
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychiatry , 20 May 2022
Sec. Molecular Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.889572
This article is part of the Research Topic Behavioral Dysfunctions in Neuropsychiatric Diseases: Exploring New Therapeutic Targets View all 6 articles
 Katharina O. Sandström1†
Katharina O. Sandström1† Olga B. Baltzersen1†
Olga B. Baltzersen1† Anouk Marsman2
Anouk Marsman2 Cecilie K. Lemvigh1Vincent O. Boer2
Cecilie K. Lemvigh1Vincent O. Boer2 Kirsten B. Bojesen1
Kirsten B. Bojesen1 Mette Ø. Nielsen1,3Henrik Lundell2Daban K. Sulaiman1
Mette Ø. Nielsen1,3Henrik Lundell2Daban K. Sulaiman1 Mikkel E. Sørensen1Birgitte Fagerlund1,4
Mikkel E. Sørensen1Birgitte Fagerlund1,4 Adrienne C. Lahti5
Adrienne C. Lahti5 Warda T. Syeda6
Warda T. Syeda6 Christos Pantelis6Esben T. Petersen2,7
Christos Pantelis6Esben T. Petersen2,7 Birte Y. Glenthøj1,3Hartwig R. Siebner2,3,8
Birte Y. Glenthøj1,3Hartwig R. Siebner2,3,8 Bjørn H. Ebdrup1,3*
Bjørn H. Ebdrup1,3*
Background: Antipsychotic drugs are primarily efficacious in treating positive symptoms by blocking the dopamine D2 receptor, but they fail to substantially improve negative symptoms and cognitive deficits. The limited efficacy may be attributed to the fact that the pathophysiology of psychosis involves multiple neurotransmitter systems. In patients with chronic schizophrenia, memantine, a non-competitive glutamatergic NMDA receptor antagonist, shows promise for ameliorating negative symptoms and improving cognition. Yet, it is unknown how memantine modulates glutamate levels, and memantine has not been investigated in patients with first-episode psychosis.
Aims: This investigator-initiated double-blinded randomized controlled trial is designed to (1) test the clinical effects on negative symptoms of add-on memantine to antipsychotic medication, and (2) neurobiologically characterize the responders to add-on memantine.
Materials and Equipment: Antipsychotic-naïve patients with first-episode psychosis will be randomized to 12 weeks treatment with [amisulpride + memantine] or [amisulpride + placebo]. We aim for a minimum of 18 patients in each treatment arm to complete the trial. Brain mapping will be performed before and after 12 weeks focusing on glutamate and neuromelanin in predefined regions. Regional glutamate levels will be probed with proton magnetic resonance spectroscopy (MRS), while neuromelanin signal will be mapped with neuromelanin-sensitive magnetic resonance imaging (MRI). We will also perform structural and diffusion weighted, whole-brain MRI. MRS and MRI will be performed at an ultra-high field strength (7 Tesla). Alongside, participants undergo clinical and neuropsychological assessments. Twenty matched healthy controls will undergo similar baseline- and 12-week examinations, but without receiving treatment.
Outcome Measures: The primary endpoint is negative symptom severity. Secondary outcomes comprise: (i) clinical endpoints related to cognition, psychotic symptoms, side effects, and (ii) neurobiological endpoints related to regional glutamate- and neuromelanin levels, and structural brain changes.
Anticipated Results: We hypothesize that add-on memantine to amisulpride will be superior to amisulpride monotherapy in reducing negative symptoms, and that this effect will correlate with thalamic glutamate levels. Moreover, we anticipate that add-on memantine will restore regional white matter integrity and improve cognitive functioning.
Perspectives: By combining two licensed, off-patent drugs, AMEND aims to optimize treatment of psychosis while investigating the memantine response. Alongside, AMEND will provide neurobiological insights to effects of dual receptor modulation, which may enable future stratification of patients with first-episode psychosis before initial antipsychotic treatment.
Clinical Trial Registration: [ClinicalTrials.gov], identifier [NCT04789915].
Antipsychotic medication (AP) is primarily effective in treating positive psychotic symptoms such as delusions, hallucinations, and disorganized thinking, which are cardinal symptoms of schizophrenia. However, AP does not ameliorate the accompanying negative symptoms (e.g., anhedonia, avolition, and social withdrawal), and cognitive deficits, which are highly disabling and predictive of patients’ long-term prognosis (1–3). Persistent negative symptoms have also shown to be a critical predictor for future treatment resistance (4). A growing body of evidence support that a shortening of the interval between onset of psychosis and initiation of an efficient intervention lead to better long-term outcome (5–7).
The pathophysiology of psychosis is complex and involves multiple neurotransmitters, e.g., serotoninergic- (8), GABAergic, and glutamatergic (9) systems. Nevertheless, modulation (particularly antagonism) of striatal dopamine D2 receptors (D2R) remain the key common denominator of all licensed antipsychotics (10). Even so, around 30% of patients with psychosis display inadequate response to antidopaminergic treatment (11, 12). Mounting evidence from post- mortem-, brain imaging-, genetic-, and pharmacologic challenge studies indicate glutamatergic dysregulation, specifically of the N-methyl-D-aspartate receptor (NMDAR), as part of the pathophysiology of psychosis and schizophrenia (13–15). Through excitotoxicity, glutamate dysregulation may underlie structural degeneration, e.g., in hippocampus, which is a key finding in patients with schizophrenia (16–19).
Using 3T magnetic resonance spectroscopy (MRS), we recently reported increased thalamic glutamate levels in antipsychotic-naïve patients with first episode psychosis (FEP) compared to healthy controls (HC). Importantly, high thalamic glutamate levels predicted poor treatment response (9). Other studies have also associated glutamate levels with treatment outcome (20–22). Nevertheless, cross-sectional studies of glutamate levels between patients with FEP and HC have shown inconsistent results, (21, 23, 24) likely reflecting differences in glutamate levels across brain regions and in patients’ variable previous antipsychotic exposure, as well as the complexity of the disorder, with individual differences regarding the neurobiological findings Studies have also shown that thalamic glutamate levels are heritable, genetically related to psychosis (25), and that in individuals at ultra-high risk of psychosis (UHR), thalamic glutamate levels are related to attention and level of functioning (26, 27). Moreover, we previously demonstrated that thalamic and anterior cingulate cortex (ACC) levels of glutamate are associated with symptomology and cognition, specifically spatial working memory, set-shifting and sustained attention both in UHR and FEP (9, 26, 28, 29).
Cutting-edge 7T MRS can non-invasively determine brain metabolite levels of e.g., γ-aminobutyric acid (GABA), N-acetylaspartate, N-acetylaspartyl and importantly, 7T allows for discrimination of glutamate concentrations from glutathione and glutamine (22, 30, 31). Moreover, multiple voxels/brain regions can be investigated with 7T. In the context of glutamate and psychosis, the thalamus, ACC, hippocampus, dorsolateral prefrontal cortex (DLPFC), and basal ganglia are of particular interest, e.g., (17, 29, 32–34).
Regarding brain structure, the use of structural 7T sequences offers increased sensitivity to quantify neurodegenerative processes such as volume loss e.g., by hippocampal subfield segmentation (35).
Also, high-resolution quantification of tissue parameters such as iron deposition using quantitative susceptibility mapping allow characterization of subtle changes in the “dopaminergic regions” of the basal ganglia, including striatum, pallidum, and substantia nigra (SN) (35). Recently, a promising non-invasive method for in vivo-investigating dopamine in neuropsychiatric illness has been developed. Neuromelanin-sensitive MRI (NM-MRI) purports to detect the content of neuromelanin (NM), a product of dopamine metabolism that accumulates in the SN. NM may be regarded as a proxy of structural and functional integrity of dopaminergic cells in SN (36). Findings indicate that NM-MRI signals correlate with NM concentration, dopamine levels in the striatum and severity of psychosis in schizophrenia, even without neurodegeneration (37).
