 Yolanda R. Schlumpf
Yolanda R. Schlumpf Ellert R. S. Nijenhuis
Ellert R. S. Nijenhuis Carina Klein1
Carina Klein1 Lutz Jäncke
Lutz Jäncke Silke Bachmann
Silke Bachmann- 1Division of Neuropsychology, Department of Psychology, University of Zurich, Zurich, Switzerland
- 2Clienia Littenheid AG, Hospital for Psychiatry and Psychotherapy, Littenheid, Switzerland
- 3Research Unit for Plasticity and Learning of the Healthy Aging Brain, University of Zurich, Zurich, Switzerland
- 4Department of Psychiatry, Psychotherapy, and Psychosomatics, University Hospitals and University of Halle (Saale), Halle, Germany
- 5Department of Psychiatry, University Hospitals of Geneva, Geneva, Switzerland
Objective: Phase-oriented trauma treatment is efficacious in the treatment of complex trauma and dissociative disorder patients. However, the neural correlates of this therapeutic effect are not yet well-understood. In the current study we investigated whether patients show a strengthening in functional network connectivity in the delta frequency band (1–3.5 Hz) over the course of phase-oriented inpatient trauma treatment while they performed an emotion regulation task. Further, we examined whether neural changes were associated with symptom reduction and improvement in emotion regulation skills.
Methods: Before and after 8 weeks of treatment, electroencephalography (EEG) was acquired in patients (n = 28) with a complex posttraumatic stress disorder (cPTSD) or complex dissociative disorder (CDD). They also completed clinical and emotion regulation questionnaires. To delimit data variability, patients participated as one dissociative part that is referred to as Apparently Normal Part (ANP). Patients' data were compared to a matched healthy control croup (n = 38), also measured twice.
Results: Prior to treatment, functional connectivity was significantly lower in patients compared to controls during cognitive reappraisal of unpleasant pictures and passive viewing of unpleasant and neutral pictures. These hypoconnected networks largely overlapped with networks typically activated during the recall of (emotional) autobiographical memories. Functional connectivity strength within these networks significantly increased following treatment and was comparable to controls. Patients showed symptom reduction across various clinical domains and improvement in the use of cognitive reappraisal as emotion regulation strategy. Treatment-related network normalizations were not related to changes in questionnaire data.
Conclusion: Phase-oriented treatment may strengthen connections between regions that are activated during autobiographical recall. These findings encourage further investigation of this circuitry as a therapeutic target in cPTSD and CDD patients.
Clinial trial registration: www.ClinicalTrials.gov, identifier: NCT02459340, https://www.kofam.ch/de/studienportal/suche/149284/studie/26681.
Introduction
According to the Theory of Structural Dissociation of the Personality (1–4) trauma-related disorders can be ranged on a continuum from simple posttraumatic stress disorder (PTSD), to complex (cPTSD), to dissociative disorder not otherwise specified example 1 (DDNOS-1), and dissociative identity disorder (DID). Whereas, simple PTSD is typically associated with a single-incident or limited adult trauma, complex trauma disorders such as cPTSD, DDNOS-1, and DID can arise in response to a history of complex interpersonal trauma during childhood. CPTSD has been listed as an official diagnostic category in ICD-11 (5) and is associated with core PTSD symptoms along with additional symptoms related to emotion regulation, self-concept, and interpersonal relationships (6). DDNOS-1 is a mild form of DID and has therefore been termed Partial DID in ICD-11 (5). In the theory of Structural Dissociation of the Personality (1–4), dissociation is defined as a division of the personality into different dissociative ‘parts'. The more severe the trauma-related disorder on the aforementioned continuum is, the more complex is the division among different dissociative parts. Several prototypical dissociative parts are distinguished (2–4). To date, DID patients have been investigated as fragile Emotional Part (EP)1 and Apparently Normal Part (ANP) (7–15). Fragile EP is the part that manages defense to potential threat. This part recollects traumatic memories and is prone to reenact these in sensorimotor and affectively charged ways that typically include mammalian defenses to major threat. These phenomena qualify as positive dissociative symptoms inasmuch as one part has them (here, fragile EP) but not another part (e.g., ANP). ANP aims to fulfill daily life goals, and in this context, it mentally and behaviorally avoids the traumatic past. As a result, ANP tends to have negative dissociative symptoms such as emotional and bodily detachment, depersonalization, derealization, and more or less extensive amnesia for trauma memories (2–4). Consistent with the theory of Structural Dissociation of the Personality, fragile EP and ANP in DID patients show distinct brain and autonomic response patterns in reaction to threat cues (7–9, 13). Fragile EP's reaction pattern includes vegetative hyperarousal and less prefrontal and anterior cingulate activation than ANP and controls. This effect can be interpreted as lack of inhibition on emotional networks including the amygdala and insula. In contrast, ANPs react with vegetative hypoarousal and emotional and bodily detachment that is linked with an excessive prefrontal and anterior cingulate control on emotional networks (11). Because of these findings, it is important to check in which dissociative part(s) traumatized and dissociative patients are measured to prevent mixing different reaction patterns to emotional cues (3).
Exposure therapy is effective in PTSD (16), however, as a stand-alone approach it can cause large side-effects in complex trauma-related disorders (17). The standard care for complex trauma and dissociative disorder patients such as cPTSD, DDNOS-1, and DID is a phase-oriented treatment (18–24). This treatment approach consists of three phases: 1) establishing safety, stabilization, and symptom reduction, 2) treatment of trauma memories, and 3) rehabilitation and personal growth. In the stabilization phase, emotion regulation strategies are taught to ensure that patients can better tolerate trauma exposure. The three phases can be regarded as a recursive spiral where patients can return to previous phases according to their treatment needs (18). A recent meta-analysis showed that the phase-oriented treatment approach is beneficial in reducing PTSD symptoms in cPTSD and dissociative disorder patients (25). Further, highly dissociative individuals show significant improvement when their trauma-related dissociation is addressed in a phase-oriented treatment format [for a review, see (26)].
The neural correlates associated with successful treatment of complex trauma and dissociative disorder patients have hardly been investigated so far. To our knowledge, our previous study (27) is the only study to date that addressed this topic and explored functional connectivity alterations in networks activated during an emotion regulation task across a phase-oriented treatment in complex trauma-related disorders. Patients participating in the study either fulfilled the diagnostic criteria of cPTSD, DDNOS-1, or DID. They received trauma- and dissociation-adapted treatment in a multimodal inpatient setting during 8 weeks. Data were acquired pre- and post-treatment and electroencephalography (EEG) functional connectivity on the source level in the theta (4–8 Hz), alpha (8.5–12 Hz), and beta (12.5–30 Hz) frequency band was assessed. During data acquisition, participants had to either cognitively reappraise unpleasant pictures or to view neutral or unpleasant pictures. Compared to mentally healthy controls, patients showed a pre-treatment hypo-connectivity in networks that disappeared after treatment. These functional connectivity alterations were restricted to the beta frequency band and mainly encompassed cognitive control regions (prefrontal cortex [PFC], anterior cingulate cortex [ACC]), lateral and mesial temporal regions (temporal gyrus, hippocampus/para-hippocampal gyrus), and the insula. In addition, patients showed a pre- to post-treatment reduction in self-reports on PTSD, depression, and general dissociative and negative dissociative symptoms involving depersonalization, derealization, and various anesthetic symptoms. Further, they exhibited a treatment-related increase in the use of cognitive reappraisal that is known to be an effective emotion regulation strategy (28–32). Network changes in the beta frequency band were neither significantly correlated with clinical symptom reduction nor with improved self-reported emotion regulation skills.
Studies relating EEG oscillations with cognitive and emotional processes have mainly focused on theta, alpha, beta, and gamma frequency bands. Some studies addressed slow delta oscillatory activity (1–3.5 Hz). Knyazev and colleagues suggest that delta oscillations modulate activity in brain circuits that are involved in basic motivational processes. These processes facilitate survival by screening of external and internal cues that indicate threat or reward (33, 34). This research implies a key role for delta oscillations in motivation, attention, and salience detection. In line with this interpretation, maximal delta oscillatory response was observed upon presentation of salient and highly arousing cues (35, 36) or during conditions that demand to internally direct the attention when a mental task is executed (e.g., solving an arithmetic problem or working memory task) (37, 38). In a condition where neutral or affectively salient stimuli are presented and participants have to respond naturally or change emotional responses to these cues, a modulation of neural activity in the delta frequency band is expected. Therefore, we here specifically focused on delta oscillations to further explore treatment-related functional connectivity changes and extended previously applied analyses to delta oscillations. All patients were exclusively tested as ANP to reduce variance in the collected data. In accordance with our previous EEG emotion regulation study (27), we hypothesized that phase-oriented treatment strengthens functional connectivity between the PFC, ACC, lateral and mesial temporal areas, and the insula in the patient group. As we did not find any significant correlation between pre- to post-treatment functional connectivity increases and self-reported symptom reduction and/or enhancement in emotion regulation in our precedent article (27), we did not propose any hypotheses on possible correlations between questionnaire data and neural connectivity in the delta frequency band.
