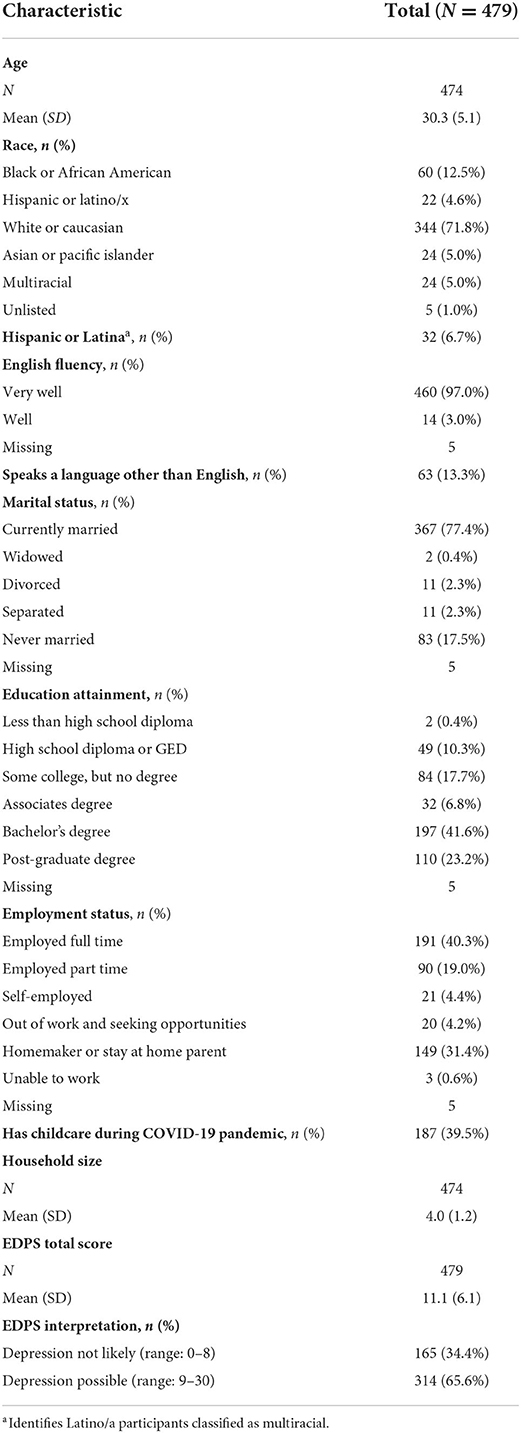
Table 1. Sample characteristics.
Of the 479 participants, 27% (126/474) reported having spoken to a counselor, therapist, or other mental health professional since giving birth. About half (64/126) of participants reported that the encounter was virtual. On average, it had been 67 (SD = 82.5) days between the time they took the survey and the last time that they spoke with their therapist via virtual encounter. Virtual encounters happened via video (42/64; 66%), telephone (29/64; 45%), and text message (8/64; 13%). Among all the participants who had received postpartum mental health care (n = 126), the degree of satisfaction with virtual mental healthcare encounters in general (regardless of the nature of their postpartum care) was significantly lower among Latinas (n = 11) compared to non-Latina participants (n = 115; Table 2). In fact, 36% more Latinas disagreed or strongly disagreed with the statement about being satisfied with the quality of care received during virtual encounters compared to non-Latina participants.
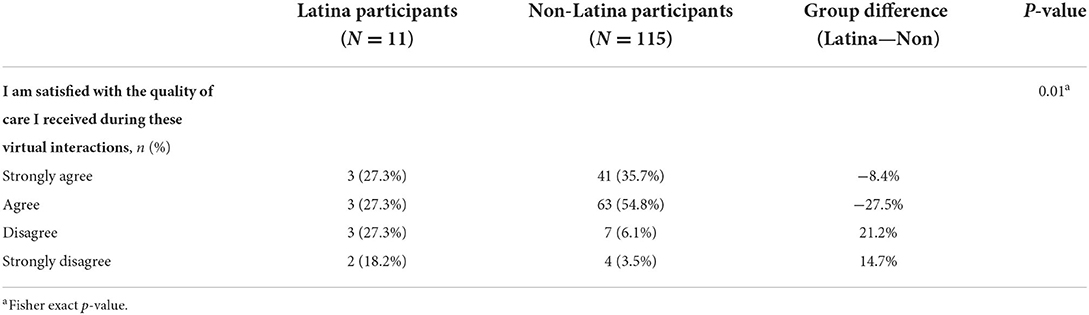
Table 2. Participant satisfaction with virtual mental healthcare encounters, by ethnicity.