NMDA-receptor modulation has been investigated in several preclinical studies (38–40). Interestingly, different NMDA-receptor compounds lead to various effects on molecular, anatomical, and behavioral levels. Specifically, memantine exerts opposite effects than ketamine on the genetic level, which may underlie the two drugs’ different clinical effects (38, 41).
Against this background, modulation of glutamatergic NMDAR has been investigated as a potential treatment target in patients with schizophrenia or other psychotic disorders. Memantine is a non-competitive NMDAR antagonist used for treatment of Alzheimer’s disease. Two recent meta-analyses (42, 43) and one systematic review (44) have concluded that adjunctive memantine to antipsychotics is safe and significantly improves negative symptoms in chronic medicated patients with schizophrenia. One of the meta-analyses also indicated a potential beneficial effect on global levels of cognition of patients treated with adjunctive memantine compared to the placebo group (42).
Memantine has been theorized to ameliorate progression of negative symptoms by counteracting excitotoxicity correlated to high glutamate levels in early stages of psychosis (45), but this has not yet been investigated in initially antipsychotic-naïve patients.
AMEND is an ongoing double-blinded clinical trial (Clinicaltrials.gov, ID: NCT04789915), where antipsychotic-naïve patients with first-episode psychosis will be randomly allocated to treatment with first-line antipsychotic compound with addition of memantine or placebo. Patients will be matched with HCs and all participants will undergo baseline and 12-weeks examinations (Figure 1).
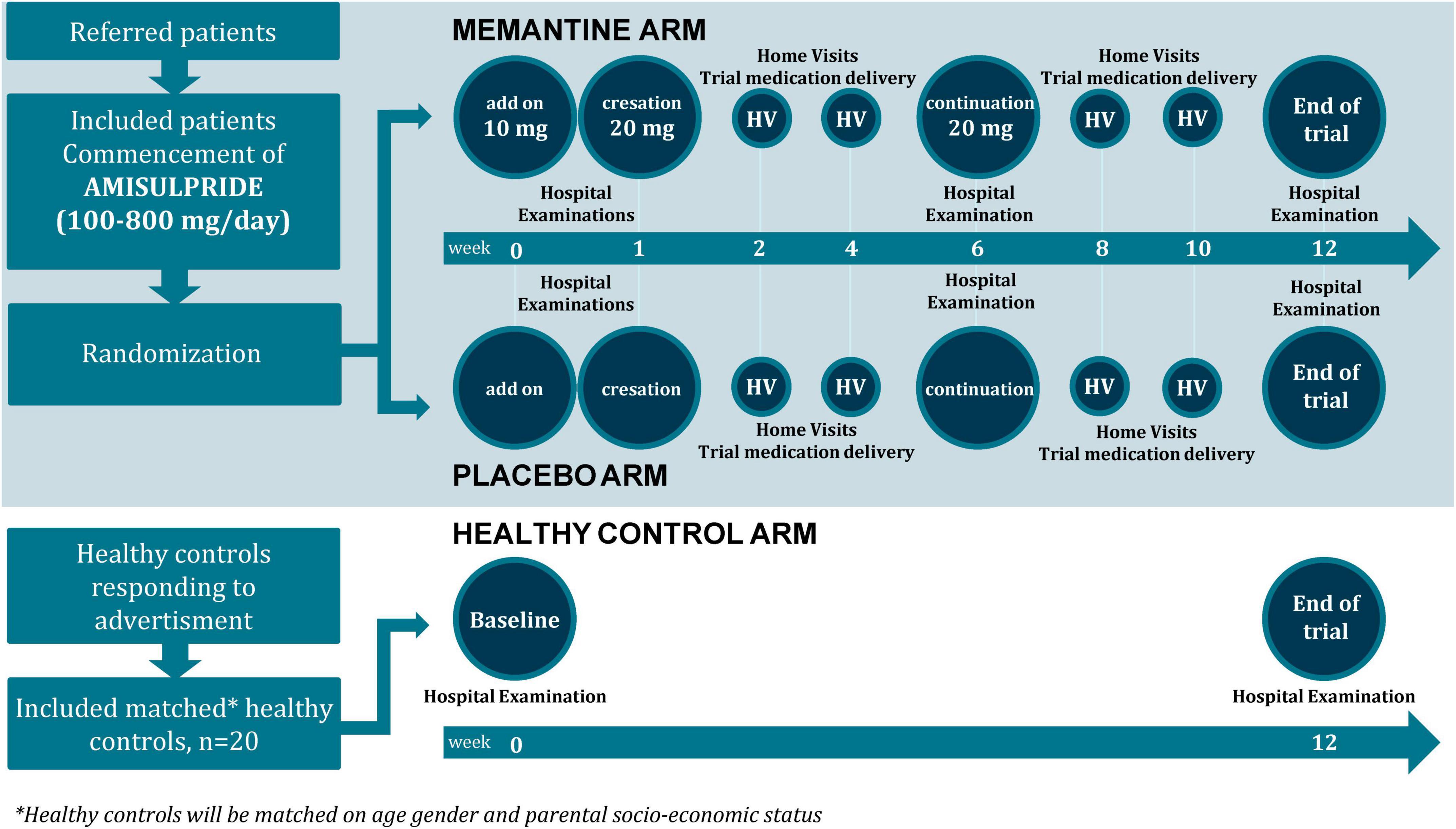
Figure 1. AMEND flow chart.
We hypothesize that add-on memantine to amisulpride will be superior to amisulpride monotherapy in reducing negative symptoms, and that this effect will correlate with thalamic glutamate levels. Moreover, we anticipate that add-on memantine will restore regional white matter integrity and improve cognitive functioning.
Double-blinded randomized controlled trial (RCT). Phase I, known medicine (memantine) tested for new indication (treatment of negative symptoms in psychosis).
We will include antipsychotic-naïve people with schizophrenia spectrum first-episode psychosis. Patients will be recruited from psychiatric hospitals and outpatient psychiatric centers in the Capital Region and in Region Zealand of Denmark. Doctor or nursing staff will inform potentially relevant patients about the project, and if he/she accepts, contact the AMEND project medical doctor. Present State Examination (PSE), will be performed by the project medical doctor, to confirm a psychosis diagnosis. Included ICD-10 diagnosis are shown in Table 1. In conjunction, a global evaluation as per general clinical practice will be performed to assess whether antipsychotic treatment is indicated. Patients will be evaluated in cooperation with a senior consultant psychiatrist. Furthermore, a brief somatic and neurological examination, as well as screening for pregnancy and substance abuse, will be performed.