Materials and methods
The current study is part of a larger project designed to investigate treatment-related changes in complex trauma and dissociative disorder patients. The methods applied here largely overlap with the methods used in Schlumpf et al. (27).
Treatment setting
At the time of measurement, the patients were inpatients on two specialized trauma wards at the Psychiatric Hospital Clienia Littenheid AG, Littenheid, Switzerland that usually lasts 8 weeks. Both wards offer a multimodal phase-oriented program including trauma- and dissociation-specific psychotherapy (in individual and group setting), stabilization groups (cognitive and body-related), and other non-verbal treatment settings (occupational, art, and music therapy). Supplementary Table 1 outlines the treatment modalities applied per patient. Most patients enrolled in the study was in the first and/or second treatment phase.
Subjects
Data of 21 patients with a cPTSD and 23 with a complex dissociative disorder (CDD) were acquired. CDD patients fulfilled criteria of a DDNOS-1 or DID (39). The Structural Diagnostic Interview for DSM-IV for Dissociative Disorders (SCID-D) (40) and the Posttraumatic Diagnostic Scale (PDS) (41) were used to verify the clinical diagnoses of DID, DDNOS-1, and PTSD. As cPTSD has become an official diagnose in ICD-11 (5) after the completion of data acquisition, the consensus criteria of cPTSD were checked using the German Version of the Structured Interview for Disorders of Extreme Stress, that is, the Interview zur Komplexen Posttraumatischen Belastungsstörung (IK-PTBS) (42). All patients suffered from chronic and severe interpersonal trauma. To delimit data variability, patients were exclusively measured as ANP. The reason for choosing ANP is that it is easier to control than EP in an experimental setting. Further, most patients were not able to willfully bring forward an EP and to stay in this part throughout the experiment. The control group consisted of 40 in age and sex matched healthy controls. Due to various reasons, we had several drop-outs: premature discharge from the clinic (2 cPTSD), inability to perform the experimental task (4 cPTSD, 4 CDD), low number of artefact-free segments (see below; 1 cPTSD, 1 CDD, 1 healthy control), technical problems during data acquisition (4 cPTSD), or back up error (1 healthy control). The final analysis was conducted in 18 CDD patients, 10 cPTSD patients, and 38 healthy controls. The reader is referred to Table 1 for details on demographic and clinical characteristics of participants and Supplementary Table 2 for details on psychotropic medication and comorbid diagnoses in the patient group (27).
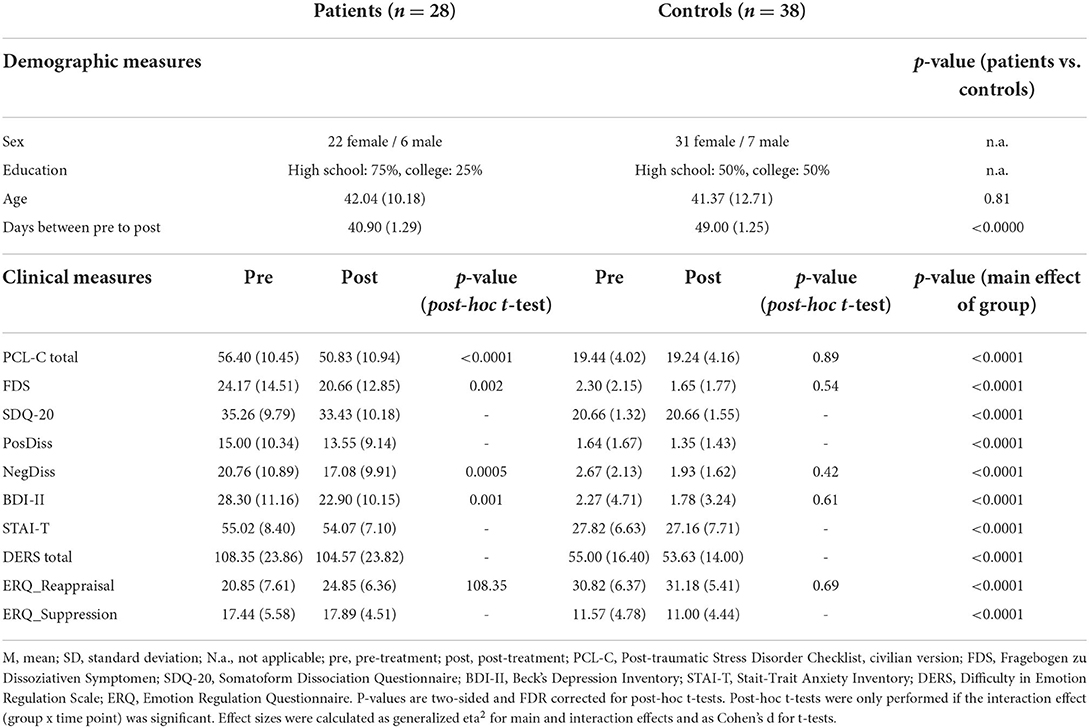
Table 1. Demographic and clinical data.
Written informed consent from each human subject was obtained prior to his/her participation. The study was approved by the local ethics committees of the cantons Zurich and Thurgau. All procedures performed in this study were in accordance with the Declaration of Helsinki.
Study design
We acquired data at two time points. The patient group was tested pre-treatment (at the beginning of their inpatient stay) and post-treatment (before discharge from the hospital). Controls were examined twice as well-within a time period of 5 to 10 weeks. Each data acquisition included an EEG experiment and the assessment of self-reports on clinical symptoms and emotion regulation capacity.
EEG paradigm
The EEG task comprised a cognitive reappraisal task that was developed according to previous cognitive reappraisal EEG studies (43–47). Cognitive reappraisal is a strategy that aims to re-interpret a stressful situation in a way to change its perceived emotional impact (48). Prior to the experiment, participants were instructed how to use self- or situation-focused cognitive reappraisal strategies [according to (49)]. Situation-focused reappraisal refers to the re-interpretation of situational aspects of a situation (e.g., imagining that the crying person on the picture will get better soon). Self-focused reappraisal refers to the re-evaluation of the self-relevance of a situation by taking a detached, third-person perspective (e.g., imagining that the picture depicts a movie rather than a real incident). Color pictures were taken from the International Affective Picture System (IAPS) (50). The following types of pictures were presented: 1) highly arousing pictures depicting humiliation, threat, and grief (unpleasant); 2) neutral pictures depicting plants, landscapes, and household objectives (neutral object); 3) neutral pictures comprising neutral interpersonal scenes or neutral faces [neutral human; for more details on the picture selection process, see supplementary materials in Schlumpf et al. (27)]. A trial is presented in Figure 1. For unpleasant pictures, participants were either requested to have their natural emotional responses to a following picture (UnpleasantNatural condition) or to reduce emotional arousal using cognitive reappraisal (UnpleasantDownregulation condition, see Figure 1A). In trials depicting either neutral objects or neutral human pictures, participants were only instructed to respond naturally to the upcoming picture (NeutralObjectNatural and NeutralHumanNatural condition, see Figure 1B). Each condition was presented 20 times in randomized order. In half of the trials, participants had to rate the pictures regarding valence and arousal using the 9-point Self-Assessment Manikin scale (51). The EEG recording lasted approximately 15 min per measurement point. Results on valence and arousal ratings are outlined in Figure 2 in Schlumpf et al. (27). These ratings suggested that patients perceived all pictures at both time points as more negative and more arousing compared to controls. Further, not only unpleasant but also neutral human pictures evoked abnormal emotional arousal in the patient group.
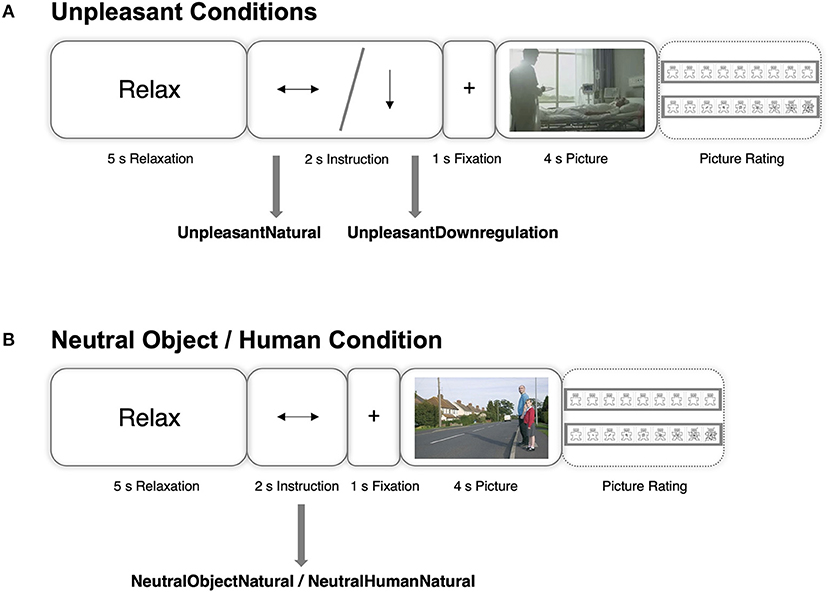
Figure 1. Schematic representation of an example trial in each condition. A horizontal arrow or a vertical arrow pointing downwards indicate that the individual has to naturally respond to or to reduce the emotional reaction to an upcoming picture, respectively. (A) Depicts trials that use unpleasant images, (B) depicts trials that use neutral object or neutral human pictures. From “Functional reorganization of neural networks involved in emotion regulation following trauma therapy for complex trauma disorders” by Schlumpf et al. (27). CC BY-NC-ND 4.0.