In the total sample, 88% of participants reported being open to consulting a mental health professional in the future. Among those open to future mental health services, 91% (382/418) reported they would consider virtual mental health services. The top concerns for accessing virtual mental healthcare were privacy (226/479; 47.2%), cost (222/479; 46.3%), time (130/479; 27.1%), and trust (128/479; 26.7%). Participants who were not interested in virtual mental healthcare encounters provided open-ended responses to further elaborate on their lack of interest. The following themes emerged from these qualitative responses: (1) preference for in-person therapy, (2) no perceived need for therapy, (3) not comfortable speaking to a therapist, and (4) lack of privacy at home.
Participants stated a preference for in-person therapy. Participants stated that they would feel uncomfortable discussing sensitive topics in a virtual environment (Box 1, extracts 1–2). These participants perceived that face-to-face conversations would be the most appropriate way to share their emotions. There was also aversion to virtual therapy because of a perception that it would not be tailored to their unique situation. Participants doubted that virtual therapy could be delivered in a way that made it feel as “personal” as a face-to-face encounter (Box 1, extract 3). Finally, participants believed that virtual therapy would not be as effective as in-person treatment. For some, this perception was influenced by negative past experiences with virtual therapy (Box 1, extracts 4–5).
Box 1. Theme 1—Preference for in-person therapy.
1. 32-year-old White participant: “I have comfort issues regarding virtual sessions of that nature and would much rather speak face to face with a counselor or therapist.”
2. 40-year-old Asian participant: “I just prefer being in person while talking about intimate things.”
3. 23-year-old African American participant: “I like for it (therapy) to feel more personal and the only way to do that is in person for me.”
4. 27-year-old White participant: “It (virtual therapy) doesn't work for me.”
5. 32-year-old White participant: “I feel like virtually would not feel as effective for me.”
Participants reported that they were not interested in virtual therapy because they currently did not have a need. Participants stated that they were not experiencing symptoms of depression and anxiety or that they felt well-emotionally (Box 2, extracts 1–3). However, the EPDS scores of 6/19 participants stating no perceived need for therapy indicated possible depression. Some participants explained that if there were days when they were feeling down (which could be triggered by the COVID-19 pandemic), they already had coping strategies, which included reaching out to a spouse/partner and other family members, engaging in physical activity, eating healthy, meditating, and getting adequate sleep (Box 2, extracts 4–5).
Box 2. Theme 2—No perceived need for therapy.
1. 29-year-old White participant (EPDS score = 8; depression not likely): “I'm not feeling down or hopeless.”
2. 32-year-old White participant (EPDS score = 3; depression not likely): “I'm not suffering from baby blues or any other depression.”
3. 22-year-old Asian participant (EPDS score = 11; possible depression): “I am sure that I am feeling okay mentally and spiritually.”
4. 32-year-old Asian participant (EPDS score = 11; possible depression): “I have a few random days here and there of anxiety, but that is related to COVID and are rare. I just do some meditation and go to sleep and feel back to normal the next day.”
5. 27-year-old White participant (EPDS score = 4; depression not likely): “I am happy and know how to navigate and pull myself back up if I happen to fall into a slump. We eat well, regularly exercise, I take my children hiking 3 days a week and do yoga 5 days a week too. I have a strong family support system and love my in-laws.”
Participants stated a disinterest in virtual therapy because they would feel uncomfortable. A few participants described experiencing shyness and social anxiety, regardless of whether interactions with others were in-person or virtual (Box 3, extracts 1–2). Other participants explained that they would be uncomfortable speaking about sensitive topics with someone they never met before (Box 3, extracts 3–5). They expressed a desire to meet the mental health professional face-to-face before transitioning to a virtual environment.
Box 3. Theme 3—Not comfortable speaking to a therapist.
1. 18-year-old Latina participant: “I wouldn't feel comfortable. I'm a very shy person.”
2. 39-year-old participant*: “I have pretty bad social anxiety so even if I do go to talk to someone ill most likely shut down at the time.”
3. 31-year-old White participant: “I would want to meet with someone in person first. I feel it is a better way of getting to know someone.”
4. 24-year-old White participant: “Not comfortable sharing sensitive information to someone I haven't seen.”
5. 23-year-old White participant: “It's hard to feel comfortable with someone you haven't met in real life.”