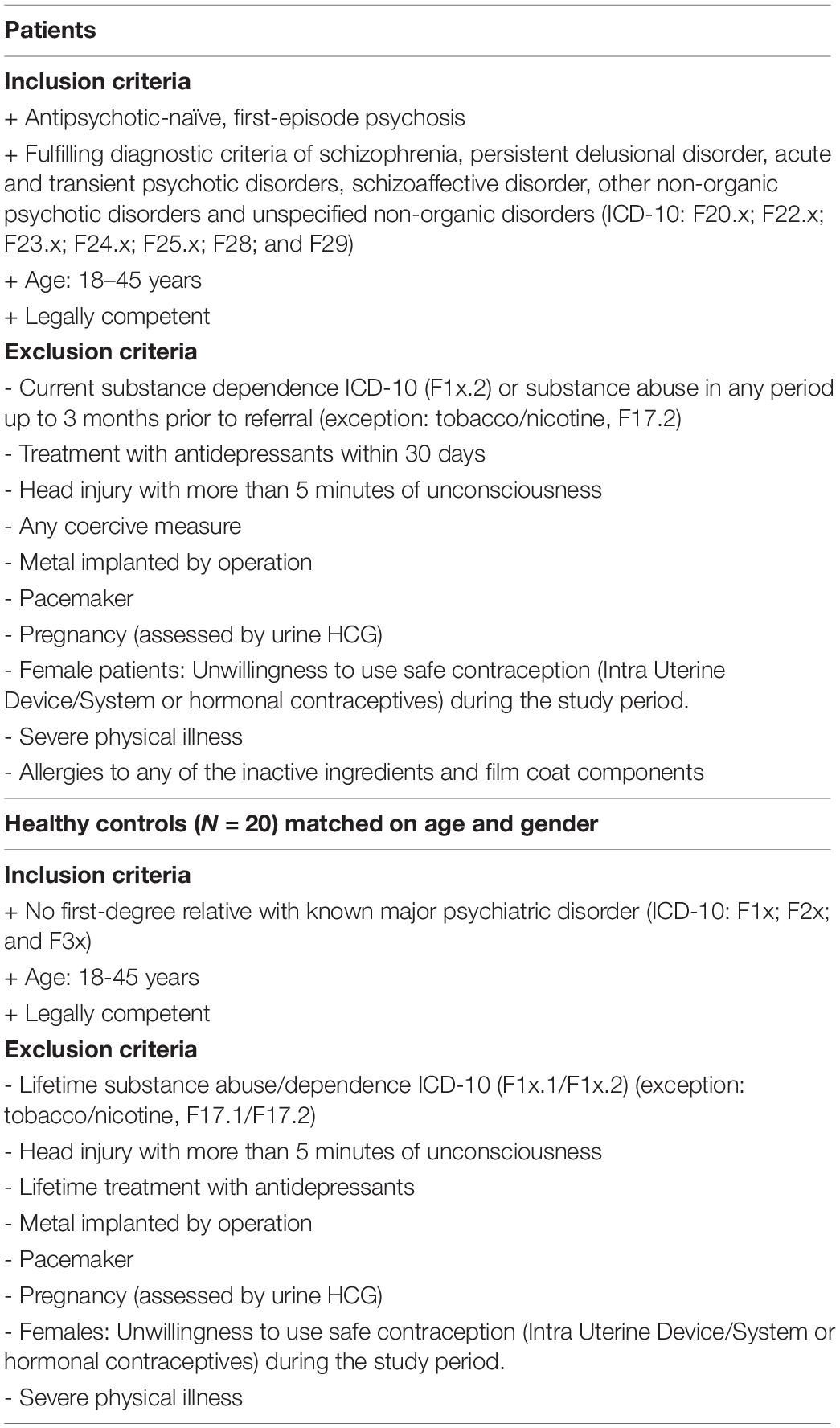
Table 1. In- and exclusion criteria in AMEND.
Patients will receive no economical compensation for participation as remuneration is not allowed according to Danish regulations. The medication will be provided free of charge and transportations costs will be covered.
Twenty healthy controls (HC) matched 1:2 on age, sex, ethnicity and parental socioeconomic status will be recruited through online advertisement per website.1 Healthy controls will receive a taxable disadvantage allowance of DKK 1,000 for completion of the baseline visit and DKK 2,000 for the end of trial visit.
In- and exclusion criteria are shown in Table 1.
At baseline in the antipsychotic-naïve state as well as after 12 weeks of treatment, patients will undergo detailed examination program including: (1) clinical ratings and assessments, (2) neurocognitive testing, and (3) Magnetic Resonance Imaging (MRI) scans. Between week 0 and week 12 regular clinical examinations will be undertaken, see examination program Table 2.
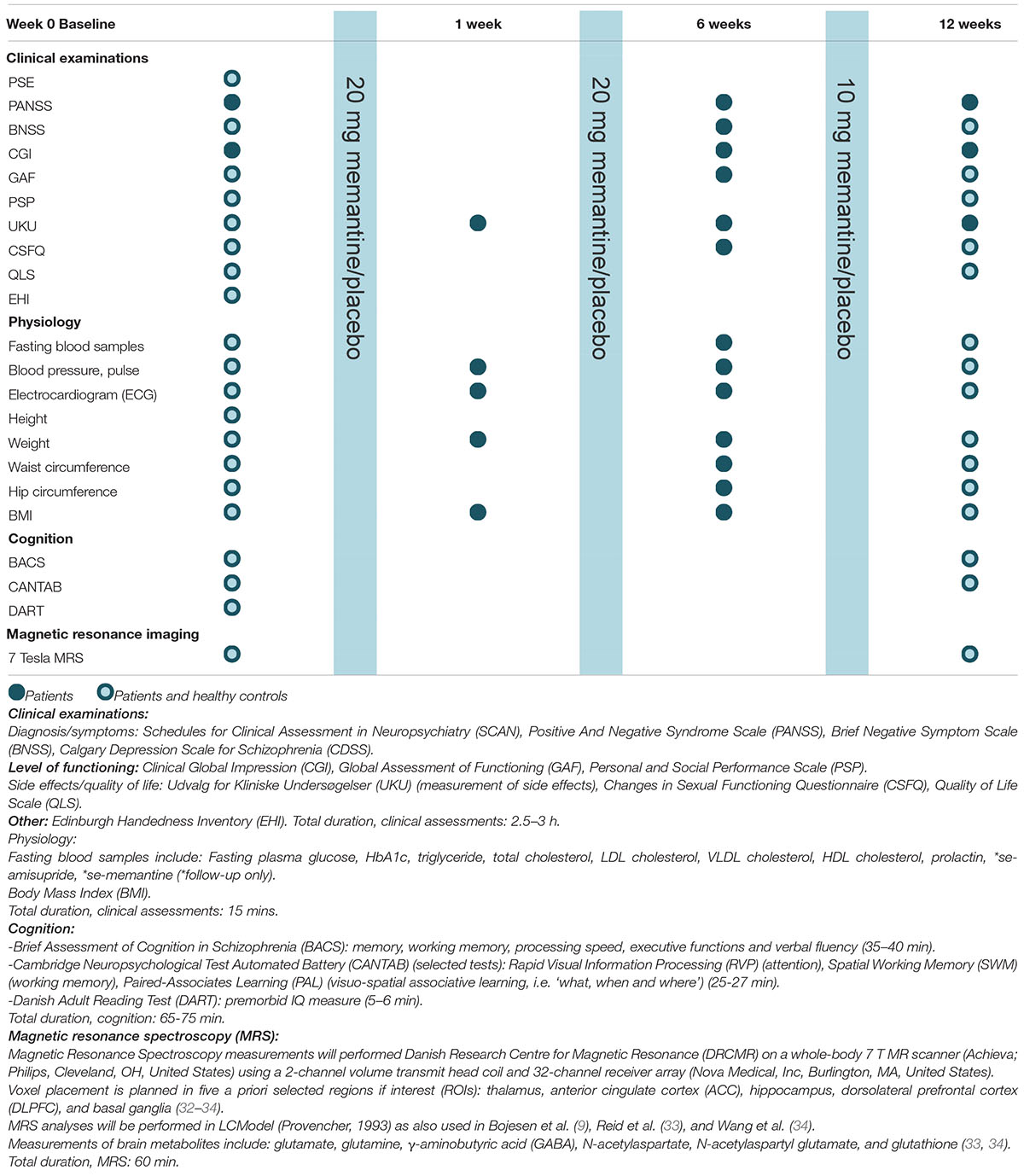
Table 2. AMEND examination program.