Self-report instruments: Clinical symptoms and emotion regulation capacity
At each measurement point, participants completed several self-report instruments. The civilian version of the Posttraumatic Stress Disorder Checklist (PCL-C) (52) is a 17-items questionnaire that evaluates the severity of DSM-IV PTSD symptom criteria. The items are scored on a scale from 1 to 5 (range: 17–85). The total score measures hyperarousal, intrusion, and avoidance/numbing. The Fragebogen zu Dissoziativen Symptomen (FDS) (53, 54) consists of 44 items that evaluate the severity of cognitive-emotional and several other dissociative symptoms. Participants have to indicate the amount of time (0–100%) they experience each symptom. The total score is calculated by summing up the 44 items score and dividing by 44 (range: 0–100). The Somatoform Dissociation Questionnaire (SDQ) (55) assesses the severity of somatoform (i.e., sensorimotor) dissociative symptoms. This questionnaire consists of 20 items that are scored on a scale from 1 and 5 (range: 20–100). Positive dissociative symptoms (e.g., intrusions, flashbacks) and negative dissociative symptoms (e.g., depersonalization, derealization, various anesthetic symptoms) were measured by composite scores including items of the FDS and SDQ-20 that were unambiguously assignable as positive (PosDiss score) or negative (NegDiss score), respectively [see (27)]. The Beck's-Depression Inventory II (BDI-II) comprises 21 items measuring the severity of depression (56). The items are scored on a scale from 0 to 3 (range: 0–63). The trait part of the Stait-Trait Anxiety Inventory (STAI-T) was used to assess trait anxiety (57). This questionnaire consists of 20 items that are scored on a scale from 1 to 4 (range: 20–80).
The Difficulty in Emotion Regulation Scale (DERS) (58) and the Emotion Regulation Questionnaire (ERQ) (59) were assessed at both time points to test emotion regulation strategies. The DERS consists of 36 items that are scored on a scale from 1 to 5 (range 36–180). The DERS total score comprises six subscales (non-acceptance of emotional responses, difficulty in goal-directed behavior, difficulty controlling impulses, lack of emotional awareness, lack of access to emotion regulation strategies, lack of emotional clarity). Higher scores suggest more severe emotion regulation difficulties. The ERQ encompasses the two subscales cognitive reappraisal (ERQ_Reappraisal) and expressive suppression (ERQ_Suppression). The 10 items are scored on a scale from 1 to 7 (range per subscale: 5–35). The higher a subscale score, the more an individual applies the corresponding strategy. Handling of incomplete data is explained in the supplementary material of Schlumpf et al. (27).
We calculated internal consistency (Cronbach's alpha) for each scale and for both measurement points separately. All values are high and are listed in Supplementary Table 3.
EEG recording and raw data pre-processing
EEG data were registered using an actiCap system in combination with a QuickAmp-72 amplifier (Brain Products Inc., http://www.brainproducts.com). Sixty-four channels were attached according to the international 10–10 electrode placement system. The average of activity at all electrodes was taken and used as a reference. During EEG recording, data were sampled at 500 Hz and filtered with a band-pass filter between 0.1 and 100 Hz and a notch filter at 50 Hz. Impedances were kept below 25 kOhm.
Preprocessing of the raw EEG data was performed using the Brain Vision Analyzer 2.0 software (Brain Products Inc.). Independent component analysis was applied to remove eye activity artifacts (i.e., saccades and eye blinks) (60). Data was then band-pass filtered between 0.1 and 40 Hz. Bad channels were reconstructed based on the interpolated values from the surrounding electrodes. Remaining artifacts (i.e., movement or muscle artifacts) were rejected using the automated raw data inspection implemented in Brain Vision Analyzer. Data were segmented into epochs of 4 s consisting of the data acquired during picture presentation. Using an acceptance criterion of 10 or more artefact-free segments per condition, three participants (1 cPTSD, 1 CDD, 1 healthy control) were excluded from the analysis due to low data quality. Thus, the artefact-free data epochs in all participants ranged from 11 to 20. Further details on data epochs can be found in the supplementary material of Schlumpf et al. (27).
Connectivity analysis on the source level
The artefact-free and segmented data was exported to the sLORETA toolbox (Version 20160611, https://www.uzh.ch/keyinst/loreta.htm) for further analyses (61). Intracranial functional connectivity values were calculated between 84 regions of interest (ROIs). These 84 ROIs relate to Brodmann areas implemented in sLORETA (BA; 42 for each hemisphere). The labels of brain regions are based on visual inspection and the Juelich Histological and the Harvard-Oxford cortical atlases that are integrated in the fMRIB software (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Atlases). The labels and coordinates of all 84 ROIs are listed in Supplementary Table 4. Details on quality check of the source estimation process are provided in the supplementary material of Schlumpf et al. (27). We used lagged coherence as functional connectivity measure. This measure is, compared to the instantaneous coherence value, not confounded by non-physiological artifacts such as low spatial resolution or volume conduction (62, 63). The 4 s preprocessed segments were divided into 2 s segments to increase statistical power. Lagged coherence values in the delta frequency band (1–3.5 Hz) were calculated between the centroid voxel of all pairs of 84 ROIs. Discrete Fourier transform was used to derive the spectral representation of the EEG signal.
Network-based statistical analyses
Based on these 84 × 84 connectivity matrices from the intracranial analysis in sLORETA, we run network-based statistics using the Network-based Statistic toolbox (NBS, https://www.nitrc.org/projects/nbs/) in MATLAB (version R2015b, http://www.mathworks.com/). This method aims to identify brain graphs that consist of brain regions (nodes) and connections between these areas (edges). Foremost, a sensitivity threshold has to be predefined. Then, a statistical test (e.g., t-test) is conducted on every single edge of the network. Edges that exceed the predefined sensitivity threshold form a graph. To make inference, permutation is used and the family-wise error (FWE) rate is controlled by running mass-univariate testing on all graph edges. The statistical significance of a graph expresses the likelihood of finding a graph with an equal or a greater number of edges by chance (64, 65).
To increase statistical power, CDD and cPTSD patients were merged to one group (n = 28)2. We followed the same statistical approach as in Schlumpf et al. (27). First, between-group differences were examined at the first measurement point for each condition (NeutralObjectNatural, NeutralHumanNatural, UnpleasantNatural, and UnpleasantDownregulation condition) separately. These four two-sample t-tests were performed for both contrasts (patients > controls, controls > patients). Second, we evaluated group x time point interactions. These interaction effects were calculated using difference maps (i.e., lagged coherence post-treatment values – lagged coherence pre-treatment values) that were submitted to two-sample t-tests. The difference maps were restricted to the networks that significantly differed between groups at the first measurement point. This approach enabled us to check for any treatment related alterations in these networks. Further, we performed two-sample t-tests to assess any post-treatment group differences in the initially altered networks. Finally, we also checked for any whole brain post-treatment group differences to explore potential network changes irrespective of the pre-treatment group differences. P-values were set to 0.05 and 5,000 permutations were used for all statistical tests. The number of days between measurement points differed significantly between groups (patients M = 40.90 (1.29), controls M = 49.00 (1.25); t = −4.51, p < 0.000, d = −1.10). Therefore, days between measurements were entered as covariate of no interest in the NBS analyses.
For the pre-treatment analyses, we chose the highest (i.e., most conservative) sensitivity thresholds reaching a significant single subnetwork (NeutralObjectNatural threshold at t = 4.0, NeutralHumanNatural threshold at t = 3.6, UnpleasantNatural threshold at t = 3.8, UnpleasantDownregulation threshold at t = 3.2). Thus, we did not select subnetworks that fall apart in different components when using a higher threshold. To ensure that we present stable findings, the pre-treatment analyses had to reveal significant results at least for a range of three thresholds when descending them in 0.1 steps. The most liberal sensitivity threshold displaying a significant result was chosen for group x time point interaction and post-treatment group analyses. This approach ensured to fully examine if initially altered networks changed across time.
The BrainNet Viewer was used to visualize the functional brain networks (www.nitrc.org/projects/bnv/) (66). Cohen's d, mean, and standard deviations were specified for each significant network revealed in the NBS analysis. These values were computed in R (version 3.4.0, https://www.r-project.org) based on mean functional connectivity scores of these networks. A mean value was calculated by averaging the coherence values of all edges of a network.