*No race or ethnicity reported.
Participants explained that they were not interested in virtual therapy because they did not have privacy at home. Some participants did not want others to find out they were speaking to a therapist (Box 4, extract 1). Other participants were worried about members of their household listening during phone calls and reading text message conversations with a therapist (Box 4, extract 2–3).
Box 4. Theme 4—Lack of privacy at home.
1. 24-year-old Latina participant: “I would not sure want anyone to know I am seeing a therapist.”
2. 27-year-old White participant: “I would be afraid I would get interrupted, other people could hear me.”
3. 35-year-old White participant: “Too worried about people breaking into that to get my info or chats.”
The mixed methods study supports that even though two-thirds of the U.S. sample of women reported possible PPD during the COVID-19 pandemic, only 27% had consulted a mental health professional. Of note, Latina women reported lower satisfaction with virtual therapy compared to non-Latina women. This finding is concerning given that the U.S. Latinx population is disproportionately affected by both COVID-19 (24) and PPD (25) compared to their White counterparts. The results support that even though U.S. residents are in the midst of a pandemic causing many healthcare services to shift to telehealth, one-quarter of the sample still reported hesitancy with virtual therapy. For those not interested in virtual therapy, primary reasons identified for apprehension included a preference for in-person therapy, no perceived need, uncomfortable with the idea of virtual therapy, and lack of privacy at home.
This study reported higher rates of possible PPD compared to previous U.S. studies (3). Through the self-reported Pregnancy Risk Assessment Monitoring System, the CDC (1) reports that 1 in 8 women experience PPD, whereas this study's results were closer to 6 in 8 women. Our increased rates might be explained by diagnostic clarity. Many cases of PPD typically go undiagnosed due to structural barriers as well as a lack of proper assessment (8, 21, 22). We used the EPDS, a scale that specifically assesses depression symptoms during the postpartum period. Another explanation is the stress associated with the COVID-19 pandemic, which has included exacerbated fear (26), isolation (27), and financial strain (28).
Only 27% of women indicated consulting a mental health professional during the postpartum period. This discrepancy in need and use necessitates an urgent solution to increase accessibility to mental health services as well as proper education of symptoms related to PPD. Of those that did receive mental health services, approximately half were done virtually via video, telephone or text message platforms. Since COVID-19 has shifted many services to virtual platforms, it is important to understand patient concerns. Consistent with pre-pandemic research (16), some participants identify a preference for in-person therapy. This preference seems to stem from perceived increased authenticity in person (16) and worries that virtual therapy is less effective (16, 29).
Participants identified that they would not engage with virtual therapy because they did not perceive a need for therapy. Interestingly, of the 19 women that listed this concern, six endorsed elevated levels consistent with possible depression on the EPDS. Previous studies have highlighted stigma and beliefs about motherhood as barriers to treatment (30). While the American College of Obstetricians and Gynecologists and the US Preventive Services Task Force have strongly recommended universal screening, there may also be an increased need for education of PPD and its treatment (31).
Participants stated they would not be comfortable with virtual therapy, and that they had concerns with a lack of privacy at home. The COVID-19 pandemic has changed home environments for many with an increase in adults working from home (32) and school-age children engaging in remote learning (33). There is evidence to support that women are taking on more care and responsibilities during the COVID-19 pandemic (9), which may be driving comfort and privacy concerns regarding virtual therapy compared to pre-pandemic times.
This study had several limitations. Because our sample was recruited through an online platform, it is likely that participants were more comfortable with technology and may have different views about data security and privacy. This study was cross-sectional, thus, opinions about virtual therapy may change over time as the population has more access to telehealth during the pandemic. Such limitations do not detract from the importance of the findings, which highlight the low utilization and trust in virtual mental health care by women who are currently using technology. Likely because of our recruitment methods, our sampling of women of color was relatively low (e.g., 7% of this sample was Latina v. 17% of the U.S. population is Latinx). The recruitment reach of the platform used for this study makes it difficult to target specific demographics; a longer study period could help to oversample specific groups (including postpartum women). Survey instruments were also available in English only, further limiting the generalizability of our findings to English-speaking women who are likely more acculturated. We recommend a future study comparing remotely recruited samples to locally recruited (and demographically targeted) samples in their acceptance of virtual mental health care. We also did not collect information about the presence of a diagnosed mental disorder; future studies could benefit from such contextual information.