Symptom severity will be assessed by the Positive and Negative Syndrome Scale (PANSS) (46). Moreover, the primary clinical endpoint, PANSS negative symptoms, will be supplemented by the Brief Negative Symptom Scale (BNSS) (47). As descriptive and explorative endpoints, quality of life will be evaluated using the Quality of Life Scale (QLS) (48). The UKU side effect rating scale (49) and Changes in Sexual Functioning Questionnaire (CSFQ) (50) will be used to asses potential side-effects. Handedness will be assessed with Edinburgh Handedness Inventory (EHI) (51). Level of functioning will be evaluated with the Personal and Social Performance Scale (PSP) (52), and Global Assessment of Functioning (GAF) (53). The Clinical Global Impression (CGI) (54) will be used to assess the patients’ overall illness severity.
Based on previous studies in similar patient populations we expect the mean PANSS negative symptom score to reside around 20, eg. (9, 55) and in order to enhance generalizability to this patient population, we did not set a minimal level of symptoms.
In order to retain comparability to other studies, e.g.,(42–44) we opted for PANSS. To address the controversy regarding of PANSS negative symptoms, we employ BNSS as secondary endpoint. We recently validated BNSS for use in Danish settings (56, 57).
Specific cognitive functions will be examined using selected tasks from The Cambridge Neuropsychological Test Automated Battery (CANTAB) (58–60) and The Brief Assessment of Cognition in Schizophrenia (BACS) (61, 62). Both batteries are well validated and have previously been applied in patients with schizophrenia, e.g., (26, 63–68).
From CANTAB we will include Spatial Working Memory (SWM) to assess visual working memory, Paired Associated Learning (PAL) to assess visual learning, and Rapid Visual Information Processing (RVP) to assess sustained attention. BACS will be used to assess verbal learning, verbal working memory, processing speed, planning and verbal fluency. Finally, premorbid intelligence (IQ) will be estimated using the Danish version of the National Adult Reading Test (DART) (69) (adapted from the National Adult Reading Test, NART) (70).
Magnetic resonance imaging scans will be performed at the Danish Research Centre for Magnetic Resonance (DRCMR), Copenhagen University Hospital Amager and Hvidovre, on a whole-body 7 Tesla (7T) MR scanner (Achieva; Philips, Cleveland, OH, United States) using a 2-channel volume transmit head-coil and 32-channel receiver array (Nova Medical, Inc., Burlington, MA, United States). MRS will be used to assess glutamate levels pre – and post treatment in five preselected regions of interest: anterior cingulate cortex (ACC), dorsolateral prefrontal cortex (DLPFC), thalamus, hippocampus, and the basal ganglia. In addition, T1- and T2 weighted structural images and diffusion sensitive sequences will be performed to explore cortical and subcortical brain structures, and the integrity of white matter tracts. Quantitative Susceptibility Mapping (QSM) will be used to estimate regional iron accumulation, and measurement of the neuromelanin (NM) concentration will be performed in substantia nigra (SN) as a proxy for structural and functional integrity of dopaminergic cells (36).
Our group has established a robust 7T protocol for glutamate MRS at our 7T MR system and validated the protocol in a cohort on healthy individuals in a study on normal cognitive aging (71, 72).
We will apply this optimized MR protocol in the AMEND study on a Philips 7T whole body MR scanner (Philips) using a dual transmit coil and a 32-channel receive head coil (NovaMedical). We will use a sLASER sequence (73) with a TR/TE = 3700/32 ms, bandwidth = 4 kHz, data points = 2048) with prospective frequency and motion correction.
For structural MRI, we will use a tailored acquisition protocol which we have successfully applied to map the SN and LC at high resolution and signal-to-noise ratio in a cohort of patients with Parkinson’s disease and age-matched controls. The neuroimaging results regarding the Locus coeruleus have been recently published (74). In addition to locus coeruleus mapping, this structural 7T MR protocol also provides exquisite high-resolution maps of the substantia nigra (unpublished data). In short, the structural MRI protocol includes a T1-weighted(T1w), high-resolution (1-mm isotropic) and a magnetization transfer weighted, three-dimensional, high-resolution (voxel size, 0.4 × 0.4 × 1.0 mm) ultra-fast gradient echo sequence (echo time/repetition time = 4.1/8.1 ms, flip angle = 7 degrees, two averages). Magnetization transfer saturation will be achieved by applying 16 block-shaped pre-pulses at a frequency offset of 2 kHz (flip angle = 278 degrees, duration = 10 ms). We will also acquire T1-weighted images with identical acquisition parameters for co-registration purposes, but with a zero-degree flip angle for the off-resonance pre-pulse.
Tablet amisulpride is a second-generation antipsychotic and a first-line, generic drug against psychosis and schizophrenia in Denmark (75). Amisulpride primarily binds to dopamine D2 and D3 receptors, but also has affinity for serotonin 5-HT7 receptors (76). In AMEND, amisulpride is used as “tool compound” because it is the most selective licensed antidopaminergic compound to treat psychosis. All patients will be treated with tablet amisulpride with initial dose 50–100 mg/day. Doses will be slowly augmented according to effect and side-effects to a maximum of 800 mg/day.
Tablet memantine is approved for treatment of Alzheimer’s Disease (AD) showing benefits on the main domains of AD i.e.,. cognition, function, behavior, and clinical global change (77). Memantine acts through uncompetitive, open-channel NMDAR antagonism, and has minimal activity for GABAergic, dopaminergic, adrenergic, histaminergic, and glycinergic receptors.
Patients will be blindly randomized to treatment with either memantine or placebo. Treatment will be initiated at 10 mg/day for 1 week, and from the second week the dose will be increased to 20 mg/day until end of trial. Tablets will be identical, provided in 10 mg or 20 mg tablets, and labeled by the Hospital Pharmacy (Region Hovedstadens Apotek) according to GCP-guidelines; marked with trial reference number, trial subject reference, dosage, administration route, storage and expiration date.
The Hospital Pharmacy will be responsible for randomization, which will be conducted 1:1. Randomization will be stratified by PANSS negative sub-score, categorizing patients in either [Low PANSS negative baseline <20] or [High PANSS negative baseline ≥20].
The randomization will use permuted blocs in sizes of 4,6 and 8 to ensure an even distribution among the two groups. The number of patients in each group will not be restricted. In need of unblinding of a patient’s treatment, the pharmacy can be contacted at any time.
Intolerable side-effects or clinical worsening (defined as a 20% increase in PANSS positive subscale score compared to baseline PANSS positive score) will result in discontinuation of study treatment and study exclusion. Patients will be consulted with the senior consultant psychiatrist associated to the research project and further treatment will be initiated according to general treatment guidelines respecting the patients’ autonomy and requests.
All tablets are provided to patients free of charge. Tablets will be administered with regular time intervals by a research nurse at the hospital or at home visits (Figure 1). Compliance will be assessed biweekly by phone-call or at clinical visits, where patients are asked how many days, if any, medication was not taken. Serum-amisulpride and serum-memantine will be measured by blood samples taken at the research department at 6 weeks and at end of treatment.
The primary endpoint will be reduction in negative symptoms as measured with the negative symptom score from the Positive and Negative Syndrome Scale (PANSS) (78). Reduction in negative symptoms after 12 weeks of treatment: [PANSS negative baseline–PANSS negative at week 12]. PANSS negative assessments will be supplemented by Brief Negative Symptom Scale (BNSS) scores (57).
Secondary endpoints include changes in cognition (in particular working memory, learning and processing speed, and sustained attention), PANSS positive and total-scores, other clinical measures, level of functioning, adverse effects, and glutamate levels in the five a priori selected regions of interest mentioned above. Additionally, dopamine function in substantia nigra will be explored using NM-MRI techniques (37).
Exploratory endpoints include associations between clinical data, quality of life, brain metabolites in other regions, e.g., ACC (33, 34), structural measures (e.g., hippocampus subfields) (35), diffusion data, and basal ganglia quantification (Table 2). Interactions between baseline brain metabolite levels and brain structure and white matter integrity in patients and HC will also be investigated.