Relationship between functional connectivity and self-reports
We tested whether treatment-related changes of the patients' functional connectivity strength were associated with alterations in clinical symptoms and emotion regulation capacity. For this purpose, mean functional connectivity values per network revealed by the group x time point NBS analyses were calculated. Changes across treatment in self-report instruments were investigated by subtracting the pre-treatment score of each patient in a questionnaire from the associated post-treatment score. These difference values (Diff_PCL-C, Diff_FDS, Diff_SDQ-20, Diff_PosDiss, Diff_NegDiss, Diff_BDI-II, Diff_STAI_T, Diff_DERS, Diff_ERQ_Reapraisal, Diff_ERQ_Suppression) were correlated with the mean functional connectivity values per network using Spearman's rank correlations. Correlational analyses were performed in R as two-tailed tests and were limited to the patient's group only. We used false discovery rate (FDR) to correct for multiple comparisons (67). FDR adjustment was applied separately for self-reports on clinical symptoms and self-reports on emotion regulation capacity.
Treatment-related changes in self-report instruments
For each self-report instrument, we performed two (groups) x two (time points) mixed-design ANOVAS. These statistical tests were conducted in R. We used the afex package (68) for factorial designs and applied a Greenhouse-Geisser correction to within subject factors if the assumption of sphericity was violated. P-values are two-tailed. In post-hoc t-tests, we applied FDR correction (67) to adjust for multiple comparisons. Effect sizes are reported as Cohen's d (69) for t-tests and as generalized eta2 (70) for main and interaction effects.
Results
In the present study, we investigated functional connectivity changes in emotion regulation networks induced by a phase-oriented inpatient treatment setting in patients with a history of chronic and severe interpersonal trauma. We extended our analyses of Schlumpf et al. (27) to delta oscillatory responses as they have been shown to be involved in the processing of salient and highly arousing cues (35, 36) or during conditions that demand internally directed attention (36, 37).
Network-based statistics
Pre-treatment and compared to the control group, patients showed hypoconnected networks in the delta frequency band in all conditions [NeutralObjectNatural: p = 0.011, FWE corrected, Cohen's d = −0.80, NBS-specific threshold at t = 4.0, patients mean (SD): 0.05 (0.03), controls mean (SD): 0.08 (0.04); NeutralHumanNatural: p = 0.015, FWE corrected, Cohen's d = −1.10, NBS-specific threshold at t = 3.6, patients mean (SD): 0.07 (0.03), controls mean (SD): 0.11 (0.05); UnpleasantNatural: p = 0.025, FWE corrected, Cohen's d = −1.07, NBS-specific threshold at t = 3.8, patients mean (SD): 0.05 (0.02), controls mean (SD): 0.09 (0.04); UnpleasantDownregulation: p = 0.042, FWE corrected, Cohen's d = −0.88, NBS-specific threshold at t = 3.2, patients mean (SD): 0.08 (0.04), controls mean (SD): 0.14 (0.08)]. The network in the NeutralObjectNatural condition comprised four left lateralized nodes and three edges involving the frontal pole, inferior temporal gyrus, and parahippocampal gyrus. In the NeutralHumanNatural condition, the network consisted of eight left lateralized nodes and eight edges encompassing the ventrolateral prefrontal cortex (vlPFC), posterior cingulate cortex (PCC), superior parietal lobule, superior temporal gyrus, parahippocampal gyrus, hippocampus, and insula. Regarding the UnpleasantNatural condition, the analysis revealed three hypoconnected edges between four left lateralized nodes encompassing the vlPFC, superior parietal lobule, superior temporal gyrus, and insula. In the UnpleasantDownregulation condition, the pre-treatment hypoconnected network involved eight nodes and nine edges between left to right connections. This network comprised of the PCC, precuneus, cuneus, occipital pole, and lingual gyrus.
Second, we investigated whether functional connectivity changed from the first to the second measurement within these networks. Group x time point interactions revealed a significant pre- to post-treatment functional connectivity increase in the patient group. The patients' priorly hypoconnected networks had disappeared in all conditions after treatment [NeutralObjectNatural: p = 0.04, FWE corrected, Cohen's d = 0.41, NBS-specific threshold at t = 1.3, patients mean (SD): 0.01 (0.05), controls mean (SD): −0.01 (0.05); NeutralHumanNatural: p = 0.05, FWE corrected, Cohen's d = 0.71, NBS-specific threshold at t = 0.4, patients mean (SD): 0.02 (0.05), controls mean (SD): −0.02 (0.06); UnpleasantNatural: p = 0.05, FWE corrected, Cohen's d = 0.66, NBS-specific threshold at t = 1.0, patients mean (SD): 0.01 (0.04), controls mean (SD): −0.02 (0.05); UnpleasantDownregulation: p = 0.05, FWE corrected, Cohen's d = 0.35, NBS-specific threshold at t = 0.6, patients mean (SD): 0.02 (0.06), controls mean (SD): 0.00 (0.10)]. These networks are depicted in Figure 2. Tables 2–5 list the edges and nodes involved in these networks. Functional connectivity changes (mean of lagged coherence values) per group and individual pre- to post-treatment trajectories are depicted in Supplementary Figures 1, 2, respectively.

Figure 2. Functional connectivity increase in the delta frequency band over the course of treatment within the initially reduced network in the patient group (group x time point interaction) in the (A) NeutralObjectNatural, (B) NeutralHumanNatural, (C) UnpleasantNatural, and (D) UnpleasantDownregulation condition. Red dots display nodes, the gray lines correspond to the connections (edges). The thickness of a line expresses the significance (t-value) of a connection (p < 0.05, FWE corrected). Inter- and intrahemispheric connections are shown in left, right, horizontal, and coronal slices. A, anterior; L, left; R, right.
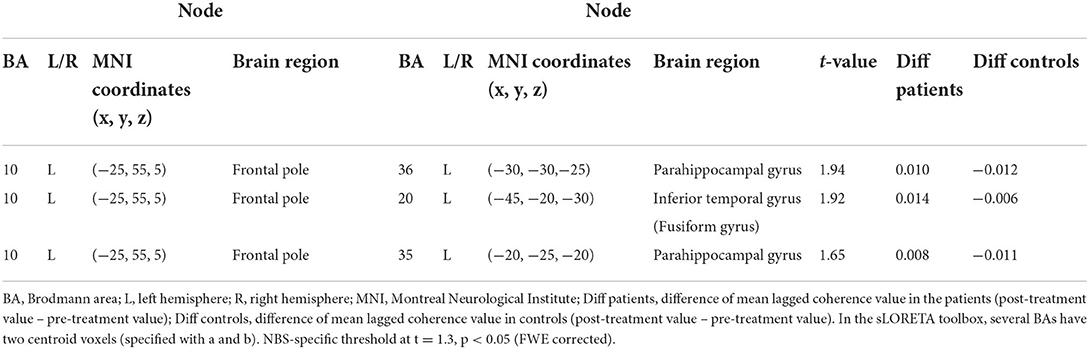
Table 2. Patients' functional connectivity increase across treatment within the initially impaired network in the NeutralObjectNatural condition.
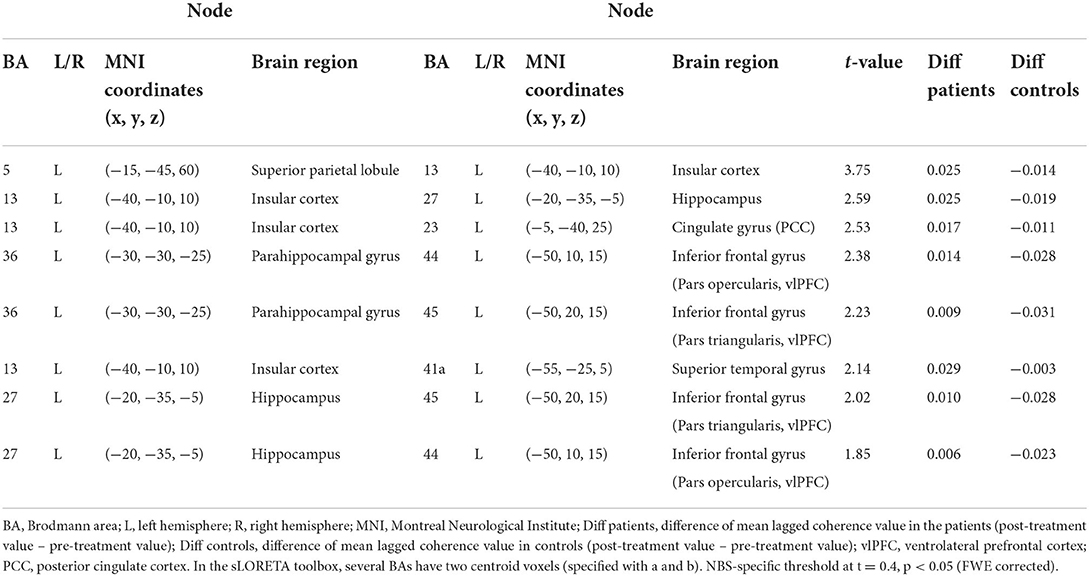
Table 3. Patients' functional connectivity increase across treatment within the initially impaired network in the NeutralHumanNatural condition.