Despite these limitations, the data from this study have important implications about the concept that virtual mental health care is a viable alternative to traditionally delivered care. To improve the approachability of virtual therapy, researchers and clinicians may employ user-centered design alongside patients and better understand how women intend to use virtual therapy for support (13).
These results further support that rates of psychological distress, such as PPD, are elevated during the COVID-19 pandemic. Despite most of our sample reporting symptoms consistent with possible depression symptoms, only one-quarter have used psychotherapy services. While many participants were open to engaging in virtual therapy, primary concerns included preference for in-person services, lack of perceived need, discomfort with virtual therapy, and lack of privacy. We recommend that researchers and clinicians continue to find ways to make virtual therapy more approachable to the needs of women experiencing PPD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of Washington Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
CG and MR: guarantors. CG, MR, PA, and NG: study concept and design. CG, MR, MD, MJ, and FM-G: acquisition, analysis, or interpretation of data. CG, FM-G, MR, MD, and AD: drafting of the manuscript. CG, MR, PA, and NG: obtaining funding. All authors critical revision of the manuscript, had full access to the study data, take responsibility for the integrity of the complete work, and the final decision to submit the manuscript.
This work was supported by the National Institutes of Mental Health (grant numbers P50MH115837, T32MH020021). The content is solely the responsibilities of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Centers for Disease Control Prevention. Reproductive Health: Depression Among Women. Centers for Disease Control and Prevention (2020). Available online at: https://www.cdc.gov/reproductivehealth/depression/index.htm (accessed February 15, 2022).
2. Howell EA, Mora PA, Horowitz CR, Leventhal H. Racial and ethnic differences in factors associated with early postpartum depressive symptoms. Obstet Gynecol. (2005) 105:1442–50. doi: 10.1097/01.AOG.0000164050.34126.37
3. Davenport MH, Meyer S, Meah VL, Strynadka MC, Khurana R. Moms are not ok: COVID-19 and maternal mental health. Front Global Women Health. (2020) 1:1. doi: 10.3389/fgwh.2020.00001
4. Bina R. Predictors of postpartum depression service use: a theory-informed, integrative systematic review. Women Birth. (2020) 33:e24–32. doi: 10.1016/j.wombi.2019.01.006
5. Goodman JH. Women's attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth. (2009) 36:60–9. doi: 10.1111/j.1523-536X.2008.00296.x
6. Kozhimannil KB, Trinacty CM, Busch AB, Huskamp HA, Adams AS. Racial and ethnic disparities in postpartum depression care among low-income women. Psychiatric Serv. (2011) 62:619–25. doi: 10.1176/ps.62.6.pss6206_0619
7. Hansotte E, Payne SI, Babich SM. Positive postpartum depression screening practices and subsequent mental health treatment for low-income women in Western countries: a systematic literature review. Public Health Rev. (2017) 38:3. doi: 10.1186/s40985-017-0050-y
8. Abrams LS, Dornig K, Curran L. Barriers to service use for postpartum depression symptoms among low-income ethnic minority mothers in the United States. Qual Health Res. (2009) 19:535–51. doi: 10.1177/1049732309332794
9. Power K. The COVID-19 pandemic has increased the care burden of women and families. Sustainabil Sci Pract Policy. (2020) 16:67–73. doi: 10.1080/15487733.2020.1776561
10. Zhou C, Hu H, Wang C, Zhu Z, Feng G, Xue J, et al. The effectiveness of mHealth interventions on postpartum depression: a systematic review and meta-analysis. J Telemed Telecare. (2020) 28:83–95. doi: 10.1177/1357633X20917816
11. Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S Bai X., et al. The role of telehealth in reducing the mental health burden from COVID-19. Telemed e-Health. (2020) 26:377–9. doi: 10.1089/tmj.2020.0068
12. Dol J, Richardson B, Murphy GT, Aston M, McMillan D, Campbell-Yeo M. Impact of mobile health interventions during the perinatal period on maternal psychosocial outcomes: a systematic review. JBI Evid Synth. (2020) 18:30–55. doi: 10.11124/JBISRIR-D-19-00191