Homogeneity of variance between the two groups will be assessed using Levene’s test. Parametric data will be evaluated using parametric testing. Non-normally distributed data or data that exhibit unequal variances will be tested using non-parametric tests as appropriate. Fisher’s or χ2 exact tests will be used for group comparisons between categorical data. The Benjamini-Hochberg procedure will be used to control the type I error rate.
Data analyses on the primary outcome and most of the secondary outcomes will be performed before un-blinding and according to the per-protocol principle. Analyses of adverse events will be performed according to the intention-to-treat principle. Demographic variables and clinical characteristics will be reported in frequency for categorical data, and in mean values (with standard deviations and range) for normally distributed, continuous variables. Group comparisons for demographic data will be performed using independent t-tests for continuous variables and Chi-square tests for nominal and ordinal variables. Primary and secondary outcomes will be tested using repeated measures (rm)ANOVA.
The power calculation is based on the primary outcome. We used the most representative clinical study we could identify and attempted to modify to the current setting. An 8-week RCT using risperidone plus memantine in stable schizophrenia patients (N = 40) reported a reduction in PANSS negative of −2.8 (SD 1.6) with memantine compared to −0.8 (SD 0.9) with placebo (79). Assuming a similar response, we expect add-on memantine to induce −2 ± 2 point more reduction in PANSS negative compared to amisulpride monotherapy. An a priori Student t-test (two-sided) with significance level α of 0.05 and a desired power (1-α) of 80%, shows that 16 completed patients in each arm is needed.
To increase power of secondary analyses, enrollment will continue until 18 participants in each arm have completed examinations. Moreover, AMEND will be extended to 12 weeks based on the median trial duration in the meta-analysis of add-on memantine [12 weeks (mean 11.5 weeks)] (42). Based on our center’s 20 years of experience with recruitment and treatment of antipsychotic-naïve patients, we expect an inclusion rate of 2 patients per month and an attrition rate of 25%. Thus, recruitment of 46 patients will take approximately 2 years.
By rational combination of two licensed, off-patent drugs, amisulpride and memantine, AMEND aims to optimize treatment of psychosis, especially the accompanying negative and cognitive symptoms, alongside with unraveling the signature of memantine response. If successful, AMEND will provide pivotal neurobiological evidence for future stratification of patients with first-episode psychosis before initial antipsychotic treatment.
There are few potential risks related to participating in the AMEND study. Side effects of memantine are relatively mild compared to antipsychotic medication. In previous memantine add-on RCTs in schizophrenia patients, the reported side effects did not differ from placebo (42) and chronic patients treated with memantine as add-on treatment had an improvement compared to placebo (79), why we assume that the added treatment also will improve patients with first-episode psychosis. The participants will have the advantages of a thorough examination program with more detailed psychopathological and neuropsychological testing than normally provided.
Magnetic resonance imaging procedures have not been associated with any health risk, however, the examination might cause discomfort for people with claustrophobia and anxiety. Participants will be followed carefully during the project and any potential discomfort will be attempted minimized by research staff. Great care will be taken by the research group to ensure that all examinations are carried out as smoothly and efficiently as possible, including breaks when needed. Scanning will be discontinued in cases of discomfort or anxiety, and communication between staff and participants will be possible during the whole scan.
Participants with head/neck tattoos or permanent make-up might experience warming and soreness of the painted area, and scanning will be interrupted should these symptoms arise. Incidental findings on MRI scans might lead to worrying and further clinical work-up. Blood samplings might cause discomfort for some people but will be taken by trained personal and under hygienic circumstances.
Participants can withdraw from the study at any time without explanation, and without any consequences for the following treatment.
Regarding the statistics, our power calculation and number of participants are not sized for all exploratory analyses, but our RCT design and previous pilot data, justify the rationale for conducting these tests. Admittedly, a mean 2-point reduction in PANSS negative symptoms may only represent a modest clinical improvement for the individual patient participating in this study. However, the RCT design in combination with 7T MRS data will provide strong neuroscientific evidence on how NMDARs may mediate effects on unresolved symptom domains. If successful, the combined clinical and neurobiological insights from AMEND will provide an important steppingstone, which will have major impact for further research, for stakeholders in the pharmaceutical industry, and for future patients with psychosis.
With the ambitious goal of moving clinical psychiatry toward pre-treatment stratification based on pathophysiological markers, AMEND will provide evidence for rational drug repurposing to optimize treatment outcome for patients with psychosis.
The trial has been approved by the Danish Health and Medicines Authority, the National Committee on Health Research Ethics, Danish National Committee on Biomedical Research, and the Danish Data Protection Agency. Trial participation presupposes oral and written informed consent of all participants. Memantine will be used off-label, and tolerability and clinical symptoms will be monitored closely. Personal integrity and privacy concerning participants will be protected by the Danish Law of Health. The study will be conducted in accordance with the Helsinki Declaration II and monitored according to Good Clinical Practice principles (ICH-GCP). AMEND is registered at EudraCT nr: 2021-001061-20 and ClinicalTrials.gov (NCT04789915). The trial can be subjected to quality audit. Research data and results (positive and negative), will be presented at national and international scientific meetings and conferences. Articles will be submitted to peer-reviewed journals. Authorships will adhere to the International Committee of Medical Journal Editors statement (ICMJE).2
The studies involving human participants were reviewed and approved by Danish Health and Medicines Authority, the National Committee on Health Research Ethics, Danish National Committee on Biomedical Research, and the Danish Data Protection Agency. The patients/participants provided their written informed consent to participate in this study.
BE conceived the study. KB, MN, BF, BG, and HS contributed to the study design was adjusted in discussions. AM, CL, VB, HL, DS, MS, AL, WS, and CP refined the clinical- and neuropsychiatric examination programs with respect to their respective fields of expertise. KS, OB, and BE drafted the manuscript. All authors approved the submitted version of the manuscript.
This AMEND study was financed by Lundbeck Foundation Ascending Investigator grant, Journal nr. R344-2020-931; DKK 4,999,812/4 years (Granted to sponsor, BE). The sponsor has previously received grants from the Lundbeck Foundation.