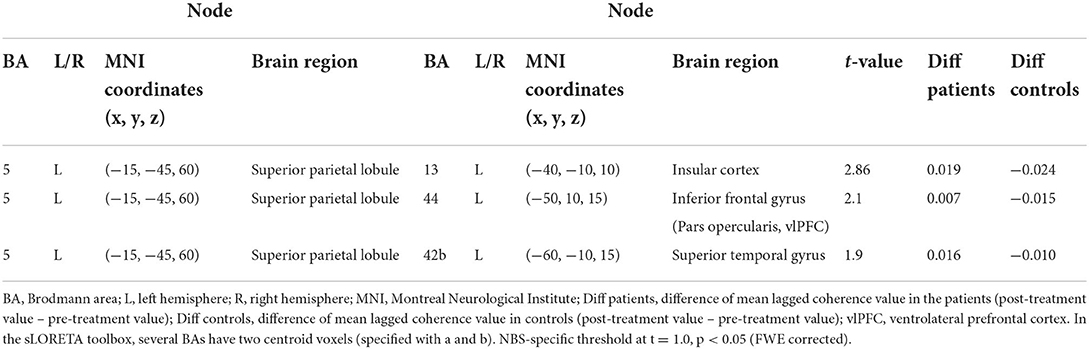
Table 4. Patients' functional connectivity increase across treatment within the initially impaired network in the UnpleasantNatural condition.
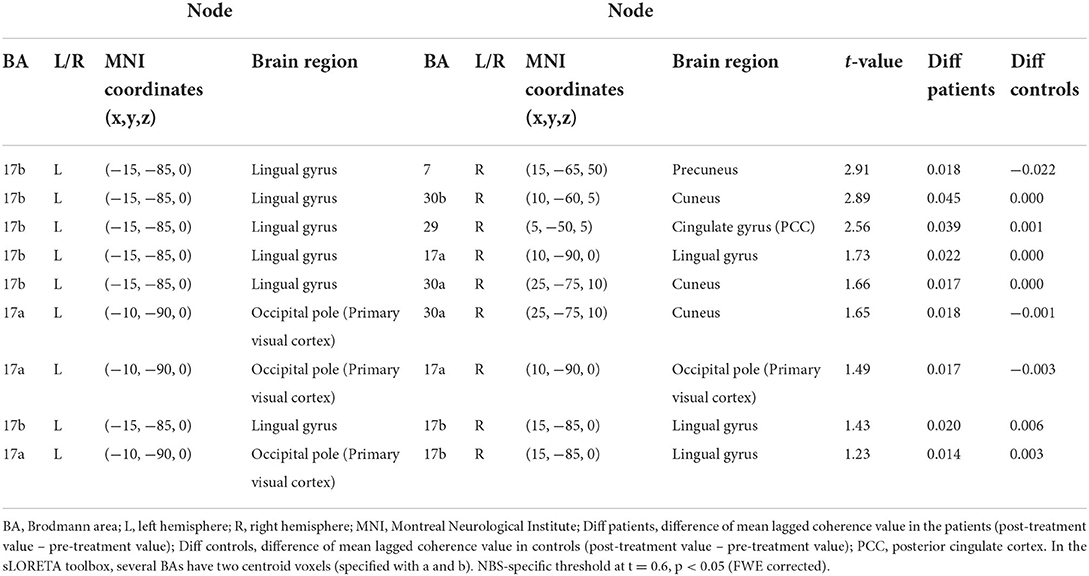
Table 5. Patients' functional connectivity increase across treatment within the initially impaired network in the UnpleasantDownregulation condition.
Third, we checked for post-treatment group differences in the initially hypoconnected networks and did not find any significant network differences (p > 0.05). Thus, patients' pre-treatment hypoconnected networks had normalized post-treatment in all conditions. Finally, we compared the groups at the second time point on the whole-brain level. There were no significant group differences regarding any of the experimental conditions (all ps > 0.05).
Correlations between functional connectivity and self-reports across treatment
We calculated correlations between treatment-related network changes and changes in self-reports on clinical symptoms and emotion regulation capacity. No Spearman's rank correlation survived FDR correction (all ps > 0.05).
Treatment-related changes in clinical symptoms and emotion regulation capacity
Two (groups) x two (time points) mixed-design ANOVAs were performed for each self-report instrument on clinical symptoms and emotion regulation capacity. Across all measures and both measurement points, we revealed more clinical symptoms and more severe emotion regulation deficits in patients compared to controls. Patients exhibited a significant symptom reduction from pre- to post-treatment in the patient group in overall PTSD symptoms (PCL-C total), general dissociative symptoms (FDS), negative dissociative symptoms, and depression (BDI-II). Further, we revealed a significant treatment-related increase in reappraisal values. Table 1 provides detailed information.
Discussion
This is the first study to show that neural networks in the delta frequency band in cPTSD, DDNOS-1, and DID patients change following trauma treatment. Pre- and post-treatment, we measured EEG to calculate delta oscillatory functional connectivity at the source-level in networks involved in cognitive reappraisal of unpleasant pictures or viewing neutral and unpleasant pictures. Before treatment, patients showed hypoconnected networks in all experimental conditions in comparison to a healthy control group. Post-treatment, the patients' functional network strength increased to the level of the healthy controls. This increase was not related to an improvement in clinical symptoms or emotion regulation skills.
During passive viewing of neutral and unpleasant pictures (NeutralObjectNatural, NeutralHumanNatural, and NeutralUnpleasant condition), we observed functional network changes from pre- to post-treatment in the patients within prefrontal regions, the PCC, superior parietal lobule, lateral and mesial temporal areas, and the insula. Network alterations were found exclusively in the left hemisphere. These networks largely overlap with a predominantly left lateralized network typically found in autobiographical memory retrieval (71–74).
Treatment-related network changes during cognitive reappraisal of unpleasant pictures (UnpleasantDownregulation condition) encompassed the PCC, precuneus, and several occipital areas (cuneus, occipital pole, lingual gyrus). All these regions have also been implicated in autobiographical memory (71). However, compared to the networks activated in the viewing conditions, this network was not lateralized but encompassed edges in both hemispheres. Bilateral brain activity has been found in several studies investigating emotional memory retrieval (71). Hence, our findings support the idea that treatment brought about increased connectivity of a neural network associated with the retrieval of emotional autobiographical events while the patients were instructed to reappraise aversive cues. We had expected to find prefrontal and anterior cingulate regions in this network as they are typically implicated in cognitive reappraisal (75–77). The lack of these regions suggests that delta oscillatory responses were not associated with group differences in cognitive reappraisal. Both groups perceived the unpleasant pictures after treatment as significantly less negative compared to before treatment. However, the patients' emotional ratings of the unpleasant pictures indicate that these appeared more negative and arousing to them compared to the healthy control group before and after treatment (12). Thus, the aversive pictures continued to have a negative meaning to them which is probably due to their trauma history.
Our results might reflect an increased capacity in patients as ANP to recollect their (painful) past, a past that they somehow associated with the neutral and unpleasant pictures. Clinical and empirical evidence shows that ANPs are typically associated with mental and behavioral avoidance of trauma-related cues (2–4, 7–9, 13–15). Most of the patients under study were in the first and/or second treatment phase that focuses on building up skills to react to emotional challenges in effective ways and on controlled confrontation with traumatic experiences (18–24). A primary goal in these phases for ANPs is to raise the capacity to tolerate strong affect, sensations, and memories related to aversive past events. This is a requirement for the integration of traumatic memories in one's autobiography and fusion of dissociative parts (2–4). To the extent that treatment is effective, ANPs may be expected to be less emotionally and physically numbed not only with regards to the trauma history but far more generally and have gained the ability to mentally avoid their common and traumatizing past less. Consequently, they might be better able to recollect their (painful) past. Hence, our results might reflect a significant treatment progress in the patients under study and is in accordance with the treatment-related decrease in negative dissociative symptoms (see Table 1) that implies that patients as ANP were less depersonalized, de-realized, and emotionally numbed following phase-oriented treatment (12).
In line with our hypothesis, we found a strengthening of neural functional networks across treatment in the patient group. However, we did not expect that these networks would show a large similarity with the autobiographical memory network. Autobiographical memories entail great personal and emotional significance (78, 79). Hence, our findings might be particularly mediated by the functional roles of delta oscillations. Delta band activity is associated with the perception of cues that are motivationally and emotionally salient and attract attention (33–38). In this line of reasoning, a strengthening in the autobiographical memory network in response to visual cues could also reflect that treatment may have helped the patients as ANP to experience and see more what is self-relevant and of affective significance to them. This interpretation is in accordance with a resting-state functional connectivity study suggesting an increased ability in ANPs to engage in self-related thinking across a phase-oriented inpatient treatment (80) and is further supported by the growing body of evidence that relates dissociation to a reduce capacity for self-reference (81–83). The increased functional coupling among occipital areas in the network involved in the execution of cognitive reappraisal suggests as well-that the patients experienced and perceived unpleasant pictures more intensely following treatment while they managed to reduce their emotional responses to these cues.