13. Fortuna LR, Tolou-Shams M, Robles-Ramamurthy B, Porche MV. Inequity and the disproportionate impact of COVID-19 on communities of color in the United States: the need for a trauma-informed social justice response. Psychol Trauma Theory Res Pract Policy. (2020) 12:443–5. doi: 10.1037/tra0000889
14. Nair U, Armfield NR, Chatfield MD, Edirippulige S. The effectiveness of telemedicine interventions to address maternal depression: a systematic review and meta-analysis. J Telemed Telecare. (2018) 24:639–50. doi: 10.1177/1357633X18794332
15. Barrera AZ, Wickham RE, Muñoz RF. Online prevention of postpartum depression for Spanish-and English-speaking pregnant women: a pilot randomized controlled trial. Int Int. (2015) 2:257–65. doi: 10.1016/j.invent.2015.06.002
16. Renn BN, Hoeft TJ, Lee HS, Bauer AM, Areán PA. Preference for in-person psychotherapy versus digital psychotherapy options for depression: survey of adults in the US. NPJ Dig Med. (2019) 2:1–7. doi: 10.1038/s41746-019-0077-1
17. Backhaus A, Agha Z, Maglione ML, Repp A, Ross B, Zuest D, et al. Videoconferencing psychotherapy: a systematic review. Psychol Serv. (2012) 9:111. doi: 10.1037/a0027924
19. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
20. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
21. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Brit J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
22. Wisner KL, Parry BL, Piontek CM. Postpartum depression. N Engl J Med. (2002) 347:194–9. doi: 10.1056/NEJMcp011542
23. Haskins Lisle A, Merenda C, Gabbard J. Using affinity diagramming to generate a codebook: a case study on young military veterans and community reintegration. Qualit Res. (2020) 20:396–413. doi: 10.1177/1468794119851324
24. Oppel RA, Gebeloff R, Lai KKR, Wright W, Smith R. The Fullest Look Yet at the Racial Inequity of Coronavirus. New York Times (2020).
25. Lucero NB, Beckstrand RL, Callister LC, Sanchez Birkhead AC. Prevalence of postpartum depression among Hispanic immigrant women. J Am Acad Nurse Pract. (2012) 24:726–34. doi: 10.1111/j.1745-7599.2012.00744.x
26. Fitzpatrick KM, Harris C, Drawve G. Fear of COVID-19 and the mental health consequences in America. Psychol Trauma Theory Res Pract Policy. (2020) S1:S17–21. doi: 10.1037/tra0000924
27. Benke C, Autenrieth L, Asselmann E, Pané-Farré CA. Lockdown, quarantine measures, and social distancing: associations with depression, anxiety, and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. (2020) 293:113462. doi: 10.1016/j.psychres.2020.113462
28. Mimoun E, Ben Ari A, Margalit D. Psychological aspects of employment instability during the COVID-19 pandemic. Psychol Trauma Theory Res Pract Policy. (2020) 12(Suppl. 1):S183–5. doi: 10.1037/tra0000769
29. Linardon J, Shatte A, Tepper H, Fuller-Tyszkiewicz M. A survey study of attitudes toward, and preferences for, e-therapy interventions for eating disorder psychopathology. Int J Eating Dis. (2020) 53:23268. doi: 10.1002/eat.23268
30. Callister LC, Beckstrand RL, Corbett C. Postpartum depression and help-seeking behaviors in immigrant Hispanic women. J Obst Gynecol Neonatal Nursing. (2011) 40:440–9. doi: 10.1111/j.1552-6909.2011.01254.x
31. Baker-Ericzén MJ, Connelly CD, Hazen AL, Dueñas C, Landsverk JA, Horwitz SM. A collaborative care telemedicine intervention to overcome treatment barriers for Latina women with depression during the perinatal period. Famil Syst Health. (2012) 30:224–40. doi: 10.1037/a0028750
32. Bick K, Blandin A, Mertens A. Work from home after the COVID-19 outbreak. Monet Eco Fluctuat. (2020). doi: 10.2139/ssrn.3786142
Keywords: postpartum depression, virtual therapy, COVID-19, telehealth, digital health
Citation: Gonzalez C, Ramirez M, Mata-Greve F, Diaz A, Duran MC, Johnson M, Grote N and Areán PA (2022) Acceptability of virtual therapy for postpartum women during COVID-19: A national mixed methods study. Front. Psychiatry 13:893073. doi: 10.3389/fpsyt.2022.893073
Received: 09 March 2022; Accepted: 17 August 2022;
Published: 09 September 2022.
Edited by:
Rosa M. Baños, University of Valencia, SpainReviewed by:
Giulia Corno, University of Quebec in Outaouais, CanadaCopyright © 2022 Gonzalez, Ramirez, Mata-Greve, Diaz, Duran, Johnson, Grote and Areán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carmen Gonzalez, Y21nb256YWxAdXcuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.