BE was part of the Advisory Board of Eli Lilly Denmark A/S, Janssen-Cilag, Lundbeck Pharma A/S, and Takeda Pharmaceutical Company Ltd; and has received lecture fees from Bristol-Myers Squibb, Boehringer Ingelheim, Otsuka Pharma Scandinavia AB, Eli Lilly Company, and Lundbeck Pharma A/S. HS has received honoraria as speaker from Sanofi Genzyme, Denmark and Novartis, Denmark, as consultant from Sanofi Genzyme, Denmark, and Lundbeck AS, Denmark, and as editor-in-chief (Neuroimage Clinical) and senior editor (NeuroImage) from Elsevier Publishers, Amsterdam, The Netherlands. He has received royalties as book editor from Springer Publishers, Stuttgart, Germany and from Gyldendal Publishers, Copenhagen, Denmark.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Demjaha A, Lappin JM, Stahl D, Patel MX, MacCabe JH, Howes OD, et al. Antipsychotic treatment resistance in first-episode psychosis: prevalence, subtypes and predictors. Psychol Med. (2017) 47:1981–9. doi: 10.1017/S0033291717000435
2. Halverson TF, Orleans-Pobee M, Merritt C, Sheeran P, Fett AK, Penn DL. Pathways to functional outcomes in schizophrenia spectrum disorders: meta-analysis of social cognitive and neurocognitive predictors. Neurosci Biobehav Rev. (2019) 105:212–9. doi: 10.1016/j.neubiorev.2019.07.020
3. Bowie CR, Reichenberg A, Patterson TL, Heaton RK, Harvey PD. Determinants of real-world functional performance in schizophrenia subjects: correlations with cognition, functional capacity, and symptoms. Am J Psychiatry. (2006) 163:418–25. doi: 10.1176/appi.ajp.163.3.418
4. Bucci P, Mucci A, van Rossum IW, Aiello C, Arango C, Baandrup L, et al. Persistent negative symptoms in recent-onset psychosis: relationship to treatment response and psychosocial functioning. Eur Neuropsychopharmacol. (2020) 34:76–86. doi: 10.1016/j.euroneuro.2020.03.010
5. Correll CU, Galling B, Pawar A, Krivko A, Bonetto C, Ruggeri M, et al. Comparison of early intervention services vs. treatment as usual for early-phase psychosis a systematic review, meta-analysis, and meta-regression supplemental content. JAMA Psychiatry. (2018) 75:555–65. doi: 10.1001/jamapsychiatry.2018.0623
6. Samara MT, Leucht C, Leeflang MM, Anghelescu IG, Chung YC, Crespo-Facorro B, et al. Early improvement as a predictor of later response to antipsychotics in schizophrenia: a diagnostic test review. Am J Psychiatry. (2015) 172:617–29. doi: 10.1176/appi.ajp.2015.14101329
7. Albert N, Madsen T, Nordentoft M. Early intervention service for young people with psychosis: saving young lives. JAMA Psychiatry. (2018) 75:427–8. doi: 10.1001/jamapsychiatry.2018.0662
8. Rasmussen H, Erritzoe D, Andersen R, Ebdrup BH, Aggernaes B, Oranje B, et al. Decreased frontal Serotonin2A receptor binding in antipsychotic-naive patients with first-episode schizophrenia. Arch Gen Psychiatry. (2010) 67:9. doi: 10.1001/archgenpsychiatry.2009.176
9. Bojesen KB, Ebdrup BH, Jessen K, Sigvard A, Tangmose K, Edden RAE, et al. Treatment response after 6 and 26 weeks is related to baseline glutamate and GABA levels in antipsychotic-naïve patients with psychosis. Psychol Med. (2019) 50:2182–93. doi: 10.1017/S0033291719002277
10. McCutcheon RA, Abi-Dargham A, Howes OD. Schizophrenia, dopamine and the striatum: from biology to symptoms. Trends Neurosci. (2019) 42:205–20. doi: 10.1016/j.tins.2018.12.004
11. Howes OD, McCutcheon R, Agid O, de Bartolomeis A, van Beveren NJM, Birnbaum ML, et al. Treatment-resistant schizophrenia: treatment response and resistance in psychosis (trrip) working group consensus guidelines on diagnosis and terminology. Am J Psychiatry. (2017) 174:216–29. doi: 10.1176/appi.ajp.2016.16050503
12. Jankowska A, Satała G, Partyka A, Wesołowska A, Bojarski AJ, Pawłowski M, et al. Discovery and development of non-dopaminergic agents for the treatment of schizophrenia: overview of the preclinical and early clinical studies. Curr Med Chem. (2019) 26:4885–913. doi: 10.2174/0929867326666190710172002
13. Reddy-Thootkur M, Kraguljac NV, Lahti AC. The role of glutamate and GABA in cognitive dysfunction in schizophrenia and mood disorders – a systematic review of magnetic resonance spectroscopy studies. Schizophr Res. (2020) S0920-9964(20)30077-3. doi: 10.1016/j.schres.2020.02.001
14. Uno Y, Coyle JT. Glutamate hypothesis in schizophrenia. Psychiatry Clin Neurosci. (2019) 73:204–15.
15. Nicoletti F, Orlando R, Di Menna L, Cannella M, Notartomaso S, Mascio G, et al. Targeting mGlu receptors for optimization of antipsychotic activity and disease-modifying effect in schizophrenia. Front Psychiatry. (2019) 10:49. doi: 10.3389/fpsyt.2019.00049
16. Modinos G, Egerton A, McLaughlin A, McMullen K, Kumari V, Lythgoe DJ, et al. Neuroanatomical changes in people with high schizotypy: relationship to glutamate levels. Psychol Med. (2018) 48:1880–9. doi: 10.1017/S0033291717003403
17. Nenadic I, Maitra R, Basu S, Dietzek M, Schönfeld N, Lorenz C, et al. Associations of hippocampal metabolism and regional brain grey matter in neuroleptic-naïve ultra-high-risk subjects and first-episode schizophrenia. Eur Neuropsychopharmacol. (2015) 25:1661–8. doi: 10.1016/j.euroneuro.2015.05.005
18. Haijma SV, Van Haren N, Cahn W, Cédric P, Koolschijn MP, Hulshoff Pol HE, et al. Brain volumes in schizophrenia: a meta-analysis in over 18 000 subjects. Schizophr Bull. (2013) 39:1129–38. doi: 10.1093/schbul/sbs118
19. van Erp TGM, Hibar DP, Rasmussen JM, Glahn DC, Pearlson GD, Andreassen OA, et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol Psychiatry. (2016) 21:547–53. doi: 10.1038/mp.2015.63
20. Howes OD, Kapur S. A neurobiological hypothesis for the classification of schizophrenia: type A (hyperdopaminergic) and type B (normodopaminergic). Br J Psychiatry. (2014) 205:1–3. doi: 10.1192/bjp.bp.113.138578
21. Egerton A, Broberg BV, Van Haren N, Merritt K, Barker GJ, Lythgoe DJ, et al. Response to initial antipsychotic treatment in first episode psychosis is related to anterior cingulate glutamate levels: a multicentre 1 H-MRS study (OPTiMiSE). Mol Psychiatry. (2018) 23:2145–55. doi: 10.1038/s41380-018-0082-9
22. Dempster K, Jeon P, MacKinley M, Williamson P, Théberge J, Palaniyappan L. Early treatment response in first episode psychosis: a 7-T magnetic resonance spectroscopic study of glutathione and glutamate. Mol Psychiatry. (2020) 25:1640–50. doi: 10.1038/s41380-020-0704-x
23. Birur B, Kraguljac NV, VerHoef L, Morgan CJ, Jindal RD, Reid MA, et al. Neurometabolic correlates of 6 and 16 weeks of treatment with risperidone in medication-naive first-episode psychosis patients. Transl Psychiatry. (2020) 10:15. doi: 10.1038/s41398-020-0700-6
24. Roberts RC, McCollum LA, Schoonover KE, Mabry SJ, Roche JK, Lahti AC. Ultrastructural evidence for glutamatergic dysregulation in schizophrenia. Schizophr Res. (2020) S0920-9964(20)30032-3. doi: 10.1016/j.schres.2020.01.016
25. Legind CS, Broberg BV, Brouwer R, Mandl RCW, Ebdrup BH, Anhøj SJ, et al. Heritability of cerebral blood flow and the correlation to schizophrenia spectrum disorders: a pseudo-continuous arterial spin labeling twin study. Schizophr Bull. (2019) 45:1231–41. doi: 10.1093/schbul/sbz007