The interpretation of our results remains speculative as we did not measure participants' mental state during the EEG measurement. In particular, we did not systematically explore if the presented pictures promoted autobiographical retrieval. It is therefore important to investigate in a follow-up study whether the pictures led to a reactivation of associations with past (traumatizing) events. However, our interpretation is in line with the capacities that are gradually developed in a phase-oriented treatment. In the patients' discharge reports, therapists reported improvements regarding containment and grounding strategies, awareness and tolerance of sensations and affects associated with the trauma and other dissociative parts, identification of triggers, remembering painful past events, realization that these are part of their life and acceptance of their meaning and implications, and becoming better reoriented in the actual presence while recollecting their past. These evaluations are consistent with the observed network changes and our interpretation thereof.
Patients experienced a significant therapy-related reduction in PTSD symptoms (PCL-C), general dissociative symptoms (FDS), and negative dissociative symptoms (NegDiss), and symptoms of depression (BDI-II) (see Table 1). Symptom reduction across several clinical domains is in accordance with cross-sectional (84) and longitudinal treatment outcome studies (85, 86). Further, the patients' use of cognitive reappraisal as emotion regulation strategy increased significantly following treatment. Nonetheless, patients still had higher values in all clinical measures after treatment compared to healthy controls. Thus, a continuation of treatment is required. Previous findings of relationships between alterations in questionnaire data and neural changes across treatment are inconsistent (27, 80, 87–90). In the present study, network changes were neither associated with self-reported symptom reduction, nor with improvement in emotion regulation capacities. A reason for the null finding on correlations between neural and questionnaire data might be that network changes in the delta frequency band do not particularly relate to changes in the assessed clinical and behavioral variables. Electrophysiological outcome in the current study might for instance rather be associated with autobiographical recall that has not been tested.
There are several limitations to this study. We did not include a waiting list control group. Nevertheless, due to the chronicity of the patients' pathology, we do not assume that time alone can explain the treatment related network changes. Patients showed high comorbidity and took psychotropic medication. Hence, confounding effects of comorbid disorders and psychotropic medication cannot be excluded. However, the study conditions were naturalistic as the patients enrolled in the study typically show high comorbidity and take psychopharmaca. Further, since individual medical therapies were heterogeneous, a systematic influence of pharmacological treatment on EEG functional connectivity is most unlikely. A large body of evidence could show that the degree of handedness is a marker for individual differences across various domains including episodic memory retrieval (91). In a volumetric analysis, individuals with less consistent hand preference showed a larger corpus callosum size compared to individuals with a consistent hand preference (92)3. According to the hemispheric interaction model (93), a larger corpus callosum size leads to a better interhemispheric interaction. This increased interhemispheric communication might explain the memory advantage in individuals with a less consistent hand preference (91). Since we found networks that contribute to autobiographical memories, future studies should include the degree of handedness as a covariate of no interest in the statistical model to control for the potential influence of handedness on functional connectivity within these networks. As patients improved clinically but substantial trauma-related symptoms persisted, a long-term follow-up study is needed to investigate clinical and neural trajectories across a longer period of time. Future studies should extend the measurement to (different types of) EP. This would further deepen our knowledge how successful treatment effects neural and clinical changes in dissociative parts that react differently to perceived threat compared to ANP. Last, this study measured an overall effect of a multimodal treatment setting. Future studies could include scales that can assess to what extent a particular treatment modality is successful. This could give further insights into which modalities prompt treatment outcome the most.
In conclusion, this work extends a previous emotion regulation functional connectivity study (27) by demonstrating that a phase-oriented treatment is associated with functional connectivity changes in the delta frequency band in networks involved in (emotional) autobiographical memory. Further, patients profited across several clinical domains. These results suggest that treatment provided by therapists who have training in complex trauma and dissociation seems to be beneficial and merits further investigation.
Data availability statement
The data that support the findings of this study are available from the corresponding author, YS, upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Local Ethics Committees of the Canton of Zurich and Thurgau. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YS conceived and planned the experiment, carried out the experiment, performed the calculations, and wrote the manuscript. CK contributed to data analysis and visualization and interpretation of the data. SB initiated the project. SB, EN, and LJ supervised the project, contributed to the interpretation of the results, and provided critical feedback to the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by Clienia Littenheid AG.
Acknowledgments
The authors would like to thank all the patients and control persons that participated in the study. We are very grateful for the support of the teams Waldegg A and B (Clienia Littenheid AG) during the study. We thank Zelda Bernardi, Ronja Dieterle, Maximiliane Ekert, Stephanie Gonzenbach, Anna Gossweiler, Amatya Mackintosh, and Corina Sager for research assistance. We also thank Dr. Julia Binder for her helpful comments on drafts of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.889560/full#supplementary-material
Footnotes
1. ^Different subtypes of fragile EPs have to be distinguished (3, 4). To date, only fragile EPs that predominantly demonstrate active, sympathetically driven defense behavior to potential threat have been investigated. Research on fragile EPs that mainly engage in passive, parasympathetically mediated tonic immobility is lacking.
2. ^Apart from alterations among dissociative parts, the symptoms are not of a different nature in these three disorders but they are less extreme in DDNOS-1 and even less pronounced in cPTSD compared to DIS.
3. ^As an aside, other studies found that corpus callosum size was particularly influenced by factors such as forebrain volume (94) or gender (95). However, a detailed discussion on associations between corpus callosum size and other factors than handedness is beyond the scope of these article.
References
1. Nijenhuis ERS, Van der Hart O, Steele K. The emerging psychobiology of trauma-related dissociation and dissociative disorders. In: D'Haenen H, Den Boer JA, Willner P, editors. Biological Psychiatry. London: Wiley (2002). p. 1079–1098 doi: 10.1002/0470854871.chxxi
2. Van der Hart O, Nijenhuis ERS, Steele K. The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization. New York, London: WW Norton & Company (2006).
3. Nijenhuis ERS. The Trinity of TRauma: Ignorance, Fragility, and Control. The evolving concept of trauma/The concept and facts of dissociation in trauma. Göttingen: Vandenhoeck & Ruprecht (2015).
4. Nijenhuis ERS. The Trinity of Trauma: Ignorance, Fragility, and Control. Enactive trauma therapy Göttingen: Vandenhoeck & Ruprecht (2017).
5. WHO. International statistical classification of diseases 11th revision. (2019). Available online at: https://icd.who.int/en
6. Maercker A, Brewin CR, Bryant RA, Cloitre M, Van Ommeren M, Jones LM, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11. World Psychiatry. (2013) 12:198–206. doi: 10.1002/wps.20057
7. Schlumpf YR, Reinders AATS, Nijenhuis ERS, Luechinger R, van Osch MJP, Jäncke L. Dissociative part-dependent resting-state activity in dissociative identity disorder: a controlled fMRI perfusion study. PLoS ONE. (2014) 9:8795. doi: 10.1371/journal.pone.0098795
8. Schlumpf YR, Nijenhuis ERS, Chalavi S, Weder EV, Zimmermann E, Luechinger R, et al. Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: an fMRI study of dissociative identity disorder. NeuroImage Clin. (2013) 3:54–64. doi: 10.1016/j.nicl.2013.07.002
9. Reinders AATS, Nijenhuis ER, Quak J, Korf J, Haaksma J, Paans AM, et al. Psychobiological characteristics of dissociative identity disorder: a symptom provocation study. Biol Psychiatry. (2006) 60:730–40. doi: 10.1016/j.biopsych.2005.12.019
10. Reinders AATS, Willemsen AT, Vos HP, Den Boer JA, Nijenhuis ER. Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states. PLoS ONE. (2012) 7:e39279. doi: 10.1371/journal.pone.0039279
11. Reinders AATS, Willemsen ATM, Den Boer JA, Vos HPJ, Veltman DJ, Loewenstein RJ. Opposite brain emotion-regulation patterns in identity states of dissociative identity disorder: a PET study and neurobiological model. Psych Res - Neuroimag. (2014) 223:236–43. doi: 10.1016/j.pscychresns.2014.05.005
12. Reinders AATS, Willemsen ATM, Vissia EM, Vos HPJ, den Boer JA, Nijenhuis ERS. The psychobiology of authentic and simulated dissociative personality states: the full monty. J Nerv Ment Dis. (2016) 204:445–57. doi: 10.1097/NMD.0000000000000522
13. Reinders AATS, Nijenhuis ERS, Paans AMJ, Korf J, Willemsen ATM, Den Boer JA. One brain, two selves. Neuroimage. (2003) 20:2119–25. doi: 10.1016/j.neuroimage.2003.08.021
14. Hermans EJ, Nijenhuis ERS, Van Honk J, Huntjens RJC, Van der Hart O. Identity state-dependent attentional bias for facial threat in dissociative identity disorder. Psychiatry Res. (2006) 141:233–6. doi: 10.1016/j.psychres.2005.03.007
15. Seidmann S, Schlumpf YR, Jäncke L. When one look is all it takes. A Single-Case Eye-Tracking Study in a Patient With Dissociative Identity Disorder, a Simulant, and Healthy Controls (Unpublished master's thesis). Zurich: University of Zurich (2014).
16. Schnyder U. Psychotherapy bei posttraumatischen Belastungsstörungen. PPmP Psychotherapie Psychosomatik Medizinische Psychologie. (2000) 50:123–33. doi: 10.1055/s-2000-13237
17. Flatten G, Reddemann L, Woeller W, Hofmann A. Therapie der posttraumatischen Belastungsstörung, In: Glatten G, Gast U, Wöller HAL, Redemann L, Siol T, Liebermann P, Petzold ER, editors. Posttraumatische Belastungsstörung: Leitlinie und Quellentext. Stuttgart: Schattauer (2004). p. 103–127.
18. Courtois. Recollection of Sexual Abuse: Treatment Principles and Guidlines. New York: W.W. Norton & Co (1999).
19. Ford JD, Courtois CA, Steele K, Van der Hart O, Nijenhuis ERS. Treatment of complex posttraumatic self-dysregulation. J Trauma Stress. (2005) 18:437–47. doi: 10.1002/jts.20051
20. Steele K, Van der Hart O, Nijenhuis ERS. Dependency in the treatment of complex posttraumatic stress disorder and dissociative disorders. J Trauma Dissoc. (2001) 2:79–116. doi: 10.1300/J229v02n04_05
21. Steele K, Van der Hart O, Nijenhuis ERS. Phase-oriented treatment of structural dissociation in complex traumatization: Overcoming trauma-related phobias. J Trauma Dissoc. (2005) 6:11–53. doi: 10.1300/J229v06n03_02
22. International Society for the Study of Trauma and Dissociation. Guidelines for treating dissociative identity disorder in adults, third revision. J Trauma Dissoc. (2011) 12:115–87. doi: 10.1080/15299732.2011.537247
23. Loewenstein RJ, Welzant V. Pragmatic approaches to stage-oriented treatment for early life trauma-related complex post-traumatic stress and dissociative disorders, In: Lanius RA, Vermetten E, Pain C, editors. The impact of early Llfe trauma on health and disease: The hidden epidemic. Cambridge: Cambridge University Press (2010). p. 257–267 doi: 10.1017/CBO9780511777042.030
24. Cloitre M, Courtois CA, Charuvastra A, Carapezza R, Stolbach BC, Green BL. Treatment of complex PTSD: results of the ISTSS expert clinician survey on best practices. J Trauma Stress. (2011) 24:615–27. doi: 10.1002/jts.20697
25. Corrigan JP, Fitzpatrick M, Hanna D, Dyer KFW. Evaluating the effectiveness of phase-oriented treatment models for PTSD - A meta-analysis. Traumatology (Tallahass Fla). (2020) 26:447–54. doi: 10.1037/trm0000261
26. Brand BL, Classen CC, McNary SW, Zaveri P, A. review of dissociative disorders treatment studies. J Nerv Mental Dis. (2009) 197:646–54. doi: 10.1097/NMD.0b013e3181b3afaa
27. Schlumpf YR, Nijenhuis ERS, Klein C, Jäncke L, Bachmann S. Functional reorganization of neural networks involved in emotion regulation following trauma therapy for complex trauma disorders. NeuroImage: Clin. (2019) 23:1–14. doi: 10.1016/j.nicl.2019.101807
28. Gross JJ. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology. (2002) 39:281–91. doi: 10.1017/S0048577201393198
29. Gross JJ, Levenson RW. Hiding feelings: The acute effects of inhibiting negative and positive emotion. J Abnorm Psychol. (1997) 106:95–103. doi: 10.1037/0021-843X.106.1.95
30. Hagemann T, Levenson RW, Gross JJ. Expressive suppression during an acoustic startle. Psychophysiology. (2006) 43:104–12. doi: 10.1111/j.1469-8986.2006.00382.x
31. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. (2010) 30:217–37. doi: 10.1016/j.cpr.2009.11.004
32. John O, Gross JJ. Healthy and unhealthy emotion regulation: personality processes, individual differences, and life span development. J Pers. (2004) 72:1301–33. doi: 10.1111/j.1467-6494.2004.00298.x
33. Knyazev GG, EEG. delta oscillations as a correlate of basic homeostatic and motivational processes. Neurosci Biobehav Rev. (2012) 36:677–95. doi: 10.1016/j.neubiorev.2011.10.002
34. Knyazev GG. Motivation, emotion, and their inhibitory control mirrored in brain oscillations. Neurosci Biobehav Rev. (2007) 31:377–95. doi: 10.1016/j.neubiorev.2006.10.004
35. Güntekin B, Başar E, A. review of brain oscillations in perception of faces and emotional pictures. Neuropsychologia. (2014) 58:33–51. doi: 10.1016/j.neuropsychologia.2014.03.014
36. Güntekin B, Başar E. Review of evoked and event-related delta responses in the human brain. Int J Psychophysiol. (2016) 103:43–52. doi: 10.1016/j.ijpsycho.2015.02.001
37. Harmony T, Fernández T, Silva J, Bernal J, Díaz-Comas L, Reyes A, et al. delta activity: An indicator of attention to internal processing during performance of mental tasks. Int J Psychophysiol. (1996) 24:161–71. doi: 10.1016/S0167-8760(96)00053-0
38. Harmony T. The functional significance of delta oscillations in cognitive processing. Front Integr Neurosci. (2013) 7:83. doi: 10.3389/fnint.2013.00083
39. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author (2013).
40. Steinberg M. Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D). Washington DC: American Psychiatric Press (1993).
41. Ehlers A, Steil R, Winter H, Foa EB. Deutsche Übersetzung der Posttraumatic Diagnostic Scale (PDS). Oxford: University, Warneford Hospital (1996).
43. Ertl M, Hildebrandt M, Ourina K, Leicht G, Mulert C. Emotion regulation by cognitive reappraisal - The role of frontal theta oscillations. Neuroimage. (2013) 81:412–21. doi: 10.1016/j.neuroimage.2013.05.044
44. Hajcak G, Nieuwenhuis S. Reappraisal modulates the electrocortical response to unpleasant pictures. Cogn, Affect, Behav Neurosci. (2006) 6:291–7. doi: 10.3758/CABN.6.4.291
45. Moser JS, Hajcak G, Bukay E, Simons RF. Intentional modulation of emotional responding to unpleasant pictures: an ERP study. Psychophysiology. (2006) 43:292–6. doi: 10.1111/j.1469-8986.2006.00402.x
46. Moser JS, Krompinger JW, Dietz J, Simons RF. Electrophysiological correlates of decreasing and increasing emotional responses to unpleasant pictures. Psychophysiology. (2009) 46:17–27. doi: 10.1111/j.1469-8986.2008.00721.x
47. Parvaz MA, MacNamara A, Goldstein RZ, Hajcak G. Event-related induced frontal alpha as a marker of lateral prefrontal cortex activation during cognitive reappraisal. Cogn Affect Behav Neurosci. (2012) 12:730–40. doi: 10.3758/s13415-012-0107-9
48. Gross JJ, Thompson RA. Emotion regulation: Conceptual foundations, Handbook of Emotion Regulation. New York: The Guilford Press (2007). p. 3–26
49. Ochsner KN, Ray RD, Cooper JC, Robertson ER, Chopra S, Gabrieli JDE, et al. For better or for worse: Neural systems supporting the cognitive down- and up-regulation of negative emotion. Neuroimage. (2004) 23:483–99. doi: 10.1016/j.neuroimage.2004.06.030
50. Lang PJ, Bradley MM, Cuthbert BN. International Affective Picture System (IAPS): Instruction Manual and Affective Ratings. Technical Report A-8. Gainesville, FL: University of Florida (2008).
51. Bradley MM, Lang PJ. Measuring emotion: the self-assessment manikin and the semantic differential. J Behav Ther Exp Psychiatry. (1994) 25:49–59. doi: 10.1016/0005-7916(94)90063-9
52. Teegen F. Deutsche Übersetzung der Posttraumatic Stress Disorder Checklist (PCL-C) des National Center for PTSD. Boston, Hamburg: Universität Psychologisches Institut III (1997).
53. Freyberger HJ, Spitzer C, Stieglitz RD. Fragebogen zu Dissoziativen Symptomen - FDS. Bern: Huber (1999).
54. Spitzer C, Freyberger HJ, Stieglitz RD, Carlson EB, Kuhn G, Magdeburg N, et al. Adaptation and psychometric properties of the German version of the dissociative experience scale. J Trauma Stress. (1998) 11:799–809. doi: 10.1023/A:1024457819547
55. Nijenhuis ERS, Spinhoven P, Van Dyck R, Van der Hart O, Vanderlinden J. The development and psychometric characteristics of the somatoform dissociation questionnaire (SDQ-20). J Nerv Mental Dis. (1996) 184:688–94. doi: 10.1097/00005053-199611000-00006
56. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation (1996).
57. Laux L, Glanzmann P, Schaffner P, Spielberger CD. Das State-Trait-Angstinventar. Theoretische Grundlagen und Handanweisung. Weinheim: Beltz Test GmbH (1981).
58. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
59. Abler B, Kessler H. Emotion Regulation Questionnaire - Eine deutschsprachige Fassung des ERQ von Gross und John. Diagnostica. (2009) 55:144–52. doi: 10.1026/0012-1924.55.3.144
60. Jung T-P, Makeig S, Humphries C, Lee T-W, McKeown MJ, Iragui V, et al. Removing electroencephalographic artifacts by blind source separation. Psychophysiology. (2000) 37:163–78. doi: 10.1111/1469-8986.3720163
61. Pascual-Marqui RD. Standardized low-resolution brain electromagnetic tomography (sLORETA): Technical details. Methods Find Exp Clin Pharmacol. (2002) 24(Suppl D):5–12.