26. Bojesen KB, Broberg BV, Fagerlund B, Jessen K, Thomas MB, Sigvard A, et al. Associations between cognitive function and levels of glutamatergic metabolites and gamma-aminobutyric acid in antipsychotic-naïve patients with schizophrenia or psychosis. Biol Psychiatry. (2021) 89:278–87. doi: 10.1016/j.biopsych.2020.06.027
27. Wenneberg C, Nordentoft M, Rostrup E, Glenthøj LB, Bojesen KB, Fagerlund B, et al. Cerebral glutamate and gamma-aminobutyric acid levels in individuals at ultra-high risk for psychosis and the association with clinical symptoms and cognition. Biol Psychiatry Cogn Neurosci Neuroimaging. (2020) 5:569–79. doi: 10.1016/j.bpsc.2019.12.005
28. Wenneberg C, Glenthøj BY, Hjorthøj C, Buchardt Zingenberg FJ, Glenthøj LB, Rostrup E, et al. Cerebral glutamate and GABA levels in high-risk of psychosis states: a focused review and meta-analysis of (1)H-MRS studies. Schizophr Res. (2020) 215:38–48. doi: 10.1016/j.schres.2019.10.050
29. Marsman A, van den Heuvel MP, Klomp DW, Kahn RS, Luijten PR, Hulshoff Pol HE. Glutamate in schizophrenia: a focused review and meta-analysis of 1H-MRS studies. Schizophr Bull. (2013) 39:120–9. doi: 10.1093/schbul/sbr069
30. Sydnor VJ, Roalf DR. A meta-analysis of ultra-high field glutamate, glutamine, GABA and glutathione 1HMRS in psychosis: implications for studies of psychosis risk. Schizophr Res. (2020) 226:61–9. doi: 10.1016/j.schres.2020.06.028
31. Godlewska BR, Minichino A, Emir U, Angelescu I, Lennox B, Micunovic M, et al. Brain glutamate concentration in men with early psychosis: a magnetic resonance spectroscopy case-control study at 7 T. Transl Psychiatry. (2021) 11:367. doi: 10.1038/s41398-021-01477-6
32. Boer VO, Andersen M, Lind A, Lee NG, Marsman A, Petersen ET. MR spectroscopy using static higher order shimming with dynamic linear terms (HOS-DLT) for improved water suppression, interleaved MRS-fMRI, and navigator-based motion correction at 7T. Magn Reson Med. (2020) 84:1101–12. doi: 10.1002/mrm.28202
33. Reid MA, Salibi N, White DM, Gawne TJ, Denney TS, Lahti AC. 7T proton magnetic resonance spectroscopy of the anterior cingulate cortex in first-episode schizophrenia. Schizophr Bull. (2019) 45:180–9. doi: 10.1093/schbul/sbx190
34. Wang AM, Pradhan S, Coughlin JM, Trivedi A, Dubois SL, Crawford JL, et al. Assessing brain metabolism with 7-T proton magnetic resonance spectroscopy in patients with first-episode psychosis. JAMA Psychiatry. (2019) 76:314–23. doi: 10.1001/jamapsychiatry.2018.3637
35. Düzel E, Acosta-Cabronero J, Berron D, Biessels GJ, Björkman-Burtscher I, Bottlaender M, et al. European ultrahigh-field imaging network for neurodegenerative diseases (EUFIND). Alzheimers Dement Diagnosis Assess Dis Monit. (2019) 11:538–49. doi: 10.1016/j.dadm.2019.04.010
36. Horga G, Wengler K, Cassidy CM. Neuromelanin-sensitive magnetic resonance imaging as a proxy marker for catecholamine function in psychiatry. JAMA Psychiatry. (2021) 78:788–9. doi: 10.1001/jamapsychiatry.2021.0927
37. Cassidy CM, Zucca FA, Girgis RR, Baker SC, Weinstein JJ, Sharp ME, et al. Neuromelanin-sensitive MRI as a noninvasive proxy measure of dopamine function in the human brain. Proc Natl Acad Sci USA. (2019) 116:5108–17. doi: 10.1073/pnas.1807983116
38. De Bartolomeis A, Sarappa C, Buonaguro EF, Marmo F, Eramo A, Tomasetti C, et al. Different effects of the NMDA receptor antagonists ketamine, MK-801, and memantine on postsynaptic density transcripts and their topography: role of Homer signaling, and implications for novel antipsychotic and pro-cognitive targets in psychosis. Prog Neuropsychopharmacol Biol Psychiatry. (2013) 46:1–12. doi: 10.1016/j.pnpbp.2013.06.010
39. Gilmour G, Pioli EY, Dix SL, Smith JW, Conway MW, Jones WT, et al. Diverse and often opposite behavioural effects of NMDA receptor antagonists in rats: implications for “NMDA antagonist modelling” of schizophrenia. Psychopharmacology (Berl). (2009) 205:203–16. doi: 10.1007/s00213-009-1530-7
40. Okada M, Fukuyama K, Kawano Y, Shiroyama T, Ueda Y. Memantine protects thalamocortical hyper-glutamatergic transmission induced by NMDA receptor antagonism via activation of system xc. Pharmacol Res Perspect. (2019) 7:e00457. doi: 10.1002/prp2.457
41. Johnson JW, Glasgow NG, Povysheva NV. Recent insights into the mode of action of memantine and ketamine. Curr Opin Pharmacol. (2015) 20:54–63. doi: 10.1016/j.coph.2014.11.006
42. Zheng W, Li XH, Yang XH, Cai DB, Ungvari GS, Ng CH, et al. Adjunctive memantine for schizophrenia: a meta-analysis of randomized, double-blind, placebo-controlled trials. Psychol Med. (2018) 48:72–81. doi: 10.1017/S0033291717001271
43. Zheng W, Zhu XM, Zhang QE, Cai DB, Yang XH, Zhou YL, et al. Adjunctive memantine for major mental disorders: a systematic review and meta-analysis of randomized double-blind controlled trials. Schizophr Res. (2019) 209:12–21. doi: 10.1016/j.schres.2019.05.019
44. Di Iorio G, Baroni G, Lorusso M, Montemitro C, Spano MC, Di Giannantonio M. Efficacy of memantine in schizophrenic patients: a systematic review. J Amino Acids. (2017) 2017:7021071. doi: 10.1155/2017/7021071
45. De Bartolomeis A, Sarappa C, Magara S, Iasevoli F. Targeting glutamate system for novel antipsychotic approaches: relevance for residual psychotic symptoms and treatment resistant schizophrenia. Eur J Pharmacol. (2012) 683:1–11. doi: 10.1016/j.ejphar.2012.02.033
46. Kay SR, Opler LA, Lindenmayer JP. The positive and negative syndrome scale (PANSS): rationale and standardisation. Br J Psychiatry Suppl. (1989) 7:59–67. doi: 10.1192/s0007125000291514
47. Kirkpatrick B, Strauss GP, Nguyen L, Fischer BA, Daniel DG, Cienfuegos A, et al. The brief negative symptom scale: psychometric properties. Schizophr Bull. (2011) 37:300–5. doi: 10.1093/schbul/sbq059
48. Heinrichs DW, Hanlon TE, Carpenter WTJ. The quality of life scale: an instrument for rating the schizophrenic deficit syndrome. Schizophr Bull. (1984) 10:388–98. doi: 10.1093/schbul/10.3.388
49. Lingjærde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K. The UKU side effect rating scale. A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand Suppl. (1987) 334:1–100. doi: 10.1111/j.1600-0447.1987.tb10566.x
50. Clayton AH, McGarvey EL, Clavet GJ. The changes in sexual functioning questionnaire (CSFQ): development, reliability, and validity. Psychopharmacol Bull. (1997) 33:731–45.
51. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. (1971) 9:97–113. doi: 10.1016/0028-3932(71)90067-4
52. Nafees B, van Hanswijck de Jonge P, Stull D, Pascoe K, Price M, Clarke A, et al. Reliability and validity of the personal and social performance scale in patients with schizophrenia. Schizophr Res. (2012) 140:71–6. doi: 10.1016/j.schres.2012.06.013
53. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The global assessment scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry. (1976) 33:766–71. doi: 10.1001/archpsyc.1976.01770060086012
54. Guy W. ECDEU Assessment Manual for Psychopharmacology, Revised. US Department of Health, Education, and Welfare Publication (ADM). Rockville, MD: National Institute of Mental Health (1976). p. 76–338.