62. Pascual-Marqui RD. Instantaneous and lagged measurements of linear and nonlinear dependence between groups of multivariate time seriesfrequency decomposition. arXiv. (2007).
63. Pascual-Marqui RD, Lehmann D, Koukkou M, Kochi K, Anderer P, Saletu B, et al. Assessing interactions in the brain with exact low-resolution electromagnetic tomography. Philosophical transactions of the royal society a: mathematical, physical and engineering. Sciences. (2011) 369:3768–84. doi: 10.1098/rsta.2011.0081
64. Zalesky A, Fornito A, Bullmore ET. Network-based statistic: Identifying differences in brain networks. Neuroimage. (2010) 53:1197–207. doi: 10.1016/j.neuroimage.2010.06.041
65. Zalesky A, Cocchi L, Fornito A, Murray MM, Bullmore E. Connectivity differences in brain networks. Neuroimage. (2012) 60:1055–62. doi: 10.1016/j.neuroimage.2012.01.068
66. Xia M, Wang J, He Y. BrainNet Viewer: A network visualization tool for human brain connectomics. PLoS ONE. (2013) 8:e68910. doi: 10.1371/journal.pone.0068910
67. Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J Royal Stat Soc. (1995) 57:289–300. doi: 10.2307/2346101
68. Singmann H, Bolker B, Westfall J, Aust F. afex: Analysis of Factorial Experiments. R package version 0.17-8. (2017). Available online at: https://CRAN.R-project.org/package=afex.
69. Cohen J. Statistical Power Analysis for the Behavioral Science. 2nd ed. New York: Academic Press (1988).
70. Bakeman R. Recommended effect size statistics for repeated measures designs. Behav Res Methods. (2005) 37:379–84. doi: 10.3758/BF03192707
71. Svoboda E, McKinnon MC, Levine B. The functional neuroanatomy of autobiographical memory: a meta-analysis. Neuropsychologia. (2006) 44:2189–208. doi: 10.1016/j.neuropsychologia.2006.05.023
72. Maguire EA. Neuroimaging studies of autobiographical event memory. Philosophical Transactions of the Royal Society B. Biol Sci. (2001) 356:1441–51. doi: 10.1098/rstb.2001.0944
73. Conway MA, Pleydell-Pearce CW, Whitecross S, Sharpe H. Brain imaging autobiographical memory. Psychol Learn Motivat - Adv Res Theory. (2002) 41:229–63. doi: 10.1016/s0079-7421(02)80008-1
74. Spaniol J, Davidson PSR, Kim ASN, Han H, Moscovitch M, Grady CL. Event-related fMRI studies of episodic encoding and retrieval: meta-analyses using activation likelihood estimation. Neuropsychologia. (2009) 47:1765–79. doi: 10.1016/j.neuropsychologia.2009.02.028
75. Buhle JT, Silvers JA, Wage TD, Lopez R, Onyemekwu C, Kober H, et al. Cognitive reappraisal of emotion: a meta-analysis of human neuroimaging studies. Cerebral Cortex. (2014) 24:2981–90. doi: 10.1093/cercor/bht154
76. Kalisch R. The functional neuroanatomy of reappraisal: time matters. Neurosci Biobehav Rev. (2009) 33:1215–26. doi: 10.1016/j.neubiorev.2009.06.003
77. Kohn N, Eickhoff SB, Scheller M, Laird AR, Fox PT, Habel U. Neural network of cognitive emotion regulation - An ALE meta-analysis and MACM analysis. Neuroimage. (2014) 87:345–55. doi: 10.1016/j.neuroimage.2013.11.001
79. Greenberg DL, Rubin DC. The neuropsychology of autobiographical memory. Cortex. (2003) 39:687–728. doi: 10.1016/S0010-9452(08)70860-8
80. Schlumpf YR, Nijenhuis ERS, Klein C, Jäncke L, Bachmann S. Resting-state functional connectivity in patients with a complex PTSD or complex dissociative disorder before and after inpatient trauma treatment. Brain Behav. (2021) 11:e02200. doi: 10.1002/brb3.2200
81. Markowitsch HJ, Staniloiu A. Memory, autonoetic consciousness, and the self. Conscious Cogn. (2011) 20:16–39. doi: 10.1016/j.concog.2010.09.005
82. Chiu C De, Tollenaar MS, Yang CT, Elzinga BM, Zhang TY, Ho HL. The loss of the self in memory: self-referential memory, childhood relational trauma, and dissociation. Clin Psychol Sci. (2019) 7:265–82. doi: 10.1177/2167702618804794
83. Chiu C De, Tseng MCM, Chien YL, Liao SC, Liu CM, Yeh YY, et al. Misattributing the source of self-generated representations related to dissociative and psychotic symptoms. Frontiers in Psychology. (2016) 7:541. doi: 10.3389/fpsyg.2016.00541
84. Brand BL, Classen CC, Lanius R, Loewenstein RJ, McNary S, Pain C, et al. naturalistic study of dissociative identity disorder and dissociative disorder not otherwise specified patients treated by community clinicians. Psychological Trauma: Theory, Research, Practice, and Policy. (2009) 1:153–71. doi: 10.1037/a0016210
85. Brand BL, McNary SW, Myrick AC, Classen CC, Lanius R, Loewenstein RJ, et al. longitudinal naturalistic study of patients with dissociative disorders treated by community clinicians. Psychological Trauma: Theory, Research, Practice, and Policy. (2013) 5:301–8. doi: 10.1037/a0027654
86. Jepsen EKK, Langeland W, Sexton H, Heir T. Inpatient treatment for early sexually abused adults: A naturalistic 12-month follow-up study. Psychological Trauma: Theory, Research, Practice, and Policy. (2014) 6:142–51. doi: 10.1037/a0031646
87. Zhu X, Suarez-Jimenez B, Lazarov A, Helpman L, Papini S, Lowell A, et al. Exposure-based therapy changes amygdala and hippocampus resting-state functional connectivity in patients with posttraumatic stress disorder. Depress Anxiety. (2018) 35:974–84. doi: 10.1002/da.22816
88. Cisler JM, Steele JS, Lenow JK, Smitherman S, Everett B, Messias E, et al. Functional reorganization of neural networks during repeated exposure to the traumatic memory in posttraumatic stress disorder: an exploratory fMRI study. J Psychiatr Res. (2014) 48:47–55. doi: 10.1016/j.jpsychires.2013.09.013
89. Shou H, Yang Z, Satterthwaite TD, Cook PA, Bruce SE, Shinohara RT, et al. Cognitive behavioral therapy increases amygdala connectivity with the cognitive control network in both MDD and PTSD. NeuroImage: Clin. (2017) 14:464–70. doi: 10.1016/j.nicl.2017.01.030
90. Helpman L, Marin MF, Papini S, Zhu X, Sullivan GM, Schneier F, et al. Neural changes in extinction recall following prolonged exposure treatment for PTSD: A longitudinal fMRI study. NeuroImage: Clin. (2016) 12:715–23. doi: 10.1016/j.nicl.2016.10.007
91. Prichard E, Propper RE, Christman SD. Degree of handedness, but not direction, is a systematic predictor of cognitive performance. Front Psychol. (2013) 4:9. doi: 10.3389/FPSYG.2013.00009/BIBTEX
92. Luders E, Cherbuin N, Thompson PM, Gutman B, Anstey KJ, Sachdev P, et al. When more is less: Associations between corpus callosum size and handedness lateralization. Neuroimage. (2010) 52:43–9. doi: 10.1016/J.NEUROIMAGE.2010.04.016
93. Propper RE, Christman SD, Phaneuf KA, A. mixed-handed advantage in episodic memory: a possible role of inter-hemispheric interaction. Mem Cognit. (2005) 33:751–7. doi: 10.3758/BF03195341
94. Jäncke L, Staiger JF, Schlaug G, Huang Y, Steinmetz H. The relationship between corpus callosum size and forebrain volume. Cerebral Cortex. (1997) 7:48–56. doi: 10.1093/CERCOR/7.1.48
Keywords: complex trauma, dissociation, trauma treatment, electroencephalography, functional connectivity
Citation: Schlumpf YR, Nijenhuis ERS, Klein C, Jäncke L and Bachmann S (2022) Functional connectivity changes in the delta frequency band following trauma treatment in complex trauma and dissociative disorder patients. Front. Psychiatry 13:889560. doi: 10.3389/fpsyt.2022.889560
Received: 04 March 2022; Accepted: 27 June 2022;
Published: 25 July 2022.
Edited by:
Emine Elif Tülay, Muğla University, TurkeyReviewed by:
Tuba Aktürk, Istanbul Medipol University, TurkeyAamir Malik, Brno University of Technology, Czechia
Copyright © 2022 Schlumpf, Nijenhuis, Klein, Jäncke and Bachmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yolanda R. Schlumpf, eS5zY2hsdW1wZkBwc3ljaG9sb2dpZS51emguY2g=