55. Nielsen MØ, Rostrup E, Broberg BV, Wulff S, Glenthøj B. Negative symptoms and reward disturbances in schizophrenia before and after antipsychotic monotherapy. Clin EEG Neurosci. (2018) 49:36–45. doi: 10.1177/1550059417744120
56. Bzdok D, Meyer-Lindenberg A. Machine learning for precision psychiatry: opportunities and challenges. Biol Psychiatry Cogn Neurosci Neuroimaging. (2018) 3:223–30. doi: 10.1016/j.bpsc.2017.11.007
57. Gehr J, Glenthøj B, Ødegaard Nielsen M. Validation of the Danish version of the brief negative symptom scale. Nord J Psychiatry. (2019) 73:425–32. doi: 10.1080/08039488.2019.1648549
58. Robbins TW, James M, Owen AM, Sahakian BJ, McInnes L, Rabbit P. Cambridge neuropsychological test automated battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dementia. (1994) 5:266–81. doi: 10.1159/000106735
59. Barnett JH, Robbins TW, Leeson VC, Sahakian BJ, Joyce EM, Blackwell AD. Assessing cognitive function in clinical trials of schizophrenia. Neurosci Biobehav Rev. (2010) 34:1161–77. doi: 10.1016/j.neubiorev.2010.01.012
60. Sahakian BJ, Owen AM. Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med. (1992) 85:399–402.
61. Keefe RSE, Harvey PD, Goldberg TE, Gold JM, Walker TM, Kennel C, et al. Norms and standardization of the brief assessment of cognition in schizophrenia (BACS). Schizophr Res. (2008) 102:108–15. doi: 10.1016/j.schres.2008.03.024
62. Keefe RSE, Poe M, Walker TM, Harvey PD. The relationship of the brief assessment of cognition in schizophrenia (BACS) to functional capacity and real-world functional outcome. J Clin Exp Neuropsychol. (2006) 28:260–9. doi: 10.1080/13803390500360539
63. Fagerlund B, Pagsberg AK, Hemmingsen RP. Cognitive deficits and levels of IQ in adolescent onset schizophrenia and other psychotic disorders. Schizophr Res. (2006) 85:30–9. doi: 10.1016/j.schres.2006.03.004
64. Fagerlund B, Pantelis C, Jepsen JRM, Raghava JM, Rostrup E, Jensen MB, et al. Differential effects of age at illness onset on verbal memory functions in antipsychotic-naïve schizophrenia patients aged 12 – 43 years. Psychol Med. (2020) 51:1570–80. doi: 10.1017/S0033291720000409
65. Jepsen JRM, Fagerlund B, Pagsberg AK, Christensen AMR, Nordentoft M, Mortensen EL. Deficient maturation of aspects of attention and executive functions in early onset schizophrenia. Eur Child Adolesc Psychiatry. (2010) 19:773–86. doi: 10.1007/s00787-010-0126-4
66. Lemvigh C, Brouwer R, Pantelis C, Jensen M, Hilker R, Legind C, et al. Heritability of specific cognitive functions and associations with schizophrenia spectrum disorders using CANTAB: a nation-wide twin study. Psychol Med. (2020) 1–14. doi: 10.1017/S0033291720002858
67. Levaux M-N, Potvin S, Sepehry AA, Sablier J, Mendrek A, Stip E. Computerized assessment of cognition in schizophrenia: promises and pitfalls of CANTAB. Eur Psychiatry. (2007) 22:104–15. doi: 10.1016/j.eurpsy.2006.11.004
68. Pantelis C, Wood S, Proffitt T, Testa R, Mahony K, Brewer W, et al. Attentional set-shifting ability in first-episode and established schizophrenia: relationship to working memory. Schizophr Res. (2009) 112:104–13. doi: 10.1016/j.schres.2009.03.039
69. Hjorthoj CR, Vesterager L, Nordentoft M. Test-retest reliability of the Danish adult reading test in patients with comorbid psychosis and cannabis-use disorder. Nord J Psychiatry. (2013) 67:159–63. doi: 10.3109/08039488.2012.691544
70. Nelson HE. National Adult Reading Test (NART): For the Assessment of Premorbid Intelligence in Patients With Dementia: Test Manual. Upton Park: NFER (1982).
71. Younis S, Hougaard A, Christensen CE, Vestergaard MB, Petersen ET, Boer VO, et al. Feasibility of glutamate and GABA detection in pons and thalamus at 3T and 7T by proton magnetic resonance spectroscopy. Front Neurosci. (2020) 14:559314. doi: 10.3389/fnins.2020.559314
72. Lind A, Boraxbekk CJ, Petersen ET, Paulson OB, Siebner HR, Marsman A. Regional myo-inositol, creatine, and choline levels are higher at older age and scale negatively with visuospatial working memory: a cross-sectional proton mr spectroscopy study at 7 tesla on normal cognitive ageing. J Neurosci. (2020) 40:8149–59. doi: 10.1523/JNEUROSCI.2883-19.2020
73. Boer VO, Siero JCW, Hoogduin H, van Gorp JS, Luijten PR, Klomp DWJ. High-field MRS of the human brain at short TE and TR. NMR Biomed. (2011) 24:1081–8. doi: 10.1002/nbm.1660
74. Madelung CF, Meder D, Fuglsang SA, Marques MM, Boer VO, Madsen KH, et al. Locus coeruleus shows a spatial pattern of structural disintegration in Parkinson’s disease. Mov Disord. (2022) 37:479–89. doi: 10.1002/mds.28945
75. Medicinrådet. Medicinrådets Behandlingsvejledning Vedrørende Antipsykotika til Behandling af Psykoiske Tilstande hos Voksne, Version 1.0. Copenhagen: Medicinrådet (2020).
76. Abbas AI, Hedlund PB, Huang X-P, Tran TB, Meltzer HY, Roth BL. Amisulpride is a potent 5-HT7 antagonist: relevance for antidepressant actions in vivo. Psychopharmacology (Berl). (2009) 205:119–28. doi: 10.1007/s00213-009-1521-8
77. Lundbeck BY. NICE Submission of Evidence: Memantine Donepezil, Galantamine, rivastigmine, and Memantine for the Treatment of Alzheimer’s Disease SUBMISSION OF EVIDENCE PREPARED FOR THE NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Ra’anana: NICE (2011).
78. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
79. Rezaei F, Mohammad-Karimi M, Seddighi S, Modabbernia A, Ashrafi M, Salehi B, et al. Memantine add-on to risperidone for treatment of negative symptoms in patients with stable schizophrenia: randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. (2013) 33:336–42. doi: 10.1097/JCP.0b013e31828b50a7
Keywords: antipsychotic-naïve first-episode schizophrenia, memantine, neuromelanin (NM), amisulpride (AMS), magnetic resonace imaging (MRI), magnetic resonance spectrography (MRS), randomized controlled (clinical) trial, glutamate
Citation: Sandström KO, Baltzersen OB, Marsman A, Lemvigh CK, Boer VO, Bojesen KB, Nielsen MØ, Lundell H, Sulaiman DK, Sørensen ME, Fagerlund B, Lahti AC, Syeda WT, Pantelis C, Petersen ET, Glenthøj BY, Siebner HR and Ebdrup BH (2022) Add-On MEmaNtine to Dopamine Antagonism to Improve Negative Symptoms at First Psychosis- the AMEND Trial Protocol. Front. Psychiatry 13:889572. doi: 10.3389/fpsyt.2022.889572
Received: 04 March 2022; Accepted: 13 April 2022;
Published: 20 May 2022.
Edited by:
Antonia Manduca, Roma Tre University, ItalyReviewed by:
Clifford Cassidy, University of Ottawa, CanadaCopyright © 2022 Sandström, Baltzersen, Marsman, Lemvigh, Boer, Bojesen, Nielsen, Lundell, Sulaiman, Sørensen, Fagerlund, Lahti, Syeda, Pantelis, Petersen, Glenthøj, Siebner and Ebdrup. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bjørn H. Ebdrup, YmpvZXJuLmViZHJ1cEByZWdpb25oLmRr
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.